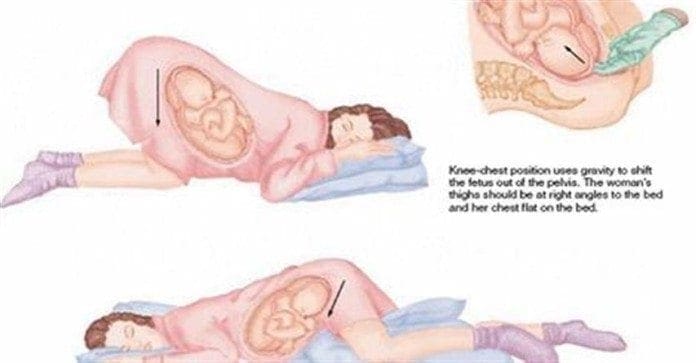
Sleeping Position: During pregnancy, you may find yourself tossing and turning, as best as you can, trying to�get comfortable before falling asleep. Unfortunately, regular�sleeping positions may no longer work during pregnancy.
There�are a number of reasons for this new discomfort, but there�are some sleeping positions that may help you get that much needed rest. When pregnant the body goes through a variety of changes. These changes tend to disrupt the peaceful sleep.
Here are a few suggestions that may not sound or look very comfortable, especially if you have a favorite sleeping position. This is often on your back or stomach. But you may find that they work. Keep in mind that you may do not have to stay in one position all night, rotating positions is completely acceptable and even encouraged.
What’s The Very Best Resting Place During Maternity Makeup Mania
Just How To Improve Rest Within The Second-Trimester Of Pregnancy
Greatest Placement In Sleeping During Pregnancy Data
Just How To Improve Rest Within The Second-Trimester Of Pregnancy
Rest Positions During Pregnancy
Greatest Sleeping Position During Pregnancy
Understand The Right Sleeping Place During Pregnancy
Greatest Sleeping Positions During Maternity Reverie
Sleeping Positions During Pregnancy Movies
Greatest Sleeping Jobs While Pregnant Fresh Health Consultant
Sleeping Positions During Maternity Superbaby
Which Sleeping Place Is The Greatest During Maternity
7 Essential Sleeping Guidelines During Third-Trimester
Sleeping Positions During Maternity Superbaby
Rest Learn To Keep Cozy Through Your Maternity
Rest Learn To Keep Cozy Through Your Maternity
7 Essential Sleeping Guidelines During Third-Trimester
Sleeping On Back Although Pregnant Could It Be Harmful
Greater Sleeping Positions During Pregnancy Workout
Sleep is the one time your body has during the day to repair and maintain its cells and systems.
It’s also essential for flushing out toxins and clearing away dead cells. Experts recommend between 7-9 hours of sleep a night.
Because sleep is so important, if there’s something that’s keeping you from getting comfortable and sleeping through the night, it helps to know what adjustments you can make to get the rest you need.
Following are some recommendations to help you find the best sleeping position to deal with your common aches and pains.
Finding Your Best Sleeping Position
These sleeping positions will make you feel like a brand new person every morning!
1. Best Sleeping Position for Lower Back Pain
Many people suffer from back pain. It’s often difficult to find a comfortable sleeping position when your back hurts. What you may need is a little support. The best sleeping position for back pain is lying on your back. Place a pillow under your knees and a rolled-up towel at the base of your back where it curves. This will relieve pressure on your lower back while adding support (1).
For those with back pain, alignment of the ear, shoulder, and hip is the most important part of sleep posture, so make sure to keep your spine aligned.
The University of Rochester Medical Center offers the following suggestions for a solid sleep without back pain, whatever the position (2):
Sleeping on your stomach can create stress on the back because the spine can be put out of position. Placing a flat pillow under the stomach and pelvis area can help to keep the spine in better alignment. If you sleep on your stomach, a pillow for your head should be flat, or sleep without a pillow.
If you sleep on your side, a firm pillow between your knees will prevent your upper leg from pulling your spine out of alignment and reduce stress on your hips and lower back. Pull your knees up slightly toward your chest. The pillow for your head should keep your spine straight. A rolled towel or small pillow under your waist may also help support your spine.
Insert pillows into gaps between your body and the mattress.
When turning in bed, remember not to twist or bend at the waist but to move your entire body as one unit. Keep your belly pulled in and tightened, and bend your knees toward the chest when you roll.
2. For Shoulder Pain
It may seem obvious but if one of your shoulders hurt, don’t add pressure by lying on it. Lie on your other side with your knees and arms bent. Place one pillow between your knees and another between your elbows so it touches your chest.
If both shoulders hurt, lie on your back with your arms by your sides.
3. For Sinus Issues
Congestion from a cold or allergies can get worse when you sleep, as gravity is working against you when you’re lying down. Prop up your head and shoulders with pillows while lying on your back so your sinuses can drain more easily into the back of your throat (3).
4. For Headaches
Sometimes a bad sleeping position can actually cause a headache by constricting muscles and nerves while you sleep. To keep your head in a neutral position, lie on your back and put a pillow or rolled-up towel on both sides of your head to keep it from wrenching during the night (4).
5. For Menstrual Pain
Cramps and bloating can make sleep difficult before and during your period. The best sleeping position for cramps is to lie on your back and place a pillow under your knees to take pressure off your abdomen and back. You can try applying a hot water bottle or heating pad to your abdomen and/or back when you go to bed to ease cramps and make you comfortable enough to fall asleep. (5)
6. For High Blood Pressure
There is a correlation between sleep and hypertension: sleep deprivation and disrupted sleep exacerbates the problem. The autonomous nervous system changes during sleep and that can affect blood pressure. (6) The worst position for sleep if you have high blood pressure is on your back. (7)
A Japanese study on the effect of sleep position found that blood pressure was reduced significantly when lying in the prone position (face down) as compared to lying on the back. (8) Lying on your stomach, however, can lead to back, neck, and joint pain and difficulty breathing, so you should alternate between positions every few nights. (9) Sleeping on your right side can ease pressure on the heart (which is on your left), lowering blood pressure. (10)
7. For Heartburn
If you have GERD (gastroesophageal reflux disease), indigestion, or heartburn, sleeping on your left side may help. This is the best sleeping position to take pressure off the stomach and esophagus (12).
8. For Poor Digestion
If you have digestive issues, placing a pillow between your legs while sleeping on your left side will take a further strain off your digestive system to allow things to flow freely while you sleep. It’s also important to wait a few hours after your last meal before hitting the hay to make sure you don’t get indigestion.
9. For Neck Pain
Supporting the neck is key, whatever position you sleep in. On your back or side are easiest on your neck. (11) If you sleep on your back, roll up a small towel (or neck roll) and stick it inside your pillowcase with your pillow, adjusting the towel so it’s just under the curve of your neck. Your head should rest comfortably on your pillow. There are also special funny-looking pillows designed specifically for neck support.
Harvard Medical School has the following additional suggestions for getting rid of that pain in the neck (12):
Try using a feather pillow, which easily conforms to the shape of the neck. Feather pillows will collapse over time, however, and should be replaced every year or so.
Another option is a traditionally shaped pillow with “memory foam” that conforms to the contour of your head and neck. Some cervical pillows are also made with memory foam. Manufacturers of memory-foam pillows claim they help foster proper spinal alignment.
Avoid using too high or stiff a pillow, which keeps the neck flexed overnight and can result in morning pain and stiffness.
If you sleep on your side, keep your spine straight by using a pillow that is higher under your neck than your head.
When you are riding on a plane, train, or car, or even just reclining to watch TV, a horseshoe-shaped pillow can support your neck and prevent your head from dropping to one side if you doze. If the pillow is too large behind the neck, however, it will force your head forward.
For Your Brain
Parting Thoughts
While we sleep, our brains are as active as when we’re awake—and it’s not just conjuring dreams, it’s cleaning house. Brain waste is processed and eliminated during sleep.
Most animals (humans included) sleep on their sides. A study published in the Journal of Neuroscience looked into why this might be. Researchers observed activities in the brain for prone (stomach), supine (back), and lateral (side) sleep positions. They found that cerebrospinal fluid that gets flushed around the brain to clear toxins is more efficient when in a lateral sleeping position. (13) The brain is, therefore, better able to eliminate waste and prevent the plaque build-up that can lead to neurodegenerative diseases like Alzheimer’s.
The best advice is to sleep however is most comfortable for you. Regular adequate sleep is crucial for all the body’s functions. Dreams are a bonus.
Older people newly prescribed sleeping pills like benzodiazepines and �Z-drugs� have over double the odds of a hip fracture in the first two weeks, scientists have found.
Experts have said there is a 53 per cent increase in risk for people taking the medication for more than two weeks.
Sleeping tablets are prescribed if people suffer severe insomnia or as a short term measure to ease symptoms of insomnia.
However, experts have warned of the dangers of the drugs as they can cause side effects – such as drowsiness the following morning, which can lead to falls.
Users can also become dependent on them.
NHS Choices said: �Doctors are usually reluctant to recommend sleeping tablets in the long-term because they just mask the symptoms without treating the underlying cause.�
The results come from a new study by researchers at Cardiff University and King�s College London.
�While �Z-drugs are fast becoming the doctor�s hypnotic prescription of choice, there is no evidence that they are a safer alternative to benzodiazepines in relation to hip fracture risk,� said Dr Ben Carter, Cardiff University�s School of Medicine and the Institute of Psychiatry, Psychology and Neuroscience, King�s College London.
�Our study shows that both appear to significantly increase the risk of hip fracture when newly prescribed by doctors.�
A study of people aged over 65 found that new users of these hypnotic medicines experienced nearly two and a half times the fracture rate, when compared with older people not taking hypnotics.
An estimated 53 per cent increase in fracture risk was identified in medium-term users – 15 to 30 days, as well as a 20 per cent increased risk of hip fracture in long-term users which scientists classed as greater than 30 days.
Dr Carter added: �Careful consideration of the immediate increased risk of hip fracture should inform the clinical decision-making process.
�Clinically effective measures like strength training to improve frailty, removal of hazards at home, visual correction and a medication review are also needed to mitigate the risk of hip fractures, particularly in the first few days of use.�
The research supports previous studies linking use of hypnotics by older people with an increased risk of accidents, dependence, cognitive decline and hip fracture.
The drugs are also thought to cause drowsiness, delayed reaction times and impaired balance.
The study, called Benzodiazepines, Z-drugs and the risk of hip fracture: A Systematic Review and Meta-Analysis has been published in the journal PLOS ONE.
If you suspect you have a damaged gut, what can you do to fix it? (Of course you should see your doctor and get a proper diagnosis, and talk to him about your issues.) First, remember that if your gut is damaged you probably aren’t absorbing the nutrients from your food – even if you’re eating GREAT food! Switching cold turkey to a diet of salads and raw veggies isn’t even always the answer for healing your gut. Some raw veggies are actually really hard for a damaged gut to digest.
El Paso, TX. Chiropractor Dr. Alex Jimenez adds to the discussion of chiropractic treatment vs. pain medication and medical care.
Which Is More Effective For Low Back Pain? Meds Or Chiropractic?
That is the�question in our research theme of the week.
A Practice-Based Study of Patients with Acute and Chronic Low Back Pain Attending Primary Care and Chiropractic Physicians: Two-Week to 48-Month Follow Up
This study based used a practice-based, observational model to look at the effectiveness of intervention in a selected group of patients with both acute and chronic lower back pain (LBP). It compared the efficacy of chiropractic intervention with standard medical care in both kinds of Low Back Pain.
2780 patients were enrolled in the research over a 2-year period (1994 to 1996) from the practices of 60 DCs (1855 patients) and 111 MDs (925 patients) in 51 chiropractic and 14 general practice clinics. Patient data was obtained via a survey distributed in person at the first visit, and the patients were followed up over a period of 4 years with 7 mailed surveys at regular time intervals. Mailings were sent at 2 weeks, 1 month, 3 months, 6 months, and 1 year following the original visit. In phase 2, patients were followed up at 36 24, and 48 months.
Patients were eligible if LBP was their primary grievance, and was of mechanical source; they were excluded if exploitation was contraindicated, or the back pain was of nonmechanical origin (such as from organic referred pain). Acute patients were those whose back pain was of less than 7 weeks duration; long-term back pain patients were those whose back pain was longer or of 7 weeks duration.
The physicians in the research produced an assortment of treatment procedures. Chiropractic care included physical therapy, spinal manipulation, an exercise strategy, and self-care education. Medical doctors gave care that included an exercise plan prescription drugs, and self-care advice; nearly 25% of these patients were referred for physical therapy.
The primary outcomes measured were present pain severity, and functional impairment, which were quantified by questionnaires sent to the patients in the above stated times.
The medical patients showed more severe baseline pain and disability when entering treatment, greater prevalence of pain and poorer general health status, than in patients. These differences were more conspicuous in the chronic patients than in the acute patients.
An edge was seen for DC attention in comparison with MD attention for the first 12 months in pain relief. This difference was small but was greater for those with chronic LBP during the first year of treatment.
There was an advantage with all the usage of chiropractic care in long-term patients with pain radiating below the knee, and some small advantages were also seen in the acute patient group. Differences were also seen through the first 3 months of care with no leg pain in chronic patients. There were the 2 kinds of medical care for pain radiating over the knee as well as no differences in the 2 groups.
All patient groups found clinically important improvement in pain and disability over the span of treatment. Advancement that was greater was seen by acute patients, with many obtaining near complete relief of their symptoms. Most realized symptom relief by 3 months, followed by a plateau through 12 months. It was followed by critical, clinical aggravation of pain at 12 to 24 months, with another plateau until 4 years. Little upsurge in impairment was seen between 12 and 48 months.
Of note, at 3 years into the research, 45% to 75% of patients noted at least 30 days of pain throughout the prior year, even in those who had gained significant pain and disability relief through early intervention. Daily pain was noted by 19% to 27% of chronic LBP patients throughout the preceding year.
Early intervention reduces chronic pain. People who received early intervention for acute lower back pain after the original injury, reported fewer days of back pain than those who waited more for intervention. Since outcomes were better than in those who delayed treatment this would support providing early intervention for patients with acute back pain.
Chiropractic is valuable for certain types of pain. Chiropractic care�was shown to be�more effective�than standard medical care in certain situations: with pain radiating below the knee in patients with persistent lower back pain, as well as for treating LBP during the first 12 months. Nearly all the relief was sustained throughout the initial year, and was obtained during the first 3 months of treatment.
This study reports pain and disability results up to 4 years for chiropractic and medical patients with low back pain (LBP) and evaluates the impact of physician kind and pain length on clinical outcomes.
Conclusion
Study findings were consistent with systematic reviews of the efficacy of spinal manipulation (the Chiropractic adjustment) for pain and disability in severe and chronic LBP. Interdisciplinary referral and patient selection needs to be prime concerns by policymakers, physicians, and third-party payers in identifying health services.
El Paso, TX. Chiropractor Dr. Alex Jimenez looks at sleep posture for back pain.
Whether you got back, neck, or pregnancy pain, your slumber posture makes a big difference in the way you feel each morning.
Great posture is a key to a healthier spine, but posture isn�t just about sitting or standing straight. Your sleep bearing has a significant effect on neck and your back. While some postures allow you to feel refreshed morning, come, others can leave you stiff, sore, and in pain.
Believe neutral, as it pertains to locating the very best sleep pose to your back and neck. Postures that put your spine in a neutral, or direct, alignment place the smallest amount of pressure on your own back and neck. Learn which postures set your back in a neutral state and those who must be prevented below.
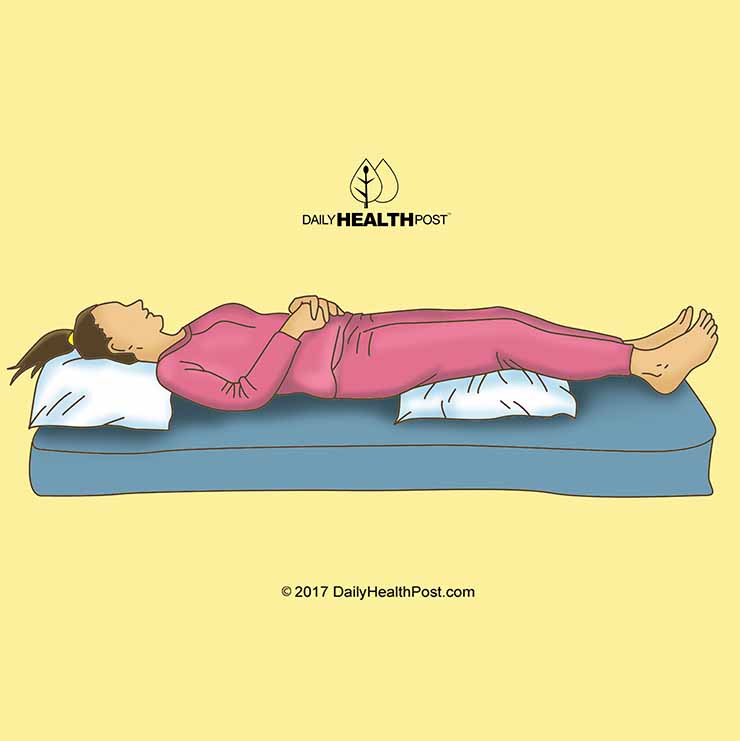
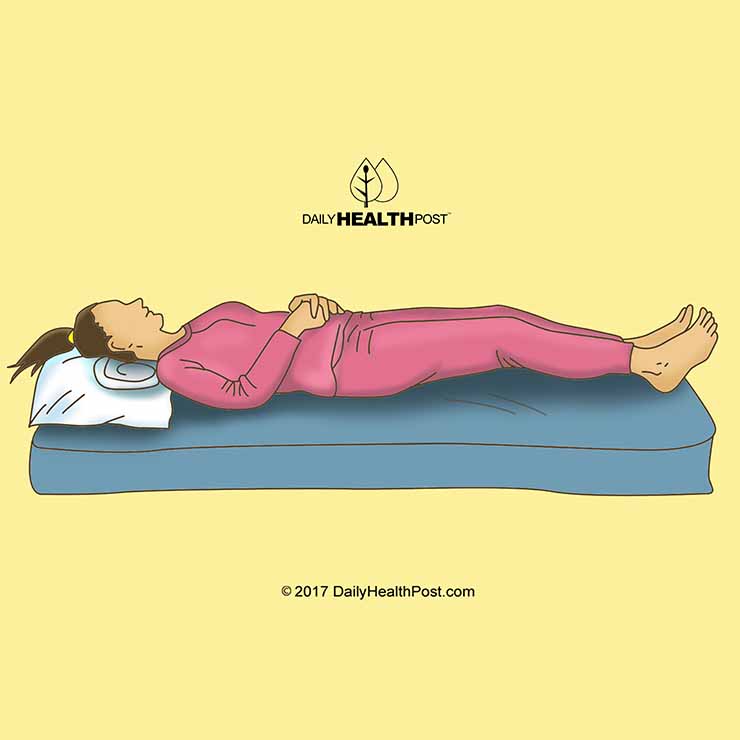
The Very Best Sleep Posture For The Back: On Your Own Back
Sleeping in your back is for putting your spine in a neutral alignment, the very best, but only 8% of people sleep in this pose.
A few strategically placed pillows can boost the advantages of back sleep. A little pillow underneath your head and neck (but not your shoulders) will help to keep your back straight. Including a pillow under your knees will provide comfort and much more support, as it encourages your back to preserve its natural curve.
It’s a few drawbacks, though back sleeping is the best on your spine:
It�s not best for individuals with sleep apnea. Back sleeping may create the tongue to obstruct the breathing tube, so those with sleep apnea must not sleep on their backs. Instead, they ought to sleep on their side with legs right.
It�s not best for snorers. Back sleeping can worsen snoring. People who snore should sleep on their side with legs right.
It’s not best for women that are pregnant. Pregnant women who sleep on their backs danger growing a multitude of health issues, from back pain to low blood pressure. Plus, the on-the-back position decreases blood flow to the baby and also the heart. The very best sleep position during pregnancy is sleeping on the side with legs bent.
�
The Next Best Choice: On Your Side With Legs�Straight
For those that snore or have sleep apnea�or in the event you just discover sleeping on your back uncomfortable�side sleeping with your torso and legs is a fantastic choice. That is the perfect sleeping pose for people and snorers with sleep apnea because it keeps your airways open. Adding a tiny pillow between your legs will also help in keeping your back neutral.
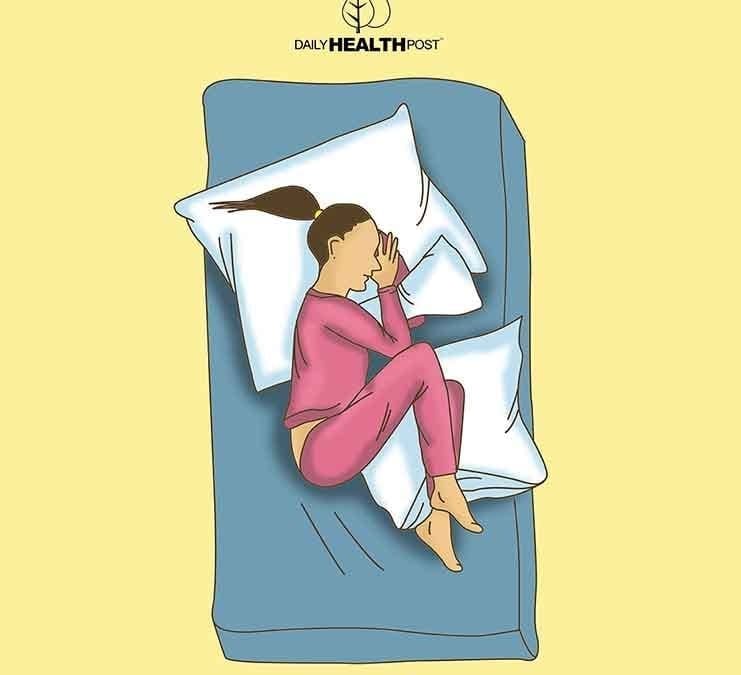
In Third: On Your Side With Legs Bent Upwards
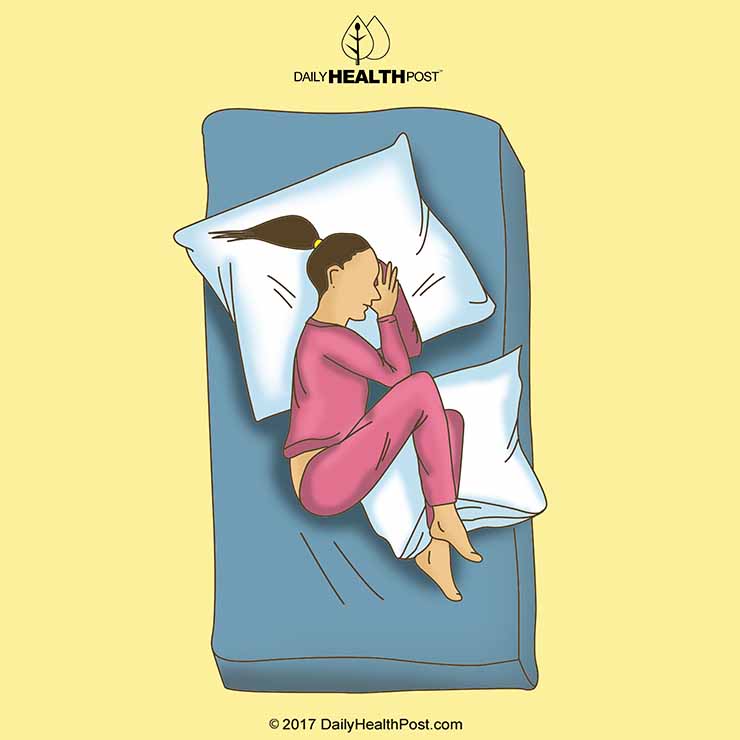
Sleeping on your side together with your legs bent upwards�also generally known as the fetal position�is the most typical sleep pose (41% of adults sleep this manner). This posture keeps your neck and upper back, though it�s a popular alternative. The fetal position also promotes an uneven distribution of weight, which can cause tender joints and back pain. You can help reduce your odds of waking up by pulling your knees and maintaining your turning angle up as high as they can go.
While this is the third-best slumber pose for most, sleeping on your side with bent legs is the best sleeping position for women that are pregnant. It supplies the most comfort and safety for a growing abdomen, and sleeping on the left side adds the additional benefits of boosting blood and nutrients to the baby. For additional support, pregnant women may put in a pillow between their bent legs and knees.
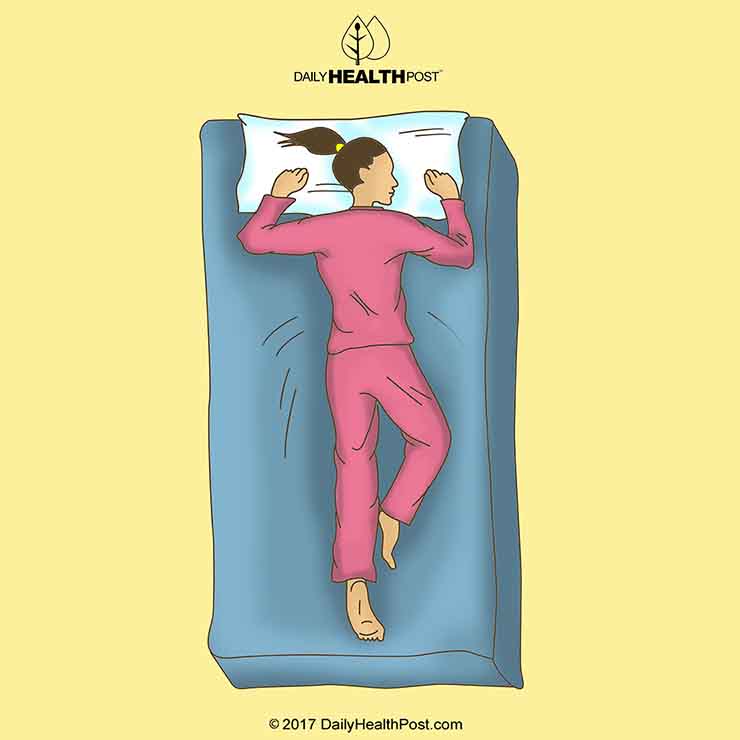
The One Sleep Position Everyone Should�Avoid
No matter the sort of pain you might have, whether it�s neck, low back, joint, or related to pregnancy, sleeping on your stomach just isn’t recommended. This posture places the most pressure on joints and your back�s muscles as it flattens the natural curve of your back. Sleeping on your stomach also compels you to turn your neck, which may cause neck and upper back pain.
Getting the sleep you need is much more important while stomach sleeping is better prevented. You are able to calm some pressure off your back by placing a pillow under your pelvis and lower abdomen, and another pillow under your head if stomach sleeping is the sole way you can snooze soundly. In the event the pillow under your head causes pain, remove.
Still Feeling Sleepy?
You struggling to get a great night�s rest, although when you yourself have sleep bearing that is healthful, factors outside your sleep position may be the offender. As an example, environmental disruptions (for example bright lights in your bedroom) or dietary customs (like eating a substantial meal before bed) could be interfering together with your slumber. Learn about some common sleep burglars and how you can combat them in Sensible Sleep Advice to get a Wholesome Spine.
El Paso, TX. Chiropractor Dr. Alex Jimenez takes a look at the psoas muscle and its relation to back pain.
All too often we find ourselves experiencing aches and pains in our bodies, especially in the low back. If you find yourself commonly searching for remedies for fast back pain relief, it might be time to research the psoas muscle.
Technically named iliopsoas, the psoas major, may very well be among the main muscles within the body. Why? This deep-seated heart muscle helps support your back and much more. In the event the psoas is weak, it might be the cause of neck pain, back pain and many other issues. In fact, the psoas major muscle is especially distinctive, particularly as it pertains to postural function. It�s the only muscle which joins reduced body and the lumbar spine. It�s clear to see taking care of this deep psoas muscle is essential to a powerful, pain free body. Many others believe a healthy psoas is very important for spiritual and mental health, also.
What’s the Psoas Muscle? Why Is It Important?
There are two psoas muscles on each side of the back. The larger one is called the psoas major and the smaller the psoas minor. The psoas major, often known as �the might psoas, � originates in the back round the bottom of the rib cage and runs down the thigh over the femur. The psoas major works by bending the hip. It runs to the bony pelvis, although the psoas minor also originates in the back across the bottom of the rib cage. It acts to bend the back that is reduced.
The psoas helps us perform including freeing the legs for walking and running all sorts of day-to-day activities. The psoas muscle is also critical in providing good posture. Anyone who takes Pilates knows the psoas intimately � the type of exercise is praised for enhancing psoas muscle health and associated back pain. Olympic weightlifters, runners, triathletes, gymnasts � heavily rely on the support of the psoas, too.
Let�s delve into where the muscle is situated. There are two muscles that create what is called the group that is iliopsoas. They may be the psoas major and iliacus. You have likely learned your fitness teacher indicate stretching the hip flexors at the end of your strength class. The psoas major and iliacus are very important to the hip flexor muscles since they help support and secure the lower back. There’s an alternative muscle known as the psoas minor, but it is useful for 4 legged animals than for people.
The word psoas means loin area and is Greek. The psoas muscle group makes an upside down V, linked to the back working its way down to the very top of the femur and beginning at about the bottom point of the rib cage. Specifically, it’s a long spindle-like muscle, found between the pelvic inlet as well as the pelvic floor. It joins the iliacus muscle which can be what forms the iliopsoas. A chiropractor can in fact use pressure in the pelvic inlet region to aid release a tight psoas. This can be commonly done to stretches for athletes in addition, though it should always be achieved by way of a soft tissue professional with expertise in psoas release.
Why Do We Need A Strong Psoas Muscle: Possible Issues
A strong psoas supports regular action, however so much as the simplest task can be made as well as causing larger problems such as power back a challenge by a weak psoas. The psoas is a vital messenger of the central nervous system and the way your body reacts to gravity is significantly diffent than intended, when there is dearth of support from it.
Muscle imbalances can often make the entire body to compensate in a different place and that may cause even and added problems harm. Some people are even identified as having psoas syndrome or iliopsoas tendonitis. These ailments cause pain in the hip area. They’re often described similarly, while these are two different illnesses; nonetheless, psoas syndrome is a condition involving a stretch, tear or rupture of tendon or the iliopsoas muscle. Iliopsoas tendonitis demands an inflamed muscle. The piriformis syndrome is also closely related with this kind of pain and may be referenced when seeking a diagnosis.
Yoga therapist Danielle Prohom Olson calls the psoas muscle �the muscle of the soul.� Olson says on her site: � The psoas is connected to the diaphragm through fascia or connective tissue which impacts our breath and anxiety reflex. This is because the psoas is linked to the most early inside part of the brain stem, the reptilian brain and spinal cord.� In fact, author of The Psoas Book, psoas specialist Liz Koch, says that lack or mental trauma of psychological support can leak to a chronically contracted psoas. This results in too little core awareness. This makes sense as your historical limbic system is closely related to emotions like fear and worry.
�
Symptoms Of Psoas Difficulties
Discomfort, pain and aches in the front hip socket
Restriction�in the hip socket
Iliopsoas bursitis/tendinitis
Restriction moving the thigh backwards
Deep pelvic pain
Deep �bellyache�
Chronic constipation
Twisted�pelvis
What Causes A Weak Psoas
There are just two common behaviours that generally cause a weak psoas: sitting poor posture and all day. The National Association of Sports Medicine notes sitting causes a psoas that is feeble. And a weak psoas can lead to lower back issues. All that sitting can cause the psoas, iliopsoas and rectus femoris to remain in a shortened position for lengthy amounts of time. What goes on is these muscles get used to this shortened state and that makes them overactive and tight. This shortening or tightening of the muscles can lead to a forward tilt of the pelvis and weakness in the gluteal muscles because these muscles are attached to the pelvis and lumbar spine. United, this may cause lower back pain. Consider a standing desk to lower your sitting time each day.
If not corrected awful posture, whether standing or sitting, can create a lot of suffering. Rounded shoulders or a forward head position might appear to be the easiest on the body, but it is going to weaken the supporting muscles of the body over time, since we’re always working against gravity.
3 Major Benefits of a Strong, Healthy Psoas Muscle
1. May Reduce Low Back Pain
A published in the Journal of American Osteopathic Association identified the psoas as a vital muscle linked to our core muscle development. The psoas had been initially missed as an alternative for back pain that the 48-year-old man was experiencing. (7) He received osteopathic manipulative treatment, defined as hands on care with a trained physician. Utilizing the hands, with extending techniques, gentle pressure and resistance by transferring the muscles and joints, a skilled professional can help diagnose, treat and even prevent illness or injury. The patient enjoyed critical development, confirming that without surgery, back pain can be removed with a the help of a professional, combined with the devotion of the patient to execute special stretches at home.
2. Can Affect Your Sports Activities
I noted previously that the psoas is actually the muscle which allows one to run. Each knee lift causes a contraction of the rope-like each time the leg swings back to its first location and muscle, the psoas will lengthen. Runner�s World reports a runner lengthen and will contract the psoas more than 5,000 times during an hour long run The psoas can be a big aspect in great carriage. The psoas, combined with other core muscles, like the abdominals and obliques, in addition to the ones that help form and support the lower back, supplies firmness offering a strong posture. Therefore it’s wise that if there is a problem with the psoas, it’ll probably change your sports actions, in particular those that need jogging.
3. Provides a More Pain-Free Pregnancy
Creates a lot of developments in the torso, certainly one of which is the shift in your center of gravity. It shifts forwards as the baby grows, causing the pelvis to go toward the front of the body. This could cause the muscles in the low back area the hamstrings and glutes and also to tighten weaken as well as to stretch out. Additionally, the ligaments connected to the uterus can come under a great deal of anxiety, causing pain and lower back. The psoas and surrounding muscles take on much of the anxiety, which may cause discomfort on account of imbalances and tightness. But, by performing stretches and exercises which help to fortify the psoas, you can remove most if not all of the pain.
Psoas Stretches & Exercises
Whether an athlete, not lively in any respect or pregnant, it�s important to release the psoas to make sure that it’s in excellent working order giving you the support you must perform any tasks � picking up those markets or your toddler. Yoga, Pilates and my core routine are excellent choices, by performing a some key stretches right at home however you can make a major difference. Here are some psoas stretches and exercises which you can do a few days a week. If possible, in the event that you sit at a desk throughout the day, I recommend which you perform these exercises daily. It just requires a couple of minutes and can alter how you go throughout your day.
Foam Rolling
While releasing the psoas must be left to your soft-tissue professional, NASM suggests foam rolling tight hip muscles that are other, such as the TFL and hip adductors. As you roll, hold on spots that are tender for 30 to 90 seconds. (16) Check by means of your physician to be sure foam rolling is OK with you. NASM notes it�s not appropriate for certain states, including aneurysms, blood clots, malignancies, anticoagulant treatment, congestive heart failure, open wounds or skin lesions, bursitis, obstructive edema, or certain other health conditions.
Hip Flexor Stretch (Thomas Stretch)
Sit tall at the end of a table. Thighs are midway off the table. Catching one knee, lean back until your lower back and sacrum and pull it to your torso are level on the table. Notice that when the back is rounding and the pelvis is tipping, you�re pulling on the knee too much. To correct, just loosen your hold. Allow the other leg to hang free. Hold for 30 to 60 seconds. Perform a few repeats on each side.
Kneeling Lunge
It is a very common exercise performed in the fitness center through the stretch segment of plenty of group fitness classes. To get it done, kneel down on one knee (you might want to have a pad below if you’re on a hard surfaced floor), with all the front leg forward at a 90-degree angle. Tuck your pelvis and softly lunge forwards. Continue to lean into the stretch ensuring that there is no uncommon pain. A tight psoas may cause you to arch your back; yet, try to keep the back straight. To include a little extending to the core, raise your arms and lean the hips forward another inch or two. Holding the lunge for 30 seconds finishing, 3 repeats on each side.
Leg Lifts
Lie on your back and extend your legs facing you. Put your hands either underneath your bottom in case your back arches too much, or above your mind by focusing on bringing your belly button to the spinal column provided that your lower back is pressed into the ground. Lift your left leg several inches above the earth and support for 3 to 5 seconds. Do 10 to 15 repetitions on each leg. As you get stronger, you can do these using ankle weights.
Ball Bridge
Lie on a stability ball like you would to perform crunching, along with your neck and shoulder resting. Make sure to engage your heart , not let your hips sag, with your feet straight ahead with toes pointing forwards, shoulder-width apart. Slowly and controlled, drop your glutes toward the floor (don�t go too far that the shoulders come away from the ball) and then push up through the heels to engage the glutes and push your hips back up in line by means of your spine.
This exercise can be used to fortify weak gluteal muscles generally associated with a tight psoas.
Psoas Massage and Release
The psoas is surrounded by vital organs is deeply embedded into the central cavity region and may be tough to find. Physical therapist or a chiropractor might be capable of help you best as it pertains to actually release the psoas. It requires complete relaxation of the patient and is a sensitive place. To really get working with a trained professional is recommended, although total body massage that is general can certainly help.
Working on releases and extending other hip muscles nearer to the surface of the body is able to go a long way in reducing total tension and will ultimately help in enhancing psoas wellness.
Precautions
It is always better to require any new exercise slow. Ahead of performing the exercises consult with your sports medicine doctor, physical therapist or chiropractor. When it comes to a psoas release, there are negative effects that are potentially dangerous in case you don�t work with someone trained and certified in this region, so you need to talk a professional.
Closing Thoughts on the Powerful Psoas Muscle
The psoas muscle is a deep-seated abdominal muscle in close proximately. Your psoas major is the muscle that joins your lower back to your lower body. The psoas muscle is many times tight and overactive, as well as other hip muscles, due and due to things like sitting that is persistent possibly as a result of chronic stress. A soft tissue professional just like a physical therapist or chiropractor should does releasing your psoas muscle. Everything you could do to boost your psoas function in the home is focus on strengthening weak gluteal muscles, extend them and perform foam rolling of other tight hip muscles such as TFL and the adductors.
While surgery is frequently prescribed for back pain, researchers are finding that focusing on enhancing psoas health can radically enhance lower back pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine