For individuals about to engage in physical activity or exercise, how does warming up the body help prepare for the work ahead?
Central Nervous System Activation
A proper warm-up before physical activity or working out prepares the mind and body to reduce risks of injury, mentally and physically transition to physical activity work, and enhance performance. A well-designed warm-up also primes the central nervous system/CNS for activity. The central nervous system transmits messages to the muscles to prepare them for action. Central nervous system activation increases motor neuron recruitment and engages the sympathetic nervous system so the body can better handle the physical stressors. The process may seem complex, but priming the nervous system is as simple as warming up with light aerobic activity before getting into more explosive movements.
CNS
The CNS consists of the brain and spinal cord. This central communication system uses another part of the nervous system known as the peripheral nervous system or PNS to transmit and receive messages throughout the body. The PNS is connected to the entire body and the brain and spinal cord (CNS).
Nerves run throughout the body, receiving signals from the CNS to the muscles, fibers, and organs, transmitting various information back to the brain. (Berkeley University. N.D.)
There are two types of systems within the peripheral nervous system – somatic and autonomic.
Somatic nervous system actions are those controlled by the person through voluntary actions like choosing to pick something up.
Properly preparing the body for an intense strength training session or other physical activity needs the correct messages to be sent through the autonomic nervous system.
Parasympathetic and Sympathetic States
The autonomic nervous system consists of two subcategories, which are parasympathetic and sympathetic.
The sympathetic nervous system helps the body get ready to face stress which includes physical stress. (R. Bankenahally, H. Krovvidi. 2016)
The fight, flight, or freeze response describes the sympathetic nervous system’s aspect.
The parasympathetic nervous system is responsible for relaxation and de-stressing.
Individuals are recommended to perform a few calming movements and actions after a workout to return the body to a parasympathetic state. This can be:
Activating the CNS can increase performance and prevent injuries. The process wakes up and alerts the body for the activity. Individuals are recommended before beginning a training session, to communicate to the body about the physical stress it is about to endure and to prepare for the work ahead. This is a concept known as post-activation potentiation/PAP. (Anthony J Blazevich, Nicolas Babault. 2019) PAP helps increase force and power production, which enhances physical performance.
Whenever an individual trains, the brain adapts and learns what the body is doing and the purpose of the training.
Muscle memory describes this interaction.
Individuals who have started up a new strength training routine or after an extended break report feeling awkward for the first few sessions, or even weeks, depending on their experience. (David C Hughes, Stian Ellefsen, Keith Baar, 2018)
However, after a few sessions, the body is more adept at performing the movements and ready to increase resistance, repetitions, or both.
This has to do with the neural drive and muscle memory than it has to do with true potential physical abilities. (Simon Walker. 2021)
The first step is a general warm-up that should use large muscle groups and be of low intensity so as not to exhaust the body before beginning the actual training. General warm-up benefits central nervous system activation and the entire body include: (Pedro P. Neves, et al., 2021) (D C. Andrade, et al., 2015)
Increases blood circulation.
Assists the release of oxygen from hemoglobin and myoglobin.
Warms the muscles, so they contract more effectively.
Increases nerve impulse speed.
Increases nutrient delivery.
Lowers joints’ resistance through increased synovial fluid/joint lubrication.
Increases joint range of motion.
Improves joint resiliency.
Removes metabolic waste quicker.
Reduces risk of injury.
A general warm-up can be simple as any aerobic activity will work. This can include:
Performing bodyweight movements – light jumping jacks or jogging in place.
Treadmill
Rowing machine
Stair climber
Elliptical trainer
It is recommended to use the rating perceived exertion scale/RPE to determine the general warm-up effort. An exertion rating of between 5 to 6 is equivalent to moderate walking or a slow jog. Individuals should be able to speak clearly without taking a pause.
Try this strategy before the next workout to see increased performance and reduced injury risks.
Blazevich, A. J., & Babault, N. (2019). Post-activation Potentiation Versus Post-activation Performance Enhancement in Humans: Historical Perspective, Underlying Mechanisms, and Current Issues. Frontiers in physiology, 10, 1359. https://doi.org/10.3389/fphys.2019.01359
Hughes, D. C., Ellefsen, S., & Baar, K. (2018). Adaptations to Endurance and Strength Training. Cold Spring Harbor perspectives in medicine, 8(6), a029769. https://doi.org/10.1101/cshperspect.a029769
Walker S. (2021). Evidence of resistance training-induced neural adaptation in older adults. Experimental gerontology, 151, 111408. https://doi.org/10.1016/j.exger.2021.111408
Andrade, D. C., Henriquez-Olguín, C., Beltrán, A. R., Ramírez, M. A., Labarca, C., Cornejo, M., Álvarez, C., & Ramírez-Campillo, R. (2015). Effects of general, specific, and combined warm-up on explosive muscular performance. Biology of sport, 32(2), 123–128. https://doi.org/10.5604/20831862.1140426
Chiropractic is a form of neuromusculoskeletal care that repairs and re-optimizes the nervous system that helps to relieve tension, inflammation, pain and restore body health. Like any piece of machinery that requires regular maintenance to operate correctly without issues, so too is the body an exquisite machine that needs regular maintenance. Treatment restores and maintains optimal function to the nervous system, muscles, bones, tendons, ligaments, and joints.
Neuromusculoskeletal Care
Central Nervous System – CNS
The Central Nervous System or CNS is the body’s computer.
It processes functions in the body and mind.
It s made up of the brain and spinal cord.
It helps process external information through sight, sound, touch, smell, and taste.
The CNS interprets sensory information that goes through the spinal cord to the brain, and the body responds accordingly.
It controls voluntary movements like walking, talking, exercising.
It controls involuntary movements like blinking, breathing, digestion.
It allows thoughts, emotions, and perceptions to be created and expressed.
When the Central Nervous System works correctly, the body is coordinated, all senses send and receive information effectively, and cognition/thinking is clear.
Peripheral Nervous System – PNS
The Peripheral Nervous System or PNS transmits signals from the outside to the Central Nervous System.
The PNS is comprised of all the nerve bundles that run throughout the body.
The PNS is responsible for transmitting information back and forth from the CNS to the rest of the body by electrical impulses and current.
When the PNS is functioning correctly, and there is thorough nerve circulation throughout the body, there are no issues like numbness, weakness, pain, and digestion is in top form.
Enteric Nervous System – ENS
The Enteric Nervous System or ENS is a branch of the peripheral nervous system that signals the digestive system.
It comprises nerves that stretch across the entire gastrointestinal tract.
It allows the nervous system to communicate with the digestive tract and regulate activity.
It can stop the digestive process when the body is under stress or strain, i.e., fight or flight response.
Inflammation and stress can cause the enteric system to disrupt and cause digestive problems.
Pain Relief
Body pain can be an indication of an imbalance in the nervous system. Misalignment from work, home activities, trauma, injury, or posture problems, a subluxation/misalignment can turn into discomfort that leads to pain and neuromusculoskeletal system issues. Pain in the neuromusculoskeletal system can result from spinal misalignment and a shifting skeletal structure. The joints and misaligned bones compress the surrounding nerves and tissue, causing inflammation that results in pain symptoms. This causes the muscular system to compensate for the lack of stability support from the skeletal structure causing awkward body posturing. A chiropractor realigns the spinal structure, removing the compression/pressure from the nerves, tissues, muscles, ligaments, and tendons.
Body Composition
Chiropractic Medicine
The nervous system is highly responsive to chiropractic care because of chiropractic’s focus on the spine, which restores and rejuvenates. Chiropractic medicine and a properly aligned spine:
Reduces and eliminates pain.
Reduces and eliminates headaches and migraines.
Improves balance and coordination.
Improves digestive function.
Improves quality of sleep.
Increases energy.
Increases flexibility and mobility.
Enhances cognition and clear thinking.
References
Goudman, Lisa et al. “The Link Between Spinal Cord Stimulation and the Parasympathetic Nervous System in Patients With Failed Back Surgery Syndrome.” Neuromodulation: journal of the International Neuromodulation Society vol. 25,1 (2022): 128-136. doi:10.1111/ner.13400
Gyer, Giles et al. “Spinal manipulation therapy: Is it all about the brain? A current review of the neurophysiological effects of manipulation.” Journal of integrative medicine vol. 17,5 (2019): 328-337. doi:10.1016/j.joim.2019.05.004
Millet, Guillaume Y et al. “The role of the nervous system in neuromuscular fatigue induced by ultra-endurance exercise.” Applied physiology, nutrition, and metabolism = Physiologie appliquee, nutrition et metabolisme vol. 43,11 (2018): 1151-1157. doi:10.1139/apnm-2018-0161
Stoll, T et al. “Physiotherapie bei lumbaler Diskushernie” [Physiotherapy in lumbar disc herniation ]. Therapeutische Umschau. Revue therapeutique vol. 58,8 (2001): 487-92. doi:10.1024/0040-5930.58.8.487
Microglial cells make up about 10 to 15 percent of all the glial cells in the human body, which can be found in the central nervous system (CNS) and play a fundamental role in the human brain. Microglial cells are responsible for maintaining and regulating changes in the physiological and pathological condition of the CNS by changing their morphology, phenotype and function. In an average physiological state, the microglial cells are continuously in charge of controlling their environment. �
However, when the homeostasis of the brain is interrupted, the microglia change into an amoeba-like shape and become a phagocyte where they can actively reveal a variety of antigens. If the homeostasis interruption in the CNS continues, the microglial cells will then trigger at a much stronger state, which is known as microglial priming. Microglia are the “Bruce Banner” of the CNS. However, once they go into protective “Hulk” mode, primed microglia become much more sensitive to stimulation and they have a much stronger possibility of reacting to stimulation, even reacting towards normal cells. �
�
Microglial priming can become a double-edged sword. As a matter of fact, primed microglia are created from different phenotypes of microglia and the phenotypes are context-dependent, which means they are associated to the sequence and duration of their exposure to different varieties of stimulation in a variety of pathologies. In the article below, we will demonstrate the effect of microglial priming on the central nervous system (CNS), especially in neurological diseases. �
Role of Microglial Cells in the CNS
Microglial cells are commonly found in the central nervous system (CNS), where they are considered to be one of the most flexible types of brain cells. Microglial cells are created from precursor cells found within mesoderm bone marrow, or more specifically found in the mesodermal yolk sac, and they are divided in different densities throughout several regions of the brain. As mentioned above, microglia will remain in a dormant state when the homeostasis of the brain remains stable. �
Microglia have a small cell body and morphological branches which extend towards all directions to help maintain and regulate the overall function of the CNS. Changes in their microenvironment can trigger microglia into an “activated� state. Research studies have demonstrated that microglia play a fundamental role in brain development and a variety of functions, including synaptic pruning and clearing out cell debris. Moreover, microglia create an immune surveillance system in the human brain and control fundamental processes associated with a variety of pathologies, including the clearance and uptake of A? and abnormal tau protein as well as the production of neurotrophic factors and neuroinflammatory factors. �
Microglial Priming Overview
Microglial priming activates when continuous interruptions in the brain’s microenvironment trigger a much stronger microglial response compared to an initial interruption which simply triggers microglial activation. Primed microglia in the CNS are also much more sensitive to possibly minor stimulation. This increased response involves microglial proliferation, morphology, physiology, and biochemical markers or phenotype. However, these changes will ultimately promote an increase in cytokines and inflammation mediator production which can have a tremendous impact on synaptic plasticity, neuronic survival, individual cognitive and behavioral function. Below is an overview of the effects of microglial priming in the CNS. �
Mechanisms of Microglial Priming in the CNS
The microenvironment of the central nervous system (CNS), by way of instance, is one of the main factors which can affect the microglial cells. Increased oxidative stress, lipid peroxidation and DNA damage associated with brain aging can all commonly trigger microglial priming. Another common factor for microglial priming includes traumatic brain injury. Research studies have shown that traumatic CNS injury activates microglia as well as the development of primed microglia. �
Many research studies have also shown that both focal and diffuse traumatic brain injury increase inflammation in the brain associated with microglia and astrocytes. CNS infections can also trigger microglial priming where viruses are the main cause of CNS infection. Both DNA and RNA viruses can trigger microglial priming including microglia and astrocytes. Recent research studies have shown that complement dysfunction can change the expression of complement receptors and trigger microglial priming after continuous activation following a variety of functions, including synapse maturation, immune product clearance, hematopoietic stem/progenitor cells (HSPC) mobilization, lipid metabolism, and tissue regeneration. �
Moreover, research studies have shown that there is increased priming of the microglia in a variety of neurological diseases. By way of instance, microglial cells with a morphological phenotype are found in large numbers in the human brain. In the last several years, research studies have suggested that neuroinflammation can continuously activate the microglia and trigger microglial priming. Furthermore, all of the previously mentioned situations are closely associated with neuroinflammation. Research studies have also demonstrated that neuroinflammation, as well as microbial debris and metabolic effects, are associated with central sensitization in neurological diseases, such as fibromyalgia, also referred to as the “brain on fire”. �
In the context of the previous situations mentioned above, microglia are primed though a series of pro-inflammatory stimulation, such as lipopolysaccharide (LPS), pathogenetic proteins (e.g., A?), ?synuclein, human immunodeficiency virus (HIV)-Tat, mutant huntingtin, mutant superoxide dismutase 1 and chromogranin A. There is also a variety of signaling pathways and it is common for different types of cells to express special pattern recognition receptors (PRRs) which can affect inflammatory signaling pathways. By way of instance, several signaling pathways, known as pathogen-associated molecular patterns (PAMPs), which can commonly increase in infected tissue, could also control microbial molecules. �
Additionally, peptides or mislocalized nucleic acids identified as misfolded proteins through a series of pathways, known as danger-associated molecular patterns (DAMPs), can also cause microglial priming. Toll-like receptors (TLRs) and carbohydrate-binding receptors commonly function in these pathways. There are also many different receptors found in microglia, including triggering receptors expressed on myeloid cells (TREM), Fc? receptors (Fc?Rs), CD200 receptor (CD200R), receptor for advanced glycation end products (RAGE), chemokine receptors (CX3CR1, CCR2, CXCR4, CCR5, and CXCR3), which can be recognized and mixed in with other signaling pathways, although some pathways are still not clear. �
Consequences of Microglial Priming in the CNS
Microglia show a low rate of mitosis in their normal state and a high rate of proliferation after microglial priming, showing that the microglia have the ability to affect cell turnover and pro-inflammation stimulation. With continued stimulation, microglia activate from their resting state, changing into amoeboid microglial cells in morphology. However, the changes in the shape of the microglia cannot differentiate the characteristics of microglial activation and the function of primed microglia depends on their phenotypes which are associated with receptors and molecules which they create and recognize. �
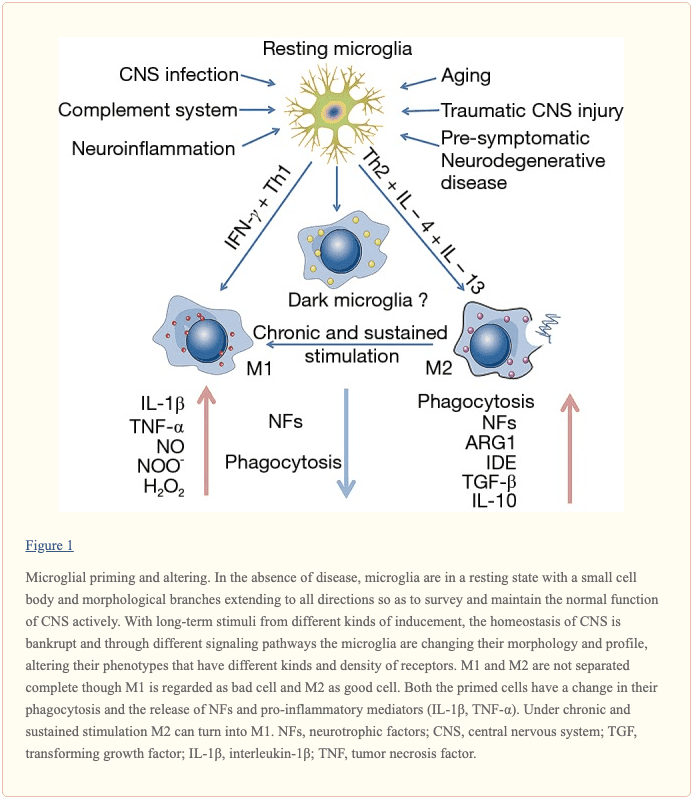
The different types of tissue macrophages, under microenvironmental impetus, are able to differentiate M1 and M2 phenotypes. First, M1 polarization, also known as classical activation, ultimately needs interferon-? (IFN-?) to be mixed with TLR4 signaling which then causes the production of inducible nitric oxide synthases (iNOS), reactive oxygen species (ROS), proinflammatory cytokines, and finally, ultimately reduces the release of neurotrophic factors, ultimately causing inflammation with increased markers of main histocompatibility complex II (MHC II), interleukin-1? (IL-1?) and CD68. �
Moreover, M2 polarization, also known as alternative activation, is ultimately believed to be associated with tissue-supportive in the situation of wound healing, reducing inflammation and improving tissue repair of collagen form. They trigger in response to IL-4 and IL-13 in vivo. M2 polarization is characterized by the increased expression of neurotrophic factors, proteases, enzymes arginase 1 (ARG1), IL-10 transforming growth factor-? (TGF-?), scavenger receptor CD206 and coagulation factors as well as improving phagocytic activity. As a matter of fact, there are currently no clear boundaries between the two polarizations and the M1 phenotype shares many similar characteristics with the M2 phenotype. �
Another phenotype of primed microglia, known as acquired deactivation, has been recently discovered. This new phenotype overlaps with M2 and has the ability to improve anti-inflammatory and functional recovery. Additionally, a research study conducted ultra-structural analyses and identified a brand-new phenotype, known as �dark microglia�, which is rarely seen in the microglial cell’s resting state. Systemic inflammation triggers microglia into an activated state to promote cell and tissue recovery and achieve homeostasis. Microglial priming is ultimately the second interruption in the CNS microenvironment. �
The primed microglia is a double-edged sword for brain health. Many research studies in vivo and in vitro have shown that neurological diseases are associated with microglial activation. The inflammatory phenotypes of the microglia create neurotoxic factors, mediators and ROS which can affect the CNS. Primed microglia play a fundamental and beneficial role in neuronal regeneration, repair, and neurogenesis. Primed microglia are also much more sensitive and respond much stronger to brain injury, inflammation, and aging as well as increase the activation of microglial cells by switching from an anti-inflammation, potentially protective phenotype to a pro-inflammation destructive phenotype, as shown in (Figure 1). �
�
In the early stages of microglial priming, the ability and function to phagocytize cell debris, misfolded proteins, and inflammatory medium are increased where more protective molecules, such as IL-4, IL-13, IL-1RA, and scavenging receptors, are created. The changes can affect wound healing and damage tissue repairment, neuron protection, and homeostasis recovery. Classically activated microglia (M1) make up a large proportion of all microglia and promote an increased creation of neurotoxic factors, such as IL-1?, TNF-?, NO and H2O2 (6), where more microglia are primed immediately afterward. �
This increased and extended neuroinflammation caused by primed microglia can ultimately be associated with the development and clustering of the protein tau and A?. Furthermore, it can lead to loss of neurons as well as the decrease of cognitive function and memory, such as in Alzheimer’s disease. Although the mechanisms are not clear enough, people have reached an agreement that primed microglia cause a chronic proinflammatory response and a self-perpetuating cycle of neurotoxicity. And this is believed to be the key factor in brain health issues resulting in neurological diseases. �
Microglia are known as the protectors of the brain and they play a fundamental role in maintaining as well as regulating the homeostasis of the CNS microenvironment. Constant stimulation causes the microglia to trigger at a much stronger state, which is known as microglial priming. Microglial cells are the “Bruce Banner” of the CNS. However, once they go into protective “Hulk” mode, primed microglia become much more sensitive to stimulation and they have a much stronger possibility of reacting to stimulation, even reacting towards normal cells. �- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Microglial cells make up about 10 to 15 percent of all the glial cells in the human body, which can be found in the central nervous system (CNS) and play a fundamental role in the human brain. Microglial cells are responsible for maintaining and regulating changes in the physiological and pathological condition of the CNS. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download�
* All of the above XYMOGEN policies remain strictly in force.
Central nervous system, or CNS, infections can be life-threatening if they are not diagnosed and treated early. Because CNS infections are non-specific, determining an accurate diagnosis can be challenging. The nucleic acid in vitro amplification-based molecular methods are starting to be utilized for routine microbial diagnosis. These molecular methods have improved beyond conventional diagnostic techniques with increased sensitivity and specificity. Moreover, molecular methods utilized on cerebrospinal fluid samples are considered the new standard for diagnosis of CNS infections caused by pathogens. �
Molecular methods for the diagnosis of CNS infections offers a variety of monoplex and multiplex PCR assays to diagnose several types of health issues. Pan-omic molecular platforms can also help diagnose CNS infections. Although molecular methods are utilized for the diagnosis of CNS infections, the outcome measures for these diagnostic techniques must be carefully identified by healthcare professionals. The following article discusses conventional diagnostic techniques and molecular methods utilized for the diagnosis of central nervous system infections, their application, and future approaches. �
Molecular Methods in the Diagnosis of CNS Infections
Because of increased sensitivity and specificity, nucleic acid in vitro amplification-based molecular methods has tremendously improved the ability to diagnose CNS infections in a reasonable and effective time frame. Several PCR-derived techniques have also ultimately increased the flexibility and rigor of currently available diagnostic techniques. �
Reverse transcriptase, or RT,-PCR was developed to increase RNA targets. Its utilization plays a fundamental role in the diagnosis of RNA-virus infections as well as managing their reaction to treatment. Timely access to enterovirus RT-PCR outcome measures has demonstrated shorter hospital stays, reduced unnecessary antibiotic utilization, and decreased ancillary laboratory evaluations and tests. Broad-range rRNA PCR techniques, which utilize a single pair of primers targeting conserved regions of genes, have been utilized to diagnose bacterial pathogens and herpes viruses in the CSF. Isothermal amplification-based techniques. including loop-mediated isothermal amplification or LAMP, have been developed to offer a diagnosis within several minutes to hours. Table 2 demonstrates commercial molecular in vitro diagnostic devices, or IVD, which have been cleared by the US Food and Drug Administration, or FDA, for diagnosis of microbial pathogens in CSF. �
Monoplex Assays
A conventional molecular method involves three phases: sample extraction, target nucleic acid amplification, and amplicon detection. One of the first molecular assays successfully utilized for the diagnosis of CNS infections was utilized for the diagnosis of HSV in cerebrospinal fluid or CSF. PCR became the test of choice when research studies demonstrated that CSF PCR was similar to culture of brain tissue for diagnosis of HSV encephalitis and meningitis. Many PCR based methods for the diagnosis of herpes and enteroviruses have become available with increased sensitivity compared to viral culture. �
Real-time PCR with nucleic acid amplification and amplicon detection further improved the transition to molecular methods in clinical laboratories. Unlike conventional PCR, the real-time system is a �closed� system and it overcomes the fundamental problem of carryover contamination. At the time of manuscript preparation, three molecular assays utilized to help diagnose HSV and enteroviruses in CSF have ultimately been approved by the FDA as demonstrated in Table 2 of the previous article. � Real-time PCR-based methods are the main diagnostic technique utilized to help diagnose the Zika virus, which was first reported in Uganda in 1947, and is now a worldwide concern after the virus spread widely in Brazil and Central America. Research studies developed a one-step RT-PCR assay utilized to diagnose the Zika virus in human serum with a limited detection of 7.7pfu/reaction. Along with plasma, the Zika virus RNA can be diagnosed through urine and plasma within the first 2 weeks after symptoms have manifested. In March 2016, the FDA approved a trioplex-PCR assay under emergency use authorization for the simultaneous diagnosis of Zika, Chikungunya, and Dengue viruses in serum, urine, CSF and amniotic fluid. The RT-PCR assay utilizes dual labeled hydrolysis probes with a LOD of 1.54�10 4 GCE/ ml of Zika virus in serum. �
Introduction of real-time PCR based diagnostic assays have affected early and effective diagnosis of several bacterial infections. Isothermal amplification-based molecular assays have excellent performance characteristics and they don’t require any specialized equipment. These assays are fundamental for the utilization of on or near point-of-care testing. LAMP-based methods have been utilized to diagnose Neisseria meningitis, Streptococcus pneumoniae, Haemophilus influenzae type b, M. tuberculosis, and JEV in the CSF. The Xpert MTB/RIF assay has tremendously improved regulation of tuberculosis by offering an integrated and automated system which allows quick clinical decision making in a POC or near-care context. Several research studies have utilized the Xpert MTB/RIF to evaluate the diagnosis of M. tuberculosis in CSF from TB meningitis. In a meta-analysis of thirteen research studies, the pooled sensitivity of the Xpert assay was 80.5 percent, or 95 percent CI 59.0 percent to 92.2 percent, against culture and 62.8 percent, or 95 percent CI 47.7 percent to 75.8 percent, against composite standard. Utilizing a large volume of sample, of at least 8�10 ml, is necessary for testing CSF and centrifugation can cause considerable improvements in yield. Despite the lack of standardization for sample processing, WHO has allowed testing CSF with the automated Xpert MTB/RIF assay as the first-line test over conventional microscopy. �
Multiplex Assays
Simplicity makes multiplex molecular assays fundamental for the diagnosis of a panel of microbial targets. Several multiplex PCR assays have been developed to diagnose bacterial pathogens in CSF targeting the most common causes of meningitis: S. pneumoniae, N. meningitis, H. influenzae, L. monocytogenes, S. agalactiae, S. aureus, E. coli, and M. pneumoniae. A multiplex PCR followed by Luminex suspension array can simultaneously diagnose eight bacterial and viral pathogens in CSF, including N. meningitis, S. pueumoniae, E. coli, S. aureus, L. monocytogenes, S. agalactiae, HSV-1/2, and VZV, among others. �
Considering the variety of pathogens involved in CNS infection, application of comprehensive molecular panels with multiple bacterial and viral targets have improved the efficiency of diagnosis. The BioFire FilmArray Meningitis/Encephalitis panel is currently the only FDA cleared multiplex assay utilized for the diagnosis of six bacterial, such as Escherichia coli K1, Haemophilus influenzae, Listeria monocytogenes, Neisseria meningitides, Streptococcus agalactiae and Streptococcus pneumoniae, seven viral, such as cytomegalovirus, enterovirus, HSV-1, HSV-2, human herpesvirus 6 or HHV-6, human parechovirus and VZV, as well as a single fungal, such as Cryptococcus neoformans/gattii, target in CSF as demonstrated in Table 2. The integrated FilmArray system takes about an hour, with only 2 minutes of hands-on time. During the preparation of the manuscript, two research studies demonstrated the performance of this assay. Utilizing 48 samples from gram stain negative CSF samples from suspected cases of meningitis, research studies demonstrated that this system diagnosed more viral pathogens, such as EBV. Four cases of WNV and a single case of Histoplasma were not diagnosed by this assay. Among HIV infected patients in Uganda, the test performance demonstrated increased sensitivity and specificity for the diagnosis of Cryptococcus. Although the FilmArray Meningitis/Encephalitis panel offers a quick diagnosis of CNS infections, further research studies are needed to determine its performance for a variety of targets and other high-risk populations. �
Co-infections are frequently found among immunocompromised patients and can ultimately be challenging to diagnose for clinicians. The multiplex design allows simultaneous diagnosis of multiple targets on the same sample. One research study utilized a panel of monoplex and multiplex molecular assays to conduct a prospective cohort research study in Uganda to comprehensively evaluate the etiology of meningitis among HIV-infected adults. Among the 314 HIV-infected patients with meningitis, EBV co-infection was diagnosed with Cryptococcus, M. tuberculosis, or other viral pathogens. EBV in CSF in these settings is not completely understood although a single research study associated increased EBV viral load as a marker of poor outcome measures in patients with bacterial meningitis and EBV co-infection/ reactivation, among others. �
Pan-Omic Molecular Assays
Technological improvements in metagenomic deep sequencing have increased its utilization for clinical diagnosis of CNS infections. Several research studies have demonstrated its ability to solve diagnostic technique problems which challenge the limits of traditional laboratory testing. Due to sterile status and protection by BBB, CSF and brain biopsies are fundamental to further explore the utilization of this technology for pathogen diagnosis. Metagenomics was successfully utilized to establish a diagnosis of neuroleptospirosis in a 14-year-old boy with severe combined immunodeficiency who also suffered from recurrent bouts of fever, headache, and coma. Similarly, high-throughput RNA sequencing performed on brain biopsy from an 18-month-old boy with encephalopathy diagnosed a new Astrovirus as the cause. Despite the utilization of metagenomics for the diagnosis of infectious disease, there are many technological and practical concerns which need to be addressed before this form of diagnostic testing can become mainstream and part of the clinical standard of care. �
Other promising advances have occurred in transcriptomics, proteomics and metabolomics. Host and microbial microRNA or miRNA, profiles have been utilized for a variety of inflammatory and infectious diseases. Two miRNAs, miR-155 and miRNA-29b, were reported as potential biomarkers for JEV infection and treatment targets for anti-JEV therapy. Host neural epidermal growth factor, including 2 and apolipoprotein B in CSF, was able to diagnose tuberculous meningitis with 83.3 percent to 89.3 percent sensitivity and 75 percent to 92 percent specificity. CSF metabolite profiling has been reported to be useful in the classification, diagnosis, epidemiology, and treatment assessment of CNS infections in HIV patients. CSF metabolic profile analysis demonstrated bioenergetic adaptation in regulating shifts of HIV-infected patients. �
Outcome Measures Associated with Diseases
Diagnosis of an etiologic agent in patients with CNS infections needs consideration of the most common causative organisms, the available diagnostic techniques and molecular methods for these agents, and the highest-yield clinical specimens for evaluation and testing. Knowledge of the epidemiology and clinical presentation of specific agents is fundamental in selecting which diagnostic methods are appropriate for patients. Animal or vector exposures, geographic location, recent travel history, season of the year, exposure of ill contacts, and occupational exposures should be considered. �
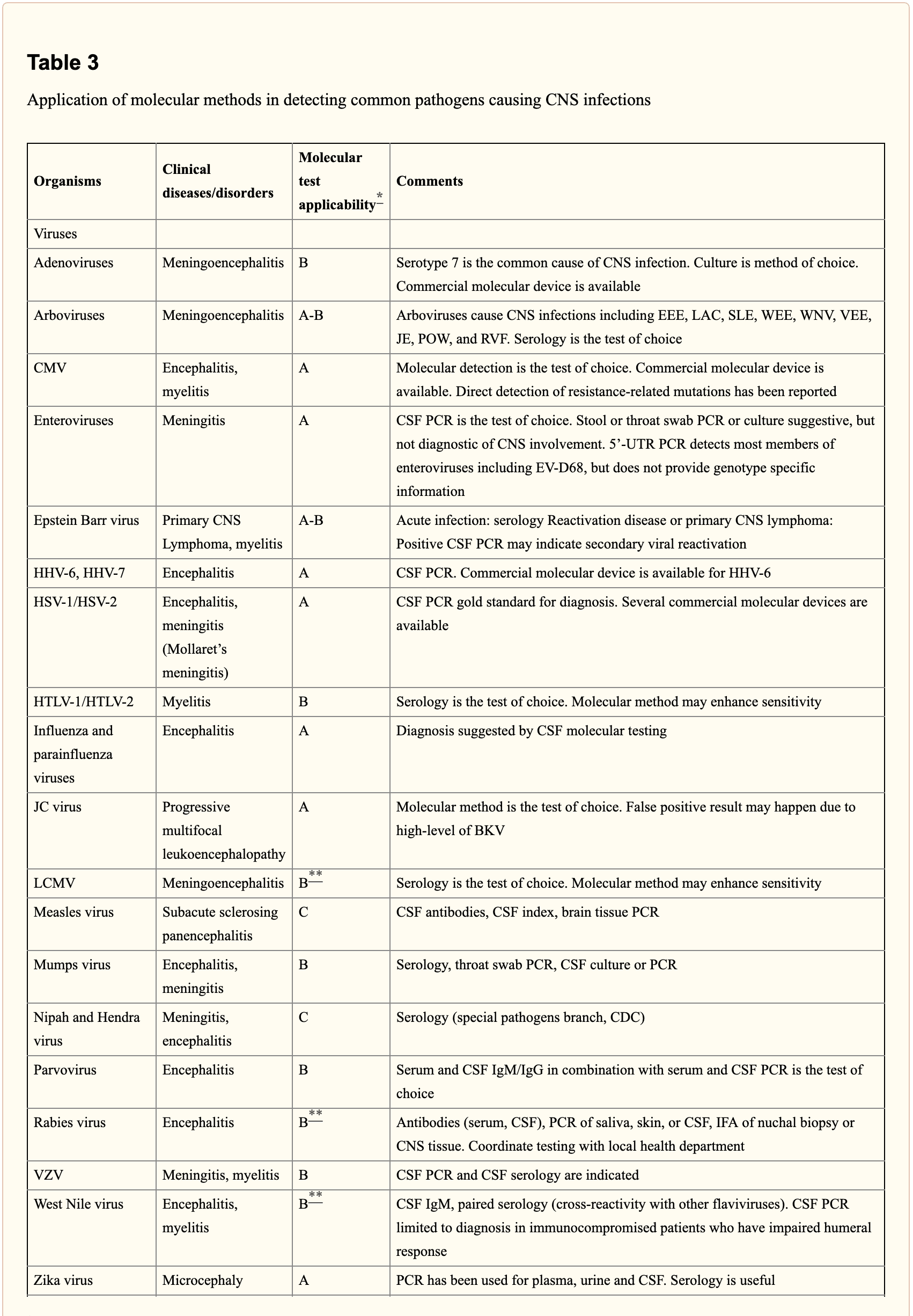
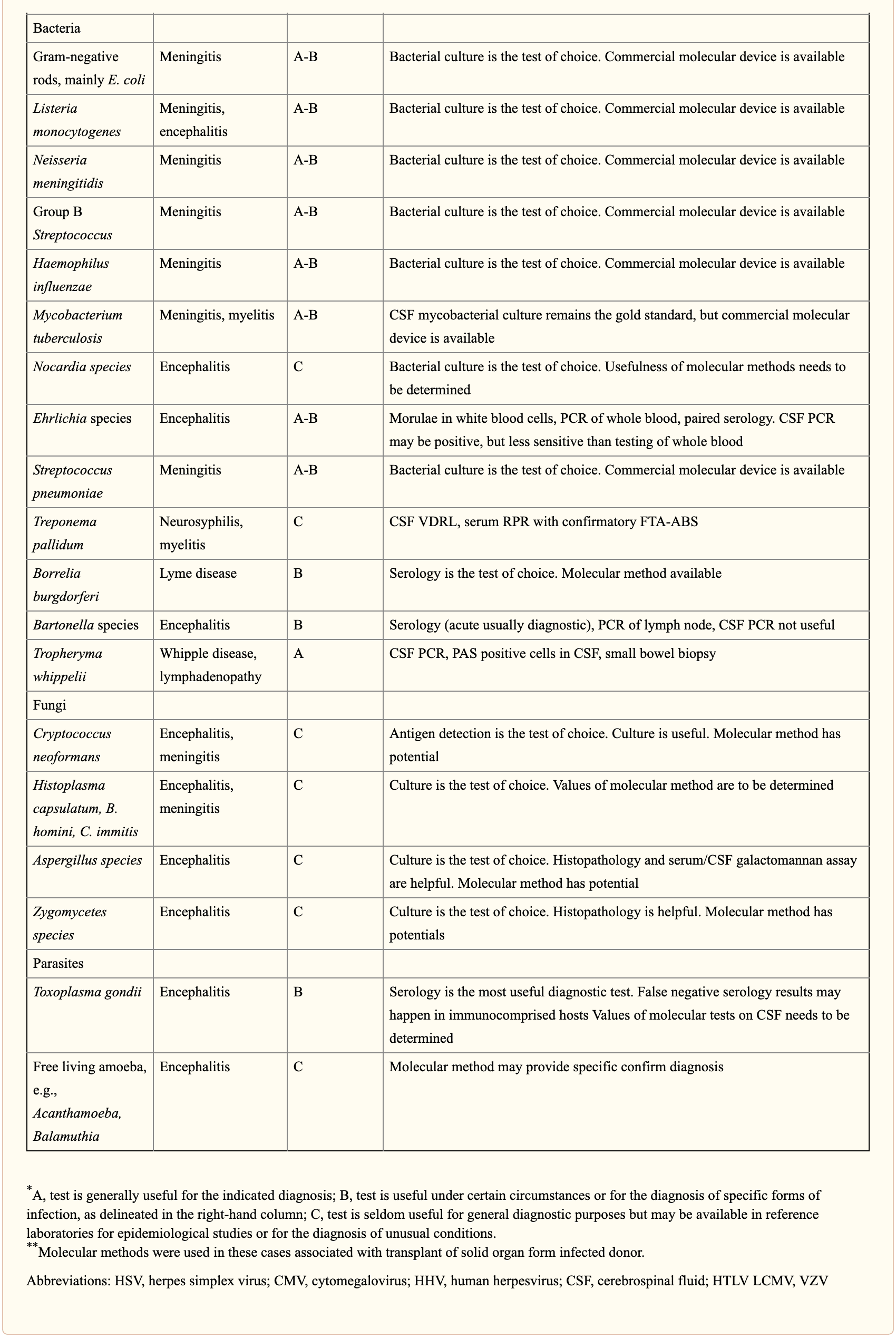
When selecting appropriate pathogen-specific molecular diagnostic methods, the following factors should be considered. CSF is the optimal specimen for PCR testing for patients with meningitis or meningoencephalitis. While indirect evidence can be determined by testing other specimen types, attempts should be made to obtain CSF samples early before treatment can compromise yield. Time of testing from the manifestation of symptoms is fundamental to understand and rule out false-negative results and recommend retesting within a certain time frame. By way of instance, HSV PCR can commonly render false-negative results if CSF sample is obtained very early or late in the process of HSE infection. Host health is also known to affect test performance characteristics. Immunocompromised patients are at risk for infection by a variety of opportunistic pathogens, by way of instance HHV-6, JC virus, Toxoplasma encephalitis in bone marrow transplant recipients and patients with HIV. Often, infection can be more severe, such as WNV, and challenging to diagnose in this population. Table 3 below demonstrates practical recommendations on application and pitfalls of molecular test for the diagnosis of CNS infections. �
Furthermore, a positive nucleic acid amplification testing results are considered to be complicated by the fact that some viruses survive latently in macrophages or neurologic tissues even if they’re incidentally diagnosed by sensitive molecular techniques without an actual pathogenic role which can potentially lead to overtreatment. Utilization of adjunctive biomarkers which help determine active replication is being explored to overcome this drawback in research studies. �
Historically, the diagnosis of microbiologic agents in patients with CNS infections has been hindered by the low yield of CSF culture for viral and fastidious bacterial organisms, delays in CNS production of organism-specific antibodies, and challenges in determining optimum samples for testing. The nucleic acid in vitro amplification-based molecular diagnostic methods and techniques have a wider and better application in clinical microbiology practice. The monoplex assay will likely be the main platform utilized for urgent, random-access, low throughput assays. Multiplex assays have the additional benefit of diagnosing multiple targets and mixed infections. As the volume of CSF sample retrieved is often small, multiplex assays enable comprehensive diagnostic analysis with a low amount of sample, obviating the need for repeated lumbar punctures. The clinical relevance and cost-effectiveness of simultaneous multi-pathogen diagnosis strategies need further research studies. Application of pan-omic techniques in challenging to diagnose CNS infections is the new exciting frontier, the technology is promising but routine implementation is expected to be slow due to various challenges, such as lack of applicable regulatory guidelines and adaptation in the clinical setting, although the outcome measures are promising. �
As previously mentioned, central nervous system, or CNS, infections can be life-threatening health issues if they are not accurately diagnosed and properly treated. However, determining a diagnosis of CNS infections can be challenging for many clinicians. Fortunately, a variety of diagnostic techniques and molecular methods can ultimately help determine the source of CNS infections and other health issues. These diagnostic techniques and molecular methods have tremendously improved over the years, as previously mentioned, and more of these evaluations are being utilized in clinical settings to accurately diagnose CNS infections for proper treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
In part 2 of our “Diagnosis of Central Nervous System Infections” article, we discussed the molecular methods and the pan-omic molecular assays which are utilized in the diagnosis of CNS infections as well as how specific testing outcome measures have ultimately been associated with clinical diseases and health issues. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 �
� �
�