Lower abdominal pain relieved by passing stool or gas
Alternating constipation and diarrhea
A hard, dry, or small stool
Use laxatives frequently
If you are experiencing any of these situations, then you must be experiencing gastrointestinal impairments in your body.
Gastrointestinal Impairments
The digestive system is consisting of the gastrointestinal tract, which is home to the intestines, the liver, the colon, the gallbladder, the pancreas, and the stomach. When there is a disruption in the gastrointestinal tract, it can cause inflammation and chronic illnesses that can harm the body. Functional disorders in the digestive tract (GI tract) can look normal in the body, but it doesn’t work correctly.
Many factors can upset the GI tract and its motility, including:
Eating a diet low in fiber
Not getting enough exercise
Traveling or changes in a routine
Eating large amounts of dairy blankets
Stress
Resisting the urge to have a bowel movement
Overusing laxatives
Taking certain medicines
Some of the most common problems that can affect the GI tract are constipation, IBS, and colon cancer.
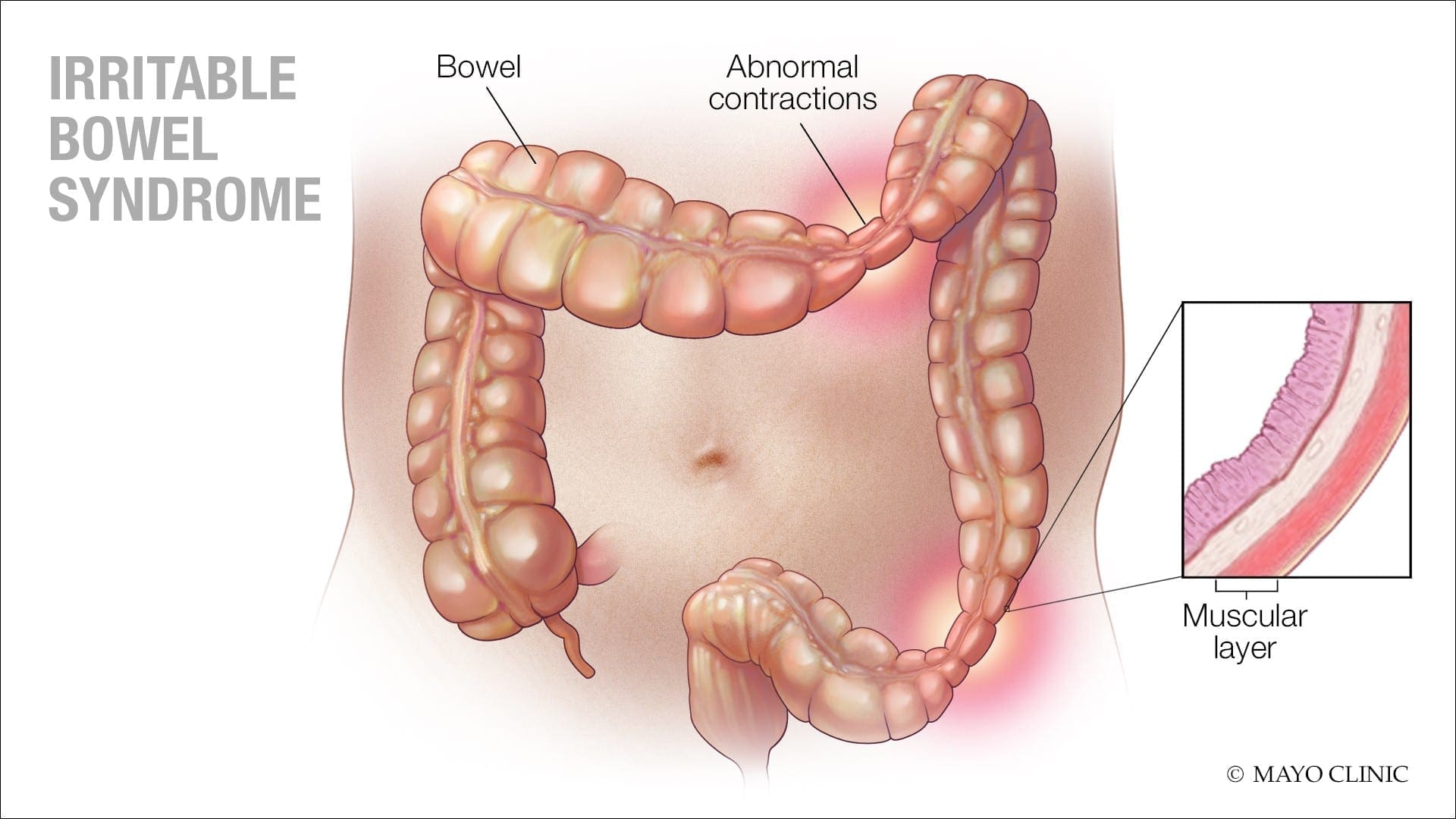
Irritable Bowel Syndrome
IBS (irritable bowel syndrome) is a long term gastrointestinal disorder. It can cause abdominal pain, bloating, mucus in the stool, irregular bowel habits, and can alternate diarrhea and constipation. IBS can cause persistent discomfort to individuals, but they can improve the symptoms over time as they learn to manage the condition.
Some of the symptoms caused by IBS are:
Changes in bowel habits
Abdominal pain and cramping that lessens after using the bathroom
A feeling that the bowels not fully emptied after using the bathroom
Excess gas
The passing of mucus from the rectum
The sudden urgent need to use the bathroom
Swelling or bloating from the abdomen.
Signs and symptoms of IBS can vary between individuals and can often resemble other diseases and conditions. IBS symptoms can often get worst after earing, and a flare-up may last about 2 to 4 days, then the symptoms may either improve or go away entirely, but IBS symptoms can affect different body parts.
These can include:
Frequent urination
Bad breath
Headaches
Joint or muscle pain
Persistent fatigue
Anxiety
Depression
Constipation
Constipation is one of the most common digestive problems that affects around 2.5 million individuals. It is a syndrome that is defined by bowel symptoms (painful or infrequent passage of stool, the hardness of stool, or a feeling of incomplete evacuation) that may occur either in isolation or secondary to another underlying disease like for example, Parkinson’s disease.
The cause of constipation is through the colon. The colon’s main job is to absorb water from leftover food as it passes through the digestive system and creates waste. When the waste is ready to be excreted out, the colon’s muscles propel the waste out through the rectum to eliminate from the body. If the debris remains in the colon for too long, though, it can be tough and challenging to excrete it out of the body.
Some factors can cause constipation; this can include:
Stress
Low-fiber diet
Lack of exercise
Certain medications
Particular diseases like a stroke, Parkinson’s disease, and diabetes
Problems with the colon or rectum
Hormonal issues
Everyone’s definition of a regular bowel movement may be different. Some people can go about three times a day, while others can go to relieve themselves about three times a week. Some of the symptoms of constipation included are:
Fewer than three bowel movements a week
Passing hard, dry stools
Straining or pain during bowel movements
Still feeling full after a bowel movement
Experiencing a rectal blockage
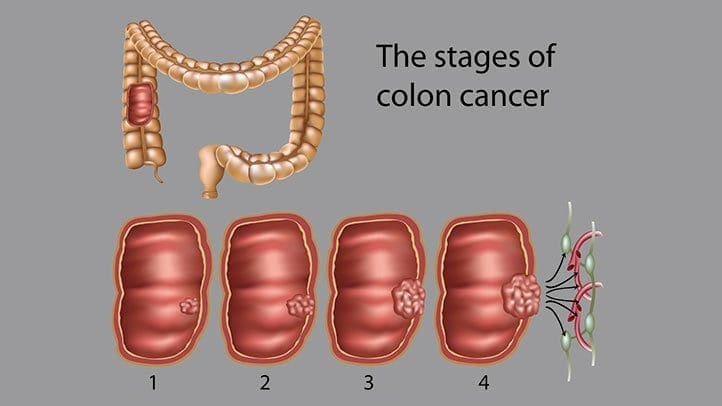
Colon Cancer
Colon cancer is the third most common type of cancer. When tumorous growths develop in the large intestine or the colon, it develops colon cancer in the GI tract. The colon, the one organ where the body draws out water and salt from solid wastes. The waste then moves through the rectum and excretes out of the body through the anus.
Even though colon cancer doesn’t cause any symptoms in the earliest stages, but it can become more noticeable as the disease progresses. Some of the sign and symptoms of colon cancer include:
Diarrhea or constipation
Changes in stool consistency
Loose, narrow stools
Blood in the stool
Abdominal pain
Weakness and fatigue
Iron deficiency
If colon cancer spreads to a new location the gastrointestinal system, it can cause additional problems in the new area.
Conclusion
Having gastrointestinal impairments can cause the body to develop chronic illnesses. There are ways to make sure that the digestive tract is functioning correctly. An individual can change their diets and lifestyle and can make sure that their gut is working properly. When there is a disruption in the GI tract like IBS, constipation, and colon cancer, it can lead to many health problems if the individual is not careful. If an individual prolongs the symptoms, then they will develop life-long issues for their body. Some products help support the intestinal tract and help strengthens the natural defenses and support the intestinal immune function.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Bharucha, Adil E, et al. �American Gastroenterological Association Technical Review on Constipation.� Gastroenterology, U.S. National Library of Medicine, Jan. 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3531555/.
Brazier, Yvette. �Irritable Bowel Syndrome (IBS): Symptoms, Diet, Causes, and Treatment.� Medical News Today, MediLexicon International, 18 Dec. 2017, www.medicalnewstoday.com/articles/37063.php.
Crosta, Peter. �Colon Cancer: Symptoms, Treatment, and Causes.� Medical News Today, MediLexicon International, 28 Aug. 2019, www.medicalnewstoday.com/articles/150496.php.
Sethi, Saurabh. �What You Should Know About Constipation.� Healthline, 23 Aug. 2019, www.healthline.com/health/constipation.
Whitfield, K Lynette, and Robert J Shulman. �Treatment Options for Functional Gastrointestinal Disorders: from Empiric to Complementary Approaches.� Pediatric Annals, U.S. National Library of Medicine, May 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC2830707/.
Do you feel that you must have sweets after meals? Do you get light-headed if you miss a meal? Or feel that craving for sweets during the day? Does your body feels shaky jittery or have tremors? If you are experiencing any of these situations, you may be experiencing LADA.
LADA
Autoimmune diabetes is a heterogeneous disease that can arise at any age. Anyone with adult-onset autoimmune diabetes who does not necessitate insulin therapy for at least six months after being diagnosed may have LADA (latent autoimmune diabetes of adulthood). LADA is a slowly progressing form of autoimmune diabetes, and it has been estimated that 20% of people are diagnosed with having non-obesity-related type 2 diabetes.
LADA occurs when the pancreas stops producing adequate insulin and slowly damages the insulin-producing cells in the pancreas, harming the body�s function. It is clear, however, that the frequency of autoimmune diabetes among adults can be underestimated, and clinical features such as age and severity of symptoms are of no help in identifying patients that have LADA since there is still more research being done to treat LADA. The body mass index and C peptide levels in the general population can increase with age, and these parameters are of limited use in identifying LADA patients.
Different Types of Diabetes
In a person, diabetes is a condition that impairs the body’s ability to process blood glucose, and roughly the estimated number of people over 18 years of age that are diagnosed and undiagnosed with diabetes is about 30.2 million. Without ongoing, careful management, diabetes can lead to a build-up of sugars in the blood, which can increase the risk of dangerous complications, including stroke and heart disease.
There are different kinds of diabetes, including LADA, that can occur, and managing the condition depends on the type of diabetes an individual has.
Type 1 Diabetes
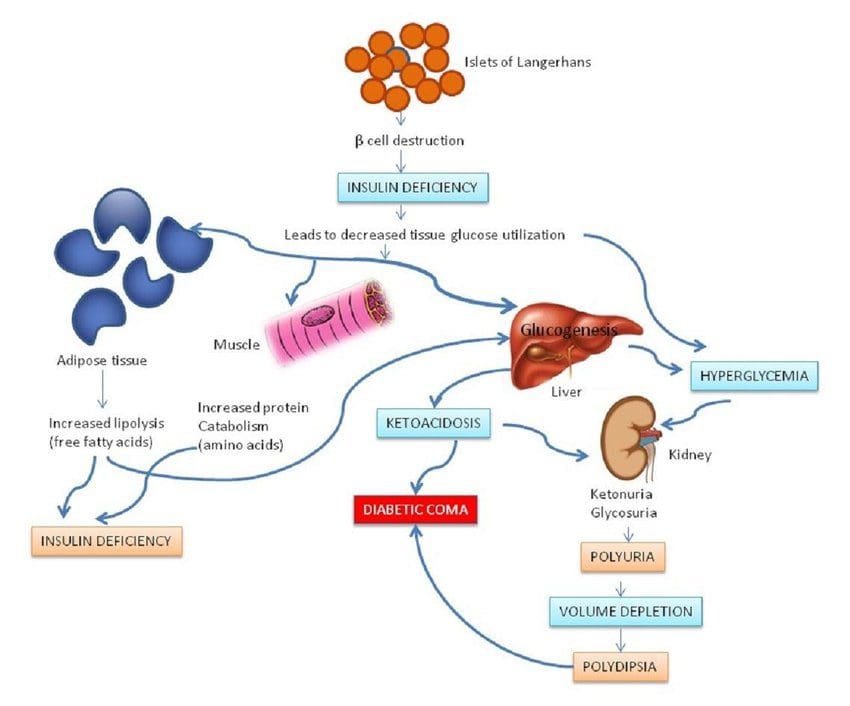
Type 1 diabetes is also known as juvenile diabetes, and the body does not produce enough insulin, and the blood glucose level remains high in the body. People with type 1 diabetes are insulin-dependent and must take artificial insulin daily to stay alive. The immune system attacks a cluster of cells known as islets in the pancreas that would typically produce insulin and stopping or slowing down the insulin production in the body.
When a person receives a diagnosis of type 1 diabetes from healthcare professionals, the islet cells are responsible for insulin secretion from the pancreas may continue to produce the insulin hormone for a while before ceasing. It can also lead to the production of LADA if it is not being monitored.
The physical effects of type 1 diabetes include:
Increased hunger and thirst
Frequent urination
Blurry vision
Tiredness and fatigue
Weight loss without an apparent trigger or causes.
Type 2 Diabetes
Type 2 diabetes is one of the most common forms of diabetes and can appear at any age, affecting over 30 million Americans. It happens when the blood sugar levels rise due to problems with the use or production of insulin.
Studies show that most people do not experience the symptoms in the early stages of type 2 diabetes, and they might have symptoms for many years. For those that do have type 2, diabetes may have acanthosis nigricans. Acanthosis nigricans is a skin condition that causes the skin to become thicker and darker. It often appears mostly on the neck, elbows, knees, knuckles, the folds around the neck and the groin.
Other early symptoms of type 2 diabetes that an individual may have included:
Frequent bladder, kidneys, or skin infections
Cuts that take longer to heal
Fatigue
Extreme hunger
Increased thirst
Urinary frequency
Blurred vision
Mixed Diabetes (Type 1.5)
Mixed diabetes or LADA is an autoimmune condition that shares the characteristics of both type 1 and type 2 diabetes in adults. It is diagnosed during adulthood and sets in the bloodstream gradually; however, unlike type 2, LADA is an autoimmune disease and is not reversible if the person changes their diet and lifestyle. �It can be triggered by the damage done to the pancreas from the antibodies against the insulin-producing cells.
If a person has LADA, their beta cells stop functioning much more quickly than type 2 diabetes. Researchers have found out that an estimated 10 percent of people who have diabetes will have LADA. It stated that the treatment for LADA patients is far less elucidated than the cases for type 1 and type 2 diabetes. Finding a treatment strategy for LADA can reduce the decline of beta-cell function, ensures adequate metabolic treatment so far.
Some of the symptoms that LADA patients may have include:
Frequent thirst
Increased urination, including at night
Unexplained weight loss
Blurred vision
Tingling nerves
If LADA is left untreated, it can lead to diabetic ketoacidosis, which is a condition where the body can not utilize sugar as fuel due to the absence of insulin and starts burning fat. It produces ketones, which are toxic to the body.
Type 3 Diabetes
Type 3 diabetes is known as brain diabetes and has an established linked to Alzheimer’s disease. This type of diabetes is triggered by a type of insulin resistance and an insulin-like growth factor dysfunction that occurs specifically in the brain, causing dementia.
Alzheimer�s disease has characteristics histopathological, molecular, and biochemical abnormalities in the brain’s cell structure. Since it has been linked with type 3 diabetes, characteristic features of type 3 diabetes include impairments in insulin actions and signaling that result in chronic hyperglycemia, irrespective of subtype, etiology, pathogenesis, or insulin availability.
Conclusion
Autoimmune diabetes can affect anyone at any age. It can damage the pancreas walls to stop producing insulin to the body, causing problems for an individual. LADA (latent autoimmune diabetes in adults) is an autoimmune disease that has the characteristics of type 1 and type 2 diabetes that are in adults. There is still more research being done to treat LADA, and there are products that can help support sugar metabolism and maintain blood sugar levels to a healthy range.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s declaration on our website to get full details on this historic moment.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Barhum, Lana. �Type 2 Diabetes: Symptoms, Early Signs, and Complications.� Medical News Today, MediLexicon International, 16 Apr. 2019, www.medicalnewstoday.com/articles/317462.php.
Castro, M. Regina. �Latent Autoimmune Diabetes in Adults (LADA): What Is It?� Mayo Clinic, Mayo Foundation for Medical Education and Research, 10 May 2019, www.mayoclinic.org/diseases-conditions/type-1-diabetes/expert-answers/lada-diabetes/faq-20057880.
de la Monte, Suzanne M, and Jack R Wands. �Alzheimer’s Disease Is Type 3 Diabetes-Evidence Reviewed.� Journal of Diabetes Science and Technology, Diabetes Technology Society, Nov. 2008, www.ncbi.nlm.nih.gov/pmc/articles/PMC2769828/.
Felman, Adam. �Type 1 Diabetes: Overview, Symptoms, and Treatment.� Medical News Today, MediLexicon International, 19 Nov. 2018, www.medicalnewstoday.com/articles/323729.php.
Hals, Ingrid K. �Treatment of Latent Autoimmune Diabetes in Adults: What Is Best?� Current Diabetes Reviews, U.S. National Library of Medicine, 2019, www.ncbi.nlm.nih.gov/pubmed/30009709.
Leonard, Jayne. �Acanthosis Nigricans: Causes, Symptoms, Treatment, and Pictures.� Medical News Today, MediLexicon International, 21 Dec. 2018, www.medicalnewstoday.com/articles/324062.php.
MSN, Rachel Nall RN. �Diabetes: Symptoms, Treatment, and Early Diagnosis.� Medical News Today, MediLexicon International, 8 Nov. 2018, www.medicalnewstoday.com/articles/323627.php.
Pozzilli, Paolo, and Silvia Pieralice. �Latent Autoimmune Diabetes in Adults: Current Status and New Horizons.� Endocrinology and Metabolism (Seoul, Korea), Korean Endocrine Society, June 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC6021307/.
Prelipcean, Maria S. �What You Need to Know About Type 1.5 Diabetes.� Healthline, 2 Nov. 2018, www.healthline.com/health/type-1-5-diabetes.
Watson, Kathryn. �Type 3 Diabetes and Alzheimer’s Disease: What You Need to Know.� Healthline, 16 Oct. 2019, www.healthline.com/health/type-3-diabetes.
Wint, Carmella, and Marijane Leonard. �What You Should Know About Diabetic Ketoacid.� Healthline, 4 Dec. 2018, www.healthline.com/health/type-2-diabetes/ketoacidosis.
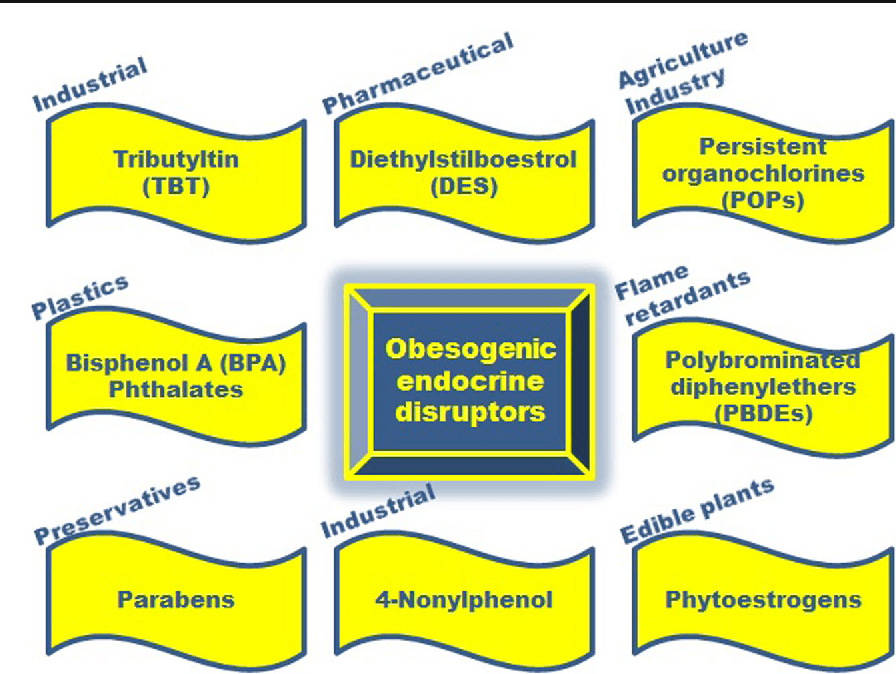
Endocrine disruptors are chemicals that may interfere with the body’s endocrine system and produce adverse developmental, reproductive, neurological, and immune effects in humans. It can be pesticides, plasticizers, antimicrobials, and flame retardants that can be EDCs. EDCs (endocrine-disrupting chemicals) can disrupt the hormonal balance and can result in developmental and reproductive abnormalities in the body.
There are four points about endocrine disruption:
Low dose matters
Wide range of health benefits
Persistence of biological effects
Ubiquitous exposure
EDC can cause significant risks to humans by targeting different organs and systems in the body. The interactions and the mechanisms of toxicity created by EDC and environmental factors can be concerning a person’s general health problems. Including endocrine disturbances in the body since many factors can cause endocrine disruptors, one of the disruptors in the food contaminated with PBDEs (polybrominated diphenyl esters) in fish meat and dairy.
Researchers also pointed out that once the contaminated foods eliminated from a person’s diet, then the endocrine disruptors decline, and the body began to heal properly. When a person eliminates the food that is causing discomfort to their bodies, they are more aware of reading the food labels to prevent discomfort anymore to the body systems.
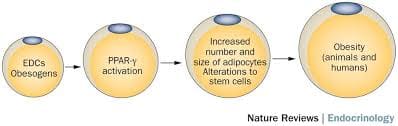
Obesogen
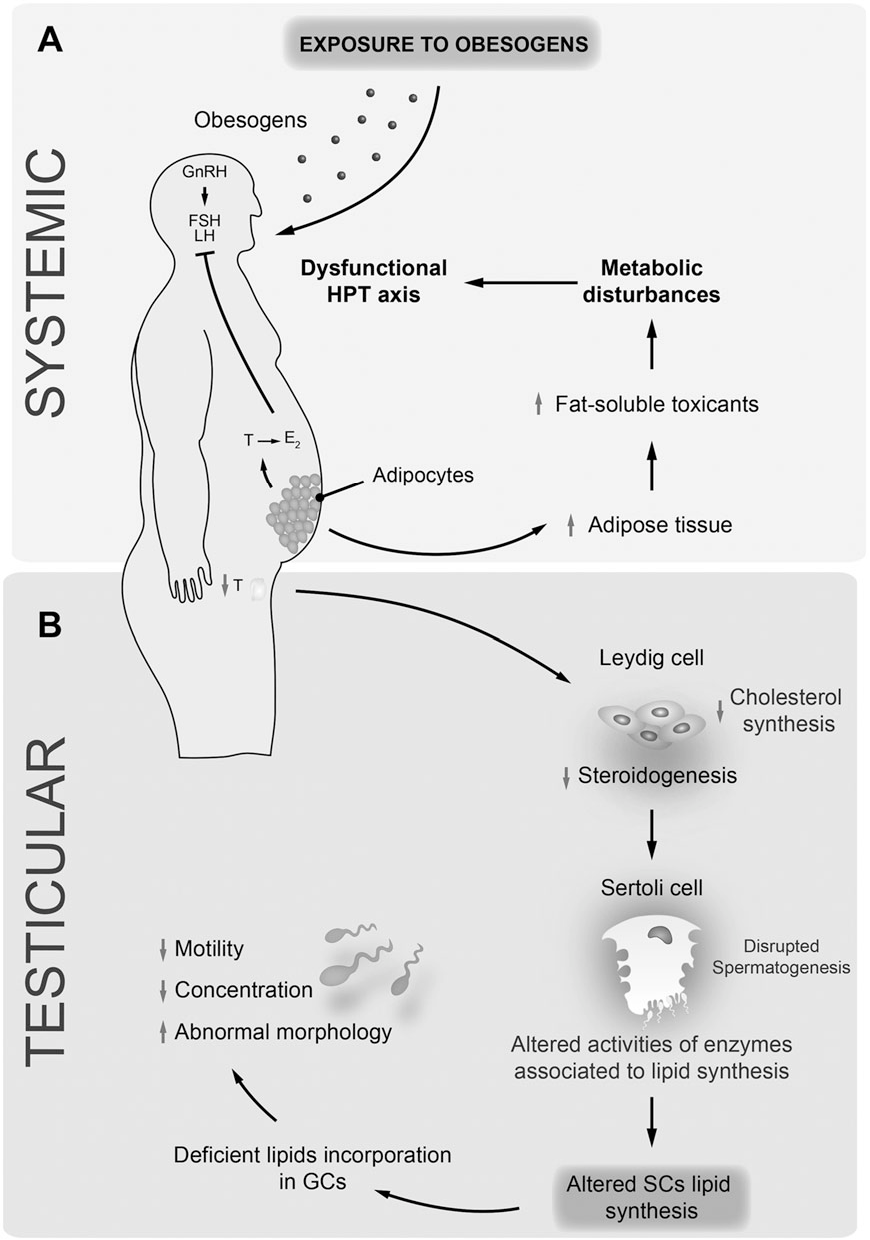
Obesogen is a subclass of endocrine-disrupting chemicals (EDC) that might predispose individuals to the development of obesity. Their structure is mainly lipophilic, and they can increase fat deposition. Since the fat cell’s primary role is to store and release energy, researchers have found that different obesogenic compounds may have different mechanisms of action.
Some of these actions can affect the number of fat cells that are producing, while others affect the size of the fat cells, and some obesogenic compounds can affect the hormones. These compounds will affect the appetite, satiety, food preferences, and energy metabolism when the endocrine system plays a fundamental role in the body to regulate the metabolism of fats, carbohydrates, and proteins. Any alternations in the body can result in an imbalance in the metabolism and causing endocrine disorders.
Studies even stated that exposure to obesogens could be found either before birth on utero or in the neonatal period. Obesogens can even cause a decrease in male fertility. When this disruption happens to the male body, environmental compounds can cause a predispose to weight gain, and obesogens can appoint as one of the contributors because of their actions as endocrine disruptors. Obesogens can even change the functioning of the male reproductive axis and testicular physiology. The metabolism in the male human body can be pivotal for spermatogenesis due to these changes.
Endocrine Disruptors and Obesity
Some endocrine disruptors that can affect the body can be through pharmaceutical drugs that can cause weight gain. A variety of prescription drugs can have an adverse effect that can result in weight gain since the chemicals found in prescription drugs have similar structures, and modes of action might have a role in obesity. Prescription medicine can stimulate the gut to consume more food, thus involving the body to gain weight.
Another endocrine disruptor is PAHs (polycyclic aromatic hydrocarbons). These are a family of environmental chemicals that occur in oil, coal, and tar deposits. They produce as by-products of fuel-burning like fossil fuel, biomass, cigarette smoke, and diesel exhaust. PAHs can either be manufactured to be used as medicines and pesticides or be released naturally from forest fires and volcanoes.
There are standard ways a person can be exposed to PAHs. One is through eating grilled, charred, or charcoal-broiled meats that a person eats. The other is through inhalation of smoke from cigarettes, vehicle exhaust, or emissions from fossil fuels that can irritate the eyes and breathing passageways in the body.
Coping with EDC Exposure
Even though obesity can adversely affect the body in a variety of health outcomes, there are ways to cope and minimize the exposure of EDC. Research shows that a person can minimize EDC exposure by consuming organic fruits, vegetables, and grain products insofar as possible. This includes an increasing number of fungicides routinely applied to fruits and vegetables that are being identified as obesogens and metabolic disruptors in the body.
Xenoestrogen vs. Phytoestrogen
When a person has an endocrine disorder, it might be due to the food they are consuming. Phytoestrogens are plant-derived compounds that are in a wide variety of food, mostly in soy. They are presented in numerous dietary supplements and widely marketed as a natural alternative to estrogen replacement therapy.
There is a health impact on phytoestrogen, and the plant-derived compound can either mimic, modulate, or disrupt the actions of endogenous estrogen. Xenoestrogen�are synthetically derived chemical agents from certain drugs, pesticides, and industrial by-products that mimic endogenous hormones or can interfere with endocrine disruptors. These chemical compounds can cause an effect on several developmental anomalies to humans. It can also interfere with the production and metabolism of ovarian estrogen in females.
Conclusion
Endocrine disruptors can interfere with the body’s endocrine system causing a health risk to an individual. EDC (endocrine-disrupting chemicals) can target many different organs and systems of the body by various factors that the human body is being exposed to. One of the EDC factors is obesogen, and it can cause a person to gain weight and be obese. Another factor is the exposure of PAHs (polycyclic aromatic hydrocarbons) through environmental factors like smoke inhalation or consuming charcoal-broiled meats. There are ways to cope with EDC exposure, and one is eating organic foods, especially fresh fruits and vegetables. Another is products that target the endocrine system and helps support the liver, intestines, body metabolism, and estrogen metabolism to ensure not only a healthy endocrine system but also a healthy body to function correctly.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott’s proclamation on our website to get full details on this historic event.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Cardoso, A M, et al. �Obesogens and Male Fertility.� Obesity Reviews : an Official Journal of the International Association for the Study of Obesity, U.S. National Library of Medicine, Jan. 2017, www.ncbi.nlm.nih.gov/pubmed/27776203.
Darbre, Philippa D. �Endocrine Disruptors and Obesity.� Current Obesity Reports, Springer US, Mar. 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5359373/.
Holtcamp, Wendee. �Obesogens: an Environmental Link to Obesity.� Environmental Health Perspectives, National Institute of Environmental Health Sciences, Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3279464/.
Janesick, Amanda S, and Bruce Blumberg. �Obesogens: an Emerging Threat to Public Health.� American Journal of Obstetrics and Gynecology, U.S. National Library of Medicine, May 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4851574/.
Janesick, Amanda S, and Bruce Blumberg. �Obesogens: an Emerging Threat to Public Health.� American Journal of Obstetrics and Gynecology, U.S. National Library of Medicine, May 2016, www.ncbi.nlm.nih.gov/pubmed/26829510.
L�r�nd, T, et al. �Hormonal Action of Plant Derived and Anthropogenic Non-Steroidal Estrogenic Compounds: Phytoestrogens and Xenoestrogens.� Current Medicinal Chemistry, U.S. National Library of Medicine, 2010, www.ncbi.nlm.nih.gov/pubmed/20738246.
Patisaul, Heather B, and Wendy Jefferson. �The Pros and Cons of Phytoestrogens.� Frontiers in Neuroendocrinology, U.S. National Library of Medicine, Oct. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC3074428/.
Singleton, David W, and Sohaib A Khan. �Xenoestrogen Exposure and Mechanisms of Endocrine Disruption.� Frontiers in Bioscience : a Journal and Virtual Library, U.S. National Library of Medicine, 1 Jan. 2003, www.ncbi.nlm.nih.gov/pubmed/12456297.
Unknown, Unknown. �Endocrine Disruptors.� National Institute of Environmental Health Sciences, U.S. Department of Health and Human Services, 2015, www.niehs.nih.gov/health/topics/agents/endocrine/index.cfm.
Unknown, Unknown. �Polycyclic Aromatic Hydrocarbons (PAHs): Your Environment, Your Health | National Library of Medicine.� U.S. National Library of Medicine, National Institutes of Health, 31 Apr. 2017, toxtown.nlm.nih.gov/chemicals-and-contaminants/polycyclic-aromatic-hydrocarbons-pahs.
Yang, Oneyeol, et al. �Endocrine-Disrupting Chemicals: Review of Toxicological Mechanisms Using Molecular Pathway Analysis.� Journal of Cancer Prevention, Korean Society of Cancer Prevention, 30 Mar. 2015, www.jcpjournal.org/journal/view.html?doi=10.15430%2FJCP.2015.20.1.12.
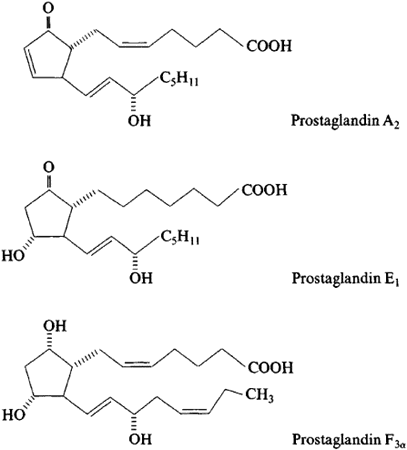
Prostaglandins are different than hormones. They are not secreted from a gland that can be carried through the bloodstream and work on specific areas around the body. Prostaglandins are made by a chemical reaction in the body that can be made in all the organs and are part of the body�s way of dealing with injuries and illnesses.
When any part of the body has been damaged, prostaglandins are made at the site of tissue damage or infection where they cause inflammation, pain and fever as part of the body�s healing process. When there is a high level of prostaglandins in the body due to the natural healing process from injuries and inflammation, it can contribute to several diseases from the unwanted inflammation.
Prostaglandins in the Omega fatty acids
In omega-6 fatty acids, DGLA (dihomo-gamma-linolenic acid) creates Prostaglandin E1(PG-1) as anti-inflammatory receptors in the body. In omega-3 fatty acids, they can create Prostaglandin E3 (PG-3) that are also anti-inflammatory receptors as well. PG-1 and PG-3 help prevent blood clotting in the body system.
When it comes to pro-inflammatory receptors, omega-6 fatty acids have these receptors as well. Pro-inflammatory receptors are created by arachidonic acid. Arachidonic acid creates Prostaglandin E2 (PG-2), which is responsible for inflammation, swelling and clotting as well.
There has to be a balance between PG-2 and PG-1,3 to provide a healthy function in the body and an ideal hormone signaling response. When one of the PGs are being disrupted by trans-fatty acids from food, it can cause health problems to a person.
Deficiencies in Prostaglandins
Trans fatty acids are a form of unsaturated fats that can be either natural or artificial. They are produced either by hydrogenation of unsaturated oils or by biohydrogenation in the stomach of ruminant animals. Numerous studies have been shown that consuming trans fatty acids continuously can increase the risk of cardiovascular diseases. This can also increase the ratio of LDL cholesterol to HDL cholesterol in the body. Trans fatty acids can block the activity of D6D (delta-6-desaturase), which is the first step in prostaglandin synthesis from essential fats in the diet.
The excess sugar consumption, insulin surges, inflammation, protein deficiencies hypothyroidism, and alcohol consumption will impair the activity of D6D and be a marker of accelerating aging to the human body. When a person has an increased consumption from fried foods and vegetable oils in an Western diet will shift the omega-6 pathway from PG-1 and into PG-2 production in the body. With the current American diet, people consume a high quantity of omega-6 fatty acids and low quantity of omega-3 fatty acids. This will cause a strong reaction of an inflammatory prostaglandin shift.
Since prostaglandins are caused by injuries and inflammation to heal the body, when an individual consumes a high omega-6 diet, it can cause an excessive amount of inflammation to the body and it can lead to chronic illnesses.
More Deficiencies in Prostaglandins
A deficiency in nutrients like nicotinic acid, pyridoxal 5� -phosphate, calcium, magnesium, zinc, and molybdenum is required for the desaturase and elongase enzymes in omega-6 and omega-3 fatty acids. Their deficiency can lead to improper production of prostaglandins. So EFAs from diets cause overconsumption of omega-6 and a lack of essential fatty acids in the body.
After that happens, then the EFAs can be synthesized into prostaglandins with desaturase and elongase enzymes. This will then cause nutrient deficiencies and metabolic factors can impair and downregulate those enzymes and causing the body to be prone to pro-inflammatory.
When that happens, prostaglandin formation will suddenly turn into abnormal ratios in the body causing problems, excessive inflammation in the endocrine glands and the body organs, and soon later on if it is not fixed, chronic illnesses will cause proper hormones to alter their components and either stop producing or create an abundance in the body.
Conclusion
Prostaglandins are a chemical reaction to the body that are different than hormones. They are caused when the body is injured and it causes inflammation so it can naturally heal itself. When there is an excessive amount of prostaglandins in the body it can lead to chronic inflammation and cause an abnormal shift in the body�s functional state. A factor that can affect the prostaglandins as well is the excessive consumption of omega-6 fatty acids. This consumption can cause inflammation and can make the body feel sluggish and not feeling great. There are products that can help the body, especially balancing the production of essential fatty acids and metabolizing the body for optimal health.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s bill on our website to get full details.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
F.Horrobin, David. �Loss of Delta-6-Desaturase Activity as a Key Factor in Aging.� Medical Hypotheses, Churchill Livingstone, 22 Mar. 2004, www.sciencedirect.com/science/article/abs/pii/0306987781900645.
Horrobin, D F. �Fatty Acid Metabolism in Health and Disease: the Role of Delta-6-Desaturase.� The American Journal of Clinical Nutrition, U.S. National Library of Medicine, May 1993, www.ncbi.nlm.nih.gov/pubmed/8386433.
Innes, Jacqueline K, and Philip C Calder. �Omega-6 Fatty Acids and Inflammation.� Prostaglandins, Leukotrienes, and Essential Fatty Acids, U.S. National Library of Medicine, May 2018, www.ncbi.nlm.nih.gov/pubmed/29610056.
Iqbal, Mohammad Perwaiz. �Trans Fatty Acids – A Risk Factor for Cardiovascular Disease.� Pakistan Journal of Medical Sciences, Professional Medical Publicaitons, Jan. 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC3955571/.
Leech, Joe. �What Are Trans Fats, and Are They Bad for You?� Healthline, 30 July 2019, www.healthline.com/nutrition/why-trans-fats-are-bad.
Ricciotti, Emanuela, and Garret A FitzGerald. �Prostaglandins and Inflammation.� Arteriosclerosis, Thrombosis, and Vascular Biology, U.S. National Library of Medicine, May 2011, www.ncbi.nlm.nih.gov/pmc/articles/PMC3081099/.
Tallima, Hatem, and Rashika El Ridi. �Arachidonic Acid: Physiological Roles and Potential Health Benefits – A Review.� Journal of Advanced Research, Elsevier, 24 Nov. 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC6052655/.
Unknown, Unknown. �Prostaglandins.� You and Your Hormones, Dec. 2016, www.yourhormones.info/hormones/prostaglandins/.
Wang, Xiaoping, et al. �Multiple Roles of Dihomo-?-Linolenic Acid against Proliferation Diseases.� Lipids in Health and Disease, BioMed Central, 14 Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3295719/.
Trouble concentrating, mood swings, headaches, and fatigue could be a common occurrence in one’s day to day life.� These symptoms are commonly brushed off as lack of sleep but did you know these symptoms are also side effects of hormone imbalance?�
Hormone imbalance is fairly common and can be tested for and treated. One of the most accurate tests to date that checks for hormone imbalances is the D.U.T.C.H test.�
What Is It?
D.U.T.C.H is a type of hormone testing that stands for Dried Urine Test for Comprehensive Hormones. Dried urine samples make it possible for scientists to see a whole day of hormones and quantify aspects that are distinct. Unlike obtaining information from a blood draw, urine contains different components that provide scientists with a new line of insight.
What Is The Goal?
When it comes to a hormone imbalance, the adrenal glands may have a large impact. The adrenals are two small glands that sit on top of the kidneys. These small glands are responsible for producing vital hormones such as sex hormones and cortisol. These hormones help the body respond to stress along with other functions.�
With the turn around time being around 10 business days, individuals can gain control and receive the insight they may have been missing. �Precision Analytical (the founders of D.U.T.C.H) employs the most innovative instruments to achieve the best outcomes for patients. The main purpose is to create an understanding of what is currently going on in the patient’s body and allows the treatment to become more specific and targeted to the needs of the individual.
There are different D.U.T.C.H tests that may be completed depending on the patient’s needs. The three main tests are
Dutch Complete– This is a comprehensive assessment of sex and adrenal hormones and their metabolites. This test measures progesterone, androgen, estrogen metabolites, cortisol, cortisone, cortisol metabolites, creatine, DHEA-S.�
Dutch Plus– This test uses 5 -6 saliva samples as well as 4 urine samples to provide the up and down pattern of cortisol and cortisone throughout the day. This test adds salivary cortisol measurements of the cortisol awakening response (CAR) to the dutch complete to bring another important piece of the HPA axis into focus
Dutch Test Cycle Mapping– This test maps the progesterone and estrogen pattern throughout the menstrual cycle. It provides the full picture of a woman’s cycle to answer important questions for patients with month-long symptoms, infertility, and PCOS. This test is targeted to measure 9 estrogens and progesterone that are taken throughout the cycle to characterize the follicular, ovulatory, and luteal phases.�
How Does This Operate?
Precision Analyical, Inc. has found a way to utilize scientists who have extensive experience and coupled them with the most advanced analytical methods and instruments. This permits them to achieve the best outcomes when it comes to the D.U.T.C.H test.
One of the reasons that many practicing offices have started to utilize D.U.T.C.H evaluations is because they have an extremely simple sample collection. Patients will collect dried urine samples within a span of 24 hours. The urine samples offer results that are excellent because the collections provide the span of a patients entire day of hormones.�
For the D.U.T.C.H test, the patient will collect 4-5 urine samples throughout a 24 hour time period. Upon opening the kit, the patient will be faced with a folder. This folder includes step by step instructions as well as a pocket. Inside the pocket, the patient will find a requisition form, an envelope, and a small clear plastic bag containing the collection paper.�
Each sample will be completed on a separate collection sheet that is labeled with the time. Once the patient opens this bag, they will be able to unfold the first sample paper. The patient will obtain the initial sample at approximately 5pm ( dinnertime). Once the samples are taken, they are to be left open to dry for 24 hours. The second sample is to be taken around 10 pm (bedtime). This third sample depends upon each individual, but in the event, the patient awakens to urinate during the night, a sample is to be gathered. The next sample ought to be collected within 10 minutes of rising. It’s very important that the patient does not lay in bed after waking and they amass this sample within the 10 minute time period that is allotted. Once the patient has collected their morning sample upon rising, they should set an alarm for two hours, since this is when the final sample will be collected. As soon as all the samples have been collected and set out open to dry for 24 hours, the patient can fold them back up and fill out the information on the back of the card ( i.e first name, last name, date of collection, time, and day of cycle for women) and place them inside the clear plastic bag.�
From here, the patient can place the plastic bag full of their samples along with the requestion form in the envelope provided. Next, place 8 stamps in the correct corner, and send it off to the lab!�
For the D.U.T.C.H Plus test, individuals will collect dried urine samples as well as saliva samples. This is best so researchers can utilize information from both collection samples to measure the cortisol and cortisone markers as well. For this test, it is completed in a 24 hour time window with 4 dried urine samples and 5 or 6 (depending on the individual) salvia samples. This test may sound more complicated, but it has a fairly easy schedule that makes it just as simple as the D.U.T.C.H complete. The kit will include labeled urine and salvia collection methods along with easy to read instructions.�
When opening this test, the patient will find an instruction book, a requisition form, 4 collection sheets for the urine (labeled with the time) and 6 labeled tubes for the saliva. For all the urine samples, fill out the backside of the card as prompted (last name, first name, date, and time). Saturate the filter paper or urinate into a clean cup and dip the filter paper for 5 seconds. Once this step is completed, leave the sample open to dry for 24 hours.�
For the saliva samples, take out the appropriate tube for the time it is to be collected. Just as done with the urine, fill out the allotted area requesting last name, first time, sample date and time. The saliva tubes have a blue cap that needs to be removed. After this cap is removed, a long cotton swab will be visible. Take out the cotton swab but leave the small tube in the long tube. The patient will then take the cotton swab and leave it in their mouth until it is fully saturated. Once this is done, place the cotton swab back in the tube as it was found and place the blue cap back on. The small tube should stay intact. There is no need to spit in the tubes.�
The first sample will be salvia and urine. These samples are to be collected immediately upon waking (no brushing of the teeth). The next two samples will be saliva. These are to be taken 30 minutes and 60 minutes after waking. After these are completed, the patient may brush their teeth. The fourth sample will be collected 2-3 hours after waking and is urine only. The fifth and sixth samples will be urine and salvia. The patient will collect these around 4-5 pm (dinnertime) and again anywhere from 10pm-midnight (bedtime). Place all saliva tubes in the freezer until they are ready to be shipped.�
The seventh saliva sample is optional. This will be collected at the time the patient wakes throughout the night if they do so.�
After all the samples have been collected and urine has dried for 24 hours, fold up the urine samples and place them back in the small plastic bag in which they came. Then, take the frozen saliva samples out of the freezer and place them in the plastic bag they arrived in. From here, take the urine samples, the frozen saliva, and the requestion form and place them all back in the kit box. Place the kit box in the return envelope provided and return using the provided carrier.�
The D.U.T.C.H cycle mapping test is the most extensive test provided, with 25 urine samples needed. Due to the fact that this test is for cycle mapping, the collection time frame will be one entire cycle. To start, the patient will need to identify the type of cycle they have ( less than 24 days (normal) long (34 days or more) or no cycle). When the patient opens this kit, they will see an instruction book, 25 urine collection cards, a requestion form, a clear bag, and an envelope.
Day one of the patient’s cycle is the first day of full menstrual flow. The collections for this test will begin on the seventh day and the last four samples will be collected on the fourth day of the patient’s next menstrual cycle. Inside the instruction book, the patient will find an easy to use collection schedule to keep track of their samples.
The ideal time to collect samples throughout this test is upon waking. This will give the lab the most concentrated urine, making the results more conclusive. The patient will collect their sample every morning for day 7 through day 36. Once collected, the patient will leave the urine sample out to dry for 24 hours before putting it in the clear bag provided. It is important for the patient to write the date of the sample on the collection schedule included in the kit.�
The final four samples (22-25) are all to be collected on the same day. Sample 22 should be taken within 10 minutes of waking. Sample 23 is to be taken two hours after waking. Sample 24 should be collected at dinnertime and the patient should not have any fluids two hours before this sample. The final sample should be collected at the patient’s bedtime (approximately 10pm).�
Once the patient has collected all of the samples and let them dry for 24 hours, they are to be placed in the clear plastic bag that was provided in the kit. Next, the patient is to place the clear bag full of samples, the completely filled out collection schedule, and the requisition form in the envelope provided in the kit. Finally, place 8 stamps on the indicated corner and send it off to the lab!�
When sent to the lab as you can see above, these urine samples will be dry. Studies show that dried urine samples will give an accurate representation of the hormone and are stable for weeks. From here, the outcomes are gone over on a team call that includes the patient’s physician and clinicians at Precision Analytical. This helps to ensure that the treatment protocol is created specifically to fit the patients needs.��
Testing is now able to be done by using top of the line integrative techniques. There are numerous reasons and advantages for an individual to complete a hormone evaluation. These tests have the capability to help a patient understand their cycle, testosterone levels, estrogen levels, why they are tired upon waking, throughout there day, and much more.
Hormone imbalances can affect anyone. People tend to associate hormone imbalance with those who are aging, but in reality, it can affect anyone of any gender or age! It might seem like a hassle at first to compelete these tests, but in reality, they are very simple and provide a great deal of information! The symptoms are common and should be discussed with a healthcare practitioner. October is Chiropractor Health Month and our office can help if you are an individual who has these symptoms. Our office implements the D.U.T.C.H test, which allows us a hassle free and easy way to let us help you get back to feeling how you used to. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
All fats, including saturated fatty acids, have very important roles in the body. The most important fats are the ones that the body can�t make and must be coming from the foods that a person eats. �Essential fatty acids are lipids that are involved in various biological processes and produce many compounds when they are metabolized in the body. The two primary EFAs (essential fatty acids) are linoleic acid (Omega-6) and alpha-linolenic acid (Omega-3). These two omegas are essential for the body since they are consumed from dietary sources because the body does not have the ability to synthesize them and EFAs are synthesized into prostaglandins, which are necessary for proper hormone signaling in the body.
Omega-6
Omega-6 fatty acids or linoleic acid are polyunsaturated fatty acids that are primarily used for energy and can be converted into longer omega-6 fats called ARA (arachidonic acid). ARA are used to produce eicosanoids, but they are prone to be more pro-inflammatory. Studies have shown that pro-inflammatory eicosanoids are important chemicals in the immune systems, however, when there are too many to produce, they can increase inflammation and inflammatory diseases in the body.
Researchers state that even though omega-6 fats are essential for a healthy body, the modern Western diet is making individuals consume more omega-6 fatty acids than the recommended amount. In a regular healthy diet, the ratio of omega-6 to omega-3s is 4:1 or less. In a Western diet however, the ratio is between 10:1 and 50:1.
Even though, an individual should consume the recommended amount of omega-6 fatty acids, research has shown that omega-6 fatty acids can lower the risk of cardiovascular diseases and treat symptoms that cause chronic diseases. In certain oils that contains omega-6 fatty acids, GLA (gamma-linolenic acid), which is an anti-inflammatory component and when consumed it converts to DGLA (dihomo-gamma-linolenic acids), which has anti-inflammatory and anti-proliferative properties against cancer.
A study has shown that when an individual takes a high dose of GLA in their diet, it can significantly reduce a number of symptoms caused by rheumatoid arthritis, and another study found that taking GLA supplements with a breast cancer drug is more effective in lowering breast cancer.
Omega-3
Just like omega-6 fatty acids, omega-3 fatty acids are polyunsaturated fats that play important roles in providing a number of health benefits for a functional body. Omega-3 fatty acids contain three important compounds that are found in foods, they are ALA (alpha-linolenic acid); which converts into energy for the body, DHA (docosahexaenoic acid); which is the key component for a functional brain and retina, and lastly, EPA (eicosapentaenoic acid); which has cardiovascular benefits including lowering serum triglyceride and non-HDL-C (non-high-density lipoprotein cholesterol) in the body.
When it comes to those three important components in omega-3s, ALA is mainly found in plants, while DHA and EPA are found in mostly animal products and algae. What makes these three components work well in the omega-3 supplements is that they are a crucial part of the human cell membrane and improve heart health, support mental health, decrease liver fats and fight inflammation.
With omega-3 fatty acids, lots of people don�t consume it as much as omega-6, due to not eating a lot of fatty fish as often and consuming omega-6 through fried food being cooked in refined vegetable oils. To balance a healthy diet, individuals can take an omega-3 supplement to balance out the omega-6 consumption to make sure the body is receiving these fatty health benefits.
Prostaglandins
Prostaglandins are a component of this regulatory system, they affect multiple hormone synthesis and secretion pathways in the hypothalamus-pituitary axis. They are a group of endogenously occurring acidic lipids that appear to play a role in the reproductive physiology.
Since prostaglandins are bioactive lipids, they exert an autocrine or paracrine function by binding to specific GPCRs (G-protein-coupled receptors) to activate intracellular signaling and gene transcription. As key regulators of reproductive processes, prostaglandins has many functions like having a role in the hypothalamic and pituitary control of gonadotropin secretion, ovulation, in luteinization and in the corpus luteum regression.
Prostaglandins also play a key role in the inflammatory response in the body. Their biosynthesis is significantly increased in inflamed tissues and can contribute to the development of the cardinal signs of acute inflammation in the body.
Researchers stated that prostaglandins have a plethora of actions in the central nervous system that can affect the progress of inflammation in the body differently, however, further studies are being tested to inhibit the role of these lipid mediators.
Conclusion
All fats play a very important role in the body. Essential fatty acids produce many compounds in the body when they are being metabolized in the body. Since the body can not produce essential fatty acids, they have to be consumed through food. The two important essential fatty acids are omega-6 and omega-3. These two fatty supplements help the body gain the nutrients the body needs to synthesize. Prostaglandins are also a key role in the body since they affect the pathways in the hypothalamus-pituitary axis and plays the role of regulating the reproductive physiology. Some products are formulated to target the immune support by creating micronized structure to increase the surface-to-volume ratio of particles to be more available to enzymatic actions.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this declaration.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Bardin, T P. �The Role of Prostaglandins in Reproductive Physiology.� The Ohio State Medical Journal, U.S. National Library of Medicine, Oct. 1970, www.ncbi.nlm.nih.gov/pubmed/4918753.
Behrman, H R. �Prostaglandins in Hypothalamo-Pituitary and Ovarian Function.� Annual Review of Physiology, U.S. National Library of Medicine, 1979, www.ncbi.nlm.nih.gov/pubmed/373605.
Brinton, Eliot A, and R Preston Mason. �Prescription Omega-3 Fatty Acid Products Containing Highly Purified Eicosapentaenoic Acid (EPA).� Lipids in Health and Disease, BioMed Central, 31 Jan. 2017, www.ncbi.nlm.nih.gov/pubmed/28137294.
Calder, Philip C. �n-3 Polyunsaturated Fatty Acids, Inflammation, and Inflammatory Diseases.� The American Journal of Clinical Nutrition, U.S. National Library of Medicine, June 2006, www.ncbi.nlm.nih.gov/pubmed/16841861.
Di Pasquale, Mauro G. �The Essentials of Essential Fatty Acids.� Journal of Dietary Supplements, U.S. National Library of Medicine, 2009, www.ncbi.nlm.nih.gov/pubmed/22435414.
Dinan, Timothy, et al. �Investigating the Inflammatory Phenotype of Major Depression: Focus on Cytokines and Polyunsaturated Fatty Acids.� Journal of Psychiatric Research, U.S. National Library of Medicine, Jan. 2009, www.ncbi.nlm.nih.gov/pubmed/18640689.
Gibson, Robert A, et al. �Conversion of Linoleic Acid and Alpha-Linolenic Acid to Long-Chain Polyunsaturated Fatty Acids (LCPUFAs), with a Focus on Pregnancy, Lactation and the First 2 Years of Life.� Maternal & Child Nutrition, U.S. National Library of Medicine, Apr. 2011, www.ncbi.nlm.nih.gov/pubmed/21366864.
Guesnet, Philippe, and Jean-Marc Alessandri. �Docosahexaenoic Acid (DHA) and the Developing Central Nervous System (CNS) – Implications for Dietary Recommendations.� Biochimie, U.S. National Library of Medicine, Jan. 2011, www.ncbi.nlm.nih.gov/pubmed/20478353.
Gunnars, Kris. �What Are Omega-3 Fatty Acids? Explained in Simple Terms.� Healthline, 23 May 2019, www.healthline.com/nutrition/what-are-omega-3-fatty-acids.
Innes, Jacqueline K, and Philip C Calder. �Omega-6 Fatty Acids and Inflammation.� Prostaglandins, Leukotrienes, and Essential Fatty Acids, U.S. National Library of Medicine, May 2018, www.ncbi.nlm.nih.gov/pubmed/29610056.
Jabbour, H N, and K J Sales. �Prostaglandin Receptor Signalling and Function in Human Endometrial Pathology.� Trends in Endocrinology and Metabolism: TEM, U.S. National Library of Medicine, Oct. 2004, www.ncbi.nlm.nih.gov/pubmed/15380812.
Kapoor, Rakesh, and Yung-Sheng Huang. �Gamma Linolenic Acid: an Antiinflammatory Omega-6 Fatty Acid.� Current Pharmaceutical Biotechnology, U.S. National Library of Medicine, Dec. 2006, www.ncbi.nlm.nih.gov/pubmed/17168669.
Kenny, F S, et al. �Gamma Linolenic Acid with Tamoxifen as Primary Therapy in Breast Cancer.� International Journal of Cancer, U.S. National Library of Medicine, 1 Mar. 2000, www.ncbi.nlm.nih.gov/pubmed/10699943.
Khanapure, Subhash P, et al. �Eicosanoids in Inflammation: Biosynthesis, Pharmacology, and Therapeutic Frontiers.� Current Topics in Medicinal Chemistry, U.S. National Library of Medicine, 2007, www.ncbi.nlm.nih.gov/pubmed/17305573.
Kim, Kyu-Bong, et al. �?-Linolenic Acid: Nutraceutical, Pharmacological and Toxicological Evaluation.� Food and Chemical Toxicology : an International Journal Published for the British Industrial Biological Research Association, U.S. National Library of Medicine, Aug. 2014, www.ncbi.nlm.nih.gov/pubmed/24859185.
M.Shewchuk, Brian. �Prostaglandins and n-3 Polyunsaturated Fatty Acids in the Regulation of the Hypothalamic�Pituitary Axis.� Prostaglandins, Leukotrienes and Essential Fatty Acids, Churchill Livingstone, 28 Sept. 2014, www.sciencedirect.com/science/article/abs/pii/S0952327814001495.
Parker, Helen M, et al. �Omega-3 Supplementation and Non-Alcoholic Fatty Liver Disease: a Systematic Review and Meta-Analysis.� Journal of Hepatology, Centre for Reviews and Dissemination (UK), Apr. 2012, www.ncbi.nlm.nih.gov/pubmed/22023985.
Petersen, Martin, et al. �Effect of Fish Oil versus Corn Oil Supplementation on LDL and HDL Subclasses in Type 2 Diabetic Patients.� Diabetes Care, U.S. National Library of Medicine, Oct. 2002, www.ncbi.nlm.nih.gov/pubmed/12351465.
Ph.D., Catharine Paddock. �Could Omega-6 Fatty Acids Help Us Live Longer?� Medical News Today, MediLexicon International, 20 Mar. 2018, www.medicalnewstoday.com/articles/321266.php.
Simopoulos, Artemis P. �The Importance of the Omega-6/Omega-3 Fatty Acid Ratio in Cardiovascular Disease and Other Chronic Diseases.� Experimental Biology and Medicine (Maywood, N.J.), U.S. National Library of Medicine, June 2008, www.ncbi.nlm.nih.gov/pubmed/18408140.
Wang, Xiaoping, et al. �Multiple Roles of Dihomo-?-Linolenic Acid against Proliferation Diseases.� Lipids in Health and Disease, BioMed Central, 14 Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3295719/.
Weylandt, Karsten H, et al. �Omega-3 Polyunsaturated Fatty Acids: The Way Forward in Times of Mixed Evidence.� BioMed Research International, Hindawi Publishing Corporation, 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4537707/.
Zurier, R B, et al. �Gamma-Linolenic Acid Treatment of Rheumatoid Arthritis. A Randomized, Placebo-Controlled Trial.� Arthritis and Rheumatism, U.S. National Library of Medicine, Nov. 1996, www.ncbi.nlm.nih.gov/pubmed/8912502.
The body secretes and circulates 50 different hormones to different organs in the body. Hormones are the chemical substances that coordinate the activities of living organism growth. They are secreted through the endocrine glands and travel through the bloodstream to different organs in the body to function properly. When there is an excessive quantity or an reduced quantity of hormones being produced, it can cause the body to malfunction and develop chronic illnesses.
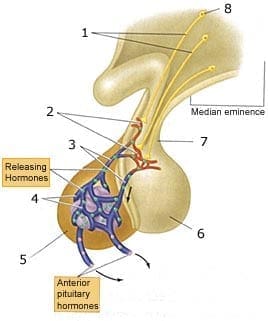
The Pituitary Gland Functions
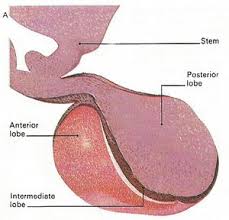
In neuroendocrinology, an endocrine gland can�t make a hormone without activation from a pituitary-stimulating hormone. The pituitary-stimulating hormone helps regulate hormones by secreting them to the endocrine glands. The pituitary gland is known as the �master gland� since it controls the activity of the other endocrine glands and it consists of 3 parts known as the anterior, intermediate and posterior lobes.
Anterior Lobe
The anterior pituitary gland is located in the sella turcica and is controlled by the hypothalamus in the brain. It secretes a quantity of peptides and glycoprotein hormones that help regulate the growth, metabolism, reproduction and stress response. The anterior pituitary gland produces 6 hormones that circulate to their respective targets in the body.
ACTH (Adrenocorticotropic hormone): This hormone is a tropic hormone as it regulates cortisol and androgen production to the adrenal cortex. Cortisol or stress hormones stimulates the release of ACTH, while the adrenal cortex secretes glucocorticoids to the body�s metabolism.
GH (Growth hormone): This hormone helps regulate the body�s growth, metabolism, and composition. GH is secreted by the somatotroph cells located primarily in the lateral wings of the anterior lobe. GH can also secrete in al pulsatile fashion and can have a maximal release during a circadian rhythm at night.
TSH (Thyroid stimulating hormone): This hormone is involved by coordinating the signal regulation of the hypothalamus, the pituitary, and the thyroid. It requires the oxidation of dietary iodine, since iodine is absorbed through the small intestine and transported to the thyroid. After the iodine is transported it can be concentrated, oxidized and then incorporated into thyroglobulin to be formed to T4 and T3 later on.
LH (Luteinizing hormone): This hormone is highly important to both men and women, since it affects the sex organs and plays a role in puberty, menstruation and fertility. For women, it creates progesterone, which help regulate menstruation and supports pregnancy in the female body. For men, it creates testosterone, which helps regulates fertility, muscle mass, fat distribution, and red blood production in the male body.
FSH (Follicle stimulating hormone): This hormone plays an important part in the reproductive system and is responsible for ovarian follicles. For females, FSH helps produce estrogen, which is a group of sex hormones that help promote the development and maintenance of female characteristics in the human body, For males, FSH helps produce spermatogenesis and regulates sperm function in the male body.
Prolactin: This is a protein hormone in the anterior lobe. It has the ability to promote lactation to nursing mothers. It synthesizes within the pituitary gland, the central nervous system, the immune system, and the uterus.
Intermediate lobe
The intermediate lobe is composed of a homogeneous population of the endocrine cells, the melanotrophs and secretes several bioactive peptides. It contains very few blood vessels and can be virtually avascular. The melanotrophs are richly supplied by nerve fibers that originate from the hypothalamus.
Melanocyte-stimulating hormone: This hormone has many functions in a diverse physiological role. It affects skin pigmentation and studies have shown that it has antiapoptotic and anti-inflammatory effects that help decrease in nephrotoxin exposure to the body.
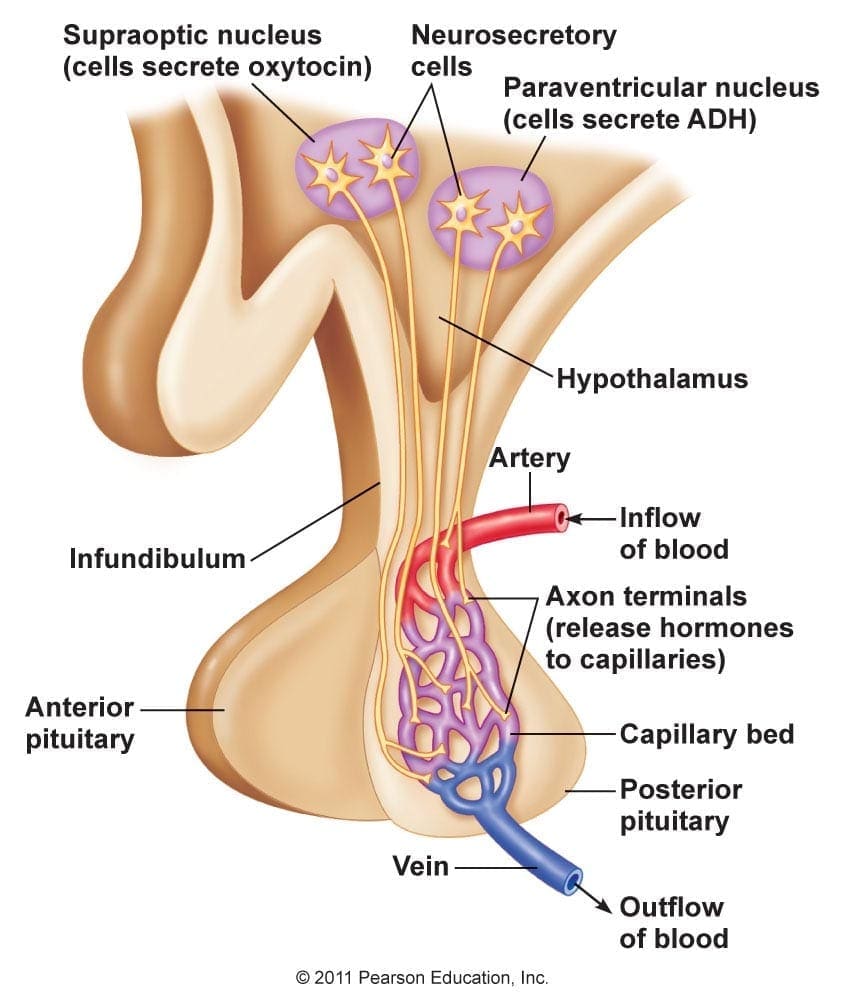
Posterior lobe
The posterior lobe is similar to the anterior lobe since they both control endocrine function and the body�s hormonal response to the environment. The hypothalamus receives neural signals from the brain and secretes polypeptide and neuropeptide hormones for storage in the posterior lobe until they are ready to be released. The hormones in the posterior lobe are in charge of regulating water retention and inducing uterine contractions.
ADH (Antidiuretic hormone): Also known as vasopressin, this hormone is a nonapeptide that is synthesized in the hypothalamus. It plays a bunch of important roles in controlling the body�s osmotic balance, regulates blood pressure, and makes sure that the kidneys are working. ADH is mainly responsible for tonicity homeostasis as they act primarily in kidneys to increase water reabsorption.
Oxytocin: Also known as the �love hormone�, oxytocin is also a neurotransmitter that is involved in childbirth and breast-feeding. It has benefits as a treatment for a number of conditions like depression, anxiety and intestinal problems and is produced in the hypothalamus. Studies show that females have a higher level of oxytocin than males, especially to nursing mothers with their babies.
Free-fraction Hormones
When an endocrine gland synthesizes a hormone, it is released into circulation and bound to as a protein. Hormones attach themselves to proteins but they can�t bind to hormone receptors. So what a hormone needs to do is to lose its binding protein to become a �free-fraction� hormone. Studies have stated that a fraction of a hormone that is free is called in vitro and it is equivalent to the fraction of a hormone that is free and available to be transported into tissues are called in vivo. Free-fraction hormones make up less than 1% of all circulating hormones since they don�t impact the hypothalamus-pituitary feedback loop.
Hormone Metabolites
Hormones are metabolized by hepatic and microbiome biotransformation pathways into various hormone metabolites. Hormone metabolites have their own impact on cell receptors, studies have shown that this impact is not fully understood yet but hormone metabolites are not a reflection of direct endocrine gland production but it can be metabolized in the liver as well. Hormone metabolites can bind to hormone receptors or can be eliminated by renal or fecal clearance pathways.
Conclusion
All in all, the body secretes and circulates 50 different hormones to different organs in the body. These hormones are chemically produced in the body and keep an eye on what each of the different organs is doing. It is important that the hormone receptors are functioning properly so that an individual is feeling good both inside and out. If there is a hormonal imbalance in the body, it can cause dysfunction and chronic illnesses to a person.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this declaration.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Allen, Mary J. �Physiology, Adrenocorticotropic Hormone (ACTH).� StatPearls [Internet]., U.S. National Library of Medicine, 3 Mar. 2019, www.ncbi.nlm.nih.gov/books/NBK500031/.
Cuzzo, Brian. �Vasopressin (Antidiuretic Hormone, ADH).� StatPearls [Internet]., U.S. National Library of Medicine, 2 Feb. 2019, www.ncbi.nlm.nih.gov/books/NBK526069/.
Ellis, Mary Ellen, and Rachel Nall. �Luteinizing Hormone (LH) Test: What It Is and Why It’s Important.� Healthline, 29 Aug. 2017, www.healthline.com/health/lh-blood-test.
Ellis, Ronald E, and Gillian M Stanfield. �The Regulation of Spermatogenesis and Sperm Function in Nematodes.� Seminars in Cell & Developmental Biology, U.S. National Library of Medicine, May 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4082717/.
Freeman, M E, et al. �Prolactin: Structure, Function, and Regulation of Secretion.� Physiological Reviews, U.S. National Library of Medicine, Oct. 2000, www.ncbi.nlm.nih.gov/pubmed/11015620.
Genes, S G. �Role of the Liver in Hormone Metabolism and in the Regulation of Their Content in the Blood.� Arkhiv Patologii, U.S. National Library of Medicine, 1977, www.ncbi.nlm.nih.gov/pubmed/334126.
Goyal, Shikha. �List of Important Hormones and Their Functions.� Jagranjosh.com, 12 Mar. 2019, www.jagranjosh.com/general-knowledge/list-of-important-hormones-and-their-functions-1516176713-1.
Gunawardane, Kavinga. �Normal Physiology of Growth Hormone in Adults.� Endotext [Internet]., U.S. National Library of Medicine, 12 Nov. 2015, www.ncbi.nlm.nih.gov/books/NBK279056/.
Hadley, M E, et al. �Biological Actions of Melanocyte-Stimulating Hormone.� Ciba Foundation Symposium, U.S. National Library of Medicine, 1981, www.ncbi.nlm.nih.gov/pubmed/6268380.
Lamacz, M, et al. �The Intermediate Lobe of the Pituitary, Model of Neuroendocrine Communication.� Archives Internationales De Physiologie, De Biochimie Et De Biophysique, U.S. National Library of Medicine, June 1991, www.ncbi.nlm.nih.gov/pubmed/1717055.
Lee, Heon-Jin, et al. �Oxytocin: the Great Facilitator of Life.� Progress in Neurobiology, U.S. National Library of Medicine, June 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC2689929/.
M., William. �Transport of Protein-Bound Hormones into Tissues in Vivo *.� OUP Academic, Oxford University Press, 1 Jan. 1981, academic.oup.com/edrv/article-abstract/2/1/103/2548700?redirectedFrom=fulltext.
MacGill, Markus. �Oxytocin: The Love Hormone?� Medical News Today, MediLexicon International, 4 Sept. 2017, www.medicalnewstoday.com/articles/275795.php.
MacGill, Markus. �Testosterone: Functions, Deficiencies, and Supplements.� Medical News Today, MediLexicon International, 6 Feb. 2019, www.medicalnewstoday.com/articles/276013.php.
Nichols, Hannah. �Estrogen: Functions, Uses, and Imbalances.� Medical News Today, MediLexicon International, 2 Jan. 2018, www.medicalnewstoday.com/articles/277177.php.
Patel, Hiran. �Physiology, Posterior Pituitary.� StatPearls [Internet]., U.S. National Library of Medicine, 27 Oct. 2018, www.ncbi.nlm.nih.gov/books/NBK526130/.
Rawindraraj, Antony D. �Physiology, Anterior Pituitary.� StatPearls [Internet]., U.S. National Library of Medicine, 25 Apr. 2019, www.ncbi.nlm.nih.gov/books/NBK499898/.
Rousset, Bernard. �Chapter 2 Thyroid Hormone Synthesis And Secretion.� Endotext [Internet]., U.S. National Library of Medicine, 2 Sept. 2015, www.ncbi.nlm.nih.gov/books/NBK285550/.
Seladi-Schulman, Jill. �Everything You Need to Know About Progesterone.� Healthline, 29 Apr. 2019, www.healthline.com/health/progesterone-function.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine