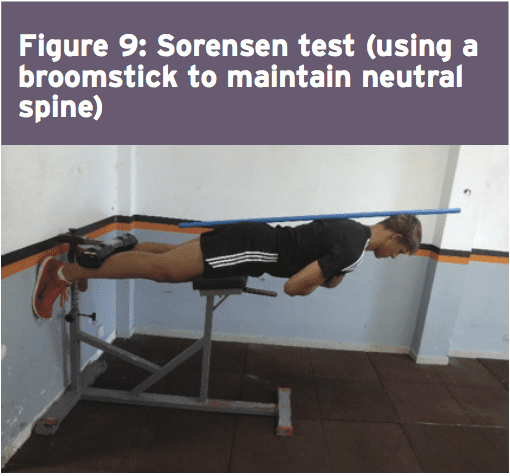
Two surgeons discuss the diagnosis and treatment of acromioclavicular injuries in athletes. El Paso, TX. Chiropractor, Dr. Alexander Jimenez follows the discussion.
Acromioclavicular (AC) joint injuries most often occur in athletic young adults involved in collision sports, throwing sports, along with overhead activities like upper-extremity strength training. They account for 3% of all shoulder injuries and 40% of shoulder sports injuries. Athletes in their second and third decade of life are more often affected(1), and men are injured more commonly than women (5:1 to 10:1)(1,2).
Acromioclavicular dislocation was known as early as 400 BC by Hippocrates(3). He cautioned against mistaking it for glenohumeral (shoulder joint) dislocation and advocated treating with a compressive bandage in an attempt to hold the distal (outer) end of the clavicle in a diminished position. Almost 600 decades later Galen (129 AD) recognized his own acromioclavicular dislocation, which he sustained while wrestling(3). He left the tight bandage holding the clavicle down as it was too uneasy. In today’s era this injury is better known, but its treatment remains a source of fantastic controversy.
Anatomy
The acromioclavicular joint combines the collarbone to the shoulder blade and therefore links the arm to the axial skeleton. The articular surfaces are originally hyaline cartilage, which affects to fibrocartilage toward the end of adolescence. The average joint size is 9mm by 19mm(4). The acromioclavicular joint contains an intra-articular, fibrocartilaginous disc which may be complete or partial (meniscoid). This helps absorb forces in compression. There is marked variability in the plane of the joint.
Stabilizers
There is little inherent bony stability in the AC joint. Stability is provided by the dynamic stabilizers — namely, the anterior deltoid muscle arising from the clavicle and the trapezius muscle arising from the acromion.
Additionally, there are ligamentous stabilizers. The AC ligaments are divided into four — superior, inferior, anterior and posterior. The superior is most powerful and blends with muscles. The acromioclavicular ligaments contribute around two- thirds of the constraining force to superior and posterior displacement; however, with greater displacement the coracoclavicular ligaments contribute the major share of the resistance. The coracoclavicular ligament consists of the conoid and trapezoid. The conoid ligament is fan-shaped and resists forwards motion of the scapula, while the more powerful trapezoid ligament is level and resists backward movement. The coracoclavicular ligament helps bunch scapular and glenohumeral (shoulder joint) motion and the interspace averages 1.3 cm.
Mechanism Of Injury
The athlete who sustains an acromioclavicular injury commonly reports either one of two mechanisms of harm: direct or indirect.
Direct force: This is when the athlete falls onto the point of the shoulder, with the arm usually at the side and adducted. The force drives the acromion downwards and medially. Nielsen(5) found that 70 percent of acromioclavicular joint injuries are caused by an direct injury.
Indirect force: This is when the athlete falls onto an outstretched arm. The pressure is transmitted via the humeral head into the acromion, therefore the acromioclavicular ligament is disrupted and the coracoclavicular ligament is stretched.
On Examination
The athlete presents soon after the severe injury with his arm splinted to his side. The patient may state that the arm feels better using superiorly directed support on the arm. Most motions are limited secondary to pain near the top of the shoulder; the degree varies with the grade of sprain. The hallmark finding is localized swelling and tenderness over the acromioclavicular joint.
In dislocations, the outer part of the collarbone will appear superiorly displaced using a noticeable step deformity (in fact, it is the shoulder which sags beneath the clavicle). Occasionally, the deformity may only be apparent later, if first muscle spasm reduces acromioclavicular separation. Forced cross-body adduction (yanking the affected arm across the opposite shoulder) provokes discomfort. The clavicle can frequently be moved relative to the acromion.
Acromioclavicular Visualisation
The typical joint width measures 1-3mm. It’s regarded as abnormal if it is more than 7mm in men, and 6mm in women. Routine anteroposterior views of the shoulder reveal the glenohumeral jointnonetheless, that the acromioclavicular joint is over penetrated and so dark to interpret. Reduced exposure enhances visualization. The individual stands with both arms hanging unsupported, both acromioclavicular joints on one film. Weighted viewpoints (stress X-rays) are obtained with 10-15 lb weights not held but suspended from the individual’s wrists. They help differentiate type II-III injuries, but are of little clinical significance and therefore are no longer recommended in our practice.
Classification Of AC Separation
The importance of identifying the injury kind can’t be over emphasized because the treatment and prognosis hinge on an accurate diagnosis. The injuries are graded on the basis of that ligaments are injured and how badly they’re torn.
Allman (6) classified acromioclavicular sprains as grades I, II and III, representing respectively, no involvement, partial tearing, and total disruption of the coracoclavicular ligaments. More recently, Rockwood (1) has further classified the more severe injuries as standard III-VI.
The injuries are classified into six categories:
Type I This is the most common injury encountered. Only a mild force is needed to sustain such an injury. The acromioclavicular ligament is sprained with an intact coracoclavicular ligament. The acromioclavicular joint remains stable and symptoms resolve in seven to 10 days. This injury has an excellent prognosis.
Type II The coracoclavicular ligaments are sprained; however, the acromioclavicular ligaments are ruptured. Most players can return to their sport within three weeks. There is anecdotal evidence to suggest that steroid injections into the acromioclavicular joint speed up the resolution of symptoms, but this practice is not universal.
Type III The acromioclavicular joint capsule and coracoclavicular ligaments are completely disrupted. The coracoclavicular interspace is 25-100% greater than the normal shoulder.
Type IV This is a type III injury with avulsion of the coracoclavicular ligament from the clavicle, with the distal clavicle displaced posteriorly into or through the trapezius.
Type V This is type III but with exaggeration of the vertical displacement of the clavicle from the scapula-coracoclavicular interspace 100-300% greater than the normal side, with the clavicle in a subcutaneous position.
Type VI This is a rare injury. This is type III with inferior dislocation of the lateral end of the clavicle below the coracoid
Treatment
The treatment of acromioclavicular joint injuries varies based on the seriousness or grade of the injury.
Initial treatment: These can be quite painful injuries. Ice packs, anti-inflammatories plus a sling are utilized to immobilize the shoulder and then take the weight of the arm. As pain starts to subside, it is important to start moving the fingers, wrist and elbow to prevent shoulder stiffness. Next, it’s important to begin shoulder motion in order to stop shoulder stiffness.
Un-displaced injuries only require rest, ice, and then a slow return to activity over two to six weeks. Major dislocations require surgical stabilization in athletes if their dominant arm is involved, and if they participate in upper-limb sports
Type I & II: Ice pack, anti-inflammatory agents and a sling are used. Early motion based on symptoms is introduced. Pain usually subsides in about 10 days. Range-of-motion exercises and strength training to restore normal motion and strength are instituted as the patient�s symptoms permit. Some symptoms may be relieved by taping (taking stress off acromioclavicular joint). The length of time needed to regain full motion and function depends upon the severity or grade of the injury. The sport and the position played determine when a player can return to a sporting activity. A football player, who does not have to elevate his arm, can return sooner than a tennis or rugby player. When a patient returns to practice and competition in collision sports, protection of the acromioclavicular joint with special padding is important. A simple �doughnut� cut from foam or felt padding can provide effective protection. Special shoulder- injury pads, or off-the-shelf shoulder orthoses, can be used to protect the acromioclavicular joint after injury.
Some Type II injuries may develop late degenerative joint changes and will need a resection of the distal end of the clavicle for pain relief. It is important to note that after a resection of the distal end of the clavicle, particularly in a throwing athlete, there may be formation of heterotopic bone on the under surface of the clavicle which can cause a painful syndrome which presents like shoulder impingement.
Type III: The treatment of type III injury is less controversial than in past years. In the 1970s, most orthopaedic surgeons recommended surgery for type III acromioclavicular sprains(7). By 1991, most type III injuries were treated conservatively(8). This change in treatment philosophy was prompted by a series of retrospective studies(9). These showed no outcome differences between operative and nonoperative groups.
What’s more, the patients treated non-operatively returned to full activity (work or athletics) earlier than surgically treated groups(10, 11). The exceptions to this recommendation include people who perform repetitive, heavy lifting, people who operate with their arms above 90 degrees, and thin patients who have prominent lateral ends of the clavicles. These patients may benefit from surgical repair(12).
Any discussion about the management of acute injuries to the AC joint must deal with which of the many methods of surgical therapy described is the best for their situation, but whether surgery should be considered at all. Surgery is generally avoided in athletes participating in contact sports since they will often re-injure the shoulder later on.
Type IV-VI: Account for more than 10-15% of total acromioclavicular dislocations and should be managed surgically. Failure to reduce and fix these will lead to chronic pain and dysfunction.
Surgery
Surgical repair can be divided into anatomical or non- anatomical, or historically into four types:
? Coracoclavicular repairs (Bosworth screws(13), cerclage, Copeland and Kessel repair).
? Distal clavicular excision.
? Dynamic muscle transfers.
? Disadvantages of surgery are that there are risks of infection, a longer time to return to full function and continued pain in some cases.
For the individual with a chronic AC joint dislocation or subluxation that remains painful after three to six months of closed treatment and rehabilitation, surgery is indicated to improve functioning and comfort.
For sequelae of untreated type IV-VI, or painful type II and III injuries, the Weaver Dunn technique is advocated. This�entails removing the lateral 2cm of the clavicle and reattaching the acromial end of the coracoacromial ligament to the cut end of the clavicle, thus reducing the clavicle to a more anatomical position.
Postoperatively, the arm is supported in a sling for up to six weeks. Following the first two weeks, the patient is permitted to use the arm for daily activities at waist level. After six weeks, the sling or orthosis is discontinued, overhead actions are allowed, formal passive stretching is instituted, and light stretching using elastic straps is initiated. Stretching and strengthening are begun slowly and gradually. The athlete shouldn’t return to their sport without restriction until full strength and range of motion has been recovered. This usually occurs four to six months following operation.
Conclusion
AC joint injuries are an important source of pain at the shoulder area and have to be assessed carefully. The management of these injuries is nonoperative in the majority of cases. Type I and II injuries are treated symptomatically. The present trend in uncomplicated type III injuries are a non operative strategy. In the event the athlete develops following problems, a delayed reconstruction might be undertaken. In athletes involved in heavy lifting or prolonged overhead activities, surgery may be considered acutely. Type IV-VI injuries are generally treated operatively.
No matter what kind of treatment is chosen, the ultimate purpose is to restore painless function to the wounded AC joint so as to reunite the athlete safely and as quickly as possible back to their sport. It is possible in the vast majority of acromioclavicular joint injuries.
References
Reza Jenabzadeh and Fares Haddad
1. Rockwood CA Jr, Williams GR, Young CD. Injuries of the Acromioclavicular Joint. In CA Rockwood Jr, et al (eds), Fractures in Adults. Philadelphia: Lippincott-Raven, 1996; 1341-1431.
2. Dias JJ, Greg PJ. Acromioclavicular Joint Injuries in Sport: Recommendations for Treatment. Sports Medicine 1991; 11: 125-32.
3. Adams FL. The Genuine Works of Hippocrates (Vols 1,2). New York, William Wood 1886.
4. Bosworth BM. Complete Acromioclavicular Dislocation. N Eng J Med 2 41: 221-225,1949.
5. Nielsen WB. Injury to the Acromioclavicular Joint. J Bone Joint Surg 1963; 45B:434-9.
6. Allman FL Jr. Fractures and Ligamentous Injuries of the Clavicle and its Articulation. J Bone Joint Surg Am 1967;
49:774- 784.
7. Powers JA, Bach PJ: Acromioclavicular Separations: Closed or Open Treatment? Clin Orthop 1974; 104 (Oct): 213-223
8. Cox JS: Current Methods of Treatment of Acromioclavicular Joint Dislocations. Orthopaedics 1992; 15(9): 1041-1044
9. Clarke HD, Mc Cann PD: Acromioclavicular Joint Injuries. Orthop Clin North Am 2000; 31(2): 177-187
10. Press J, Zuckerman JD, Gallagher M, et al: Treatment of Grade III Acromioclavicular Separations: Operative versus
Nonoperative Management. Bull Hosp Jt Dis 1997;56(2):77-83
11. Galpin RD, Hawkins RJ, Grainger RW: A Comparative Analysis of Operative versus Nonoperative Treatment of Grade III Acromioclavicular Separations. Clin Orthop 1985; 193 (Mar): 150-155
12. Larsen E, Bjerg-Nielsen A, Christensen P: Conservative or Surgical Treatment of AC Dislocation: A Prospective, Controlled, Randomized Study. J Bone Joint Surg Am 1986;68(4):552-555
13. Bosworth BM. Complete Acromioclavicular Dislocation. N Engl. J. Med. 241: 221-225,1949.
Core chiropractor, Dr. Alexander Jimenez continues from part I through the core stability routines.
Menu 6: Pulley, Standing
This menu challenges pelvic stability during unilateral standing upper body movements. The kinds of arm movements undertaken in many sports create strong rotational forces that have to be controlled by the trunk and pelvic muscles. The aim of these exercises, therefore, is to develop co-ordination and control of the pelvis.
Research has shown that unilateral exercises increase the recruitment of the core musculature. The core and pelvic muscles will all be using static contractions to hold the required postures, while the upper body muscles will be producing the limb movements. The resistance load on the arm is secondary to the stability challenge of the core. Overall this menu is intermediate.
Rear Sling
Overview: The challenge of this exercise and its pair (see opposite) is to establish perfect pelvic alignment, while standing on one leg, against a rotational force from the upper body.
Technique: Stand on one leg to the side of the pulley column. Handle is attached at below-hip height. Grasp the handle with the hand on the opposite side (opposite to standing leg). Set perfect posture and pelvic alignment.
Brace the core and then pull the weight up and around the body, keeping the elbow straight, so that the arm rotates up
and out. Finish with hand above your head and out to the side slightly. The aim is to maintain perfect balance and pelvic
alignment as you raise and lower the arm diagonally. Reposition to repeat exercise for opposite leg/arm.
Perform 10 reps each side increasing to 20 reps; 2 to 3 sets.
Progression: Increase the weight.
Front Sling
Overview: This is the natural opposite of the rear sling exercise. It involves a forward arm rotation, which must be controlled.
Technique: Stand on one leg to the side of pulley column. Handle is attached at above shoulder height. Grasp the handle with the arm nearest the column (opposite side to standing leg). Set perfect posture and pelvic alignment.
Brace your core; pull the weight down and around the body, keeping the elbow straight so that the arm rotates down and round. Finish with hand next to your hip across your body. The aim is to maintain perfect balance and pelvic alignment as you lower and raise the arm. Reposition to repeat with opposite leg/arm.
Perform 10 reps each side, increasing to 20 reps; 2 to 3 sets.
Progression: Increase the weight.
One Leg, One Arm Rowing
Overview: The challenge of this exercise is to maintain stability while standing on one leg and controlling against a pulling force from the upper body. The pelvis must stay fixed when the upper back and shoulder are pulling backwards.
Technique: Stand on one leg, facing the pulley column. Handle is attached at waist height. Grasp the handle with the opposite arm (same side as lifted leg). Your hand will be out directly in front of you in the start position. Set perfect posture and pelvic alignment, standing tall with shoulders back.
Brace your core; pull on the cable, leading with the elbow in a rowing movement Finish with hand by your side and elbow behind you. The aim is to maintain perfect balance and pelvic alignment as you perform the rowing movement. Reposition to repeat with opposite leg/arm.
Perform 10 reps each side; 2 to 3 sets.
Progression: Increase the weight.
Menu 7: Medicine Ball, Floor
The four exercises in this menu all involve throwing and catching the medicine ball while performing a trunk flexion or rotation movement. The action of throwing the ball during the muscle-shortening phase of each of the exercises increases the force production of the trunk muscles. The action of catching the ball at the start or during the muscle-lengthening phase of each exercise not only increases the force production but also the overall stability challenge.
The impact that the catch has on the upper limb has to be controlled by the trunk. You should be aiming to maintain good spine alignment and correct movement while making the catch. Only use a weight of medicine ball that will allow you to perform the exercises with good technique. If the ball is too heavy, you will sacrifice core stability, irrespective of your arm strength.
Overall these exercises are advanced. However they are also safe and effective for young athletes using light medicine balls to develop dynamic trunk movement and control.
Sit Up & Throw
Overview: An advanced version of a sit-up exercise, in which the throwing action makes the crunch phase faster and the catching action adds load to the return phase.
Level: Advanced
Muscles targeted: Abdominals (Plus upper body)
Technique: You will need a partner to receive and pass the ball. Alternatively perform the exercise in front of a wall and use a medicine ball that will bounce back.
Start in the sit-up position (knees bent) with hands up ready�to receive the ball. Catch the ball and begin to lower back down. Do not collapse back down, control it with the abs and keep hands above the head as you lower down.
Once shoulders are touching the floor (keeping head up and eyes forward), reverse the movement. Throw the ball forward and crunch up at the same time. Follow the throwing action and complete the sit-up as fast as possible. Make sure you crunch as you throw so that the abs contribute to the force of the throw and help you sit up faster. Men should start with a 5kg ball; women with a 3kg ball.
Perform 10 to 20 reps; 2 to 3 sets
Progression: Progress to heavier ball once 3 sets of 20 reps is comfortable
45-degree Sit, Catch and Pass
Overview: A very tough stability exercise that requires massive trunk musculature co-contraction to hold a good spine alignment against the impact of making the catch.
Technique: Sit up with knees bent and lean back at 45 degrees. Aim to hold a �lengthened� spine, with lumbar spine in neutral, shoulders back and neck long and relaxed. It takes a fair amount of control and strength endurance simply to hold this posture perfectly. Aim to get this right before progressing on to the catch and pass.
Raise hands in front of your face and receive a pass from a partner, around this height. As you catch the ball you must hold the long spine position. Do not flex the low back, or become round-shouldered. Gently throw the ball back. Men should start with a 3kg ball; women with a 2kg ball.
Complete a few passes, holding the position for 30 seconds. Perform 2 to 3 sets.
Progression: Raising the hands to above head height makes the stability challenge of the catch significantly harder. Catches made to either side of the head are also more challenging.
Sit & Twist Pass
Overview: A trunk rotation exercise involving catching and passing the medicine ball, which provides a challenge to the obliques to produce powerful rotation, but also pelvic stability, so that the sitting position is stable throughout the movement.
Level: Advanced
Muscles targeted: Abdominals, Obliques
Technique: Sit up with knees bent and lean back at 45 degrees. Aim to hold a �lengthened� spine, with lumbar spine in neutral, shoulders back and neck long and relaxed. Your feet, knees and hips should remain reasonably still throughout this exercise, the rotation coming from your waist and not your hips.
Hold hands to one side ready to receive the ball. Catch the ball to one side and absorb the catch by turning your shoulders further to that side. Reverse the rotation, turning back to the middle and release the ball. Continue rotating to the other side; receive the ball the other side and continue. Ensure you�can hold good posture throughout the movement, with a long spine and wide shoulders. Men should start with a 4 to 5kg ball; women with a 2 to 3kg ball.
Perform 10 to 20 reps.
Progression: Increase the weight of the ball once you can perform a set of 20 reps comfortably with perfect technique.
Kneeling Twist Pass
Overview: To perform the rotation movement in this position demands a greater range of motion, helping to develop strength through the full range of trunk rotation. It may also help to develop trunk rotation range of movement.
Level: Intermediate to advanced
Muscles targeted: Obliques
Technique: Kneel upright with good posture (lumbar spine in neutral, chest out, shoulders low). Start with the ball in hands and twist shoulders and head round as far as you can. Then, under control, twist around to the other side as far as possible, and hand the ball to partner. Turn back to the start position, receive the ball again and continue.
The aim of the movement is to rotate through the biggest shoulder turn you have. You can allow the hips to rotate a little with the shoulders, but not too much. You should feel a stretch in the side at the end of each twist.
As you gain greater flexibility and stability you will be able to�fix your pelvis square to the front and rotate through an increasingly full range of motion. Men should start with a 5 to 6kg ball; women with a 3 to 4kg ball.
Perform 10 reps then take the ball to the opposite side and repeat.
Menu 8: Medicine Ball, Standing
The aim of this menu is to perform trunk movements while standing on one leg. This is functional training for balance in sports and daily living activities. These exercises are advanced because of the requirements for lower limb balance and body movement awareness, which makes controlled performance of these trunk movements quite difficult. These moves also use the hip rotator and abductor muscles for control and stability.
One-leg Twist Pass
Overview: A trunk rotation exercise performed on one leg. This requires good pelvic stability at the hip of the standing leg, for the trunk rotation to be dissociated from the pelvis.
Technique: Stand on one leg with hips facing square to the front. Hold medicine ball slightly out in front. Slowly twist from side to side. The rotation comes from the waist only,�head turning with the shoulders. Keep pelvis fixed square and knee in line with second toe throughout. Men should start with a 5 to 6 kg ball; women with a 3 to 4 kg ball.
Perform 10 slow reps; 2 to 3 sets. Repeat on other leg.
Progression: Swap the ball for a pulley machine and add resistance, once you have mastered the controlled balance on one leg.
One-leg Deadlifts with Rotation
Overview: An advanced exercise for the posterior chain of muscles, which includes rotation to challenge control of pelvis.
Level: Advanced
Muscles targeted: Erector spinae, Gluteals (max and med) Hamstrings, Piriformis
Technique: Stand on one leg. Flex the free leg a little at the knee to lift it off the floor, but do not flex or extend the hip of the free leg throughout the movement, in order to keep pelvis in control. Hold the ball in front of you.
Bend down, flexing at the knee and the hip. Lower down until the ball touches the floor by your foot, all the time keeping your arms straight and without reaching excessively with your upper back (ie, maintain a reasonably flat back). Stand back up, pushing down through the foot to use your gluteals correctly to extend the hips.
Alternate between touching the ball down on the inside and then the outside of the standing foot. This means you are internally or externally rotating the hip on alternate repetitions, challenging control of hip rotation. Keep the knee in line with�second toe as much as possible throughout. Men should use a 5kg ball; women use a 3kg ball.
Start with 5 slow controlled reps, 2 to 3 sets. Build up to 10 reps. Repeat on the opposite leg.
Progression: Increase the weight of the ball or use a dumb-bell as you get stronger.
One-leg Catch & Pass
Overview: The main aim of this exercise is to control the impact of the catch without losing balance or rotating excessively at the hips. It�s all about how effectively you can anticipate the impact and produce the required stiffness throughout the body to retain good posture and control. This is a very useful �reaction�-type stability exercise.
Level: Advanced
Muscles targeted: Everything
Technique: Stand on one leg with good posture (lumbar spine neutral, chest out, shoulders wide) and with hips square to the front. Hold hands up ready to catch. Receive catches anywhere within arm�s reach. Make sure the passes are varied in their placement. Aim to restrict movement to arms and/or turning your shoulders, keeping the pelvis and lower limb stable. Use a 2 to 3kg ball that is not too big, so it is easy to catch.
Start with 30 sec bouts of catch and pass on each leg; 2 to 3 sets.
Progression: Receive more forceful passes so the impact of the catch is greater.
Menu 9: Resistance-Based
Menu rationale
The aim of these three exercises is to progress the loading in order to build high-level trunk muscle strength. These exercises can be performed in the 5- to 10-repetition range with a suitably high weight for this number of reps. As you get stronger, you should prioritize an increase in weight rather than an increase in the number of reps. Overall, these exercises are very advanced.
Crunch with Weight
Overview: The standard isolated abdominal exercise with increased load.
Level: Advanced
Muscles targeted: Abdominals
Technique: Perform the crunch in the usual way: knees bent, low back flat, head up and looking forward. Curl the shoulders up and down using just the abdominals. The weight (medicine ball, dumb-bell or barbell weight plate) should be held above or behind the head. Arms are fixed, all they do is hold the weight in place. Do not use arms to move the weight relative to head as the crunch is performed. Keeping the elbows out helps to achieve this.
Perform 5 to10 reps; 2 to 3 sets.
Progression: Increase weight, maintaining the range of 5 to 10 reps per set.
Reverse Hypers
Overview: An excellent hip and back extension exercise to which it is very simple to add load.
Level: Advanced
Muscles targeted: Erector spinae, Gluteals
Technique: Lie on your front on a horizontal bench, with hips just off the end of the bench. Grasp bench legs firmly for support. Your legs should be straight with a dumb-bell between the ankles for resistance. Squeezing the gluteals, extend hips and lift legs and the dumb-bell off the floor. Stop when your back is slightly hyper-extended and hips are fully extended. Lower slowly until feet are just off the floor and continue.
Perform 8 to 10 reps; 2 to 3 sets.
Progression: Increase weight, maintaining the range of 8 to 10 reps per set.
Reverse Crunch with Weight
Overview: This is a great exercise, as it requires good co- ordination and strength. Research shows that the obliques as well as the abdominals work very hard during this exercise, making it excellent value.
Level: Advanced
Muscles targeted: Abdominals, Obliques
Technique: Lie on back with hands behind head and elbows out to the sides. Knees should be bent and heels close to bum. Hold weight between your legs. Initiate the movement by curling the pelvis upwards (flattening the back into
the floor) and then continue to use the abs to pull the low back and pelvis off the floor. This is the bit that requires good co- ordination, as the temptation is to kick with the legs and pull the hips up with the hip flexors. Learn to focus on the abs before you add weight, as if you do this strictly it is very tough, especially for women (whose pelvises are relatively heavier).
Perform 5 to 10 reps; 2 to 3 sets.
Progression: Increase weight, maintaining the range of 5 to 10 reps per set.
Menu 10: Hanging Bar
Menu rationale
The aim of these three exercises is to work the abdominals as hard as possible with very advanced, gymnastic-style movements. Reasonable upper body strength is required for these exercises.
Hanging Leg Lifts
Overview: This exercise requires you to lift the full weight of your legs and (if possible) your pelvis, while hanging from a bar. Anyone who can perform these movements well through a good range of motion has achieved good strength.
Level: Advanced
Muscles targeted: Abdominals, Obliques, Hip flexors
Technique: Hang from a bar with arms straight. Lift knees, bringing them up as high as possible. At the top of the movement the knees should be near the chest and pelvis should be curled upwards (low back flexed). This extra curl of the pelvis ensures that the abdominals are working maximally. Do not kick legs up or swing the body excessively. Simply draw up knees, crunching as you lift. It is important to feel that the abdominals are doing the lion�s share of the work rather than the hip flexors or front of thigh muscles.
Perform 5 to 10 reps;, 2 to 3 sets.
Progression: Perform the same exercise with straight legs, lifting them up to 90 degrees in front of you, curling the pelvis at the top of the movement.
Windscreen Wipers
Overview: The ultimate ab-buster. Anyone who can do 10 reps of this exercise with good technique has a very strong core!
Level: Super advanced
Muscles targeted: Abdominals, Obliques, Hip flexors
Technique: Hang from bar with arms straight. Lift legs up in the air until feet are at approx head height. Maintaining the height of the lift, take the legs from side to side in an arc. The movement will look like a windscreen wiper, moving from side to side. Aim for at least 45 degrees of movement to each side.
Perform 5 to10 reps; 2 to 3 sets.
Progression: The straighter the legs, the harder the exercise. Increasing the range of movement to each side also makes it tougher.
Candlesticks
Overview: Another beauty! Lots of strength required to control this movement; only for the very strong.
Level: Super advanced
Muscles targeted: Abdominals, Obliques, Hip flexors
Technique: Lie flat and raise yourself up to a shoulder stand position, holding on to a bench/table leg/partner’s leg with your hands above your head. Establish a fully extended hip and leg position and then begin to lower your body down slowly to the floor. The body should move in an arc as a single unit (no sagging in the back, or bending at the hips or knees). Lower under control from vertical to just above horizontal.
Gripping firmly for stability, lift your body back up into shoulder stand, again keeping everything straight and aligned in a single unit.
Slow and controlled movement on the way down will help, and a maximal contraction of everything will get you back up.
El Paso, TX. science based chiropractor, Dr. Alexander Jimenez looks at this uncommon problem � and how it can be treated.
The true incidence of obturator externus accidents is unknown, as frequently they may be misdiagnosed as hip joint pathology and/ or groin pathology as the website of symptoms as well as also the presenting objective signals may mimic other pathologies such as hip joint labrum pathology, anterior femoral triangle issues and perhaps even gluteal pathology.
Injury for this muscle gifts as a deep obscure groin/hip pain and functionally the muscle may still hide direct involvement as a pain generator since it is primarily a equilibrium muscle rather than a force-producing hip muscle.
This case study presents an unusual case of hip-related pain in a professional baseball player which also shown itself as an injury to the contralateral adductor longus.
The Player
As he was wrestled to the floor, his right hip was compelled at a rapid and loaded flexion/internal turning position. His first sensation was pain deep inside the anterior hip/groin area.
When he presented to the medical team with the accident, he complained of a profound catching sensation inside the hip joint location. It had been difficult to fully bend the hip and to also twist on the stationary limb (because he did whilst kicking a ball). His prior background consisted of a right-sided inguinal hernia repair five seasons before as well as a few gentle on again/off back osteitis pubis-type signs that would normally flare from the first period as his goal-kicking amounts have been increased. He was obviously a left- footed goal kicker.
On examination, he observed that the pain to become worse on passive flexion/internal rotation of the hip (hip walkway test). He was noticeably tight and irritated from the shallow TFL muscle, and also posteriorly across the greater trochanter around the insertion for the gluteals and deep hip rotators. He was also particularly high tone in the right iliopsoas muscle.
He was initially diagnosed clinically because of hip joint sprain due to the mechanism of harm being a pressured flexion/internal rotation type position that would always put pressure on the anterior hip joint capsule/labrum.
He was treated initially with deep iliopoas muscle sparks and hip joint mobilizations using a seat belt to gap the hip joint. He reacted reasonably well with the therapy and immediately felt more comfortable on a hip joint quadrant test. He was rested from coaching for 2 days and ran on the next day and played a match on the fourth day. But during the match, though his right hip did not create any pain, he’d notice pain on his left adductor source that was more pronounced during kicking.
Three days post-game he detected this ongoing left adductor origin pain and it was made worse by kicking again through training. An MRI was performed to Look at the left adductor origin and also the report noted:
Grade 1 left adductor longus strain deep in the
Grade 2 right obturator externus strain on its femoral attachment
Grade 1 right iliopsoas muscle strain in the MTJ.
The surprise finding on the MRI of a grade 2 obturator strain prompted the medical team to more formally assess the participant for ongoing hip joint disorder. The particular features to notice from this medical examination were:
Subjective
? A sensation of weakness and instability in the right hip whilst kicking with the left foot.
? No pain in the right hip with running, even with top-end speed. However, the left adductor longus was symptomatic on running and kicking.
Objective
? Pain on passive right hip internal rotation whilst in 90-degree hip flexion. This pain was deep anteriorly in the hip, almost presented as a groin problem.
? Some discomfort on resisted right hip flexion/external rotation deep inside the iliac fossa.
? Pain and weakness in the left adductor on adductor squeeze tests. These squeeze tests performed at 0/45/90 degrees of knee flexion with a pressure cuff between the knees. Usual pre-season scores measured 260/260/250. On current testing they measured 150/170/180. Pain was felt at the end of the squeeze.
? Discomfort with prone lie hip passive internal rotation. This pain was more focused around the right greater trochanter posteriorly.
Pathomechanics
It had been suspected that this player had endured a secondary injury to the left adductor longus (a muscle used a lot in goal-kicking) due to the inherent failure in bolstering the proper hip throughout the plant phase of the kick due to the inhibition of the right obturator externus, a muscle considered to be an important hip stabilizer and turning control muscle at the hip. With insufficient hip stabilization in kicking, the left hip was required to create more power to compensate for the unstable right hip to gain the length from the kick. Then the left adductor longus failed along with a strain injury led.
Management
The management of the matter initially centered on the two key features being the left-sided adductor strain and the right- sided obturator externus strain.
In the week following the accident, the player was sent to get a series of Actovegin shots to the left adductor longus. This was done according to protocol that was three injections every 48 hours — Monday/ Wednesday/Friday. In this five-day period the adductor longus was handled with deep tissue flush massage and gentle isometric adduction exercises at supine (chunk squeezes) in the three positions of examining — 0/45/90 levels of knee flexion — also as wall squat adductor squeezes in the same positions. The obturator externus was medicated with heavy tissue releases (obtained through the anterior groin region) and direct theraband strengthening of hip external rotation in sitting and in prone. Actovegin shots to the obturator externus are regarded as difficult because of problems with accessing this muscle through the superficial hip musculature.
The adductor exercises progressed into through array adduction with theraband resistance (equally with the left leg being the motion leg as well as the stability leg).
By 12 days post-injury it had been detected that the obturator externus strength had not improved and the player still had deep- seated right back pain pain. It was rationalised that perhaps the direct treatment to this muscle and also the direct open kinetic chain strengthening was possibly making the muscle texture worse. The choice was made to stop any direct hands-on therapy to the muscle and also to prevent any direct open kinetic chain strengthening. Instead the player lasted with bilateral theraband exercises of both hips into flexion and then abduction and expansion in addition to adduction. The avoidance of lead obturator externus soft tissue treatment and exercise appeared to improve the hip function immediately.
The participant started running 20 times post-injury and quickly progressed through running stages over a five-day period of conducting on alternate days. At this point the player’s adductor squeeze scores had improved to steps according to pre- season baselines. However, daily the player ran direct adductor strength operate using a Pilates reformer as a slider drill to immediately load into adduction in addition to hammering theraband adduction exercises in standing and in supine lying.
By 27 days post-injury the player managed to begin kicking, change in direction and rugby training. He played at 30 times post-injury with no ill effects.
Discussion
It arises immediately around the medial side of the obturator foramen, as well as the inferior ramus of the ischium; it also arises in the lateral two-thirds of this outer surface of the obturator membrane, and also in the tendinous arch which completes the canal to the passage of the obturator nerves and vessels.
The action of the muscle is to externally rotate the hip and also helps in hip adduction. It’s postulated to also work as a hip balance muscle in one legged stance along with the obturator internus, quadrutus femoris, piriformis and the gemelli muscles. In a practical activity such as kicking, the muscle acts to stabilize or hold the ball of the femur into the socket (acetabulum).
The incidence of harm to the obturator externus muscle is unknown because there are only a handful of case reports from the medical literature that highlight injuries for this muscle. Additionally, among the vexing issues is the difficulty in creating the correct clinical diagnosis based on the history and physical evaluation. MRI imaging is needed to correctly picture injuries to this muscle.
From the case study introduced, injury for the muscle was a direct result of forceful flexion/internal rotation mechanism to the hip joint. As the muscle primarily functions as a hip stabilizer during jogging, it is possible that a patient can mask symptoms during functioning as the muscle isn’t required to produce any hip skate for locomotion.
Nonetheless, in this event the muscle has a role in stability of the hip during kicking, and for that reason may have produced a poor pelvic/hip complicated during kicking that then led to an accident to the adductor longus on the other hand.
In addition, it seems that direct treatment to the muscle in the form of deep trigger point releases and also direct strengthening may actually delay healing in the muscle in case of injury. This may highlight the value of the muscle as a hip stabilizer instead of a legitimate torque manufacturer in hip rotation.
Most of us will experience it at some point — but how does it influence on athletic performance? Chiropractic injury specialist, Dr. Alexander Jimenez investigates.
Research postulates that 80 percent of the populace will undergo an acute onset of back pain at least once in their lifetimes. This adds a considerable financial burden not just on the medical system (physician consultations, prescribed drugs, physiotherapy) but also the financing of the workforce in lost employee hours and loss in productivity.
The types of lower back pain that an individual may experience include (but are not limited to):
1. Lumbar spine disc herniation with/ without sciatica
8. Inflammatory arthritis such as rheumatoid and anklyosing spondylitis
9. Facet joint sprains
10. Bone injuries such as stress fractures, pars defects and spondylolisthesis.
The focus for this paper will be on the previous group — that the bone injuries. This may be simply postural (slow onset repetitive trauma) or related to sports; for instance, gymnastics.
The two demographic groups that tend to endure the most extension-related low back pain are:
1. People who endure all day, for instance, retailers, army, security guards etc.. Prolonged position will obviously force the pelvis to start to migrate to an anterior tilt management. This may begin to place compressive pressure on the facet joints of the spinal column as they also change towards an expansion position since they accompany the pelvic tilt.
2. Extension sports such as gymnastics, tennis, swimming, diving, football codes, volleyball, basketball, track and field, cricket fast bowlers. This is more pronounced in sports that involve extension/rotation.
Pathomechanics
With normal extension of the lumbar spine (or backward bending), the facet joints begin to approximate each other and compress.�The articular processes of this facet above will abut the articular process of the facet below. This is a normal biomechanical movement. However, if the extension ranges are excessive, the procedures will impinge quite aggressively and damage to the cartilage surfaces within the facet joint can result. Sports such as gymnastics, functioning in tennis, and handling in American Soccer may all involve uncontrolled and excessive extension.
It would be unlikely that a bone stress response or even a stress fracture could be brought on by an isolated expansion injury. It would be more likely that a sudden forced extension injury may damage an already pre-existing bone strain reaction.
Similarly, if an individual stands daily and the pelvis migrates into lateral tilt, then the aspects will be placed under low load compression but for extensive intervals.
With ongoing uncontrolled loading, stress is then transferred from the facet joint to the bone below (pars interarticularis). This originally will manifest as a pressure reaction on the bone. This bone strain may advance to a stress fracture throughout the pars if uncorrected. This fracture is also referred to as a “pars flaw”, or spondylolysis.
It was initially considered that stress fractures of the pars was a congenital defect that introduced itself at the teenage years. However, it is now agreed that it is probably obtained through years of overuse into extension positions, especially in young sportspeople involved with expansion sports. What’s more, one-sided pars defects often occur more commonly in sport which also included a rotational component such as tennis serving or fast bowling in cricket.
The stress fracture can then advance to impact the opposite side, causing a bilateral strain fracture, with anxiety subsequently being transferred to the disk in between both levels.
Spondylolisthesis features bilateral pars defects which could possibly be a result of repetitive stress into the bilateral pars in extension athletics, but more likely it is an independent pathology that manifests in the early growing stages (9-14) as this pathology is often viewed in this age category. If they become symptomatic in later years because of involvement in expansion sports, it is exceedingly likely that the defects were there by a young age but presented asymptomatically. As a result of rapid growth spurts in teenage years and the high-volume training experienced by teenaged athletes, it is possible that these dormant spondylolisthesis then pose as ‘acute onset’ back pain in teenage years.
In summary, the progression of this bone stress reactions tends to follow the following continuum:
1. Facet joint irritation
2. Pars interarticularis stress response
3. Stress fracture to the pars
4. Pars defect (or spondylolysis)
5. Spondylolisthesis due to activity or more likely congenital and found later in teenage years due to participation in�extension sports.
The landmark publication related to spondylolysis and spondylolisthesis was presented by Wiltse et al (1976) and they classified these injuries as follows:
1. Type I: dysplastic � congenital abnormalities of L5 or the upper sacrum allow anterior displacement of L5 on the sacrum.
2. Type II: isthmic � a lesion in the pars interarticularis occurs. This is subclassified as
a. lytic, representing a fatigue fracture of the pars,
b. elongated but intact pars, and c. acute fracture.
3. Type III: degenerative � secondary to long-standing intersegmental instability with associated remodeling of the articular processes.
4. Type IV: traumatic � acute fractures in vertebral arch other than the pars.
5. Type V: pathological � due to generalized or focal bone disease affecting the vertebral arch.
The vast majority of spondylolysis and sponylolisthesis accidents are Type II — the isthmic variety.
For the purposes of this paper, we will refer to the above stages as the posterior arch bone stress injuries (PABSI).
Epidemiology
It is a lot more widespread at the L5 level (85-90 percent). It’s a high asymptomatic prevalence in the general population and is often found unintentionally on x ray imaging. Nonetheless, in athletes, particularly young athletes, it is a common reason for persistent low back pain. From the young athlete, the problem is often referred to as ‘active spondylolysis’.
Active spondylolysis is normal in virtually every gamenevertheless, sports such as gymnastics and diving and cricket pose a much greater danger due to the extension and turning character of the sport. The progression from an active spondylolysis into a non-union type spondylolisthesis has been associated with a greater prevalence of spinal disk degeneration.
Early detection through screening and imaging, therefore, will highlight those early at the bone stress phase and if caught early enough and managed, the progression to the larger and more complicated pathologies are avoided as a result of therapeutic capacity of the pars interarticularis in the early stages.
It is more common to find teens and young adults afflicted by PABSI. This will highlight the rapid growth of the spine through growth spurts that is also characterized by a delay in the motor control of the muscle system during this period. Furthermore, it’s thought that the neural arch actually gets stronger in the fourth decade hence possibly explaining the low incidence of bone stress reactions in mid ages.
The incidence of spondylolysis has been reported to be around 4-6% in the Caucasian population (Friedrikson et al 1984). The rates seem to be lower in females and also in African-American males. It has also been suggested that a link exists between pars defects and spina bifida occulta.
The incidence of spondylolysis seems to be higher in the young athletic population than in the general population. Studies in gymnasts, tennis, weightlifting, divers and wrestlers all show disproportionately high incidence of spondylolysis compared with the general population of age-matched subjects.
Tennis
The tennis serve generates excessive extension and rotation force. In addition, the forehand shot may also produce elevated levels of spinning/ extension. The more traditional forehand shot demanded a great deal of weight shift through the legs to the torso and arms. However, a more favorite forehand shot is to currently face the ball and also generate the force of this shot utilizing hip rotation and lumbar spine extension. This action does increase ball speed but also puts more extension and compressive loads on the spine potentially resulting in a greater degree of stress on the bone components.
Golf
The most likely skill component involved in golf that may cause a PABSI are the tee shot with a 1 wood when forcing for distance. The follow-through of this shot entails a significant quantity of spine rotation with maybe a level of spine expansion.
Cricket
Fast bowlers in cricket are the most susceptible to PABSI. This will occur on the opposite side to the bowling arm. As the front foot engages on plant stage, the pelvis abruptly stops moving but the spine and chest continue to proceed. With the wind-up of this bowling action (rotation), when coupled with expansion this can place large forces on the anterior arch of the thoracic. More than 50% of fast bowlers will create a pars stress fracture. Young players (up to 25) are most vulnerable. Cricket governments have implemented training and competition guidelines to avoid such injuries by restricting the number of meals in training/games.
Field Events
The more common field events to cause a PABSI would be high leap followed by javelin. Both these sports create enormous ranges of backbone extension and under significant load.
Contact Sports
Sports like NFL, rugby and AFL all require skill components that need backbone expansion under load.
Gymnastics/Dancers
It goes without saying that gymnastics and dancing involves a substantial amount of repetitive spine expansion, particularly backflips and arabesques. It has been suggested that nearly all Olympic degree gymnasts could have suffered from a pars defect. Many organizing bodies now put limits on the number of hours young gymnasts can instruct to prevent the repetitive loading on the spine.
Diving
Spine extension injuries occur mostly off the spring board and on water entrance.
Diagnosis Of PABSI In Athletes
Clinical investigation
These can pose as preventable injuries. Research shows that the incidence was emphasized from the general population that have nil indicators of back pain. But, individuals will typically complain of back ache that is deep and generally unilateral (one side). This may radiate into the buttock area. The most offending movements tend to be described as expansion moves or backward bending movements. This may be a slow progression of pain or might be initiated by one acute episode of back pain in a competitive extension motion.
On clinical examination:
1. Pain may be elicited with a one-leg extension/rotation test (standing on the leg on the affected side) � stork test.
2. Tenderness over the site of the fracture.
3. Postural faults such as excessive anterior tilt and/or pelvic asymmetry.
The one-legged hyperextension test (stork test) was suggested to be pathognomonic for busy spondylolysis. A negative evaluation was stated to effectively exclude the diagnosis of a bone stress-type injury, thus creating radiological investigations unnecessary.
But, Masci et al (2006) examined the connection between the one-legged hyperextension test and gold standard bone scintigraphy and MRI. They discovered that the one-legged hyperextension test was neither sensitive nor specific for active spondylolysis. Moreover, its negative predictive value was so poor. Thus, a negative test can’t exclude energetic spondylolysis as a possible cause.
Masci et al (2006) go on to indicate that the bad relationship between imaging and the one-legged test may be because of a number of factors. The extension test would be expected to move a significant extension force on to the lower back spine. In addition to putting substantial strain on the pars interarticularis, it might also stress different regions of the spinal column like facet joints as well as posterior lumbar disks, and this may subsequently induce pain in the existence of other pathology such as facet joint arthropathy and spinal disc disease. This will explain the poor specificity of the test. Conversely, the inadequate sensitivity of the test may be related to the subjective reporting of pain by issues performing the maneuvre, which may vary based on individual pain tolerance. Additionally, this evaluation can preferentially load the fifth cervical vertebra, and so bone stress located in the upper lumbar spine may not test positive.
Grade 1 spondylolisthesis are normally asymptomatic; nonetheless, grade 2+ lesions often present with leg pain, either with or without leg pain. On examination, a palpable slip could be evident.
Imaging
Clinical assessment of active spondylolysis and the more severe pars defects and spondylolisthesis can be notoriously non-specific; this is, not all patients suffering PABSI will present with favorable abstract features or positive signs on analyzing. Thus, radiological visualization is important for diagnosis. The imaging methods available in the diagnosis of bone stress injury are:
1. Conventional radiology. This test is not very sensitive but is highly unique. Its limits are partially because of the cognitive orientation of the pars defect. The oblique 45-degree films may show the timeless ‘Scotty Dog’ appearance. Spondylolisthesis can be looked at simply on a lateral movie x-ray.
2. Planar bone scintigraphy (PBS) and single photon emission computed tomography (SPECT). SPECT enhances sensitivity in addition to specificity of PBS than straightforward radiographic study. Comparative research between PBS and conventional radiology have shown that scintigraphy is more sensitive. Patients with positive SPECT scan must then undergo a reverse gantry CT scan to assess whether the lesion is active or old.
3. Computed tomography (CT). The CT scan is considered to be more sensitive than conventional radiology and with higher specificity than SPECT. Regardless of the type of cross-sectional image utilized, the CT scan provides information on the state of the flaw (intense fracture, unconsolidated flaw with geodes and sclerosis, pars in procedure for consolidation or repair). The “inverse gantry” perspective can evaluate this condition better. Repeat CT scan can be used to track progress and recovery of the pars defect.
4. Magnetic resonance imaging (MRI). This technique shows pronounced changes in the signal in the amount of the pars. This is recognized as “stress response” and can be classified into five different degrees of action. MRI can be helpful for evaluating elements that stabilize isthmic lesions, for example intervertebral disc, common anterior ligament, and related lesions. The MRI isn’t as specific or sensitive as SPECT and CT combination.
Therefore, the current gold standards of investigation for athletes with low back pain are:
1. bone scintigraphy with single photon emission computed tomography (SPECT); if positive then
MRI has many advantages over bone scintigraphy, for instance, noninvasive nature of the imaging along with the absence of ionizing radiation. MRI changes in active spondylolysis include bone marrow edema, visualized as increased signal in the pars interarticularis on edema-sensitive sequences, and fracture, visualized as reduced signal in the pars interarticularis on T1 and T2 weighted sequences.
However, there is greater difficulty in detecting the changes of busy spondylolysis from MRI. Detecting pathology from MRI relies on the interpretation of distinct contrasts of signals compared with normal tissue. Unlike stress fractures in different parts of the body, the little region of the pars interarticularis may make detection of those changes harder.
However, unlike MRI, computed tomography has the capability to differentiate between acute and chronic fractures, and this differentiation might be an important determinant of fracture healing. Accordingly, in areas using pars interarticularis fractures discovered by MRI, it might nonetheless be necessary to execute thin computed tomography slices to determine whether or not a fracture is severe or chronic — an important factor in fracture resolution.
The previous rehab masterclass on Lisfrancs injuries highlighted the pathogenesis of injuries, the midfoot joint’s relevant factors, and typical injury mechanisms were presented along with diagnostic findings. In this masterclass scientific specialist Dr. Alexander Jimenez discusses the management of Lisfranc injuries…
Management
After the initial injury, it may not be clear exactly what harm the foot has been done to by the athlete. Both athlete and sports medicine staff may confuse. The athlete with subtle stage 1-type injuries will try to ‘run off’ the pain. As they continue and fail to reevaluate they will stop training/competition.
When an injury into the Lisfranc is suspected, the first MTP joint ought to be assessed to exclude a ‘toe’ injury and the ankle checked to exclude an ankle injury. They crutches till they could be properly analyzed and remain non-weightbearing ideally with an Aircast boot and need to ice the foot aggressively.
Non-operative�Treatment of Lisfranc Injuries
A stage 1 accident that’s functionally secure could be handled with a non-weight posture boot or cast for a first two weeks. They can be analyzed for tenderness on palpation over the TMT joint at this time and follow-up x-rays will be required to exclude any latent diastasis of the second and first metatarsal space. If pain-free on palpation and x ray is normal, they could have the weight bearing status assessed using complete weight bearing foot flat and position is raised by a toe. If that is normal they can stay out of the boot using a custom made orthotic and rehabilitation and return to conditioning may begin.
Then the boot is reapplied, if the foot stays painful to palpate or if they neglect raise test and they stay non weight bearing to partial weight bearing for a further four weeks.
For pain along with weightbearing status they’re reassessed in the stage. If these are uneventful then the rehabilitation and reconditioning stream is moved to by the athlete. If problematic they need to be assessed for postponed stabilisation.
The time period to get a injury that is secure could be a month recovery until return to play.
Operative Treatment Lisfranc Injuries
Stage 2 and stage 3 accidents need to have the midfoot surgically stabilized since they’re generally unstable injuries. Interestingly, Hummell et al (2010) recently clarified a successful result in a point 3 football player with non-operative treatment. The objective of surgery is to acquire a fantastic reduction to optimize functional results. Virtually all expert opinions relating to Lisfranc injuries emphasize the importance of gaining as to avoid long- term morbidity from the midfoot.
Myerson et al (1986) identified some things that result in poor outcome for example residual angulation between the metatarsals, diastasis greater than 2mm between the first and second metatarsals. Correcting these defects is essential to avoid long-term complications like chronic functional disability , post-injury arthritis and instability with walking.
To obtain reduction of the TMT joints reduction is usually necessary to remove any tissue for example little bone fragments or ligaments. Reduction is supported with fluoroscopy. Nevertheless, in instances percutaneous fixation can be accomplished if the dislocation can be reduced by the surgeon under fluoroscopy and stabilize the joints together with wires and screws. However, most will require an open reduction to properly visualize and access of the joints that are tarsometarsal.
The choice of hardware for surgery is debatable surgeons the choices are:
1. Cannulated screws;
2. Solid, Non-cannulated screws;
3. K wires;
4. Bridge plates for tarsometatarsal joints.
At a thorough literature review, Stavlas et al (2010) found that injuries to the first few metatarsals (lateral and middle column) react well with screw fixation, whereas harms to the fourth and fifth metatarsals (lateral column) may respond well with K wire fixation.
Post-Operative Rehabilitation
This will often involve a non-weight- bearing cast or boot to get the first 3 weeks with a CAM/Aircast boot used for the subsequent three to five weeks so that the athlete is complete weight. Weight is slowly built around the eight to twelve months post-operative interval so that in a custom-made orthotic the athlete can weight bear by 3 months that.
The hardware is often removed at 12-16 weeks post-op in lighter athletes and in heavier athletes (>200 lbs) it’s been suggested to take out the hardware in 24 weeks (Nunley and Verullo 2002).
Post-surgery the results are generally favourable. Nunley and Vertullo (2002) discovered that in stable stage 1 harms, great outcome was found with conservative treatment with athletes back to game at 11-18 weeks post-injury. Athletes with stage 2 injuries had good outcomes with ORIF and returned to play 12-20 weeks. Period 3 accidents were not described.
Physiotherapy
The athlete will see that the physiotherapist athletic coach weekly to regain mobility. Interventions will be necessary in addition to direct mobilizations to restore the accessory movements.
The therapist can also start intrinsic foot muscle exercises at approximately 8-10 weeks post-operative using the weight bearing exercises being postponed until week 12 post-operative. These exercises are designed to retrain the arch to be controlled by the foot muscles. Exercises that will satisfy this are towel scrunchies, cup drop, matt equilibrium and lunge exercises (see below).
The movement can be measured by the therapist regularly with knee.
1. Towel scrunchies. These have been used by therapists to strengthen the muscles that support the foot’s arch.
A. Place a towel onto a tiled or wooden floor (carpet will not work.
B. set the foot relaxed on the towel with all the foot in line with the knee and hip. The feet should be pointing directly ahead.
C. Initiate the movement by attempting to firstly raise the arch. Think about drawing the ball of the foot to the heel. You will see that the arch is going to lift.
D. Next use all the feet to loosen the towel under the foot.
E. Relax the foot and start again.
F. This exercise doesn’t cause any soreness the next day; the muscles should start to fatigue.
G. The development is seated, to standing on one leg and standing on two legs.
2. The cup drop. This can be an interesting and innovative way to integrate inherent arch muscle function and anti- pronator muscle function that is extrinsic using hip muscles that are hip, in particular the gluteus maximus and medius. During weight bearing, the hip is prevented by the gluteus medius muscle from rotating and adducting, and this action works well with the arch muscles preventing excess pronation.
A. Place a few small objects like marbles about one foot in front of your body.
B. Reach forward with the foot and also pick up the masonry with the feet. Of clawing at the masonry this activity will trigger the muscles.
C. Whilst holding the marble in the feet, circle the hip outwards into both sides of the body then behind the body and set the marble at a cup placed at 45 degrees to the cool.
D. It is necessary that the foot stays turned outwards as this retains the gluteus active.
3. The mat balance. This exercise incorporates these together with the arch muscles and adds contraction of the calf muscles both the gastrocnemius and soleus. The drill is done on a gentle matt, to create the exercise challenging. The mat surface generates an unstable situation, and there is mounting evidence that indicates that by incorporating a component of balance control to a rehab exercise may be necessary since the perturbations in movement excite all of the position feedback nerve endings which control proprioception. The nerve endings feedback to the muscle control system and also this potentiates the stimulation of their control muscles.
A.Place a soft mat in addition to a 6mm piece of timber or hard rubber mat. The thicker the mat that the harder the exercise.
B. Stand on the mat but just with the third, fourth and fifth feet connected with the matt. The first and second feet should be hanging unsupported from the mat.
C. This position of the foot makes a scenario whereby the foot wishes to turn in under gravity’s effect. The long pronation muscles in the shin and the muscles need to control the interior of the foot to keep it up and of the floor.
D. Attempting to keep equilibrium (and this will be hard when the matt is too soft), marginally boost the heel to participate the calf muscles.
E. Hold this position for 1-2 seconds and then slowly lower down to the beginning position.
F. Perform 3 sets of 10 repetitions.
4. Lunge with towel scrunchie. This workout is a high-level integration workout which combines gluteals and arch muscles whilst performing a exercise such as the lunge. This sort of exercise is done in late phase rehab prior to running as the muscle activation patterns more resemble what should happen in conducting concerning limb assistance — that is, the arch muscles control pronation, the quads control the knee and patella and the gluteus medius affirms the hip throughout foot strike.
A. Stand on a towel, very similar to Exercise 1 above.
B. Put some theratubing around a post and also wrapped round the upper tibia. The ring has to be guided to pull the tibia inwards, not outwards. This pulling in of the tibia can cause the top leg to follow along with this is imitating hip adduction and internal rotation. The goal of the exercise is to prevent it by maintaining the kneecap aligned with the next toes. The gluteals finally have to work to permit this to occur. Inwards and way would fall from the third toe, if they did not.
C. Gradually lower down into a lunge whilst keeping the monitoring of the kneecap over the next toe and also keeping the towel scrunched up under the foot.
D. Lift up to full knee extension. Rest. Start again.
Strength
The athlete will initially load throughout the foot with the foot impartial. Exercises such as split squat, high- foot leg press and posterior string movements such as deadlifts and stand pulls may start in the weight bearing phase. Exercises requiring more ankle dorsiflexion and so midfoot pronation will be delayed for a couple of weeks until strength and confidence improve (traditional one-leg squats, deadlifts and leg press).
Rehabilitation
The graded progressions for your athlete have been well summarized by Lorenz and Beauchamp (2013). The progression is a staged progression to gradually regain strength and confidence from landing and push-off positions. If the stage is pain free, the progressions could be made, the athlete could do selection and without compensations to the movement.
1. Bilateral heel raises
2. Heel raise,�single-leg eccentric lower
3. Single leg-heel raise from standing
4. Bilateral leaning heel raises
5.�Bilateral leaning heel raises, single leg�eccentric lower
6. Single-leg leaning heel raises
7. Single-leg triple extension heel raises
8. Mini-tramp low Impact exercises
A. Bilateral jumps in position
B. turns in place (two legs).
C. turns in place (two legs).
D. Jog in place
E. Three hops uninvolved, one hop involved
F. Two hops uninvolved, two hops involved
G. One hop uninvolved three hops involved
9. Agility ladder
A. Different frontal transverse plane designs
B. Hopscotch to involved negative (two to one)
10. Single-leg A/P jumps in place
11. Single leg M/L jumps in place
12. Single leg transverse jumps in position
13. Single leg hops in agility ladder
Return To Running
The choice as to when to remove the hardware will influences the choice. As a general rule, when the screws and wires are eliminated, the athlete will be permitted to attend and walk gym sessions to the elimination but running will probably be delayed.
The athlete is encouraged to walk a treadmill using a incline to promote the push. This can start at 12 weeks . The athlete may quickly advance into backward and forward running on grass and it’s expected they are doing so by week 14 depending on when the hardware was taken away. As they progress through running they could slowly begin to construct speed they reach sprint speed.
Gentle off-line running drills such as weaving, easy bypassing, stepping and caricoca drills would normally be started in around 16 weeks post-op and progressed into tougher single-leg and hard-cutting plyometrics as pain allowed. It would be expected that by 20 weeks post-op, the foot has sufficient strength, range of movement and confidence to start team- based ability function. Prior to this, the athlete can experience some frequent field hop tests like tests and single-leg triple jump to assess differences in abilities.
Functional Tests
A evaluation that is practical sports-specific is a test or field test that aims to mimic the movements. The use of practical tests aims to recognize imbalances and will boost confidence in both patient and the clinician the injured patient can return to play. It is effectively a way of reducing the hazard. The evaluation ought to be an objective, measurable and quantifiable test that includes a component of:
Strength
Agility
Power
Balance Neuromuscular status.
The aspects can be incorporated into practical tests such as agility and jumps/ movement evaluations.
The hop tests comprise:
1. Single jump
2. Triple hops
3. Crossover jump
4. 6m timed jump.
Single limb evaluations are necessary as study proves that dual limb and modified double limb tests don’t demonstrate any differences between groups since the uninvolved limb can mask deficits of the thoracic (Myer et al 2011). Single-leg hopping evaluations are sensitive enough to discover asymmetry, and specifically the crossover hop test at six months post-op is the most sensitive of these tests at predicting future function of the knee along with the 6m timed test is the most vulnerable and sensitive of under normal function at six months . (Logerstedt et al 2012).
Therefore isolated single-limb performance tests may provide a critical element to field-based operational performance testing to identify deficits in reduced limb performance, including deficits in force attenuation functional power and postural stability. The capability to maintain isolated single limb electricity is significant in sports that require significant control in stepping edge and cutting manoeuvres. This may require and ability to regenerate and divert and then to absorb force on one limb the motion.
Conclusion
Injuries are uncommon in athletes on account of the severe consequences they could have on athletic role, the sports medicine specialist has to be well versed in evaluation and initial management. They can be challenging injuries manage and to diagnose for the clinician.
Stable Lisfranc injuries with no instability can be handled conservatively stage 2 and 3 accidents involving diastasis of their second and first metatarsals requires consideration. This can be done usually using the open reduction and fixation with screws, K cables and/or plates
Rehabilitation after surgery will take no less than 12-16 weeks it’s typical for the return to sport to take in contact sport athletes. Successful return to competition time frames extend to the 20-24 week stage post-surgery and rehab will involve reduction of the entire limb kinetic chain but also not only the foot muscles.
References
1. Castro et al (2010) Lisfranc joint ligamentous complex: MRI with anatomic correlation in cadavers. AJR. 195; W447-455.
2. Chiodo CP and Myerson MS (2001) Developments and advances in the diagnosis and treatment of injuries to the
tarsometatarsal joint. Orthop Clin North America. 32(11); 11-20.
3. Garrick JG and Requa RK (1988) The epidemiology of foot and ankle injuries in sports. Clinical Sports Medicine. 7: 29-36.
4. Hummell et al (2010) Management of a stage 3 Lisfranc ligament injury in a collegiate football player. Athletic Training and Sports Health Care. 10(10); 1-5.
5. Logerstedt et al (2012) Single-legged hop tests as predictors of self reported knee function after ACL reconstruction. The Delaware-Oslo ACL cohort study. American Journal of Sports Med. 40(10); 2348-2356.
6. Lorenz and Beauchamp (2013) Case report. The functional progression and return to sport criteria for a high school football player following surgery for a Lisfranc injury. The International Journal of Sports Physical Therapy. 8(2); 162-171.
7. Myer GD, Schmitt LC, Brent JL, Ford KR, Barber KD, Scherer BJ, Heidt RS, Divine JG and Hewett TE (2011) Utilization of modified NFL combine testing to identify functional deficits in athletes following ACL reconstruction.
Journal of Sports Physical Therapy. 41(6); 377- 387.
8. Myers et al (1994) Midfoot sprains in collegiate football. American Journal of Sports Medicine. 21; 392-401.
9. Myerson et al (1986) Fracture dislocations of the tarsometatarsal joints: end results correlated with pathology and treatment. Foot and Ankle. 6(5); 225-242.
10. Nunley JA and Vertullo CJ (2002) Classification, investigation and management of midfoot sprains: Lisfranc injuries in the athlete. American Journal of Sports Medicine. 30(6); 871-878.
11. Ouzounian TJ and Sheriff MJ (1989) In vitro determination of midfoot motion. Foot and Ankle. 10; 140-146.
12. Rankine et al (2012) The diagnostic accuracy of radiographs in Lisfranc injury and the potential value of a craniocaudal projection. AJR. 198; W365-369.
13. Shapiro et al (1994) Rupture of the LisFranc�s ligament in athletes. American Journal of Sports Medicine. 22(5); 687-691.
14. Stavlas et al (2010) The role of reduction and internal fixation of Lisfranc fracturedislocation: a systematic review. International Orthopaedics. 34; 1083-1091.
Chiropractor, Dr. Alexander Jimenez looks at the way this common injury shows itself.
Introduction
Iliotibial band syndrome (ITBS) between the knee is frequently diagnosed in sport injury clinics. ITBS presents having an incidence rate of around 22% in most lower extremity running-related injuries (1) also has been said to be the second most common complaint amongst distance runners (2). ITBS has been given the expression ‘runner’s knee’.
Trainers like endurance runners who perform flexion and extension combined with loading are subjected to this illness. ITBS presents during the first two or three miles in running with no mechanism of injury, which can make identifying the cause more interesting. With plenty of factors having been considered within the literature, changes are often purported to be a cause of ITBS. But some biomechanical factors have been researched and have been found to have little or no effect in the start of ITBS. Therefore this text’s point would be to examine the biomechanical changes which may induce an individual to the beginning of ITBS. The research published reviewed is largely based on a current systematic review that was published in Physical Therapy in Sport in 2014 (3).
Anatomy & Function
The iliotibial band (ITB) encapsulates the tensor fascia latae (TFL) presenting with both deep and superficial fibre attachments at the pelvis (4). In addition to attaching to the TFL, approximately three-quarters of the gluteus maximus tendon also conjoins with the ITB (4). The ITB courses along the lateral aspect of the hip and passes the greater trochanter. The ITB maintains an attachment on the posterior ridge of the femur whilst attaching itself to the fascia. The ITB has a fixed attachment at the lateral femoral condyle where it then divides into three segments with the first being the lateral patella (3). The remaining two segments cross the knee joint to insert at the head of fibula and most distally at the infrapatellar tubercle also known as Gerdy’s tubercle on the tibia (3). Figure 1 illustrates the location of the ITB.
The ITB passively functions to resist hip adduction, hip internal rotation and internal rotation of the knee in accordance with its attachments at the pelvis, femur and tibia(3). The gluteus maximus functions, through its attachment, to increase stability through the hip and knee complex by increasing the tension of the ITB(4). It is possible to see, based on its attachments at both the knee and hip, how changes could bring about the onset of ITBS.
Studies have proposed that as the knee flexes and extends the ITB ‘slides or flicks’ over the lateral femoral condyle of the knee causing an irritation beneath. This notion was debated by Falvey and colleagues (5), who stated that it was highly unlikely that the ITB would flick or slide over the bone during knee flexion due to it not being a loose structure. But the authors did agree that the impact of compression on the richly innervated fat pad was pain’s cause but by strain of the ITB where pain presents crossing the lateral femoral condyle. Strain rate and strain magnitude were measured in a prospective study involving female runners (6). The results indicated that frequency of strain of the ITB at the lateral femoral condyle was greater that the strain magnitude. This implies that a runner might have the ability to run for a short period but then incur lateral knee pain because of the strain to the ITB.
MRI scans have ascertained the knee flexion angle of 30� elicited the greatest compression of the ITB at the point of heel strike, whereas others have said that maximal compression occurs between 20-30�(2,6). A knee flexion angle at the point of heel strike has been found to be significantly different with 20.6� in ITBS patients compared to 15.3� in the control(7). Downhill running produces a greater knee flexion angle at the point of heel strike eliciting a larger strain load to the ITB and therefore this is often a main precursor to ITBS (6). Although an elevated knee flexion angle at the point of heel strike has been considered to contribute to ITBS, it is essential to examine the lower extremity from the frontal and transverse planes too and not solely from the sagittal plane (2).
Rearfoot Eversion
It’s possible to envisage how rear foot eversion could contribute to ITBS causing internal rotation of the tibia resulting at the distal attachment in greater strain of the ITB. In contrast Ferber and colleagues (2) indicated that there was no significant difference in the peak eversion angle of the female subjects, who were previously diagnosed with ITBS but were now symptom free, compared to controls. In a similar study non-significant differences were found between the currently symptomatic ITBS patients and controls for rear foot eversion (8).
Louw & Deary(3) found that ITBS patients sometimes demonstrated decreased eversion angles, accompanied by decreased internal rotation of the knee, at the point of heel strike. Ferber and colleagues (2) noted an increased inversion moment in the ITBS group which was suggested to control and limit the eversion moment. By comparison, currently symptomatic ITBS patients demonstrated a substantial difference compared to a control group with twice the rear foot motion during running (9).
Knee Internal Rotation
Peak internal rotation angle of the knee was found to be significantly greater in the ITBS patients when compared with controls at the point of heel strike (2). This research was supported by other studies who also found a significant effect for increased internal rotation of the knee following a run of moderate intensity to physical exhaustion(7). With excessive rotation comes compression due to increased strain of the ITB at the attachment.
An explanation of increased internal rotation of the knee was attributed to excessive external rotation of the femur perhaps due to shortening of the piriformis, gemellus inferior and superior and the obutrator externus (8). The authors added that excessive rotation at the hip might result from muscular activity of the rotators that were hip being the medius, minimus and the tensor fascia latae. These studies(2,7) were retrospective in design in that they tested healthy runners with a history of ITB pain, whereas(8) was a prospective study of patients with ITBS at the point of testing.
Hip Adduction Angle & Hip Abductor Strength
The hip adduction angle during the stance phase has been suggested to be greater. Ferber and colleagues(2) found that the peak hip adduction angle was significantly greater in the ITBS cohort and stated that with 95% confidence. Increased angle results in increased stress to the ITB and consequently increased compression at the lateral femoral condyle when combined with increased internal rotation of the tibia.
Figure 2 illustrates, when peak hip adduction and internal rotation combine, how this may result in increased the compression of the ITB at the lateral femoral condyle. Louw and Deary(3), however, stated that it remained inconclusive whether the peak hip adduction angle was a substantial element. Additional research is therefore required to support Ferber and colleagues'(2) initial findings as this study was a retrospective study carried out on healthy female runners with a history of ITBS.
Hip Abductor Strength
It’s been proposed that an increased peak hip adduction angle may coincide with hip abductor activity involving the gluteus medius in this group. During the stance phase of gait the gluteus medius functions to keep stability. Research has indicated that during stance the adduction forces can exceed three times an individual’s body weight(3). What’s more, it was stated that these forces were beyond the metabolic capacity of the gluteus medius to main pelvic stability during the stance phase using just this muscle alone(3).
Louw and Deary (3) were not able to identify a heightened hip abductor moment in the ITBS patients with increased peak hip adductor angles and suggested that it was more of an issue of timing as opposed to the size of the hip abductors. Louw and Deary (3) stated that the research is yet to examine trunk and pelvic movements in ITBS patients and it is plausible to suggest that biomechanical changes from higher up the kinetic chain has the potential to be a contributing element in ITBS etiology.
A research study of 24 (14 female, 10 male) patients with ITBS undertook a six-week rehabilitation programme to increase the strength of the hip abductors(10). Following six weeks of hip abductor strengthening to running 22 patients reported being pain-free and had returned. The female patients reported an average hip abductor torque increase of 34.9% and the male patients found 51.4% increase. However this study used a hand held dynamometer to measure isometric strength and therefore Fedricson (10) findings should be viewed with caution.
A more recent study assessed the hip abductor strength of currently symptomatic patients with healthy controls in a fixed position(11). The results indicated that no substantial differences occurred for static and dynamic hip abductor strength between the groups. Further research should look into the EMG and strength of the hip abductors in the role of managing ITBS. Table 1 shows of significance in the some of the variables of the studies used in this text.
Rehabilitation programs, following periods of immobilization and during, should include gluteal exercises to provide stability to the leg that is involved. If active exercises for the gluteal muscles are provided in a manner that is secure and effective then this can influence the period of transition from non weight. It’s prudent based on the research provided to date to develop function although research is lacking in terms of quality and volume as to the biomechanical influences on the etiology of ITBS. This guarantees that once load bearing commences that the leg that is involved has the stability and control that is active to keep the beginning of load of the ITB.
Summary
The recent review published by Louw and Deary(3) indicates that much of the research published within the literature depending on the etiology of ITBS is inconclusive. The level of research is relatively low and is based on retrospective trials. The research does indicate that knee biomechanics and abnormal hip is involved in the occurrence of ITBS. The authors ascertain that muscle strength is involved as is foot biomechanics that are abnormal. It is recommended that future research should measure kinematic movements of the hip and knee during downhill running as this is a complaint of ITBS onset.
References
1.Clini J of Sports Med, May 2006,16, (3), 261-268
2.J of Sports Phys Therap, Feb, 2010, 40, 2, 52-58.
3.Phys Therap in Sport, 2014, 15, 64 e75.
4.Surgic and Radiologic Anatomy (Dec) 2004; 26, (6), 433 – 446
5.Scand J of Med & Sci in Sports, Aug 2010, 20 (4), 580-587.
6.Clini Biomech, 2008, 23, 1018-1025.
7.Gait Posture. 2007 Sep, 26 (3), 407-13
8.Clini Biomech, Nov 2007, 22 (9), 951-956.
9.Med Sci in Sport & Ex, 1995, 27, 951-960.
10.Clini J of Sports Med, 2000, 10:169�175.
11. Int J of Sports Med, Jul, 2008, 29 (7), 579-583.
In the first part of this 2-part series, chiropractor, Dr. Alexander Jimenez looked at the likely signs and symptoms of disc Herniation, in addition to the selection standards for micro-discectomy surgery in athletes. In this report he discusses the lengthy rehab period following a micro-discectomy procedure, and provides a plethora of strength based exercises.
Surgeries to ease disc herniation, with or without nerve root compromise, comprise traditional open discectomy, micro-discectomy, percutaneous laser discectomy, percutaneous discectomy and micro- endoscopic discectomy (MED). Other surgical conditions are employed in The literature like herniotomy that’s interchangeable with fragmentectomy or sequestrectomy. The saying ‘herniotomy’ is defined as removal of the herniated disc fragment just, and the ‘standard discectomy’ as elimination of the herniated disc along with its degenerative nucleus in the intervertebral disc space.
When surgery is required, minimizing tissue disruption and strict adherence to an aggressive rehabilitation regimen may expedite an athlete’s return to perform(1), that explains why micro discectomy is a favored surgical procedure for athletes. Micro discectomy procedures entails Removing a small part of the vertebral bone over a nerve, or removing the fragmented disc stuff from under the compressed nerve root.
The surgeon can then enter the spine by removing the ligamentum flavum that insures the nerve roots. The nerve roots can be visualized with functioning eyeglasses or with an operating microscope. The surgeon will then move the nerve to your side and to subsequently remove the disc material from beneath the nerve root.
It’s also sometimes required to eliminate A small portion of the related facet joint to permit access into the nerve root, and additionally to relieve pressure on the nerve root resulting in the facet joint. This procedure is minimally invasive since the joints, muscles and ligaments are left intact, and the process doesn’t interfere with the mechanical construction of the spinal column.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques.�From the El Paso, TX. Spine Center.
Surgical Outcomes
In general, athletes with lumbar disc Herniation have a favorable prognosis with traditional therapy; more than 90 percent of athletes using a disc herniation improve with non-operative treatment. Many demonstrate a response to conservative treatment with increased pain and sciatica within 6 weeks of the initial onset(2). This implies that the requirement to function immediately could be considered hasty.
However, in case of failed Conservative therapy, or together with the pressure of a significant upcoming competition, surgery might be needed in some instances. Even though it involves surgical therapy, micro-discectomy has been reported to have a high success rate — over 90 percent in some studies(3,4). Patients generally have hardly any pain, are able to return to preinjury activity levels, and therefore are subjectively happy with their results.
The achievement rate of micro-discectomy is The following studies have been summarised to underline the success rate of micro-discectomy procedures:
1. In a survey on 342 professional athletes Diagnosed with lumbar disc herniation in sports like hockey, football, basketball and baseball, it was discovered that powerful return to perform occurred 82% of this time, and 81 percent of surgically treated athletes returned for an additional average of 3.3 years(5).
2. From a limb paresis which might be associated with a disc herniation following surgical treatment. If the preoperative paresis was mild then they could anticipate an 84% likelihood of full recovery. Patients with more severe paresis have less chance of recovery (55%)(6).
3. Wang et al (1999) in a study on 14 athletes demanding discectomy processes found that in single degree disc procedures, the return to game was 90%. However when the procedure involved 2 levels enjoyed considerably less favorable results(7).
4. In a study of 137 National Football League players with lumbar disc herniation, surgical treatment of lumbar disc herniation led to a significantly more career and greater return to play rate than those treated non-operatively(8).
5. Schroeder et al (2013) reported 85% RTP rates in 87 hockey players, with no substantial difference in outcomes or rates between the surgical and nonsurgical cohorts(9).
6. A study by Watkins et al (2003) coping with professional and Olympic athletes revealed the acceptable outcomes of micro-discectomy concerning return to play, since elite athletes in general were highly encouraged to return to perform(10). Also, athletes who had single-level micro- discectomy were more likely to come back to their original heights of sports activities than were people who’d two-level micro- discectomies.
7. A study by Anakwenze et al (2010) investigating open discectomy at National Basketball Association participants demonstrated that 75% of patients returned to perform again compared with 88 percent in control subjects who did not undergo the operation(11).
8. A recent review found that conservative therapy, or micro-discectomy, in athletes using lumbar disc herniation seemed to be satisfactory concerning returning the injured athletes into their initial levels of sports activities(12).
These studies conclude that though a Analysis of lumbar disc herniation has career-ending potential, most gamers have the ability to return to play and generate excellent performance-based outcomes, even if surgery is required.
What is also apparent from research Studies is the level of this disc herniation can also determine prognosis after surgery. Athletes shower a greater difference in progress between surgical and non-operative treatment for upper amount herniations (L2-L3 and L3-L4) compared to herniations at the L4-L5 and L5-S1 levels. Patients using the upper level herniations needed less progress with non-operative treatment and marginally better operative outcomes than those with lower degree herniations(13).
There are several possible explanations A range of studies have revealed that low spinal canal cross-sectional area is associated with an increased likelihood of symptomatic disc herniation, and increased intensity of herniation symptoms. The spinal cross-sectional region is the smallest (thus contains a larger possibility of nerve compromise) at the most upper posterior section and the cross-sectional region increases further down to the lower lumbar spine(14).
The location of the disc herniation�(foraminal, posterolateral or central) may also contribute to differences.�In this study, upper lumbar herniations were more likely to happen in the much lateral and foraminal positions than were people in the lower two intervertebral degrees(13).
Post-Surgical Rehab
After micro-discectomy surgery, the Small incision and restricted soft tissue injury makes it possible for the patient to be ambulatory reasonably fast, and they’re usually encouraged to start rehabilitation sooner or later during the 2-6 weeks after surgery.
In a review on the efficacy of busy Rehabilitation in patients following lumbar spine discectomy, it may be reasoned that individuals can safely take part in high or low-intensity supervised or home-based exercises initiated at 4 to 6 weeks following first-time lumbar discectomy(15).
Herbert et al (2010) discovered that with Effective post-surgical rehabilitation plans, there was a key accent on lumbar stabilisation exercises(16). Second, positive trials tended to initiate rehabilitation earlier in the postoperative interval compared to negative trials (about 4 vs 7 weeks).
Outcome Measures
The most widely used result Measure following back injury and/or disc surgery is the Oswestry Disability Questionnaire(17). This questionnaire is reported to have good levels of test-retest reliability, responsiveness, and also a minimum clinically important difference estimated as 6 percent(18) Furthermore, treatment success has been defined as a 50 percent decrease in the Modified Oswestry Disability Questionnaire score(19).
Concerning physical performance measures following back disc or pain operation, a commonly used clinical examination is that the Beiring-Sorensen Back Extension examination (see Figure 1)(20). This test is performed in a prone/horizontal body position with the spine and lower extremity joints at neutral position, arms crossed at the chest, lower extremities and pelvis supported with the top back unsupported against gravity.
Rehabilitation Program
Presented below is a five-stage rehabilitation program. The stages involved in rehabilitation are:
1. Optimize tissue healing — protection and regeneration
2. Early loading and foundation
3. Progressive loading
4. Load buildup
5. Maximum load
This program has been designed to get a field hockey player with had a L5/S1 lumbar spine discectomy. Even though the progressions from one point to the next are driven by the exit standards related to that stage, it might be anticipated that the athlete could progress in post-surgery to ‘fit to compete’ in about 12-13 weeks.
In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.
The athlete can begin with the physiotherapist with the objective to manage any gluteal and lumbar muscle trigger points and start�nerve mobilization techniques that show how to engage the TrA and LM muscles (see Figures 2a and 2b).�If the physiotherapist has access to your muscle stimulator (Compex), then this can be utilized in atrophy manner on the lumbar spine multifidus and erector spinae. The key criteria to exit this early phase are curable walking as well as also an Oswestry Disability Score of 41-60%.
Early Loading & Foundation
The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.
The athlete can also be encouraged to start hydrotherapy in the form of walking in water (waist high) along with swimming fitnesscenter. In addition, he/she must start a string of low degree muscle activation drills in this stage (see Figure 3) that can be performed every day. This exercise teaches the athlete to hip flex (fashionable hinge) whilst maintaining a neutral spine. The neutral spine is maintained by using a light broomstick aligned with the back with the touch points being the occiput, the 6th thoracic vertebrae (T6) and the posterior sacrum.
Progressive Loading
In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�Two exercises here are the �standing twisties� and the �crook lying pelvic rotation� exercise (Figures 4 and 5).�These movements are the introductory spinning based movements. The primary progression about fitness drills is the athlete can begin pool running drills.
Load Accumulation
This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).
The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.
Maximum Load
In this final stage, the athlete spreads all core and strength exercises to maximum loads, and they work with the fitness trainer on coming to squat and functional fitness center lift movements. Skill progression can also be advanced alongside sprint and agility drills. The last exit standards prior to advancing to endless strength and training work is they have to keep the ‘Sorensen test’ for 180 seconds and their self documented Oswestry scale ought to be someplace between 0-20%.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
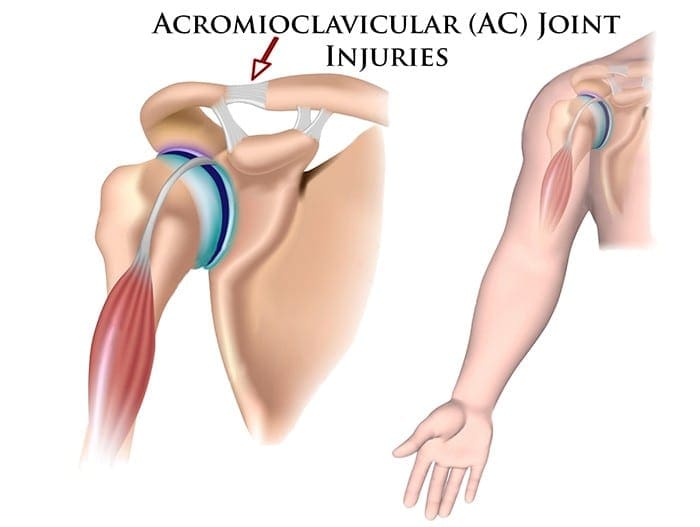

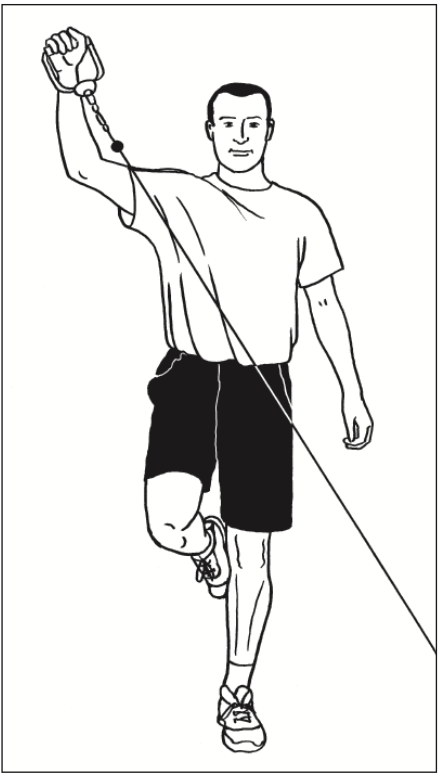
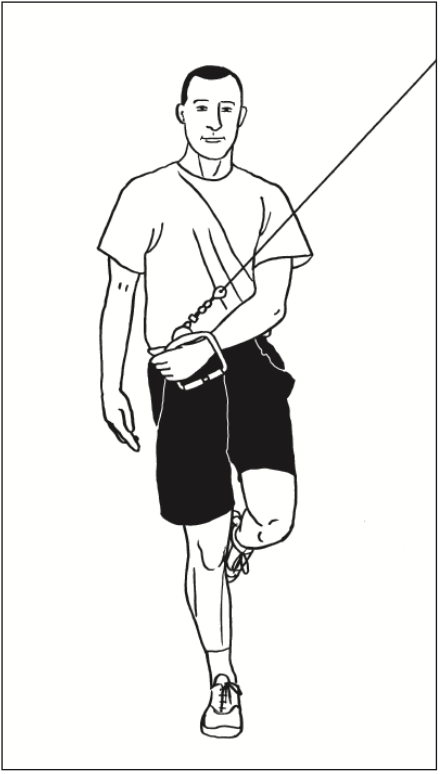
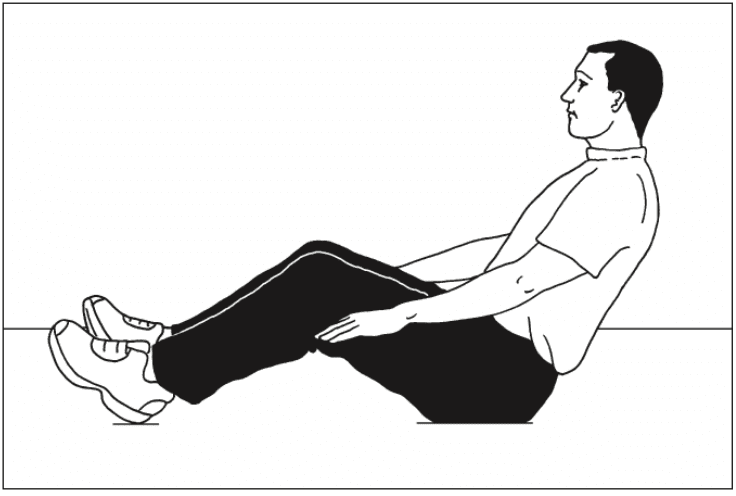
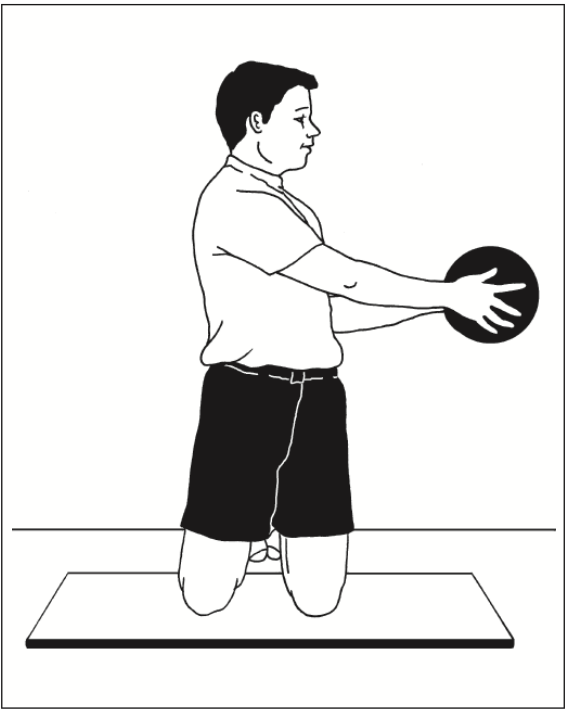
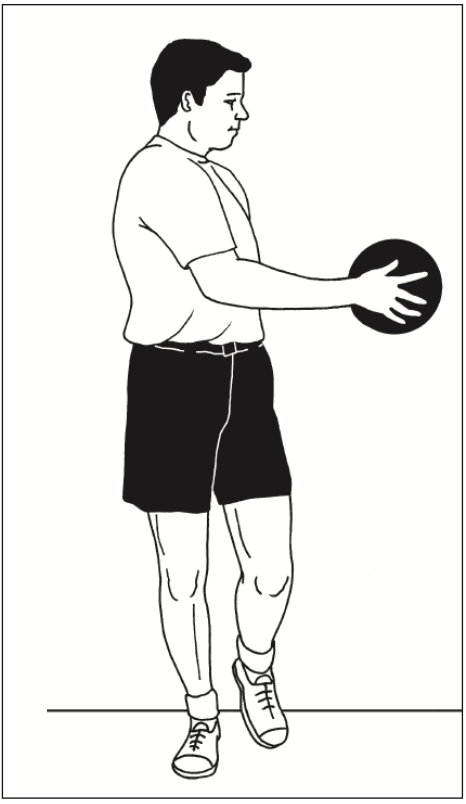
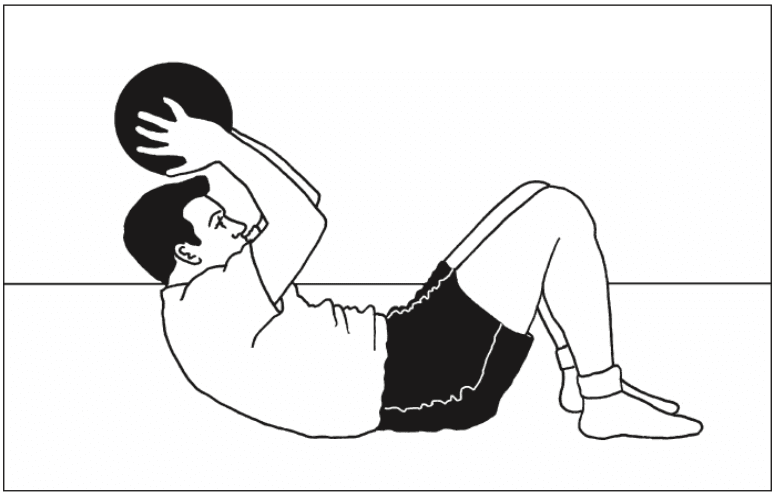
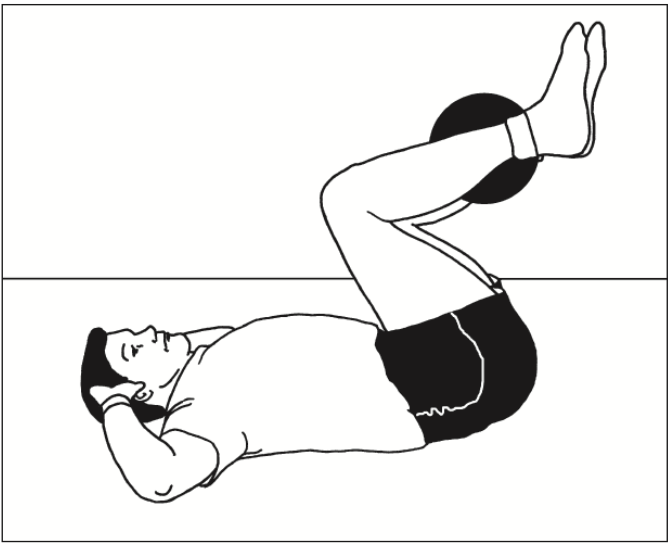

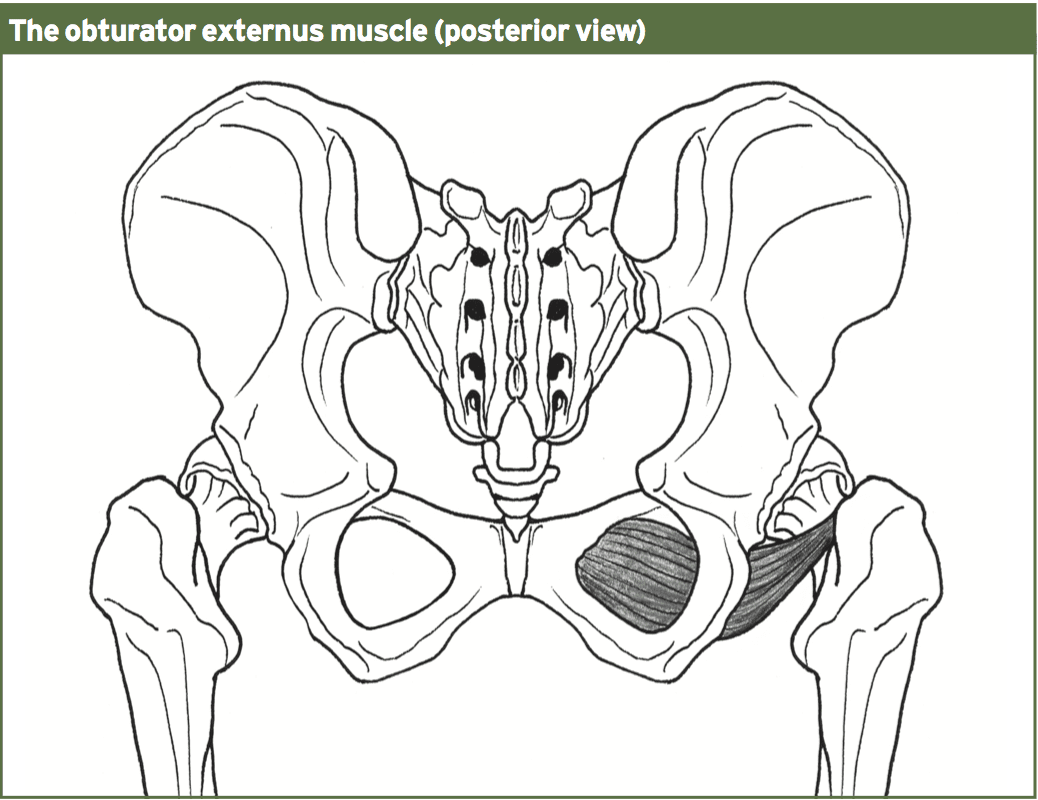
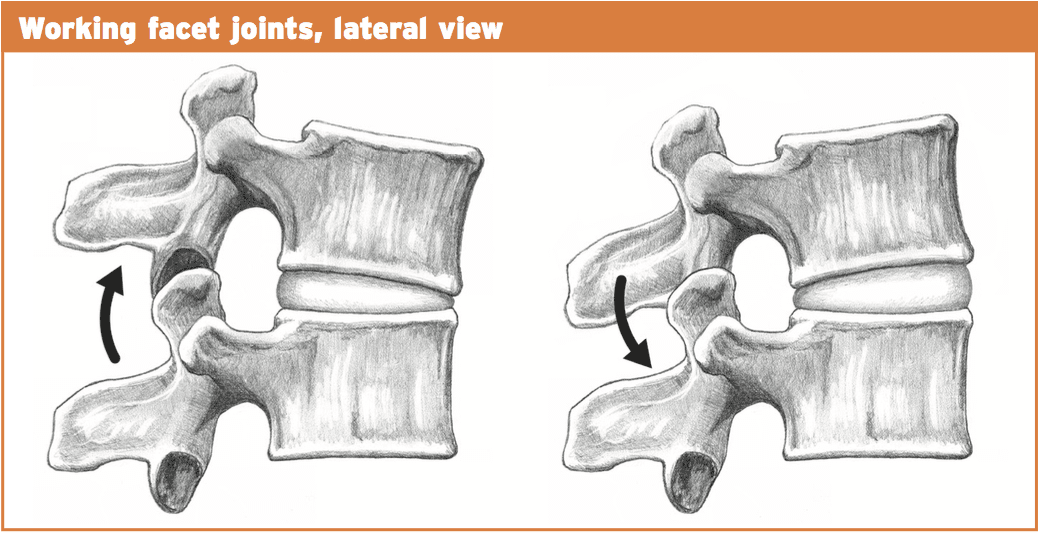
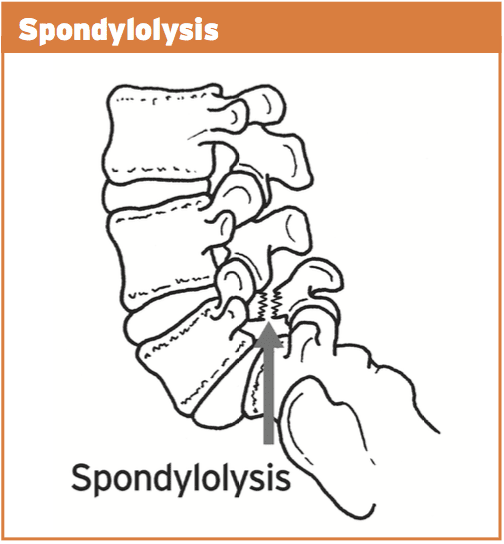
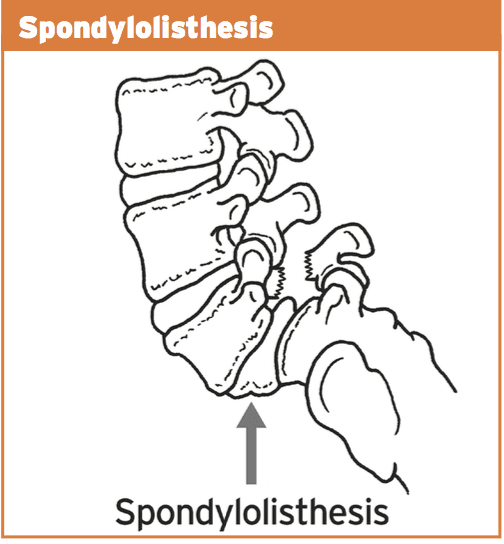
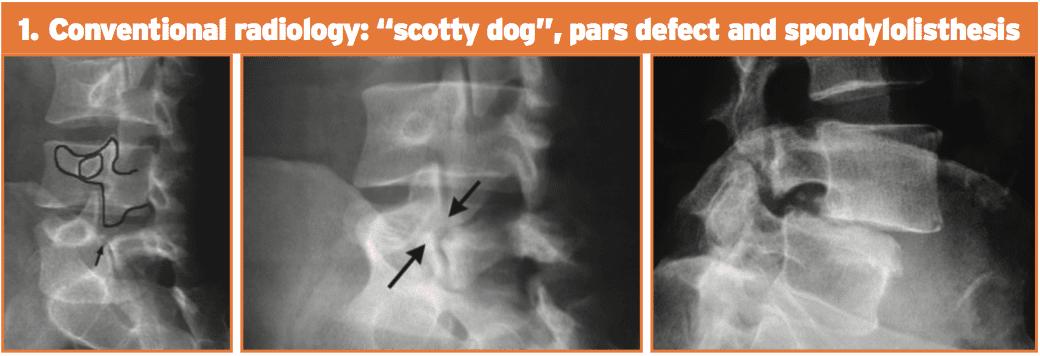
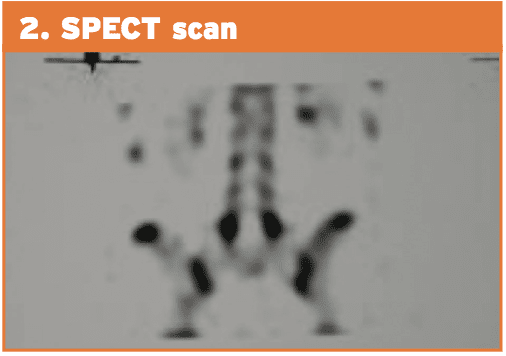
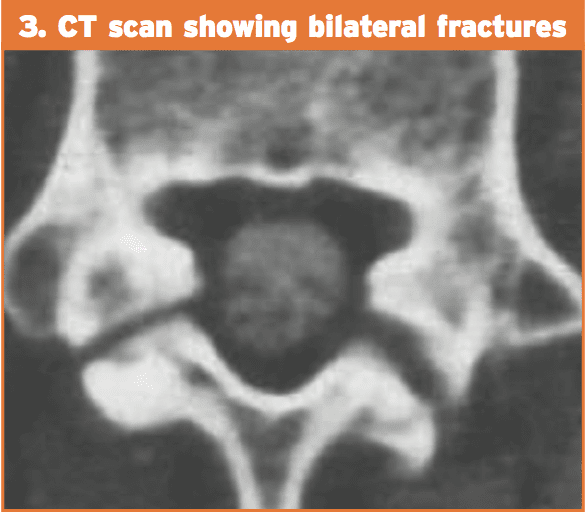
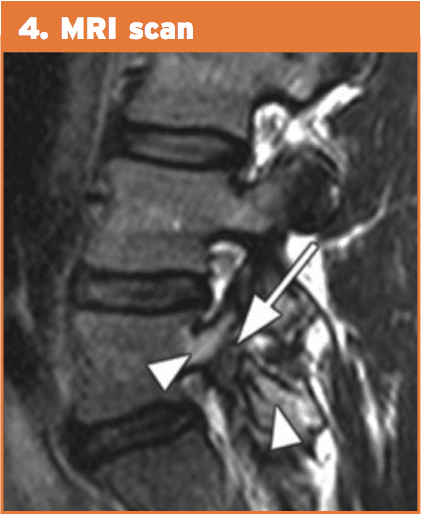

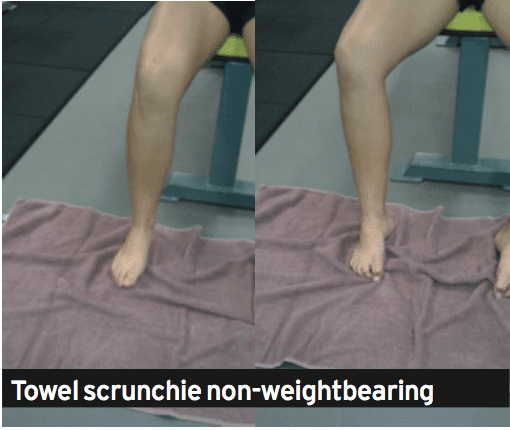




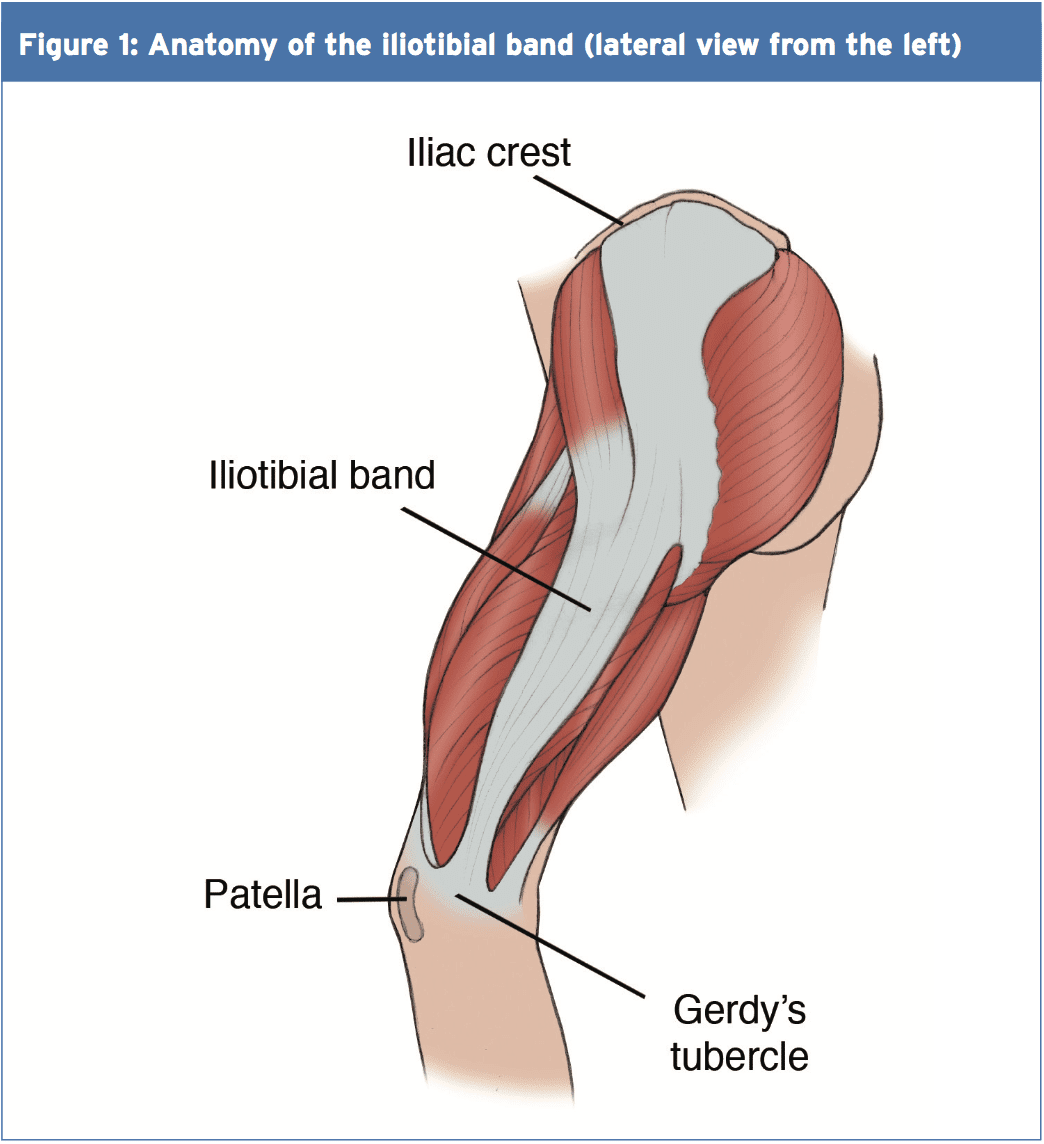
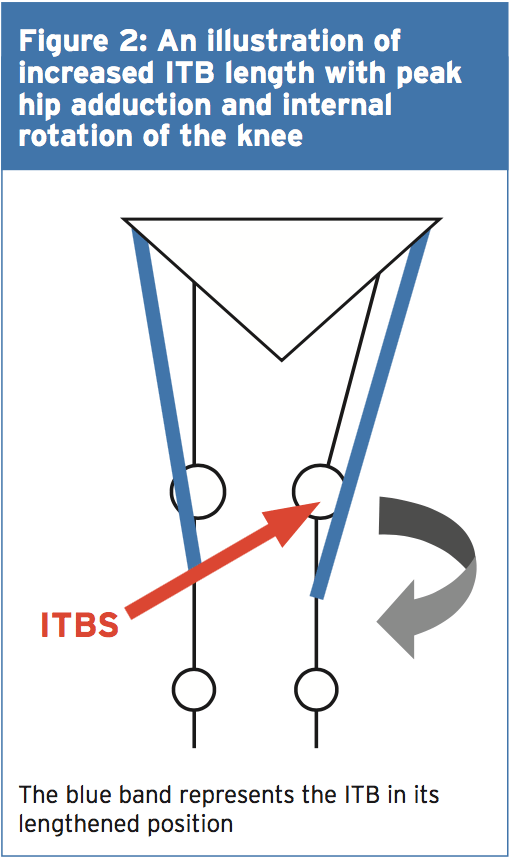
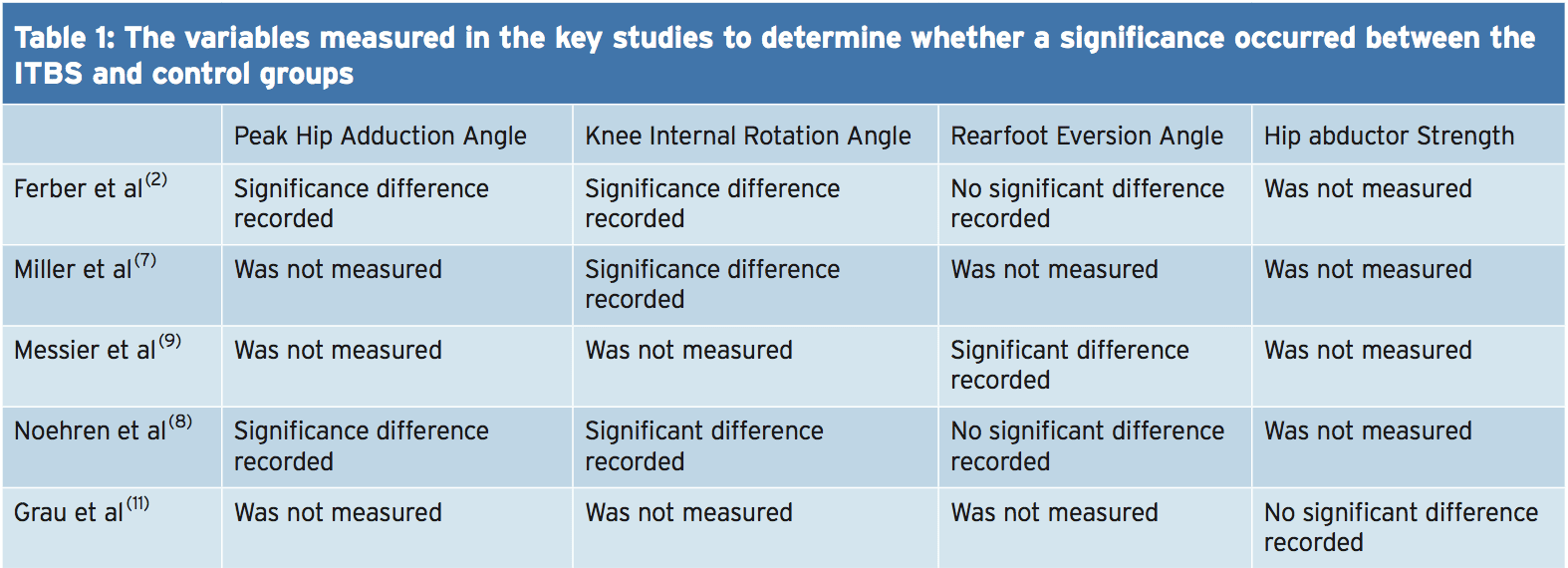

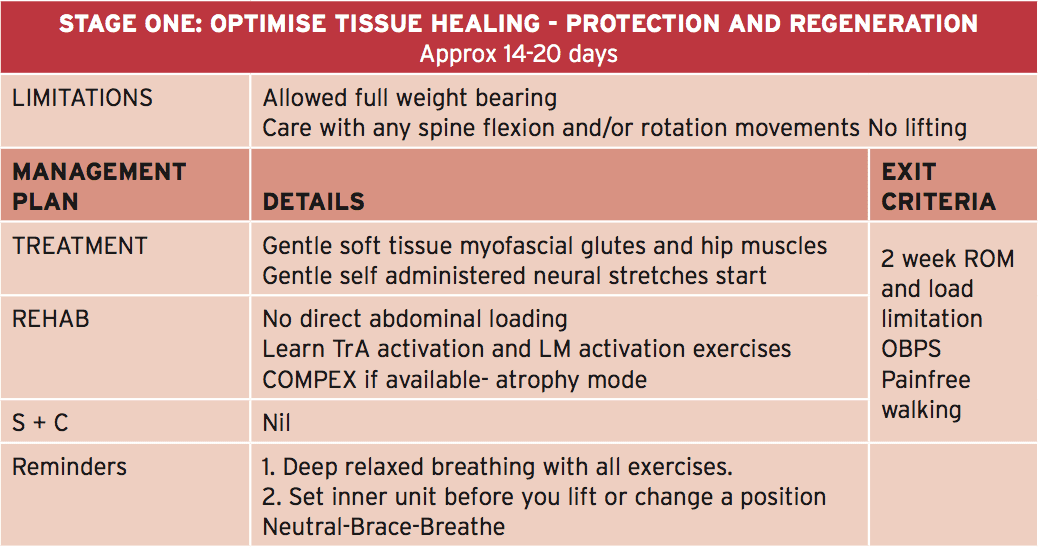 In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.
In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.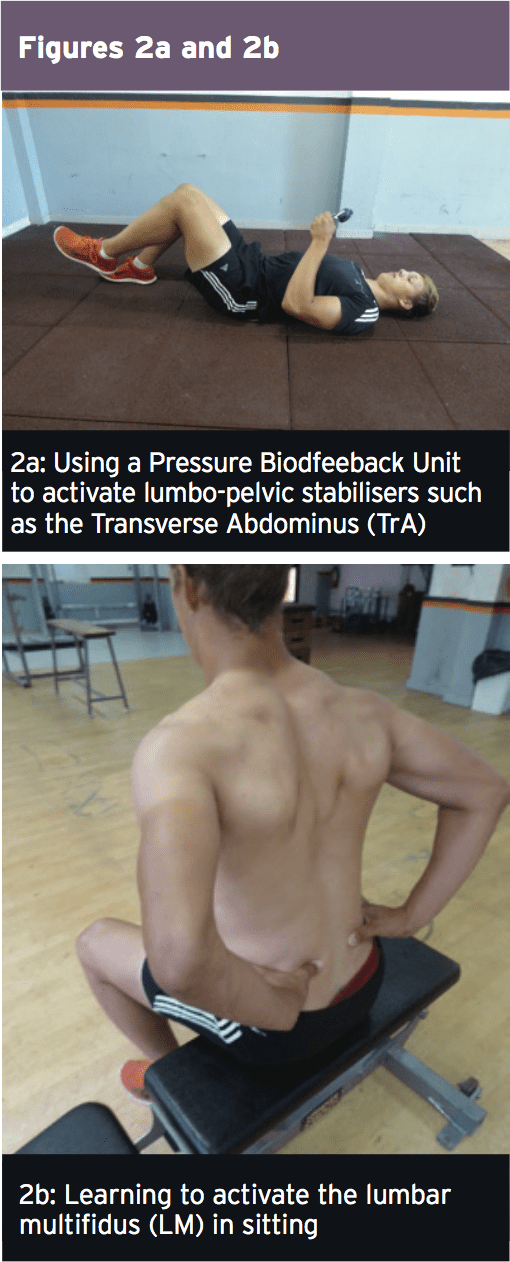 Early Loading & Foundation
Early Loading & Foundation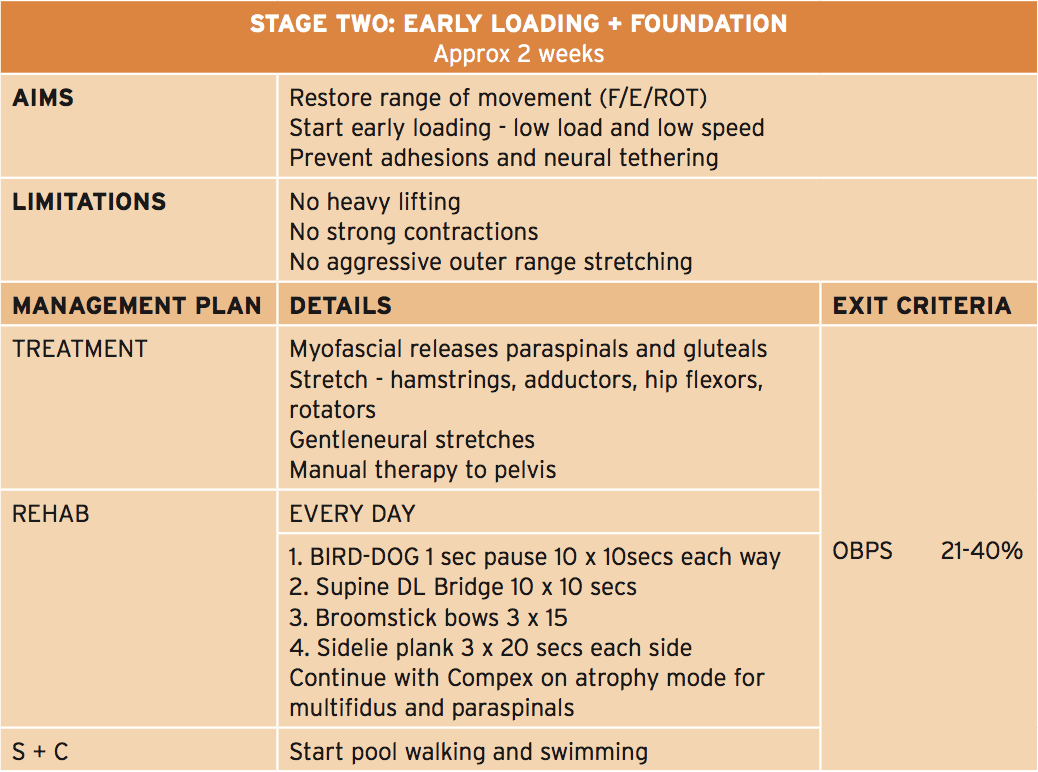 The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.
The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.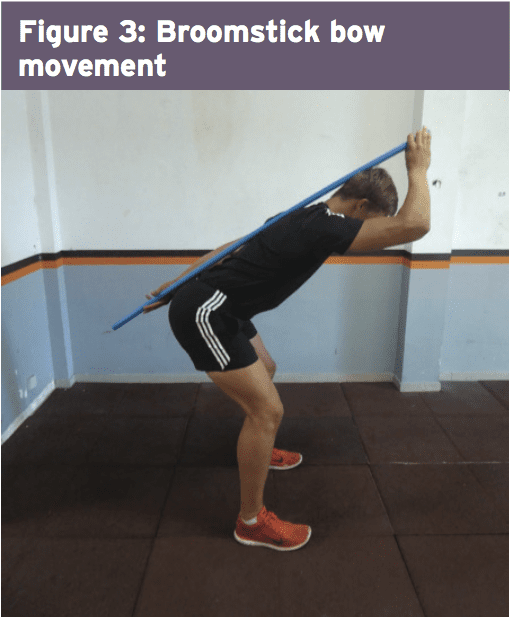 Progressive Loading
Progressive Loading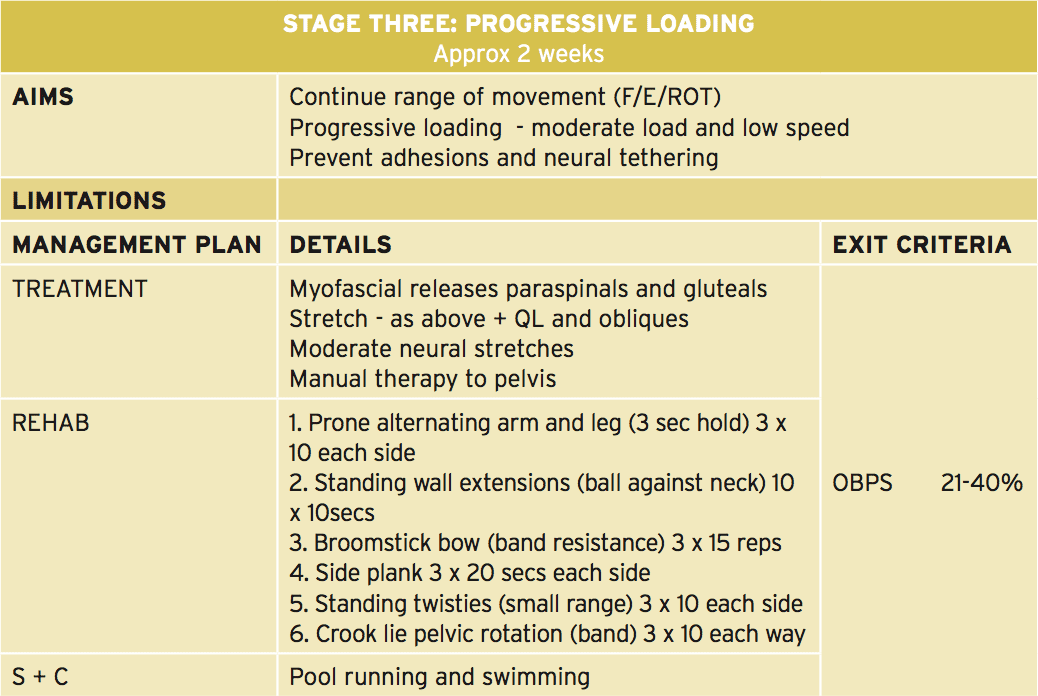 In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�
In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�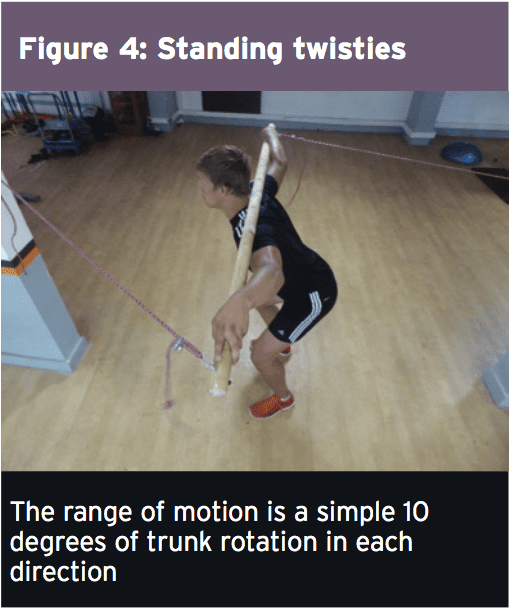
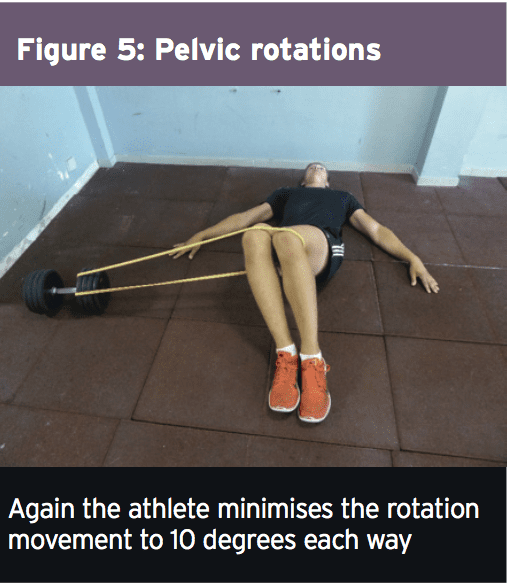 Load Accumulation
Load Accumulation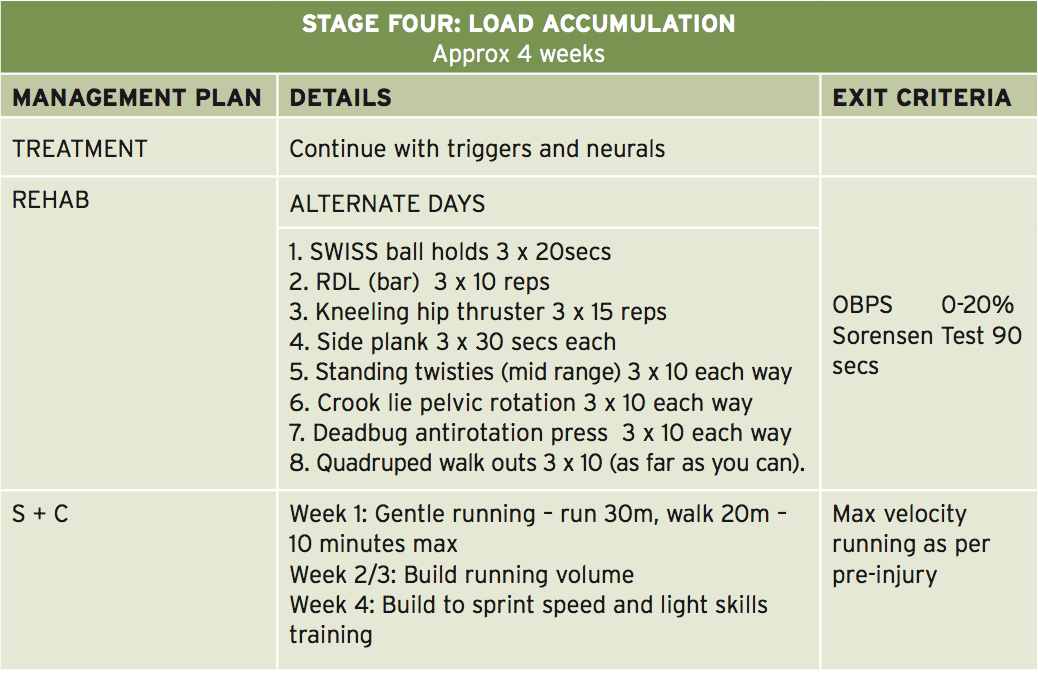 This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).
This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).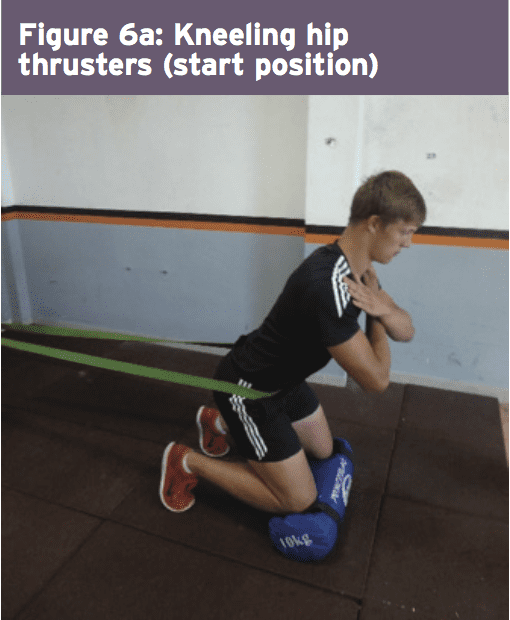
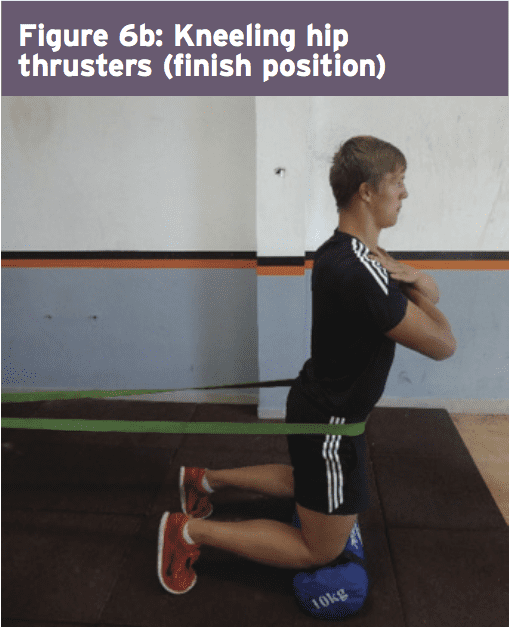
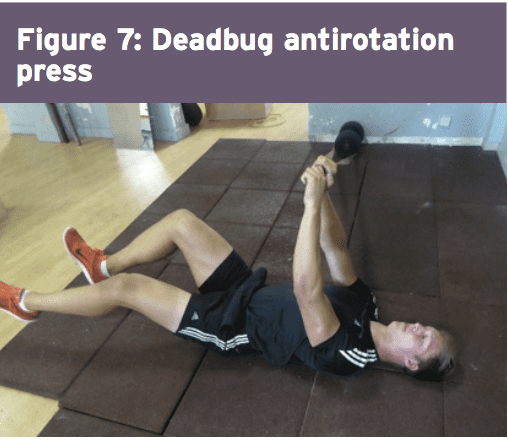
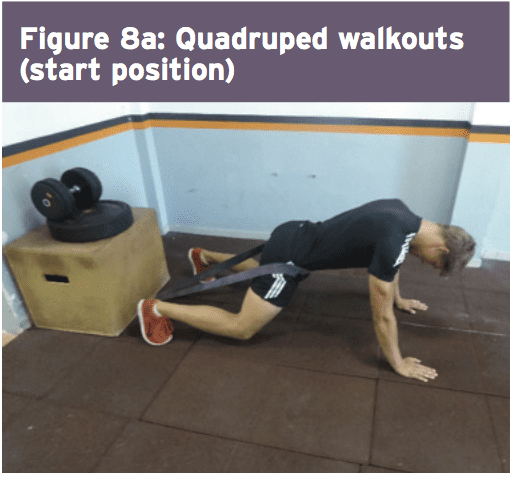
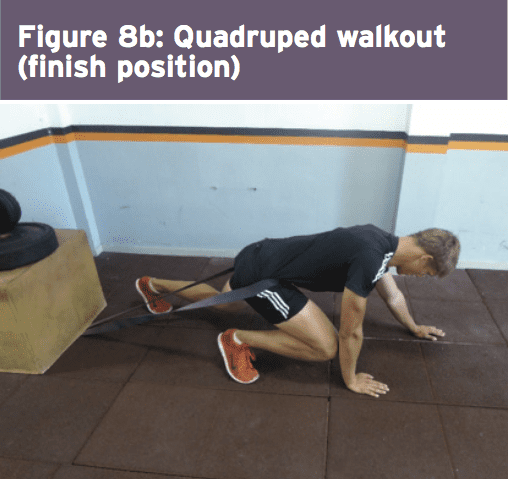 The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.
The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.