
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Chiropractic, Functional Medicine, Health, Hormone Balance, Integrative Functional Wellness, Wellness
Hormone testing can now be done by using top of the line integrative methods and techniques. There are multiple reasons and benefits for an individual to complete a hormone test. These tests have the ability to help a patient understand their cycle, testosterone/ estrogen levels, why they are tired upon waking or throughout their day, and more.
Precision Analyical, Inc. has discovered a way to use scientists who have extensive experience and coupled them with the most advanced analytical methods and instruments. This allows them to achieve the best results when it comes to the dutchtest.
What is D.U.T.C.H?
D.U.T.C.H stands for ” Dried Urine for Comprehensive Hormones” and is comprised of multiple tests designed by Precision Analytical Inc. Dried urine samples allow scientists to see an entire day of hormones and measure multiple different aspects. There are different D.U.T.C.H tests that can be completed depending on the patient’s needs.�
- Dutch Complete– This is a comprehensive assessment of sex and adrenal hormones and their metabolites. This test measures progesterone, androgen, estrogen metabolites, cortisol, cortisone, cortisol metabolites, creatine, DHEA-S.�
- Dutch Sex and Hormone Metabolites– This test is focused on testing progesterone, androgen, estrogen metabolites
- Dutch Adrenal– This is important to measure because it controls the stress hormone and the levels in the body to help with energy upon waking. This test specifically measures cortisol, cortisol metabolites, creatinine, DHEA-S
- Dutch OATS “Organic Acid Tests”-� This test will give insights to symptoms such as mood and fatigue. This test measures 9-OHdG, melatonin.
- Dutch Plus– This test uses 5 saliva samples to provide the up and down pattern of cortisol and cortisone throughout the day. This test adds salivary cortisol measurements of the cortisol awakening response (CAR) to the dutch complete to bring another important piece of the HPA axis into focus
- Dutch Test Cycle Mapping– This test maps the progesterone and estrogen pattern throughout the menstrual cycle. It provides the full picture of a woman’s cycle to answer important questions for patients with month-long symptoms, infertility, and PCOS. This test is targeted to measure 9 estrogens and progesterone that are taken throughout the cycle to characterize the follicular, ovulatory, and luteal phases.�

How Does It Work?
One of the reasons that many practicing offices are starting to use the D.U.T.C.H tests is because they have an extremely simple sample collection. Patients will collect just 4-5 dried urine samples over a period of 24 hours. This makes transportation and collection of the sample hassle-free. The dried urine samples provide excellent results due to the fact that the collections offer a span of the entires day hormones. The time of testing looks as follows:
- The patient obtains the first sample at approximately 5pm ( dinnertime)
- The� second sample is to be taken around 10 pm ( bedtime)
- This next sample is dependent upon each individual, but if the patient wakes to urinate during the night, a sample is to be collected at this time.
- The third sample should be collected within 10 minutes of rising. It is very important that the patient does not lay in bed after waking and they collect this sample within those allotted 10 minute time frame.
- Once the patient has collected their third sample upon rising, they should set an alarm for 2 hours, as this is when the fourth and final sample is to be collected.
As one can see above, these urine samples will be dry when sent off to the lab. Studies show that dried urine samples are stable for weeks and will give an accurate representation of the hormone levels that are being assessed. From here, the results are gone over with a team of clinicians from Precision Analytical with the doctor who ordered the test. This ensures that the best treatment protocol is created for the patient.��
What Is The Purpose?�
With the turn around time being just 7-10 business days, individuals can gain control fairly quickly. As mentioned, Precision Analytical uses the most advanced instruments to achieve the best results for patients. The main purpose is to create an understanding of what is going on inside the patient’s body and allows the treatment to be more specific and targeted to the individual’s needs. As Chiropractic Health Month approaches, there is no better time than now to get started!�
�I highly recommend the D.U.T.C.H test. Knowing and understanding your hormones and the times that they are rising and falling throughout the day opens so many doors. It allows an individual to have an understanding of why they are so tired or why they can not fall asleep and take distinctive steps towards correcting that issue, rather than shooting in the dark. In addition, it allows patients to have knowledge of what is occurring when it comes to their sex hormone metabolites. This test gives the ordering doctor a complete look at the patient’s hormones and ensures they can be confident in creating a treatment protocol. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gastro Intestinal Health, Gut and Intestinal Health, Health
For anyone that has dealt with mold knows that it is mostly found in fresh produce when it hasn’t been eaten. It is even there is a new damp spot in the house, and it�s left untreated. Mold is a type of fungus that is presented everywhere, including the air. It can actually cause someone highly sensitive to mold exposure to have chronic raspatory illnesses like asthma and bronchitis.
Studies show that the most common species of mold is Stachybotrys chartarum or black mold. This type of fungus thrives in warm, moist environments, including the basement, the bathroom, and the kitchen. It releases toxins in the air that is irritating or harmful to individuals with existing health conditions and becoming mycotoxin.
What is Mycotoxin?

A mycotoxin is a secondary metabolite being produced by organisms of the fungal kingdom. It can move in and out of cells in the body, causing inflammation when it is indigested. Researchers suggest that mycotoxin can link to serious health problems to people who live in contaminated buildings, and it can have long-term results. In most cases, mycotoxin can cause problems in the gut by consuming moldy food; causing leaky gut and destroying the gut microflora.
Here are some of the symptoms of mycotoxin:
- Aches and pains
- Mood changes
- Headaches
- Brain fog
- Asthma
- Watery, red eyes
- Runny or blocked nose
- Gut inflammation
- Sore throat
They are teratogenic, mutagenic, nephrotoxic, immunosuppressive, and carcinogenic. They can cause DNA damage, cancer, immune suppression, neurological issues, and a variety of adverse health effects on the human body. With mycotoxins, they have spores and pieces of hyphae that releases toxins into the air. They are tiny, but they are not easily detectable in the bloodstream since they can attach themselves to enzymes that are involved in insulin receptors. This results in dysfunction the in cells ability to intake and process glucose in the gut.
When mycotoxin is in the gut, it damages the intestinal barrier. It can cause malabsorption of food and disrupts the protein synthesis. When that happens, the individual�s autoimmunity will rise up, causing their bodies to go into overdrive to fight the problem.
Mycotoxin can actually grow in grains such as rice. The fungal mycotoxin has been known to cause liver damage since the contaminated food is being consumed by people, and it creates a rise in inflammation. When this happens, individuals start being sensitive to the contaminated foods that they are consuming. There is still more research to mycotoxin that is being produced to create a resistance to mycotoxin exposure.
Diagnosing Mycotoxin
Mycotoxin can�t be diagnosed by the symptoms themselves, doctors can perform one of these tests to determine the severity of mycotoxins in individuals.
- Blood test: Physicians can take a patient�s blood sample and send it to a testing lab to test. This is to see if there is a reaction of specific antibodies in the patient�s immune system. A blood test can even check the individual�s biotoxins in their blood to see if mycotoxin present.
- Skin prick test: Healthcare professionals can take tiny amounts of mold and use a small needle to apply it onto the patient�s skin. This is to determine if the individual is breaking out in bumps, a rash or hives, then they are allergic to any mold species.
Diagnosing mycotoxin is known by many names, but it is mostly called mast cell disorder. Even though they are different and have different manifestations, diagnosing them in the body is essential to help individuals to heal their ailments. With technology getting better, healthcare physicians can detect mycotoxins in the body much faster.
Treating Mycotoxin
There are many ways to treat mycotoxin. Options include:
- Avoiding the mold whenever possible.
- A nasal rinse to flush out the mold spores that are in the nose.
- Antihistamines to stop the itchiness, runny noses, and sneezing due to mold exposure.
- A short term remedy for congestion is using decongestant nasal spray.
- Montelukast is an oral medication to reduce the mucus in a patent�s airways to lower the symptoms for both mold allergies and asthma.
- Doctors can recommend patients an allergy shot to build up the patient�s immunity to mycotoxin if the exposure is long term.
How to check for mycotoxin?
When individuals are checking for mycotoxins in their environment, it is best to hire professionals to help identify and remove it. A lot of individuals can look for black clusters growing in warm, moist rooms and can search for the causes of mold growth like any leaks, old food, papers, or wood. People can throw away the items that are affected by mold or that are contributing to mold growth. They can also remove the things that are not affected by mold exposure.

Wearing a mold-resistant suit, mask, gloves, and boots can protect individuals as they are getting rid of mildew and mold from their environment. Even purchasing a HEPA air purifier can help get rid of the spores to ensure that no allergens will affect the body�s immune system. When individuals are removing the mold exposure out of the affected area, they can cover the non-affected surfaces with bleach or a fungicidal agent. Then let it dry to prevent the mold from reproducing on the same area it has infected.
Conclusion
Since researchers are still doing a test on mycotoxin, mold exposure is still all around the world and in many forms. It can even contaminate food and places where it can thrive and grow. Individuals can prevent it from locating the source and can take precautions when they are exposed to the spores. If the individual is exposed to mycotoxin, going to the doctors to get tested is the best route to go. The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References
Borchers, Andrea T, et al. �Mold and Human Health: a Reality Check.� Clinical Reviews in Allergy & Immunology, U.S. National Library of Medicine, June 2017, www.ncbi.nlm.nih.gov/pubmed/28299723.
Do�en, Ina, et al. �Stachybotrys Mycotoxins: from Culture Extracts to Dust Samples.� Analytical and Bioanalytical Chemistry, Springer Berlin Heidelberg, Aug. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4939167/.
Gautier, C, et al. �Non-Allergenic Impact of Indoor Mold Exposure.� Revue Des Maladies Respiratoires, U.S. National Library of Medicine, June 2018, www.ncbi.nlm.nih.gov/pubmed/29983225.
Hurra�, Julia, et al. �Medical Diagnostics for Indoor Mold Exposure.� International Journal of Hygiene and Environmental Health, U.S. National Library of Medicine, Apr. 2017, www.ncbi.nlm.nih.gov/pubmed/27986496.
Jewell, Tim. �Black Mold Spores and More.� Black Mold Exposure, 1 June, 2018, www.healthline.com/health/black-mold-exposure.
Leonard, Jayne. �Black Mold Exposure: Symptoms, Treatment, and Prevention.� Medical News Today, MediLexicon International, 17 Sept. 2019, www.medicalnewstoday.com/articles/323419.php.
Pitt, John I, and J David Miller. �A Concise History of Mycotoxin Research.� Journal of Agricultural and Food Chemistry, U.S. National Library of Medicine, 23 Aug. 2017, www.ncbi.nlm.nih.gov/pubmed/27960261.
Sun, Xiang Dong, et al. �Mycotoxin Contamination of Rice in China.� Journal of Food Science, U.S. National Library of Medicine, Mar. 2017, www.ncbi.nlm.nih.gov/pubmed/28135406.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Supplements, Wellness
Supplements are essential as we take them for our overall health. Since we can�t produce supplements naturally, we make it in pill form or eat whole, nutritious food. When we don�t take our supplements, our bodies will not function properly, and we can have a severe health risk. In the last article, we took a look at what vitamins does to our micronutrients in our bodies to perform functional and healthy. Today we will discuss what some supplement that will help our micronutrients in our bodies.
The Supplements
Since supplements can come in many types of foods and can be found as pills in whole food stores in the vitamin section.� Here are some of the leading supplements to ensure that your body’s micronutrients are getting the essentials to promote a long healthy life.
Vitamin K1 and K2
Vitamin K is known for its role in blood clotting. With vitamin K1 and K2, they can provide the health benefits that will help you from getting a blood clot. Vitamin K was accidentally discovered in the 1920s and 1930s after researchers found that animals having a restricted diet leads to excessive bleeding.
Vitamin K1 (phylloquinone) is found in plants foods like leafy green vegetables. With K2, it is found in fermented foods and animal products. Vitamin K2 (menaquinones) can be produced by gut bacteria and help promote a healthy gut. These two vitamins are fat-soluble that share the same chemical structure and have different effects on your health.
Vitamin K1 can be absorbed quickly than vitamin K2 and can stay in the bloodstream for hours. Vitamin K1 is transported primarily to and used by the liver. Even though vitamin K1 is mostly found in plant foods, here are some of the food sources that are caulked filled with this vitamin and amazing when cooked.
- Kale
- Collard greens
- Spinach
- Turnip greens
- Broccoli
- Brussel sprouts
Vitamin K2 is mostly found in animal products that contain fat. Even though it provides fatty compounds, vitamin K2�s long side-chain allows it to circulate the blood longer than K1 can remain in the blood for days.� Here are some fermented food sources and animal products that vitamin K2 as MK-10 and MK-11.
- Natto
- Pork sausage
- Hard cheeses
- Porkchop (with the bone)
- Chicken (leg/thigh)
- Soft cheeses
- Egg yolk
Calcium

Calcium is one of the most essential supplements that is for all living organisms. It is found naturally in many foods and added to certain products like supplements. Calcium promotes bone health, and without it, bone density can happen when we don�t take in the supplement. It also helps regulate muscle contractions, including the beating of the heart muscle. When that happens, calcium helps the proteins in the muscle to carry out the work of the contraction. Here are some of the foods and drinks that are richly filled with calcium.
- Milk
- Cheese
- Yogurt
- Seaweed
- Beans
- Figs
- Tofu
Manganese

Manganese is an essential supplement for your brain and nervous system as well as many of your body�s enzyme system. Our body stores up to 20 mg of manganese in our kidneys, liver, pancreas, and bones. In a 2011 study, manganese helps form an antioxidant enzyme called SOD (superoxide dismutase). It helps break down one of the most dangerous free radicals called superoxide; into smaller components that are not harmful. Researchers also suggested that SOD is beneficial as a therapeutic agent for inflammatory diseases. Small amounts of manganese are present in these food sources.
- Raw pineapple and pineapple juice
- Pinto beans
- Spinach
- Black and green teas
- Sweet potato
- Almonds
- Instant oatmeal
Copper

Copper is an essential trace supplement that is necessary for survival. It is found in all the body tissues and plays a vital role in making red blood cells, maintaining nerve cells and the immune system. When you have sufficient copper in your diet, it may help prevent cardiovascular diseases and osteoporosis. Copper deficiency is a rare case, but low levels of copper can lead to anemia, loss of skin pigmentation, thyroid problems, and the rare disease Menkes disease. Since copper is found in a wide variety of foods, here are some excellent food sources that contain it.
- Oysters and other shellfish
- Whole grains
- Cocoa
- Black pepper
- Organ meats (liver and kidneys)
- Potatoes
- Dried fruit
Chromium
Also known as chromium picolinate, this supplement does serve several vital functions in the body. Chromium can improve your body�s blood sugar by impacting on the hormone insulin. Several studies indicate that people with diabetes take the chromium supplement to improve their blood sugar. While another study researched that people who are overweight or obese, taking the chromium supplement can lose weight.
Iron
Iron is one of the essential supplements that are vital to the human body. It helps hemoglobin function properly by transporting oxygen in the blood. Iron also plays a huge role as it functions in a variety of other vital processes in the body. With iron�s health benefits, the supplement can promote a healthy pregnancy, regulate body temperature, preserve universal energy and focus, help the gastrointestinal process, and support the immune system.

When we don�t get enough iron in our system, we do suffer from anemia, which causes fatigue, heart palpitations, pale skin, and breathless. So it is crucial that when we eat iron-rich foods so that way, we won�t have that deficiency. There are two types of dietary iron that we consumed, and they are known as heme and non-heme. These two forms are both animal source food and plant food, and here are what the food sources contain.
- Canned clams
- Cooked Pacific oysters
- Beef liver
- Lean ground beef
- Cooked spinach
- Dark chocolate
- Firm tofu
- Medium baked potato
Magnesium
Magnesium is an essential mineral that is found in the earth, sea, plants, animals, and humans. In our body, there is about 60% of magnesium in our bones. While the rest is in the muscles, soft tissues, and fluids, including blood. Magnesium helps to prevent problems with our bones, the cardiovascular system, diabetes and fights depression.

The recommended intake amount to take magnesium is 300-420mg per day for men and 310-320mg per day for women. We can get it from both food sources and supplements, here are some of the food sources that contain magnesium.
- Dark chocolate (70-85% cocoa)
- Cashews
- Quinoa, cooked
- Avocado
- Spinach, boiled
- Mackeral
Selenium

Selenium is an essential supplement that can help contribute thyroid hormone metabolism, process a healthy immune system, and protect against oxidative damage and infections in the body. Selenium deficiency is rare, but the supplement can be found in whole grains and animal products than fresh fruits and vegetables. Here are some of the food sources that contain selenium.
- Brazil nuts
- Tuna
- Brown rice
- White bread
- Egg
- Halibut
Omegas

The Omega supplements are very well known, especially Omega-3; which can help us with our brain, eyes, and immune health. Without the supplement, it can lead to reduced energy, loss of attention and concentration, dry, irritated skin problems, and many more symptoms. It is mostly found in fish and seafood as well as some vegetables and seed oils. Here are some of the omega supplements to help promote a healthy body.
- DHA (docosahexaenoic acid): This omega supplement helps with muscle growth.
- DPA (docosapentaenoic acid): This omega supplement is the most influential on reducing inflammation and helping people who are profiled for cardiac risk.
- EPA (eicosapentaenoic acid): This omega supplement is vital to boost the brain and moods.
- LA (linoleic acid): This omega supplement can�t be synthesized in the body, but does help fight cancer. It is needed to help out with omega 3 and is primarily found in beef.
Conclusion
Granted that these are only some of the supplements here that can help your body function properly. There are many supplements and vitamins out there in the world that are in both pill and food form to help our bodies grow and overall makes us healthier. These supplements and vitamins help us by making sure that our bodies don�t get sick and suffer from chronic diseases that we may encounter. So go out there and enjoy some whole, nutritious food that oozing with beneficial vitamins and supplements.
Cites:
Almquist, H J. �Early History of Vitamin K.� OUP Academic, Oxford University Press, 1 June 1975, academic.oup.com/ajcn/article-abstract/28/6/656/4716361?redirectedFrom=fulltext.
Beulens, Joline W J, et al. �The Role of Menaquinones (Vitamin K?) in Human Health.� The British Journal of Nutrition, U.S. National Library of Medicine, Oct. 2013, www.ncbi.nlm.nih.gov/pubmed/23590754.
Brinton, Eliot A, and R Preston Mason. �Prescription Omega-3 Fatty Acid Products Containing Highly Purified Eicosapentaenoic Acid (EPA).� Lipids in Health and Disease, BioMed Central, 31 Jan. 2017, www.ncbi.nlm.nih.gov/pubmed/28137294.
Calder, Philip C. �Docosahexaenoic Acid.� Annals of Nutrition & Metabolism, U.S. National Library of Medicine, 2016, www.ncbi.nlm.nih.gov/pubmed/27842299.
DeLoughery, Thomas G. �Iron Deficiency Anemia.� The Medical Clinics of North America, U.S. National Library of Medicine, Mar. 2017, www.ncbi.nlm.nih.gov/pubmed/28189173.
Di Bona, Kristin R, et al. �Chromium Is Not an Essential Trace Element for Mammals: Effects of a �Low-Chromium� Diet.� Journal of Biological Inorganic Chemistry: JBIC: a Publication of the Society of Biological Inorganic Chemistry, U.S. National Library of Medicine, Mar. 2011, www.ncbi.nlm.nih.gov/pubmed/21086001.
Fu, Xueyan, et al. �Measurement of Multiple Vitamin K Forms in Processed and Fresh-Cut Pork Products in the U.S. Food Supply.� Journal of Agricultural and Food Chemistry, U.S. National Library of Medicine, 8 June 2016, www.ncbi.nlm.nih.gov/pubmed/27191033.
Goodson, Amy. �10 Evidence-Based Benefits of Manganese.� Healthline, Healthline Media, 31 Aug. 2018, www.healthline.com/nutrition/manganese-benefits.
Gr�ber, Uwe, et al. �Magnesium in Prevention and Therapy.� Nutrients, MDPI, 23 Sept. 2015, www.ncbi.nlm.nih.gov/pubmed/26404370.
Harshman, Stephanie G, et al. �Vegetables and Mixed Dishes Are Top Contributors to Phylloquinone Intake in US Adults: Data from the 2011-2012 NHANES.� The Journal of Nutrition, Oxford University Press, July 2017, www.ncbi.nlm.nih.gov/pubmed/28566528.
Kaur, Gunveen, et al. �Short Update on Docosapentaenoic Acid: a Bioactive Long-Chain n-3 Fatty Acid.� Current Opinion in Clinical Nutrition and Metabolic Care, U.S. National Library of Medicine, Mar. 2016, www.ncbi.nlm.nih.gov/pubmed/26808265.
Li, Chang, and Hai-Meng Zhou. �The Role of Manganese Superoxide Dismutase in Inflammation Defense.� Enzyme Research, SAGE-Hindawi Access to Research, 2011, www.ncbi.nlm.nih.gov/pmc/articles/PMC3185262/.
Megan Ware, RDN. �Copper: Health Benefits, Recommended Intake, Sources, and Risks.� Medical News Today, MediLexicon International, 23 Oct. 2017, www.medicalnewstoday.com/articles/288165.php.
Naughton, Shaan S, et al. �Linoleic Acid and the Pathogenesis of Obesity.� Prostaglandins & Other Lipid Mediators, U.S. National Library of Medicine, Sept. 2016, www.ncbi.nlm.nih.gov/pubmed/27350414.
Newman, Tim. �Calcium: Health Benefits, Foods, and Deficiency.� Medical News Today, MediLexicon International, 21 Aug. 2017, www.medicalnewstoday.com/articles/248958.php.
Schurgers, Leon J, et al. �Vitamin K-Containing Dietary Supplements: Comparison of Synthetic Vitamin K1 and Natto-Derived Menaquinone-7.� Blood, U.S. National Library of Medicine, 15 Apr. 2007, www.ncbi.nlm.nih.gov/pubmed/17158229.
Serefko, Anna, et al. �Magnesium in Depression.� Pharmacological Reports: PR, U.S. National Library of Medicine, 2013, www.ncbi.nlm.nih.gov/pubmed/23950577.
Suksomboon, N, et al. �Systematic Review and Meta-Analysis of the Efficacy and Safety of Chromium Supplementation in Diabetes.� Journal of Clinical Pharmacy and Therapeutics, Centre for Reviews and Dissemination (UK), June 2014, www.ncbi.nlm.nih.gov/pubmed/24635480.
Tian, Hongliang, et al. �Chromium Picolinate Supplementation for Overweight or Obese Adults.� The Cochrane Database of Systematic Reviews, John Wiley & Sons, Ltd, 29 Nov. 2013, www.ncbi.nlm.nih.gov/pubmed/24293292.
Yasui, K, and A Baba. �Therapeutic Potential of Superoxide Dismutase (SOD) for Resolution of Inflammation.� Inflammation Research: Official Journal of the European Histamine Research Society … [Et Al.], U.S. National Library of Medicine, Sept. 2006, www.ncbi.nlm.nih.gov/pubmed/17122956.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Nutrition, Vitamins, Wellness
Mostly everyone takes their vitamins in any shape and form. It can be from the foods that we eat to the supplements and vitamins pills that we make throughout the day. We can get the boost of micronutrients in our bodies with vitamins and foods. It can help with our diets when we are trying to get a head start in our healthy lifestyle change through healthy, nutritious, whole foods. Without it, it can cause our bodies to react differently with ailments. For example, a person has a healthy lifestyle, but they are feeling out of place in their daily lives; it might be due to their low levels of the vitamins they are not taking. We will be taking a look at the micronutrition in vitamins and supplements in this two-part series for the body.
The Vitamins
Vitamins are essential for the body since we can�t produce them naturally. When we feel sluggish or horrible, it might be due to the low vitamin intake that we are missing to make us feel better. Here are some of the vitamins that can help your body if you feel a bit weak in life.
Vitamin A

Vitamin A is a fat-soluble compound that is an essential nutrient for the body. It is stored in the liver for later use and is transferred to the tissues when needed. Vitamin A helps maintain the integrity and function of all surface tissues and the eyes. Vitamin A has two forms which are retinol and retinyl esters and provitamin A carotenoids. Retinol and retinyl esters health benefits can help prevent macular degeneration to your eyes, and with the provitamin A carotenoids can have potent antioxidants to fight off free radicals in your body.
Deficiencies: Having a Vitamin A deficiency can lead to blindness in the eyes of some people. Anyone who has a deficiency in Vitamin A can have skin issues like hyperkeratosis and acne. Not only that, but it can increase any infections as well as have pregnancy complications for pregnant women.
Food Sources: Here are some of the foods that are very rich with vitamin A that are all carotenoid-rich in both animals and plants.
- Egg yolks
- Beef liver
- Cod liver oil
- Salmon
- Sweet potatoes
- Carrots
- Dandelion greens
- Cabbage
Vitamin B

All B vitamins are water-soluble, and your body can�t store them. They are used to reduce fatigue and boost your mood. There are 8 B vitamins are vital and have many essential functions for maintaining good health.
- B1 (thiamine): Thiamine helps our bodies metabolism by helping convert nutrients into energy. Some food sources include pork, sunflower seeds, and wheat germ.
- B2 (riboflavin): Riboflavin converts food into energy and acts as an antioxidant in the body. Some of the food sources that are high in riboflavin are organ meats, beef, and mushrooms.
- B3 (niacin): Niacin plays a role in cellular signaling, metabolism and DNA productions, as well as repairs it as well. Some food sources include chicken, tuna, and lentils.
- B5 (pantothenic acid): Like other B vitamins, pantothenic acid helps our bodies obtain energy from the food we eat. It also involves hormone and cholesterol production. Some food sources include liver, fish, yogurt, and avocado.
- B6 (pyridoxine): Pyridoxine helps produces red blood cells in the body. It helps create amino acid metabolism and neurotransmitters for the body. Foods that are highly rich with this vitamin are chickpeas, salmon, and potatoes.
- B7 (biotin): Biotin is highly essential for carbohydrate and fat metabolism and can regulate gene expression in the body. The best food sources that contain biotin are yeast, eggs, salmon, cheese, and liver.
- B9 (folate): Our bodies need folate for cell growth, amino acid metabolism, the formation of red and white blood cells as well as proper cell division. Folate can be found in foods like leafy greens, liver, beans and in supplements like folic acid.
- B12 (cobalamin): One of the best- known of all the B vitamins, B12 is vital for neurological function, DNA production, and red blood cell count. It can be found naturally in animal food sources like meats, eggs, seafood, and dairy.
Deficiencies: Even though taking the B vitamins are essential, there are side effects to taking a high dose of the vitamin, especially B3 and B6. Some of the side effects include vomiting, high blood sugar levels, skin lesions, nerve damage, and even liver damage.
Vitamin C

Vitamin C is one of the most essential vitamins since it can�t be produced by the body. It has so many roles and has been linked to many impressive health benefits. It can help boost antioxidant levels, reduce high blood pressure, and heart disease risk. It can protect your body against any gout attacks and reduce your risk of dementia while improving your iron absorption and boosting your immunity.
Deficiencies: When you don�t take enough vitamin C, it can raise up your blood sugar. Without it, you can develop scurvy if you don�t have enough of vitamin C in your system. You can get really sick, and your immune system will be shot if you don�t take vitamin C.
Food Sources: The most common way to get vitamin C in your body is through citrus fruit. There are lots of foods that contain vitamin C and are very delicious.
- Red and green peppers
- Oranges and orange juice
- Kiwi
- Guava
- Broccoli
- Strawberries
- Brussel sprouts
- Tomato juice
- Cantaloupe
Vitamin D3

Also known as the sunshine vitamin, vitamin D3 is essential for maintaining healthy bones and teeth. It can support the immune system, brain, and nervous system by keeping it healthy. It will even regulate insulin levels and help managing diabetes. However, vitamin D3 can be synthesized to our body whenever sunlight hits our skin.
Deficiencies: Even though the body can create vitamin D, there many reasons that vitamin D deficiency can occur. If a person has a darker skin color and uses sunscreen to reduce the absorption of UVB (ultraviolet radiation B) rays from the sun. They can stop the production of vitamin D. Some of the symptoms of vitamin D deficiency include getting sick more, fatigue, muscle pain, and depression. And if it continues for long periods, it can lead to obesity, diabetes, hypertension, chronic fatigue syndrome, fibromyalgia, and osteoporosis, just to name a few.
Food Sources: There are a few foods that contain vitamin D naturally. And for vitamin D3 it is mostly animal produced.
- Salmon
- Sardines
- Egg yolk
- Shrimp
- Milk (fortified)
- Cereal (fortified)
- Yogurt (fortified)
Vitamin E

Vitamin E is one of the most essential nutrients that is available as a dietary supplement and can occur naturally in foods. It is an antioxidant that can help protect your cells damage and is fat-soluble. Researchers have investigated that vitamin E can be used as a treatment for various degenerative diseases, including high blood pressure, heart disease, and cancer. It is a rare case for a vitamin E deficiency; however, it is a rare condition that is being researched.
Since Vitamin E is the most common nutrient found in most foods, here are some of the foods, including cooking oils that are exceptional.
- Wheat Germ Oil
- Sunflower seeds
- Almonds
- Hazelnut Oil
- Goose meat
- Peanuts
- Mango
Conclusion
So with these vitamins, it can help your body feel so much better in the long run. Without them, our bodies will have various health problems that can hurt us in the long haul. When we take these vitamins, our bodies began to heal properly, and we can see that our moods are a bit better. We can have normal functions without the vitamins because we eat the food that contains them, but when we need that extra boost of energy, vitamins are the way to go.
Cites:
Basavaraj, K H, et al. �Diet in Dermatology: Present Perspectives.� Indian Journal of Dermatology, Medknow Publications, 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC2965901/.
Chiu, Zelia K, et al. �Patterns of Vitamin D Levels and Exposures in Active and Inactive Noninfectious Uveitis�Patients.� Ophthalmology, U.S. National Library of Medicine, 11 July 2019, www.ncbi.nlm.nih.gov/pubmed/31519386.
Choi, Hyon K, et al. �Vitamin C Intake and the Risk of Gout in Men: a Prospective Study.� Archives of Internal Medicine, U.S. National Library of Medicine, 9 Mar. 2009, www.ncbi.nlm.nih.gov/pubmed/19273781.
Ettarh, R R, et al. �Vitamin C Lowers Blood Pressure and Alters Vascular Responsiveness in Salt-Induced Hypertension.� Canadian Journal of Physiology and Pharmacology, U.S. National Library of Medicine, Dec. 2002, www.ncbi.nlm.nih.gov/pubmed/12564647.
Institute of Medicine (US) Panel on Micronutrients, Unknown. �Vitamin A.� Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc., U.S. National Library of Medicine, 1 Jan. 1970, www.ncbi.nlm.nih.gov/books/NBK222318/.
Kubala, Jillian. �Vitamin A: Benefits, Deficiency, Toxicity and More.� Healthline, 4 Oct. 2018, www.healthline.com/nutrition/vitamin-a.
Martel, Julianna L. �Vitamin B1 (Thiamine).� StatPearls [Internet]., U.S. National Library of Medicine, 14 Aug. 2019, www.ncbi.nlm.nih.gov/books/NBK482360/.
Megan Ware, RDN. �Vitamin D: Health Benefits, Facts, and Research.� Medical News Today, MediLexicon International, 13 Nov. 2017, www.medicalnewstoday.com/articles/161618.php.
Meyer-Ficca, Mirella, and James B Kirkland. �Niacin.� Advances in Nutrition (Bethesda, Md.), American Society for Nutrition, 16 May 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4863271/.
N/A, Unknown. �Office of Dietary Supplements – Vitamin E.� NIH Office of Dietary Supplements, U.S. Department of Health and Human Services, 0AD, ods.od.nih.gov/factsheets/VitaminE-HealthProfessional/.
O’Leary, Fiona, and Samir Samman. �Vitamin B12 in Health and Disease.� Nutrients, Molecular Diversity Preservation International, Mar. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC3257642/.
Ozuguz, Pinar, et al. �Evaluation of Serum Vitamins A and E and Zinc Levels According to the Severity of Acne Vulgaris.� Cutaneous and Ocular Toxicology, U.S. National Library of Medicine, June 2014, www.ncbi.nlm.nih.gov/pubmed/23826827.
Pham-Huy, Lien Ai, et al. �Free Radicals, Antioxidants in Disease and Health.� International Journal of Biomedical Science : IJBS, Master Publishing Group, June 2008, www.ncbi.nlm.nih.gov/pubmed/23675073.
Senoo, Haruki, et al. �Hepatic Stellate Cell (Vitamin A-Storing Cell) and Its Relative–Past, Present and Future.� Cell Biology International, U.S. National Library of Medicine, Dec. 2010, www.ncbi.nlm.nih.gov/pubmed/21067523.
Wong, Cathy. �Benefits of Vitamin C You May Not Know About.� Verywell Health, Verywell Health, 17 July 2019, www.verywellhealth.com/the-benefits-of-vitamin-c-supplements-89083.
Zempleni, Janos, et al. �Biotin.� BioFactors (Oxford, England), U.S. National Library of Medicine, 2009, www.ncbi.nlm.nih.gov/pubmed/19319844.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Gut and Intestinal Health, Nutrition, Wellness
Today, we will be talking about what does the protein compounds and the peptide compounds do when a patient is being tested for food sensitivity. And we will also discuss what the Lectin and Dairy Zoomer do when a patient has a reaction to those types of food groups. In the last article, we mentioned about immunoglobulins in the intestinal barrier. And what do IgA and IgG antibodies do to the peptide and protein level?
Proteins vs. Peptides
So let us take a look at proteins and peptides since this is what Vibrant Food Zoomers are actually testing on a patient. Remember that the Food Zoomers are testing the peptides in the whole protein and testing all the links to see what the patient is actually sensitive to the foods they are consuming.
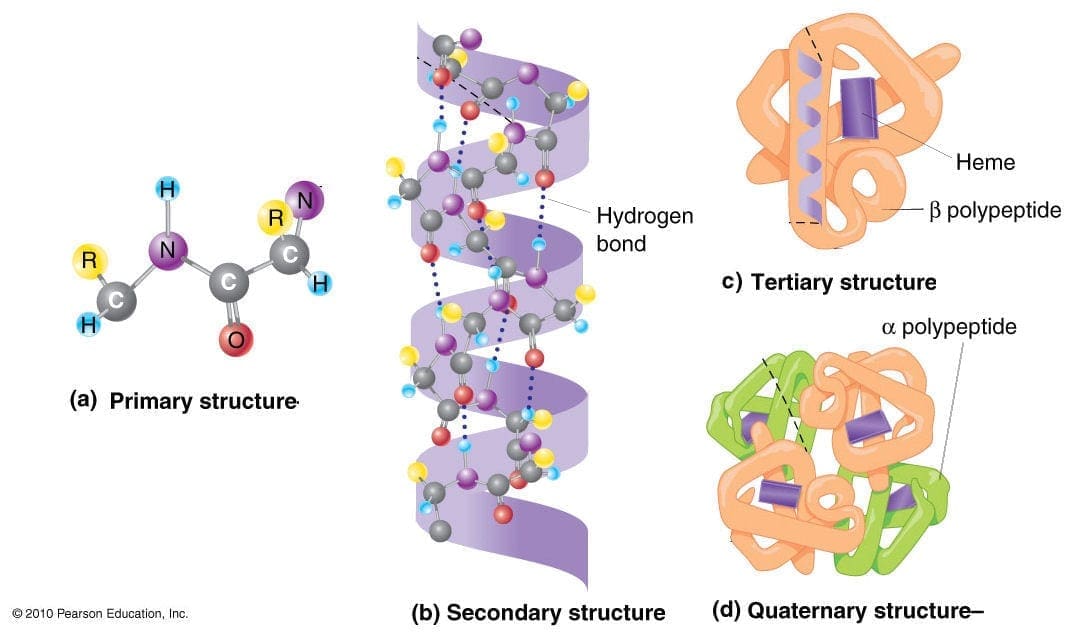
Proteins
Protein is basically abundant biomolecule that is consist of one or more long chains of amino acid residues. Proteins can be found in whole foods like meats and vegetables that can help the muscles in our bodies. In the last article, we talked about how IgA and IgG antibodies are used for food sensitivity testing.
However, there is a limitation of a whole protein food sensitivity testing on a patient. Practitioners do make the assumption that the patient�s gut barrier is functional and intact since there are no signs of a leaky gut syndrome presented in the results. But, if that patient has the leaky gut syndrome, then the food sensitivity test will reflect what the patient has been eating. Another assumption is that the patient�s HCI and digestive enzymes are sufficient for tolerable proteolysis. Which means that those enzymes are breaking down whole proteins into smaller peptides.
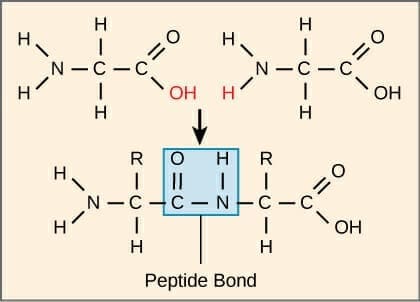
Peptides
Peptides are what in protein molecules as they are short chains of amino acids and are linked by the peptide bonds. When they are being tested by the food sensitivity tests, the reproducibility is higher. It doesn�t rely on the excess HCI (hydrochloric acid) or enzymes. What the test eliminates is the cross-reactivity because peptides in proteins are not going to have molecular mimicry to other unrelated proteins.
The antibodies are highly specific to the peptides because they are not going to be generalized or more massive antibodies of proteins since cross-reactivity is eliminated. Another thing is that the peptide test does is that it can measure thousands of peptides in one protein for a full spectrum of reactivity.
When patients are coming in with digestive problems and inflammatory condition/symptoms, practitioners take note that a lot of patients commonly have hypochlorhydria and deficiencies of enzymes and/or bile acids. Most patients sometimes have moderate to severe impairment of the intestinal barrier. When that happens, local doctors discuss with them that they may have to change their diets slowly but surely. And with integrative functional medicine that can occur.� Local practitioners look at their patient�s ailments and start detoxifying their bodies slowly. This helps their bodies heal and recommend them whole, nutritious, organic foods, and supplements to help repair the body naturally. Sometimes medicines can cause disruption to our bodies, however with whole natural foods and specific diets, it can help restore our bodies. Plus making sure that we exercise to make our bodies feel good and look good.
So now that we understand what proteins and peptides do when they are being tested. Let�s take a look at the food zoomers that can help you in case you have a sensitivity to these food groups. These are the Vibrant Lectin Zoomer and the Dairy Zoomer.
Lectin Zoomer
The Lectin Zoomer is consist of a handful of lectins and a handful of aquaporins. The most common lectins that people consume are barley, bell pepper, chickpea, corn, cucumber, potato, etc. And the most common aquaporins that people consume are spinach, soybean, tomato, tobacco, etc.
Difference between Lectins and Aquaporins
The difference between lectins and aquaporins is that lectins are sugar-binding proteins that are found in both animals and plants, which can bind to the carbohydrate structures on cells. While aquaporins are water channels that are found in cavities in both plants and humans. Some aquaporins can cross-react and can lead to primarily neurological symptoms.
How Problematic are Lectins?
Some studies show cell toxicity in humans is done by using extreme cytotoxic lectins. Ricin, for example, is a common biological warfare element that is not from the commonly consumed legumes or grains. It contains cytotoxic lectins and is being consumed by animals like mice or pigs. The assumption is being made that there are similarities with humans and animal gut glycosylation (the process of sugar-binding) in these situations.
Unfortunately, though it hasn�t been demonstrated thoroughly. But lectins have biological activity in the human body. They have been used as a cancer treatment mechanism because they can agglutinate cancer cells. Which means that they produce cytotoxicity to cancer cells and can actually carry chemotherapy across cancer cell membranes.
Even though that is a good thing, lectins can facilitate the bacterial endotoxins across the epithelial barrier and go into the peripheral tissues. And that can cause inflammation to the intestinal epithelial barrier in the small intestines. Animals studies show that raw lectin consumptions can cause hemagglutinating effects, causing inflammation.
But we as humans don�t eat raw lectins because they are cooked, not pressurized cook. Certain foods that are lectins can be eaten raw or cooked. But animal studies stated that they are using for these studies are grain and legume lectins that are raw like beans and grains. But the upside is that lectins can affect the metabolism of nutrients to increase fat loss which is a positive side effect.
Measuring the Sensitivity to Lectins
On the Food Zoomers test, lectins are really not included in each analysis, except for the Wheat Zoomer. Surprisingly, a Food Zoomer may be non-reactive, but whoever is sensitive to a lectin component in the food they eat, may be reactive. So when that happens, it is necessary to eliminate the food temporarily.
If you are sensitive to a particular food, you can have a Food Zoomer and a lectin Zoomer combine. Because if you are sensitive to the food you consume, and it doesn�t show up on the Food Zoomer, but it shows up on the Lectin Zoomer. Then you should eliminate it from your diet for a bit until you retake the test.
Conditions Associated with Lectins
If you do have a lectin sensitivity, here are some of the terms that can affect your body.
- Arthritis/rheumatoid arthritis
- Connective tissue disorder
- Gastrointestinal inflammation
- Intestinal permeability
- Possible cancer in established cancer patients
Now let�s take a look at the Dairy Zoomer and its functions if you are sensitive to whole dairy products.
Dairy Zoomer
The Dairy Zoomer is a peptide level assessment of the full spectrum of immune response possible to proteins in cow�s milk dairy. What this means that the Dairy Zoomer is only specific to cow�s milk. Since some proteins in cow�s milk are similar enough in the molecular structure to have the same homology to goat or sheep�s milk.
This means that these other kinds of milk may be potential can cause inflammatory in some individuals. The oral challenge for alternative types of fluid may be warranted, but use your best clinical judgment after the intestinal barrier is healed.
What the Dairy Zoomer does is that it takes the milk protein and breaking each individual protein down to its different peptides. If you are wondering if the Dairy Zoomer is a test for lactose intolerance, it is not. Since lactose intolerance is not an immune-based reaction to dairy and does not involve any protein constituents of the food, therefore no antibodies are being generated.
What it is going to test for is the casein and whey proteins in the milk product from all animals, and the ratio of these proteins will vary by species. But all the proteins and milk will generally fall into one of these two proteins.
What to do with the results?

Once your patient comes back after taking the Food Zoomers test, here are some of the things to look for when you are retesting them.
- If there are any IgA antibodies still in your patient, warrant an immediate elimination, regardless that it�s moderate or positive.
- If there are any Moderate IgG antibodies in your patient, then it should be eliminated in the short term. Then rotate after a 30-60-day elimination and assessing the status of the intestinal permeability to confirm that that gut barrier is no longer �leaky.�
- If there is a positive IgG result, then it should be eliminated long term and only reintroduced after 90+ days and confirm of an intact intestinal barrier.
Conclusion
So all in all, food sensitivity combine with the food zoomers test are an excellent way to help your body, especially the intestinal system. The Food Zoomers we used is functional for our patient�s wellness. Because we want to get rid of the excess antibodies and heal our patient�s body through the use of functional medicine.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Chiropractic, Functional Medicine, Functional Medicine Series, Wellness
As a doctor who practices functional medicine, Dr. Jimenez utilizes the Neural Zoomer Plus. This is a blood test that analyzes neurological autoantibodies which offer very specific antibody-to-antigen recognition. The Neural Zoomer Plus tests the reactivity an individual has to 48 neurological antigens. These neurological antigens may be related to neurological disease and can help individuals assess the presence of a neurological condition.

There are 48 markers that are measured and they can be summed up and categorized into 7 larger groups. These groups include demyelination antigens, blood-brain barrier disruption, optical and autonomic nervous system disorders, peripheral neuropathy, neuromuscular disorders, brain autoimmunity, brain inflammation, and infections. (For a full list of the markers that the Neural Zoomer Plus measures, click here).�
The truth of the matter is that autoimmune disorders affect 5-10% of the general population and can target virtually and structure within the central or peripheral nervous system. Symptoms of an autoimmune disorder involving the CNS/PNS include but are not limited to:�
- Cognitive decline
- Memory loss
- Ataxia
- Balance problems
- Neuropathy
- Alzheimer’s disease
- Multiple sclerosis
- Encephalitis
- Muscle spasms
- Huntington’s disease
- Epilepsy
- Parkinson’s disease
- Dementia�
- Myasthenia gravis
- Muscle stiffness/rigidity�
- Optical decline
- Neuromyelitis Optica
- History of concussion
- Autism
- PANDAS/ANDAS/OCD
- Demyelinating diseases�
 �
�
Having the tools to prevent a disease or disorder can be life-changing. With the ability to assess these markers, the rate of cognitive decline can steadily reduce. If you suffer from any of the above symptoms, the Neural Zoomer Plus may be right for you.
The intention of having our patients complete a Neural Zoomer Plus is to help us detect an individual’s IgA, IgG, and IgM sensitivity to antigens, down to the peptide level. Once we receive the results, not only do we have a resource that aids in the early detection of neurological diseases, but we also have a path. This path allows us to create a personalized prevention plan that will focus on the patient along with their lifestyle. – Kenna Vaughn, Senior Health Coach�
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gastro Intestinal Health, Gut and Intestinal Health, Wellness
The usage of integrated functional medicine is essential when it comes to our bodies overall health. Local practitioners and health coaches, talk with patients on what seems to bother them. Sometimes it is a simple adjustment, but mostly it�s what�s causing them problems on the inside. Some patients have inflammation around their intestinal epithelial barriers, and it can cause a leaky gut.
In the previous article, we talked about what the microbiomes do in our intestines and what is their functions are in the intestinal epithelial barrier. However, today we will discuss what the immunoglobulins antibodies do with proteins and peptides in the intestinal permeability. As well as explaining what the Lectin Zoomer and the Dairy Zoomer does when a patient has a food sensitivity and needs testing in a two-part series about the intestinal permeability and food zoomers.
Immunoglobulins
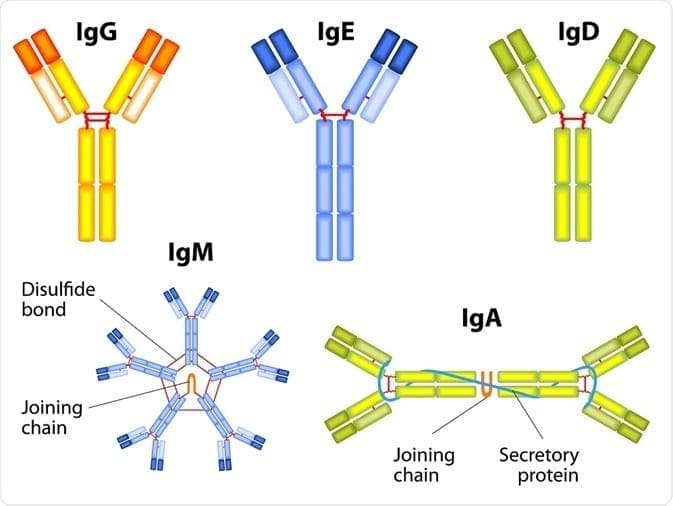
The first thing that we need to know is that immunoglobulins are immune-mediated reactions. So anything that involves the immune system will cause a hypersensitivity reaction to one or more food or foreign proteins, and their presence can be of one or more types of immunoglobulins.
There are 3 terms of hypersensitivities that can be involved with immunoglobulins:
- Allergies are the ones that are most common and are associated with anaphylaxis. Patients can have a very severe and acute immediate reaction to specific allergens like food or environmental like pollen or a bee sting.
- Non-allergies, sensitivity reactions involved either chemical mediators or antibody reactions.
- Food intolerances are non-immune-mediated reactions, and a good example is Lactose Intolerance or a bile salt deficiency. These can make somebody who has a food intolerance, can�t digest fat.
These three terms are often mistaken and used interchangeably clinically, but they are entirely different since they are not interchangeable. Especially when it comes to sensitivities and intolerances because those two commonly get used in place of each other, but they are totally different.
If you are testing your patient�s immunoglobulins, remember that antibodies are particular to each type of foreign substances and can be in three types of hypersensitivity. Antibodies will only bind an react to the specific proteins of the foreign material but not to the substance�s extract. The most common ones are type 3, where it involves IgG, IgA, and IgM. This type can tell us what cells and mechanisms are involved.
Type 3 Hypersensitivity Mechanisms
Here are the types of mechanisms that are involved with Type 3 immunoglobulins.
- Antigens are a foreign protein that is present and is recognized as a threat or non-self.
- Antibodies will bind to the antigen to neutralize or keep it from linking to anywhere else in the body. This is where the immune complex is formed.
- Immune complexes insert themselves into the small blood vessel, joints, tissues, and glomeruli, causing symptoms to the body.
- They are far more capable of interacting with complement proteins to form medium-sized complexes; which has an excess amount of antigens that are high pathogenic.
- However, once the immune complex is in the tissue, it can induce an inflammatory response and cause damage to the body. This damage is the result of the action of cleaved complement anaphylatoxins, which can mediate a mast cell degranulation.
- With the recruitment of inflammatory cells in the tissue, it can lead to tissue damage through phagocytosis.
IgA and IgG
In a previous article, we mentioned the mechanics of the intestinal permeability. However, we going to discuss what IgA antibodies and IgG antibodies do to the gut and to the entire body.
IgA Antibodies
IgA antibodies are found in the body where there is a mucosal lining around the areas like the nose, breathing passages, digestive tract, ears, eyes, and vaginal region. These surfaces are exposed to the outside of the environment either by air, food, or other foreign substances regularly.
IgA antibodies actually protect the body surfaces that are exposed to outside foreign substances, and these antibodies can be found in saliva, tears, and blood.
In the gut, however, it can bind to the mucosal layer on the top of the intestinal epithelial cells to form a barrier to neutralizing threats before they reach the cell. And that is very important, especially since IgA is like an insurance policy for your gut.
IgA antibodies are considered as non-inflammatory. Which means that they don�t stimulate inflammatory processes in the body like IgG does. They do, however, create a mucosal response to a foreign antigen, and it is usually microbial (ex., bacteria, yeast, viruses, parasites) or microbial toxins. They can also generate a response to pollutants, toxins, and recognized undigested food as a foreign protein.
In the intestinal lumen, IgA can be indicative of an immune response stimulated by T-b cell interaction. So a healing intervention, if a patient has an abundance of IgA antibodies may need to target TH1 and TH2 balance so it can regulate T-reg production.
IgG Antibodies
IgG antibodies are found in all body fluids. They happen to be the smallest but the most common of all antibodies as they make-ups about 75% to 80% of antibodies found throughout the entire body. These antibodies are essential as they fight against bacterial and viral infections, and they are the only type that can cross the placenta.
They do indicate exposure to a specific antigen, but they don�t always necessarily indicate active inflammation; however, they can contribute to it in a dose-independent.
Why measure IgA and IgG?
So why do we measure IgA and IgG? Surprisingly some people don�t produce as much or any IgA antibodies, and therefore, local practitioners would not know if their patients have formed a reactivity to an antigen if they don�t check their IgG levels.
Surprisingly, some IgG antibodies are not an indicator of actual inflammation or disease process. Some IgG antibodies are formed in response to a protein as sort of a tracker in the body but do not elicit a reaction. However, IgA antibody is coupled with IgG to indicate a bit stronger immune response to an antigen in some cases.
IgA and IgG in the Protein Level
IgA and IgG testing in the protein level is what the food sensitivity tests are looking at. They look for the whole protein, which is the extract level. All food sensitivity test looks for residues of carbohydrate and lipid-based particles. It�s not pure protein but that what the test does, it seems for the reactive compound. Some of the strengths are that the test gives an acute measure of IgG and IgA to a specific protein. It can also be suitable for associating Type 3 reactions involving IgG and IgA complexes, and if the IgG is pathogenic, then it will be beneficial.
Some of the weaknesses are that IgG can be a protective antibody, and it may be a good thing. It means that the immune system is handling it and there�s nothing necessarily wrong about that. IgG and IgA antibodies represent whole proteins being presented to the immune system can it also be an indicator that a patient may have a lack of sufficient digestive capacity when many food sensitivities are being detected.
IgG and IgA in the Peptide Level
When IgG and IgA are being tested at the peptide level, this is where the food zoomer test focuses on. This is because there is a high level of antibodies specificity, cross-reactivity is minimized if not completely eliminated. The concept of foods that are cross-react, for example, gluten, might cross-react to other foods that are similarly shaped in their molecular structure, then you should eliminate the gluten out of your diet as well as the foods that are in contact with them.
However, if the antibodies to gluten are being picked up at the peptide level, then it won�t look at those foods that are being cross-reactive to gluten. The antibodies will only bind to the individual peptides than the whole protein. This will be a more accurate assessment of whether or not that the patient is sensitive to the foods their body is reacting to.
What is Loss of Oral Tolerance?
Loss of oral tolerance is a term used to describe the phenomenon of someone developing a sensitivity, whether it is accompanied by symptoms or not, and it�s usually a commonly consumed or semi-regularly consumed food. When that happens, there is a production of inflammatory cytokines and antibodies that will respond to the continued exposure to the food.
For the inflammatory responses to be eliminated, patients have to remove the offending food for about 3 to 4 weeks if IgA antibodies are present or 3 to 6 months if the IgG antibodies are present as well. This is the only way for the antibodies to disappear, and the intestinal permeability can heal. But the disappearance of antibodies does not guarantee that oral tolerance has been established. If you are retesting a patient and if the antibodies are gone, that indicates that the patient has done an excellent job in eliminating that food from their diet. However, the only way to know is to reintroduce the food and retest after a few months, just to make sure that no antibodies are being produced after the intestinal barrier has been fully healed.
Conclusion
All in all, that is what the intestinal permeability does when we have IgA and IgG antibodies and what do they do when there is food sensitivity in the body.� However, it is crucial that our patients understand that we here at Injury Medical Clinic, take the time to study what causes inflammation in our patients and using integrated functional medicine to make sure that their intestines are being healed naturally. In the next article, we will discuss the difference between peptides and proteins, and about the Lectin and Dairy Zoomer.






