Back problems and discomfort symptoms are a common ailment that many types of healthcare providers diagnose and treat it. Can knowing a little about what each back pain specialist does and what they have to offer help in choosing a provider?
Back Pain Specialists
Nowadays individuals have options for treating back pain. Primary healthcare providers, general practitioners, pediatricians, and emergency room workers are usually the first to examine the injury or problem. If they are unable to properly diagnose or treat the injury, they will refer the individual to a specialist. Specialists include:
Osteopaths
Chiropractors
Orthopedists
Rheumatologists
Neurologists
Neurosurgeons.
They specialize in chronic conditions and diseases like arthritis or problems like herniated discs. Complementary and alternative providers treat individuals solely or with help from a care team. They look at the whole body and focus on improving overall function.
Family and General Practitioners
When neck or back pain begins a regular doctor that’s usually a family or general practitioner/GP or primary care provider PCP is a recommended place to start. They will:
Order diagnostic tests.
Recommend exercises and stretches.
Prescribe medication.
Refer the patient to a physical therapist or other back pain specialist.
However, studies suggest general providers can be uninformed and slow to adopt new back treatments. (Paul B. Bishop, Peter C. Wing. 2006) It is recommended to research possible treatment options, ask a lot of questions during an appointment, and ask or request a referral to a specialist.
Pediatricians
Pediatricians diagnose and treat children. They cover a wide range of issues including back problems and injuries. As with a general practitioner or primary care provider, a child’s pediatrician is the place to start. Depending on the child’s needs, they’ll refer them to the proper specialist.
Emergency Healthcare Providers
When there is serious neck or back trauma, individuals need to go to the emergency room. Trauma can include automobile collisions, sports accidents, work accidents, and/or personal home accidents. Someone with a possible spinal injury should not be moved. (W Yisheng, et al., 2007) Go to the ER if there is back pain with loss of bowel or bladder control, or the legs become progressively weaker. These are symptoms of an emergency condition known as cauda equina syndrome. (American Association of Neurological Surgeons. 2023)
Orthopedists
Orthopedists and orthopedic surgeons treat the musculoskeletal system, which includes:
Muscles
Bones
Joints
Connective tissues
Cartilage
Common orthopedic issues include:
Repetitive stress injuries
Sports injuries
Bursitis
Tendonitis
Ruptured discs
Nerve impingement
Scoliosis
Osteoporosis
Osteoarthritis
Orthopedics can overlap with other specialties. As orthopedists and rheumatologists both treat arthritis and orthopedic surgeons and neurosurgeons do some of the same procedures that include spinal fusions and discectomies.
Rheumatologists
A rheumatologist treats autoimmune, inflammatory, and musculoskeletal conditions that can include different types of arthritis, lupus, and Sjogren’s syndrome. A primary care provider may refer a patient to a rheumatologist if they have symptoms that include:
Sacroiliitis – inflammation of the sacroiliac joint at the base of the spine.
Axial spondylosis – a form of spinal arthritis.
Axial spondylosis – spinal arthritis that causes the bones to fuse together.
Rheumatologists can also treat spinal stenosis or advanced osteoarthritis as they overlap with orthopedists.
Neurologists
A neurologist specializes in the function of the nervous system. They treat disorders of the brain, spinal cord, and nerves that include:
Parkinson’s disease
Multiple sclerosis
Alzheimer’s disease
Chronic back or neck pain
They are experts in the origins of pain. (David Borsook. 2012) However, a neurologist does not perform spine surgery.
Neurosurgeons
A neurosurgeon specializes in nervous system surgical procedures that include the brain, spine, and spinal cord. However, neurosurgeons do not provide overall treatment for back pain because they are usually the last to be seen after exhausting all other treatment options.
Osteopaths
An osteopath is a licensed physician who practices medicine using conventional treatments and osteopathic manipulative medicine. They have the same education as an MD plus 500 hours of musculoskeletal system studies. (National Library of Medicine. 2022) They take the same exams and are licensed as an MD. Many osteopaths are primary care providers. For back pain, they will focus on:
Posture rehabilitation and training.
Stretching
Therapeutic massage
Spinal manipulation
The goal is to relieve pain and muscle tension, increase mobility, and improve musculoskeletal function.
Physiatrists
Physiatrists are holistic providers that focus on physical function. They can be thought of as a primary care provider plus a physical therapist. These back pain specialists provide rehabilitation for various types of conditions and injuries including:
Back pain
Sports injuries
Stroke
Often they will coordinate a team of specialists to develop a targeted treatment plan.
Chiropractor
Chiropractic is a hands-on alternative medicine. The goal is to restore neuromusculoskeletal function by realigning the spine to its proper form. They do this with spinal manipulations, non-surgical mechanical decompression, traction, and massage techniques. (Michael Schneider, et al., 2016)
The purpose of most chiropractic adjustments is to relax and retrain tight muscles and increase flexibility.
Chiropractic helps to relieve stiff muscles and restore range of motion.
Individuals may not be referred to a chiropractor if they:
Have loose-joints
Have connective tissue problems or conditions.
Have osteoporosis/thinning bones
All types of back pain specialists provide various forms of therapy that may be able to help.
Spinal Decompression in Depth
References
Bishop, P. B., & Wing, P. C. (2006). Knowledge transfer in family physicians managing patients with acute low back pain: a prospective randomized control trial. The spine journal : official journal of the North American Spine Society, 6(3), 282–288. https://doi.org/10.1016/j.spinee.2005.10.008
Yisheng, W., Fuying, Z., Limin, W., Junwei, L., Guofu, P., & Weidong, W. (2007). First aid and treatment for cervical spinal cord injury with fracture and dislocation. Indian journal of orthopaedics, 41(4), 300–304. https://doi.org/10.4103/0019-5413.36991
Schneider, M., Murphy, D., & Hartvigsen, J. (2016). Spine Care as a Framework for the Chiropractic Identity. Journal of chiropractic humanities, 23(1), 14–21. https://doi.org/10.1016/j.echu.2016.09.004
Nowadays, individuals trying to avoid surgery have more therapy options. Can regenerative medicine help treat neuromusculoskeletal injuries?
Regenerative Medicine
Regenerative medicine utilizes the body’s raw cells and is used in cancer treatment and to reduce the risk of infections. (American Cancer Society. 2020) Researchers are looking for other ways to use these cells in medical therapies.
What are These Cells
Stem cells are unspecialized cells that can develop into any cell and in certain cases renew themselves an unlimited number of times. (National Institutes of Health. 2016)
Regenerative cell therapy uses these cells as a treatment for a disease or condition.
Regenerative cells are given to individuals to replace cells that have been destroyed or have died.
In the case of cancer, they may be used to help the body regain the ability to produce regenerative cells after treatment. (American Cancer Society. 2020)
For individuals with multiple myeloma and certain types of leukemia, regenerative cell therapy is used to eliminate cancer cells.
The therapy is called graft-versus-tumor effect/GvT, where a donor’s white blood cells/WBCs are used to eliminate the cancerous tumor. (American Cancer Society. 2020)
What They Can Treat
This is a new treatment that is still going through research. The Food and Drug Administration has only approved it for certain cancers and conditions that affect the blood and immune system. (Centers for Disease Control and Prevention. 2019) Regenerative cell therapy is FDA-approved to treat: (National Cancer Institute. 2015)
Leukemia
Lymphoma
Multiple myeloma
Neuroblastoma
It is also used to decrease the risk of infection after regenerative cell transplantation in individuals with blood cancers. (U.S. Food & Drug Administration. 2023)
Researchers are studying how these cells can treat other conditions. Clinical trials are analyzing how to use the therapy for neurodegenerative diseases like:
During regenerative cell therapy, the cells are given through an intravenous line. The three places where blood-forming cells can be obtained are bone marrow, the umbilical cord, and blood. Transplants can include: (American Cancer Society. 2020)
Autologous
The cells are taken from the individual who will be receiving the therapy.
Allogeneic
The cells are donated by another individual.
Syngeneic
The cells come from an identical twin, if there is one.
Safety
The therapy has shown to provide benefits but there are risks.
One risk is known as graft-versus-host disease – GVHD.
It occurs in one-third to half of allogeneic recipients.
This is where the body does not recognize the donor’s white blood cells and attacks them causing problems and symptoms throughout the body.
To treat GVHD medications are given to suppress the immune system to stop attacking the donor cells. (American Cancer Society. 2020)
The future of regenerative cell therapy is promising. Research is ongoing to find out how these cells can treat conditions and find new ways to treat and cure diseases.
Regenerative medicine has been researched for over twenty years for conditions like macular degeneration, glaucoma, stroke, and Alzheimer’s disease. (National Institutes of Health. 2022) This therapy is a new medical treatment that could be used in future therapies as part of a multidisciplinary approach to neuromusculoskeletal injuries and conditions.
For individuals with a broken collarbone, can conservative treatment help in the rehabilitation process?
Broken Collarbone
Broken collarbones are very common orthopedic injuries that can occur in any age group. Also known as the clavicle, it is the bone over the top of the chest, between the breastbone/sternum and the shoulder blade/scapula. The clavicle can be easily seen because only skin covers a large part of the bone. Clavicle fractures are extremely common, and account for 2% – 5% of all fractures. (Radiopaedia. 2023) Broken collarbones occur in:
Babies – usually during birth.
Children and adolescents – because the clavicle does not fully develop until the late teens.
Athletes – because of the risks of being hit or falling.
Through various types of accidents and falls.
The majority of broken collarbones can be treated with nonsurgical treatments, usually, with a sling to let the bone heal and physical therapy and rehabilitation.
Sometimes, when clavicle fractures are significantly shifted out of alignment, surgical treatment may be recommended.
There are treatment options that should be discussed with an orthopedic surgeon, physical therapist, and/or a chiropractor.
A broken collarbone is not more serious than other broken bones.
Once the broken bone heals, most individuals have a full range of motion and can return to the activities before the fracture. (Johns Hopkins Medicine. 2023)
Types
Broken clavicle injuries are separated into three types depending on the location of the fracture. (Radiopaedia. 2023)
Mid-Shaft Clavicle Fractures
These occur in the central area which can be a simple crack, separation, and/or fractured into many pieces.
Multiple breaks – segmental fractures.
Significant displacement – separation.
Shortened length of the bone.
Distal Clavicle Fractures
These happen close to the end of the collarbone at the shoulder joint.
This part of the shoulder is called the acromioclavicular/AC joint.
Distal clavicle fractures can have similar treatment options as an AC joint injury.
Medial Clavicle Fractures
These are less common and often related to injury to the sternoclavicular joint.
The sternoclavicular joint supports the shoulder and is the only joint that connects the arm to the body.
Growth plate fractures of the clavicle can be seen into the late teens and early 20s.
The bruising can extend down to the chest and armpit.
Numbness and tingling down the arm.
Deformity of the collarbone.
In addition to swelling, some individuals may have a bump in the place where the fracture occurred.
It can take several months for this bump to fully heal, but this is normal.
If the bump appears inflamed or irritated, inform a healthcare provider.
Clavicular Swelling
When the sternoclavicular joint swells up or gets bigger, it is referred to as clavicular swelling.
It is commonly caused by trauma, disease, or an infection that affects the fluid found in the joints. (John Edwin, et al., 2018)
Diagnosis
At the healthcare clinic or emergency room, an X-ray will be obtained to assess for the specific type of fracture.
They will perform an examination to ensure the nerves and blood vessels surrounding the broken collarbone are unsevered.
The nerves and vessels are rarely injured, but in severe cases, these injuries can occur.
Treatment
Treatment is accomplished either by allowing the bone to heal or by surgical procedures to restore the proper alignment. Some common treatments for broken bones are not used for clavicle fractures.
For example, casting a broken collarbone is not done.
In addition, resetting the bone or a closed reduction is not done because there is no way to hold the broken bone in proper alignment without surgery.
If surgery is an option the healthcare provider looks at the following factors: (UpToDate. 2023)
Location of Fracture and Degree of Displacement
Nondisplaced or minimally displaced fractures are usually managed without surgery.
Age
Younger individuals have an increased ability to recover from fractures without surgery.
Shortening of the Fracture Fragment
Displaced fractures can heal, but when there is a pronounced shortening of the collarbone, surgery is probably necessary.
Other Injuries
Individuals with head injuries or multiple fractures can be treated without surgery.
Patient Expectations
When the injury involves an athlete, heavy job occupation, or the arm is the dominant extremity, there can be more reason for surgery.
Dominant Arm
When fractures occur in the dominant arm, the effects are more likely to be noticeable.
The majority of these fractures can be managed without surgery, but there are situations where surgery can produce better results.
Supports for Non-surgical Treatment
A sling or figure-8 clavicle brace.
The figure-8 brace has not been shown to affect fracture alignment, and many individuals generally find a sling more comfortable. (UpToDate. 2023)
Broken collarbones should heal within 6–12 weeks in adults
3–6 weeks in children
Younger patients are usually back to full activities before 12 weeks.
The pain usually subsides within a few weeks. (UpToDate. 2023)
Immobilization is rarely needed beyond a few weeks, and with a doctor’s clearance light activity and gentle motion rehabilitation usually begins.
Edwin, J., Ahmed, S., Verma, S., Tytherleigh-Strong, G., Karuppaiah, K., & Sinha, J. (2018). Swellings of the sternoclavicular joint: review of traumatic and non-traumatic pathologies. EFORT open reviews, 3(8), 471–484. https://doi.org/10.1302/2058-5241.3.170078
Garlic tea is an herbal tonic made from garlic, lemon, and honey. What medicinal uses and benefits can garlic provide that is supported by scientific research?
Garlic Tea
Garlic tea:
Garlic – Allium sativum – is a perennial plant from Central Asia.
The plant produces a bulb that is used in cooking and in health remedies all over the world.
Garlic powder, oil, and supplements are available.
Supplements can be made from garlic oil or from fresh, dried, or aged garlic.
The tea is commonly made with garlic, lemon, and honey, but can be made with a variety of different ingredients.
It is used for cold symptoms like congestion and cough.
Health Benefits
Some, but not all benefits are supported by scientific evidence. It is important to keep in mind that these studies are analyzing garlic, and not necessarily garlic tea. The dose of garlic in tea may not be the same as a more concentrated dose that is used in the studies. Also, cooking or boiling garlic can change its therapeutic effects.
The scientific evidence about garlic’s benefits. Garlic is a healthy source of organosulfur compounds, including alliinase, which is released when it is crushed or chopped. (Leyla Bayan, Peir Hossain Koulivand, Ali Gorji. 2014)
Organosulfur compounds are believed to provide health benefits.
An overview of garlic studies found that there are promising health benefits, however, the researchers caution that larger studies are needed to confirm the results and verify the right dosage to get the results. (Johura Ansary, et al., 2020)
The current studies show the following possible benefits:
Some studies have also shown that garlic could be able to stimulate the immune system and decrease tumor growth in certain cancers, like colorectal cancer.
However, research investigating the cancer-preventing benefits has shown mixed results. (Xi Zhou, et al., 2020)
Common side effects of garlic consumption include bad breath, upset stomach, and body odor.
Garlic can also cause bloating, gas, and heartburn for some.
There are allergies to garlic and individuals with an allergy can experience more severe symptoms.
The NIH also advises that taking garlic may increase your risk of bleeding.
Individuals taking a blood thinner like warfarin or about to undergo surgery should discuss taking supplements or drinking garlic tea with their healthcare provider.
Garlic has been found to interfere with the effectiveness of some drugs that are used to treat HIV infection.
Lemon can cause tooth erosion so it is recommended to rinse teeth after drinking.
Honey has sugar content so it is recommended to use it in small quantities.
Healthy Diet and Chiropractic
References
National Center for Complementary and Integrative Health. Garlic.
Bayan, L., Koulivand, P. H., & Gorji, A. (2014). Garlic: A review of potential therapeutic effects. Avicenna journal of phytomedicine, 4(1), 1–14.
Ansary, J., Forbes-Hernández, T. Y., Gil, E., Cianciosi, D., Zhang, J., Elexpuru-Zabaleta, M., Simal-Gandara, J., Giampieri, F., & Battino, M. (2020). Potential Health Benefit of Garlic Based on Human Intervention Studies: A Brief Overview. Antioxidants (Basel, Switzerland), 9(7), 619. https://doi.org/10.3390/antiox9070619
Zhang, S., Liu, M., Wang, Y., Zhang, Q., Liu, L., Meng, G., Yao, Z., Wu, H., Xia, Y., Bao, X., Gu, Y., Wang, H., Shi, H., Sun, S., Wang, X., Zhou, M., Jia, Q., Song, K., & Niu, K. (2020). Raw garlic consumption is inversely associated with prehypertension in a large-scale adult population. Journal of human hypertension, 34(1), 59–67. https://doi.org/10.1038/s41371-019-0257-0
Zhou, X., Qian, H., Zhang, D., & Zeng, L. (2020). Garlic intake and the risk of colorectal cancer: A meta-analysis. Medicine, 99(1), e18575. https://doi.org/10.1097/MD.0000000000018575
Avci, A., Atli, T., Ergüder, I. B., Varli, M., Devrim, E., Aras, S., & Durak, I. (2008). Effects of garlic consumption on plasma and erythrocyte antioxidant parameters in elderly subjects. Gerontology, 54(3), 173–176. https://doi.org/10.1159/000130426
Burian, J. P., Sacramento, L. V. S., & Carlos, I. Z. (2017). Fungal infection control by garlic extracts (Allium sativum L.) and modulation of peritoneal macrophage activity in a murine model of sporotrichosis. Brazilian journal of biology = Revista brasleira de biologia, 77(4), 848–855. https://doi.org/10.1590/1519-6984.03716
Kato, Y., Domoto, T., Hiramitsu, M., Katagiri, T., Sato, K., Miyake, Y., Aoi, S., Ishihara, K., Ikeda, H., Umei, N., Takigawa, A., & Harada, T. (2014). Effect on blood pressure of daily lemon ingestion and walking. Journal of nutrition and metabolism, 2014, 912684. https://doi.org/10.1155/2014/912684
Samarghandian, S., Farkhondeh, T., & Samini, F. (2017). Honey and Health: A Review of Recent Clinical Research. Pharmacognosy Research, 9(2), 121–127. https://doi.org/10.4103/0974-8490.204647
Cisgender has nothing to do with an individual’s sexual orientation. Therefore how do sex and gender differ and where does cisgender fall within the spectrum of gender identities?
Cisgender
Cisgender is a segment of the larger spectrum of gender identities. Also referred to as “cis,” it describes an individual whose gender identity corresponds to the sex they were assigned at birth. Therefore if an individual assigned sex at birth is female and identifies as a girl or a woman they are a cisgender woman.
The term describes how a person sees themselves and helps others communicate more accurately and respectfully.
Although many individuals may identify as cisgender, a cisgender person is not typical nor has qualities or characteristics that inherently differentiate them from a person of other gender identities.
Cisgender women commonly use the pronouns she and her.
A common mistake is using the term cis-gendered.
The proper usage of the term is cisgender.
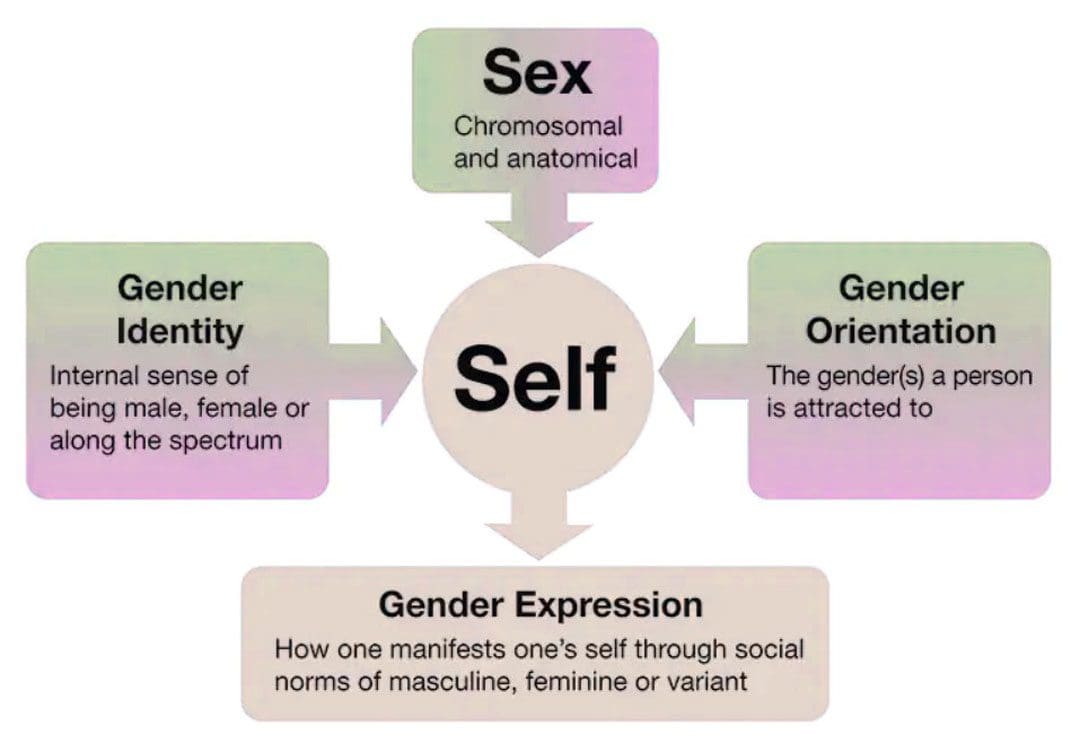
Sex and Gender Differences
The terms sex and gender are often used interchangeably, however, they are not the same.
Sex is a biological and physiological designation based on an individual’s sex chromosomes and sexual organs.
This includes an individual’s genitals and sex organs.
It also encompasses secondary characteristics – like body size, bone structure, breast size, and facial hair – that are regarded as female or male.
Differences
Gender is a social construct that refers to roles and behaviors that society assigns as being masculine or feminine. The construct infers behaviors that are accepted or appropriate based on how an individual behaves, speaks, dresses, sits, etc.
Gender titles include sir, ma’am, mister, or miss.
Pronouns include him, she, he, and her.
Roles include actress, actor, prince, and princess.
Many of these suggest a power hierarchy of who has it and who does not.
Cisgender women often fall victim to these dynamics.
Sex
Refers to an individual’s chromosomes and the way that their genes are expressed.
Typically described in terms of male and female characteristics or the sex assigned at birth.
Gender
A social construct.
Refers to the social roles, behaviors, and expectations considered and/or deemed appropriate for men and women.
Historically defined as masculine and feminine, however, definitions can change as society changes.
Gender Identities Glossary
Today, gender is viewed as a spectrum where an individual might identify as one gender, more than one gender, or no gender. The definitions are often subtle and can often overlap, co-exist, and/or change. Gender identities include:
Cisgender
An individual whose gender identity matches their assigned sex at birth.
Transgender
An individual whose gender identity does not align with their assigned sex at birth.
Non-binary
An individual who feels their gender identity cannot be defined.
Demigender
An individual who experiences a partial, but not full/complete connection to a particular gender.
Agender
An individual who feels neither male nor female.
Genderqueer
Similar to non-binary but infers refusal of societal expectations.
Gender-neutral
Non-binary similarities but focuses on abandoning gender labels.
Gender fluid
An individual who experiences multiple genders or shifts between genders.
Polygender
An individual who experiences or expresses more than one gender.
Pangender
An individual who identifies with all genders.
Third gender
Third gender is a concept in which individuals are categorized, either by themselves or by society, as neither male nor female, not transitioning.
They are a different gender altogether.
Twin gender
A Native American term describing someone who is male and female or of two spirits simultaneously.
Cis Woman Identity
The terms cis woman or cis female are used to describe individuals who were assigned female at birth and identify as a woman or female. For cisgender woman, this means their gender identity aligns with their primary sex organs and secondary sex traits that include:
Higher pitch voice.
Wider pelvis.
Broadening of hips.
Breast development
It can also involve cisnormativity – a concept that everyone identifies as the gender they were assigned at birth. This could inform how a cis woman is expected to dress and act. An even more extreme concept is gender essentialism – this is the belief that gender differences are rooted purely in biology and cannot be changed. However, even cisnormativity beauty standards can influence the perceptions of transgender women that end up reinforcing gender stereotypes. (Monteiro D, Poulakis M. 2019)
Cisgender Privilege
Cisgender privilege is the concept that individuals who are cisgender receive added benefits compared to individuals who don’t conform to the gender binary norm. This includes cisgender women and men. Privilege happens when a cisgender individual assumes they are the norm and consciously or unconsciously takes action against those who are outside the definition of masculine and feminine. Examples of cisgender privilege include:
Not being denied work and social opportunities because of not fitting into the boy’s or girl’s club.
Not having to have sexual orientation questioned.
Not being denied healthcare due to provider discomfort.
Not fearing that civil rights or legal protections will be taken.
Not worrying about being bullied.
Not having to worry about attracting questioning looks in public.
Not being challenged or questioned about the clothes being worn.
Not being demeaned or mocked because of pronoun use.
Gender identity and sexual orientation are not the same.
A cisgender individual can be heterosexual, homosexual, bisexual, or asexual and so can a transgender individual.
Being cisgender has no correlation to an individual’s sexual orientation.
Chiropractic Care After Accidents and Injuries
References
Clayton, J. A., & Tannenbaum, C. (2016). Reporting Sex, Gender, or Both in Clinical Research? JAMA, 316(18), 1863–1864. https://doi.org/10.1001/jama.2016.16405
Monteiro, Delmira and Poulakis, Mixalis (2019) “Effects of Cisnormative Beauty Standards on Transgender Women’s Perceptions and Expressions of Beauty,” Midwest Social Sciences Journal: Vol. 22: Iss. 1, Article 10. DOI: https://doi.org/10.22543/2766-0796.1009 Available at: https://scholar.valpo.edu/mssj/vol22/iss1/10
Moleiro, C., & Pinto, N. (2015). Sexual orientation and gender identity: review of concepts, controversies and their relation to psychopathology classification systems. Frontiers in Psychology, 6, 1511. https://doi.org/10.3389/fpsyg.2015.01511
Gender transitioning is the process of affirming and expressing an individual’s internal sense of gender rather than the one assigned at birth. How can learning the aspects of gender and gender transitioning help support the LGBTQ+ community?
Gender Transitioning
Gender transitioning or gender affirmation is a process through which transgender and gender-nonconforming individuals align their internal gender identity with their external gender expression. It can be described as a binary – male or female – but can also be non-binary, meaning an individual is neither exclusively male nor female.
The process can involve aesthetic appearances, changes in social roles, legal recognitions, and/or physical aspects of the body.
Social affirmation – dressing differently or coming out to friends and family.
Legal affirmation – changing name and gender on legal documents.
Medical affirmation – using hormones and/or surgery to change certain physical aspects of their body.
Transgender individuals can pursue some or all of these.
Barriers
Gender transitioning can be obstructed by various barriers that can include:
Cost
Lack of insurance
Lack of family, friends, or partner support.
Discrimination
Stigma
Addressing All Aspects
The process does not have a specific timeline and is not always linear.
Many transgender and gender-nonconforming individuals prefer gender affirmation to gender transitioning because transitioning is often taken to mean the process of medically transforming the body.
An individual does not have to undergo medical treatment to affirm their identity, and some transgender people avoid hormones or gender-affirming surgery.
Transitioning is a holistic process that addresses all aspects of who a person is inwardly and outwardly.
Certain aspects of transitioning may be more important than others, like changing one’s name and gender on their birth certificate.
Reevaluation and revision of gender identity can be continual rather than a step-by-step, one-way process.
Exploring Gender Identity
Gender transitioning often starts in response to gender dysphoria which describes the constant sense of uneasiness that occurs when the gender an individual was assigned at birth does not match how they experience or express their gender internally.
Some individuals have experienced symptoms of gender dysphoria as early as 3 or 4 years of age. (Selin Gülgöz, et al., 2019)
Gender dysphoria can be largely informed by the culture that surrounds the individual, specifically in cultures where strict codes determine what is masculine/male and feminine/female.
Unease Expressed in Different Ways
Dislike of one’s sexual anatomy.
A preference for clothes typically worn by the other gender.
Not wanting to wear clothes typically worn by their own gender.
A preference for cross-gender roles in fantasy play.
A strong preference for engaging in activities that are typically done by the other gender.
Dysphoria
Gender dysphoria can fully emerge during puberty when awareness about how an individual’s body defines them creates internal distress.
Feelings may be amplified when an individual is described as a tomboy, or a sissy, or is criticized and attacked for acting like a girl or acting like a boy.
During puberty, the physical changes can cause long-standing feelings of not fitting in and may evolve into feelings of not fitting in their own body.
This is when individuals can undergo a process referred to as internal transitioning and begin to change how they see themselves.
Gender transitioning/affirmation becomes the next step. Transitioning is not about changing or recreating oneself but about expressing their authentic self and asserting who they are socially, legally, and/or medically.
Social
Social transitioning involves how a person publicly expresses their gender. The transition can include:
Changing pronouns.
Using chosen name.
Coming out to friends, family, coworkers, etc.
Wearing new clothes.
Cutting or styling hair differently.
Changing mannerisms like moving, sitting, etc.
Changing voice.
Binding – strapping the chest to hide breasts.
Wearing breast and hip prosthetics to accentuate feminine curvature.
Packing – wearing a penile prosthesis to create a penile bulge.
Tucking – tucking the penis to conceal a bulge.
Playing certain sports
Pursuing different lines of work.
Participating in activities that might typically be seen as male or female.
Legal
Legal transitioning involves changing legal documents to reflect the individual’s chosen name, gender, and pronouns. This includes governmental and non-government documents that can include:
Birth certificates
Social Security ID
Driver’s license
Passport
Bank records
Medical and dental records
Voter registration
School ID
Provisions allowing for changes can vary by state.
Some states only allow changes if bottom surgery – genital reconstruction is performed.
Others will allow the changes without any form of gender-affirming surgery.
Medical transitioning typically involves hormone therapy to develop some of the male or female sex characteristics. It can also involve surgery to change certain physical aspects combined with hormone therapy.
Hormone therapy assists individuals to physically look more like the gender they identify as.
They can be used on their own and can also be used before gender-affirming surgery.
Hormone therapy takes two forms:
Transgender Men
Testosterone is taken to help deepen the voice, increase muscle mass, promote body and facial hair, and enlarge the clitoris. (M S Irwig, K Childs, A B Hancock. 2017)
Transgender Women
Estrogen is taken as well as testosterone blockers to redistribute body fat, increase breast size, reduce male-pattern baldness, and reduce testicle size. (Vin Tangpricha 1, Martin den Heijer. 2017)
Surgery
Gender affirmation surgery aligns an individual’s physical appearance to their gender identity. Many hospitals provide gender-affirming surgery through a transgender medicine department. Medical procedures include:
Facial surgery – Facial feminization surgery.
Breast augmentation – Increases breast size with implants.
Chest masculinization – Removes contours of breast tissues.
Tracheal shaving – Reduces the Adam’s apple.
Phalloplasty – Construction of a penis.
Orchiectomy – Removal of the testicles.
Scrotoplasty – Construction of a scrotum.
Vaginoplasty – Construction of a vaginal canal.
Vulvoplasty – Construction of the outer female genitalia.
Roadblocks
Transgender individuals are protected from public and private insurance discrimination under federal and state laws, including Medicare and Medicaid. (National Center for Transgender Equality. 2021)
Medicaid programs in nine states do not cover gender-affirming medical treatments, and only Illinois and Maine offer comprehensive standard care recommended by the World Professional Association for Transgender Health/WPATH. (Kaiser Family Foundation. 2022)
Medicare also has no consistent policy regarding the approval of gender-affirming surgery.
Others report family or partner disapproval as the main reason why they discontinue gender affirmation. (Jack L. Turban, et al., 2021)
If you know someone who is transgender or is considering transitioning, learning about gender and gender transitioning and how to be supportive is a great way to be an ally.
Enhancing Your Lifestyle
References
Gülgöz, S., Glazier, J. J., Enright, E. A., Alonso, D. J., Durwood, L. J., Fast, A. A., Lowe, R., Ji, C., Heer, J., Martin, C. L., & Olson, K. R. (2019). Similarity in transgender and cisgender children’s gender development. Proceedings of the National Academy of Sciences of the United States of America, 116(49), 24480–24485. https://doi.org/10.1073/pnas.1909367116
Irwig, M. S., Childs, K., & Hancock, A. B. (2017). Effects of testosterone on the transgender male voice. Andrology, 5(1), 107–112. https://doi.org/10.1111/andr.12278
Tangpricha, V., & den Heijer, M. (2017). Estrogen and anti-androgen therapy for transgender women. The Lancet. Diabetes & endocrinology, 5(4), 291–300. https://doi.org/10.1016/S2213-8587(16)30319-9
National Center for Transgender Equality. Know Your Rights in Health Care.
Kaiser Family Foundation. Update on Medicaid coverage of gender-affirming health services.
Center of Medicare and Medicaid Services. Gender dysphoria and gender reassignment surgery.
Transgender Legal Defense and Education Fund. Health insurance medical policies.
National Center for Transgender Equality and National Gay and Lesbian Task Force. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey.
Turban, J. L., Loo, S. S., Almazan, A. N., & Keuroghlian, A. S. (2021). Factors Leading to “Detransition” Among Transgender and Gender Diverse People in the United States: A Mixed-Methods Analysis. LGBT health, 8(4), 273–280. https://doi.org/10.1089/lgbt.2020.0437
For individuals, does knowing about food condiments nutritional values help with overall health?
Food Condiments
Condiment options go beyond the standard mayonnaise, ketchup, and mustard. Today there are various options to use as toppers, to marinate, tenderize, increase flavor, and add an appeal to the dish. Most condiments don’t provide much nutrition, but some do contain healthy ingredients like herbs, spices, heart-healthy fats, and antioxidants.
Healthy
The food condiments that are made the healthiest are those that are low in calories and unhealthy fat and they are made with less or no processed additives and quality ingredients that provide health benefits.
Pico de Gallo
This is a low-calorie, low-fat, nutrient-dense salsa that can zest up any meal.
It is made with tomatoes, onions, jalapeños, and lime.
Easily make your own to control sodium levels.
Top salads, vegetables, or protein with the salsa to add flavor.
Use as a dip for fresh raw vegetables as a snack.
Mustard
Mustard is a very low-calorie – 5 calories in 1 teaspoon, low-carbohydrate, and fat-free condiment that can increase the flavor of food by adding a sweet, sour, or spicy kick.
Most traditional mustards – yellow and spicy – are made with mustard seed, distilled vinegar, garlic powder, onion powder, salt, spices, and turmeric.
This means that mustard contains little or insignificant calories, fat, protein, and carbohydrate in one serving.
Studies have shown that turmeric can provide health benefits from a compound called curcumin.
Preclinical studies suggest that curcumin can act as an antioxidant and has anti-inflammatory, anticancer, and neuroprotective properties. (Abrahams S, et al., 2019)
Flavored mustards, like honey flavor, can contain added sugars, therefore, it is recommended to read the label before eating.
Balsamic, red or white wine or apple cider vinegar can be used on side dishes, salads, sandwiches, and to marinate.
This condiment ranges from 0 calories to 10 calories per tablespoon and contains no sodium.
Studies have shown that apple cider vinegar can reduce fasting blood sugar in individuals at risk for type 2 diabetes. (Johnston CS, Quagliano S, White S. 2013)
Hot Sauce
Hot sauce is made from red chili peppers.
Top eggs, vegetables, or whole grains with a few dashes.
Studies suggest that adding spice can help satisfy hunger, help curb appetite and possibly speed up metabolism. (Emily Siebert, et al., 2022)
Read labels as sauces can contain added sugars.
Ketchup
Because of its carbohydrate and sugar content, ketchup is a condiment that needs to be portion-controlled, especially for individuals with diabetes who are following a modified nutritional plan.
Although much of the fat is unsaturated/healthy type, it can be hard to portion control this food condiment, which can result in excess calorie intake.
Barbecue Sauce
Barbecue sauce is moderate in calories, around 60 in two tablespoons, but it can contain a large amount of sodium and sugar.
Most brands can contain 10 to 13 grams of sugar/equivalent to 3 teaspoons and 280 to 350 milligrams of sodium.
The recommended serving size is two tablespoons.
Individuals trying to watch calorie and sugar intake are recommended to stick to one serving.
Sour Cream
Sour cream contains 60 calories and 6 grams of fat in two tablespoons.
Regularly consuming saturated fat has been linked with heart disease, high cholesterol, and diabetes.
A healthy substitute for sour cream can be a tablespoon or two of low-fat or non-fat plain Greek yogurt.
Regardless of the healthy or non-healthy food condiments, it is recommended not to drown the food in them and stick to the recommended serving sizes.
Benefits of Healthy Diet and Chiropractic Care
References
Abrahams, S., Haylett, W. L., Johnson, G., Carr, J. A., & Bardien, S. (2019). Antioxidant effects of curcumin in models of neurodegeneration, aging, oxidative and nitrosative stress: A review. Neuroscience, 406, 1–21. https://doi.org/10.1016/j.neuroscience.2019.02.020
Spicy brown mustard. FoodData Central. U.S. Department of Agriculture.
Johnston CS, Quagliano S, White S. Vinegar ingestion at mealtime reduced fasting blood glucose concentrations in healthy adults at risk for type 2 diabetes. J Funct Foods. 2013;5(4):2007-2011. doi:10.1016/j.jff.2013.08.003
Siebert, E., Lee, S. Y., & Prescott, M. P. (2022). Chili pepper preference development and its impact on dietary intake: A narrative review. Frontiers in nutrition, 9, 1039207. https://doi.org/10.3389/fnut.2022.1039207
Ketchup. FoodData Central. U.S. Department of Agriculture.
Caesar dressing. FoodData Central. U.S. Department of Agriculture.
Vinaigrette. FoodData Central. U.S. Department of Agriculture.
Mayonnaise. FoodData Central. U.S. Department of Agriculture.
Sour cream, regular. FoodData Central. U.S. Department of Agriculture.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine