6 Supplements For Kidney Health
Do you feel:
- Complicated, infrequent bowel movements?
- Frequent urination?
- Poor bowel function?
- Have more than three bowel movements daily?
- Feeling that bowels do not empty completely?
If you are experiencing any of these situations, then you might want to consider these six supplements for your kidneys.
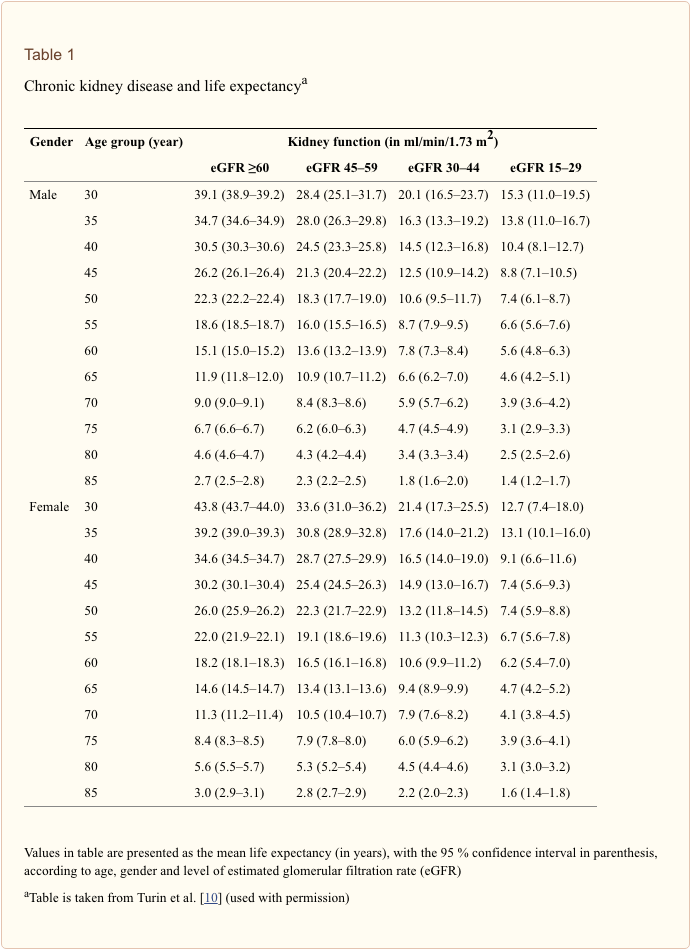
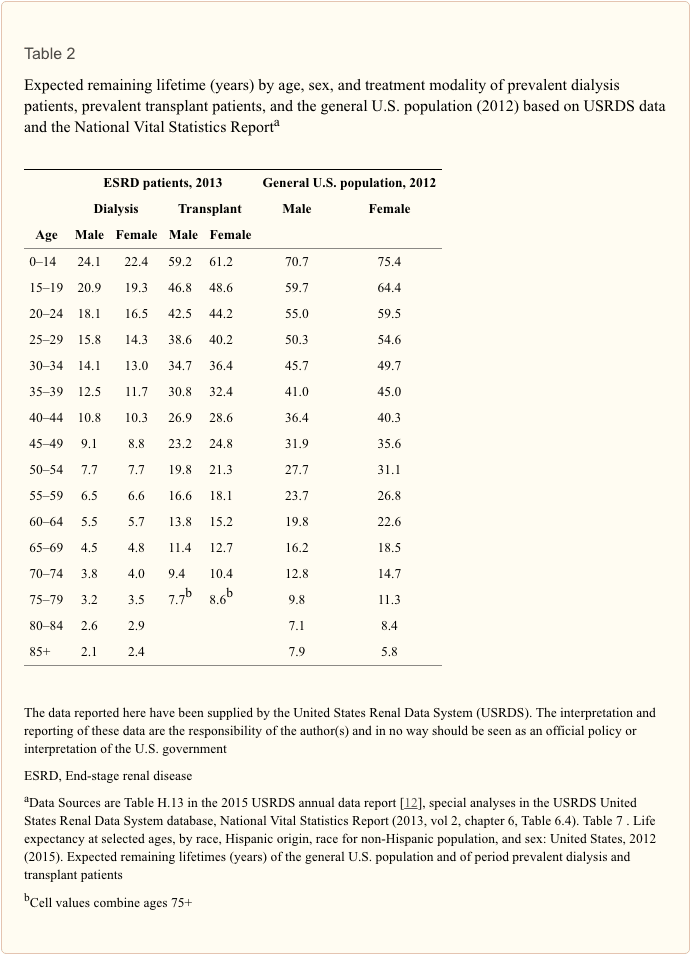
It is estimated that 31 million Americans have suffered from chronic kidney disease. It might be due to the misery of the production of kidney stones. It is more common that 9 out of 10 individuals that have moderately decreased kidney function will not even know that they have it. Chronic kidney disease does not get much recognition, but it does kill more people than either breast or prostate cancer.
One reason that chronic kidney disease is not on the radar for most people is that there are no symptoms until the disease is in the advanced stage. When it does appear in the body, they include a range of symptoms that can stay in the body for a long time. Since many of the symptoms do not set off the alarms in the body, it is easy to ignore them until the person is diagnosed with kidney failure. Fortunately, with a little awareness and some natural kidney support, individuals can prevent the symptoms from escalating on the body.
Good Kidney Health
The kidneys are two bean-shaped organs that are located behind the lower rib cage on either side of the spine in the body. Vital to the overall health, the kidneys filter waste and toxins out of the blood and moving them to the bladder so they can be excreted out of the body as urine. The kidneys also regulate the body�s fluid balance, the minerals balance in the bloodstream, and activating vitamin D, so that way the body can use it. The kidneys also release hormone production directly to the bloodstream and regulating blood pressure.

It is essential to take the necessary steps to maintain kidney health, especially if an individual has an increased risk of chronic kidney disease. Factors can affect the body and can cause individuals to have a higher risk of chronic kidney disease. Some of these factors include:
- Being diabetic
- Someone in the family that has a history of kidney disease, diabetes or high blood pressure
- Someone having some form of cardiovascular disease
- Obesity
- Diagnosed with chronic urinary tract infections
While some of these risks are beyond a person’s control, it is crucial to adopt a few healthy lifestyle habits and adding kidney supporting supplements to prevent the spread of chronic kidney diseases and other ailments that have damaged the kidneys in the body.
The Best Ways for Kidney Health
When optimizing kidney health, changing lifestyle habits is highly essential. While quitting smoking, moderate alcohol consumption, and increasing physical activity is beneficial for the body and can boost kidney health overall. Improving the diet is one of the most accessible lifestyle modifications anyone can make.
For decades, doctors have recommended patients with CKD, a renal diet that limits dietary potassium, and phosphorus intake. The only problem with this type of diet is that it reduced some of the essential foods like fruits, vegetables, whole grains, legumes, and nuts. However, recent studies pointed out that well-rounded diets like the Mediterranean diet or the DASH diet are the way to go for those who are with or want to prevent CDK. With these healthier diets, they focus on whole-minimally-processed foods and low, moderate amounts of protein and as a result, they support kidney health and help reduce the risk of related health issues like high blood pressure, heart disease, obesity, and diabetes.
It is also a smart move to stay hydrated with fluids, especially water, since it helps clear the sodium and toxins from the kidneys.
The 6 Supplements For Healthy Kidneys
When a person is at risk for kidney disease or wants to optimize these amazing filters, these six supplements are excellent for playing a supportive role in helping the kidneys.
Alpha-lipoic acid
Alpha-lipoic acid is a powerful antioxidant that is made inside the mitochondria, where it helps key enzymes turn into nutrients and energy for the body. This antioxidant plays another crucial role by protecting the cells from oxidative damage, including those in the kidneys. A study showed that alpha-lipoic acid produces a significant uptick in two other antioxidants, SOD (superoxide dismutase) and CAT (catalase) in kidney tissue. This can help reduce inflammation and oxidative stress in the kidneys as well as preventing kidney stones from forming.
Andrographis

Andrographis is a kidney supporting herb that people do not think about when they are indulging in their favorite alcoholic beverage; however, it should be. In the Journal of Ethnopharmacology found that the two compounds that are in Andrographis, which is andrographolide and arabinogalactan proteins; help protect the kidneys from alcohol toxicity. For anyone that is enjoying a glass wine with dinner, having a beer or two with friends, or drinking the occasional cocktail, taking a dose of Andrographis before consuming alcohol can provide the protection the kidneys need.
Moringa

Moringa is a superfood that comes from the leaves of the moringa tree that is essential parts of Asia, Central and South America, Africa, and Australia. These medicinal plants have possessed the ability to protect SOD and CAT levels in the kidneys. Studies have been shown using a model of acetaminophen toxicity and found that the moringa supplementation has reversed both the oxidative damage and inflammation in the kidneys.
NAC
Also known as n-acetylcysteine, NAC is the precursor to glutathione, the body�s master antioxidant. NAC is an antioxidant in its rights by protecting the kidney cells from heavy metals and other damaging toxins. Research has shown that NAC can also limit the damage from AGEs (advanced glycation end production.) AGEs are formed when glucose reacts with the proteins in the blood vessel walls, including the blood vessels within the kidneys. The resulting damage caused by AGE includes oxidative damage that can be a contributing factor to chronic kidney disease, but proactively including NAC as part of the person’s supplement routine that can help protect the harmful effects of AGEs.
Probiotics

Beneficial bacteria found in probiotics can do more than just enhancing the body’s gut health. Probiotics can also help protect against the complication of CKD by decreasing inflammation and the production of uremic toxin. This dual-action helps the kidney function. Probiotics can protect the body from the leaky gut syndrome, which is a common condition people with CKD, allowing harmful bacteria to “leak” from the intestinal tract into the blood. Supplementing with probiotics can improve the bacterial balance in the gut, lessening the permeability of the intestinal barrier, and reducing the complications of CKD.
Resveratrol

Resveratrol is found in grapes, berries, and peanuts. Only making the headlines a few years ago, due to its heart-healthy properties and new evidence has been found that resveratrol can protect the kidneys from a variety of toxins, including heavy metals, drugs, and alcohol that can cause renal injury. This antioxidant and anti-inflammatory compound can help fortify the kidneys against injury and improves renal function once the injury has occurred.
Conclusion
With these six supplements, they can provide anyone the help they need to prevent chronic kidney disease. Even though the symptoms of chronic kidney disease do not show at a later date, individuals must add these supplements to their diet and lifestyle to prevent chronic kidney disease.�Some products can help with inflammation in the body system by containing collagen-based proteins and targeting amino acids that can offer support to the gastrointestinal system.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900�.
References:
Al, H S. �Protective Effect of Resveratrol against Aluminum Chloride Induced Nephrotoxicity in Rats.� Saudi Medical Journal., U.S. National Library of Medicine, Apr. 2016, www.ncbi.nlm.nih.gov/pubmed/?term=27052279.
Albertoni, G, and N Schor. �Resveratrol Plays Important Role in Protective Mechanisms in Renal Disease–Mini-Review.� Jornal Brasileiro De Nefrologia: ‘Orgao Oficial De Sociedades Brasileira e Latino-Americana De Nefrologia., U.S. National Library of Medicine, 2019, www.ncbi.nlm.nih.gov/pubmed/?term=25923757.
Chauveau, Philippe, et al. �Mediterranean Diet as the Diet of Choice for Patients with Chronic Kidney Disease.� Nephrology, Dialysis, Transplantation: Official Publication of the European Dialysis and Transplant Association – European Renal Association, U.S. National Library of Medicine, 1 May 2018, www.ncbi.nlm.nih.gov/pubmed/29106612.
Cigarran, S, et al. �Gut Microbiota in Chronic Kidney Disease.� Nefrologia: Publicacion Oficial De La Sociedad Espanola Nefrologia., U.S. National Library of Medicine, 2019, www.ncbi.nlm.nih.gov/pubmed/?term=27553986.
Gallieni, Maurizio, and Adamasco Cupisti. �DASH and Mediterranean Diets as Nutritional Interventions for CKD Patients.� American Journal of Kidney Diseases: the Official Journal of the National Kidney Foundation, U.S. National Library of Medicine, Dec. 2016, www.ncbi.nlm.nih.gov/pubmed/27884277.
Karthivashan, G, et al. �The Modulatory Effect of Moringa Oleifera Leaf Extract on Endogenous Antioxidant Systems and Inflammatory Markers in an Acetaminophen-Induced Nephrotoxic Mice Model.� PeerJ., U.S. National Library of Medicine, 7 July 2016, www.ncbi.nlm.nih.gov/pubmed/?term=27441110.
Ko, Gang Jee, et al. �Dietary Protein Intake and Chronic Kidney Disease.� Current Opinion in Clinical Nutrition and Metabolic Care, U.S. National Library of Medicine, Jan. 2017, www.ncbi.nlm.nih.gov/pubmed/27801685.
Petronilho, F, et al. �Alpha-Lipoic Acid Attenuates Oxidative Damage in Organs After Sepsis.� Inflammation., U.S. National Library of Medicine, Feb. 2016, www.ncbi.nlm.nih.gov/pubmed/?term=26431839.
Singha, P K, et al. �Protective Activity of Andrographolide and Arabinogalactan Proteins from Andrographis Paniculata Nees. against Ethanol-Induced Toxicity in Mice.� Journal of Ethnopharmacology., U.S. National Library of Medicine, 20 Apr. 2007, www.ncbi.nlm.nih.gov/pubmed/?term=17127022.
Unknown, Unknown. �6 Supplements That Improve Your Kidney Health.� Fullscript, 1 Oct. 2019, fullscript.com/blog/kidney-health.
Unknown, Unknown. �Facts About Chronic Kidney Disease.� National Kidney Foundation, 19 July 2019, www.kidney.org/atoz/content/about-chronic-kidney-disease.
Unknown, Unknown. �Kidney Disease Statistics for the United States.� National Institute of Diabetes and Digestive and Kidney Diseases, U.S. Department of Health and Human Services, 1 Dec. 2016, www.niddk.nih.gov/health-information/health-statistics/kidney-disease.
Xia, Q, et al. �N-Acetylcysteine Ameliorates Contrast?Induced Kidney Injury in Rats with Unilateral Hydronephrosis.� Molecular Medicine Reports., U.S. National Library of Medicine, Feb. 2018, www.ncbi.nlm.nih.gov/pubmed/?term=29207099.