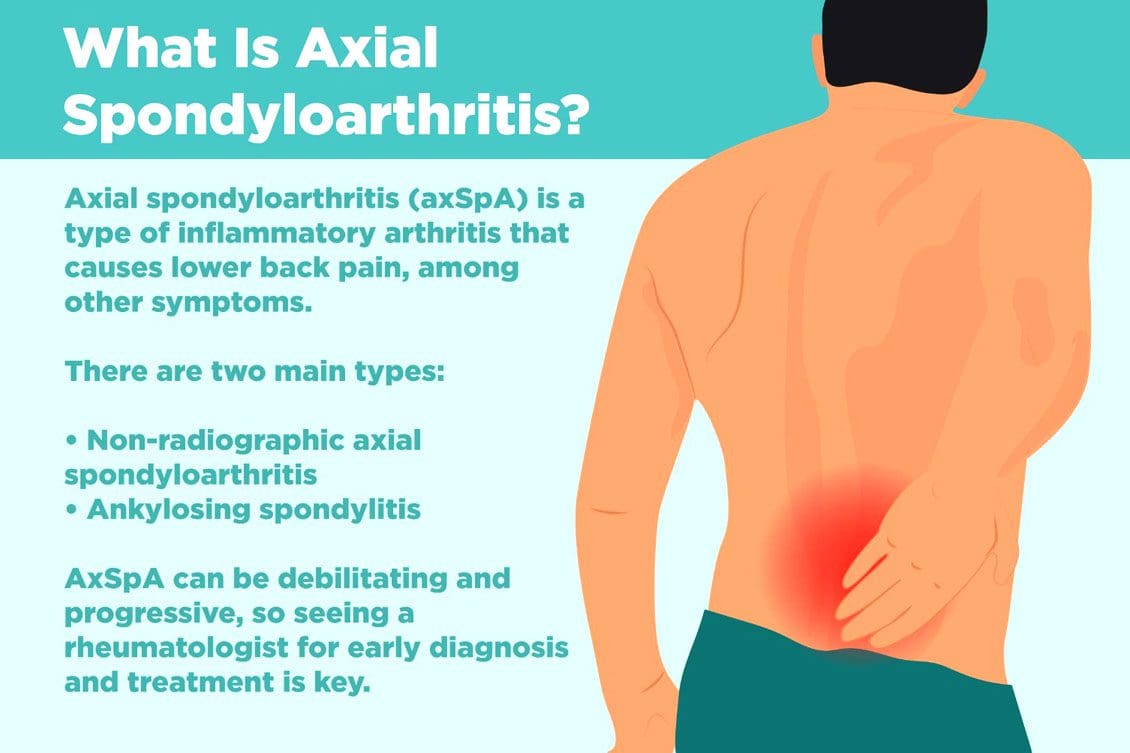
Non-radiographic axial spondyloarthritis or nr-axSpA and non-radiographic ankylosing spondylitis/AS are related. However, non-radiographic axial spondyloarthritis can present AS symptoms with active inflammation of the spine and sacroiliac/SI joints, causing back and hip pain but does not reveal joint damage on X-rays or MRIs. Injury Medical Chiropractic and Functional Medicine Clinic can explain what it means to have non-radiographic axial spondyloarthritis, how it can be managed, and what to do to prevent it from turning into ankylosing spondylitis.
Non-Radiographic Axial Spondyloarthritis
Non-radiographic axial spondyloarthritis means there are early AS symptoms but have not developed enough joint inflammation or damage to show up on an X-ray or other form of imaging. Early evidence of joint inflammation includes blurring of the joint edges and localized regions of joint erosion. It can be difficult for physicians to see these subtle changes on an x-ray.
Ankylosing Spondylitis
Ankylosing spondylitis, or AS, is a form of inflammatory arthritis that affects joints in the spine and elsewhere.
It is a chronic, inflammatory, autoimmune disease.
Medical research is still ongoing to determine the exact cause, but a genetic component is believed to be contributing factor.
Around 85% of individuals with ankylosing spondylitis have inherited the HLA-B27 gene, which is associated with multiple autoimmune conditions.
In the early stages, individuals will present lower back pain around the sacroiliac joints or the joints that connect the spine to the pelvis.
Later stages have more obvious X-ray findings, like the fusing of the sacroiliac joints and the lower spine that takes place over time.
Joint inflammation can progress, causing permanent joint damage and spine rigidity.
Most individuals with the condition can manage their symptoms with NSAIDs, chiropractic care, physical and massage therapy, and range of motion exercises.
Stage 1
There is no evidence of spinal inflammation on x-rays.
MRI provides more detailed images of bones and may reveal bone marrow edema or accumulation of fluid in the structures of the spinal bones and joints.
Individuals with non-radiographic axial spondyloarthritis, you are here.
Stage 2
There is visible inflammation of the spinal joints on the x-ray.
The sacroiliac joints between the spine and the pelvis are the most affected.
Stage 3
Chronic inflammation of the joints has caused bone loss and permanent joint damage, resulting in spine rigidity.
Symptoms of Non-Radiographic Axial Spondyloarthritis
There are differences between back pain associated with muscle strain and arthritis. Back pain symptoms include:
Starts to present before age 40.
It has a gradual onset and can go unnoticed for years.
Improves with movement or activity.
Eases up throughout the day.
Starts up in the evening when resting.
Other symptoms include:
Joint stiffness
Swollen fingers
Heel pain
Bilateral buttock discomfort and pain
Slowing Progression
Progression from non-radiographic axial spondyloarthritis to ankylosing spondylitis occurs in 10% – 20% of individuals over a two-year period. Progression factors include genetics, gender, degree of joint damage, and level of inflammatory markers at the time of diagnosis.
Early diagnosis and treatment can slow the progression before significant joint damage with anti-inflammatory therapy, rheumatological therapy, and targeted exercise.
Work with a specialist like an orthopedic spine specialist and rheumatologist that understands the disorder and is up to date on the most recent treatment modalities.
Individuals with non-radiographic axial spondyloarthritis should expect to have serial X-rays to gauge the progression of the disease.
Staying healthy and active is recommended to slow the progression of nr-AxSpA and AS.
Recent medical advances and lifestyle adjustments can slow the progression in most cases.
axSpA
References
Six tips for living well with ankylosing spondylitis. Available at https://www.mayoclinic.org/diseases-conditions/ankylosing-spondylitis/in-depth/6-tips-for-living-well-with-ankylosing-spondylitis/art-20478753. Accessed 11/07/2022.
Ankylosing spondylitis. Mayo Clinic. Available at https://www.mayoclinic.org/diseases-conditions/ankylosing-spondylitis/symptoms-causes/syc-20354808. Accessed 11/05/2022.
D. J. Pradeep, A. Keat, K. Gaffney, Predicting outcome in ankylosing spondylitis, Rheumatology, Volume 47, Issue 7, July 2008, Pages 942–945, https://doi.org/10.1093/rheumatology/ken195
Kucybała, Iwona, et al. “Radiologic approach to axial spondyloarthritis: where are we now and where are we heading?.” Rheumatology international vol. 38,10 (2018): 1753-1762. doi:10.1007/s00296-018-4130-1
Michelena, Xabier, López-Medina, Clementina, and Helena Marzo-Ortega. “Non-radiographic versus radiographic axSpA: what’s in a name?”.” National Center for Biotechnology Information. October 14, 2020. https://doi.org/10.1093/rheumatology/keaa422
Swift D. Ankylosing spondylitis: disease progression varies widely. Medpage Today. Accessed 11/05/2022.Available at https://www.medpagetoday.com/rheumatology/arthritis/49096
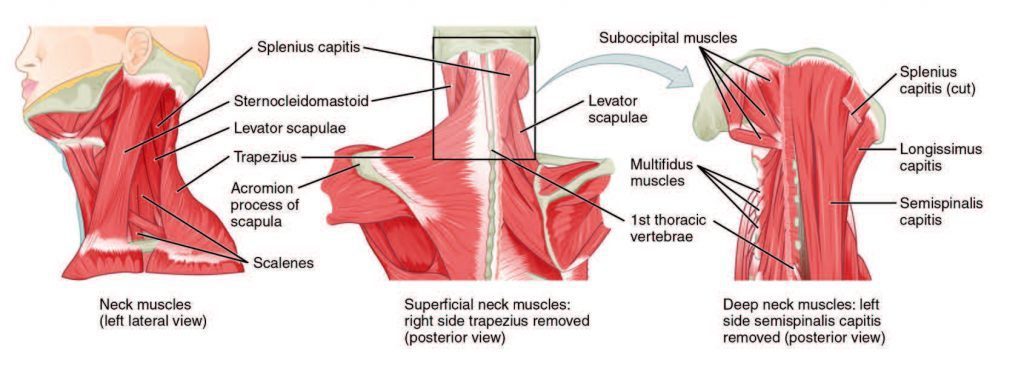
Axial neck pain is also known as uncomplicated neck pain, whiplash, and cervical/neck strain. They refer to pain and discomfort running along the back or posterior of the neck. Axial is defined as forming or around an axis. This type of pain stays around the neck and immediate surrounding structures. It does not spread/radiate out to the arms, hands, fingers, and other areas of the body. Axial neck pain differs from two other neck conditions. They are:
Cervical radiculopathy describes irritation or compression/pinching of the nerve as it exits the spinal cord. The nerves of the cervical spine are known as the peripheral nerves. They are responsible for relaying signals to and from the brain to specific areas of the arms and hands. The signals sent from the brain are for muscle movement, while signals going to the brain are for sensation.
When one of these nerve/s gets irritated, inflamed, or injured, it can result in:
Muscle pain
Weakness
Numbness
Tingling sensation
Burning pain
Other types of abnormal sensations in the arms, hands, or fingers.
Cervical myelopathy describes compression of the spinal cord itself. The spinal cord is the information highway/pipeline to all parts of the body. There is a range of symptoms that can include:
Same symptoms as cervical radiculopathy
Balance problems
Coordination problems
Loss of fine motor skills
Bowel and bladder incontinence
Axial neck pain
Axial neck pain is a quite common type of neck pain. It affects around 10% of the population. However, the majority of these cases do not involve severe symptoms that limit daily activity.
Symptoms
Pain in the back of the neck is the primary and most common symptom. Sometimes the pain travels to the base of the skull, shoulder, or shoulder blade. Other symptoms include:
Neck stiffness
Headaches
Localized muscle pain
Warmth
Tingling
Developmental Risk factors
Poor posture, lack of ergonomics, and muscle weakness increase the chances of developing axial neck pain. Risk factors for development include:
Age
Trauma – Auto accident, sports, personal, work injury
Headaches
Depression
Chronic neck pain
Sleep problems
Diagnosis
Based on symptoms and physical exam findings are how a diagnosis is usually achieved. A doctor will typically order an x-ray, CT, or MRI of the cervical spine. This calls for an immediate visit to a hospital/clinic for evaluation. There could be severe symptoms that could indicate something more dangerous, causing pain like infection, cancer, or fracture. These symptoms include:
Prior trauma/injury from a fall, automobile accident, sports, work injury
Fever
Weight loss
Night sweats
Constant night pain
Rheumatic conditions/diseases that cause neck pain can include morning stiffness and immobility that gets better as the day progresses. If symptoms continue for more than 6 weeks, imaging of the spine could be recommended, especially for individuals that have had previous neck or spine surgery or if it could be cervical radiculopathy or myelopathy.
Treatment
There is a wide range of treatment options. Surgery is rarely required except for severe cases. Returning to normal activities almost right away is one of the most important things to prevent the pain from becoming chronic. First-line treatments typically begin with:
Physical therapy
Chiropractic
Stretching routine
Strengthening exercises
Acetaminophen
Anti-inflammatory medication/s
Muscle relaxants are sometimes prescribed
If a cervical spine fracture has been diagnosed, a neck brace could be recommended for short-term use. A soft collar could be utilized if the pain is severe, but a doctor usually discontinues use after 3 days. Other non-invasive treatment options include:
Invasive treatments like injections, nerve ablation, and surgery are rarely required. But if necessary, it can be beneficial for those cases.
Causes
A variety of the neck’s anatomical structures can contribute to the pain. Common causes include:
Poor posture
Age
Degeneration
Ergonomics
Injury to muscles or ligaments
Arthritis
All of these can affect vertebral bodies, discs, and facet joints. Shoulder arthritis or a rotator cuff tear can imitate axial neck pain. Dysfunction of the temporomandibular jaw joint or the blood vessels of the neck can cause axial pain, but it is rare.
Prognosis
Symptoms are usually alleviated within 4-6 weeks from when the pain started. Pain that continues beyond this should encourage a visit to a chiropractic physician.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine