Lumbar Disc Herniation & Micro-Disectomy Surgery
Chiropractor, Dr. Alex Jimenez looks at lumbar spine disc herniation. What are the Likely signs and symptoms associated with disc herniation, and what would be the selection criteria for micro-discectomy operation in athletes? Complaint in the young college age athlete and professional athlete, and it’s been estimated that over 30% of athletes complain of back pain at least once in the profession(1).
Lumbar spinal disc herniation is one kind Of lumbar injury that can’t just cause painful low back pain, but can also compress nerve roots and create radicular referral of pain into the lower leg with related sensation changes and muscle contraction. This injury will not only influence the short-term opponent ability of the athlete, but might also reoccur and eventually become persistent possibly causing a career ending injury.
Managing disc herniation from the athlete Usually begins with conservative therapy and if this fails, surgical solutions are considered. But often elite athletes will request a quicker resolution to their symptoms to minimize time away from competitors. Therefore, providing the criteria for lumbar spine surgery are suggested, the conservative period will often be compressed, and surgery will be sought earlier. The favored surgical process for the athlete with a disc herniation is that the lumbar disc micro-discectomy.
Anatomy & Biomechanics
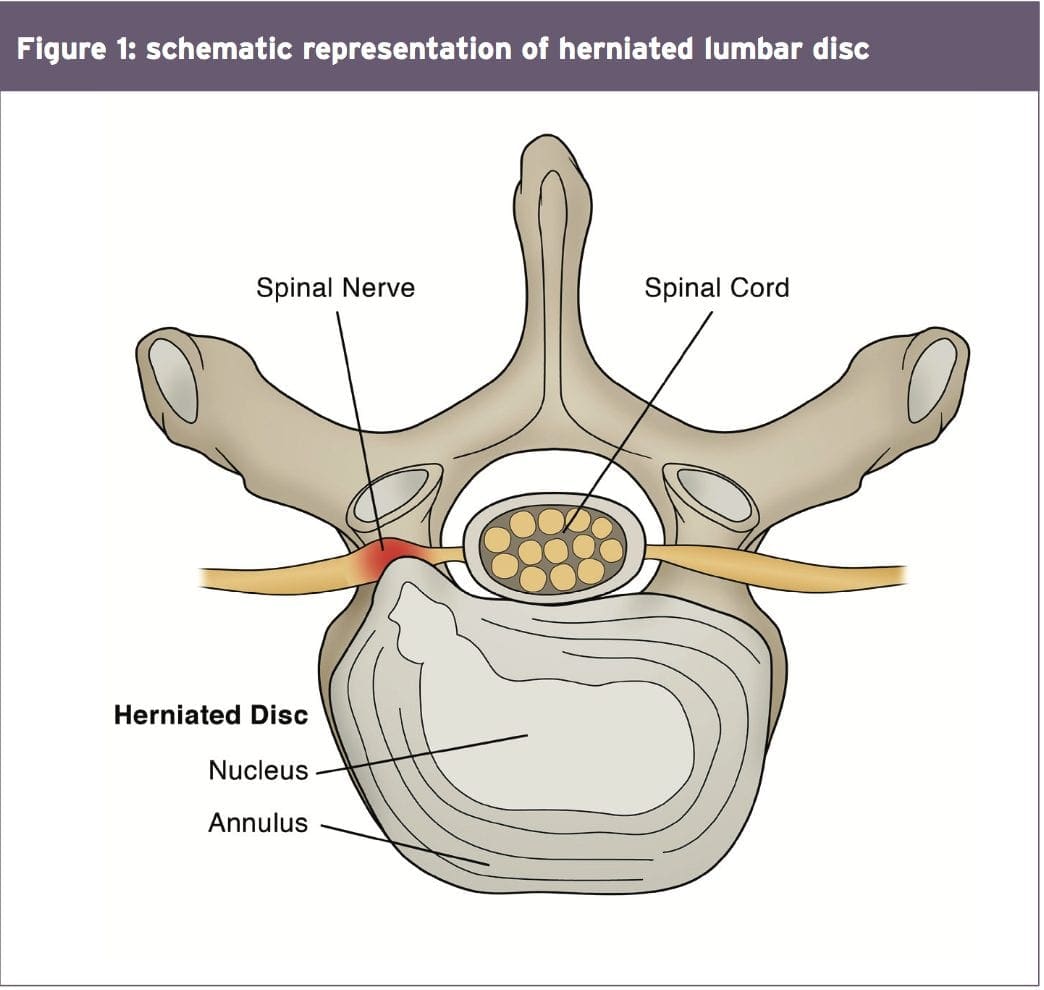
A significant biomechanical role in the spine, allowing for motion between the spinal segments while spreading compressive, shear, and torsional forces(2). These discs include a thick outer ring of fibrous cartilage termed the annulus fibrosis (akin to the onion rings enclosing the center of the onion), which encompasses a more gelatinous core called the nucleus pulposus, which is included within the cartilage end plates inferiorly and superiorly.
The intervertebral disc consists of Cells and substances such as collagen, proteoglycans, and thin fibrochondrocytic tissues, which enable transmission and absorption of forces arising from body weight and muscle activity. To do so, the disc depends mainly on the structural condition of the nucleus pulposus, annulus fibrosis and the vertebra lend plate. If the disc is normal and is functioning optimally, then forces are spread across the disc evenly(3).
But disc degeneration (mobile Degradation, lack of hydration( disc failure) may decrease the capacity of the disc to withstand extrinsic forces, as forces are no longer distributed and spread evenly. Tears and fissures from the annulus can lead, and with adequate external forces, the disc material may herniate. Alternatively, a sizable biomechanical force set on a healthy, ordinary disc may cause extrusion of disc material as a result of crushing failure of this annular fibers — illustrations include a hefty compression type mechanism because of a fall on the tailbone, or strong muscle contraction such as heavy weight lifting(4).
Herniations represent protrusions of Disc material beyond the confines of this annular lining and in the spinal canal (see Figure 1)(5). If the protrusion does not invade the canal or undermine nerve roots then back pain may be the only symptom.
Endoscopic Discectomy 3D Simulation
The pain associated with lumbar Radiculopathy happens due to a mix of nerve root ischemia (due to compression) and inflammation (because of neurochemical inflammatory mediators released from the disc). Throughout a herniation, the nucleus pulposus puts pressure on weakened regions of the annulus, and proceeds through the diminished websites in the annulus in which it ultimately forms a herniation(6 ft). It follows from this that some kind of disc degeneration may exist prior to the disc may really herniated(7).
In contrast to other respiratory Tissues, discs have a inclination to degenerate earlier in life, with some studies demonstrating adolescents presenting signs of degeneration between the ages of 11 to 16(8). With increasing age, there’s further degeneration of the intervertebral discs.
While the disc might be in danger of harm in All fundamental planes of motion, it’s particularly susceptible during repetitive flexion, or hyper-flexion, combined with lateral bending or rotation(10). Traumatic events such as excessive axial compression may also damage the inner structure of the disc. This can occur as a result of a fall or powerful muscular forces developed during tasks such as heavy lifting.
Athletes are generally exposed to high loading conditions. Examples of this include:
1. World-class power lifters, in which the calculated compressive loads on the backbone are involving 18800 Newtons (N) and also 36400N acting in the L3-4 motion segment(11).
2. Elite level football linesmen who have Been proven to present time-related hypertrophy of this disc and changes in vertebrae endplate in response to this repetitive high loading and axial pressure(12).
3. Long distance runners have been Shown to undergo significant strain into the intervertebral disc, indicated by a reduction in disc height(13).
Herniations could be classified depending on Ultimately, herniations are also identified based on level, with most herniations happening at the L4/5 and L5/S1 intervertebral disc level; these can then in turn affect the L5 and S1 nerve roots resulting in clinical sciatica(15). Upper level herniations are less common, and when they do occur with radiculopathy, they will affect the femoral nerve. Finally, the prevalence of disc injury rises increasingly caudally, with the best numbers at the L5/S1 degrees(16).
Herniation In Athletes
The offending movements implicated in The 20-35 age group are the most common group to herniate a disc, most likely because of the fluid nature of the nucleus pulposis and due to behavior(18). This age group are more likely to participate in sports which need high lots of flexion and spinning or are reckless with their positions and positions during loading.
The sports most at risk of disc herniation are:
- Hockey
- Wrestling
- Soccer
- Swimming
- Basketball
- Golf
- Tennis
- Weightlifting
- Rowing
- Throwing events
These are the sports that involve either significant Furthermore, those who take part in more and more severe training regimes seem to be at higher risk of spinal pathologies, as do people involved in sports.
Signs & Symptoms Indicating Discectomy
The efficacy of management programs for lumbar spine disc herniation — in terms of the decision to operate or treat conservatively — will be discussed in greater depth in part 2 of this series. However, the decision to operate within an athlete is generally driven by the motivation and approaching goals the athlete has put themselves. They may in fact favor a comparatively simple micro-discectomy instead of waiting for symptoms to abate through an extended period of rehabilitation.
This conservative period of Management may involve medicine therapy, epidural injections, relative back and back muscle recovery, acupuncture, osteo/chiropractic interventions. On the other hand, the normal presenting symptoms and signs that suggest a substantial disc herniation that will require surgical intervention in the athlete comprise:
- Low back pain with pain radiating down one or both legs
- Positive straight leg raise test
- Radicular pain and neurological signs consistent with the nerve root level affected
- Mild weakness of distal muscles such as extensor hallucis longus, peroneals, tibialis anterior and soleus. These would fit with the myotome relevant for the disc level
- MRI confirming a disc herniation
- Possible bladder and bowel symptoms
- Failed conservative rehabilitation
Time span in which to enable conservative rehabilitation to be effective. In the overall population, medical practitioners will most likely prescribe a minimal 6-week traditional period of treatment with an overview at 6 weeks as to whether to expand the rehabilitation a further 6 weeks or to seek a specialist opinion. The expert may then attempt more medically orientated interventions such as epidural injections.
The athlete nevertheless will have these They might be more inclined to experience an epidural very early in the conservative period to assess the effectiveness of this procedure. If no signs of progress are evident in a couple of weeks then they may choose to get an immediate lumbar spine micro- discectomy.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques. From the El Paso, TX. Spine Center.
Imaging
MRI remains the favored system of Identifying lumbar spine disc herniation, since it’s also very sensitive to detecting nerve root impingements(23). However, abnormal MRI scans can occur in otherwise asymptomatic patients(25); hence, clinical correlation is always essential before any surgical thought. What’s more, patients can present with clinical signs and symptoms which suggest the diagnosis of acute herniated disc, and yet lack evidence of sufficient pathology on MRI to warrant operation.
Therefore it has been proposed that a Volumetric analysis of a herniated disc on MRI may be potentially beneficial in checking the suitability for operation. Several writers have previously mentioned the possible value of volumetric evaluation of herniated disc on MRI as part of their selection criteria for lumbar surgery(26).
In a survey conducted in Michigan State University, it was found that the size and positioning of the herniated disc determined that the likelihood for operation with what researchers called ‘types 2-B’ and ‘types 2-AB’ being the most likely candidates for surgery(27).
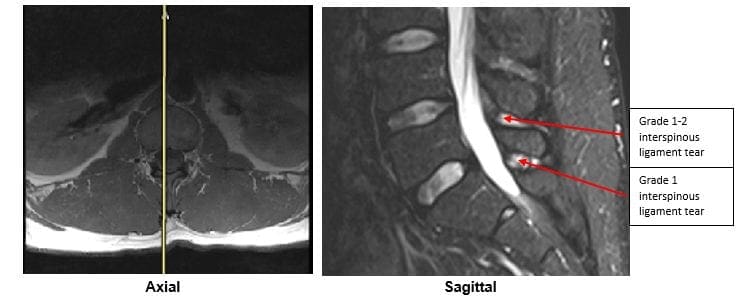
The MRI protocol to your lumbar spine consists of (see Figure 2)
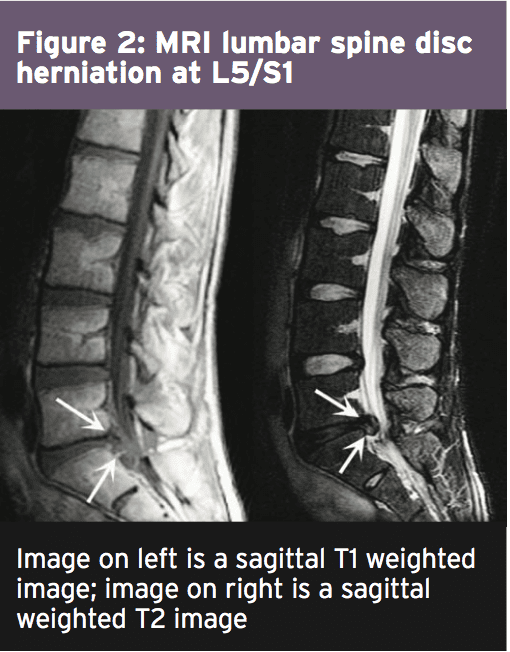
1.Sagittal plane echo T1- weighted sequence
2. Sagittal fast spin echo proton density sequence
3. Sagittal fast spin echo inversion recovery sequence
4.Axial spin echo T1- weighted sequence
Summary
Disc herniations are not a common Complaint in athletes, but they do happen in sports which involve high loads or repetitive flexion and rotation movements. Sufferers of a disc herniation will normally feel focused low-back pain, maybe with referral in the lower limb with associated neurological symptoms if the nerve root was compressed.
Managing a disc herniation within an General population as frequently the risk of a Protracted failed rehabilitation period is Bypassed for the protected and low risk Micro-discectomy procedure. In the Discuss the exact surgical alternatives involved Observing a lumbar spine micro-discectomy.
References
1. Sports Med. 1996;21(4):313�20
2. Radiology. Oct 2007;245(1):62-77
3. Arthritis Research & Therapy. 2003;5(3):120-30
4. The Journal of Bone and Joint Surgery. American volume. Feb 2004;86-A(2):382 � 96
5. Radiology. Oct 2007;245(1):43-61
6. Spine. Sep 15 1996;21(18):2149-55
7. Spine. May-Jun 1982;7(3):184-91
8. Spine. Dec 1 2002;27(23):2631-44
9. Lancet 1986;2:1366�7
10. Disease-A-Month:DM. Dec 2004;50(12):636-69
11. Spine. Mar 1987;12(2):146-9
12. The American Journal of Sports Medicine. Sep 2004;32(6):1434-9
13. The Journal of International Medical Research. 2011;39(2):569-79
14. Spine. 2001;26:E93-113
15. Spine. 1990;15:679-82
16. British Journal of Sports Medicine. Jun 2003;37(3):263-6
17. Prim Care. 2005;32(1):201�29
18. McGill, S.M. Low back disorders: Evidence based prevention and rehabilitation, Human Kinetics Publishers, Champaign, IL, U.S.A., 2002. Second Edition, 2007
19. Spine. Apr 1991;16(4):437-43
20. Skeletal radiology. Jul 2006;35(7):503-9
21. British Journal of Sports Medicine. Nov 2007;41(11):836-41
22. The American Journal of Sports Medicine. Jun 2009;37(6):1208-13
23. Spine. Mar 15 1995;20(6):699-709
24. Phys Sportsmed. 2005;33(4):21�7
25. J Bone Joint Surg Am 1990 . 2:403�408
26. J Orthop Surg (Hong Kong) 2001. 9:1�7
27. Eur Spine J (2010) 19:1087�1093



 Hip Pain
Hip Pain