Introduction To The Cerebellum | El Paso, TX. | Part II
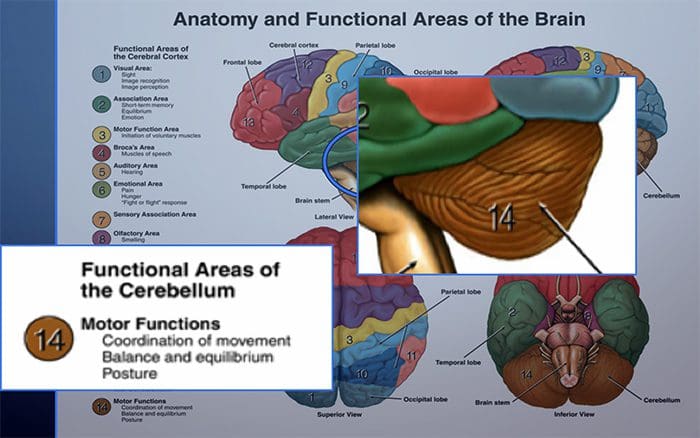
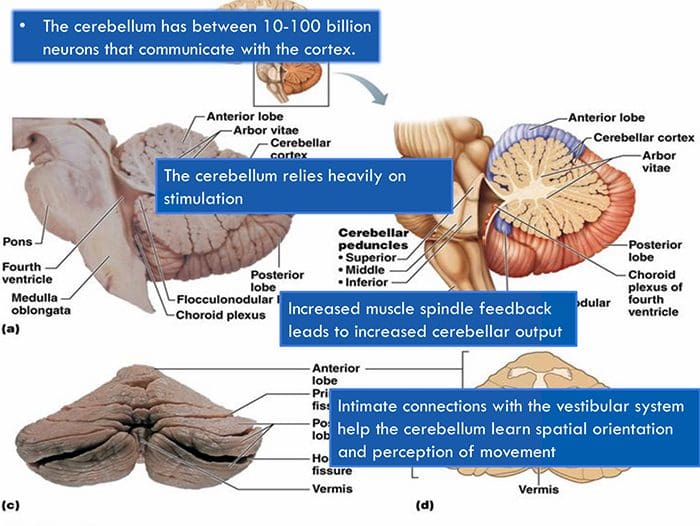
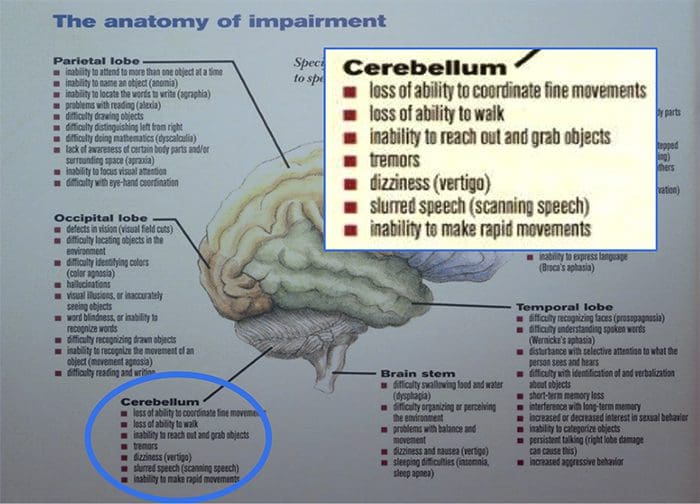
El Paso, TX. Chiropractor, Dr. Alexander Jimenez continues with the cerebellum overview. The cerebellum is one of the most identifiable parts of the brain based on its unique shape and location. It is an extremely important part of the brain. It is responsible for being able to perform everyday voluntary tasks likes walking and writing. And it’s essential for being able to keep balance and remain upright. People who have suffered from a damaged cerebellum struggle with balance and maintaining proper muscle coordination.
EVERYTHING PERIPHERAL HAS A CENTRAL CONSEQUENCE!
CASE STUDY
Cerebellar Ataxia
54-YEAR-OLD FEMALE PRESENTED TO OUR CLINIC FOR FEELINGS OF �UNSTEADINESS�

- Patient woke up one morning over one year ago with vertigo.
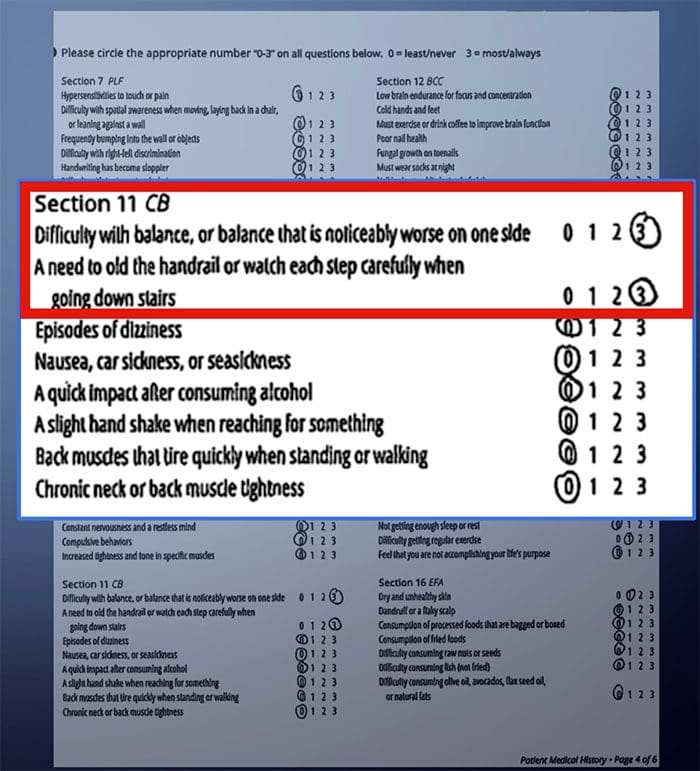
- Patient has difficulty with balance and walking. She sometimes resorts to using a cane. Extreme difficulty walking downstairs
- Patient has been proactive in her weight loss, however, this has served as a speed bump in her plan of getting back to health.
- She has not been able to exercise like she had in the past.
- Patient has been to several vestibular rehabilitation clinics to no avail.
PHYSICAL EXAMINATION HIGHLIGHTS
 Cranial nerves I-XII WNL
Cranial nerves I-XII WNL- Wide-based gait
- Right cerebellar findings
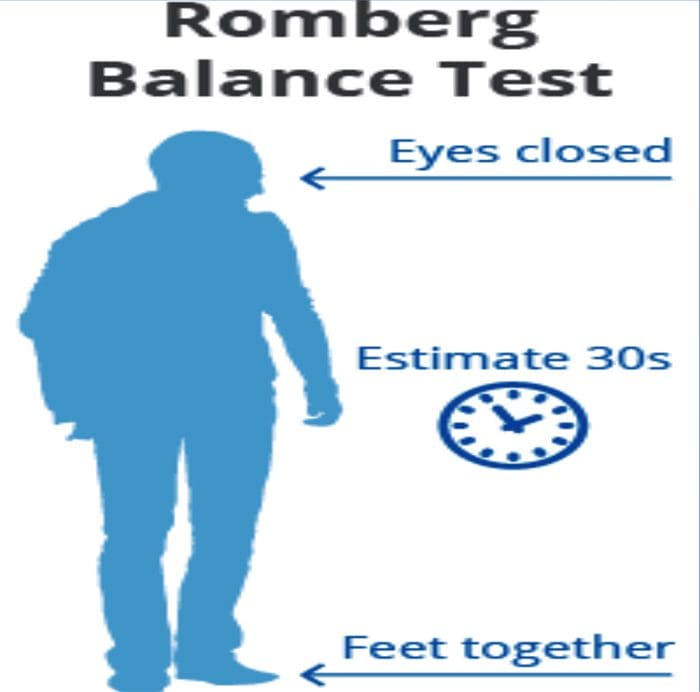
- Provocative Romberg testing produced significant sway in the right posterior and left anterior canal position.
THERAPEUTIC INTERVENTIONS
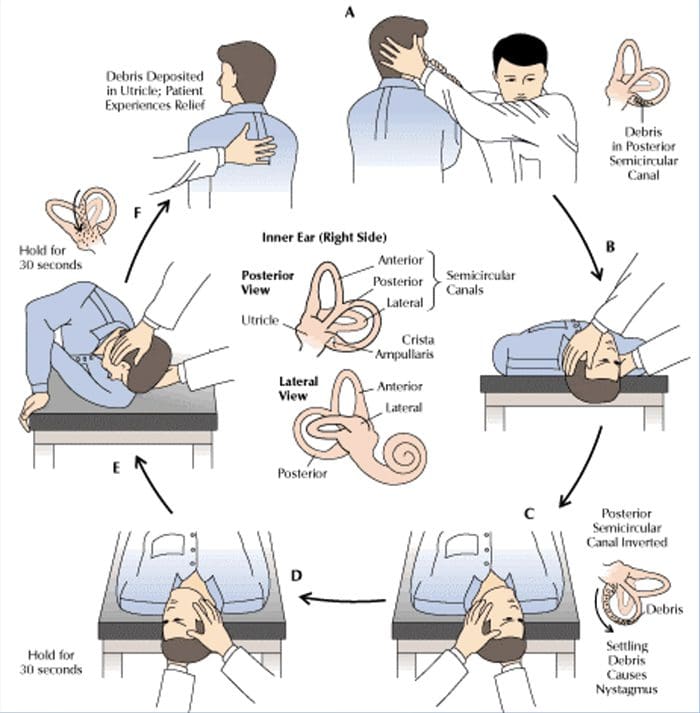 Right Posterior Canal Repositioning Maneuver.
Right Posterior Canal Repositioning Maneuver.- Right Cerebellar Novel Exercises.
- Chiropractic Adjustments
AFTER 1ST DAY
 Marked improvement in balance.
Marked improvement in balance.- Comfortable walking and standing with more narrow- based gait.
- Ability to walk down stairs without holding handrail.
CASE STUDY
Meet Aaron & McKayla
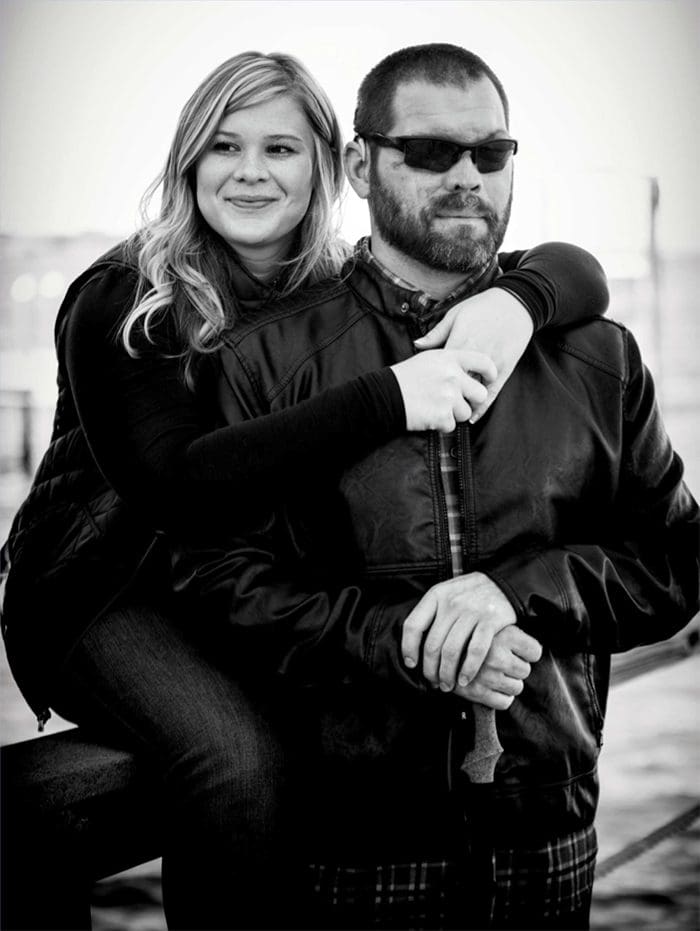
**Permission given to use names, images and whatever else needed to spread the word
A 39-year-old retired Explosives Ordinance Disposal Technician who in 2011…
And in 2015…

WHAT CAN FUNCTIONAL NEUROLOGY DO FOR AARON?
HOW CAN WE HELP HIS BALANCE?
IF YOU DON�T USE IT….
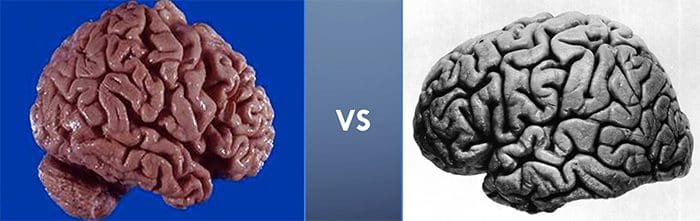
 WHAT DO YOU SEE?
WHAT DO YOU SEE?
 WHAT DO YOU SEE?
WHAT DO YOU SEE?
WHAT DO YOU SEE?

WHAT DO YOU SEE?
WHAT DOES IT MEAN?
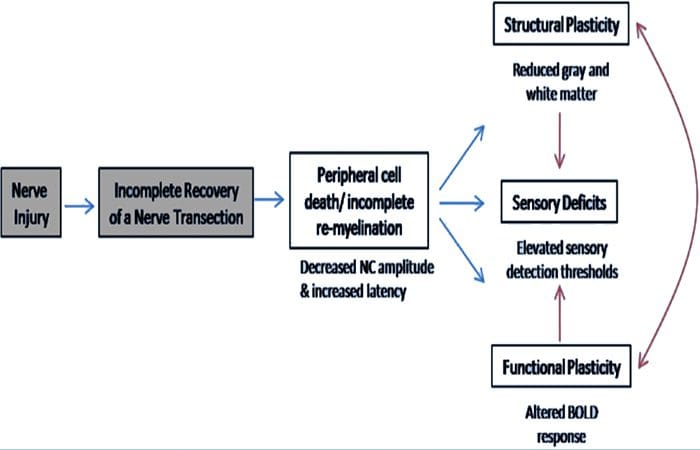
 AFFERENTATION WITH METABOLIC CONSIDERATIONS
AFFERENTATION WITH METABOLIC CONSIDERATIONS
A-BETA – MECHANORECEPTORS
- Merkel�s disc � slow adapting to pressure and texture. Sharpest resolution for spatial patterning. �steady light pressure�
- Meissner�s Corupuscle � superfiicial motion detection. Two point discretion.
- Ruffini�s Corpuscle � located in dermis. Steady skin stretch and joint pressure.
- Pacinian Corpuscle � rapid adapter, Associated with vibration.
GOLGI TENDON ORGAN IB FIBERS
- Responds to muscle tension changes.
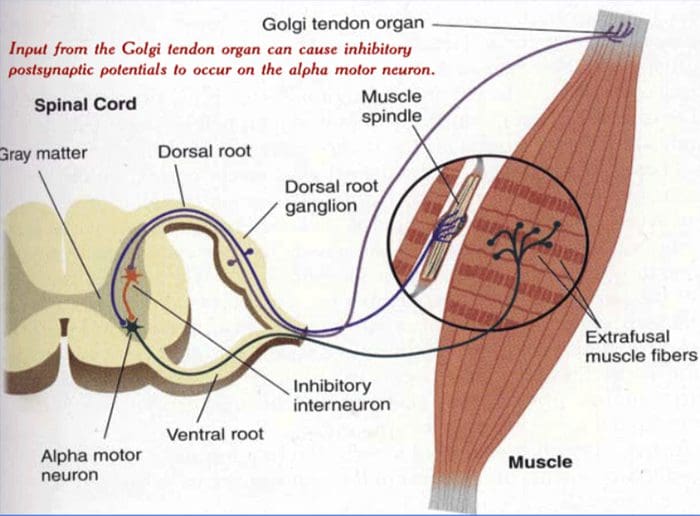
1A IIA SOMATOSENSORY
- Muscle spindle fiber is the largest fiber in the human body.
- Respond to the rate of change in muscle length, as well to change in velocity, rapidly adapting.
- This will require the most demands on metabolic capacity.
BACK TO THE CASE
 In 2011, Aaron had lost both of his eyes in an IED explosion.
In 2011, Aaron had lost both of his eyes in an IED explosion.- Due to the blast, Aaron also lost his sense of smell and taste.
- After several months of rehab, Aaron learned how to �be really good at being blind.�
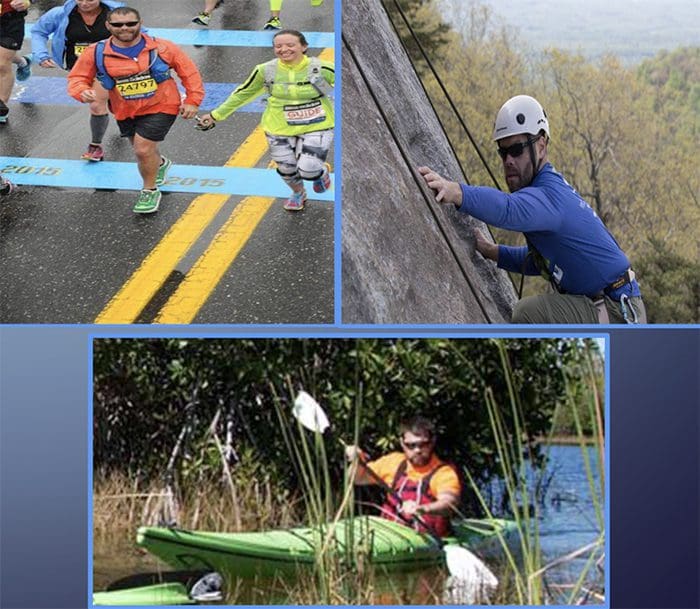
- Although he could not see, balance was no major issue. �I was climbing mountains, running marathons, kayaking…you name it.�
- In 2015, a few months after running the Boston Marathon, Aaron was on the phone with Mckayla.
- �He said he was not feeling well and was going to go lie down. I was concerned but did not think much of it.�
- After a day and a half of waiting for his call, McKayla found out Aaron contracted meningitis and was intubated in the ICU.

-
Finding out Aaron is completely deaf after meningitis…

-
The meningitis obliterated his hearing and left him completely deaf for 5 months.
-
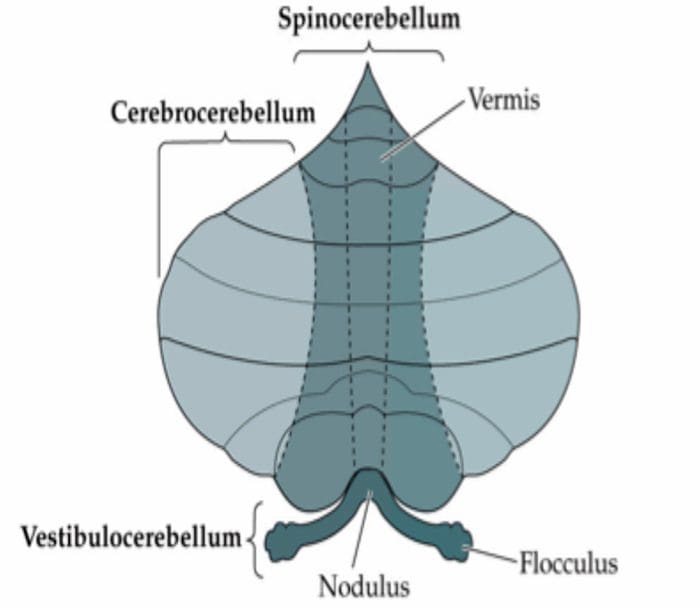
Not only that, the meningitis wreaked havoc on Aaron�s balance centers (his vestibulocerebellum) and he suffered from severe vertigo and difficulty standing and walking.
 After recovering from meningitis:
After recovering from meningitis:
-
�You can see how he’s walking on the treadmill in the very beginning. It took so much out of him to be able to do that.� � Mckayla
-
Remember �metabolic capacity?�

-
Aaron was actually able to get himself back into running shape and ran one of his best times in Ohio, but not without struggle.
-
�Every little change in pace and every little movement was a huge calibration for me and it took a lot out of me.�
-
�I still have a lot of work to do…�

 CHALLENGE ACCEPTED
CHALLENGE ACCEPTED
-
Sooooo….back to the basics!

-
We utilized different surfaces to challenge his balance system (foam pads, wobble boards, etc….
-
We also had him do most of his therapies barefoot to increase afferentation to the somatosensory cortex
 Updates from McKayla:
Updates from McKayla:
-
�Pace is a 7:30 and he’s doing 6 miles. Completed core work too.�

-
Typically in the OVARD we would spin Aaron in specific directions and he would tell us which direction he was spinning in.
-
At first this was very difficult and he could not perceive the movement, however it was not long until he was sensing each direction of his spin.
-
We let him have a little fun in this particular video….

-
I asked Aaron and McKayla how they felt therapy was going.
-
They responded �great, but we won�t really know until he goes for a run outside…�
-
So we went on a seven mile run at an 8 minute pace.
-
Here we are working on turns.

-
Cured!
-
Aaron is back home in Florida continuing his training for Boston in two weeks.
-
He is continuing at-home exercises and vestibular rehab with specialists
-
He and I are running a half marathon together in the not-so-distant future
 SOME SIMPLE CEREBELLAR THERAPIES
SOME SIMPLE CEREBELLAR THERAPIES
GENERAL CEREBELLAR EXERCISES
-
Spinning in desk chair will stimulate ipsilateral cerebellum
-
Passive muscle stretch will stimulate ipsilateral cerebellum
-
Squeezing tennis ball will stimulate ipsilateral cerebellum
-
Passive or active non-linear complex movements will stimulate ipsilateral cerebellum
-
Finger to nose pointing will stimulate ipsilateral cerebellum
Vermal & Paravermal Exercises
-
Passive and active gaze stabilization exercises with central fixation
-
Wobble board/unsteady surface exercises
-
Balance beam exercises and tandem walking
-
Bouncing a ball against the ground or throwing it against the wall
-
Core exercises such as planks, sit-ups and yoga
-
Learning how to balance on a bicycle
-
Supine cross crawl activity
Lateral Cerebellum Exercises
-
Cognitive processes
-
Learning a musical instrument
-
Tracing a maze
-
Playing �catch�
-
Tapping fingers/hand or toes/feet to the beat of a metronome
-
Trying to write with eyes closed
-
Strategic board games
THE LANGUAGE OF THE BRAIN IS REPETITION!
By RYAN CEDERMARK, RN BSN MSN DC DACNB
 Responsibilities:
Responsibilities:


 WHAT CAN YOU DO?
WHAT CAN YOU DO? Have the patient perform balance exercises:
Have the patient perform balance exercises:


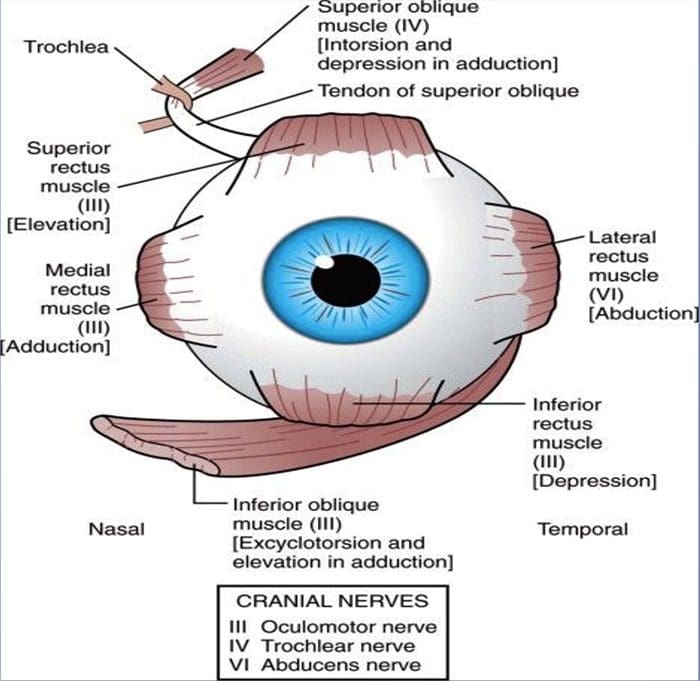
 EYE MOVEMENT REVIEW
EYE MOVEMENT REVIEW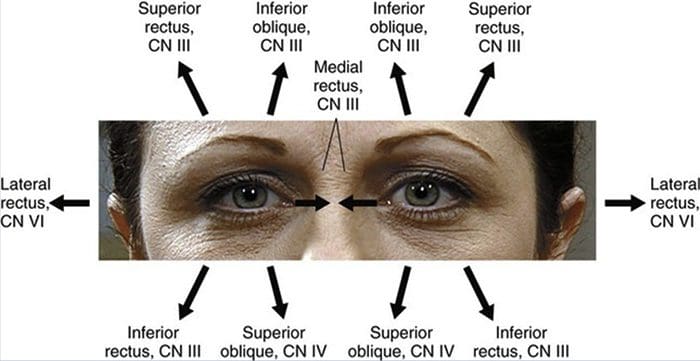
 WHAT CAN YOU DO?
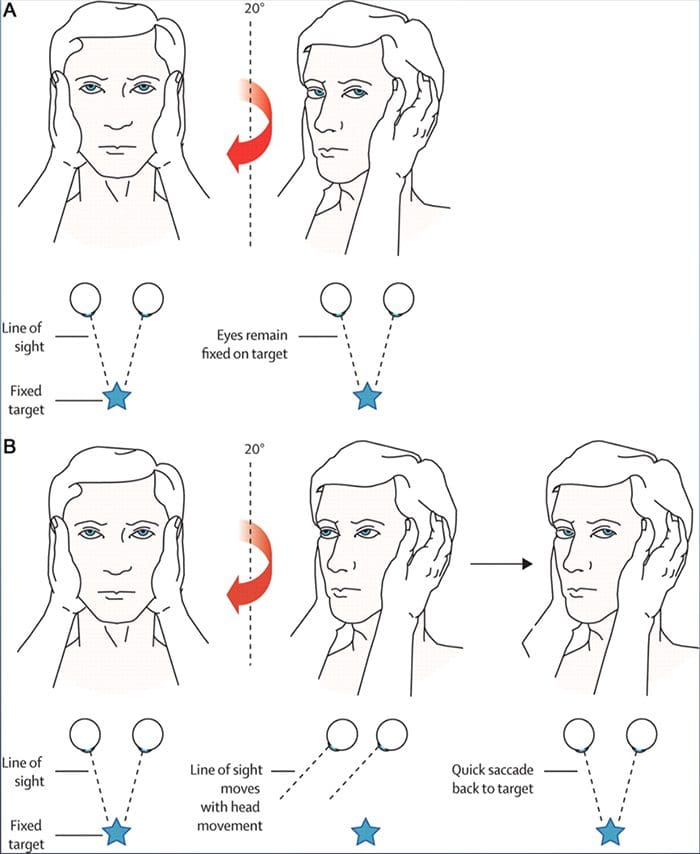
WHAT CAN YOU DO? Have the patient perform gaze stability exercises:
Have the patient perform gaze stability exercises:


 WHAT CAN YOU DO?
WHAT CAN YOU DO?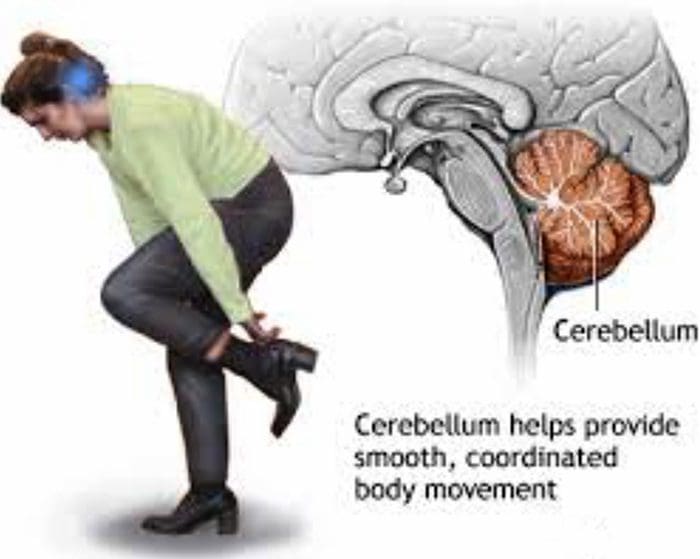 Have the patient perform coordinated movements!
Have the patient perform coordinated movements!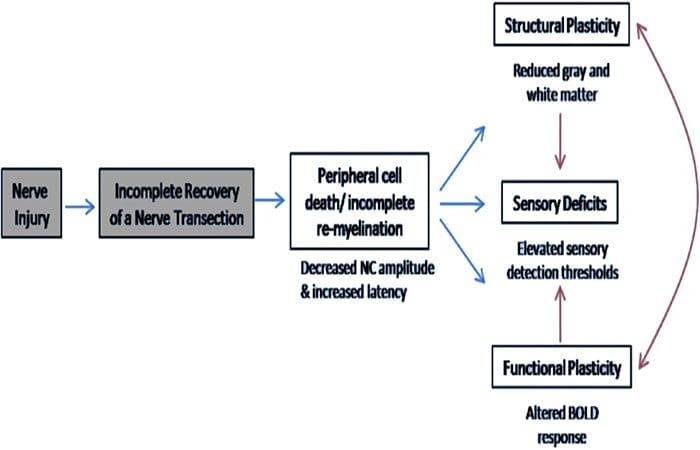

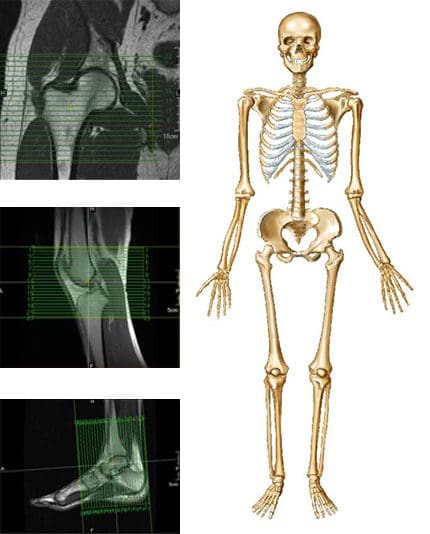 MRI may be requested for:
MRI may be requested for: