Vegan and vegetarian diet have long been touted as some of the healthiest diets for people of all walks of life. There is a lot of confusion and many misconceptions, though, about the two.
What most people don�t realize is that there are many sub-category diets that fall under vegetarianism, some of which include animal by-products, seafood, and even meat. Understanding veganism and vegetarianism as well as knowing the benefits of these diets can help chiropractic patients stay healthier, get more active, and stave off many chronic illnesses.
Is There A Difference Between Vegan & Vegetarian Diets?
There are distinct differences between veganism and vegetarianism although many books and even food companies fail to clearly distinguish the two. While it is true that they are very similar diets, the differences are significant.
Vegans do not eat any animal by-products or animal flesh at all. This includes seafood. They also do not use products that use animal testing or that are made from animals including leather products.
On the other hand, vegetarians typically abstain from eating animal flesh, but do often eat animal by-products such as dairy products and eggs. Some also eat seafood including fish, shrimp, and crab. They are also a little more relaxed when it comes to the products they purchase as well.
What Is A Vegetarian Diet?
The vegetarian diet comes in several varieties. The standard vegetarian diet consists of eggs and dairy products but excludes fish and meat. This is also called a �lacto ovo vegetarian.� However, some vegetarians include dairy products but exclude eggs while others include the eggs and exclude the dairy. A �demi-vegetarian� includes seafood.
There are also what are known as �semi-vegetarians� although there is some controversy over whether they should be classified as vegetarian or not.
Pollo Vegetarian � includes poultry but excludes other meats and seafood.
Pesco Vegetarian � includes fish and chicken but excludes red meat.
Flexitarian � includes any kind of meat whenever they want but adhere mainly to a standard vegetarian diet.
What Is A Vegan Diet?
A vegan diet excludes all animal by products and meats. True vegans do not use or wear anything derived from animals (leather, snakeskin, etc.) or that is tested on animals. Most vegans tend to avoid sodas, sugary sweets, processed foods, and ready-meals, while choosing organic, high quality foods.
Still, there are a few variations of veganism too. For instance, a raw vegan combines a vegan diet with a raw diet meaning that they exclude all products and foods of animal origins as well as food that has been cooked at a temperature greater than 118 degrees Fahrenheit.
The Paleo vegan is defined by the types of foods that are eaten. It is still meat and animal product free, but the foods that are chosen are selected from the Paleo diet.
This type of diet centers on certain types of foods that are believed to have been consumed during the Paleolithic era. It includes fish, meat, fruit, and vegetables but excludes grain and dairy products. Of course, for vegan purposes, the meat and fish are excluded.
What Are The Benefits Of Vegan & Vegetarian Diets?
Vegetarian and vegan diets have many health benefits. The tend to be much higher in vitamins C and E, magnesium, folic acid, and potassium. The fat content tends to be more unsaturated.
Vegan diets typically have less cholesterol and unsaturated fat that vegetarian diets and they contain more fiber. This translates to lower blood pressure, lower serum cholesterol, less risk of diabetes and heart disease, and much lower incidence of obesity. While some of these diets may require certain vitamin supplements such as calcium, vitamin D, vitamin B-12, and omega 3 fatty acids, most doctors agree that vegan and vegetarian diets are very healthy when done correctly.
Injury Medical Clinic: Migraine Treatment & Recovery
There has been a lot in the media lately about alkalinity and acidity in the body, but finding solid, straightforward information isn�t always easy. In short, acidity can cause a number of health issues. There are many benefits of bringing your body into balance.
What Is High Acidity?
The term acidity describes a condition where the body is affected by the excess production of gastric acids. Under normal conditions, hydrochloric acid is secreted by the stomach, aiding in the digestion and breakdown of food.
However, when this normal process is triggered in such a way that it causes overproduction of the acid, it can result in health problems. Acidity can be caused by irregular eating patterns, fad diets, alcohol consumption, stress, smoking, an unhealthy diet, and a sedentary lifestyle. Symptoms can include:
Indigestion
Burning in the stomach
Belching
Sour taste
Burning in the throat
Constipation
Nausea
Restlessness
What Are The Dangers Of High Acidity In The Body?
When the body is acidic, it can affect everything from immunity to neurological function to bone health. The Japanese have linked acidity to degenerative diseases like arthritis, cancer, and osteoporosis.
An acidic body is also a very hospitable environment for bacteria and viruses to thrive meaning the person will often get sick more often. When the body is out of balance it becomes susceptible to conditions as simple as dandruff and as complex as diabetes. Interestingly, many people have reversed or gone into remission by simply bringing their body into balance.
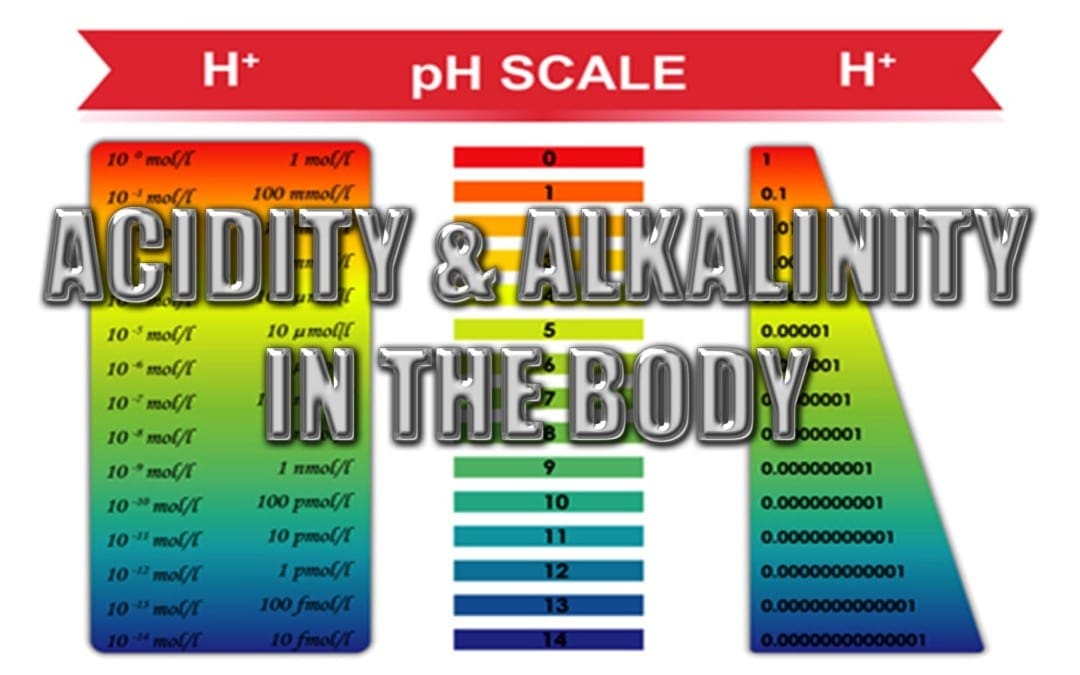
What Is Alkalinity?
In order to understand alkalinity, you need to understand pH levels. This is the measure used to determine how alkaline or acid something is. A pH of 0 is at the acidic end of the scale and means the thing being measured is completely acidic. At the other end of the scale, a pH of 14 is totally alkaline. The neutral point is a pH of 7.
Different parts of the body have different pH levels, meaning that some parts are more acidic while others are more alkaline. For instance, blood typically has a pH that is between 7.35 and 7.45, making it slightly alkaline. The stomach, on the other hand, is highly acidic, registering a pH of 3.5 or lower. Making the body more alkaline is not about making it completely alkaline � you need some acidity, it is necessary for digestion and other processes � it is more about bringing the body into balance.
What Are The Benefits Of Alkalinity?
When the body has increased alkalinity, bringing it into better pH balance, it is healthier and has a decreased risk of chronic illness. There is also less likelihood of illness. When the body is in a better pH balance it can result in many benefits including:
More energy
Improved cognitive function
Slowed aging process
Weight loss
Lower cancer risk
Decreased risk of chronic illness
Increased immunity
How Can You Bring Your Body Into Balance?
The best way to bring your body into better pH balance is by modifying your diet. As a rule of thumb, animal based foods like meat, eggs, and dairy tend to be more acidic. A vegetarian diet rich in plant-based foods like vegetables and fruits tend to be more alkaline. While the body does need a diet that includes both acidic and alkaline foods, a diet of processed foods and foods high in fat and sugar can cause too much acidity. By adjusting the diet, eliminating processed foods, and maintaining a healthier, more vegetarian based diet, you can bring your body into balance and enjoy better health as a result.
Injury Medical Clinic: Elderly & Geriatric Fitness
Many supermarkets have started offering their shoppers a choice in produce: organic or conventionally farmed. This can leave many wondering just what the difference is.
The truth is, both foods taste the same � or very close. Both have the same vitamins, minerals, and other nutrients, so what is the big difference?
It comes down to two major areas: safety and nutrition. That is what consumers need to understand when they are trying to make a decision on whether to purchase foods that have been conventionally farmed, or foods that are natural.
What Is �Organic�?
This is a misused word but the true meaning is that the term refers to how food is grown and processed. Organic farming is intended to encourage water and soil conservation as well as reduce pollution.
This type of farming does not use chemicals for controlling weeds, eliminating insects, or fertilizing. Most of the methods are completely natural. For instance, a farmer may use natural fertilizers to enrich the soil, strategically placed plants to control insects, and mulch or crop rotation to control weeds.
Organic Vs. Conventional Foods
Conventionally farmed products will often use chemicals for insect control and weed control. They often use some type of processing on their foods.
The fertilizer used in planting often has chemicals. The foods may even be genetically modified. Animals may be injected with steroids and hormones which can cause unpleasant or even harmful side effects.
These types of foods do not use any chemicals, they are not genetically modified, and they are not injected with antibiotics or steroids. The food has been very minimally processed � if at all.
There are no additives that don�t belong and could be potentially harmful. These foods are safer for human consumption and they are typically more nutritious.
How To Identify Organic Foods
In the United States, a food or product that is labeled as organic is required to be certified by the U.S. Department of Agriculture (USDA). The USDA has a certification program for natural growers and it has a set of very stringent standards that the product or food must meet.
There are some exemptions. For instance, a producer who does not sell more than $5,000 annually just in organic foods is not required to get the certification although they do have to adhere to the USDA�s stringent requirements for organic foods.
When a food carries the USDA Organic label, it means that it meets the requirements. While natural producers are not required to put the label on their products, many do.
The labeling varies, depending on the type of food. Single ingredient foods like eggs, vegetables, and fruits are considered to be 100 percent natural and are allowed to carry the USDA seal.
Foods that contain two or more ingredients, like breakfast cereal, are still allowed to use the USDA seal, but also must include the following information:
Organic � The product must be 95 percent organic or greater in order to be able to use this term
100 percent organic � The product must be completely organic or all of its ingredients must be natural
Made with organic ingredients � The product contains no less than 70 percent natural ingredients
If the product has less than 70 percent natural ingredients, they are not allowed to use the word �organic� anywhere on their product labels.
Health Benefits Of Natural Foods
The greatest health benefit of natural foods is what it does not provide. Organic growers do not use synthetic pesticides to protect their crops from disease, insects, and molds. This means that the food itself has never been touched by these chemicals.
Natural foods also do not have the food additives that conventional foods often do. They are free from artificial sweeteners, flavorings, and colorings as well as preservatives and monosodium glutamate. This means eating natural means that you aren�t putting those chemicals into your body. Plus, many people say that organic foods simply taste better.
If you have further questions or concerns about your particular diet, please ask us! Our Doctor of Chiropractic can help guide you toward a more healthy life, including the foods you consume.
Injury Medical Clinic: Accident Treatment & Recovery
Osteoporosis is a significant health problem in the United States and worldwide. An estimated 10 million individuals have osteoporosis in the U.S. alone and an additional 18 million individuals are at risk of developing the disease, according to the American Academy of Orthopaedic Surgeons (AAOS). Females make up 80 percent of individuals who suffer from osteoporosis, but it also occurs in males although it is often underdiagnosed and thus underreported.
What is equally disturbing is that another 34 million individuals in the U.S. are at risk of developing osteopenia, a common precursor to osteoporosis. Many experts blame the typical American diet and lifestyle, although genetics can also contribute to a person�s likelihood of developing either of the diseases. The prevalence of both osteoporosis and osteopenia are serious health issues so it is important to understand them.
What Is Osteopenia?
Osteopenia is often a warning sign of impending osteoporosis. Nearly half of all Americans who are more than 50 years old have the disease.
Osteopenia is a bone disease, marked by a decrease in bone mineral density � or bone loss. While it is not as devastating as osteoporosis, it is a strong indicator that the patient will eventually develop the disease.
Nutrition and exercise are common treatments for osteopenia. Occasionally doctors will prescribe medication, but that is usually not the preferred treatment. Exercise, specifically weight bearing exercise, is a very effective treatment and preventative measure against these diseases.
Incorporating calcium and vitamin D are also common treatments. These can be in the form of supplements, but patients are also encouraged to eat calcium rich foods such as yogurt, leafy greens like spinach, and sardines.
What Is Osteoporosis?
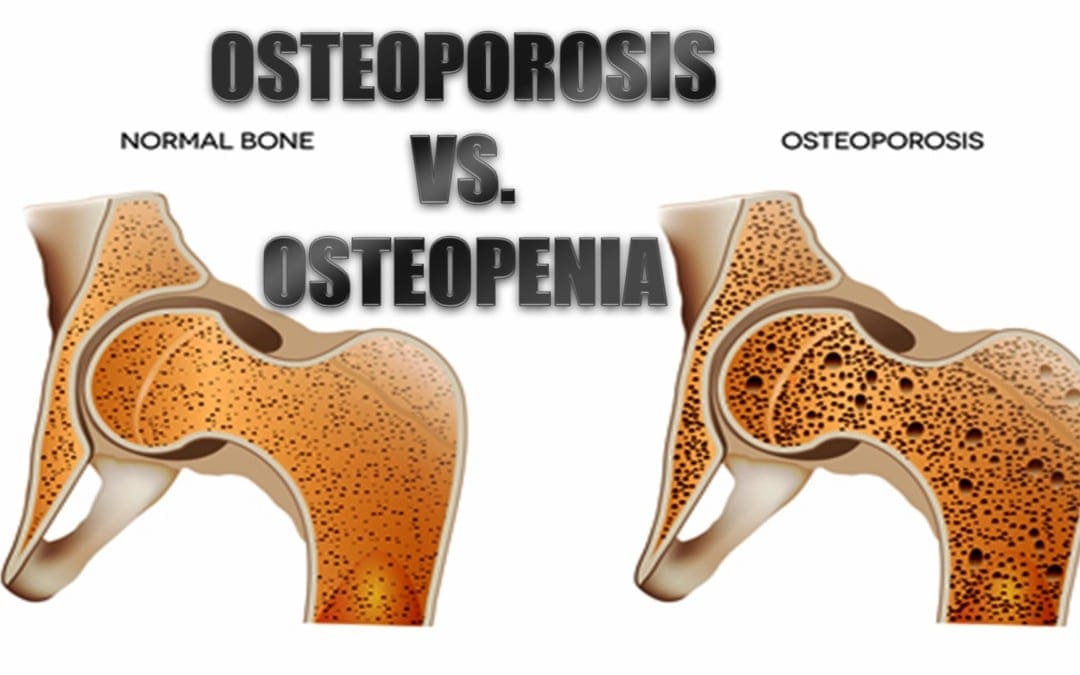
Osteoporosis is a serious condition that causes bones to become extremely brittle and weak. The word �Osteoporosis� literally means �porous bone� which is indicative of the primary characteristic of the disease.
When the bone is viewed under a microscope, it has tiny holes in its surface. While healthy bone has a honeycomb appearance under a microscope, bone with osteoporosis has much larger spaces and holes. The mass and density of osteoporotic bone is severely compromised. This can result in frequent broken bones as well as chronic pain and a patient can even lose several inches in height.
Patients with osteoporosis can also experience limited mobility due to the disease or broken bones that may occur as a result. This can lead to other health problems including depression and obesity. These conditions can exacerbate the disease itself and increase the patient�s pain. Often patients with osteoporosis, particularly at advanced stages, require long term care in a facility such as a nursing home.
The real danger is not how devastating it is to bones, it is the way it can go undetected for so long. Often it is not discovered until a bone is actually broken or the patient�s upper back begins curving forward. Sometimes the patient may become shorter. At that stage it is usually very advanced. With the right treatment, though, it can be slowed or stopped. Sometimes bone density can be improved and the disorder can be reversed at least to some degree.
What To Do If You Have Osteoporosis Or Osteopenia
If you suspect that you may have osteoporosis or osteopenia, or may be at risk for developing it, the first thing you need to do is talk to your doctor to confirm that you do have it. From there you can decide on a course of action which is usually exercise, diet, lifestyle changes, and chiropractic treatments. The sooner you take steps to protect and improve your health, the less likely you are to develop long term conditions.
Injury Medical Clinic: Fibromyalgia Care & Treatment
Everyone has stiff, sore muscles now and then. From overdoing it at the gym to sleeping in an awkward position, there are many reasons you might feel some muscular aches and pains. Some medical conditions or illnesses can also cause soreness. Several studies have found a remarkable, effective, inexpensive cure that is natural and safe � magnesium.
Pain � It�s All In Your Head
Well, it�s in your brain, anyway. A chemical in the brain, NMDA, is responsible for pain. When this brain chemical is overly stimulated, the body experiences pain. The way the brain processes pain in an individual determines how that person will experience it and manage it.
There are very few medications that deal directly with NMDA, balancing it and decreasing its production. However, the side effects of these drugs are usually significant and undesirable. Magnesium has been found to calm production of NMDA without causing the side effects or toxicity. What�s more, magnesium is very inexpensive. It is far cheaper than pharmaceuticals at just pennies a dose. One drawback is that the FDA has not yet put its stamp of approval on the mineral that is often called the �gateway to health.�
Clinical Studies Find Magnesium Is An Effective Way To Relieve Pain
A study published in The Journal of Physiology in October 2010, explores the effectiveness of magnesium in decreasing nerve pain. The study, conducted on rats, found a strong link between magnesium deficiency and pain. In fact, that authors of the study suggest that pain is increased, or the sensitivity to pain is increased, due to magnesium deficiency.
As people are moving away from fresh foods, processed foods are becoming more prevalent. While processed foods offer easy, quick preparation and gratification, the trade-off has been a significant decrease in nutrition, leaving most people magnesium deficient. However, adding a magnesium supplement that provides 250 to 500 mg of the mineral will not only eliminate the deficiency, but decrease the pain as well. This usually happens surprisingly quickly � after only a few weeks you will notice a definite difference.
Chia Seeds Are High In Magnesium.
Other Benefits Of Magnesium
Magnesium has a wide range of uses and benefits for the entire body. It has long been used to treat indigestion as well as constipation when taken by mouth. For heartburn and indigestion, magnesium hydroxide has been noted as the fastest acting. It is also given to pregnant women to treat high blood pressure (pre-eclampsia and eclampsia). When given as a shot or by IV, magnesium helps lower blood pressure during pregnancy. It is also the treatment of choice for eclampsia because it reduces the risk of seizures that accompany the condition.
Magnesium, given intravenously, is effective in treating torsades de pointes, a type of irregular heartbeat. Additionally, it is believed to help these other conditions:
Various types of pain including nerve damage associated with certain cancers, pain after surgery, pain after hysterectomy, and chest pain.
A healthy diet, regular exercise, and reducing the stress in your life will also help with your pain management. When your body is properly nourished it functions at a more optimal level, meaning not just less pain, but better management of it. Exercise causes your brain to produce endorphins which not only minimize pain, but also boost your mood.
Stress can make you more sensitive to pain, causing you to feel it more and experience it on a more intense level. It decreases your ability to tolerate pain and manage it. Even learning relaxation techniques and breathing exercises can help you better manage stress that you may not be able to eliminate completely. Adding magnesium to your diet can help improve your overall wellbeing as well as decrease your pain.
Foods: Arthritis pain can be debilitating. According to the Centers for Disease Control (CDC), between the years of 2010 and 2012, an estimated 22.7 percent, or 52.5 million, adults in the United States alone were diagnosed by a doctor with arthritis, rheumatoid arthritis, lupus, gout, or fibromyalgia � annually. Also during that time, almost 50 percent of adults 65 or older were diagnosed with arthritis. It is estimated that by the year 2040, 78 million Americans ranging in age from 18 years old to 85-year-old will be diagnosed with arthritis. What�s more, nearly 1 in every 250 (around 294,000) children in the U.S. under 18 years old suffer from a form of arthritis or rheumatic condition.
A Case For Healthy Eating
As medications and treatments get more expensive and drugs have significant unpleasant (and sometimes horrifying) side effects, more people are looking toward natural ways to treat their arthritis pain. In most cases they need look no further than the foods that they eat. While there is not nutritional magic bullet, studies have shown that getting the right nutrition from certain foods can help to minimize inflammation and pain that comes from arthritis. It can also help with your overall health and influence the symptoms as well as progression of conditions that may be related to arthritis.
There are certain foods that act as anti-inflammatories while other can increase inflammation. Arthritis sufferers who learn what foods to eat and which ones to avoid can enjoy better pain management, improved mobility, a more active lifestyle, and a more positive outlook on life. These foods provide great benefits for patients with rheumatoid arthritis, osteoarthritis, osteoporosis, gout, and other forms of inflammation caused by arthritis.
Foods That Fight Arthritis Inflammation
Different types of foods seem to affect different types of arthritis. The Arthritis Foundation offers some very good guidelines on dietary recommendations for arthritis sufferers based on their type of arthritis.
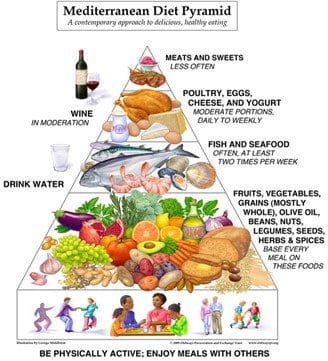
Foods rich in omega-3 fatty acids, phytochemicals, and antioxidants have powerful anti-inflammatory properties. These types of foods are the core of the Mediterranean style diet which consists of olive oil, fish, fresh vegetables, fruits, beans, seeds, and nuts. It should be stressed that choosing fresh foods in these categories is best. The key is to select foods that are as minimally processed as possible and contain no additives or preservatives. This means that most canned foods should be excluded. However, many supermarkets now have olive bars and other fresh, healthier food options that direct consumers away from processed, unhealthy food items. Fiber also plays a significant part in reducing arthritic inflammation.
Specific foods to incorporate into your diet to combat arthritis pain include:
Salmon
Extra virgin olive oil
Tuna
Mackerel
Egg yolks
Milk
Green tea
Oatmeal
Wild and brown rice
Barley
Quinoa
Beans
Tart cherries
Berries � blueberries, blackberries, raspberries, and strawberries
Broccoli
Brussels sprouts
Cabbage
Foods That Increase Arthritis Inflammation
Just as there are foodstuff that help alleviate arthritis pain, there are also foods that increase it. The Arthritis Foundation offers advice on foods that should be avoided by arthritis sufferers as they have been shown to increase pain and inflammation.
Sugar � Read the labels! Anything ingredient that ends in �ose� is a form of sugar. This includes sucrose and fructose.
Saturated fat � Cheese, pizza, red meat, pasta dishes, full fat dairy
Trans fats � Processed snacks, cookies, crackers, stick margarine, fast food, donuts, anything fried, frozen breakfast products
Refined carbs � Crackers, rolls, bread, white potatoes, white rice
MSG � A food additive found in soy sauce and many Asian prepared meals, deli meats, prepared soups, salad dressings
Gluten and casein � Dairy and wheat products, whey protein, rye, and wheat
Aspartame � Most diet sodas, artificial sweeteners, many �diet� or �sugar free� products
Alcohol
Paying attention to what you put into your body will not only help you better manage pain and inflammation, it will also help you feel better both physically and emotionally. A healthy, fresh diet can literally change your life.
Injury Medical Clinic: Elderly & Geriatric Fitness
The human body needs vitamin D in order to build strong muscles and bones. When the body does not get enough vitamin D, it is not able to absorb calcium effectively. This makes it very important for good bone health. Children who do not get adequate vitamin D develop rickets, a condition that causes weak bones, deformities in the skeleton, and a stooped posture.
What Is Vitamin D?
Most people believe that vitamin D is a vitamin; it isn�t. It is actually a hormone. A vitamin is a nutrient that the human body requires but is unable to produce. This means that it can only be obtained through supplements and food.
However, the body is able to manufacture this vitamin. When the skin is exposed to the appropriate sunlight, the body begins a process that produces vitamin D. It should also be noted that vitamin D plays a part in a strong immune system and can prevent certain chronic diseases in older adults.
There are supplements for people who do not produce enough vitamin D or who do not get adequate amounts in the food that they eat (fish liver oils, certain fish, and egg yolks are good sources). Children and adults typically do not get enough from their foods and activities. People spend a great deal of time indoors with adults at work and children at school. The emergence of digital devices and video games has managed to keep children inside as they engage in these activities.
This vitamin is not measured in milligrams like many other supplements, but in International Units (IU) instead. Research has caused the daily recommended allowance for vitamin D to increase over the years, and the current recommendation is 400 IU. It has been determined that this amount is the most beneficial in promoting healthy bones.
The Role Of The Skeletal System
The skeletal system has several functions. The first and most obvious is that it is the structural support for the body. It also protects vital organs.
For instance, the skull protects the brain and the rib cage protects the lungs and heart. It is also an anchor point for muscle so it helps with mobility. The red bone marrow provides illness fighting white blood cells, as well as red blood cells. Calcium is stored in the marrow, as is phosphorous. Certain minerals and fats are stored in the yellow marrow which is found in the long bones of the body.
How Vitamin D Benefits The Skeletal System
Getting enough vitamin D helps the body absorb calcium which is a bone building mineral. In addition to that task, it also promotes good muscle health.
Stronger muscles can work much more effectively in protecting the muscles and supporting the skeletal system. This can help with joint health as well. Older people who have adequate vitamin D do not fall down as often and people of all ages have fewer broken bones.
Results Of Vitamin D Deficiency
Vitamin D deficiency is a serious condition mainly due to its essential role in the body�s ability to absorb calcium. Muscle weakness and bone pain are two common symptoms, but are typically seen in more severe cases.
A simple blood test can check for vitamin D levels � and it should be checked regularly. Even �minor� cases of low vitamin (those without any symptoms) have been linked to some serious health conditions including:
Increased risk of death due to cardiovascular disease
Vitamin D is generally very accessible. You can get it through foods and sunlight or via a supplement. People who may have some trouble getting adequate amounts are those who have limited exposure to sunlight, fail to consume the necessary levels of the vitamin, and people who have dark skin. If you think that you may have low vitamin D, it is best to talk to your doctor so you can come up with a plan to get your body back in balance.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 What Is Osteoporosis?
What Is Osteoporosis?