
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Nutrition, Remedies, Wellness
The cold and flu season can cause havoc on a person�s body during the colder seasons. An individual can feel overly tired, congested, the body has aches and shivers, and lastly, the immune system will work overtime to help fight off the germs. When this happens, many remedies can help these symptoms when a person feels a little bit under the weather. They help the body give that extra boost to recover from cold and flu symptoms and can provide the body a chance to rest.
When anyone is starting to feel sick, an important note is to try and get as much rest as they possibly can. It can be anything like getting more sleep, scaling down on exercising, or take some time off of work to heal more quickly. In this article, here are some of the top 5 foods to help the body improve and recover from the cold and flu season, with some additional remedies to boost the immune system as well.
Soups

Soups are one of the most excellent sources of feeling better during cold and flu season. They are easily digestible and helps soothe the body by containing ample waters to keep it hydrated. Water-based soups like chicken noodle, Hippocrates soup, and vegetable soup incorporates all the essential nutrients that the body needs when it is the colder season, helping to combat the flu.
Garlic

Garlic has a wide variety of health benefits that can help the body during the cold and flu season. It can help reduce the risk of heart diseases, improve mental health, and enhance the immune system. Studies have shown that whole garlic contains a compound called alliin. When garlic is chopped, chewed, or crushed, it will help boost the disease-fighting response of white blood cells in the body when they are encountering viruses that cause the common cold or flu.
Studies also stated that garlic helps support neurodegenerative health, cardiovascular health, and compromised liver functioning from excessive alcohol use. Researchers at the Toxicology, School of Public Health, Shandong University in China, have isolated the garlic compound, DADS (diallyl disulfide), as the main compound that helps protects the body from ethanol-induced oxidative stress.
Foods That Are Rich in Vitamin C

Foods that contain vitamin C is highly essential when it comes to battling the cold or flu. Vitamin C is a powerful, potent supplement that has antioxidants and immune system boosters that protects the body from environmental factors like reducing oxidative stress, prevent and treat respiratory and systemic infections. With vitamin C-rich foods, they contain essential minerals, vitamins, and high in flavonoids that help individuals who don�t feel like eating or preferring bland foods to consume when they are sick. Initially, they can eat vitamin C rich food by either juice or soup. Here are some delicious fruits and juices that contain a high amount of vitamin C to combat the cold and flu.
- Guava
- Strawberries
- Tomato juice
- Oranges and Orange juice
Apple Cider Vinegar

Apple Cider Vinegar can provide many minerals and enzymes that can fight off pathogens that can be caused by the common cold or flu. A 2011 study has shown that the probiotics in apple cider vinegar have an immune-boosting effect that can shorten the duration of a cold when an individual drinks apple cider vinegar. Taking apple cider vinegar with a glass of water can also help the body when it is not cold and flu season. Apple cider vinegar helps inhibits bacterial growth, can support healthy blood pressure levels in the body, as well as an excellent addition to the medicine cabinet during cold and flu season.
Ginger

Ginger is a medicinal root plant that has been used for thousands of years. This root has been known to relieve motion sickness and nausea in the digestive system. Studies have shown that 70% of the immune system is found in the gut, and so it is highly essential that the digestive system in the body is working efficiently. Since ginger is made up of hundreds of compounds, some of them have potent antioxidants and can help support healthy inflammatory pathways in the body. Ginger can be found as a fresh root, dried, as an extract or oil, tinctures, capsules, and lozenges. Here are some of the foods that contain ginger to help the body fight the common cold or flu.
- Ginger tea
- Curry
- Gingerbread
- Cookies
- Gingersnaps
- Ginger ale
 “It is highly essential to stay hydrated during the cold and flu season. Ample fluids like water, coconut water, and herbal teas are the first line of defense.
“It is highly essential to stay hydrated during the cold and flu season. Ample fluids like water, coconut water, and herbal teas are the first line of defense.
Additionally, getting a good night’s sleep helps the immune system in the body recover faster. It is also essential to avoid eating foods like processed foods, alcohol, soda, fried foods, and dairy when it is cold and flu season. Since it can cause inflammation and aggravate the immune system when the body is trying to recover from being sick.”- Dr. Alex Jimenez D.C., C.C.S.T. Insight – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Conclusion
All in all, when it is cold and flu season, people can start stocking up on these five remedies and taking antibiotics to get a head start on not getting sick. When the body does get sick, taking these remedies, getting lots and lots of rest, staying hydrated, and relaxing can ensure that the body will recover faster. Since food matters to people�s health, it�s vital to give the body the nourishment it needs for the cold and flu season.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this declaration.
So the mechanisms of an autoimmune disease can be either by genetics or by environmental factors that can cause an individual to have problems in their body. There are many autoimmune diseases, both common and rare, that can affect the body. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Biotics Education Team, Unknown. �5 Foods to Eat During the Cold & Flu Season.� Biotics Research Blog, 16 Sept. 2019, blog.bioticsresearch.com/5-foods-to-eat-during-the-cold-flu-season.
Borlinghaus, Jan, et al. �Allicin: Chemistry and Biological Properties.� Molecules (Basel, Switzerland), MDPI, 19 Aug. 2014, www.ncbi.nlm.nih.gov/pubmed/25153873.
Carr, Anitra C, and Silvia Maggini. �Vitamin C and Immune Function.� Nutrients, MDPI, 3 Nov. 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5707683/.
Das, Arabinda, et al. �Garlic Compounds Generate Reactive Oxygen Species Leading to Activation of Stress Kinases and Cysteine Proteases for Apoptosis in Human Glioblastoma T98G and U87MG Cells.� Wiley Online Library, John Wiley & Sons, Ltd, 23 July 2007, onlinelibrary.wiley.com/doi/full/10.1002/cncr.22888.
Felman, Adam. �Antibiotics: Uses, Resistance, and Side Effects.� Medical News Today, MediLexicon International, 18 Jan. 2019, www.medicalnewstoday.com/articles/10278.php.
Newman, Tim. �Congestive Heart Failure: Causes, Symptoms, and Treatments.� Medical News Today, MediLexicon International, 3 Jan. 2018, www.medicalnewstoday.com/articles/156849.php.
Song, Fu-Young, et al. �The Activation of HO-1/Nrf-2 Contributes to the Protective Effects of Diallyl Disulfide (DADS) against Ethanol-Induced Oxidative Stress.� Biochimica Et Biophysica Acta (BBA) – General Subjects, Elsevier, 28 June 2013, www.sciencedirect.com/science/article/pii/S0304416513002882.
Surh, Y J, et al. �Chemoprotective Properties of Some Pungent Ingredients Present in Red Pepper and Ginger.� Mutation Research, U.S. National Library of Medicine, 18 June 1998, www.ncbi.nlm.nih.gov/pubmed/9675305.
Vighi, G, et al. �Allergy and the Gastrointestinal System.� Clinical and Experimental Immunology, Blackwell Science Inc, Sept. 2008, www.ncbi.nlm.nih.gov/pmc/articles/PMC2515351/.
Watson, Kathryn. �Apple Cider Vinegar for Colds.� Healthline, 22 Jan. 2018, www.healthline.com/health/apple-cider-vinegar-for-colds.
West, Helen. �How Garlic Fights Colds and The Flu.� Healthline, 17 Mar. 2016, www.healthline.com/nutrition/garlic-fights-colds-and-flu.
Yagnik, Darshna, et al. �Antimicrobial Activity of Apple Cider Vinegar against Escherichia Coli, Staphylococcus Aureus and Candida Albicans; Downregulating Cytokine and Microbial Protein Expression.� Scientific Reports, Nature Publishing Group UK, 29 Jan. 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5788933/.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Health, Hyper Thyroid, Hypo Thyroid, Wellness
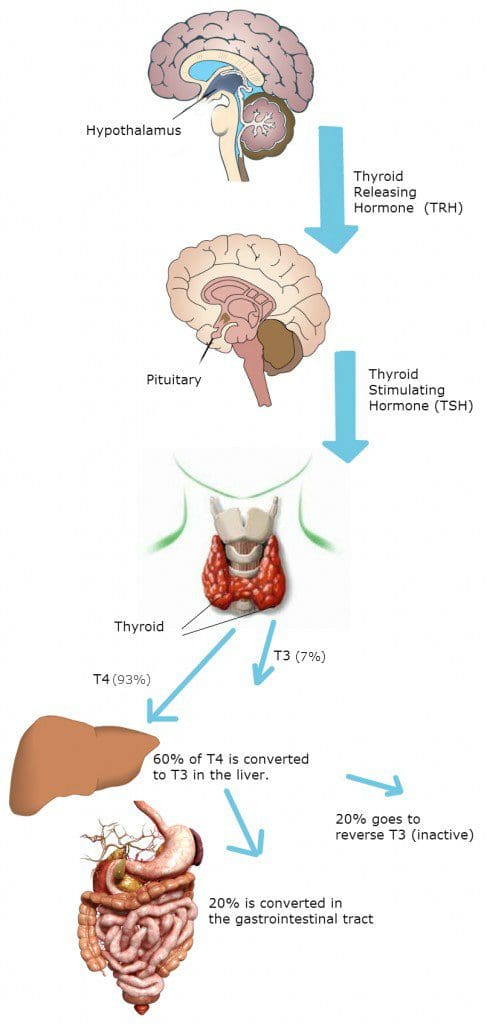
The thyroid is a small, butterfly-shaped gland that is located in the anterior neck producing T3 (triiodothyronine) and T4 (tetraiodothyronine) hormones. These hormones affect every single tissue and regulate the body�s metabolism while being part of an intricate network called the endocrine system. The endocrine system is responsible for coordinating many of the body’s activities. In the human body, the two major endocrine glands are the thyroid glands and the adrenal glands. The thyroid is controlled primarily by TSH (thyroid-stimulating hormone), which is secreted from the anterior pituitary gland in the brain. The anterior pituitary gland can stimulate or halt the secretion to the thyroid, which is a response only gland in the body.
Since the thyroid glands make T3 and T4, iodine can also help with the thyroid hormone production. The thyroid glands are the only ones that can absorb the iodine to help hormone growth. Without it, there can be complications like hyperthyroidism, hypothyroidism, and Hashimoto�s disease.
Thyroid Influences on The Body Systems
The thyroid can help metabolize the body, such as regulating heart rate, body temperature, blood pressure, and brain function. Many of the body�s cells have thyroid receptors that the thyroid hormones respond to. Here are the body systems that the thyroid helps out.
Cardiovascular System and the Thyroid
Under normal circumstances, the thyroid hormones help increase the blood flow, cardiac output, and heart rate in the cardiovascular system. The thyroid can influence the heart�s �excitement,� causing it to have an increasing demand for oxygen, therefore increasing the metabolites. When an individual is exercising; their energy, their metabolism, as well as their overall health, feels good.
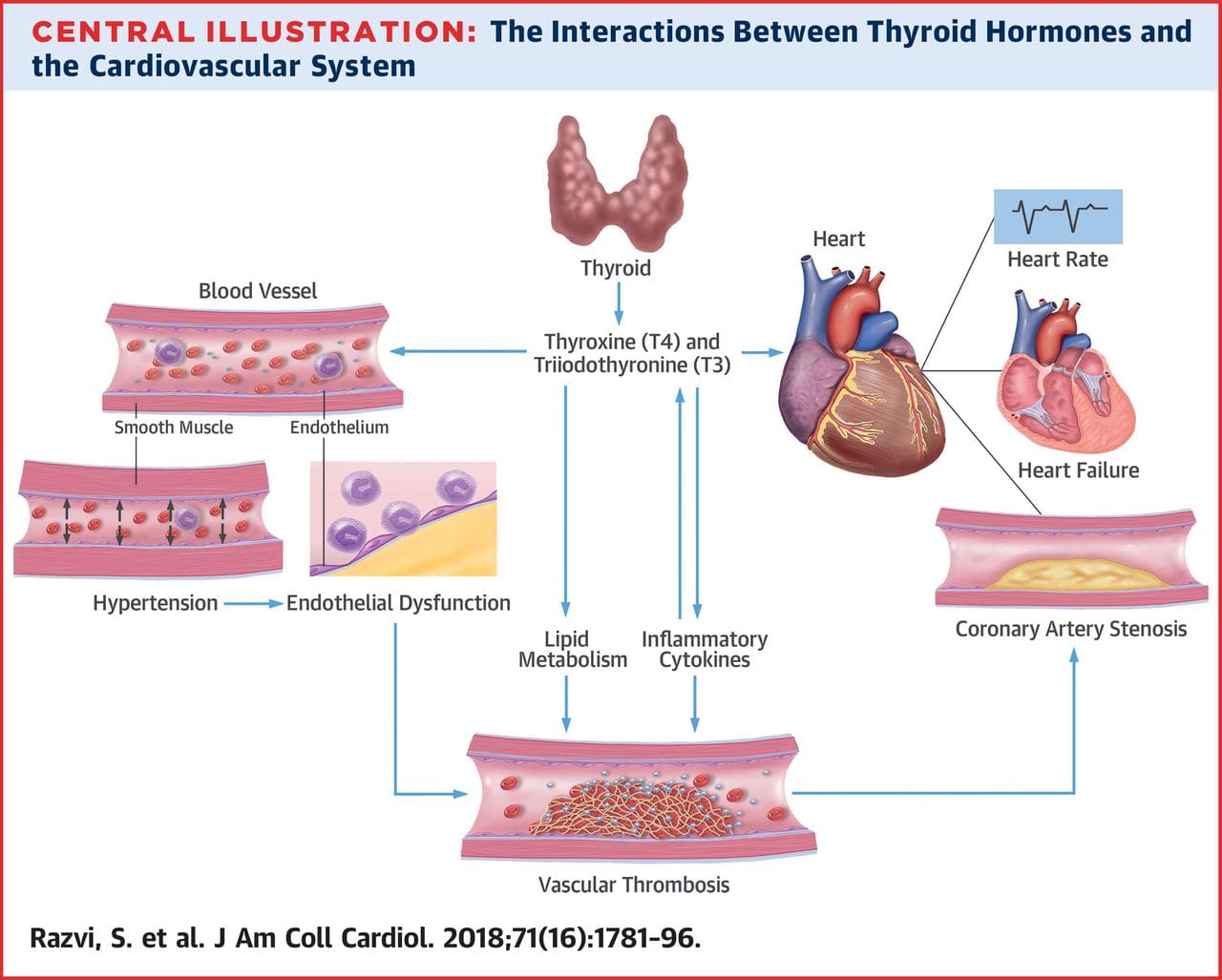
The thyroid actually strengthens the heart muscle, while decreasing the external pressure because it relaxes the vascular smooth muscle. This results in a decrease of arterial resistance and diastolic blood pressure in the cardiovascular system.
When there is an excess amount of thyroid hormone, it can increase the heart�s pulse pressure. Not only that, the heart rate is highly sensitive to an increase or decrease in the thyroid hormones. There are a few related cardiovascular conditions listed below that can be the result of an increased or decreased thyroid hormone.
- Metabolic Syndrome
- Hypertension
- Hypotension
- Anemia
- Arteriosclerosis
Interestingly, iron deficiency can slow the thyroid hormones as well as increase the production of the hormones causing problems in the cardiovascular system.
The Gastrointestinal System and the Thyroid
The thyroid helps the GI system by stimulating carbohydrate metabolism and fat metabolism. This means that there will be an increase in glucose, glycolysis, and gluconeogenesis as well as an increased absorption from the GI tract along with an increase in insulin secretion. This is done with an increased enzyme production from the thyroid hormone, acting on the nucleus of our cells.
The thyroid can increase the basal metabolic rate by helping it increase the speed of breaking down, absorbing, and the assimilation of the nutrients we eat and eliminate waste. The thyroid hormone can also increase the need for vitamins for the body. If the thyroid is going to regulate our cell metabolism, there has to be an increased need for vitamin cofactors because the body needs the vitamins to make it function properly.
Some conditions can be impacted by thyroid function, and coincidentally can cause thyroid dysfunction.
- Abnormal cholesterol metabolism
- Overweight/underweight
- Vitamin deficiency
- Constipation/diarrhea
Sex Hormones and the Thyroid

The thyroid hormones have a direct impact on ovaries and an indirect impact on SHBG (sex hormone-binding globulin), prolactin, and gonadotropin-releasing hormone secretion. Women are dramatically more affected by thyroid conditions than men due to hormones and pregnancy. There is also another contributing factor that women share, their iodine vitals and their thyroid hormones through the ovaries and the breast tissue in their bodies. The thyroid can even have either a cause or contribution to pregnancy conditions like:
- Precocious puberty
- Menstrual issues
- Fertility issues
- Abnormal hormone levels
HPA Axis and the Thyroid
The HPA axis�(Hypothalamic-Pituitary-Adrenal Axis) modulates the stress response in the body. When that happens, the hypothalamus releases the corticotropin-releasing hormone, it triggers the ACH (acetylcholine hormone) and the ACTH (adrenocorticotropic hormone) to act on the adrenal gland to release cortisol. Cortisol is a stress hormone that can lower inflammation and increase carbohydrate metabolism in the body. It can also trigger a cascade of �alarm chemicals� like epinephrine and norepinephrine (fight or flight response). If there is an absence of lowered cortisol, then the body will desensitize for the cortisol and the stress response, which is a good thing.
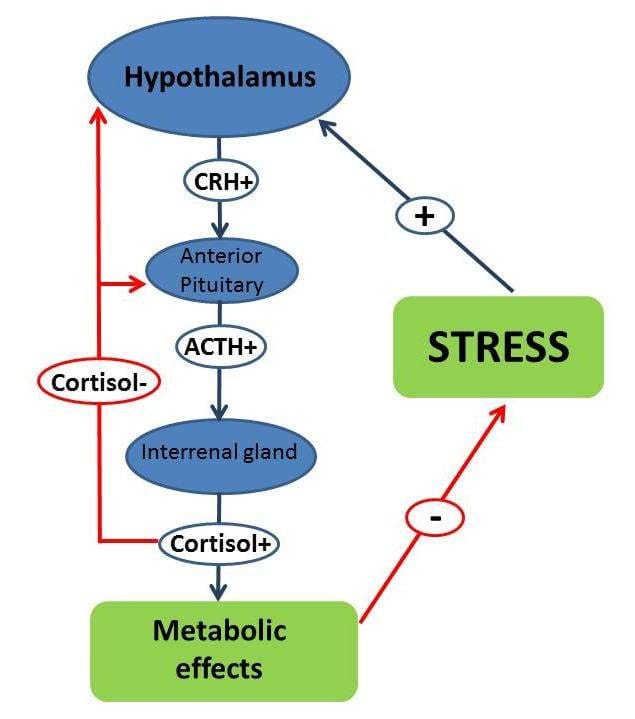
When there is a higher level of cortisol in the body, it will decrease the thyroid function by lowering the conversion of the T4 hormone to T3 hormone by impairing the deiodinase enzymes. �When this happens, the body will have a less functional thyroid hormone concentration, since the body can�t tell the difference of a hectic day at work or running away from something scary, it can either be very good or horrible.
Thyroid Problems in the Body
The thyroid can produce either too much or not enough hormones in the body, causing health problems. Down below are the most commonly known thyroid problems that will affect the thyroid in the body.
- Hyperthyroidism: This is when the thyroid is overactive, producing an excessive amount of hormones. It affects about 1% of women, but it�s less common for men to have it. It can lead to symptoms such as restlessness, bulging eyes, muscle weakness, thin skin, and anxiety.
- Hypothyroidism: This is the opposite of hyperthyroidism since it can�t produce enough hormones in the body. It is often caused by Hashimoto�s disease and can lead to dry skin, fatigue, memory problems, weight gain, and a slow heart rate.
- Hashimoto�s disease: This disease is also known as chronic lymphocytic thyroiditis. It affects about 14 million Americans and can occur in middle-aged women. This disease develops when the body�s immune system mistakenly attacks and slowly destroys the thyroid gland and its ability to produce hormones. Some of the symptoms that Hashimoto�s disease causes are a pale, puffy face, fatigue, enlarged thyroid, dry skin, and depression.
Conclusion
The thyroid is a butterfly-shaped gland located in the anterior neck that produces hormones that help function the entire body. When it doesn�t work correctly, it can either create an excessive amount or decrease the number of hormones. This causes the human body to develop diseases that can be long term.
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. To learn more about the proposal on our website.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
America, Vibrant. �Thyroid and Autoimmunity.� YouTube, YouTube, 29 June 2018, www.youtube.com/watch?feature=youtu.be&v=9CEqJ2P5H2M.
Clinic Staff, Mayo. �Hyperthyroidism (Overactive Thyroid).� Mayo Clinic, Mayo Foundation for Medical Education and Research, 3 Nov. 2018, www.mayoclinic.org/diseases-conditions/hyperthyroidism/symptoms-causes/syc-20373659.
Clinic Staff, Mayo. �Hypothyroidism (Underactive Thyroid).� Mayo Clinic, Mayo Foundation for Medical Education and Research, 4 Dec. 2018, www.mayoclinic.org/diseases-conditions/hypothyroidism/symptoms-causes/syc-20350284.
Danzi, S, and I Klein. �Thyroid Hormone and the Cardiovascular System.� Minerva Endocrinologica, U.S. National Library of Medicine, Sept. 2004, www.ncbi.nlm.nih.gov/pubmed/15282446.
Ebert, Ellen C. �The Thyroid and the Gut.� Journal of Clinical Gastroenterology, U.S. National Library of Medicine, July 2010, www.ncbi.nlm.nih.gov/pubmed/20351569.
Selby, C. �Sex Hormone Binding Globulin: Origin, Function and Clinical Significance.� Annals of Clinical Biochemistry, U.S. National Library of Medicine, Nov. 1990, www.ncbi.nlm.nih.gov/pubmed/2080856.
Stephens, Mary Ann C, and Gary Wand. �Stress and the HPA Axis: Role of Glucocorticoids in Alcohol Dependence.� Alcohol Research: Current Reviews, National Institute on Alcohol Abuse and Alcoholism, 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3860380/.
Wallace, Ryan, and Tricia Kinman. �6 Common Thyroid Disorders & Problems.� Healthline, 27 July, 2017, www.healthline.com/health/common-thyroid-disorders.
Wint, Carmella, and Elizabeth Boskey. �Hashimoto’s Disease.� Healthline, 20 Sept. 2018, www.healthline.com/health/chronic-thyroiditis-hashimotos-disease.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Chiropractic, Functional Medicine, Hormone Balance, Wellness
Hormone deficiencies and imbalances are more common than one might originally think. Research suggests that “nearly half of the women in the United States have experienced a hormone imbalance” (Grinta, 1) . However, hormone imbalance does not just affect women, “as nearly 35% of males in their seventh decade have lower testosterone levels than younger men”. (McBride, 2)��An imbalance in hormones can cause an array of symptoms and ultimately affect an individuals day to day life.�
Symptoms�
The symptoms of hormone deficiency might not be as obvious as one could imagine. Some symptoms are small and could be brushed off as stress or lack of sleep, but it is important to look at the symptoms for what they really are. “In women, low estrogen can contribute to:
- mood swings
- hot flashes
- headaches
- depression
- trouble concentrating
- fatigue
- irregular or absent periods
- increased UTI’s “
(Swns, 3)�
In men, some of the symptoms are similar to those in women, but also include:
- decreased bone mass
- sleep disturbances
- decreased motivations
- increased body fat
- decreased muscle mass
- hair loss
- libido
(Wallace, 4)
Solutions�
If these symptoms are affecting an individual’s lifestyle, there are multiple steps that can be taken to diagnose the problem and ultimately reduce symptoms. In today’s medical world, practitioners are able to use integrative techniques towards functional medicine, focusing on the biochemical level. If a patient is seeking solutions, the first step taken is an extensive questionnaire. This allows the doctor to pinpoint the exact symptoms, issues, and gives an insider look as to what direction to head towards first.
An example of the questions asked are as follows:
Once the questionnaire is completed and reviewed, a lab test is needed in order to confirm and view the exact levels the hormones are at. D.U.T.C.H ( Dried Urine Test for Comprehensive Hormones) provides one of the most accurate results. To gain more insight on D.U.T.C.H and how it works, please see last week’s article, linked here.
Testing & Conclusions
Filling out the questionnaire�essentially allows the practitioner to score and rate the severity of the issues. Adding the D.U.T.C.H results to the questionnaire gives the practitioner a factual level and complete understanding of their patient’s sex and adrenal hormones and metabolites.
This further allows the practitioner to diagnose (if necessary) and suggest nutraceuticals to help the patient’s hormone levels return to normal and minimize symptoms. There are many factors and systems involved when it comes to treating hormones and having tests completed that reflect the numbers that need to be adjusted is necessary. A hormone imbalance can easily take charge of an individual’s life, but now is the time to get these symptoms under control and get back to feeling like you used to!
A great place to start is to find a doctor or healthcare provider who will supply you with a full questionnaire and listen to the symptoms you’re having. This condition is fairly common and can be treated! October is Chiropractor Health Month, and we would love to see you and aid in providing treatment if you are experiencing any of these symptoms. Due to the fact that hormones can be complex and affect different body systems, we take the time to really understand and check all aspects before jumping to a conclusion. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Bibliography
(1) Ginta, Daniela. �What Are the Symptoms of Low Estrogen in Women and How Are They Treated.� Healthline, 31 Jan. 2017, www.healthline.com/health/womens-health/low-estrogen-symptoms.
(2) McBride, J Abram, et al. �Testosterone Deficiency in the Aging Male.� Therapeutic Advances in Urology, SAGE Publications, Feb. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4707424/.
(3) Swns. �Nearly Half of Women Have Been Affected by a Hormonal Imbalance.� New York Post, New York Post, 22 Feb. 2019, nypost.com/2019/02/22/nearly-half-of-women-have-been-affected-by-a-hormonal-imbalance/.
(4) Wallace, Ryan, and Kathleen Yoder. �12 Signs of Low Testosterone .� Healthline, 25 Apr. 2019, www.healthline.com/health/low-testosterone/warning-signs.

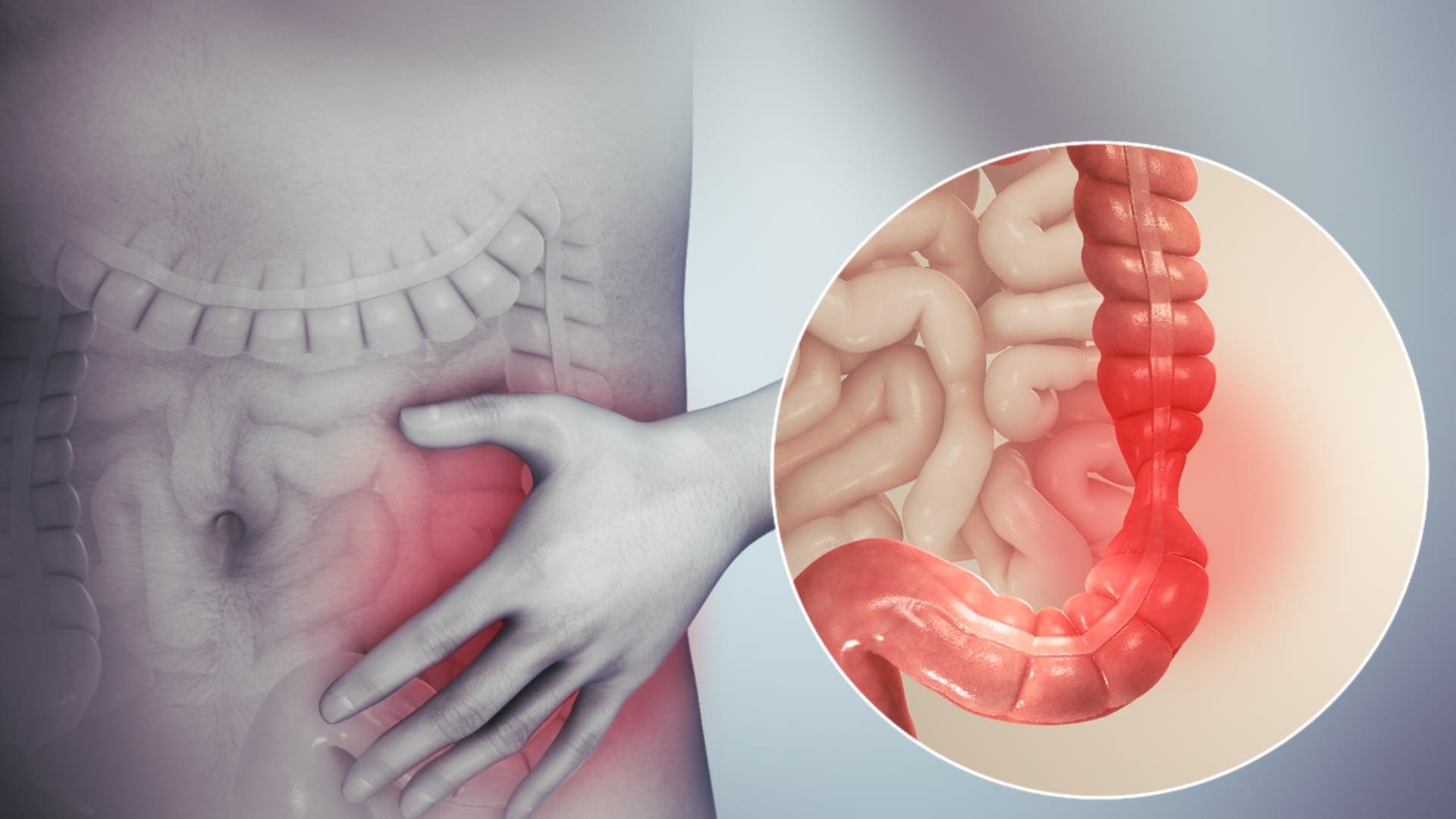
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gut and Intestinal Health, Health, Wellness
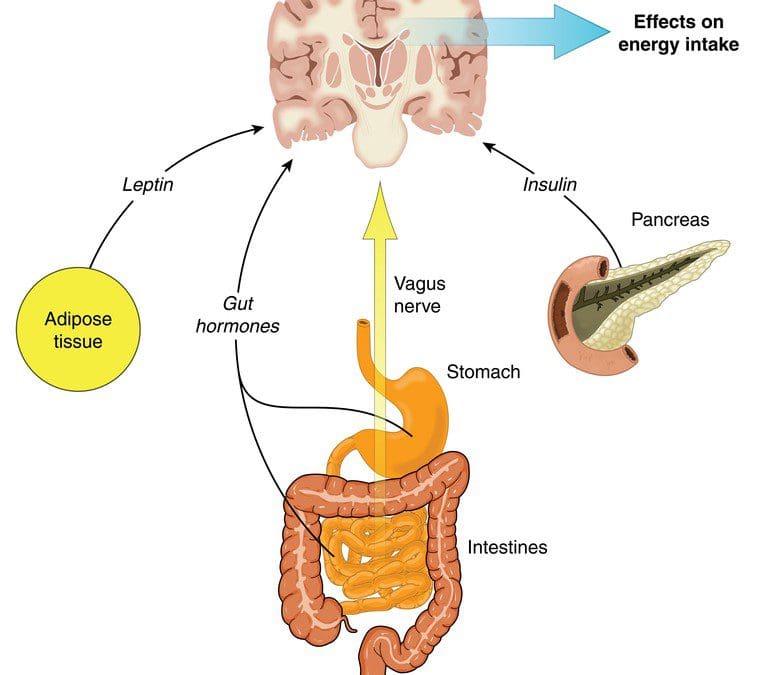
The gut-brain connection is essential in the body. If an individual has a leaky gut that is causing inflammation, it can send the signal to the brain and it can create problems like neurotransmitter dysfunction to systems that just don�t connect. The leaky gut can lead to brain dysfunction or brain dysfunction can lead to leaky gut. Sometimes an autoimmunity disease in the stomach can lead to a disruption in the mind. Then, brain disruption can also lead to inflammation in the gut. It�s a never-ending loop that the brain and gut can go on forever. Studies have stated that gut microbiota appears to influence the development of emotional behaviors like stress, pain modulation systems, and brain neurotransmitter systems.
The Brain System to the Gut System
The brain is the main control room that controls the body�s system and how the body should behave. The human brain also contains neuron cells that are found in the central nervous system. With the gut-brain connection, two critical systems help send the signal to the brain and the gut; these are known as the vagus nerve and the neurotransmitters.
The Vagus Nerve
There are approximately 100 billion neurons in the brain, while the gut contains about 500 million neurons, which is connected to the brain through the nerves in the nervous system. The vagus nerve is one of the most significant nerves that send signals back and forth to the brain and the gut. When the body is stressed, the stress signal inhibits the vagus nerve, and it can cause problems to the gut-brain connection. Animal studies have shown that any stress that is in the animal�s body can cause gastrointestinal issues and PTSD. While another study stated that individuals that have IBS (irritable bowel syndrome) have a reduced function of the vagus nerve.
There are ways to reduce the stress hormone so that the vagus nerve can function properly and send the right signals to the gut and the brain. Probiotic foods can help lower the amount of stress hormone in the bloodstream. When that happens, the body can start healing naturally when the stress is reduced; however, if the vagus nerve is damaged, then the probiotic has no effect.
Neurotransmitters
Neurotransmitters are produced chemically in the brain by controlling feelings and emotions in the body. Since the brain and gut are connected to neurotransmitters, the neurotransmitters can create these compounds that help contribute to the body. In the brain, the neurotransmitter can produce serotonin to make the person feel happy and help control their body�s biological clock.
In the gut, there are trillions of microbes that live there, and interestingly researchers stated that serotonin is mainly being produced by the gut system. Another neurotransmitter that is provided in the gut is called GABA (gamma-aminobutyric acid), which helps control the feeling of fear and anxiety. When the brain feels overly anxious or has been through a traumatic experience that has caused them to be fearful, it can cause them to be hypersensitive and can cause a chemical imbalance to the gut, causing inflammation or leaky gut if it is severe.
The Gut System to the Brain System
The gut microbes can produce neurotransmitters to send to the brain, protect the intestinal barrier and the tight junction integrity, regulate the mucosal immune system, and modulates the enteric sensory afferents. The gut microbe produces a lot of SCFA (short-chain fatty acids) that form a barrier between the brain and blood flow called the blood-brain barrier. The blood-brain barrier protects the CNS (central nervous system) from toxins, pathogens, inflammation, injury, and disease.
The gut microbes also metabolize bile and amino acids to help produce other chemicals that affect the brain. When the body is stressed, it can reduce the production of bile acid by gut bacteria and alter the genes that are involved. When that stress is still creating problems in mind, the gut can develop gastrointestinal issues that will destroy the permeability barrier that is protecting the intestines.
The gut-brain connection plays an essential role in the body�s immune system as it controls inflammation and what passes into the body. Since the immune system controls inflammation, if it is turned on for too long, inflammation can occur as well as several brain disorders like depression and Alzheimer�s disease. Stress can even disrupt the gut by causing contractions to the GI tract, make inflammation worse in the intestinal permeability, and making the body more at risk to infections.
When the body starts to alleviate stress, it can naturally heal itself, and the gut-brain connection can begin functioning normally. With changes in a person�s eating habits and lifestyle, it can drastically change a person�s mood and recover from intestinal ailments they may have. If the brain feels right, then the gut feels good as well. They work together side by side to make sure that the body is functioning correctly. When either one is being disrupted, then the body does not function properly.
Conclusion
Therefore, the gut-brain connection is vital to the body. Neurotransmitters and other components that are in both systems work together to make sure that the body is working correctly. When one of the connections is being disrupted, however, the body can develop many chronic illnesses even if the person seems fine. By altering little things like changing a person�s diet and lifestyle, it can help improve the body and bring the balance back to the gut-brain connection.
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. To learn more about the proposal on our website.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Anguelova, M, et al. �A Systematic Review of Association Studies Investigating Genes Coding for Serotonin Receptors and the Serotonin Transporter: I. Affective Disorders.� Molecular Psychiatry, U.S. National Library of Medicine, June 2003, www.ncbi.nlm.nih.gov/pubmed/12851635.
Bravo, Javier A, et al. �Ingestion of Lactobacillus Strain Regulates Emotional Behavior and Central GABA Receptor Expression in a Mouse via the Vagus Nerve.� Proceedings of the National Academy of Sciences of the United States of America, National Academy of Sciences, 20 Sept. 2011, www.ncbi.nlm.nih.gov/pubmed/21876150.
Carabotti, Marilia, et al. �The Gut-Brain Axis: Interactions between Enteric Microbiota, Central and Enteric Nervous Systems.� Annals of Gastroenterology, Hellenic Society of Gastroenterology, 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4367209/.
Daneman, Richard, and Alexandre Prat. �The Blood-Brain Barrier.� Cold Spring Harbor Perspectives in Biology, Cold Spring Harbor Laboratory Press, 5 Jan. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4292164/.
Herculano-Houzel, Suzana. �The Human Brain in Numbers: a Linearly Scaled-up Primate Brain.� Frontiers in Human Neuroscience, Frontiers Research Foundation, 9 Nov. 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC2776484/.
Lucas, Sian-Marie, et al. �The Role of Inflammation in CNS Injury and Disease.� British Journal of Pharmacology, Nature Publishing Group, Jan. 2006, www.ncbi.nlm.nih.gov/pmc/articles/PMC1760754/.
Mayer, Emeran A, et al. �Gut/Brain Axis and the Microbiota.� The Journal of Clinical Investigation, American Society for Clinical Investigation, 2 Mar. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4362231/.
Mayer, Emeran A. �Gut Feelings: the Emerging Biology of Gut-Brain Communication.� Nature Reviews. Neuroscience, U.S. National Library of Medicine, 13 July 2011, www.ncbi.nlm.nih.gov/pmc/articles/PMC3845678/.
Mazzoli, Roberto, and Enrica Pessione. �The Neuro-Endocrinological Role of Microbial Glutamate and GABA Signaling.� Frontiers in Microbiology, Frontiers Media S.A., 30 Nov. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC5127831/.
Pellissier, Sonia, et al. �Relationship between Vagal Tone, Cortisol, TNF-Alpha, Epinephrine and Negative Affects in Crohn’s Disease and Irritable Bowel Syndrome.� PloS One, Public Library of Science, 10 Sept. 2014, www.ncbi.nlm.nih.gov/pubmed/25207649.
Rooks, Michelle G, and Wendy S Garrett. �Gut Microbiota, Metabolites and Host Immunity.� Nature Reviews. Immunology, U.S. National Library of Medicine, 27 May 2016, www.ncbi.nlm.nih.gov/pubmed/27231050.
Sahar, T, et al. �Vagal Modulation of Responses to Mental Challenge in Posttraumatic Stress Disorder.� Biological Psychiatry, U.S. National Library of Medicine, 1 Apr. 2001, www.ncbi.nlm.nih.gov/pubmed/11297721.
Yano, Jessica M, et al. �Indigenous Bacteria from the Gut Microbiota Regulate Host Serotonin Biosynthesis.� Cell, U.S. National Library of Medicine, 9 Apr. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4393509/.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Health, Wellness
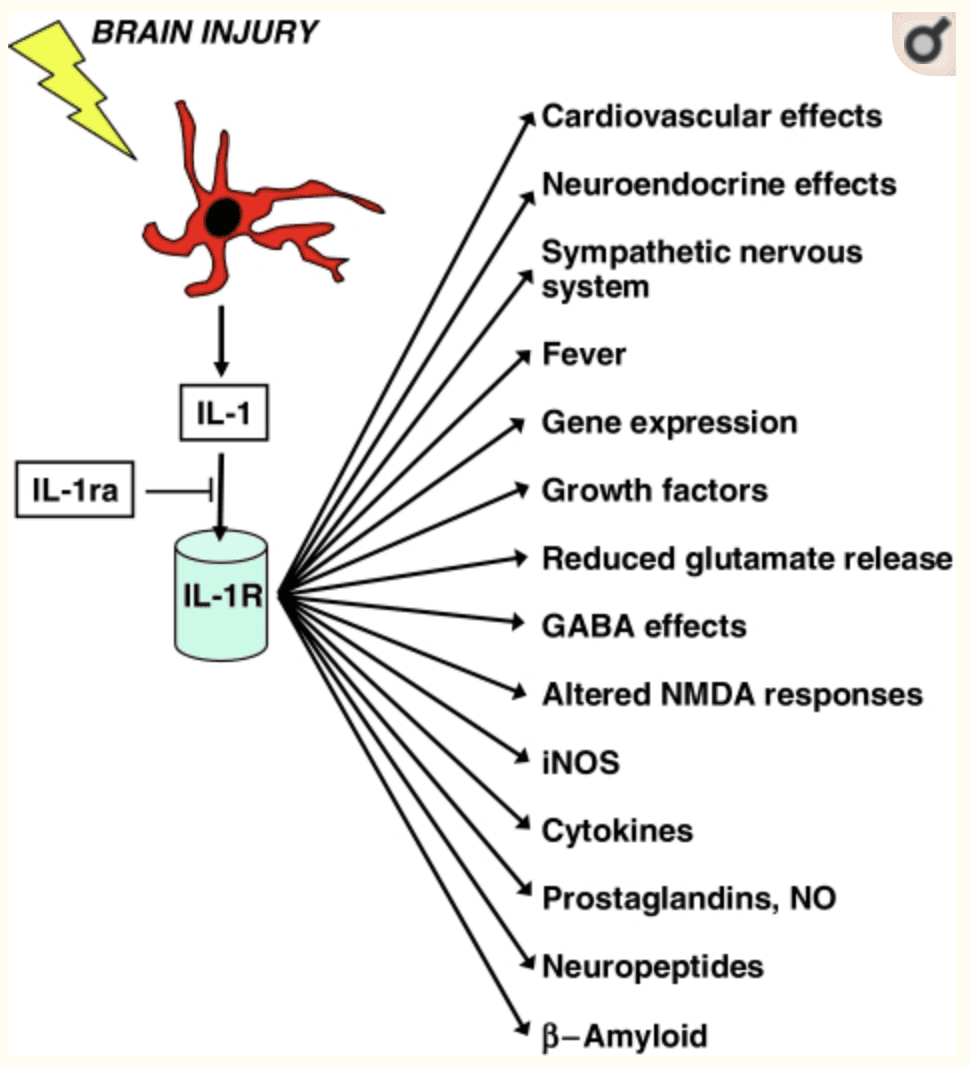
Autoimmune disease is the disease of the modern era. It is a condition where the body�s immune system mistakenly attacks the body. Since the body�s immune system usually guards against bacteria and viruses, it can sense the foreign cells and send out fighter cells to attack them. When it�s an autoimmune disease, however, the immune system starts to make mistakes to certain parts of the body. It starts attacking the joints, the skin, or the musculoskeletal system as foreign cells and attacking them. The immune system releases autoantibody proteins to attack the healthy cells, thus causing autoimmune disease in the body.
What Triggers the Activation of the Autoimmune Mechanism?
Surprisingly, the body�s antibodies go through a process by cleaning up the old and damaged cells, so that way, new healthy cells can grow and replace the old cells. Although if the body has an excessive number of antibodies in their system, it can cause the individual to have an autoimmune disease. Research has shown that a part of the autoimmune ecology, the influence of environmental exposure can not only develop autoimmune disorder but shape the function of the immune system.
Another study stated that approximately 30% of all autoimmune diseases come from genetic disposition while 70% is due to environmental factors, including toxic chemicals, dietary components, gut dysbiosis, and infections in the body. So some of the ecological factors that are included are adjuvants (immunostimulant effects). These are typically used in vaccines to produce a more effective immunization reaction.
Researchers stated that molecular mimicry is one of the mechanisms, where a foreign antigen shares a sequence or structural similarities with self-antigens. This means that any infections that can initiate and maintain autoimmune responses can lead to specific tissue damage in the body. It is a phenomenon that molecular mimicry and cross-reactivity are identical. Cross-reactivity is significant when it comes to food allergies and is often responsible for many disorders. It affects the scope of the disease, the reliability of diagnostic testing, and has implications for any current and potential therapies.
Common and Rare Autoimmune Diseases
The primary function of the immune system is to repair the body with new cells. Individuals with an autoimmune disease will have many chronic illnesses that are both common and rare when they are being diagnosed. Below is a list of autoimmune diseases that range from common to some of the rarer autoimmune conditions an individual may experience.
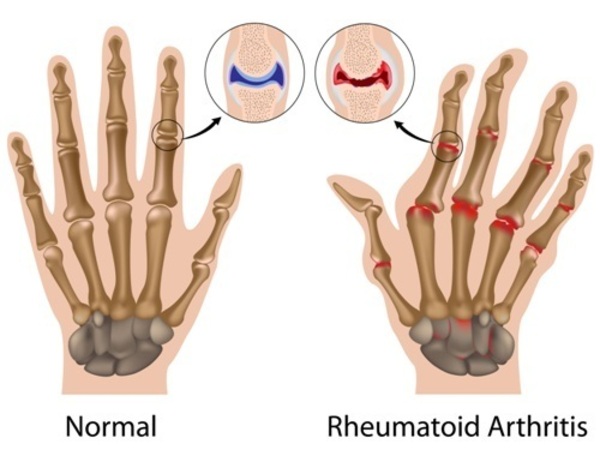
Rheumatoid arthritis (RA)
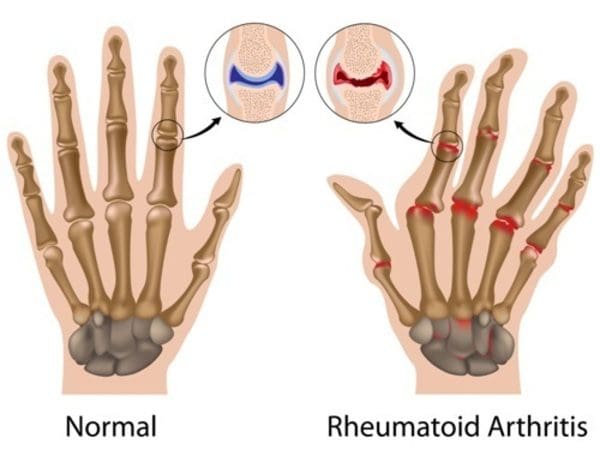
Rheumatoid arthritis is when the immune system is attacking the joints. This attack causes redness, warmth, soreness, and stiffness. It�s one of the most common autoimmune diseases that is found in women but can affect men and elderly people as well. Studies have shown that if a family member has rheumatoid arthritis, it is likely that other family members may have an increased chance of developing this autoimmune disease. The signs and symptoms of rheumatoid arthritis can vary depending on the severity of the inflamed joints, potentially causing them to deform and shift out of place.��
Lupus

Lupus is a systemic autoimmune disease that occurs when an individual�s immune system starts attacking their own tissue and organs. Even though lupus is difficult to diagnose because it often mimics other ailments, it can cause inflammation to different body systems. These body systems include the joints, skin, kidneys, blood cells, brain, heart, and lungs. A distinctive sign of lupus is a facial rash that resembles butterfly wings unfolding across booth cheek.
Ehlers-Danlos Syndrome (EDS)
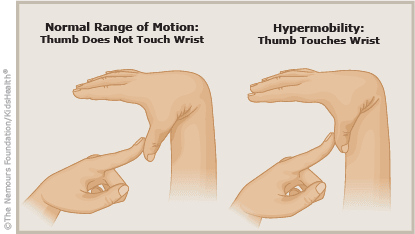
EDS (Ehlers-Danlos Syndrome) is a rare autoimmune disease that causes soft connective tissues to be fragile in the body. This autoimmune disease is still new for doctors; however, there is always more research to be done about this disease. The symptoms can vary from mild skin and joint hyperlaxity to severe physical disability and life-threatening vascular complications. One of the most common symptoms is joint hypermobility. This disease can cause the joints to be unstable or loose, and it can cause the body�s joints to have frequent dislocations and pain.
Polymyalgia Rheumatica

Polymyalgia rheumatica is an inflammatory musculoskeletal disorder that is most common in elderly adults. This disease causes muscle pain and stiffness around the joints, most commonly occurring in the morning.�It also shares similarities with another disease known as giant cell arteritis. If an individual has polymyalgia rheumatica, they can have the symptoms of giant cell arteritis as well. The symptoms are inflammation in the lining of the arteries. The two factors that can cause the development of polymyalgia rheumatica are genetics and environmental exposure that can increase the chances of having the disorder.
Ankylosing spondylitis
Ankylosing spondylitis is an autoimmune inflammatory disease that can cause some of the vertebrae in the spine to fuse over time. When this happens, the fusing makes the spine less flexible and causes the body to be in a hunched-forward posture. It is most common for men, and there are treatments to lessen the symptoms and possibly slow down the progression of the disease.
Celiac disease
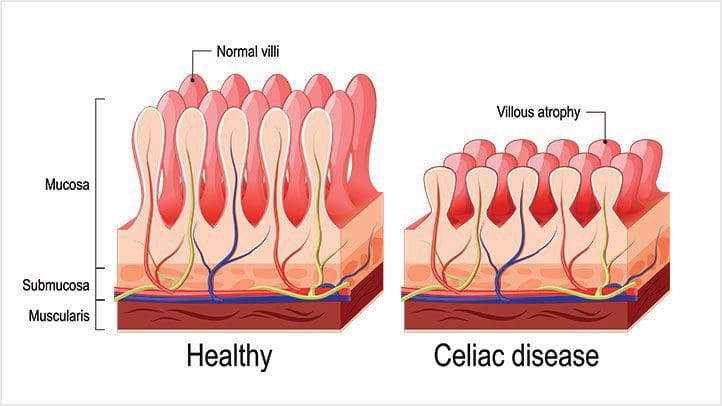
Celiac disease is an autoimmune disease that occurs in about 1% of individuals. This disease makes the individual have an inflammatory reaction to the intestinal permeability barrier from eating gluten found in wheat, rye, and barley. Studies show that patients with celiac disease and autoimmune disease have to be on a gluten-free diet to heal the gut. Symptoms can include bloating, digestive issues, inflammation, and skin rashes.
Conclusion
Mechanisms of an autoimmune disease can be caused by genetics or induced by environmental factors. This can cause an individual to have problems in their body related to inflammation.�There are many autoimmune diseases�that can affect the body from the most common to some of the rarer kinds and it can have lasting effects.
In honor of Governor Abbott’s declaration, October is Chiropractic Health Month. To learn more about the proposal on our website.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Anaya, Juan-Manuel, et al. �The Autoimmune Ecology.� Frontiers in Immunology, Frontiers Media S.A., 26 Apr. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4844615/.
Bonds, Rana S, et al. �A Structural Basis for Food Allergy: the Role of Cross-Reactivity.� Current Opinion in Allergy and Clinical Immunology, U.S. National Library of Medicine, Feb. 2008, www.ncbi.nlm.nih.gov/pubmed/18188023.
Clinic Staff, Mayo. �Ankylosing Spondylitis.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 7 Mar. 2018, www.mayoclinic.org/diseases-conditions/ankylosing-spondylitis/symptoms-causes/syc-20354808.
Clinic Staff, Mayo. �Lupus.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 25 Oct. 2017, www.mayoclinic.org/diseases-conditions/lupus/symptoms-causes/syc-20365789.
Clinic Staff, Mayo. �Polymyalgia Rheumatica.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 23 June 2018, www.mayoclinic.org/diseases-conditions/polymyalgia-rheumatica/symptoms-causes/syc-20376539.
Cusick, Matthew F, et al. �Molecular Mimicry as a Mechanism of Autoimmune Disease.� Clinical Reviews in Allergy & Immunology, U.S. National Library of Medicine, Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3266166/.
De Paepe, A, and F Malfait. �The Ehlers-Danlos Syndrome, a Disorder with Many Faces.� Clinical Genetics, U.S. National Library of Medicine, July 2012, www.ncbi.nlm.nih.gov/pubmed/22353005.
Schmidt, Zsuzsa, and Gyula Po�r. �Polymyalgia Rheumatica Update, 2015.� Orvosi Hetilap, U.S. National Library of Medicine, 3 Jan. 2016, www.ncbi.nlm.nih.gov/pubmed/26708681.
Scott, David L, et al. �Rheumatoid Arthritis.� Lancet (London, England), U.S. National Library of Medicine, 25 Sept. 2010, www.ncbi.nlm.nih.gov/pubmed/20870100.
Vojdani, Aristo, et al. �Environmental Triggers and Autoimmunity.� Autoimmune Diseases, Hindawi Publishing Corporation, 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4290643/.
Watson, Stephanie. �Autoimmune Diseases: Types, Symptoms, Causes, Diagnosis & More.� Healthline, Healthline Media, 26 Mar. 2019, www.healthline.com/health/autoimmune-disorders.
by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Gut and Intestinal Health, Health, Wellness
SIBO (small intestinal bacterial overgrowth) is defined as 105 up to 106 organisms of bacteria in the small intestines. It is highly relevant to remember that the abundance of bacteria in the small intestine that has SIBO, are healthy bacteria that live in the gastrointestinal tract. It means that the bacteria in the digestive tract is either missed or dislocated and is in the wrong place in the small intestines. While SIBO still remains a poorly understood disease, it is frequently implicated to be the cause of chronic diarrhea and malabsorption. Individuals who have SIBO can also suffer from many chronic illnesses. This includes unintended weight loss, nutritional deficiencies, and osteoporosis.
SIBO and IBS

Studies have indicated that 84% of individuals that has IBS (irritable bowel syndrome) will have SIBO. SIBO is one of the causes of leaky gut, and leaky gut is one of the triad factors that can lead the body to have an autoimmune disease. Health care professionals that diagnose individuals who have SIBO can link the virus to other health problems that the individual may have. Studies have mentioned that when LPS (lipopolysaccharide) is moving from the large intestines to the small intestines, it can contribute to developing intestinal inflammation. With LPS, it can cause an increase of intestinal tight junction permeability or leaky gut.
So SIBO will release LPS into the gut, causing the leaky gut to the gut system in the body. Another study showed that autoimmune diseases are always a triad of a few different things. To have an autoimmune disease, you have to have the gene to get the disease. Although most people know that if they have a gene, doesn�t mean that they will have an autoimmune disease. Even if they don�t have an autoimmune disease, there�s an environmental trigger that will come on and creates an epigenetic change. This will cause the gene in the human body to be expressed.
So the first two factors of the autoimmune disease, are a genetic factor and an environmental factor, the third and final factor is intestinal permeability. So if the primary two factors that are causing disruption to the intestinal permeability, they will prevent the intestinal permeability to actually heal itself. With all three elements being linked to autoimmune disease and SIBO, it will cause the body to have the leaky gut syndrome and health problems to individuals.
So when doctors are diagnosing the patient that has SIBO, they will do a lactulose breath test. What this test does, is that it will indicate that the patient has IBS bloating, and it is causing them discomfort in their gut. Research stated that the lactulose breath test shows the correlation between the pattern of the bowel movements and the type of excreted gas in the stomach. So for anyone that is positive with IBS and takes the breath test, they will understand the consequences of the factors that are leading to the SIBO disease and causing leaky gut.
How do we get SIBO?
With the understanding of what SIBO is, we can see that SIBO is not the only cause of irritable bowel syndrome, but the big player of the syndrome. So taking a step back, we have to discuss what the MMG (Migrating Motor Complex) is before we go further in explaining the pathogenesis of the SIBO disease. Migrating motor complexes are waves of electrical activity that is sweeping through the intestines in a regular cycle. It often happens when a person is fasting, therefore with MMG, we can look at the acute gastroenteritis in the body.
With acute gastroenteritis, the body has some sort of severe infection like bloating, diarrhea, constipation, or a variety of things that are infectious to the gut; however, they are self-limiting. Healthcare professionals who see patients with these acute infections can see that most of the bacteria can cause gastroenteritis, pile up, and release CTD (cytolethal distending toxin). What CTD does is that it will create a reaction against vinculin; which regulates the ICC (interstitial cells of Cajal) and the ICC then regulates the migrating motor complex.
So when the CTD releases toxins in the gut, it causes a reaction to a molecular mimicry reaction. That reaction causes the body to create antibodies to fight against that toxin but through molecular mimicry. CTD looks exactly like vinculin and cross-reacts with the antibodies, So now those antibodies are attacking vinculin, thus damaging the ICC. Since the MMC clears the intestinal tract, when a person is fasting, and the CTD is damaging the intestines, SIBO is created since the body can not flush out the bacteria.
Studies have shown that there are many ways to get SIBO, it can happen by either food poisoning, abdominal surgery, or low stomach acid. Another thing to mention is that mostly 70% of SIBO is caused by food poisoning. Most people who had to suffer from food poisoning don�t realize that SIBO is already in their gut. So the research states that small bowel motility disorders can be the predispose development of SIBO since the bacteria may not be effectively swept from the bowel into to colon.
Treating SIBO

There are many ways to treat SIBO, healthcare professionals can suggest these treatments to their patients who have SIBO and start restoring their intestinal barrier in the long haul. So here are some of the procedures that can help the body and treat SIBO.
- Pharmaceuticals: If a patient has constipation and is taking rifaximin if the symptoms are not clearing up, adding another medication with rifaximin for 14 days may help in battling SIBO. It will take a bit longer, but it will help clear the SIBO out of the gut.
- Herbal Treatment: With herbal treatments, there are many ways to help treat SIBO naturally. It can be berberine containing herbs, oil of oregano, neem, garlic, Lactobacillus plantarum, Lauricidin, and Antrantil. These herbal treatments can naturally help to fight against SIBO, and studies show that 46% of patients feel a lot better in a short amount of time.
Conclusion
So SIBO is a bacterial disease that can disrupt the gastrointestinal tract and cause the leaky gut to the body. It will cause inflammation and can be in an individual�s body through three factors like genetics, environmental triggers, and food poisoning. It can be treated through pharmaceuticals and herbal treatments prescribed by doctors.� In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month, learn more about this proposal on our website and read what the proposal is all about. The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Bezine, Elisabeth, et al. �The Cytolethal Distending Toxin Effects on Mammalian Cells: a DNA Damage Perspective.� Cells, MDPI, 11 June 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4092857/.
Brown, Kenneth, et al. �Response of Irritable Bowel Syndrome with Constipation Patients Administered a Combined Quebracho/Conker Tree/M. Balsamea Willd Extract.� World Journal of Gastrointestinal Pharmacology and Therapeutics, Baishideng Publishing Group Inc, 6 Aug. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4986399/.
Chedid, Victor, et al. �Herbal Therapy Is Equivalent to Rifaximin for the Treatment of Small Intestinal Bacterial Overgrowth.� Global Advances in Health and Medicine, Global Advances in Health and Medicine, May 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4030608/.
Dukowicz, Andrew C, et al. �Small Intestinal Bacterial Overgrowth: a Comprehensive Review.� Gastroenterology & Hepatology, Millennium Medical Publishing, Feb. 2007, www.ncbi.nlm.nih.gov/pmc/articles/PMC3099351/.
Endo, EH, and Dias Filho. �Antibacterial Activity of Berberine against Methicillin-Resistant Staphylococcus Aureus Planktonic and Biofilm Cells.� Austin Journal of Tropical Medicine & Hygiene, 19 Feb. 2015, austinpublishinggroup.com/tropical-medicine/fulltext/ajtmh-v1-id1005.php.
Fasano, Alessio, and Terez Shea-Donohue. �Mechanisms of Disease: the Role of Intestinal Barrier Function in the Pathogenesis of Gastrointestinal Autoimmune Diseases.� Nature News, Nature Publishing Group, 1 Sept. 2005, www.nature.com/articles/ncpgasthep0259.
Ghonmode, Wasudeo Namdeo, et al. �Comparison of the Antibacterial Efficiency of Neem Leaf Extracts, Grape Seed Extracts and 3% Sodium Hypochlorite against E. Feacalis – An in Vitro Study.� Journal of International Oral Health: JIOH, International Society of Preventive and Community Dentistry, Dec. 2013, www.ncbi.nlm.nih.gov/pubmed/24453446.
Guo, Shuhong, et al. �Lipopolysaccharide Regulation of Intestinal Tight Junction Permeability Is Mediated by TLR4 Signal Transduction Pathway Activation of FAK and MyD88.� Journal of Immunology (Baltimore, Md. : 1950), U.S. National Library of Medicine, 15 Nov. 2015, www.ncbi.nlm.nih.gov/pubmed/26466961.
Lin, Henry C. �Small Intestinal Bacterial Overgrowth: a Framework for Understanding Irritable Bowel Syndrome.� JAMA, U.S. National Library of Medicine, 18 Aug. 2004, www.ncbi.nlm.nih.gov/pubmed/15316000.
Preuss, Harry G, et al. �Minimum Inhibitory Concentrations of Herbal Essential Oils and Monolaurin for Gram-Positive and Gram-Negative Bacteria.� Molecular and Cellular Biochemistry, U.S. National Library of Medicine, Apr. 2005, www.ncbi.nlm.nih.gov/pubmed/16010969.
Sienkiewicz, Monika, et al. �The Antibacterial Activity of Oregano Essential Oil (Origanum Heracleoticum L.) against Clinical Strains of Escherichia Coli and Pseudomonas Aeruginosa.� Medycyna Doswiadczalna i Mikrobiologia, U.S. National Library of Medicine, 2012, www.ncbi.nlm.nih.gov/pubmed/23484421.
Soifer, Luis Oscar, et al. �Comparative Clinical Efficacy of a Probiotic vs. an Antibiotic in the Treatment of Patients with Intestinal Bacterial Overgrowth and Chronic Abdominal Functional Distension: a Pilot Study.� Acta Gastroenterologica Latinoamericana, U.S. National Library of Medicine, Dec. 2010, www.ncbi.nlm.nih.gov/pubmed/21381407/.

by Dr Alex Jimenez DC, APRN, FNP-BC, CFMP, IFMCP | Functional Medicine, Health, Integrative Functional Wellness, Wellness
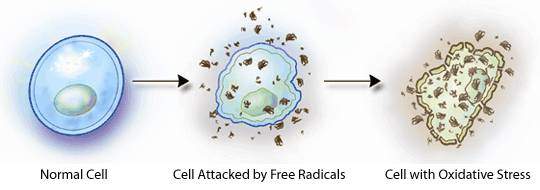
The Nrf2 cell defense creates a pathway that provides protection against oxidative stress and disorders. It plays a vital role in maintaining cellular homeostasis and keeping each cell strand in check. Without the Nrf2 cell defense, oxidative stress can be excessive and directly cause or contribute to many common diseases. This includes cancer, osteoporosis, inflammatory bowel diseases, and neurodegeneration. Studies show that even oxidative stress can contribute to insulin resistance and multiple sclerosis.
Certain foods that are beneficial to the Nrf2 cell structure, due to their antioxidative properties; can enhance the Nrf2 cell gene gradually. Researchers studied that dietary sources that contain antioxidants flavonoids, fermented food and drinks that contain lactobacilli, and sulforaphane from cruciferous vegetables; are the contributors to aid the Nrf2 cell structure. With these certain foods in a person�s diet, it can be beneficial to combating oxidative stress and preventing oxygen toxicity from producing in the bloodstream.
Food That Helps the Nrf2 Cell
Here are some of the foods that contain nutrients to help out the Nrf2 cell:
- Fruits: Red, blue and purple berries, red and purple grapes, apples, citrus fruits and juices (oranges, grapefruits, and lemons)
- Red wine
- Teas: Green, white, black, and oolong
- Chocolate
- Vegetables: Yellow onion, scallions, kale, broccoli, celery, hot peppers, greens beans
- Herbs: Parsley, thyme
- Legumes: Soybeans and other soy products, chickpeas, mung beans
With these types of antioxidant foods, they can help aid the body by lowering the stress compound naturally without the usage of medications. There are ways to get the nutrients of the different food groups to support the body and activate the Nrf2 pathways. Fermented foods that contain lactobacilli can express and activate the gene pathway.
Let�s start with Lactobacillus plantarum and Lactobacillus brevis. These two are the good bacteria that are found in traditional vegetables, fruit, and fermented malt whiskey. They help the body by breaking down the food that is being consumed, absorbing the nutrients, and fighting off the harmful organisms that are causing discomfort to the gut. When these two bacteria are expressing PAD (phenolic acid derivatives) and being introduced to a caffeic acid; the results are astonishing.
Studies indicate that particular strains of lactobacilli can biotransform the caffeic acid to potently activate the Nrf2 pathways from an inactive precursor. �So let�s say that if an individual is stressed and then they eat some food. Suddenly they feel a bit better after eating, that is because of the Nrf2 pathways mixed with the enhanced lactobacilli in their food helped neutralized the stress compound in the body.
With sulforaphane in cruciferous vegetables, it can help with the Nrf2 pathways. Since cruciferous plants have natural fighting properties against cancer, they have a good source of phytonutrients and the sulforaphane combined.
Here are some of the cruciferous vegetables that can help the Nrf2 pathway in the body.
- Arugula
- Bok choy
- Broccoli
- Brussels sprouts
- Cabbage
- Cauliflower
- Kale
- Radish
- Turnips
These vegetables are nutritious when they are eaten raw or cooked. Sulforaphane in the many cruciferous plants has been linked to many health benefits such as improving heart health and digestion. This compound has an inactive form of glucoraphanin, but when it comes in contact with myrosinase, it releases the glucosinolates. This means that when the cruciferous vegetables are either damaged, cut, chopped or chewed on, the myrosinase enzymes are activated and turning into sulforaphane.
Studies have even been shown that sulforaphane can prevent cancer cell growth by releasing antioxidants and detoxifying enzymes that protect carcinogens, which are substances that can cause cancer.
How the Nrf2 Cell Activates
The various molecules in them can exhibit a robust activation in the Nrf2 defense system. Researchers have studied that the Nrf2 defense pathway can provide natural protection against oxidative stress and chemical toxicity through relatively small electrochemical co-factors called Nrf2 activators.
These activators actually amplify the effect of ROS (reactive oxygen species) by cycling through oxidation-reduction reactions and liberating Nrf2 in the human endothelial cells. Since the human body can get sick from stress, it is essential to eat foods that can fight off the harmful organisms. Nrf2 cells do regulate the oxidative stress by releasing itself into the body�s system. It is crucial to make sure that good, nutritious food that is beneficial in helping the Nrf2 cells by doing it naturally.
With a person�s hectic lifestyle gets in the way, they start to feel overly stressed. The body begins to develop chronic ailments that can harm not only the outside of the body but the inside as well. When individuals go to see health care professional for any chronic diseases that they may have, they will be informed of remedies to help aid them the best way they can. Individuals can find ways to deal with the stress hormone and calm it down through functional medicine. So when the body develops oxidative stress, it will affect the organ system, the nerve system, and the neurological system.
With the Nrf2 cells, the cell structure goes towards the oxidative stress compound and put a stop to it. And with the nutritious food that is available to aid the Nrf2 cell more. When we can calm down our anxious mind through the use of functional medicine and by eating healthy, organic, whole foods; we are actually repairing the body from the inside out.
Conclusion
As stated from the beginning, the Nrf2 cell helps the body by protecting it against oxidative stress. When we add nutritious food into the collection, it is aiding the Nrf2 cells a whole lot. Since the entire body needs the nutrients from the different food groups to assist not only the Nrf2 cells but to all crucial organs that need the nutrient sources to function correctly. The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References
Bryan, Holly K, et al. �The Nrf2 Cell Defence Pathway: Keap1-Dependent and -Independent Mechanisms of Regulation.� Biochemical Pharmacology, U.S. National Library of Medicine, 15 Mar. 2013, www.ncbi.nlm.nih.gov/pubmed/23219527.
Coyle, Daisy. �Sulforaphane: Benefits, Side Effects, and Food Sources.� Healthline, 26 Feb. 2019, www.healthline.com/nutrition/sulforaphane.
Prochaska, H J, et al. �On the Mechanisms of Induction of cancer-protective Enzymes: a Unifying Proposal.� Proceedings of the National Academy of Sciences of the United States of America, U.S. National Library of Medicine, Dec. 1985, www.ncbi.nlm.nih.gov/pubmed/3934671.
Senger, Donald R., et al. �Activation of the Nrf2 Cell Defense Pathway by Ancient Foods: Disease Prevention by Important Molecules and Microbes Lost from the Modern Western Diet.� PLOS ONE, Public Library of Science, 17 Feb. 2016, journals.plos.org/plosone/article?id=10.1371%2Fjournal.pone.0148042.
Shaw, Pamela. �The Nrf2 Diet.� ALS Worldwide, 27 Jan. 2015, alsworldwide.org/care-and-support/article/the-nrf2-diet.
Su, Xuling, et al. �Anticancer Activity of Sulforaphane: The Epigenetic Mechanisms and the Nrf2 Signaling Pathway.� Oxidative Medicine and Cellular Longevity, Hindawi, 6 June 2018, www.ncbi.nlm.nih.gov/pubmed/29977456.






