by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Chiropractic, Functional Medicine, Health
The Neural Zoomer Plus is a blood test that is designed to test 48 neurological antigens. When testing for these antigens, the results these markers find can help physicians determine if a patient is at risk for neurological conditions later on. To view last week’s article containing a full list of the signs and 48 markers, click here.�
When a patient comes to us with concerns, we listen very intently and make sure our patient’s concerns are addressed. More often than not, patients reveal they are having issues that relate to neurological declines, such as, muscle spasms or memory loss. With symptoms like these, the patient is referred to get a Neural Zoomer Plus.�
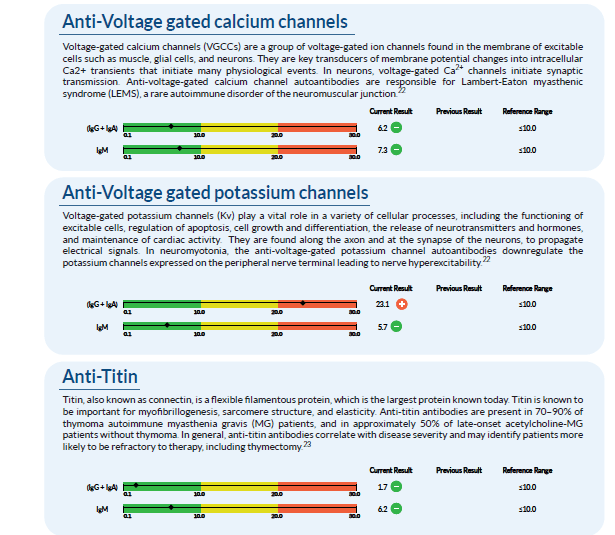
Once we receive the results back, it is compiled into a large report. From here, we assess it and go through all of the markers with an additional team of clinicians. An example of a few of the markers tested in a Neural Zoomer Plus is below. One can see that this patient has an elevated �Anti-Voltage gated potassium channel�. Anti- Voltage-gated potassium channels are responsible for multiple cellular processes such as cell growth and differentiation.�
After analyzing the data, we take these findings and create a treatment protocol that is specific to each patient and their lifestyle. Due to the fact that this patient shows an elevation in specific markers, there are certain adjustments we make in order to help prevent or reverse the cognitive and physical effects of neurological disorders.�
The first step we take is to change the diet of the patient. Many foods are not properly digested, leading to gut inflammation, which further leads to �leaky gut� which then enters the bloodstream and into the blood-brain barrier, causing neurological decline. In order to reverse these effects, we want to make sure the gut is getting the proper nutrients from foods that will not cause inflammation. For this patient, we recommend the Wahls Protocol.�
The second step we take is to usually get the patient involved in a more active lifestyle. By having this patient start to exercise with activities like yoga, it can improve the state of mind and their mind-body connection.�
The third step is usually nutraceuticals. These are supplements that will naturally help the body and brain with no addictive or harsh chemicals. With every patient, the nutraceuticals and amount needed vary depending on their specific body. For this case, we recommend:��
N-acetyl-L-cysteine:� (NAC) is a precursor to glutathione, the body�s most important cellular�antioxidant. NAC supplements have been shown to increase cellular glutathione levels.
Vitamins B12, B6, and folate: These are metabolic cofactors important for cellular metabolism and maintenance of all tissue cell types, but particularly important to nerve cells. Deficiencies in�B12 or folate can raise homocysteine levels, which have been associated with a higher risk for�vascular disease and dementia.
Alpha Lipoic Acid:� (ALA) is an essential cofactor in normal cellular metabolism and cellular�energy production.
Vitamin C and vitamin E: Can reverse symptoms caused by vitamin C and E�deficiencies.
As mentioned before, each patient is different and their lab work shows varying needs. However, with the Neural Zoomer Plus, we are able to get ahold of these symptoms, create a personalized treatment plan, and get them under control.�
As one can see, the data and knowledge we gain from these tests are truly eye-opening and give us an early advantage to help reverse or aid in prevention methods. We take the needs and concerns of every patient very seriously and work extremely hard to figure out the right method of treatment for them. Our goal is to help ensure that this lifestyle change is as smooth and easy on the patient as possible so they can get back to enjoying the activities they love and spending time with loved ones. The transition into a new lifestyle can be stressful, but with the information we gain from the tests, the knowledge we use from the doctor, and the willingness to change from the patient, we are set up to be the best team you can have to get your life back! – Kenna Vaughn, Senior Health Coach�

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Chiropractic, Functional Medicine, Nerve Injury, Wellness
When we look at our patients, we try to figure out what is causing their ailments from living their best lives. Some practitioners would prescribe medications to alleviate pain. While other practitioners will start trying to figure out what is causing the patient to have these ailments. Here at Injury Medical Clinic, we talk to our patients about the importance of functional medicine and how it can benefit them. In this article, we will be discussing Connective Tissue Disorder and how it is linked to wheat-related disorders.
What is Connective Tissue Disorder?
CTD (Connective Tissue Disorder) is an autoimmune disorder that can affect the connective tissues such as the collagen and elastin in our skins. This disease is highly inflammatory and can occur alongside with other autoimmune diseases, and it is common if families have a history of Connective Tissue Disorder.

About 3% of the population has a connective tissue disorder, and it is most likely to occur in women than men. In fact, women who are diagnosed with connective tissue disorder have a ration of 10:1, compared to men.
CTD includes (but is not limited to) the following conditions:
- Systemic Lupus Erythematosus (SLE): SLE is a widespread and chronic autoimmune condition, for unknown reasons, can cause the immune system to attack the body�s own tissue and organs, including joints, kidneys, heart, lungs, brain, blood, and skin.
- Sjogren�s Syndrome: This autoimmune disease causes white blood cells to attack moisture-producing glands, such as the tear ducts and salivary glands. This can make it very difficult for the body to produce tears and saliva.
- Systemic sclerosis (scleroderma): This condition causes the skin and connective tissue to harden and tighten.
- Rheumatoid arthritis (RA): RA is a chronic inflammatory condition and an autoimmune disorder that can generally affect the lining of the joints, but mostly in the hands and feet. Rheumatoid arthritis causes painful swelling that can eventually lead to deformity and erosion in the joints and bones.
- Polymyositis: This is a persistent inflammatory muscle disease that causes weakness in the skeletal muscles, which can affect your body movement.
- Dermatomyositis: This is an uncommon inflammatory disease that is marked by muscle weakness and can cause a distinctive skin rash.
These conditions can group together and can be very hard to diagnose because of the research and many tests that the patient is taking. Surprisingly, the average patient suffers from symptoms for 3.6 years before meeting diagnostic criteria. And the systems alone are difficult to classify, and often mimic or overlap other conditions. Some of the symptoms include hair loss, muscle pain, numbness or tingling, inflammation, low-grade fever, weakness and fatigue, joint pain, sensitive skin, and rashes.
Increased Need For Advanced Testing and Early Diagnosis

Sadly though, patients wait longer when they have these conditions, and it can worsen in the process as it takes years to get diagnosed for CDT. Practitioners can use treatments on their patients, but the medications act as a band-aid to mask the symptoms, but it does not adequately address the root causes of the disease. Sometimes the symptoms can progress faster than the current diagnostic test. So if you want to make sure your patients have any autoimmune diseases, run a diagnostic test on them, so you can detect early stages of the disease and start treating them so it can go away.
ENA and ANA
Extractable nuclear antigen (ENA) is a blood test that looks for antibodies to about 6 or 7 different proteins in the body.
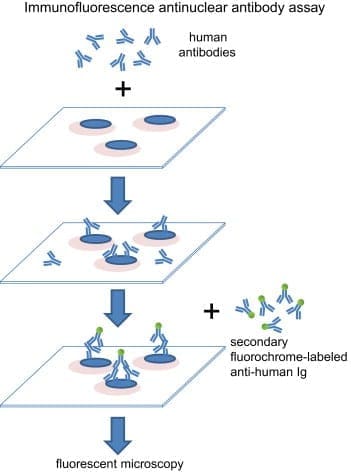
Antinuclear antibody (ANA) is used as an initial test that can help evaluate a person for an autoimmune disorder that can affect many tissues and organs throughout the body. It is most often used when practitioners are diagnosing patients for systemic lupus erythematosus.
Surprisingly ENA can be more predictive than ANA. However, patients were followed for 2 years, and about 20% of those patients developed positive ENA.
Vibrant Wellness Wheat Zoomer
In�a�previous article, we talked about gluten sensitivity and introduced the wheat zoomer. What the Vibrant Wheat Zoomer does is that it actually runs a test on your microbiomes to determine if you have a wheat sensitivity or a gluten sensitivity. It can actually detect IgG and IgA antibodies as well as detecting if your body has the celiac disease and intestinal permeability.� It pairs well with the Vibrant Gut Zoomer, and here at Injury Medical, we use the Wheat Zoomer on our patients to inform them about what is causing them to have gut inflammation or even leaky gut.
Celiac Disease and Wheat Allergens
Celiac Disease and Wheat Allergens is an autoimmune disorder in genetically susceptible individuals, and it affects about 1% of the population. In a previous article, we mentioned the hidden problems that gluten does to the body. And surprisingly, any wheat-related disorders can exist on a spectrum, this includes wheat allergy, gluten sensitivity, and wheat sensitivity.
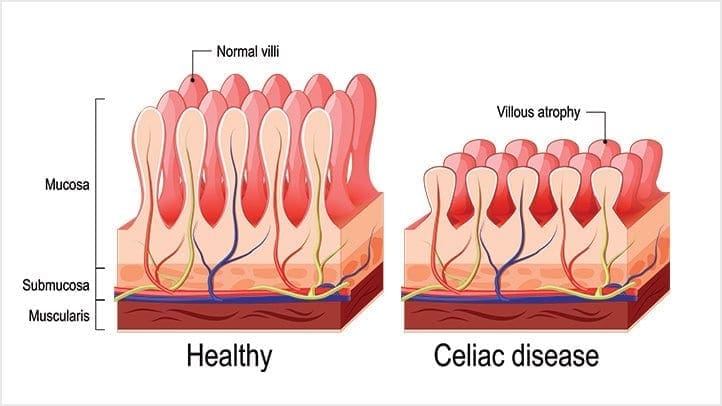
When a person, has the celiac disease, having any traces of wheat can actually upset their intestinal permeability and causing them to have a leaky gut.
The Connection to CTD and Celiac Disease
But how do connective tissue disorder and celiac disease are connected? Well, surprisingly, Rheumatoid arthritis (RA) and celiac disease (CD) share multiple aspects in epidemiology and clinical manifestations. Both disorders have been proven to be influenced by comparable environmental factors and a recent incidental surge of associated antibodies. Even though they have different depositions, both of them are mediated by endogenous enzymes that target different tissues and organs.
Conclusion
However through functional medicine; local chiropractors and health coaches here at Injury Medical Clinic, strive to understand what do our patients need to make their bodies feel better. If we can use functional medicine to prevent leaky gut at the early stages and help our patients with any ailments that they may have, then we can gently push them into the right direction of exercising throughout the week (even if it is about thirty minutes) and eating nutritious, whole, organic foods; as well as, preventing their ailments coming back then their bodies can finally heal.
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gut and Intestinal Health, Health, Wellness
In the last article, we talked about what the polyphenols do in the microbiome and in the previous section, we discussed about the microbiome functions in our bodies. However, today we will be concluding the three-part series of the microbiome functions in our bodies as well as presenting on the top 5 environmental toxins that can disrupt the gut microbiome, finding ways to de-stress ourselves, and learning about the different foods that can help detoxify our bodies so we can live a healthier life.
Top 5 Environmental Toxins Disrupting the Gut Microbiome
Triclosan
This is a synthetic antibacterial chemical found in personal care products such as soap, mouthwash, toothpaste, hand sanitizer, and deodorant. It is easily absorbed through the skin and gastrointestinal tract and rapidly alters the microbial composition of the digestive tract if it is ingested. However, this rapid restructuring of the gut microbiome impairs the immune system-regulating activities of gut microbes.
We use this chemical mostly in our daily skincare and hygiene routine so that way we won�t be sick. We tend to use this chemical compound to make us smell, look, and feel good frequently, especially in the cold and flu seasons where we use them the most so we won�t get sick. In fact, the frequent use of antibacterial products has been associated with an increased risk of food sensitivities, seasonal allergies, and asthma.
Pesticides

Surprisingly there are a staggering 1 billion pounds of pesticides used per year in the United States, and 5.6 billion pounds are used worldwide. Most farmers used it to spray down the insects so that way their crops won�t be destroyed. And we used pesticides on our lawns to get rid of weeds and keep the bugs off our gardens.
However, did you know that pesticides can kill beneficial bacteria in our gut? Studies, especially animal studies, indicate that pesticides can destroy the beneficial gut bacteria and can increase the risk of intestinal dysbiosis and cause immune system disorders, among with many other chronic health issues.
Plasticizers
These are chemicals that provide flexibility or rigidity to plastic products. These chemicals are highly prevalent in our environment and have a significant impact on gut bacteria. �Surprisingly the most common plastics are mostly BPA (Bisphenol-A).

Bisphenol-A (BPA) can be found in plastic water bottles, receipts, and the lining of canned foods. They can alter the healthy gut flora and disrupts the body�s hormonal system by mimicking the hormone estrogen. We do use these to put our leftovers in after we consume food. But now and days when we meal prep our food, we do look for containers that are BPA- free. However, while often being marketed as �BPA-free,� the plastic alternatives may be equally, if not more, harmful to our gut microbes.
Bisphenol-S and bisphenol-F demonstrate endocrine-disrupting effects that are comparable to BPA. These adverse effects may extend to the gut microbiome, causing disruption. Phthalates are another class of endocrine-disrupting plasticizers that are used as solvents in personal care products and vinyl plastic, and they also reduce the levels of beneficial gut bacteria.
Heavy Metals
Heavy metals, such as cadmium, lead, and arsenic, can reduce the levels of beneficial bacteria in the gut that protect against intestinal inflammation and may promote inflammatory gastrointestinal disorders. All microbes are responsible for methylating or demethylating metals, and the exposure may exceed the capacity to perform this. Due to industrial pollution, heavy metals are the most common contaminants that are in the soil and drinking water when we grow food and drink from the tap.
Pharmaceutical Drugs

Surprisingly most pharmaceutical drugs can help our bodies fight off infections or alleviate some pains we may be inflicted. But those antibiotics can disrupt the gut microbiome and cause an imbalance to our gut bacteria. We here at Injury Medical clinic, actually recommend our patients to alternatives to these drugs if you don�t want to disrupt your gut microbiome.
Functional medicines like whole foods and supplements can actually alleviate the pains that may cause disruption in your body.
Protecting the Microbiome From Environmental Toxins
When you want to live a healthier life and want to protect your body�s microbiome try these alternatives to get rid of these environmental toxins.
- Instead of using conventional cleaning products, which often contain triclosan, try switching to a plant-based brand. Also, try making your own cleaning products at home with natural ingredients.
- Avoid commercial body care products, as these are a significant source of triclosan, phthalates, and parabens. If you have any absorption of these chemicals, try checking out the Environmental Working Group�s Skin Deep Cosmetics Database. This database can help you find natural, healthy body care products that don�t contain microbiome-disrupting chemicals.
- Eat organic produce. Conventionally-grown fruits and vegetables are a significant source of microbiome-disrupting pesticide exposure. Research indicates that consuming organic food can significantly lower your body burden of pesticides, thus protecting your gut microbes. But y9ou are going to eat organic produce, remember to wash it first to get rid of excess pesticides.
- Try reducing your plastic intakes and limit your consumption of canned foods to reduce your exposure to BPA and BPA alternatives. When you are meal prepping, try using glass or stainless-steel water bottles and storage dishes instead of plastic, and opt for fresh food instead of canned.
- Try filtering your drinking and bathing water. Unfortunately, tap water is rife with pesticide residues, heavy metals, plasticizers, and pharmaceutical drug residues and can come off as a milky white if it�s not treated. So try to consider investing in a high-quality water filter that can remove these substances from your drinking water.
- Support your gut microbiome by consuming prebiotics and probiotics. In a previous article, we talked about probiotics in our gut. Probiotics can add beneficial bacteria to your stomach and may even help in the metabolism of toxins that are in your body�s microbiome. Prebiotics, a form of indigestible dietary fiber, that feeds probiotics and helps to support their growth and proliferation in the gastrointestinal tract.
Other Forms of Whole Body Detoxification

There are many ways to try and detoxify our bodies, so here are some examples:
- Sauna therapy
- Yoga, trampoline
- Meditation
- Energy healing/shamanism
- Taking a much-needed vacation
- Learn communication methods to accommodate multiple needs and to deal with stressful situations
Rebuilding the Gut Microbiome
When local health coaches, practitioners, and chiropractors are helping patients, they can provide a comprehensive strategy to help them gain a healthier life. When you want to rebuild your gut microbiome, try to reconstruct the natural digestive function with food/herbals. This will help support the immune system and nutritional status by creating the good bacteria in your liver and flushing out the toxins out of your system. However, try to avoid any foods that can trigger inflammation and can cause leaky gut.
Rebuild Natural Digestive Function
When you are rebuilding your natural digestive function, try finding food and supplements that contain zinc, Vitamin C, and bitter greens that can aid in the production of hydrochloric acid (HCL). However, avoid excessive amounts of fat in your diet so you won�t cause a leaky gut Also take some enzymes if you need them until your digestive is balanced and fully restored.
Support the Immune System and Nutritional Status
When your immune system is being overworked, try using micronutrient testing to identify deficiencies. Most SIBO patients are typically low in B12/iron, zinc, magnesium, and vitamin D.� But all these vitamins and supplements can support the immune system. With SIBO patients, they try to work on cleaning out their liver since it�s one of the major organs that flushes out the toxins in our bodies. If you do have SIBO, try adding more fruits and plant foods that can help �clean out the liver.� Certain fruits can be tolerated and titrated up after treatment over time, but try to reduce meat/animal fats and fats in general; since they are harder to digest and can contribute to imbalanced bile acid secretion. Also, use liver support herbs and supplements such as glutathione and silymarin.
Avoid Foods that Can Provoke Inflammation

In a previous article, we talked about food sensitivity and what to do if you have it. Some testing can be helpful to determine if other foods may need to be eliminated. Here are the most common foods that provoke inflammation in dysbiosis are:
- Gluten
- Dairy
- Eggs
- Soy
- Corn
So if you have a food sensitivity, start by slowly build the natural SCFA�s with small amounts of natural resistant starch (e.g., cooked/cooled potatoes). However, if the patient is being treated with SIBO, introduce it after. Also considering adding other sources of food so it can help grow the good bacteria in your gut. But also keep HCL production active to clean out the stomach and upper part of the small intestine.
This will ensure that the good bacteria will grow over time with your diet and the help of probiotics and fermented food. But if a patient has SIBO take caution so the patient won�t disrupt the treatments they are in and are completed.
If you are taking care of a patient, carefully choose probiotic based on symptoms they have. Some will need a d-lactate free formula, and you can bring up the dosage over time until their treatment is complete. Some CFUs (colony forming units) will vary by product and viability through the GI tract (enteric-coated vs. not), and some probiotics may need to be used long term in some individuals.
Fermentation

Fermented foods are very beneficial to our gut flora as they actually help in the production of good bacteria in our intestinal barriers. Fermented foods and beverages are literally alive with strong pronounced flavor and nutrition. However, not all preserved foods are fermented with live cultures; some may be brined through the use of vinegar and/or salt, and do not impart probiotic benefit.
 �Fermentation is the transformation of food by various bacteria, fungi, and the enzymes they produce. It is important to recognize that fermentation is a natural phenomenon much broader than social, culinary practices; cells in our bodies are capable of fermentation. In other words, humans did not invent fermentation; it would be more accurate to state that fermentation created us.� � Dr. Alex Jimenez�D.C., C.C.S.T.
�Fermentation is the transformation of food by various bacteria, fungi, and the enzymes they produce. It is important to recognize that fermentation is a natural phenomenon much broader than social, culinary practices; cells in our bodies are capable of fermentation. In other words, humans did not invent fermentation; it would be more accurate to state that fermentation created us.� � Dr. Alex Jimenez�D.C., C.C.S.T.
Conclusion
So all in all, those are some of the many ways to actually help our bodies microbiome when we want to live a healthier life. Here at Injury Medical Clinic, local chiropractors and health coaches, actually use functional medicine to patients so that way, they can fix their ailments naturally, without the use of drugs and non-conventional methods. If we can change a person�s lifestyle with functional medicine, we can repair the microbes in our bodies, one at a time naturally, of course.
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gut and Intestinal Health, Health, Wellness
In the last article, we talked about how the microbiomes in our body worked and functioned. As well as learning what each microbe does in our bodies but mostly in our gut. When we are learning more and more about the microbiome, we discover many exciting things that our bodies are capable of as well as being the workers in our intricate immune system. In today�s article, we will be taking a look at what polyphenols does to our microbiomes as well as specific vitamins that are very helpful to our gut and going in-depth more with SCFAs (Short Chain Fatty Acids) and the Tight Junction.
The Role of Polyphenols in Microbiome Balance
Polyphenols, or phenolic compounds, are considered a type of micronutrients, and they are plentiful in plants. They have been well-studied for their role in the prevention of chronic diseases such as CVD, cancer, and neurodegenerative diseases. They also have antioxidant properties, and there are several hundreds of polyphenols that are found in edible plants that serve a giant purpose of defending our bodies against ultraviolet radiation or aggression by pathogens.
To figure this out, think of it like this: The bacteria in our large intestine releases polyphenols from the plants we eat in our diets. It is then transformed into a diet composition that alters the bacterial ecosystem (through the prebiotic effects and antimicrobial properties) to make our gut happy.
Here are some of the microbes that are in polyphenols:
- Phenolic acids: These are derivatives of benzoic acid and derivatives of cinnamic acid.
- Flavonoids: These microbes contain flavonols (e.g., quercetin), flavones, isoflavones (e.g., phytoestrogens), flavanones, anthocyanidins, and flavanols (e.g., catechins and proanthocyanidins)
- Stilbenes: These microbes are resveratrol
- Lignans: these are minor in the human diet and are linseed oil
Surprisingly some factors affect the polyphenol content of plants, and these include:
- The ripeness at the time of harvest
- The environmental factors (exposure to light, soil nutrients, pesticides)
- processing and storage
When we eat organic fruits and vegetables, they have more polyphenol content that is usually, due to growing under slightly more stressed conditions. Which requires the plant to generate a stronger �defense and healing� response to the environment, and only 5�10% of the total polyphenol intake is absorbed in the small intestine. And 90-95% polyphenols that are linked to fibrous components must be liberated through hydrolysis by bacteria in the large intestine.
Surprisingly some polyphenols do not show up in plasma in humans after ingestion, and a large quantity is metabolized by intestinal bacteria or used to neutralize various pro-oxidizing agents in the intestinal lumen.
Clostridium and Eubacterium (which are both Firmicutes), are the primary metabolizers of polyphenols. Studies theorized that higher polyphenol intake may play a role in shaping the Bacteroidetes to Firmicutes ratio (e.g., inflammatory response potential, obesity, etc.) and can be harmful to our bodies.
However, more recent studies have shown effects of inhibition on Clostridium and Staphylococcus of polyphenols such as grape seed extract, in favor of Lactobacillus and other studies have demonstrated potent inhibition of phenolic compounds thymol (thyme) and carvacrol (oregano) on Escherichia, Clostridia and other pathogens, while simultaneously leaving Lactobacilli and Bifidobacteria have been unaffected.
Here are some other examples of some polyphenols:
- Resveratrol increases Clostridia, Lactobacillus, and Bifidobacteria
- Blueberry phenolics increase Bifidobacteria
- Phenolic compounds in tea suppress C difficile and C perfringens
- Catechins (found in high doses in teas and chocolate) act on different bacterial species (E. coli, Bordetella bronchiseptica, Serratia marcescens, Klebsiella pneumonia, Salmonella cholestasis, Pseudomonas aeruginosa, Staphylococcus aureus, and Bacillus subtilis) by generating hydrogen peroxide and by altering the permeability of the microbial membrane
- Some studies have shown that polyphenols can interfere with bacterial cell signaling and quorum sensing (environmental sampling)
- Polyphenols can also cause bacterial populations to stop expansion through signaling interference
- Some research indicates certain polyphenols may be able to block the production of bacterial toxins (H. pylori and tea/wine polyphenols)
The Applications for A Diet

When it comes to eating a healthy diet, variety does matter. The colors, the types of fibers each organic food has, and whether you are going to do it daily or weekly. When you are trying to be in a healthy lifestyle, it always starts with the food. When you are looking for fresh produce, try to emphasize fresh, organic, and minimally processed versions of polyphenol-rich foods. However, don�t boil produce. Instead, try steaming then, and it is the best, but roasting or light frying is not only better, but it tastes so good.
Vitamins that help our Microbiome
When we are older, we tend to lose specific vitamins that actually helps us and our bodies to be healthier. Here are some of the vitamins that are really good for our gut and can help us prevent leaky gut.
Vitamin D
Vitamin D controls the development of gut-associated lymphoid tissue in our bodies. It is trafficking between gut dendritic cells, and they can differentiation of T-regs and T-reg function in our gut. But the expression of VDR, which influences IL (interleukin) production and tight junction integrity to help our gut.

When it comes to our gut, here are some of the effects of Vitamin D on the gut microbiome. The higher the Vitamin D levels are, they will allow commensal bacteria to secrete more AMPs (antimicrobial peptides). When patients take a high dose of Vitamin D, over 5 weeks can lead to a significant reduction in Pseudomonas spp and Shigella/Escherichia spp in upper gut intestines.
Another thing that Vitamin D does is that it can increase T cell differentiation in the colon. A lack of T-regs increased the incidence of asthma, allergies, autoimmune, and autism. But T-regs can prevent the development of aberrant immune responses such as autoimmune and food sensitivities. We here at Injury Medical Clinic, talk about functional medicine to our patients and try to help them recover from their ailments.
Because Vitamin D exposure fluctuates seasonally for many individuals, it has been observed that lower Vitamin D levels in the winter tend to lead to changes in the intestinal microbial balance. This will make our bodies have a decreased level of Bacteroidetes and an increased level of Firmicutes. This is the reason for �winter weight gain� in many individuals as F: B ratio changes.
Vitamin A

This is a retinoic acid that is required by dendritic cells (DCs) to induce T-cells (and B cells) which are the �tracking and regulation system� of the mucosal immune response. Because of this, T-cells must differentiate into T-regs to maintain a �calm and cool� system or immune tolerance to both our environment, symbiotic organisms, and food.
Omega-3 Fatty Acids

We talked about Omega-3s in a previous article as they are one of the many supplements that we can�t produce in our bodies. It can be mostly found in fish, and some plants can contain omega-3s. But it is a vital team player when we are trying to be healthy and can prevent a leaky gut. Not only that but omega-3s are crucial importance to more youthful skin.
SCFAs (Short Chained Fatty Acids)
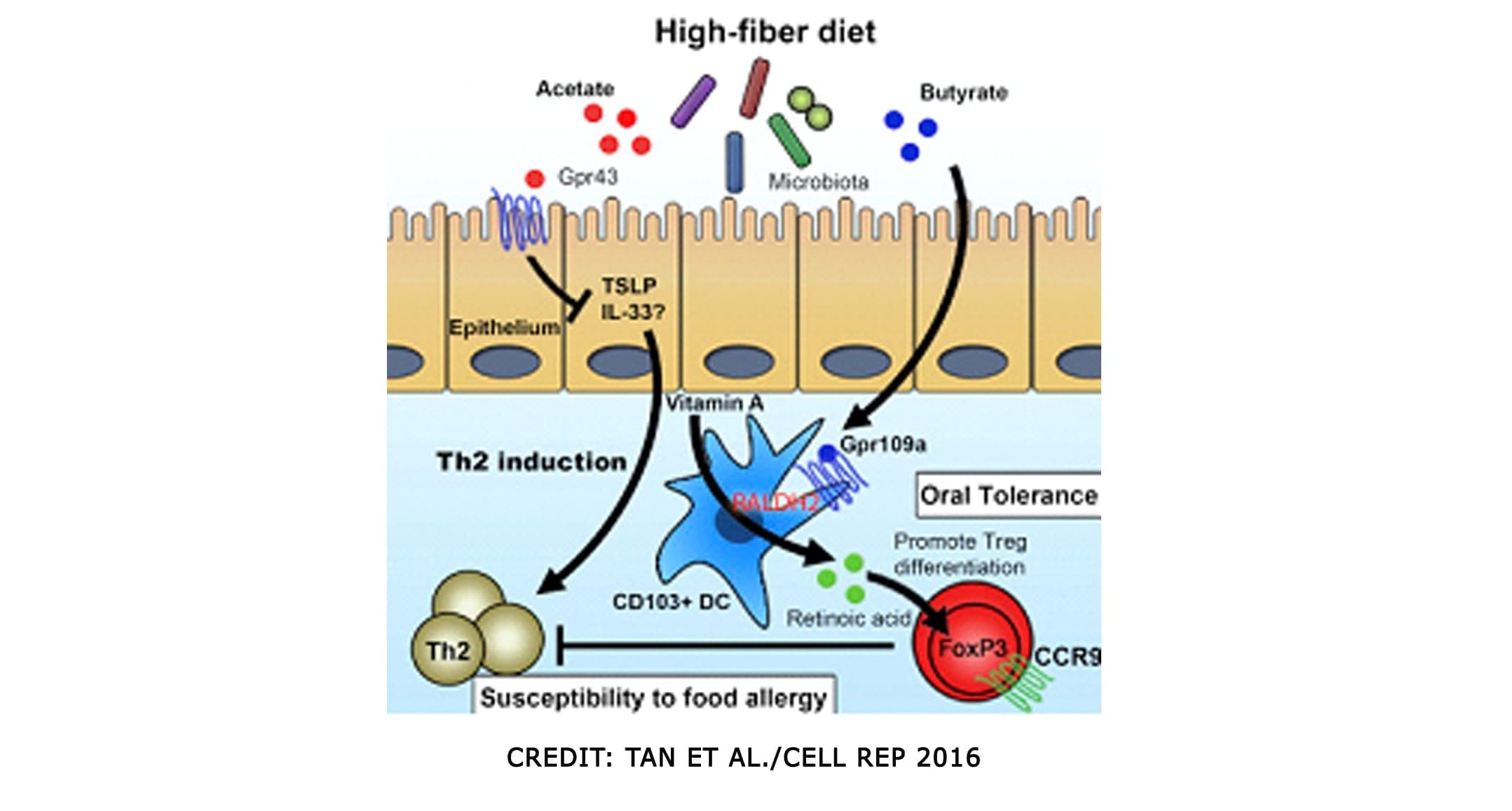
SCFAs (Short Chained Fatty Acids)�are well-studied to demonstrate anti-inflammatory properties in the large intestine. They are the primary source of fuel for cells lining the intestinal epithelium of the large intestine. They contained: �Butyrate, Proprionate, Acetate. In a previous article, we discussed what SCFAs do when we eat fatty food. It can be both good or bad, depending on what kinds of food you consume. SCFAs act on G-protein coupled receptors to induce differentiation of T-cells, but also on those GPRs in DCs. They can both be direct and indirect influences on our gut.
SCFAs can produce bacteria and can directly impact T-reg production. And that SCFAs inhibit the mucosa and competitively inhibit opportunists. Some foods that provide higher resistant starch will typically yield the most short-chain fatty acids upon microbial fermentation
Tight Junction Modulations
The tight junctions are the gateways between the epithelial cells. In a previous article, we took a look at what the tight junction is. They control the flow of nutrients, macromolecules, and other substances that are usually allowed to pass through without cellular diffusion or absorption.
Conclusion
All in all, we covered a lot of information about what polyphenols does as well as specific vitamins and supplements that can help our bodies prevent a leaky gut. The microbiomes in our collection and the use of functional medicine can be beneficial in helping us not only to a better, healthier life but, a working, functional body for us when we are older. Tomorrow we will end this three-part series with foods and tips to have a healthy microbiome in our gut and our bodies.
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gut and Intestinal Health, Wellness
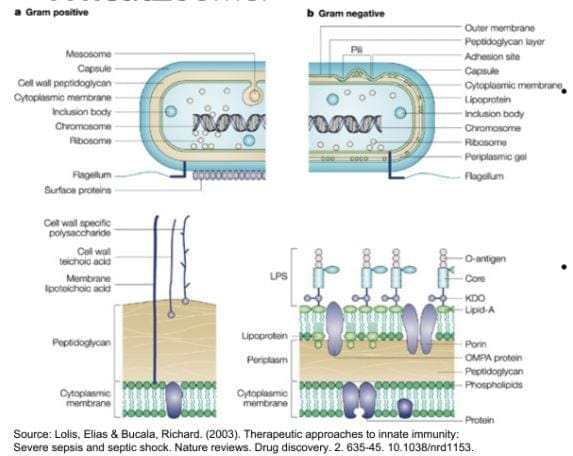
To understand exactly how lipopolysaccharides and gram-negative bugs affect the immune system we must first investigate what lipopolysaccharides are and their role in gram-negative bacteria and the human body as a whole.
LPS (Lipopolysaccharides)
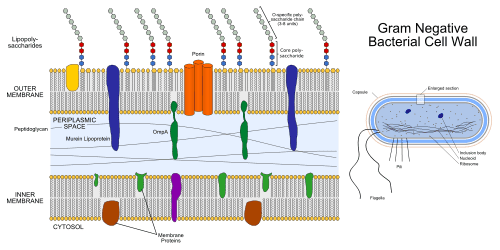
Lipopolysaccharides (LPS) are large molecules consisting of a lipid (fatty acid) and a polysaccharide composed of the O-antigen, outer core, and the inner core all joined by covalent bonds. �Lipid A in LPS is the hydrophobic component responsible for the major bioactivity of LPS. Hydrophilic polysaccharides consist of long chains of monosaccharides (simple sugars) linked together by glycosidic linkages. LPS play their role in the outer membrane of gram-negative bacteria by supporting the structure of the bacteria and shielding the membrane from chemical attack. Gram-negative bacteria are related to foodborne diseases, respiratory infections, plagues, and some sexually transmitted diseases. Some gram-negative bacteria have become so resistant to antibiotic drugs that they are often very difficult to treat and unfortunately vaccines are not available for these types of bacterial infections. Additional enzymes can sometimes alter the structure of the LPS, and though the structure is not required for the bacteria�s survival it is closely related to the virulence of bacteria. For example, the lipid A component of LPS can cause toxic reactions when lysed by immune cells. LPS in humans trigger the immune system to produce cytokines (hormone regulators). Production of cytokines is a common cause of inflammation.
Now that we are able to recognize the relationship between LPS, gram-negative bacteria, and inflammation/infections in the human body, we must understand how to prevent and treat infections related to gram-negative bacteria. Gram-negative bacterial infections are caused by contact between infected and non-infected peoples. They are very common in healthcare settings, but by taking simple measures such as hand washing and keeping a strong immune system will help prevent them. How do we keep a strong immune system? Choosing a healthy lifestyle is the first most basic step in this process. Because the immune system is a system, we must understand that there is no direct way to improve its strength. It is strengthened through what we put into our body and how we treat our body. However, it is important to distinguish between building a strong immune system and boosting the number of immune cells in our body. It is potentially harmful to boost the number of immune cells because there are so many different kinds of cells in the immune system that respond to so many different microbes in so many ways. Diet, exercise, reducing stress levels, and some herbs and supplements all contribute to building and supporting a strong immune system.
Conclusion
Throughout this article, we have learned about lipopolysaccharides and the role they play in gram-negative bacteria. Gram-negative bacteria are known to be harmful to the human body so we have found ways to prevent the harmful infections it causes. The immune system plays an obviously important role in fighting infections, but it needs to be strong to support our body and fight infections efficiently. This basic knowledge is provided to set the basis for further research on how to support the immune system.
Resources:
https://www.niaid.nih.gov/research/gram-negative-bacteria
https://www.scbi.nih.gov/pubmed/20593260
https://en.wikipedia.org/wiki/gram-negative_bacteria
https://www.health.harvard.edu/staying-healthy/how-to-boost-your-immune-system
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gut and Intestinal Health, Wellness
The microbiomes in our bodies are fascinating. They help our various organs function correctly, helping out our immune systems battle terrible stuff. They can tell us what we are doing to our bodies when we consume food. However, the microbiomes in our gut tell us a different story as we are going to discuss what does microbiomes do as it functions in our body as well as our gut.
The relationship between the gut microbiota and its host plays a crucial role in:
- immune system maturation
- food digestion
- drug metabolism
- detoxification
- vitamin production
- prevention of pathogenic bacterial adhesion
Also, the composition of the microbiota is influenced by environmental factors such as diet, antibiotic therapy, and environmental exposure to microorganisms.
Why Don�t We All Have the Same Microbiome?

Whenever we are trying to live a healthy lifestyle, our bodies will go through so many changes. When we get rid of the bad stuff that is causing us problems and the beautiful thing start taking effect in what we put in our bodies. We, as humans, have different body structures and body types that are way different. Some people lose or gain weight differently. When other people exercises, they go at their own pace, and several factors influence the bacterial composition in taxa type and abundance. These factors include:
- host phenotype, such as age, gender, body mass index (BMI)
- lifestyle
- immune function
- geographical belonging and environmental factors
- use of antibiotics, drugs, and probiotics
- DIET
Moreover, long-term dietary habits have been shown to play a crucial role in creating an inter-individual variation in microbiota composition.
Manipulating the Microbiome: Key Terms
Here are some key terms to remember when we are talking about the microbiome.
- Stability: resistance to change and the ability to maintain homeostasis.
- Resilience: capacity to return to homeostasis after disturbance.
- Diversity: DIVERSE microbiomes are more stable and more resilient (to antibiotics); more resistant to foreign invasion (pathogens).
- Relative Abundance: Even �good� bacteria can be too abundant without balance from symbiotic species; the presence of �bad� bacteria is not necessarily always harmful if enough �good� are there to balance.
- Colonization Resistance: The capacity of the microbiome communities to resist new colonization by pathogens and other transients.
- This is a KEY factor for preventing GI infections; but also explains why probiotics are not always practical.
- Our COMMENSAL microbiome is our first line and of defense
- Microbial depletion: Infection; Antibiotics; Toxins/Chemicals; Stress
- Restore balance/� reseeding�: (the term �reinoculate� is not really correct) Probiotics; Fermented foods; Prebiotics/Polyphenols.
Advantages to DNA Testing

For many practitioners, measuring microorganism DNA allows for:
- Detection of a more diverse collection of microorganisms, (more genus and species, particularly anaerobic species)
- They can measure at the species and subspecies level
- They have a much better snapshot of dysbiosis and diversity
- Have better accuracy of results
- Much faster turnaround time and much less expensive
- Concept of �epigenetics.�
However, DNA is DNA-dead or alive whenever practitioners are looking at a patient�s DNA structure. Culture Technology is still considered �gold standard� but has several limitations. They are trying to culture anaerobic bacteria, but some of the most important bacteria are anaerobic commensals. There is a limited detection of several microorganisms, but it�s usually genus level only. Microorganisms can grow and/or die in transit and what�s measured in the culture dish is not always 100% indicative of the sample at the time of collection; the environment can morph while in transit to the lab and changes in pH etc.
Important Groups
These are some of the microbiomes that are very functional to our bodies and what parts do they play.
Commensals

This microbiome provides the host with essential nutrients and contains Aerobic and Anaerobic microbiomes.
- Aerobic (survives better in oxygenated environments; less prevalent in the colon, however, some are considered �obligate anaerobes�). They are:
- Lactobacillus
- Bifidobacterium
- Bacillus
- Anaerobic (more likely to be found colonizing the distal colon due to limited oxygen). They are:
Lactobacillus and Bifidobacteria
These two are the most well-researched genus of bacteria. They are widely available in commercially available probiotic products.

- Lactobacillus are:
- lactic-acid forming bacteria
- Form biofilms which allow surviving harsh/low pH conditions (stomach acid)
- Helps maintain the integrity of the intestinal barrier
- Abundant in probiotics/fermented foods

- Bifidobacteria are:
- One of the first bacteria to colonize the gut after birth
- Aids in digestion, reducing inflammation, and stimulation of immune cells
Bacillus

These are spore-forming bacteria. They form spores in harsh environments which makes them more resilient, heat-stable, and have better viability in the gastric environment. But they may have better efficacy as probiotic therapy in SIBO population. These are in another category of commercially-produced probiotics beyond the standard Lactobacillus and Bifidobacterium.
In the health world, known as �Soil Based Probiotics.� They are very prominent in the environment and their primary role in immunomodulation; stimulation of the immune system. They are a production of GALT-Gut Associated Lymphoid Tissue and are known to be significant players in the production of B Vitamins and Vitamin K2 in the gut known as Bacillus subtilis
Clostridia
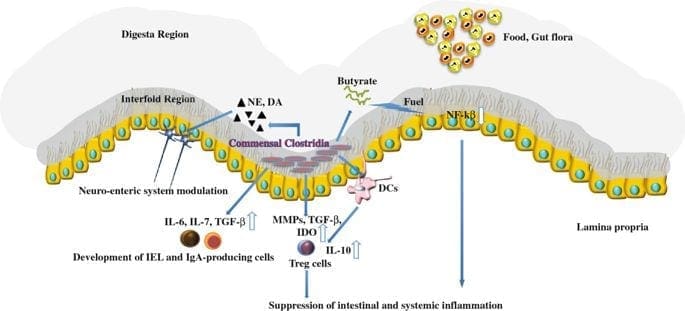
These are a major anaerobic group of commensals. They comprise 10% to >50% of the microbiome and are critical for the health of the gut barrier and intestinal lining, and barrier integrity. These are essential producers of butyrate (SCFA) and secondary bile acids. They also thrive on a high and diverse fiber diet, grape, and red wine polyphenols such as Blautia, Butyrivibrio, Eubacterium, Faecalibacterium prausnitizi, Roseburia, Ruminococcus, etc. However, there are usually no probiotic supplements to directly increase the abundance of clostridia.
Akkermansia

These microbiomes make up 1-3% of a healthy microbiome, and they help maintain the health and integrity of the mucosal barrier.
- Akkermansia muciniphila = mucin lover
They also help with reducing inflammation and may impart protection of inflammatory bowel diseases. These microbiomes are keystone species that are highly correlated with higher microbiome diversity.
Proteobacteria

This is a PHYLUM category of bacteria. This microbiome contains gram-negative and all bacteria that carries an LPS. This group includes plenty of beneficial bacteria but also contains several pathogens that tend to thrive in pro-inflammatory condition.
Gram (+) vs Gram (-) Bacteria
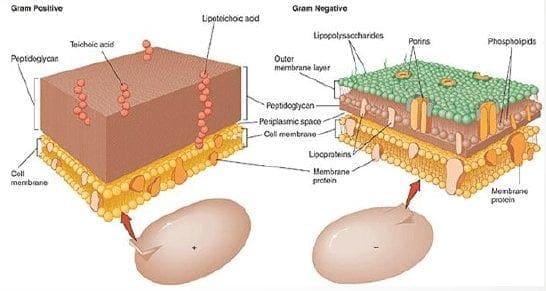
These two types of bacteria are in our bodies as they have very different functions that can either protect or disrupt our gut.
- Gram-Positive (+) contains:
- Peptidoglycan
- Lipoteichoic acid
- Gram-Negative (-) contains:
- LPS as a component of their cell wall
- LPS is a very powerful ENDOTOXIN- a known contributor to induce significant inflammation and potent immune response
- LPS antibodies are measured on Vibrant Wellness Wheat Zoomer/Intestinal Permeability Panel
However we can�t generalize Gram (-) as �bad� or Gram (+) as �good� or vice-versa, but we can control it with the Zoomers test.
LPS(Lipopolysaccharide)
In the last article, we mentioned them briefly, but here is a refresher on what theses microbes do. They are a fat/sugar molecule that lines the gram-negative bacteria inside the gut, and they protect those bacteria from bile salts. They are present inside the gut lumen under normal physiological conditions, and they usually should not enter the bloodstream. But if it does open in the blood then�
- 1) LPS antibodies are created-tagged as �non-self.�
- 2) Indication of intestinal permeability.
- 3) triggers multiple inflammatory cascades = ENDOTOXEMIA
- 4) Can help differentiate if leaky gut is happening between cells or through cells (or both), which are Transcellular vs. Paracellular pathways
Conclusion
These are the microbiomes that are in our body and how each of them plays a role to make our bodies healthy. We here at Injury Medical Clinic, do talk with our patients about what goes on in their bodies. We inform them on how to take care of themselves through the means of functional medicine. This is part one of a three-part series since tomorrow we will be discussing the roles of polyphenols in the Microbiome balance.
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gut and Intestinal Health, Health, Wellness
In the last three articles, we introduced the wheat zoomer, went in-depth about the intestinal permeability, and the microbes in our gut. We also talked about the hidden problem with gluten as well. Today we will be discussing what to do after your patient comes in for a check-up after completing their gut healing process. For this to work, patients have to be gluten-free for the results to work. After the healing phase, local chiropractors, health coaches, and physicians can introduce gluten back slowly into the patient’s diet.
Checkups
When the patient comes in for a check-up, here are some of the things doctors look for:
- If everything is green, re-introducing gluten may be possible for patients.
- If anything is still yellow or red, patients must continue to avoid gluten and keep the gut healing process until the test results are all green.
After the appointment, patients can retest the wheat zoomer in about 3-9 months. However, there are about 50% of individuals with celiac disease that may also have antibodies to casein and may have to go dairy-free to heal their gut. Although some individuals are gluten sensitive may not be lactose intolerant but can go dairy free if they want to.
Lectins
Surprisingly all plants have lectin, but some of them are not problematic to humans thankfully. Legumes and grains play a role in increasing the diversity of microbes that may be beneficial or harmful to our bodies. Wheat Germ Agglutinin is the only specific lectin to the Wheat Zoomer, but it doesn�t reflect the overall lectin sensitivity but, consider the lectin zoomer to determine any particular lectins that your patient is sensitive to without eliminating unnecessary foods that are beneficial to the gut healing process.
Soy

Many studies show that soy may be a problem due to the saponin since it does have higher lectin count. Here at Injury Medical clinic, we suggest that running the Lectin Zoomer on our patients with intestinal permeability makes sense for them to heal correctly. But animal studies stated that soybean agglutinin has the effect of the increasing release of zonulin away from the TJ (tight junction). And a human study reported that if the soy saponin is poorly absorbed or utilized by the human intestinal epithelial cell will end up metabolizing the intestinal bacteria and cause more harm to human.
Surfactants

Known as sucrose monoester fatty acids is mostly used in cosmetics, food preservatives, food additives. Sucrose esters are used as a surface treatment on some fruits like peaches, pears, cherries, apples, and bananas. It keeps the moisture on the peel or rind controlled. Sucrose mono ester used in cosmetics as an emulsifier.
Bone broth/Collagen

Up to this date, there are minimal studies that have examined the role of bone broth or collagen that it repairs the intestinal barrier. It all depends on the animal and the bone it comes from and the contents that people have put in a bone broth soup.
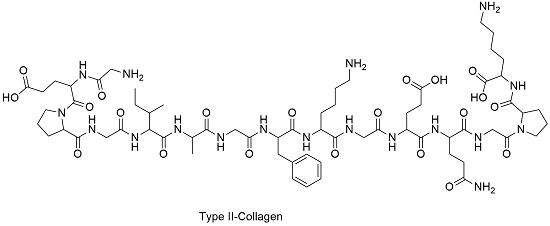
However, there is a small body of evidence for the use of collagen peptides seem to support the usage in their autoimmune disease treatment protocol. But the results cant be extrapolated whether bone broth would have similar effects. So more studying about bone broth is needed.
Organic Produce

When people say that they are going organic, it is beneficial for people that are willing to change to a healthy lifestyle. Granted that organically produces are locally grown, but still, organic produce or non-organic produce will not have less or safer pesticides. They are different, but all of the crops like fruits and vegetables are grown with pesticides.
Just like all fruits and vegetables, still, wash them thoroughly to reduce the number of pesticides and surfactants exposure and enjoy them to your heart’s content.
Resistant Starches

Resistant starch foods are a form of carbohydrates that can be converted to short fatty acids by SCFA-producing bacteria. With higher SCFA levels, these starches aid immune tolerance, T-cell differentiation, and intestinal barrier homeostasis. Other types of fibers are high value, and variety is essential. Like for example, cooked/cooled rice and potatoes are excellent resistance starch foods.

“Eat like a vegetarian who eats meat.”- Dr. Alex Jimenez�D.C., C.C.S.T.
Polyphenol Foods
Polyphenols, flavonoids and other phenolic compounds will aid to maintained TJ stability through inhibiting phosphorylation of TJ complexes.
Fermented Foods
Fermented food or drinks that contain live probiotic cultures are excellent in promoting a healthy gut. However, it is challenging to study fermented food and beverages due to highly variable stains, composition, nutrient content. But studies found that participants who drink a fermented plant extract drink saw improvements in their body and increased total antioxidants and total phenolic in plasma as well as with reducing total C and LDL-C.
Beneficial bacteria like Bifido and Lactobacillus were increased while E Coli and C perfringens were decreased in the gut. So drinking or eating fermented food can help our gut and help our bile growth to be flushed out.
Granted, we all know that trying to be healthy is very hard. It is true that even though exercising is easy because we can do it over and over again until we are masters at it but, when we overdo the exercises it will cause harm to our bodies and hurting it in the process. �Eating healthy is hard as well because our bodies may have a food allergen or a food sensitivity that will make us disappointed that we can�t enjoy the foods we want to eat. Yes, eliminating diets are very hard and challenging to follow in the long term and have poor compliances when we don�t put in the work. So start by exploring other tests to tailor patients diets to meet their health needs and prolong their recovery period.
Supplements

Supplements are fantastic to aid the valuable nutrients and minerals our bodies can�t produce. Common supplements prescribed include:
- L-glutamine
- Vitamin D3
- Collagen
- Colostrum
- Zinc carnosine
- Ox bile
- Omega-3s
- Turmeric/Quercetin
- Magnesium
Stress Management

Granted that stress is part of our lives and we can manage small amounts of it, and it is beneficial to us, but some people have chronic stress and have to go to a doctor to get it treated. But there is hope as there are ways to manage stress and doing it functionally and naturally.
Conclusion
So all in all, just to recap, if your patient is good to go and their test results are all green, you can introduce gluten back to their diets again in small increments and can be rested in about 3 to 9 months. But if your patient does have a gluten allergen then just let them know that they must continue to be gluten-free. We here at Injury Medical Clinic, always put our patient�s needs first for them to live their best lives with functional natural medicine.






