Watermelon, one of the summer’s main fruits, is low in calories and rich in water. It provides an excellent source of vitamins A and C and lycopene and is less acidic than citrus fruits and tomatoes. The whole fruit is edible. The watermelon can be used as frozen chunks for water or seltzer drinks, smoothies, salsas, and salads; the rind can be stir-fried, stewed, or pickled, and the subtle sweetness pairs well with cheese, nuts, and other protein sources.
Watermelon
Watermelon poses few risks, with research deeming the fruit nontoxic. Side effects from eating too much watermelon can include abdominal discomfort, bloating, and gas.
The fruit does contain sugar, recommending individuals with diabetes should be careful to avoid sugar spikes.
Vitamins and Minerals
A fully ripe red watermelon contains higher nutrients than a less ripe watermelon.
A single serving is a healthy source of vitamins C and A, providing a significant percentage of the daily requirement.
Vitamin C aids in wound healing and can help increase anti-aging properties and immune system function.
Vitamin A is important for eye health.
Calories
One cup of diced or balled watermelon contains about 46 calories.
Wedges around one-sixteenth of the melon, or 286 g, contain approximately 86 calories.
These antioxidants can help cell repair and lower the risk of infections and certain cancers.
Contributes to Weight Loss
A group of overweight adults participated in a study that found the group that ate watermelon instead of low-fat cookies felt fuller.
The watermelon group also showed reductions in body weight, body mass index, waist-to-hip ratio, and blood pressure.
Reduce Muscle Fatigue
The fruit contains a significant amount of the amino acid citrulline.
Capsules of concentrated citrulline are sold as nutritional supplements.
The benefits are not conclusive, but some studies show that supplements could reduce the feeling of fatigue.
Nutrition Fundamentals
References
Bailey, Stephen J et al. “Two weeks of watermelon juice supplementation improves nitric oxide bioavailability but not endurance exercise performance in humans.” Nitric oxide: biology and chemistry vol. 59 (2016): 10-20. doi:10.1016/j.niox.2016.06.008
Burton-Freeman, Britt, et al. “Watermelon and L-Citrulline in Cardio-Metabolic Health: Review of the Evidence 2000-2020.” Current atherosclerosis reports vol. 23,12 81. 11 Dec. 2021, doi:10.1007/s11883-021-00978-5
Figueroa, Arturo, et al. “Watermelon extract supplementation reduces ankle blood pressure and carotid augmentation index in obese adults with prehypertension or hypertension.” American Journal of Hypertension vol. 25,6 (2012): 640-3. doi:10.1038/ajh.2012.20
Glenn, J.M., Gray, M., Wethington, L.N. et al. Acute citrulline malate supplementation improves upper- and lower-body submaximal weightlifting exercise performance in resistance-trained females. Eur J Nutr 56, 775–784 (2017). https://doi.org/10.1007/s00394-015-1124-6
Martínez-Sánchez A., Ramos-Campo D. J., Fernández-Lobato B., Rubio-Arias J. A., Alacid F., & Aguayo E. (2017). Biochemical, physiological, and performance response of a functional watermelon juice enriched in L-citrulline during a half-marathon race. Food & Nutrition Research, 61. Retrieved from https://foodandnutritionresearch.net/index.php/fnr/article/view/1203
Naz, Ambreen, et al. “Watermelon lycopene and allied health claims.” EXCLI journal vol. 13 650-60. 3 Jun. 2014
Panche, A N et al. “Flavonoids: an overview.” Journal of nutritional science vol. 5 e47. 29 Dec. 2016, doi:10.1017/jns.2016.41
Volino-Souza, Mônica et al. “Current Evidence of Watermelon (Citrullus lanatus) Ingestion on Vascular Health: A Food Science and Technology Perspective.” Nutrients vol. 14,14 2913. 15 Jul. 2022, doi:10.3390/nu14142913
Gelatin is a stabilizer and thickener used to make desserts like fruit gelatin, pudding, mousse, marshmallows, candy, cakes, ice cream, and certain yogurts. It is also used in some shampoos and skincare products. Because animal products are used to make gelatin, it is not a vegan-friendly food, and even some non-vegans choose not to eat it. However, there are gelatin alternatives that are made from non-animal sources. The use of gelatin may provide certain health benefits, and there are some medical uses for pharmaceutical-grade gelatin.
Gelatin Health
Gelatin is affirmed as generally recognized as safe/GRAS by the U.S. Food and Drug Administration. Gelatin is made by boiling the skin, tendons, ligaments, or bones of animals – cows or pigs in water. This process releases collagen, a protein that provides structure and is the most abundant in the human body. Once the collagen is extracted, it is:
Concentrated
Filtered
Cooled
Extruded
Dried
Alternatives
Thickening agents can be made from different ingredients. These include:
Agar-agar
Also called agar, this thickener is made from cooked and pressed seaweed.
This gelling agent is available online and in some supermarkets in powdered, flaked, and bar form.
When cooking with it, substitute agar for gelatin using equal amounts if using the powder.
If using flakes, a tablespoon equals about a teaspoon of the powder.
Certain citrus fruits require more agar when substituting.
Agar does not gel well for recipes that include uncooked mangoes, papaya, and pineapple.
Pectin
Pectin is a gelling agent found naturally in apples and citrus fruits.
Food manufacturers use pectin to make some yogurts and candies and enhance fruit-based beverages.
It can also thicken jams, jellies, and other foods.
This thickener is usually for making softer gels and puddings.
Benefits
Improved Bone Health
A benefit of gelatin is the protection of bones; however, evidence supporting its use is limited.
An early study found that hydrolyzed gelatin, such as pharmaceutical grade, may help reduce pain symptoms in individuals with knee or hip osteoarthritis.
Researchers thought that it could have a beneficial effect on cartilage metabolism.
A study found that adding gelatin to an intermittent exercise program improved collagen synthesis and could aid in injury prevention and tissue repair.
Treatment of Diarrhea
Some studies have suggested that gelatin tannate, which contains tannic acid, can reduce chronic diarrhea.
One study found that using gelatin tannate and other products like probiotics could be effective.
However, further research is needed.
Recipe Alternative
Individuals following specific diets or nutritional plans can use gelatin to thicken foods instead of ingredients that they are avoiding or removing from their eating plan.
It can be used by those following low or no – carb or grain-free diets.
Individuals with wheat allergies, celiac disease, non-celiac gluten sensitivity, or who follow a gluten-free diet can use gelatin or other thickeners instead of flour.
Adding flour to foods like soups and stews can increase the carbohydrate count.
Cornstarch is one replacement that thickens when food is heated, like flour; however, gelatin thickens when food is cooled.
For example, some chefs use 1 ½ teaspoons of gelatin per cup of stock to thicken soups.
Nutrition
The USDA provides the following nutrition information for a single envelope or around one tablespoon/7 grams of gelatin.
Carbohydrates
There are about 30 calories per tablespoon, and none of the calories are from carbohydrates.
There are 0 grams of total carbohydrates, 0 grams of sugar, and 0 grams of fiber.
Because there are no carbohydrates, it will not impact blood sugar levels.
However, it is not usually consumed by itself.
It is commonly used to thicken desserts with sugar and carbohydrates that can elevate blood sugar levels.
Fats
There is no fat in a tablespoon serving of gelatin.
A 100-gram serving contains less than a gram of fat.
Protein
Gelatin provides about 6 grams of protein in one tablespoon serving.
It should not be considered a high-protein food.
Vitamins and Minerals
The powder does not contribute any significant micronutrients.
Does not provide vitamins or minerals.
Storage and Safety
It should be kept in a sealed container and stored in a cool, dry place.
It should stay fresh for about three years when unopened and stored correctly.
It should not be frozen.
Chiropractic Success Story
References
Blanco, Francisco J, and Ronald K June 2nd. “Cartilage Metabolism, Mitochondria, and Osteoarthritis.” The Journal of the American Academy of Orthopaedic Surgeons vol. 28,6 (2020): e242-e244. doi:10.5435/JAAOS-D-19-00442
Daneault, Audrey, et al. “Biological effect of hydrolyzed collagen on bone metabolism.” Critical Reviews in food science and Nutrition vol. 57,9 (2017): 1922-1937. doi:10.1080/10408398.2015.1038377
Florez, Ivan D et al. “Gelatin tannate for acute diarrhea and gastroenteritis in children: a systematic review and meta-analysis.” Archives of Disease in Childhood vol. 105,2 (2020): 141-146. doi:10.1136/arch dis child-2018-316385
Hölzl, Katja, et al. “Gelatin methacryloyl as an environment for chondrocytes and cell delivery to superficial cartilage defects.” Journal of tissue engineering and regenerative medicine vol. 16,2 (2022): 207-222. doi:10.1002/term.3273
Lopetuso, L et al. “Gelatin tannate and tyndallized probiotics: a novel approach for the treatment of diarrhea.” European Review for Medical and pharmacological sciences vol. 21,4 (2017): 873-883.
Shaw, Gregory, et al. “Vitamin C-enriched gelatin supplementation before intermittent activity augments collagen synthesis.” The American Journal of clinical nutrition vol. 105,1 (2017): 136-143. doi:10.3945/ajcn.116.138594
Tehranzadeh, J et al. “Cartilage metabolism in osteoarthritis and the influence of viscosupplementation and steroid: a review.” Acta radiologica (Stockholm, Sweden : 1987) vol. 46,3 (2005): 288-96. doi:10.1080/02841850510016027
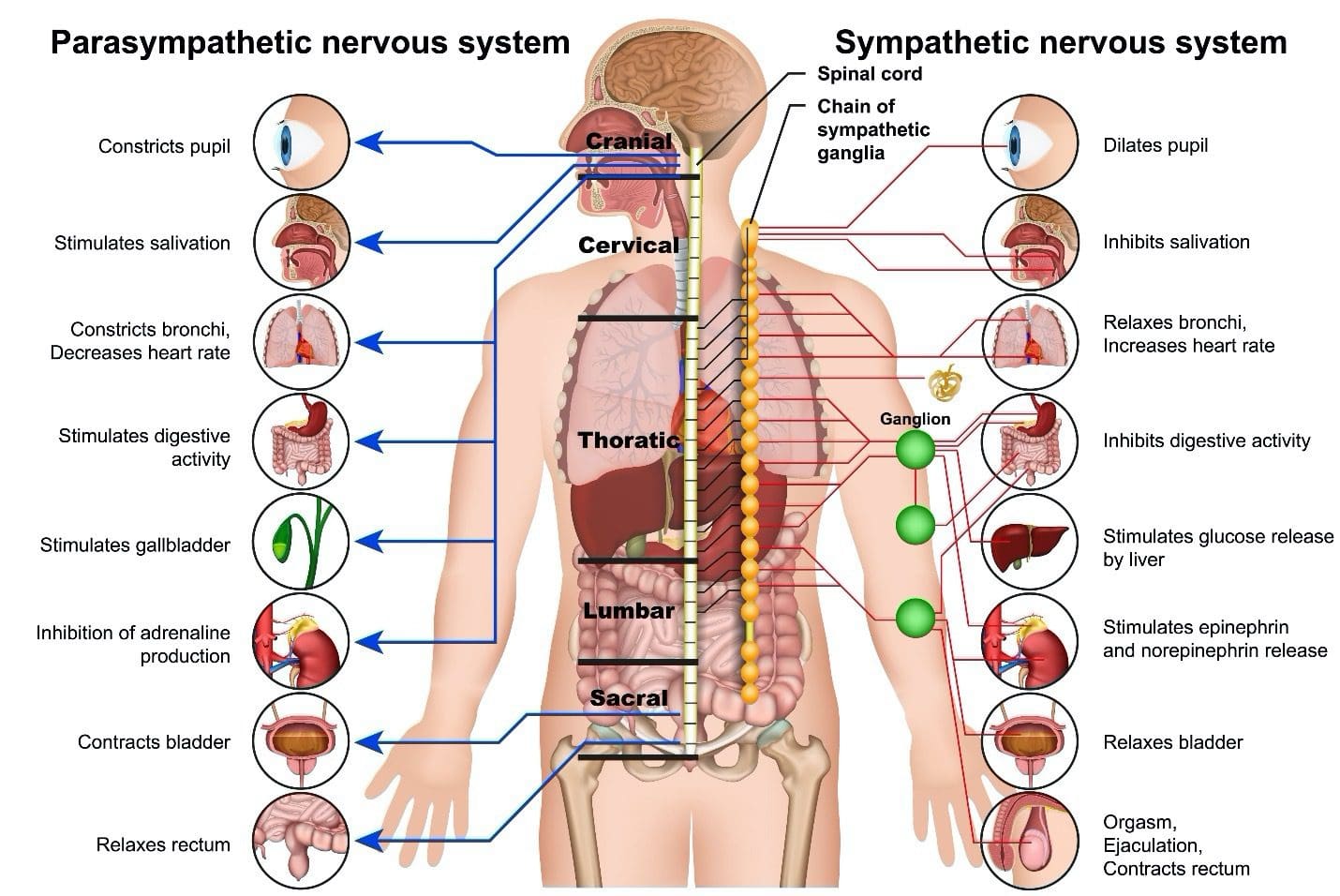
The nervous system is a network of roads that feed into highways that connect to an interstate system. The roads are the nerves that innervate the muscles and the extremities; the interstate is the spinal cord. When the system works optimally, the nerves consistently transmit signals/messages to and from the brain without any problems. The signals travel back and forth, and the traffic flows smoothly. When the activities of these nerves and cells get disrupted, the central nervous system fails to perform basic functions that can cause musculoskeletal issues, conditions, and CNS diseases. Keeping the nervous system strong can be done by adopting ways to maintain health and function.
The Nervous System
The system regulates and coordinates body activities and is made up of two major divisions, these include the following:
Central nervous system – consists of the brain and spinal cord.
Peripheral nervous system – consists of all other neural elements, including the peripheral and autonomic nerves.
The principal organs of the nervous system include:
Brain
Spinal cord
Eyes
Ears
Sensory taste organs
Sensory smell organs
Sensory receptors are located in the muscles, joints, skin, and other areas throughout the body.
A complex network of nerves, the nervous system reacts to internal and external stimuli through several physical actions to maintain vital bodily functions. These include:
The symptoms of a nervous system disorder may present like other medical conditions or problems. Always see a professional healthcare provider for proper diagnosis.
Keeping the Nervous System Strong
Nutrition To Transmit Signals
Nerves need minerals, proteins, and vitamins to send electrical impulses. Foods that contain these nutrients include:
Calcium — regulates the generated and transmitted electrical impulses. Milk, leafy greens and eggs are rich sources of calcium.
Potassium – bananas, oranges, pomegranates, and prunes, are good sources of potassium.
Dark chocolate contains tryptophan, an amino acid that produces and maintains neurotransmitters.
Vitamin B — Vitamins B1, B2, and B6 assist the nerves in sending impulses from the brain to the body.
B Vitamins Provide Nerve Protection
A myelin sheath covers the nerves for protection and provides insulation for transmitting. Worn-out or damaged myelin sheaths have been associated with illnesses like Alzheimer’s. Vitamin B12 helps repair damaged nerves and regenerate fibers. It is found in beef, poultry, eggs, and seafood.
Folate or vitamin B9 promotes Schwann cell proliferation, migration, and production of nerve growth factor. This vitamin is found in spinach, pomegranates, and beets.
Stretching and Breathing
Stress produces the hormone cortisol. Constant production of cortisol affects the nervous system, which can affect reflexes, concentration, and memory. Stretching the body and learning breathing exercises and relaxation techniques activates the part of the nervous system responsible for breathing and heart rate, decreasing cortisol levels.
Chiropractic Care and Functional Medicine
The spinal cord has multiple functions in restoring, rejuvenating, and keeping the nervous system strong. Chiropractic care has a highly responsive therapeutic effect on the nervous system because of its focus on the spine. Spinal decompression, traction, soft tissue manipulation, and other treatments help regulate and restore the function of the nervous system. Chiropractic benefits:
Reduces or eliminates pain.
Regulates respiration.
Lowers heart rate.
Improves the quality of sleep.
Increases energy.
Improves digestive function.
Improves cognition and clarity.
Improves balance and coordination.
Increases flexibility and mobility.
Reduces or eliminates headaches and migraines.
Hyperhomocysteinemia
References
Archibald, Lennox K., and Ronald G. Quisling. “Central Nervous System Infections.” Textbook of Neurointensive Care 427–517. 7 May. 2013, doi:10.1007/978-1-4471-5226-2_22
Bhagavati, Satyakam. “Autoimmune Disorders of the Nervous System: Pathophysiology, Clinical Features, and Therapy.” Frontiers in neurology vol. 12 664664. 14 Apr. 2021, doi:10.3389/fneur.2021.664664
Gyer, Giles, et al. “Spinal manipulation therapy: Is it all about the brain? A current review of the neurophysiological effects of manipulation.” Journal of integrative medicine vol. 17,5 (2019): 328-337. doi:10.1016/j.joim.2019.05.004
Jessen, Kristján R et al. “Schwann Cells: Development and Role in Nerve Repair.” Cold Spring Harbor perspectives in biology vol. 7,7 a020487. 8 May. 2015, doi:10.1101/cshperspect.a020487
Powers, Scott K et al. “Disease-Induced Skeletal Muscle Atrophy and Fatigue.” Medicine and science in sports and exercise vol. 48,11 (2016): 2307-2319. doi:10.1249/MSS.0000000000000975
Nutrition is integral to optimal health and can help treat and manage diseases that threaten the body. Mushrooms come in various shapes, sizes, and colors and have been used for their unique ability to add flavor and taste without sodium or fat. They are also healthy and tasty and contain various vitamins and minerals. Different mushrooms can provide distinct health benefits that can be increased brain function, help with hormonal balance, and as an antioxidant.
Mushroom
Research continues to uncover how mushrooms can improve everyday health and help mitigate the risk of developing health conditions like Alzheimer’s, heart disease, cancer, and diabetes. Mushrooms are recommended because they are:
Fat-free
Low in sodium
Low-calorie
Cholesterol-free
Packed with fiber
Nutritional benefits vary depending on the type of mushroom.
B vitamins
Mushrooms are rich in B vitamins: riboflavin, niacin, and pantothenic acid, which help maintain heart health. Riboflavin supports red blood cells. Niacin assists the digestive system and helps keep healthy skin. Pantothenic acid supports nervous system function and helps the body make necessary hormones.
Minerals
They are a great source of minerals – Selenium, Copper, Thiamin, Magnesium, and Phosphorus. Copper helps the body create red blood cells to deliver oxygen and maintain healthy bones and nerves. Potassium supports heart, muscle, and nerve function.
Antioxidants
Antioxidants help protect the body from damaging free radicals that can cause heart disease and cancer. They also protect against damage from aging and increase immune system function.
Beta-glucan
Beta-glucan is a soluble dietary fiber linked to improved cholesterol levels and supports heart health. It helps the body regulate blood sugar, which helps reduce the risk of type 2 diabetes.
Cordyceps
Cordyceps increases energy levels by utilizing oxygen more efficiently and enhancing circulation. This can be especially helpful for athletes or individuals who regularly work out and has been shown to improve exercise and athletic performance and speed up muscle recovery.
Shiitake
This mushroom has benefits that are particularly good for the heart, as they contain phytonutrients, which aid in:
Preventing plaque buildup
Maintaining blood pressure
Maintaining circulation
Lowering cholesterol
Chaga
Chaga mushrooms are full of antioxidants, making them excellent for fighting free radicals and inflammation. This mushroom combats oxidative stress, inflammation, and aging. And it can help prevent or slow cancer growth and has been found to help lower low-density lipoprotein – LDL cholesterol.
Mushroom Preparation
Mushrooms are almost always available in the produce section of any grocery or health food store. Make sure to wash them thoroughly first. Example: Cremini mushrooms can be:
Eaten raw or cooked, sliced or unsliced.
Simmered in water for 5 minutes until soft
Sauteed – cook the mushrooms in a pan with olive oil on medium heat for eight minutes, frequently stirring until they brown at the edges.
Sprinkled raw over meals to add more texture and flavor.
Ways to add mushrooms to a nutrition plan:
With eggs in the morning.
Mix into cooked beef, chicken, or turkey.
Cook mushrooms with garlic and butter for a side dish.
Add to a stir-fry with other vegetables.
Add to homemade pizza.
As an ingredient in pasta sauce.
Add to salads.
Make cream of mushroom soup.
Always talk to a doctor, nutritionist, or dietician before to confirm whether adding mushrooms is safe, especially if pregnant or using medications, as certain mushrooms can cause side effects like an upset stomach or allergies.
Food as Medicine
References
Fukushima, M et al. “Cholesterol-lowering effects of maitake (Grifola frondosa) fiber, shiitake (Lentinus edodes) fiber, and enokitake (Flammulina velutipes) fiber in rats.” Experimental biology and medicine (Maywood, N.J.) vol. 226,8 (2001): 758-65. doi:10.1177/153537020222600808
Kabir, Y et al. “Effect of shiitake (Lentinus edodes) and maitake (Grifola frondosa) mushrooms on blood pressure and plasma lipids of spontaneously hypertensive rats.” Journal of nutritional science and vitaminology vol. 33,5 (1987): 341-6. doi:10.3177/jnsv.33.341
Kolotushkina, E V et al. “The influence of Hericium erinaceus extract on myelination process in vitro.” Fiziolohichnyi zhurnal (Kiev, Ukraine : 1994) vol. 49,1 (2003): 38-45.
Ma, Gaoxing, et al. “Health benefits of edible mushroom polysaccharides and associated gut microbiota regulation.” Critical reviews in food science and nutrition vol. 62,24 (2022): 6646-6663. doi:10.1080/10408398.2021.1903385
Rop, Otakar, et al. “Beta-glucans in higher fungi and their health effects.” Nutrition reviews vol. 67,11 (2009): 624-31. doi:10.1111/j.1753-4887.2009.00230.x
Tuli, Hardeep S et al. “Pharmacological and therapeutic potential of Cordyceps with special reference to Cordycepin.” 3 Biotech vol. 4,1 (2014): 1-12. doi:10.1007/s13205-013-0121-9
Venturella, Giuseppe, et al. “Medicinal Mushrooms: Bioactive Compounds, Use, and Clinical Trials.” International journal of molecular sciences vol. 22,2 634. 10 Jan. 2021, doi:10.3390/ijms22020634
Arteries carry blood from the heart to the rest of the body. The veins transport blood back to the heart, and the valves in the veins stop the blood from flowing backward. When the veins have difficulties sending blood from the limbs back to the heart, this is known as venous insufficiency. With this condition, the blood does not flow back properly to the heart, causing blood to accumulate in the veins of the legs. Chiropractic care, therapeutic massage, and functional medicine can increase and improve circulation and help manage symptoms.
Venous Insufficiency
The circulatory system is responsible for transporting blood, oxygen, and nutrients to the cells in the body. This system consists of the heart, arteries, veins, and capillaries. When blood circulation is restricted, it can lead to a buildup of toxins and waste products, which can cause various health problems, including fatigue, muscle cramps, and dizziness. Unhealthy circulation can also contribute to other health conditions like heart disease, stroke, and diabetes. The most common causes of venous insufficiency include:
Blood clots
Varicose veins
A family history of venous insufficiency.
Deep vein thrombosis.
When forward flow through the veins is obstructed, such as in the case of a blood clot, blood builds up below the clot, which can lead to venous insufficiency.
In varicose veins, the valves can be missing or damaged, and blood leaks back through the defective valves.
In some cases, weakness in the leg muscles that push blood forward can also contribute to venous insufficiency.
Venous insufficiency is more common in women than men and is more likely in adults over 50.
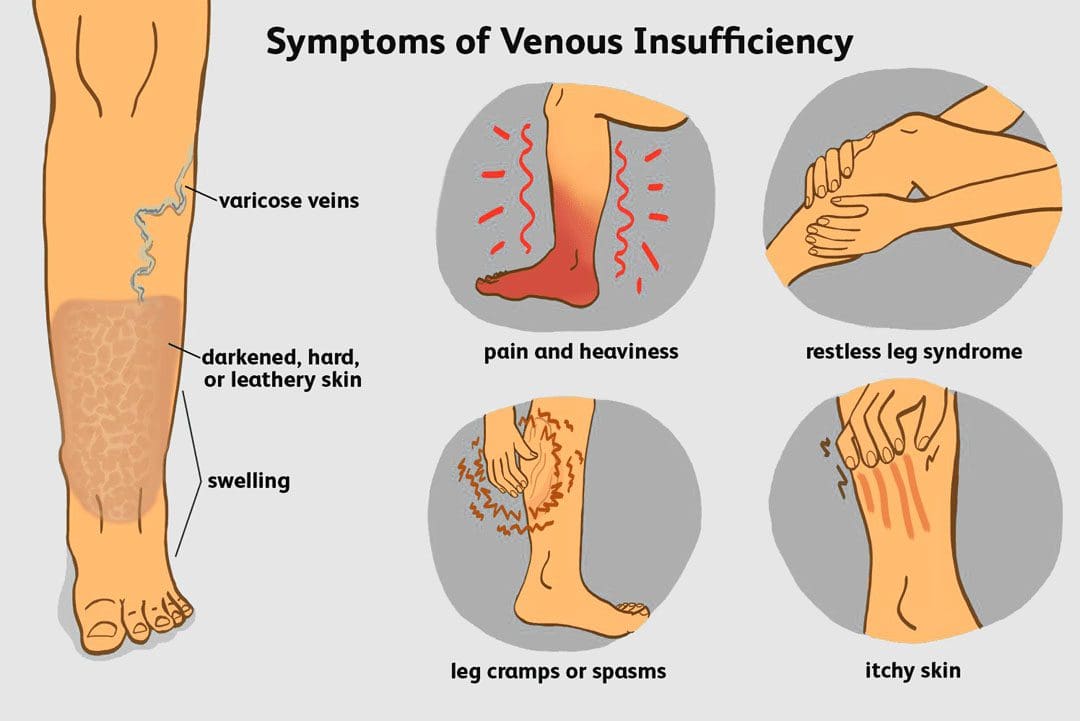
Circulation Symptoms
There are different symptoms associated with unhealthy circulation, and can include:
A doctor will perform a physical examination and take a complete medical history. They may order imaging tests to locate the source of the problem. These tests may include a venogram or a duplex ultrasound.
Venogram
A doctor will insert an intravenous contrast dye into the veins.
Contrast dye causes the blood vessels to appear opaque on the X-ray image, which helps the doctor see them on the image.
This dye will give the doctor a clear image of the blood vessels.
Duplex Ultrasound
A duplex ultrasound tests the speed and direction of blood circulation in the veins.
A technician will place gel on the skin and press a small hand-held instrument on and around the area.
The instrument uses sound waves that bounce back to a computer and produce images of blood circulation.
Treatment
Treatment will depend on various factors, including the reason for the condition and individual health status and history. Other factors a doctor will consider include:
These special stockings apply pressure on the ankle and lower leg.
They help improve blood circulation and reduce leg swelling.
Compression stockings come in a range of prescription strengths and lengths.
Strategies
Treatments can include several methods.
Improving Circulation
Chiropractic adjustments and vascular massage therapy on the legs can help improve blood circulation. Massage therapies such as vascular and lymphatic drainage massages aim to increase circulation, improve tissue nutrition, and can benefit patients with varicose veins and chronic venous insufficiency.
The technique for lymphatic drainage involves light strokes to move lymph fluid into lymph vessels.
The technique used to improve circulation involves short strokes to move blood from the valves to the veins.
However, massage therapy is not for all patients with vein diseases and conditions.
Massage therapy is not recommended for patients with advanced-stage vein disease, in which large and bulging veins, ulcerations, and discoloration are present.
Massaging the area could cause the weakened veins to burst, worsening the condition.
Massage therapy is also unsafe for patients with deep vein thrombosis (DVT), as it could dislodge a clot and cause it to travel.
Medications
Medications may be prescribed. These include:
Diuretics – medications that draw extra fluid from the body and are excreted through the kidneys.
Anticoagulants – medicines that thin the blood.
Pentoxifylline – medicine that helps improve blood circulation.
Surgery
More serious cases may require surgery. A doctor may suggest one of the following surgical procedures:
Surgical repair of the veins or valves.
Removing the damaged vein.
Minimally invasive endoscopic surgery – The surgeon inserts a thin tube with a camera to see and tie off damaged veins.
Laser surgery – A treatment that uses laser light to fade or close off damaged veins.
Vein bypass – A healthy vein is transplanted from a different body area. Generally used only in the upper thigh and as a last option for severe cases.
Venous Insufficiency: What You Need To Know
References
Annamaraju P, Baradhi KM. Pentoxifylline. [Updated 2022 Sep 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559096/
Evrard-Bras, M et al. “Drainage lymphatique manuel” [Manual lymphatic drainage]. La Revue du praticien vol. 50,11 (2000): 1199-203.
FIELDS, A. “Leg cramps.” California medicine vol. 92,3 (1960): 204-6.
Felty, Cindy L, and Thom W Rooke. “Compression therapy for chronic venous insufficiency.” Seminars in vascular surgery vol. 18,1 (2005): 36-40. doi:10.1053/j.semvascsurg.2004.12.010
Mayo Clinic Staff. (2017). Varicose veins.mayoclinic.org/diseases-conditions/varicose-veins/diagnosis-treatment/drc-20350649
Patel SK, Surowiec SM. Venous Insufficiency. [Updated 2022 Aug 1]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430975/
Youn, Young Jin, and Juyong Lee. “Chronic venous insufficiency and varicose veins of the lower extremities.” The Korean journal of internal medicine vol. 34,2 (2019): 269-283. doi:10.3904/kjim.2018.230
Bone Broth Benefits: Bone broth is made by simmering the bones and connective tissue from just about any animal, including chicken, turkey, beef, pork, fish, lamb, bison, buffalo, and venison. It is a highly nutritious stock commonly used in soups, sauces, and gravies and recently as a health drink.Research has shown bone broth benefits, including increased immune system function and helping build up the body’s systems to overcome disorders like allergies, asthma, and arthritis. And the broth form allows the body to easily absorb minerals like calcium, magnesium, phosphorus, silicon, and sulfur.
Bone Broth Benefits
Bone broth dates back to prehistoric times when inedible animal parts like bones, hooves, and knuckles were turned into broth. It is important to understand that most store-bought stocks and broths are not made of bone or animals. Companies, instead, use lab-produced meat flavors. Homemade bone broth is made by simmering bones, water, and vinegar for 10 -12 hours, extracting the collagen from the bones into the liquid. This creates a rich form of stock. Bones are often roasted before making the broth.
Simple Recipe
Making bone broth is very simple, and there are many recipes online. A large pot, water, bones, and vinegar are all that is necessary to get started, here’s an easy recipe:
Ingredients
One gallon (4 liters) of water.
2 tbsp (30 mL) apple cider vinegar.
Adding vinegar is important because it extracts valuable nutrients out of the bones and into the water.
2–4 pounds (around 1–2 kg) of animal bones.
Salt and pepper, to taste.
Vegetables, herbs, or spices can be added to create and enhance flavor.
Garlic, onion, celery, carrot, parsley, and thyme can be added in step one.
Directions
Place all ingredients in a large pot or slow cooker.
Bring to a boil.
Reduce to a simmer and cook for 12–24 hours.
The longer it cooks, the better it tastes and provides more nutrition.
Let the broth cool.
Strain into a large container and discard the bones.
Because of the long cooking, large amounts of collagen are extracted, making the bone broth gelatinous at room temperature.
Benefits
Digestion
Bone broth is a rich source of glutamine, an amino acid that improves digestion and gut health.
It can be particularly beneficial for people with digestive conditions such as leaky gut syndrome or inflammatory bowel disease.
Gelatin can also bind to water in the digestive tract, which helps foods move through the gut more easily.
Bone broth can benefit individuals with the following:
Leaky gut
Irritable bowel syndrome – IBS.
Inflammatory bowel disease/IBD like ulcerative colitis or Crohn’s disease.
Low Glycemic Index
Homemade vegetarian or meat-based broths are very low glycemic, with no added sugar, low in calories, and a great way to hydrate the body.
It can be a healthy snack between meals without an insulin spike that can lead to post-meal energy crashes.
Collagen Improves Hair, Skin, and Nail Health
Bone broth contains collagen. Collagen is a protein in structural and connective tissues that includes skin, bones, muscles, tendons, and ligaments.
The fibrous structure contributes to strength, shape, and elasticity and can fortify hair, skin, and nails.
Bone broth can be beneficial for pregnant women, as it can help preserve skin elasticity during pregnancy while the skin stretches and grows.
Anti-Inflammation
The amino acids glycine and arginine have anti-inflammatory effects.
Arginine may be especially beneficial for fighting chronic inflammation.
Protects Bones and Joints
Bone broth contains calcium for maintaining strong bones and preventing bone loss as the body ages.
Collagen also protects joints from age-related deterioration.
It can help individuals with bone and joint conditions like osteoarthritis.
Bones
Instead of throwing leftover bones from meals in the garbage, save them. They can be collected in a bag and stored in the freezer until ready to roast and cook. Individuals who don’t buy and eat whole chickens and bone-in meat can ask for them at the local butcher or farmers market. The meat department at most grocery stores will often have them. They’re inexpensive, and a butcher may even offer them for free. It is recommended to find pastured chicken or grass-fed beef bones as these are the healthiest and provide maximum health benefits.
Storage
Making broth in large batches is recommended, as it can only be stored safely in the refrigerator for up to 5 days.
To help the broth last longer, it can be frozen in small containers and heated up for individual servings as needed.
Functional Nutrition
References
Koutroubakis, I E et al. “Serum laminin and collagen IV in inflammatory bowel disease.” Journal of clinical pathology vol. 56,11 (2003): 817-20. doi:10.1136/jcp.56.11.817
Mar-Solís, Laura M et al. “Analysis of the Anti-Inflammatory Capacity of Bone Broth in a Murine Model of Ulcerative Colitis.” Medicina (Kaunas, Lithuania) vol. 57,11 1138. 20 Oct. 2021, doi:10.3390/medicina57111138
McCance, R A et al. “Bone, and vegetable broth.” Archives of disease in childhood vol. 9,52 (1934): 251-8. doi:10.1136/adc.9.52.251
Peterson, Orion J et al. “Neuroprotective Effect of Enriched Chicken Bone Broth as a Dietary Supplement in a Model of Migraine Mediated by Early Life Stress.” Journal of medicinal food vol. 23,12 (2020): 1259-1265. doi:10.1089/jmf.2019.0312
Maintaining kidney health is important to the body’s overall health and well-being. The kidneys are fist-sized organs located beneath the rib cage on both sides of the spine. A kidney detox maintains health allowing the body to filter and expel waste properly and produce hormones to help the body function at its full potential.
Kidney Health
The kidneys perform several functions that include:
Filters and cleanses out impurities from the blood.
Produces hormones that regulate blood pressure and control the production of red blood cells.
Filter’s waste products stored in the bladder and expelled through urine.
Activates vitamin D to support body absorption of calcium for bone repair and regulating muscle function.
Kidney Detox
A key measure of keeping the kidneys clean and healthy is to engage in a healthy nutrition plan. Doctors recommend implementing lifestyle changes to help the kidneys filter at full capacity. Certain foods can help detox the kidneys and promote their health.
Pumpkin seeds
Pumpkin seeds can help prevent the accumulation of uric acid, one of the compounds that cause kidney stones.
Grapes
These fruits contain a compound called resveratrol to reduce kidney inflammation.
Lemons
Lemons help with digestion.
They have vitamin C, which enhances the immune system and supports white blood cells to fight infections.
Citrate binds with calcium in the urine to stop the growth of calcium crystals, preventing kidney stones.
Carrots
Carrots have beta-carotene, alpha-carotene, and vitamin A.
Antioxidants for inflammation.
Ginger
Ginger can help in the dissolving process of kidney stones and prevents them from reforming.
Beets
Improves blood circulation to the kidneys.
Celery
Celery has alkaline and diuretic properties to help expel excess fluids.
It has coumarins which can help to increase vascular flow.
It is rich in vitamins D, C, and K.
Apples
Apples contain fiber to unclog the arteries, specifically the kidney arteries will improve filtration.
Maintain Hydration
The human body is almost 60 percent water, with every organ requiring water.
The kidneys (body filtration system) require water to secrete urine.
Urine is the primary waste product that allows the body to eliminate unwanted and unnecessary substances.
Low water intake means low urine volume.
Low urine output can lead to kidney dysfunction, like kidney stones.
Maintaining the body’s hydration is crucial so the kidneys can thoroughly flush out excess waste materials.
This is an example of a two-day kidney cleanse to help strengthen the kidneys and detoxify the body.
Day 1
Breakfast
Smoothie made with:
8 ounces of fresh lemon, ginger, and beet juice
1/4 cup of sweetened dried cranberries
Lunch
Smoothie made with:
1 cup almond milk
1/2 cup tofu
1/2 cup spinach
1/4 cup berries
1/2 apple
Two tablespoons of pumpkin seeds
Dinner
Large mixed-greens salad
4 ounces of lean protein – chicken, fish, or tofu
Top with 1/2 cup of grapes
1/4 cup peanuts
Day 2
Breakfast
Smoothie made with:
1 cup soy milk
One frozen banana
1/2 cup spinach
1/2 cup blueberries
One teaspoon spirulina
Lunch
A bowl of:
1 cup orzo rice
1 cup fresh fruit
Two tablespoons of pumpkin seeds
Dinner
Large mixed-greens salad
4 ounces of lean protein – chicken, fish, or tofu
Top with 1/2 cup of cooked barley
Add fresh lemon juice
4 ounces each of unsweetened cherry juice and orange juice
Consult a healthcare provider, nutritionist, or dietitian to ensure it is safe.
Dietary Prescription
References
Chen, Teresa K et al. “Chronic Kidney Disease Diagnosis and Management: A Review.” JAMA vol. 322,13 (2019): 1294-1304. doi:10.1001/jama.2019.14745
Den Hartogh, Danja J, and Evangelia Tsiani. “Health Benefits of Resveratrol in Kidney Disease: Evidence from In Vitro and In Vivo Studies.” Nutrients vol. 11,7 1624. 17 Jul. 2019, doi:10.3390/nu11071624
Pizzorno, Joseph. “The Kidney Dysfunction Epidemic, Part 1: Causes.” Integrative medicine (Encinitas, Calif.) vol. 14,6 (2015): 8-13.
Saldanha, Juliana F et al. “Resveratrol: why is it a promising therapy for chronic kidney disease patients?.” Oxidative medicine and cellular longevity vol. 2013 (2013): 963217. doi:10.1155/2013/963217
Tack, Ivan MD, Ph.D. Effects of Water Consumption on Kidney Function and Excretion. Nutrition Today: November 2010 – Volume 45 – Issue 6 – p S37-S40
doi: 10.1097/NT.0b013e3181fe4376
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine









 Bone Broth Benefits
Bone Broth Benefits







