Learning how to stay active with busy lives and schedules takes practice. There are daily ways to incorporate physical movement into the everyday routine and shed sedentary habits in favor of more active ones resulting in improved overall health, elevated mood, and better energy levels. Regular movement lowers body weight and reduces the risk of medical conditions like cardiovascular disease, diabetes, and arthritis. And regularly incorporating small physical activities throughout the day can make the exercise more fun and not like a chore that begins to become second nature.
Daily Ways To Stay Active
Like most individuals, much time is spent sitting in the car, workstation/desk, or couch. Research has found that maintaining physical activity can reduce the risk of colon and breast cancer.
Movement
Everyone is different, and there is no one-size-fits-all daily or weekly movement plan. The Centers for Disease Control and Prevention recommends that adults ages 18 to 64 get around 150 minutes of moderate-intensity weekly exercise combined with functional strength training. This can seem like a lot, but still, some activity is better than none. Wherever an individual is in physical fitness, it is never too late to make incremental adjustments and rebuild health one step at a time.
Brisk walking is an example of moderate-intensity exercise.
Individuals with busy schedules can break up their daily movement into smaller chunks.
5 or 10 minutes here and there add up to significant health benefits.
Start With Stretching
A quick morning stretch of 10 minutes can help limber up the muscles, get circulation pumping, and reduce stress.
A study found that a regular 10-minute stretching plan helped reduce anxiety and physical pain and increase flexibility.
Stand Up and Walking Around More
Standing up every 20-30 minutes at home or work is recommended during seated activities.
Walking and thinking increases creative output.
Mobility gets the blood pumping and increases caloric output.
With regular practice, individuals learn to feel their muscles tensing from too much sitting and know it’s time to get up and move.
One way to stand and move is to pace the room during a phone call.
Take the Long Way
Take the stairs or park farther from the store to increase walking steps.
Physical activity in small bursts creates a mindset of an added challenge.
Choosing to go the long way does make a difference and can significantly affect other areas of life.
Move to Music
Research shows that music has amazing effects on physical activity.
It distracts from pain and fatigue.
It increases endurance.
Makes physical activity and exercise feel like less of an effort.
Playing moving music around the office, if possible/headphones and house can get the body naturally moving more.
This could be washing dishes after dinner, using the whole body
Vacuuming the house can work the muscles and elevate the heart rate.
A 150-pound person can burn serious calories from a full hour of cleaning and chores.
Added mental health benefits from the work reduce anxiety, depression, and negative mood.
Get Up When Commercials Come On
Get up and move during commercial breaks.
But with streaming services, commercials aren’t the same.
When watching shows or movies without built-in commercials, make a habit of getting up.
For shows or movies with no commercials, pause and take a quick stretch, do a quick round of jumping jacks, or walk to the other end of the house or twice in an apartment and back.
A brief break is not an actual workout, but it will get the heart pumping more than staying sedentary.
The more you do it, the more natural it will become.
Military Training and Chiropractic Care
References
Habay, Jelle, et al. “Interindividual Variability in Mental Fatigue-Related Impairments in Endurance Performance: A Systematic Review and Multiple Meta-regression.” Sports medicine – open vol. 9,1 14. 20 Feb. 2023, doi:10.1186/s40798-023-00559-7
Hotta, Kazuki, et al. “Daily muscle stretching enhances blood flow, endothelial function, capillarity, vascular volume and connectivity in aged skeletal muscle.” The Journal of Physiology vol. 596,10 (2018): 1903-1917. doi:10.1113/JP275459
Kruse, Nicholas T, and Barry W Scheuermann. “Cardiovascular Responses to Skeletal Muscle Stretching: “Stretching” the Truth or a New Exercise Paradigm for Cardiovascular Medicine?.” Sports medicine (Auckland, N.Z.) vol. 47,12 (2017): 2507-2520. doi:10.1007/s40279-017-0768-1
Maltese, Paolo Enrico et al. “Molecular foundations of chiropractic therapy.” Acta bio-medica : Atenei Parmensis vol. 90,10-S 93-102. 30 Sep. 2019, doi:10.23750/abm.v90i10-S.8768
Ma, Peng, et al. “Daily sedentary time and its association with risk for colorectal cancer in adults: A dose-response meta-analysis of prospective cohort studies.” Medicine vol. 96,22 (2017): e7049. doi:10.1097/MD.0000000000007049
Rangul, Vegar, et al. “The associations of sitting time and physical activity on total and site-specific cancer incidence: Results from the HUNT study, Norway.” PloS one vol. 13,10 e0206015. 23 Oct. 2018, doi:10.1371/journal.pone.0206015
Shen, Dong, et al. “Sedentary behavior and incident cancer: a meta-analysis of prospective studies.” PloS one vol. 9,8 e105709. 25 Aug. 2014, doi:10.1371/journal.pone.0105709
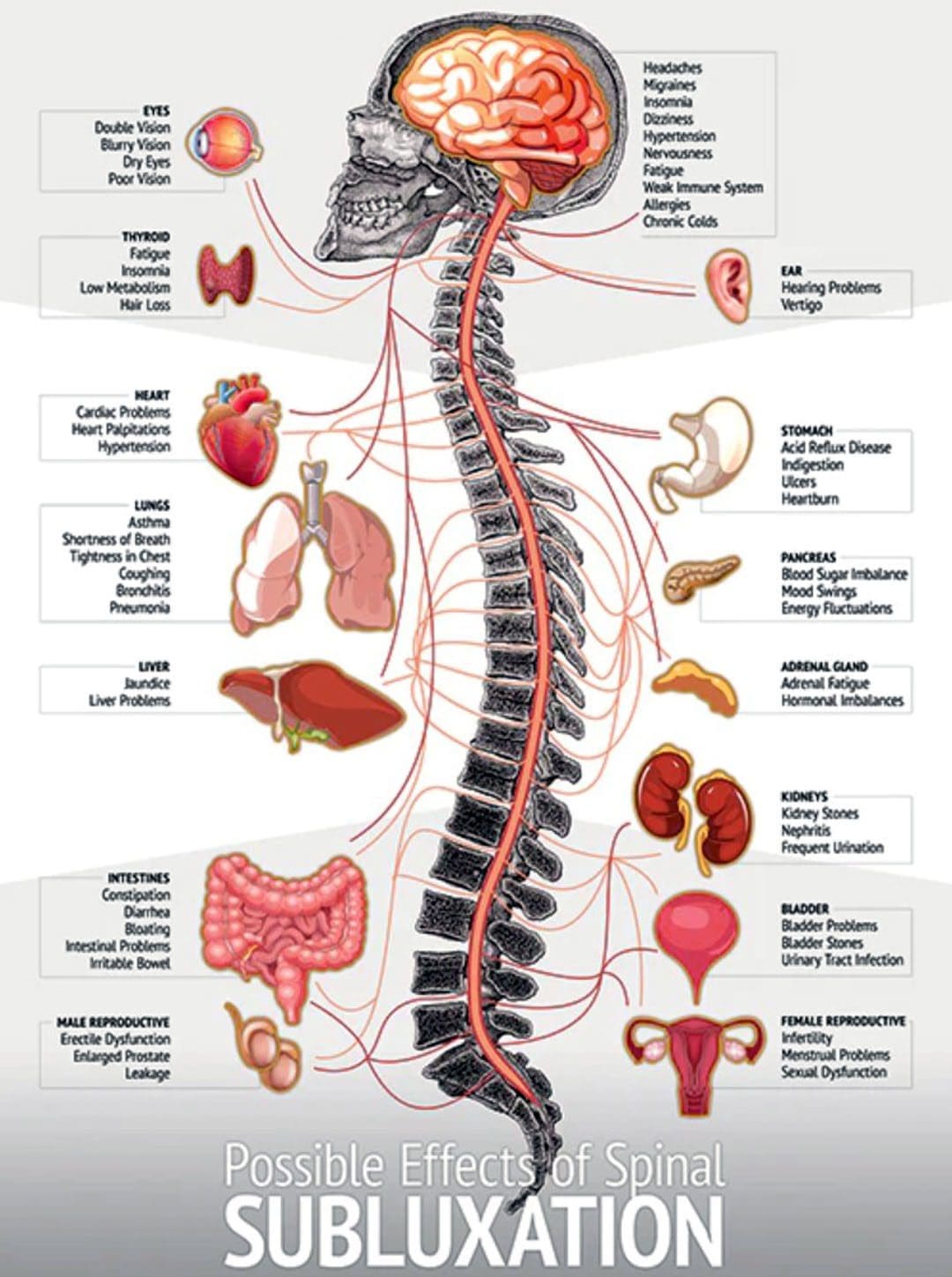
Body misalignment can cause various symptoms to be experienced, ranging from headaches, neck and back pain, sore feet, discomfort in the joints, muscles, or nerves, and digestive problems. Improperly aligned vertebrae can press against nerves, pinching or compressing them, causing the nerve signals of the digestive system, including those in the stomach and intestines, to misfire or fail to transmit at the appropriate moment. This can cause the organs to malfunction, resulting in heartburn, gas, constipation, cramping, diarrhea, and other symptoms. Chiropractic realignment adjustments are an effective treatment option for frequent stomachaches, reflux, constipation, and other gastrointestinal conditions.
Body Misalignment Digestive Problems
There are over a million nerve cells within the digestive system. A collection of nerves branch out from the lower part of the spinal cord and travels to the stomach and intestines. Nerve transmission plays an essential role in the following:
Digestion.
Movement of food through the gastrointestinal system.
Absorption of nutrients and minerals.
Removal of waste products.
Misalignments of the vertebrae are known as subluxations. Pressure on nerve roots caused by misalignment can interfere with the function of the bowel and other organs, which can lead to gastrointestinal issues. Muscle tension in the abdomen can also contribute to digestive problems, whether because of stress or sitting for long hours daily.
Misalignment Symptoms
When the body is out of alignment, symptoms of discomfort begin to appear. The most common include:
Fatigue.
Stiff neck.
Sore shoulders.
Chronic headaches.
Sore muscles.
Pain throughout the back.
Joint pain throughout the body.
Chronic aches.
Tight hips.
Difficulty walking.
Tingling, pins and needles, and numbness nerve sensations – sciatica.
Constantly getting sick.
Healthy Gut
A balanced healthy gut will have less difficulty processing food and eliminating waste, leading to reduced and eventually alleviated symptoms. The following show healthy gut function:
Regular, consistent energy levels.
Increased mental clarity.
Regular and healthy bowel movements.
No pain or discomfort symptoms.
A normal amount of gas and bloating.
Healthy stress levels.
Chiropractic
Chiropractic care will realign the body to its proper form, improving gastrointestinal issues. The chiropractic team will use various tools and techniques to guide and correct any subluxations, relax the muscles, and increase nerve and blood circulation.
Healthy Diet and Chiropractic
References
Ernst, Edzard. “Chiropractic treatment for gastrointestinal problems: a systematic review of clinical trials.” Canadian Journal of Gastroenterology = Journal canadien de Gastroenterologie vol. 25,1 (2011): 39-40. doi:10.1155/2011/910469
Hills, Ronald D Jr, et al. “Gut Microbiome: Profound Implications for Diet and Disease.” Nutrients vol. 11,7 1613. 16 Jul. 2019, doi:10.3390/nu11071613
Hornbuckle, William E., et al. “Gastrointestinal Function.” Clinical Biochemistry of Domestic Animals (2008): 413–457. doi:10.1016/B978-0-12-370491-7.00014-3
Leeming, Emily R et al. “Effect of Diet on the Gut Microbiota: Rethinking Intervention Duration.” Nutrients vol. 11,12 2862. 22 Nov. 2019, doi:10.3390/nu11122862
Li, Yuanyuan, et al. “The Role of Microbiome in Insomnia, Circadian Disturbance, and Depression.” Frontiers in psychiatry vol. 9 669. 5 Dec. 2018, doi:10.3389/fpsyt.2018.00669
Redwood, Daniel. “Chiropractic and visceral disorders.” Journal of Alternative and complementary medicine (New York, N.Y.) vol. 13,5 (2007): 479-80. doi:10.1089/acm.2007.7146
Valdes, Ana M et al. “Role of the gut microbiota in nutrition and health.” BMJ (Clinical research ed.) vol. 361 k2179. 13 Jun. 2018, doi:10.1136/bmj.k2179
Individuals may not be aware that back discomfort/pain symptoms can be connected to not staying hydrated. When the body is dehydrated, it reduces the amount of fluid in the spinal discs making them smaller, resulting in decreased cushioning and support for the spine. The stress can lead to swelling, causing further back discomfort, even a herniated disc. Individuals that experience frequent back pain could find relief by increasing their H2O consumption.
Staying Hydrated
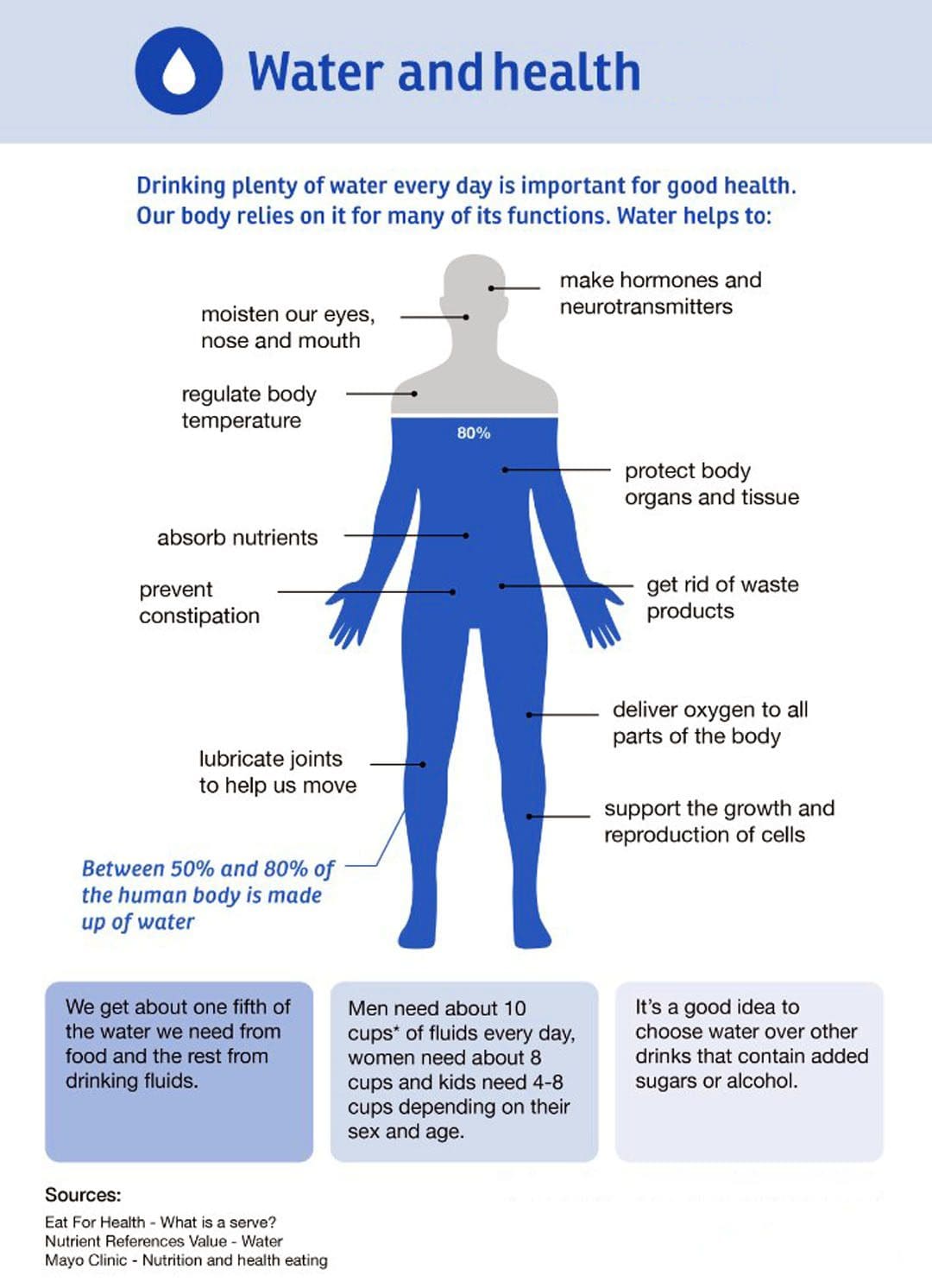
Physical activity and healthy nutrition are important for healthy living. However, individuals can forget the basic need for water, often resulting in dehydration. The body needs to maintain hydration levels to function correctly. Dehydration can cause the body’s fascia/connective tissue which supports every cell and organ, to lose lubrication that allows the muscles to move, slide, and glide smoothly, causing stiffness, and tangled knots/trigger points, making movement difficult and painful.
The Body’s Overall Health
The body is 60% water.
Hydration replaces body fluids lost through exhaling, sweating, and waste elimination.
The body loses and needs to replace around 2-3 quarts of water daily.
Proper hydration regulates temperature, keeps the joints functioning smoothly, protects the spine, and facilitates waste removal.
Dehydration
Even being a little dehydrated is not healthy. Studies have shown that losing 1-2% of body weight without replacing fluids causes thinking and memory problems. A 4% deficit causes headaches, irritability, and sleepiness. Physical work or working outdoors without proper hydration impairs muscle endurance and strength. Dehydration stresses the spine even more which can cause painful swelling and bulged discs. Chronic pain conditions can be worsened by dehydration. This includes:
Overall stiffness
Headaches
Migraines
Joint pain
Arthritis
Fibromyalgia
All can be affected by dehydration.
Lack of water levels can lead to back pain because the discs between the vertebrae need fluid to cushion the bones. They begin to dry out when not properly hydrated, exacerbating back discomfort symptoms that could lead to similar symptoms in the neck or legs.
The spinal discs are filled with a gel substance of around 75% water.
The inner and outer rings/nucleus pulposus are made almost entirely of water.
Water is slowly released from the spinal discs throughout the day.
The discs absorb most of the shock from everyday movements while protecting the spinal cord.
The discs rehydrate during sleep.
Indicators of Dehydration
Other than back pain and discomfort, other symptoms of dehydration.
Fatigue
Irritability
Muscle Cramps
Headaches
Dark Urine
Dry Skin
Dry Eyes
Blurry Vision
Bad Breath
Dizziness
Fever
Caffeinated beverages – soft drinks, tea, and coffee count partly toward daily fluid intake. They do not dehydrate the body, but they can increase urination and are recommended not to be the primary source of liquids during the day.
Hydration
Throughout the day, drink plenty of water and move around and stretch to circulate the H2O.
Increase Water Intake
Sixty-four ounces, eight glasses per day, is the common recommendation.
Water intake encompasses all the liquids consumed in a day, including coffee, tea, and soup.
Foods like cantaloupe and watermelon count toward daily water consumption.
The best sources are water and drinks, primarily water sport replacement drinks, herbal teas, lemon water, and vegetable broth.
Drink more when working out and being active. More water is needed on top of the 64 ounces when active.
Keep hydrating long after the physical activity or workout is over.
When the brain signals thirst, the body is already dehydrated.
Stay ahead by sipping water throughout the day.
Keep a water bottle close by at school or work, refill it twice daily, and increase refills on hot days.
Monitor Hydration Levels
An easy way to assess dehydration is by looking at urine color.
Light yellow or clear is healthy.
Dark yellow or cloudy indicates dehydration.
The Injury Medical Chiropractic and Functional Medicine Team can realign the spine and body to optimal function and assist in developing a nutrition plan to maintain health and wellness.
Benefits Of Healthy Eating and Chiropractic Care
References
El-Sharkawy, Ahmed M et al. “Acute and chronic effects of hydration status on health.” Nutrition Reviews vol. 73 Suppl 2 (2015): 97-109. doi:10.1093/nutrit/nuv038
Johannaber, Kenneth, and Fadi A Fathallah. “Spinal disc hydration status during the simulated stooped posture.” Work (Reading, Mass.) vol. 41 Suppl 1 (2012): 2384-6. doi:10.3233/WOR-2012-0470-2384
Manz, Friedrich, and Andreas Wentz. “The importance of good hydration for the prevention of chronic diseases.” Nutrition Reviews vol. 63,6 Pt 2 (2005): S2-5. doi:10.1111/j.1753-4887.2005.tb00150.x
Ritz, Patrick, and Gilles Berrut. “The importance of good hydration for day-to-day health.” Nutrition Reviews vol. 63,6 Pt 2 (2005): S6-13. doi:10.1111/j.1753-4887.2005.tb00155.x
Providing the body with adequate hydration and nutrition at the right time can maximize performance abilities, endurance, and muscle repair and restoration. Eating the right foods at the right time will fuel the body to support intense exercises. That means plenty of energy for cardiovascular and strength training. The optimal combination of pre-workout nutrition depends on the type of workout and how long it takes for the body to absorb the nutrients to get moving. Injury Medical Chiropractic and Functional Medicine Clinic can develop a fitness and nutritional plan customized to the individual’s needs and health goals.
Pre-Workout Nutrition
The three main macronutrients are carbohydrates, proteins, and fats when preparing pre-workout meals and snacks. Ratios are based on the specific needs of the workout. For example, going for a one-mile jog or a light aerobics class requires different amounts for different purposes. The longer and more intense the exercise, the more food is needed. Individuals may only need to modify or adjust their eating habits slightly for light workouts. Their roles vary:
Carbohydrates
Fats
Proteins
Each has a different role in supplying fuel for powering through physical activity.
Carbohydrates
Carbs are an important fuel for exercise.
Carbs can be found in grains, fruits, vegetables, and dairy products.
These are the easiest energy foods for the body to turn into glucose.
Glucose is stored in the muscles as glycogen.
Without enough carbohydrates, the body will be depleted of energy and become exhausted.
Proteins
This macronutrient is found in poultry, eggs, fish, and nuts.
Takes longer for the body to digest.
Protein helps the body feel full.
The body uses various nutrients to repair and build muscles.
Getting protein throughout the day can help with recovery after a workout.
Fats
The body burns fat for longer low to moderate-intensity workouts, such as a long run or bicycle ride.
However, fat takes more effort and time for the body to digest.
So, eating healthy fats is not the best right before exercise.
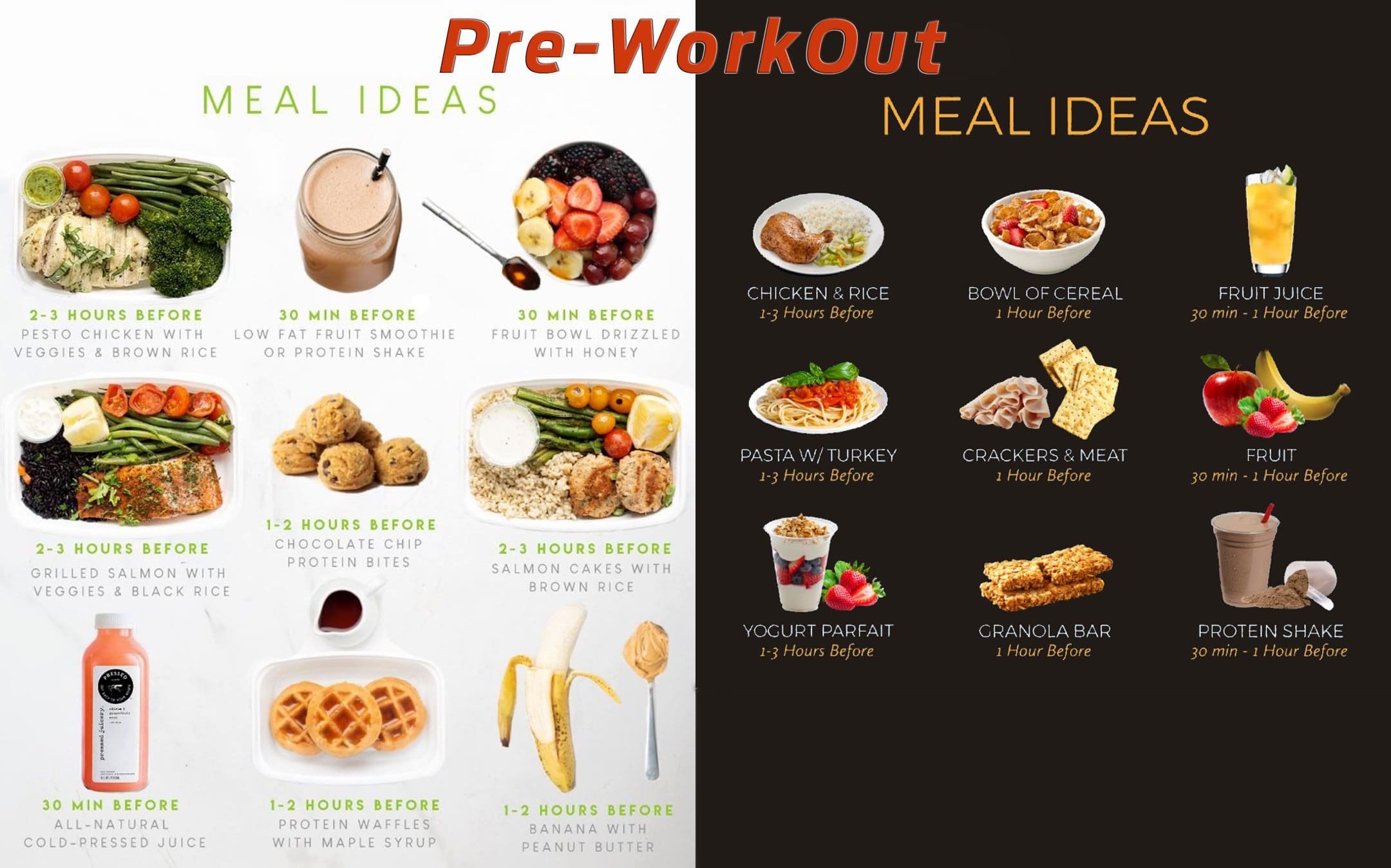
Pre-Workout Nutrition Guidelines
The exact mix of foods/nutrients ideal for the workout depends on when the individual can eat in relation to the time of the activity and intensity of the exercise.
Two to Four Hours Before Exercising
Have a meal containing a mix of carbohydrates, fats, and protein.
Oatmeal with fruit and nuts, a turkey sandwich with vegetables and some fruit, or a chicken and rice bowl with vegetables and avocado.
One to Two Hours Before Exercising
A light meal or snack.
Cereal with low-fat milk, peanut butter with crackers, or a fruit smoothie.
Avoid foods high in fiber and fat because they take longer to digest and can lead to digestion/stomach issues during exercise.
Before Morning Exercise
Going to the gym or out for a run first thing in the morning, something small, like a banana or granola bar.
For individuals that can’t eat early, don’t force yourself.
Have an extra portion at dinner or a snack before bed to have enough fuel for the morning.
During Workout
Have easy-to-digest carbs if the exercise session lasts more than an hour.
A banana or pretzels.
Sports drink during the workout contains electrolytes and minerals like sodium, magnesium, and potassium that assist in regulating functions like muscle contractions lost as the body sweats.
Hydration
Liquids are lost when the body sweats. Sipping water before, during, and after the workout is important.
Even a small dip in hydration levels can lower exercise performance and lessen mental sharpness.
Drinking two to three cups of water two to three hours before exercise is recommended.
During the workout, you should get at least a half to a full cup of water every 15 to 20 minutes.
After the workout, replenish hydration levels with two to three more cups.
Pre-Workouts
References
Jensen, Jørgen, et al. “The role of skeletal muscle glycogen breakdown for regulation of insulin sensitivity by exercise.” Frontiers in physiology vol. 2 112. 30 Dec. 2011, doi:10.3389/Phys.2011.00112
Jeukendrup, Asker. “A step towards personalized sports nutrition: carbohydrate intake during exercise.” Sports medicine (Auckland, N.Z.) vol. 44 Suppl 1, Suppl 1 (2014): S25-33. doi:10.1007/s40279-014-0148-z
Lowery, Lonnie M. “Dietary fat and sports nutrition: a primer.” Journal of sports science & Medicine vol. 3,3 106-17. 1 Sep. 2004
Ormsbee, Michael J et al. “Pre-exercise nutrition: the role of macronutrients, modified starches, and supplements on metabolism and endurance performance.” Nutrients vol. 6,5 1782-808. 29 Apr. 2014, doi:10.3390/nu6051782
Rothschild, Jeffrey A et al. “What Should I Eat Before Exercise? Pre-Exercise Nutrition and the Response to Endurance Exercise: Current Prospective and Future Directions.” Nutrients vol. 12,11 3473. 12 Nov. 2020, doi:10.3390/nu12113473
Shirreffs, Susan M. “The importance of good hydration for work and exercise performance.” Nutrition Reviews vol. 63,6 Pt 2 (2005): S14-21. doi:10.1111/j.1753-4887.2005.tb00149.x
When it comes to the body, the lower portion has three compartments of muscles that work together to provide stability and mobility to the host when they are in motion. The anterior, posterior, and lateral compartments have numerous muscles, tissues, and ligaments that support the spine and allow the musculoskeletal system to do various movements without pain. When normal factors affect the body, it can cause symptoms of overlapping risk profiles that can lead to musculoskeletal pain disorders associated with pain-like symptoms in the joints and muscles. Today we will look at one of the muscle compartments known as the postural muscles, how postural pain affects the body, and how manual therapy combined with the MET technique can improve the postural muscles. We mention valuable information about our patients to certified medical providers who use methods like the MET combined with manual therapy to reduce pain-like symptoms associated with musculoskeletal disorders. We encourage patients by referring them to our associated medical providers based on their findings. We support that education is a marvelous way to ask our providers the most interesting questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., incorporates this information as an educational service. Disclaimer
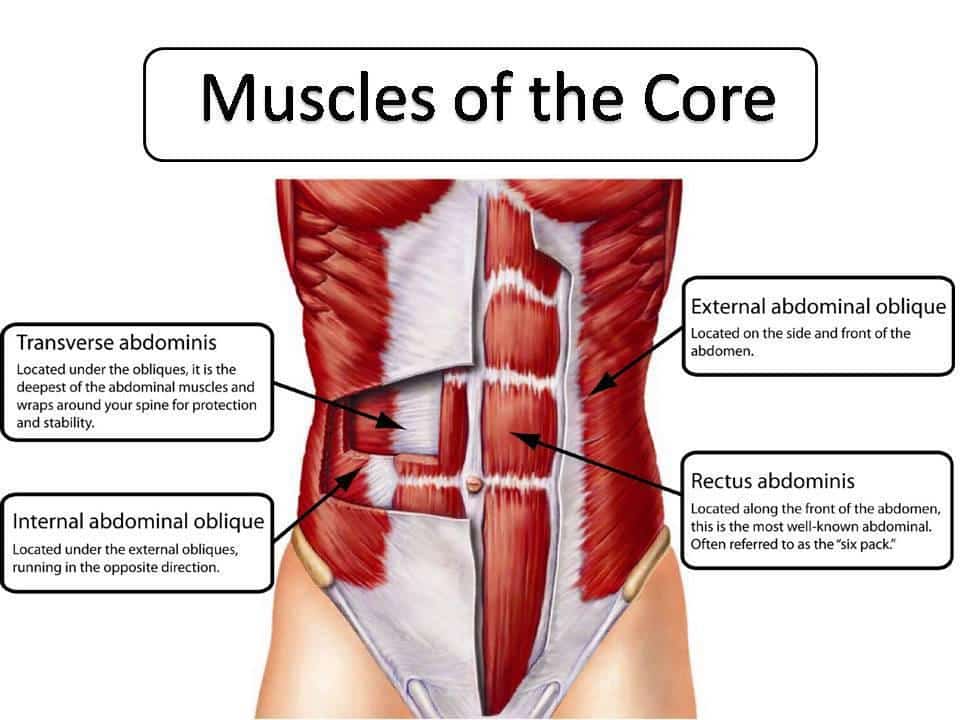
What Are The Postural Muscles?
Are you experiencing muscle stiffness in your lower back? What about aches and pain in your shoulders and neck? Or have you noticed your legs feel heavy after sitting down for a long time? Many of these issues are associated with the postural muscles that are causing pain to the musculoskeletal system. So what are the postural muscles in the musculoskeletal system? Well, they are the core muscles that are deep within the abdomen, pelvis, and back. Research studies reveal that the curvature of the spine (cervical, thoracic, and lumbar regions) communicates and works with the central nervous system and musculoskeletal system to provide balance, support, and resistance against pressure on the body. The postural muscles are important in the body as they ensure the host has perfect posture when walking, sitting, or standing. Additional studies mentioned that good postural and stability control are the fundamentals for motor skills. When a person has good postural control, it can help give them a stable gait when walking. However, as the body ages, the postural muscles can become weak and lead to muscle strain while affecting the joints and tendon structures.
The Effects Of Postural Pain In The Body
So what happens to the body when dealing with pain in the postural muscles, and how does it affect one’s posture? Research studies reveal that reducing back muscle endurance from prolonged sitting, slouching, or constantly looking down can cause muscle strain symptoms in the postural muscles. To that point, it can lead to increased development of low back pain and lumbar discomfort in the joints. As stated earlier, other factors like slouching, prolonged sitting, and constantly looking down can affect the lower back, shoulders, and neck. The various muscles that make up the shoulders and neck would become strained and tensed, leading to shoulder and neck pain that can cause discomfort. When these overlapping symptoms affect the body, it can cause many overlapping symptoms that can overlap and cause the individual to be miserable.
How Neck Injuries Affect The Body- Video
Have you been experiencing any muscle strain in your neck, shoulders, or lower back? Does stretching bring temporary relief? Or have you been dealing with heaviness in your legs? Many of these factors are associated with weak postural muscles that can contribute to poor posture, low back and neck pain, and other musculoskeletal issues. The video above explores the common causes and symptoms of neck injuries and how treatments like chiropractic care can help alleviate the symptoms. Treatments like chiropractic care utilize manual manipulation and various techniques to help realign the body and reduce any musculoskeletal disorders associated with pain. Chiropractic care is non-invasive and works with other medical professionals to restore the body naturally.
Manual Therapy & MET On Postural Muscles
So what can one do when dealing with postural pain and trying to find relief? Many individuals go to treatments like chiropractic care, which can allow the body to be realigned and restored naturally. Treatments like chiropractic care can help restore good posture in the spine while relieving and reducing excess pain and strain on the various muscles, tendons, and joints. Additionally, chiropractors use techniques like the MET technique to reduce stress on the soft tissues and restore the joint’s range of motion. According to the book, “Clinical Applications of Neuromuscular Techniques,” Leon Chaitow N.D., D.O., and Judith Walker DeLany L.M.T., stated that muscle restoration is accompanied by biomechanical solutions and strategies that are introduced to the body and become a key focus on the muscles that required strengthening, enhancing, and improve breathing and posture function. When therapists like chiropractors and massage therapists use the MET technique, the affected muscles can be stretched and strengthened while restoring the structural and functional imbalances the body has endured. This can help improve postural muscles while allowing the body to heal naturally. This allows the individual to be mindful of how they present themselves with good posture.
Conclusion
Overall, the body requires the postural muscles to help stabilize and keep the body mobile. When musculoskeletal disorders associated with pain started to affect the muscles through bad posture or other normal factors, it can cause these muscles to be weak and develop musculoskeletal conditions that can lead many individuals to constant pain. Luckily therapies like chiropractic care combined with the MET technique allow the affected muscles to be stretched and strengthened. This allows the body to be realigned and restored naturally. Incorporating stretching combined with chiropractic care can help many individuals be mindful of their posture and enable them to continue their health and wellness journey without pain.
References
Carini, Francesco, et al. “Posture and Posturology, Anatomical and Physiological Profiles: Overview and Current State of Art.” Acta Bio-Medica : Atenei Parmensis, U.S. National Library of Medicine, 28 Apr. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6166197/.
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Jung, Kyoung-Sim, et al. “Effects of Prolonged Sitting with Slumped Posture on Trunk Muscular Fatigue in Adolescents with and without Chronic Lower Back Pain.” Medicina (Kaunas, Lithuania), U.S. National Library of Medicine, 23 Dec. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7822118/.
Ludwig, Oliver, et al. “Neuromuscular Performance of Balance and Posture Control in Childhood and Adolescence.” Heliyon, U.S. National Library of Medicine, 31 July 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7398941/.
The various muscle groups in the body allow the host to move around and function through many actions without feeling any discomfort or pain. The body has two sections: upper and lower portions that have different functions, from turning the neck from side to side to allowing the legs to enable the body to move around. When various issues or factors begin to affect the body over time, like muscle injuries or normal factors like poor posture and prolonged sitting, it causes overlapping risk profiles that can lead to chronic musculoskeletal conditions. When musculoskeletal disorders affect the body, it can lead to muscle and joint pain that can cause misalignment in the spine and cause the muscle fibers to become short and tense. Luckily there are available treatments that allow the body to realign itself and stretch those short muscles. Today’s article looks at how muscle pain affects the body and how different variations of the MET technique are used to reduce and stretch muscle pain. We mention and provide valuable information about our patients to certified medical providers who use techniques like the MET and therapy for individuals with muscle strain associated with body pain. We give encouragement to patients by referring them to associated medical providers based on their diagnostic findings. We support that education is a marvelous way to ask our providers the most interesting questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., incorporates this information as an educational service. Disclaimer
How Does Muscle Pain Affect The Body?
Have you been dealing with muscle strain or pain in different body areas? Are you experiencing any referred pain in other body locations? Or are your muscles feeling extremely tight that it is causing you pain? When the body is dealing with various issues that are causing the muscle fibers to be tensed, it can lead to muscle pain and cause many people to suffer. Studies reveal that muscle pain is caused when painful conditions like mechanical forces, ischemia, and inflammation stimulate the body’s free nerve endings. Many of these factors also correlate with musculoskeletal disorders like fibromyalgia and myofascial pain that can develop trigger points (palpable, small nodules) in the muscle fibers to cause the muscles to become stiff and contract. Additional studies also reveal that when the muscles begin to cramp up, especially the calves, it can become extremely painful and involuntary as it affects the entire muscle group, the muscle itself, or any selected muscle fibers. This causes the individual to be in pain in an acute setting as the muscle relaxes; however, if the muscle fibers are still in constant contraction, it can lead to chronic issues that affect the muscle group.
Overcoming Pain With Chiropractic Care-Video
Regarding muscle pain in the body, studies reveal that the nociceptive nerve endings in the muscles and tissue fibers can cause the neuron signals from the central nervous system to become hyperexcitable, and hyperactivity can lead to muscle pain. This causes the muscle group and the surrounding muscles to tense and invokes pain when in motion. To that point, it can cause the individual dealing with muscle pain to try and find various treatments to alleviate the pain and continue their lives. When it comes to pain can be relieved through treatments like chiropractic care and massage therapy to reduce the effects of the muscle pain associated with musculoskeletal disorders. The video above explains how treatments like chiropractic care incorporate different techniques to realign the body from subluxation and help stretch the tight, short muscles using manual manipulation and the MET technique.
Variations Of The MET Technique
When the muscles in the musculoskeletal system are dealing with pain in different locations or one location in the body, it can cause the individual to be in constant pain. Luckily treatments like chiropractic care are non-invasive and therapeutic as they utilize different techniques to realign the spine and stretch the tight muscle groups. In “Clinical Applications of Neuromuscular Techniques,” written by, Leon Chaitow, N.D., D.O., and Judith Walker DeLany, L.M.T., stated that when muscle pain affects tone muscle or causes structural changes to the joint’s ROM (range of motion) can lead to shortness and stress to the muscle group. Studies reveal that MET is a stretching technique therapists use to contract the affected muscle in a precisely controlled direction voluntarily. Many stretch variations of the MET technique allow the muscles to be stretched, strengthening and improving local circulation while mobilizing joint restriction. Down below are some of the variations of stretching techniques with MET.
Isometric Contraction: Reciprocal Inhibition In Acute Setting
The isometric contraction technique is used for reciprocal inhibition in an acute setting where the affected muscles are dealing with symptoms of muscle spasms. The isometric contraction allows the therapist to help relax acute muscular spasms and mobilize restricted joints while preparing the joints for manipulation.
Starting point: When acute muscles or joint problems affect the body’s functionality, therapists must commence an easy restriction barrier.
Modus Operandi: The affected muscles are used in an isometric contraction, allowing the short muscle to relax.
Forces: The therapist and individual forces are matched and involve 20% of the individual’s strength to increase no more than 50%.
Duration: Initially7-10 seconds while increasing up to 20 seconds.
Action following contraction: The area of the muscle and joint are taken to a new restricted barrier without stretching after complete relaxation. Therapists should perform the movement to a new restricted barrier on exhalation.
Repetitions: Repeat three to five times until no further gain in the range of motion is possible.
Isometric Contraction: Post-isometric Relaxation In Chronic Setting
The isometric contraction technique is used for post-isometric relaxation in a chronic setting where the muscles are severely contracted. The isometric contraction technique is known as post-facilitation stretching, where therapists stretch chronic or subacute restricted, fibrotic, contracted soft tissues or muscle tissues affected by myofascial trigger point pain.
Starting point: Short of resistance barrier
Modus Operandi: The affected muscles are used in the isometric contraction that allows the shortened muscles to relax and let an easier stretch.
Forces: Both the therapist and individual forces match and increase about 30% of the patient’s strength and increase to 50% of contractions up to 20 seconds.
Duration: Initially 7-10 seconds and increasing up to 20 seconds.
Action following contraction: The rest period is 5 seconds so the body can relax completely before being stretched, and during exhalation, the muscle goes through a painless, new restriction barrier position that is held for at least 10-60 seconds.
Repetitions: Repeat three to five times.
Isotonic Eccentric Contraction
The isotonic eccentric contraction is an isolytic technique to strengthen weak postural muscles that are tensed or tight from prolonged sitting or poor posture.
Starting point: At the restriction barrier
Modus Operandi: When the muscle is contracted and prevented, the therapist uses this technique to slowly overcome and reverse the contracting muscle so it can be stretched to full resting length.
Forces: Therapists use greater forces on the individual and build up subsequent contractions for the affected muscle (*Utilize this stretch on individuals who are not dealing with osteoporotic issues in their muscles and joints)
Duration: Five to seven seconds
Repetitions: Repeat three to five times if discomfort is not excessive.
Isokinetic
The isokinetic technique is a combination of isotonic and isometric contractions that many pain specialists like chiropractors and massage therapists use to tone weakened musculature, build strength in all the surrounding muscles that are involved in a particular joint function, and help train and balance the effects on the body’s muscle fibers.
Starting point: Easy mid-range position
Modus Operandi: The individual uses moderate resistance as the therapist puts the joint through a rapidly full range of movement as this technique is different than simple isotonic exercises, and resistance varies from each person. This technique progressively increases as the procedure progress.
Forces: The therapist uses moderate forces to prevent movement from the individual and then progresses to full forces.
Duration of contraction: Up to four seconds.
Conclusion
Different stretching techniques in MET therapy allow the affected muscles to be stretched and lengthened while reducing muscle pain affecting a body’s location. It is important to be mindful of the movements that can cause the muscles to be overstretched or cramped up, which can cause pain. Treatments incorporating these various stretching techniques allow the affected muscles to relax and restore naturally.
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Faqih, Anood I, et al. “Effects of Muscle Energy Technique on Pain, Range of Motion and Function in Patients with Post-Surgical Elbow Stiffness: A Randomized Controlled Trial.” Hong Kong Physiotherapy Journal : Official Publication of the Hong Kong Physiotherapy Association Limited = Wu Li Chih Liao, U.S. National Library of Medicine, June 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6467834/.
Gregory, Nicholas S, and Kathleen A Sluka. “Anatomical and Physiological Factors Contributing to Chronic Muscle Pain.” Current Topics in Behavioral Neurosciences, U.S. National Library of Medicine, 2014, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4294469/.
Mense, Siegfried. “The Pathogenesis of Muscle Pain.” Current Pain and Headache Reports, U.S. National Library of Medicine, Dec. 2003, https://pubmed.ncbi.nlm.nih.gov/14604500/.
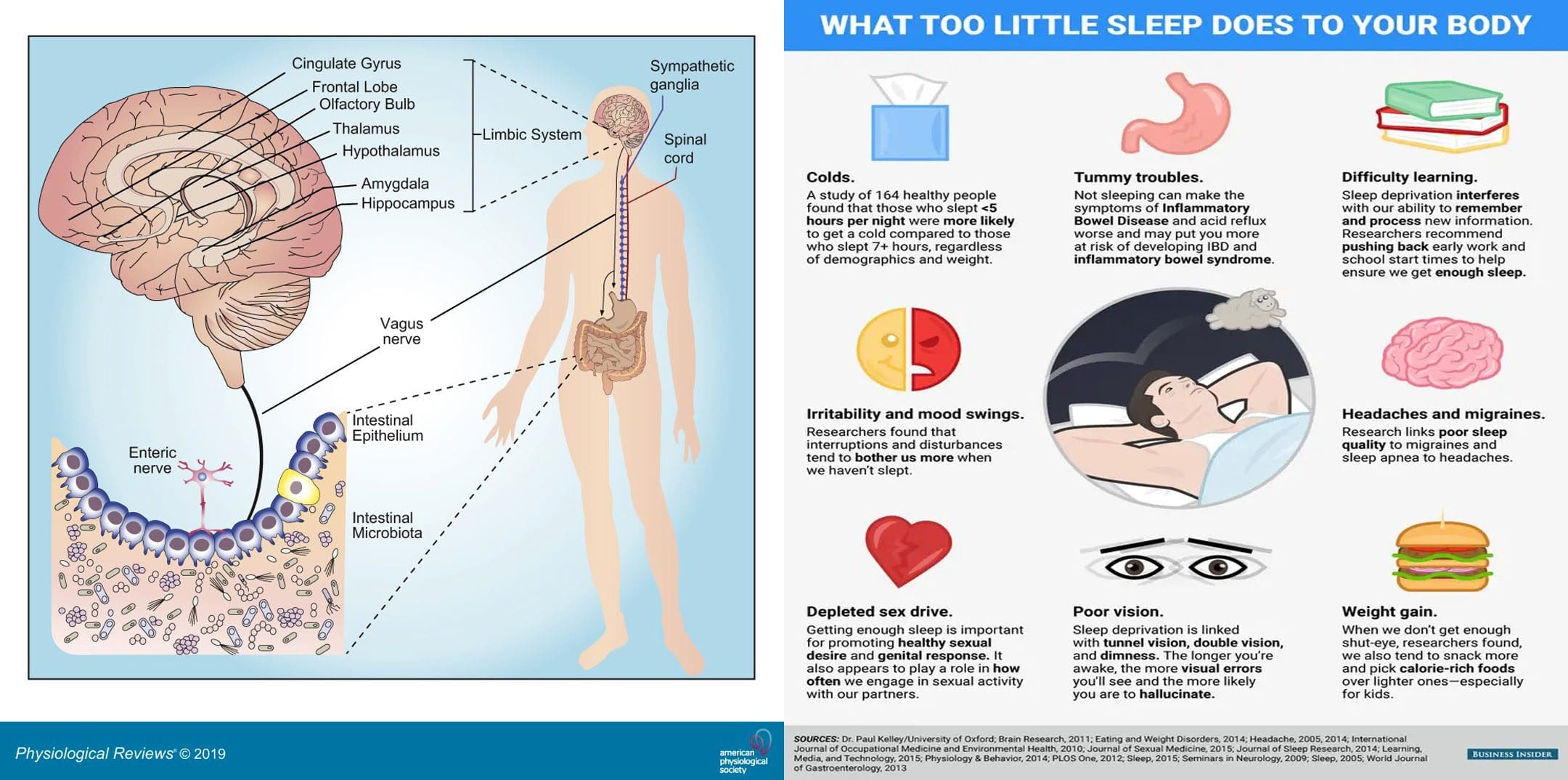
Viruses, bacteria, fungi, and protozoa are the microorganisms that naturally live in the digestive tract. Sleep affects gut health and vice versa. A healthy gut microbiota consists of all kinds of microorganisms that produce thousands of compounds and coexist harmoniously. A healthy diet and lifestyle are the biggest factors influencing bacteria variety, and maintaining a varied diet preserves microbiota diversity. Everybody’s gut microbiome is different; the more diverse the gut microbiome, the healthier sleep will be. The Injury Medical Chiropractic and Functional Medicine Clinic Team can develop a personalized nutritional plan to improve gut health and sleep patterns.
Sleep Affects Gut Health
Not having a diverse gut microbiome has been linked to autoimmune diseases, Parkinson’s disease, and mental health issues like anxiety and depression. Not getting healthy sleep is associated with many diseases and disorders, including:
Gastrointestinal disorders
Infections
Diabetes
Cardiovascular disease
Neurological disorders
Anxiety
Depression
Cancer
Changes in sleep patterns influence the central nervous system and the immune system, which affect different organ systems. For example, studies have shown some gastrointestinal disorders, like irritable bowel syndrome – IBS could be associated with increased REM sleep or the fourth part of the sleep cycle when vivid dreaming occurs. In Crohn’s disease or ulcerative colitis, long-term immune response activation can result in poor sleep, insufficient quality sleep, or other sleep problems. The deepest stages of sleep are when the brain and gut communicate to repair the body, restore nutrients, and remove and release toxins.
Sleep Cycle
During sleep, the immune system produces proteins called cytokines that perform functions during the inflammatory response, either by increasing or blocking inflammation, depending on the body’s needs. Cytokines help promote sleep, fight infection, or stop inflammation in chronic inflammatory diseases like Crohn’s disease or ulcerative colitis.
Insufficient sleep significantly alters cytokine production, and infection-fighting cells decrease in numbers when sleep deprived, making it harder for the body to fight infections and lessening protection. This increases the inflammatory response and keeps the immune system on.
Chronic or long-term immune response activation can result in sleep disturbances or disorders.
Some disorders include small intestinal bacterial overgrowth and inflammation caused by microbiome abnormalities or dysbiosis.
The gut barrier function begins to malfunction, leading to bacteria and pathogens leaking into blood circulation/leaky gut, triggering immune responses.
Ways to Improve Sleep
One of the main ways to improve sleep quality and gut microbiome health is to practice healthy sleep hygiene. According to the National Sleep Foundation, individuals should:
Nap Smart
Naps can be a great way to refresh the mind and body and replenish energy levels during the day.
The bright lights from phones and screens can make it difficult to fall asleep fully.
Use an alarm clock with a soft night light and keep the bedroom tech-free.
Create Sleep Routine
Take a warm shower, read a book, or do light stretches.
Create a wind-down routine to relax before bed to signal the body that it’s time for sleep.
Avoid Caffeine and Alcohol Before Bed
These substances make it harder for the mind and body to fall or stay asleep.
Food As Medicine
References
Chabé, Magali et al. “Gut Protozoa: Friends or Foes of the Human Gut Microbiota?.” Trends in parasitology vol. 33,12 (2017): 925-934. doi:10.1016/j.pt.2017.08.005
Deng, Feilong, et al. “The gut microbiome of healthy long-living people.” Aging vol. 11,2 (2019): 289-290. doi:10.18632/aging.101771
Gut Bacteria Research: Physicians’ Committee for Responsible Medicine. (2019). “Gut Bacteria: Optimize Gut Health With a Plant-Based Diet,”
Ianiro, Gianluca, et al. “How the gut parasitome affects human health.” Therapeutic advances in gastroenterology vol. 15 17562848221091524. 30 Apr. 2022, doi:10.1177/17562848221091524
Lozupone, Catherine A et al. “Diversity, stability and resilience of the human gut microbiota.” Nature vol. 489,7415 (2012): 220-30. doi:10.1038/nature11550
Sleep and Gut Microbiome Study: PLoS One. (2019). “Gut microbiome diversity is associated with sleep physiology in humans.
Sleep Hygiene Information: National Sleep Foundation. (2019). “Sleep Hygiene.”
Vaishnavi, C. “Translocation of gut flora and its role in sepsis.” Indian journal of medical microbiology vol. 31,4 (2013): 334-42. doi:10.4103/0255-0857.118870
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine