Cerebrovascular disease is a designated group of conditions that can lead to cerebrovascular event/s, i.e. stroke. These events affect the blood supply and vessels to the brain. With a�blockage, malformation, or hemorrhage�happens,�this�prevents brain cells from getting enough oxygen, which can cause brain damage. Cerebrovascular diseases can develop in different ways. These include deep vein thrombosis (DVT) and atherosclerosis.
Types of cerebrovascular disease: Stroke, transient ischemic attack, aneurysms, and vascular malformations
In the U.S. cerebrovascular disease is the fifth most common cause of death.
Contents
Cerebrovascular Disorders
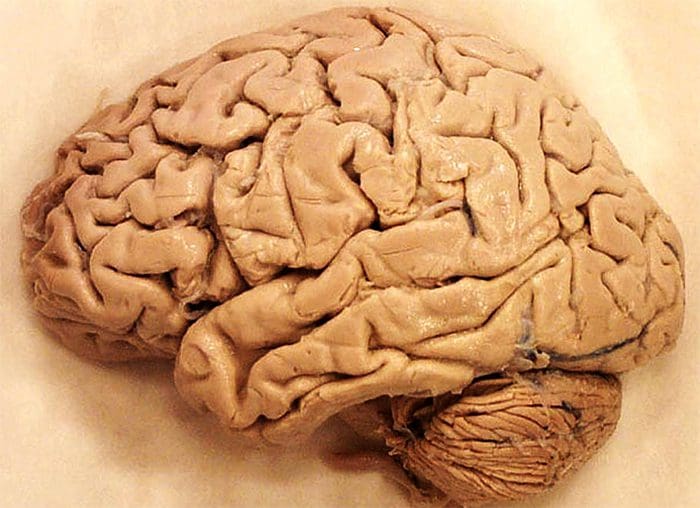
The Brain
- Makes up ~2% of the body weight
- Accounts for ~10% of the body�s oxygen use
- Accounts for ~20% of the body�s glucose use
- Receives ~20% of the cardiac output
- Per minute, requires ~50-80cc of blood per 100g of grey matter brain tissue and ~17-40cc of blood per 100g of white matter
- If blood supply to the brain is <15cc per 100g of tissue, per minute, neurologic dysfunction occurs
- As with all tissues, the longer there is ischemia, the more likely there is to be cell death and necrosis
- The brain depends on a constant, uninterrupted supply of oxygen and glucose
- 3-8 minutes of cardiac arrest can result in irreversible brain damage!
Autoregulation In The Brain
- Systemic hypotension causes reactive cerebral vasodilation to allow more blood flow to the brain
- The brain can extract enough oxygen from the brain if systolic pressure is 50 mmHg
- Atherosclerotic narrowing can produce reactive vasodilation to attempt to reduce excess pressure
- Increased blood pressure can result in vasoconstriction, reducing likelihood of hemorrhage
- If systolic pressure averages >150 mmHg for prolonged periods, this compensation may fail
- Labelled hypertensive encephalopathy
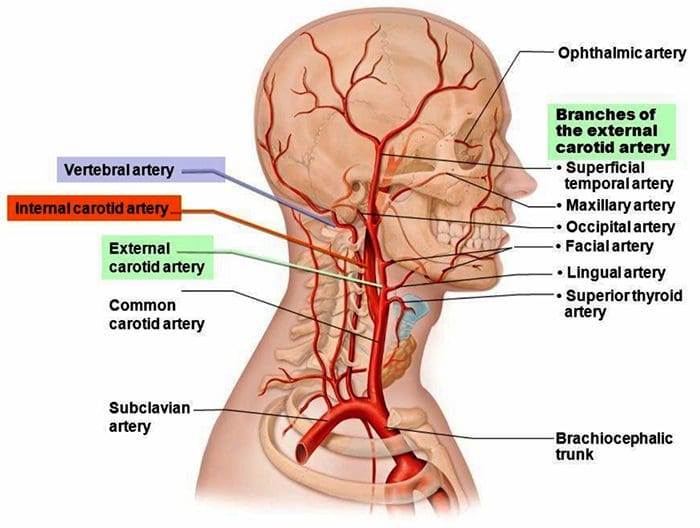
Blood Supply To The Head
 http://madeinkibera.com/lingual-arterie-anatomie
http://madeinkibera.com/lingual-arterie-anatomie
Collateral Circulation
- In slowly developing occlusion such as atherosclerotic thrombosis, collateral circulation has time to develop
- Circle of Willis connects the carotid and basilar systems
- Anterior and posterior communicating arteries provide collateral supply
- Anastomoses between main cerebral and cerebellar arteries in some people
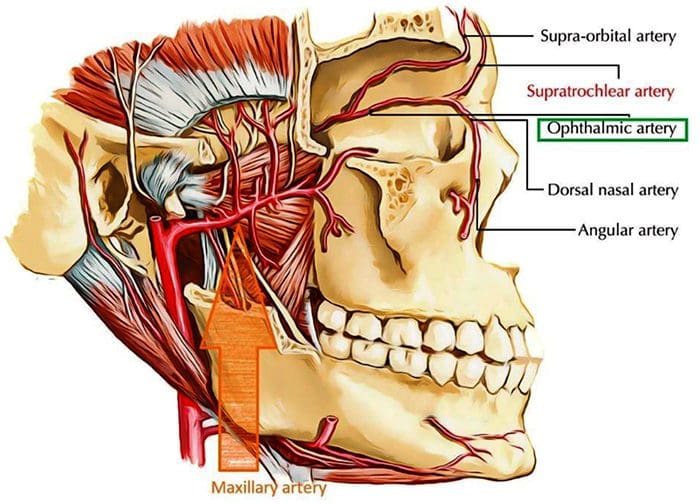
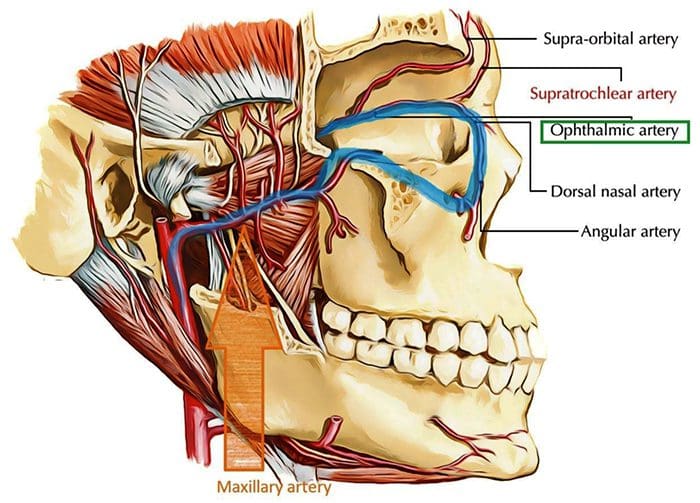
- Internal and external carotid artery connection via the ophthalmic & maxillary arteries
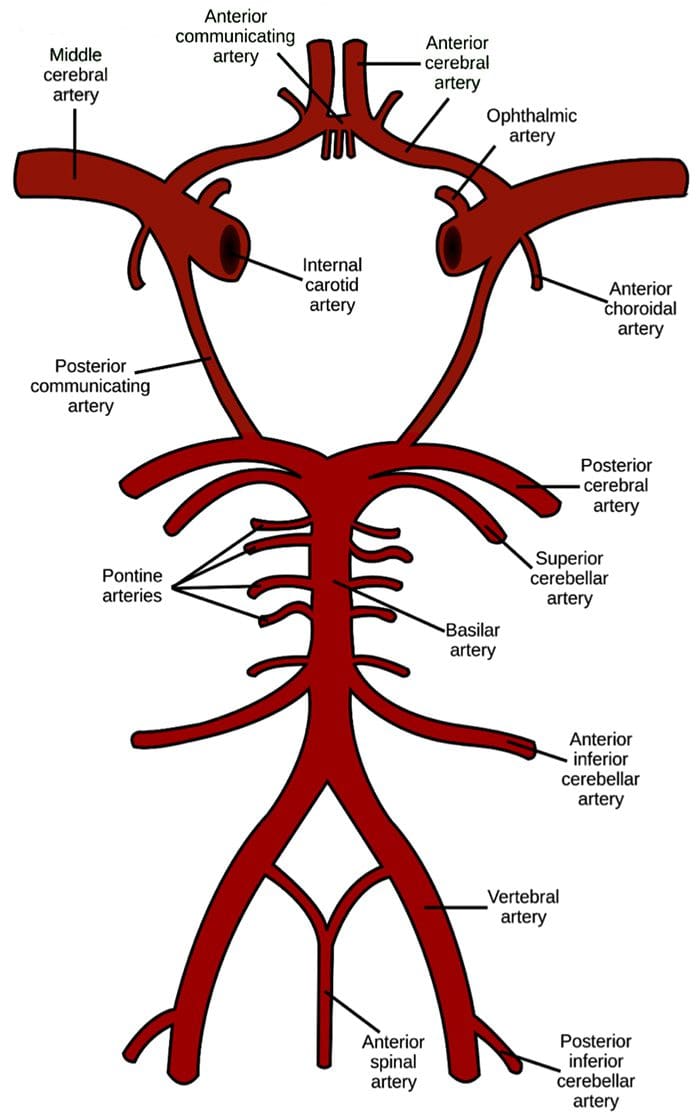
Circle Of Willis
- Connects the vertebrobasilar system with the internal carotid system
- While providing helpful collateral circulation, is also the most susceptible area to Berry Aneurysms which can lead to hemorrhagic stroke
 https://en.wikipedia.org/wiki/Circle_of_Willis
https://en.wikipedia.org/wiki/Circle_of_Willis
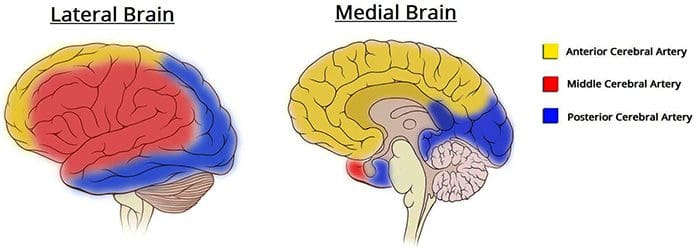
Blood Supply To The Brain
 http://teachmeanatomy.info/neuro/vessels/arterial-supply/
http://teachmeanatomy.info/neuro/vessels/arterial-supply/
Maxillary & Ophthalmic aa.
Cerebrovascular Disorders
- ~700,000 adults in the US have a stroke each year
- Third most common cause of death in the US
- ~2 million people are disabled due to stroke
- By far more common in persons of advanced age
- Occlusive/Ischemic Disease
- 80% of all strokes
- Most common site of occlusion is at the internal carotid artery just above the bifurcation of the common carotid a.
- Atherothrombotic
- Embolic
- Small vessel
- Hemorrhagic Disease
Occlusive/Ischemic Stroke
- Can be due to artery OR vein occlusion
- Artery occlusion is much more common
- Due to lack of blood & oxygen supply reaching a particular area of the brain
- Sudden onset of neurologic deficits, correlating to the distribution of a specific artery
- Deficits will differ depend on which artery�s distribution has been disrupted
Venous Occlusion
- Hyperviscocity
- Dehydration
- Thombocytosis
- Elevated red or white blood cells counts
- Polycythemia
- Hypercoagulability
- Elevated homocysteine
- Prolonged immobility or airplane travel
- Genetic clotting factor disorders
- Pregnancy
- Cancer
- Hormone replacement & OCP use
Atherothrombotic
- Neurologic deficits may be transient or develop slowly over time
- Possible causes/types:
- Dissection of the tunica intima and tunica adventitia
- Can occur in younger patients with connective tissue disorders
- Inflammatory materials deposit & build up in the vessel walls
- Oxidized LDLs deposit in vessel walls
Embolic
- Neurologic deficits likely to have sudden onset
- Dislodged tissue from dissection of the tunica intima and tunica adventitia
- Any dislodged thrombus can become an embolus blocking/closing the lumen of smaller vessels
Small Vessel
- Lipohyalinosis
- Vessel wall micro-trauma & ballooning
- Amyloid Angiopathy
- Accumulation of amyloid proteins in vessel walls
- More common in patients >65 years old
- Causes narrowing (leading to ischemia) but can also cause vessel fragility (leading to hemorrhage)
- Associated with Alzheimer�s disease
- Inflammatory
- Spasmotic
Risk Factors For Occlusive Stroke
- Hypertension
- Diabetes Mellitus
- Cardiac abnormalities
- Right-left shunts (Patent foramen ovale, VSD, tetralogy of fallot, etc)
- Atrial fibrillation
- Valve disease/artificial heart valves
- Advanced age
- Obesity
- Hyperlipidemia
- Especially high LDL and low HDL
- Sedentary lifestyle
- Cigarette/Tobacco smoking
- High oxidation status
- Elevated homocysteine
- Contributed to by low folic acid, B6 & B12 statuses
- Interacts with LDL cholesterol
- Hyperviscocity and hypercoagulability states as shown on previous slide
Transient Ischemic Attack (TIA)
- Fully reversible episodes of neurologic deficit due to vascular insufficiency generally lasting no more than 30 minutes at a time
- Occasionally can last 24 hours or more
- Half of patients who suffer from a complete occlusive stroke previously had transient ischemic attack(s)
- 20-40% of patients with TIA go on to have complete stroke
- In is important to identify patients with TIAs to that they can be appropriately managed and modifiable risk factors reduced
History of Transient Neurologic Deficit In Patient > 45 y/o
- DDx
- TIA most likely dx
- Migraine
- Focal seizures
- BPPV
- Meniere�s
- Demyelinating diseases
- Temporal arteritis
- Hypoglycemia
- Tumor
- Arteriovenous malformations
Carotid Artery Disease
- High pitched systolic bruit heard over the carotid artery may indicate carotid stenosis
- Requires duplex ultrasound evaluation
- Lesions narrowing the lumen >70% can possibly cause ischemia
- Many carotid occlusions do not cause ischemia due to slow development allowing for collateral circulation to be developed as well
- Fast forming occlusions or emboli can produce problems with <70% stenosis
- Surgical intervention should be considered for patients with >70% stenosis and symptoms of TIA
Occlusive Stroke
- If there is an onset of definitive substantial neurologic deficit, the patient should have a CT to rule out hemorrhage
- If hemorrhage is ruled out, tissue plasminogen activator should be given within the first 4.5 hours
- It should not be given later than this because it can increase risk of bleeding during reperfusion of brain tissue
- After this initial period, focused thrombolysis or mechanical extraction of the embolus
Intracranial Hemorrhage
- Approximately 20% of stroke cases
- Severe HA or vomiting suggest hemorrhage over occlusion
- Two types
- Spontaneous intracranial hemorrhage
- Hypertension
- Arterial aneurysms
- Arteriovenous malformations
- Bleeding disorders
- Vessel weakening due to amyloid angiopathy
- Traumatic
Aneurysm Sites
- Intraparenchymal hemorrhage
- 50% – Lenticulostriate branches of the middle cerebral artery
- Affects the putamen and external capsule
- 10% – Penetrating branches of the posterior cerebral artery
- Affects the thalamus
- 10% – Penetrating branches of the superior cerebellar artery
- Affects the cerebellum
- 10% – Paramedian branches of the basilar artery
- Affects the basilar pons
- 20% – Various vessels affecting areas of white matter
- Subarachnoid hemorrhage
- Berry aneurysms at communicating artery junctions
Bleeding Disorders
- Thrombocytopenia
- Leukemia
- Excess anticoagulant therapies
Risk Factors For Hemorrhagic Stroke
- Hypertension
- Arterial aneurysms
- Arteriovenous malformations
- Bleeding disorders
- Vessel weakening due to amyloid angiopathy
- Head trauma
Signs Of Stroke: Teach Patients F.A.S.T
 http://chrcsf.org/expert-tips-to-help-with-detecting-the-early-signs-of-stroke/
http://chrcsf.org/expert-tips-to-help-with-detecting-the-early-signs-of-stroke/
Common Transient Symptoms
- Vertigo
- Bilateral blurring or loss of vision
- Ataxia
- Diplopia
- Bilateral or unilateral sensory and motor deficits
- Syncope
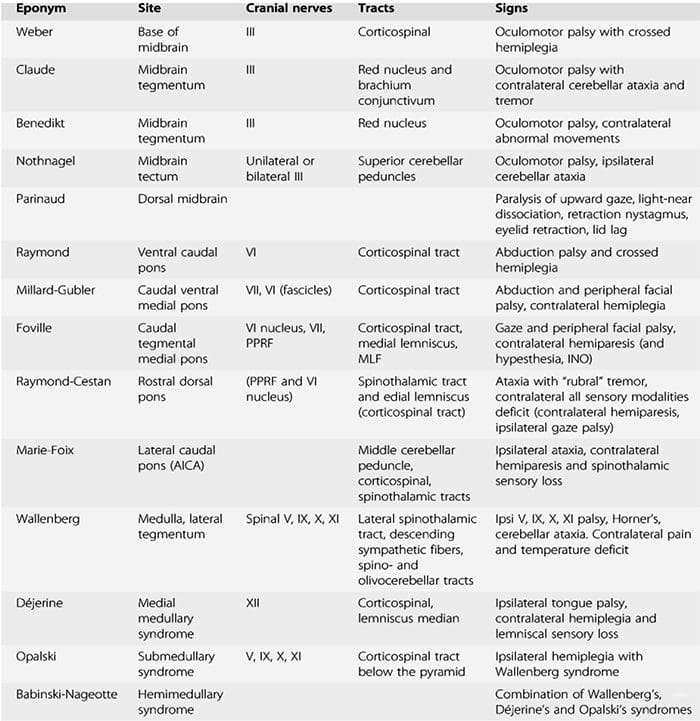
- Weakness in the distribution of a motor cranial nerve one side of the head with a contralateral hemiparesis (medial brainstem damage)
- Damage to a sensory cranial nerve & Horner�s syndrome on one side of the head and loss of contralateral pain and temperature sensation in the body (lateral brainstem damage)
Long-Term Symptoms Depend On Area Affected
- Monocular visual obscuration (amaurosis fugax) that is due to retinal ischemia
- Contralateral hemiparesis
- Hemisensory deficit
- Visual field deficits
- Dysphasia
- Receptive aphasia (Wernicke�s area lesion)
- Expressive aphasia (Broca�s areas lesion)
- Contralateral neglect (on-dominant parietal lobe lesion)
- Problemswithinitiationofmovement(Supplementarymotorcortex lesion)
- Difficulty with voluntary gaze to the contralateral side (Frontal eye field lesions)
- Short-term memory deficits(medial temporal lobes lesioned)
Brain-Stem Syndromes
 http://roho.4senses.co/stroke- syndromes/common-stroke- syndromes-chapter-9-textbook-of- stroke-medicine.html
http://roho.4senses.co/stroke- syndromes/common-stroke- syndromes-chapter-9-textbook-of- stroke-medicine.html
Stroke Recovery
- Rehab needs depend upon the area of brain tissue that was affected by the stroke
- Speech therapy
- Restriction of functioning limbs
- Balance and gait exercises
- Encourages neuroplastic restructuring
- Symptoms may improve within the first 5 days due to reduction in edema
- Edema may cause herniation through the foramen magnum which can cause brainstem compression and death � patients with this problem may require craniectomy (last resort)
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
Swenson, R. Cerebrovascular Disorders. 2010
General Disclaimer, Licenses and Board Certifications *
Professional Scope of Practice *
The information herein on "Cerebrovascular Disorders" is not intended to replace a one-on-one relationship with a qualified health care professional or licensed physician and is not medical advice. We encourage you to make healthcare decisions based on your research and partnership with a qualified healthcare professional.
Blog Information & Scope Discussions
Welcome to El Paso's Premier Wellness and Injury Care Clinic & Wellness Blog, where Dr. Alex Jimenez, DC, FNP-C, a Multi-State board-certified Family Practice Nurse Practitioner (FNP-BC) and Chiropractor (DC), presents insights on how our multidisciplinary team is dedicated to holistic healing and personalized care. Our practice aligns with evidence-based treatment protocols inspired by integrative medicine principles, similar to those on this site and on our family practice-based chiromed.com site, focusing on naturally restoring health for patients of all ages.
Our areas of multidisciplinary practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Our information scope is multidisciplinary, focusing on musculoskeletal and physical medicine, wellness, contributing etiological viscerosomatic disturbances within clinical presentations, associated somato-visceral reflex clinical dynamics, subluxation complexes, sensitive health issues, and functional medicine articles, topics, and discussions.
We provide and present clinical collaboration with specialists from various disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for musculoskeletal injuries or disorders.
Our videos, posts, topics, and insights address clinical matters and issues that are directly or indirectly related to our clinical scope of practice.
Our office has made a reasonable effort to provide supportive citations and has identified relevant research studies that support our posts. We provide copies of supporting research studies upon request to regulatory boards and the public.
We understand that we cover matters that require an additional explanation of how they may assist in a particular care plan or treatment protocol; therefore, to discuss the subject matter above further, please feel free to ask Dr. Alex Jimenez, DC, APRN, FNP-BC, or contact us at 915-850-0900.
We are here to help you and your family.
Blessings
Dr. Alex Jimenez, DC, MSACP, APRN, FNP-BC*, CCST, IFMCP, CFMP, ATN
email: [email protected]
Multidisciplinary Licensing & Board Certifications:
Licensed as a Doctor of Chiropractic (DC) in Texas & New Mexico*
Texas DC License #: TX5807, Verified: TX5807
New Mexico DC License #: NM-DC2182, Verified: NM-DC2182
Multi-State Advanced Practice Registered Nurse (APRN*) in Texas & Multi-States
Multi-state Compact APRN License by Endorsement (42 States)
Texas APRN License #: 1191402, Verified: 1191402 *
Florida APRN License #: 11043890, Verified: APRN11043890 *
Colorado License #: C-APN.0105610-C-NP, Verified: C-APN.0105610-C-NP
New York License #: N25929, Verified N25929
License Verification Link: Nursys License Verifier
* Prescriptive Authority Authorized
ANCC FNP-BC: Board Certified Nurse Practitioner*
Compact Status: Multi-State License: Authorized to Practice in 40 States*
Graduate with Honors: ICHS: MSN-FNP (Family Nurse Practitioner Program)
Degree Granted. Master's in Family Practice MSN Diploma (Cum Laude)
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card
Licenses and Board Certifications:
DC: Doctor of Chiropractic
APRNP: Advanced Practice Registered Nurse
FNP-BC: Family Practice Specialization (Multi-State Board Certified)
RN: Registered Nurse (Multi-State Compact License)
CFMP: Certified Functional Medicine Provider
MSN-FNP: Master of Science in Family Practice Medicine
MSACP: Master of Science in Advanced Clinical Practice
IFMCP: Institute of Functional Medicine
CCST: Certified Chiropractic Spinal Trauma
ATN: Advanced Translational Neutrogenomics
Memberships & Associations:
TCA: Texas Chiropractic Association: Member ID: 104311
AANP: American Association of Nurse Practitioners: Member ID: 2198960
ANA: American Nurse Association: Member ID: 06458222 (District TX01)
TNA: Texas Nurse Association: Member ID: 06458222
NPI: 1205907805
| Primary Taxonomy | Selected Taxonomy | State | License Number |
|---|---|---|---|
| No | 111N00000X - Chiropractor | NM | DC2182 |
| Yes | 111N00000X - Chiropractor | TX | DC5807 |
| Yes | 363LF0000X - Nurse Practitioner - Family | TX | 1191402 |
| Yes | 363LF0000X - Nurse Practitioner - Family | FL | 11043890 |
| Yes | 363LF0000X - Nurse Practitioner - Family | CO | C-APN.0105610-C-NP |
| Yes | 363LF0000X - Nurse Practitioner - Family | NY | N25929 |
Dr. Alex Jimenez, DC, APRN, FNP-BC*, CFMP, IFMCP, ATN, CCST
My Digital Business Card






