Stomach pain, burning, or aching 1-4 hours after eating?
If you are experiencing any of these situations, then you might be experiencing low glycine levels in your body.
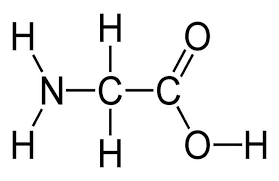
Glycine
Glycine is a vital amino acid that is beneficial to the body. It helps support the gastrointestinal system, the neurological system, the musculoskeletal system, and the body�s metabolism from harmful factors that can cause the human body to malfunction. Glycine is even a neurotransmitter and can help increase glutathione in the brain by providing anti-inflammatory effects. Glycine provides a sweet taste when it is consumed in the body. Even though glycine has a crucial role in the human body, the amino acid has received little to no attention until recently.
The fantastic thing about glycine is that it is a “non-essential” amino acid. What this means is that the body can make glycine by itself and distribute it to the necessary systems that need glycine. This is different from the “essential” amino acids since some nutrients and vitamins must come from the food diet themselves. When there is a mild deficiency of glycine, it is not harmful to the body; however, when there is a severe shortage of glycine, it can lead to immune response failure, slow body growth, and abnormal nutrient metabolism.
Glycine for The Brain
Since glycine is a neurotransmitter for the brain, it composes both excitatory and inhibitory capacities. For the excitatory capacity function, glycine serves as the antagonist for NMDA receptors for the brain. For inhibitory capacities, glycine helps increase the neurotransmitter serotonin. Studies show that serotonin is the ancestor of melatonin. When the levels are increased due to glycine supplements, the beneficial factors it causes can help reduce insomnia and provide better sleep quality.
Glycine on Sleep
Despite being a massive impact on serotonin, glycine has been known to be used as a therapeutic option for individuals to improve their sleep quality as a novel and safe approach.� Studies show that glycine can increase the blood flow to extremities by reducing the body�s core temperature, which is an important signal to initiate sleep. When this happens, glycine can increase a person�s time when they are in REM sleep, providing the person to have a good night’s sleep. Further research shows that glycine can inhibit the stimulatory orexin neurons that are responsible for arousal and energy homeostasis, which is critical and can induce non-REM sleep or even night waking.
Glycine�s Cognitive Effects
There are many beneficial cognitive effects that glycine has to offer. Research shows that the beneficial effect of glycine can help improve episodic memory in young and middle-aged adults. This can be beneficial for patients who have schizophrenia, Parkinson’s disease, and Huntington’s disease. Additional research also shows that patients who have Alzheimer’s disease use glycine as energy production for their brains.
Glycine Osteoprotective Effects
There is even more information on glycine supplementation, providing estrogen-like osteoprotective effects for menopausal women. The research shows that glycine helps decreased weight gain and providing an increase in vaginal weight gain caused by ovariectomy. Many healthcare providers recommend their female patients that have menopause to use glycine in their diet.
More Glycine Effects
Since glycine is a non-essential amino acid and a neurotransmitter for the central nervous system, this supplement can help supple muscle, bone, and connective tissue with collagen. Glycine has a small R group, which forms a triple helix structure that makes up of tropocollagen. In the body, 33% of all collagen is composed of glycine. Collagen levels in the body can decrease naturally due to anyone getting old. When this happens, inflammatory symptoms like arthritis occur. Researchers hypothesize that supplemental doses of glycine can strengthen joints and prevent reactive arthritis by blunting cytokine release by increasing chloride influx in the body.
Glycine is one of the three amino acids that can help aid the production of glutathione for the human body. Since this amino acid is a scavenger antioxidant, it will oppose proinflammatory signals from hydrogen peroxide. Studies show that glycine supplementation plays a vital role in balancing the redox reactions caused by metabolic syndrome in the human body and protecting patients from oxidative damage. There is even more research as a study stated that glycine has a vital role in the metabolism and nutrition of mammals and humans. Since glycine protects from inflammation and has fantastic health benefits for the body, when there are decreased levels of glycine in the body, it can be linked to metabolism-related disorders like type 2 diabetes and fatty liver disease.
Glycine provides cytoprotective effects on the liver and gastrointestinal tract by conjugating bile acids. This is crucial because glycine plays a role in helping lipids to be digested and lipid-soluble vitamins to be absorbed in the body. In alcohol-induced hyperlipidemia, studies have shown that glycine can reduce alcohol levels in the bloodstream while also retaining the membrane integrity by reducing lipid levels. Glycine can even protect the stomach and intestines from damages caused by gastrointestinal disorders. Since glycine can maintain enterocyte integrity and prevent apoptosis, its anti-inflammatory effects can fight oxidative stress. They can provide the requirements to the intestines and the gut in the body.
Conclusion
Glycine is a vital amino acid that provides anti-inflammatory properties for not only the body’s metabolism but also helps the gastrointestinal system. With more and upcoming research about glycine, it is essential for this amino acid to continue to provide outstanding effects to the human body and to make sure that it functions properly. When harmful factors start entering the body, or there is a glycine deficiency, it can cause the body to malfunction. So incorporating glycine-rich foods in the daily diet can help alleviate the symptoms gradually. Some products are beneficial for the body since they help support the immune system and make sure the body is functioning.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Bannai, Makoto, et al. �Oral Administration of Glycine Increases Extracellular Serotonin but Not Dopamine in the Prefrontal Cortex of Rats.� Wiley Online Library, John Wiley & Sons, Ltd (10.1111), 17 Mar. 2011, onlinelibrary.wiley.com/doi/full/10.1111/j.1440-1819.2010.02181.x.
D�az-Flores, Margarita, et al. �Oral Supplementation with Glycine Reduces Oxidative Stress in Patients with Metabolic Syndrome, Improving Their Systolic Blood Pressure.� Canadian Journal of Physiology and Pharmacology, U.S. National Library of Medicine, Oct. 2013, www.ncbi.nlm.nih.gov/pubmed/24144057.
File, S E, et al. �Beneficial Effects of Glycine (Bioglycin) on Memory and Attention in Young and Middle-Aged Adults.� Journal of Clinical Psychopharmacology, U.S. National Library of Medicine, Dec. 1999, www.ncbi.nlm.nih.gov/pubmed/10587285.
Griffin, Jeddidiah WD, and Patrick C Bradshaw. “Amino Acid Catabolism in Alzheimer’s Disease Brain: Friend or Foe?” Oxidative Medicine and Cellular Longevity, Hindawi Publishing Corporation, 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5316456/.
Kawai, Nobuhiro, et al. �The Sleep-Promoting and Hypothermic Effects of Glycine Are Mediated by NMDA Receptors in the Suprachiasmatic Nucleus.� Neuropsychopharmacology: Official Publication of the American College of Neuropsychopharmacology, Nature Publishing Group, May 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4397399/.
Kim, Min-Ho, et al. “Estrogen-like Osteoprotective Effects of Glycine in Vitro and in Vivo Models of Menopause.” Amino Acids, U.S. National Library of Medicine, Mar. 2016, www.ncbi.nlm.nih.gov/pubmed/26563333.
Li, X et al. “Dietary Glycine Prevents Peptidoglycan Polysaccharide-Induced Reactive Arthritis in the Rat: Role for Glycine-Gated Chloride Channel.” Infection and Immunity, American Society for Microbiology, Sept. 2001, www.ncbi.nlm.nih.gov/pmc/articles/PMC98707/.
McCarty, Mark F, et al. �Dietary Glycine Is Rate-Limiting for Glutathione Synthesis and May Have Broad Potential for Health Protection.� The Ochsner Journal, The Academic Division of Ochsner Clinic Foundation, 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5855430/.
Razak, Meerza Abdul, et al. �Multifarious Beneficial Effect of Nonessential Amino Acid, Glycine: A Review.� Oxidative Medicine and Cellular Longevity, Hindawi, 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5350494/.
Ross, Krista Anderson. �Glycine: Another Tool for the Hormone and Sleep Balancing Kit.� Doctor’s Data Specialty Testing Clinical Laboratory, 3 Dec. 2019, www.doctorsdata.com/resources/uploads/newsletters/Glycine’s-Role-in-Sleep-and-Hormone-Balancing.html.
Do digestive problems subside with rest or relaxation?
Stomach pains, burning, or aching 1-4 hours after eating?
Redden skin?
Nausea or vomiting?
If you are experiencing any of these situations, then you might be experiencing some digestive stress. Try some chamomile to reduce that stress and anxious mind.
Chamomile and its products are well-known for encouraging a healthy state of mind and for enhancing amazing sleep quality for anyone who takes this herb. This white and yellow blossom, however, has several impressive health benefits that are beneficial with anyone that’s feeling anxious in their daily, hectic lives and can provide other benefits for the body that has some ailments.
What is Chamomile?
Chamomile is an ancient medicinal plant by the Asteraceae family and is frequently known as the “earth apple on the ground” due to the apple-like fragrance it produces. Its blossoms have unique properties that could boost a person�s wellbeing and supplying beneficial nutrients that are remarkable for the body to relax and feel calm. This plant has existed for centuries and is native to eastern and southern Europe. Tons of research have shown that chamomile has been used in herbal remedies in ancient times during the Roman era, Greek era and Egypt era. The plant contains a thin spindle-shaped stem that produces tiny flower blossoms that resemble a daisy.
Chamomile Benefits
The chemicals of chamomile can serve as antioxidants in the human body and can prevent flare-ups from occurring. Because of this, when an individual is consuming chamomile goods; the health properties might help prevent the common cold, intestinal disorders from the gut, inflammation and many more body ailments that can affect the human body from functioning properly. There are two varieties of chamomile that have amazing properties that have been used for natural remedies are the German chamomile and the Roman chamomile.
German Chamomile: This type of chamomile is popular around the world and native to southern and eastern Europe. Studies have shown that people would take chamomile by the mouth to relieve ailments caused by environmental factors. There are some people that will even apply chamomile on their skin as an ointment. There is some scientific evidence that using German chamomile as an oral rinse could be helpful for cancer patients that have mucositis, which is inflammation and ulceration of the mucosal membrane lining in the digestive tract caused from chemotherapy and radiotherapy.
Roman Chamomile: This type of chamomile provides the same benefits as German Chamomile as it relieves the same ailments that environmental factors caused but also provides a bit more help to the body. Roman chamomile has hypnotic properties that help a person relax and falls asleep faster. There have been studies that this herb offered hypnotic effects to animals and when consumed, it decreased the amount of time for them to fall asleep.
The benefits that the chamomile plant provides are that it promotes the body to relax and other benefits that are essential to the body. When it is used as an essential oil for aromatherapy, the patient can feel less anxious when they breathe in the vapors and finally let their anxious mind relax.
Reducing Pain
The anti-inflammatory effect that both the essential oil and the chamomile flower itself can aid the body by reducing the pain that it has encountered. Since the chamomile plant has been used for hundreds, people have been using this plant to help reduce pain from inflammatory-related symptoms in the body they might be experiencing.
Studies have shown that people who consume herbal tea for their joint inflammation have shown an improvement especially in the knees and lower back. The antioxidant and anti-inflammatory properties that this herbal tea produces polyphenols that affect systemic inflammation and joint function in the body. Another study shows that patients with knee osteoarthritis used chamomile oil to decrease the stiffness in their joints and provide some beneficial effects on their physical function.
Heals and Promotes Skin Health
For anyone that has eczema and uses topical creams to reduce the redness, they might want to try using chamomile essential oil. The benefits of using chamomile essential oil are that it can help reduce irritated skin. A person can mix the chamomile essential oil with a carrier oil or lotion and apply it to their skin as the anti-inflammatory and antibacterial properties can calm down the red, dry, irritated skin while also decreasing breakouts from happening.
In some instances, there have been statements that chamomile is more effected than hydrocortisone lotion for skin lesions. Researchers found in a 2010 study, that German chamomile oil has been used to alleviate atopic dermatitis, which is a chronic skin disorder, by containing three major sesquiterpene constituents (azulene, bisabolol, and farnesene) by healing the skin gradually.
Improving Digestion
Another widespread use for chamomile, especially when it is brewed in a tea, is reducing unwanted symptoms that are associated with poor digestion in the digestive system. With chamomile tea, it can soothe an upset stomach, cramping, flatulence, and diarrhea. The therapeutic compounds that are found in chamomile can act as a digestive relaxant.
Improves Sleep and Relaxation
When it is brewed into a tea, chamomile can promote a person�s frame in mind and can enhance their sleep quality to provide them the necessary 8 hours of sleep. Research shows that individuals who drink chamomile tea before going to bed, have a better night’s sleep and relaxing a bit more. Apigenin provides a stimulant effect from chamomile tea and is bind with the benzodiazepine receptors in the brain, providing benefits that can help reduce stress from the body while also promoting a good night�s sleep.
In a 2017 study, the research shows that adults over the age of 60, consumed chamomile tea before they go to bed. The results showed that their sleep quality improved by reducing sleep complications like sleep apnea and the consumption of using sleep medication while improving their moods drastically over time.
Boosting Mental Wellness
Using chamomile products can benefit a person�s wellness. Since chamomile has beneficial properties to make the body relax, it can also help reduce the sensation of depression and anxiety in a person when it is consumed. Studies have stated that long-term chamomile intake is safe and may considerably reduce the effects of moderate to severe GAD symptoms in the body. Even using the oil for aromatherapy can be considered as an alternative for treatments for patients.
Conclusion
Thus chamomile is an effective and secured plant that has been used by individuals who have been experiencing a number of symptoms. Since chamomile is excellent for reducing pain, have better skin, improve mental health and provide many beneficial factors. When it is used in aromatherapy or consumed into the body, chamomile is a natural cure for a nervous mind. Some products combined with chamomile are designed to offer support to the gastrointestinal tract and make sure that sugar metabolism is functioning properly.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Abdullahzadeh, Mehrdad, et al. �Investigation Effect of Oral Chamomilla on Sleep Quality in Elderly People in Isfahan: A Randomized Control Trial.� Journal of Education and Health Promotion, Medknow Publications & Media Pvt Ltd, 5 June 2017, www.ncbi.nlm.nih.gov/pubmed/28616420.
Charousaei, Firuzeh, et al. �Using Chamomile Solution or a 1% Topical Hydrocortisone Ointment in the Management of Peristomal Skin Lesions in Colostomy Patients: Results of a Controlled Clinical Study.� Ostomy/Wound Management, U.S. National Library of Medicine, May 2011, www.ncbi.nlm.nih.gov/pubmed/21617262.
Christiansen, Sherry. �The Health Benefits of Roman Chamomile.� Verywell Health, Verywell Health, 14 Jan. 2019, www.verywellhealth.com/roman-chamomile-4571307.
Drummond, Elaine M, et al. �An in Vivo Study Examining the Antiinflammatory Effects of Chamomile, Meadowsweet, and Willow Bark in a Novel Functional Beverage.� Journal of Dietary Supplements, U.S. National Library of Medicine, Dec. 2013, www.ncbi.nlm.nih.gov/pubmed/24237191.
Health Team, eMedicine. �German Chamomile:Uses, Side Effects, Dosage, Interactions & Health Benefits.� EMedicineHealth, EMedicineHealth, 17 Sept. 2019, www.emedicinehealth.com/german_chamomile/vitamins-supplements.htm.
Mao, Jun J, et al. �Long-Term Chamomile (Matricaria Chamomilla L.) Treatment for Generalized Anxiety Disorder: A Randomized Clinical Trial.� Phytomedicine : International Journal of Phytotherapy and Phytopharmacology, U.S. National Library of Medicine, 15 Dec. 2016, www.ncbi.nlm.nih.gov/pubmed/27912875.
Shoara, Ruhollah, et al. �Efficacy and Safety of Topical Matricaria Chamomilla L. (Chamomile) Oil for Knee Osteoarthritis: A Randomized�Controlled Clinical Trial.� Complementary Therapies in Clinical Practice, U.S. National Library of Medicine, Aug. 2015, www.ncbi.nlm.nih.gov/pubmed/26256137.
Singh, Ompal, et al. �Chamomile (Matricaria Chamomilla L.): An Overview.� Pharmacognosy Reviews, Medknow Publications Pvt Ltd, Jan. 2011, www.ncbi.nlm.nih.gov/pmc/articles/PMC3210003/.
Srivastava, Janmejai K, et al. �Chamomile: A Herbal Medicine of the Past with Bright Future.� Molecular Medicine Reports, U.S. National Library of Medicine, 1 Nov. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC2995283/.
Do you feel irritable, nervous, shaky, or light-headed between meals? Do you have difficulty eating large meals in the morning? Do you feel fatigued after meals? Do you have sugar and sweet cravings after meals? Do you have an increased appetite?�If so, you may be experiencing early SIBO symptoms. �
SIBO, or small intestinal bacterial overgrowth, is a severe health issue that ultimately affects the small intestine in the digestive system. This gastrointestinal (GI) tract condition happens when the bacteria that generally grows in several different regions of the gut begin to grow in the small intestine. SIBO can commonly cause pain, discomfort, and diarrhea, among other symptoms. It can also cause malnutrition as bacteria utilize the human body�s nutrients.�
What are the Symptoms of SIBO?
Small intestinal bacterial overgrowth, or SIBO, is a serious condition that includes symptoms which can commonly affect the gut. These can include: �
pain or discomfort in the stomach
gas
bloating
constipation
diarrhea
cramps
indigestion
a general feeling of fullness
weight loss
What are the Causes of SIBO?
Small intestinal bacterial overgrowth (SIBO) is a severe health issue that is unfortunately not yet fully understood by researchers and healthcare professionals. According to research studies and clinical trials, however, this gastrointestinal, or GI, tract condition can ultimately happen when the small intestine is anatomically abnormal, due to pH changes in the small intestine, when the human body’s immune system isn’t functioning accordingly, or due to malfunctions in the muscular activity of the small intestine which can commonly cause food and bacteria to remain and not be removed from the organ. �
SIBO, or small intestinal bacterial overgrowth, is also commonly associated with a variety of health issues. These can involve the following, including: �
a stomach bug, known as viral gastroenteritis
celiac disease
Crohn�s disease
low stomach acid levels, known as hypochlorhydria
IBS or irritable bowel syndrome
gastroparesis
portal hypertension
nerve damage
cirrhosis
several gastric bypass procedures
surgical interventions which cause strictures or adhesions
What are the Risk Factors of SIBO?
Moreover, researchers and healthcare professionals have determined that an underlying chronic health issue and a previous surgery or surgical intervention that affects the gastrointestinal (GI) tract can be several risk factors of SIBO. Other wellness problems which can ultimately cause SIBO include: �
diabetes
scleroderma
hypothyroidism
Parkinson’s disease
HIV
narcotics or drugs/medications which slow down the digestive system
What is the Diagnosis for SIBO?
If you’ve experienced any of the SIBO symptoms mentioned above, see your doctor immediately. The doctor will ask the patient about their symptoms and medical history. The doctor will also perform a physical examination which may include palpating or gently feeling the patient’s abdomen. A qualified and experienced healthcare professional may also order additional blood, fecal, and/or any other tests to diagnose small intestinal bacterial overgrowth. �
A breath test is another common test utilized for the diagnosis of SIBO. Excess bacteria in the small intestine can cause the release of hydrogen and methane, two common gases which can be identified through a breath test. This test is non-invasive and can be performed in a doctor�s office. Before a breath test, the patient will need to fast overnight. During a breath test, the patient will first breathe into a tube. Then, the patient will take a specialized sweet drink provided by the doctor and they will breathe into several other tubes at regular intervals for 2 to 3 hours after taking the specialized sweet drink. �
If common tests for SIBO are inconclusive, the doctor may need to sample the fluid from the patient’s small intestine to see what bacteria is growing there. �
What is the Treatment for SIBO?
Common treatment approaches for SIBO, or small intestinal bacterial growth, can ultimately include a combination of antibiotics and diet modifications. �
Antibiotics
Treatment for SIBO first involves getting the bacteria in the digestive system under control. This is generally achieved by utilizing antibiotics, such as ciprofloxacin (Cipro), metronidazole (Flagyl), or rifaximin (Xifaxan). Further treatment for SIBO may also require intravenous (IV) therapy for nutrition and fluids if the serious gastrointestinal (GI) tract condition has ultimately caused malnutrition or dehydration, among a variety of other symptoms. �
Although antibiotics may help reduce the amount of bacteria in the small intestine, however, these will not always help address the underlying chronic health issues that caused the wellness problem in the first place. If the qualified and experienced healthcare professional determines that the patient’s SIBO is due to an underlying chronic health issue, the patient will also need to begin treatment for that wellness problem. Diet modifications may also help treat SIBO. �
Diet Modifications
Further research studies and clinical trials are still required to demonstrate if diet can cause small intestinal bacterial overgrowth (SIBO) but, many people with SIBO have reported feeling relief from their symptoms after diet modifications. Talk to your doctor before making any modifications to your diet. �
Furthermore, people with SIBO or other chronic health issues may only need to make small diet modifications to treat their symptoms. These can include: �
Eating a balanced and nutritious diet
Consuming minimal meals more often to prevent having too much food sit in the stomach
Avoid eating gluten products, if you have celiac disease or any other similar chronic health issues
The doctor may also recommend the patient to try an elemental diet to help treat SIBO. An elemental diet replaces food and drinks with several liquid formulas throughout an extended period of time. In one small-scale research study and clinical trial, approximately 80 percent of participants with SIBO had a normal breath test result following an elemental diet for 15 days. The researchers ultimately determined that an elemental diet may be a highly effective treatment approach for SIBO. However, further evidence is still needed. Talk to your doctor before starting an elemental diet and follow their instructions. �
Taking probiotics may also help restore the gut bacteria. A 2010 research study and clinical trial demonstrated that probiotic treatment can be more safe and effective for SIBO than taking antibiotics. However, a 2016 review determined that further evidence for the efficiency of probiotics in SIBO treatment was ultimately inconclusive. The best treatment approach for a patient with SIBO is to follow a qualified and experienced healthcare professional’s advice. �
SIBO, or small intestinal bacterial overgrowth, is a well-known and often severe health issue that generally occurs because of an underlying chronic condition or disease. Common symptoms may ultimately determine the presence of SIBO. In addition, if the patient has a chronic health issue, such as celiac disease or Crohn’s disease, they should talk to a doctor to develop a long-term treatment plan. SIBO, or small intestinal bacterial overgrowth is treatable. If left untreated, this gastrointestinal (GI) tract problem can also cause dehydration and malnutrition. Patients should contact a doctor immediately if they suspect they have SIBO so that they can begin treatment right away. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
�
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Madormo, Carrie. �Everything You Should Know About Small Intestinal Bacterial Overgrowth (SIBO).� Edited by Suzanne Falck, Healthline, Healthline, 14 June 2017, www.healthline.com/health/sibo#symptoms.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
If you are experiencing any of these situations, then you might have experienced some trouble losing weight.
Trying to lose weight is harder than it looks. While the secret of losing weight is more accessible said than done, people are always trying to live healthier lives by exercising and eating right. Some people can maintain a healthy weight throughout their lives effortlessly; however, for others, it is a struggle that starts from when they were a kid, and it gets harder when they start growing up. There have been books on how to lose weight, and people gaining weight when they are middle-aged, it is shown around their mid-section of their bodies. Although when a person is trying to lose weight due to health reasons or wanting to get better, it can be a long, arduous journey.
There are many reasons why individuals are having trouble losing weight. It might be due to being older and that the body changes along with getting older as well. Here are some of the reasons why it is difficult to lose weight, the older a person gets.
Losing Muscle Mass
When a person age, their metabolism changes with them. When they are younger, their metabolism can make a person exercise with high intensity. As they get older, their metabolism changes, and they will slow down a bit when they are exercising. Not only that, but a person can lose their muscle mass when they reach the age of 30.
Studies have shown that the amount of lean muscle mass can naturally decline 3 to 8 percent per decade when a person hits 30, and it will be much harder when they are at the age of 60. This is due to sarcopenia. Sarcopenia is a condition that is characterized by losing skeletal muscle mass and functioning. This condition is progressive, and some of the risk factors include age, gender, and the level of physical activity a person is doing. Since the strength and muscle mass decline in older adults mostly, it can lead to acute and chronic diseases that can harm the body.
There is a way to combat muscle loss for anyone that wants to have lean muscles and to lose weight, is to add weight training to their exercise regime. Research shows that lifting weights is perfect for anyone to make sure that the body stays toned and muscular while also preventing a metabolic slowdown. Since male and females bodies are different, doing weight lifting will help the muscles look lean and toned for females, while for males, their muscles look more prominent and bulker, depending on the weights they are using and how many reps they are doing.
Getting Overly Stressed
As we get older, the more stress we can get. Stress is made up of the hormone cortisol, which is released into the body. It can also be in two categories, which are short term and long term. With short term stress, it is effortless to manage since a person can be worried about a project for school, getting a job interview, or worrying about the little things, the cortisol hormone is short term and can be easily managed.
When it is long-term stress, it can lead to chronic illnesses if it is in a person for far too long. The pressures of work, having too many obligations, or stressing out due to deadlines for projects are bad for a person to have since the cortisol levels are building up in the body. Even having a sedentary job can cause the body to develop stress and weight gain.
There are ways to reduce stress in the body like finding hobbies to enjoy, exercising, always help the body release the tension that is pent up, even having a self-care day can do many wonders to a person and their body. Trying to de-stress the body is excellent and beneficial to anyone because being stress-free is essential for losing weight.
Major Lifestyle Changes
When it comes to significant lifestyle changes, it can be any one of these changes that can cause a person to gain weight. It does not always happen from the inside, but it can happen to people when they enter their thirties. Some changes can include starting a family, trying to find time out of a hectic schedule, distractions, or homework. Whatever the reasons are, these lifestyle changes require much attention. When that happens, then the pounds start to creep in, causing weight gain.
Medical Condition
Sometimes when a person gains weight, it is due to a medical condition they might have, and it makes it harder for them to lose weight as well. These medical conditions include PCOS (polycystic ovarian syndrome), sleep apnea, and hypothyroidism. When these conditions affect the targeted body systems, it can cause many health problems to the body by causing it to dysfunction.
“There are many reasons why losing weight is hard for anyone. There is a wide variety of reasons like eating junk foods, not getting enough sleep, staying hydrated, or a hectic lifestyle. If we take the time to change one thing to maintain a healthy lifestyle, then the weight will slowly but surely go away.” -Dr. Alex Jimenez D.C., C.C.S.T. Insight
Conclusion
Losing weight is hard for anyone, and it can be easy for some while difficult for others. Since everyone has a different body structure, trying to lose weight is one of the more laborious tasks if an individual has problems trying to shed off the weight. By changing some of the habits that are causing the weight gain, it may be beneficial to not only the person but to their body. Some products can help the body’s metabolism and support the function of sugars and amino acids that help support even the gastrointestinal lining, the endocrine system, and help maintain the blood sugar levels.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Dray, Tammy. �Why Is It Harder to Lose Weight as You Get Older?� LIVESTRONG.COM, Leaf Group, 2019, www.livestrong.com/article/417064-why-is-it-harder-to-lose-weight-as-you-get-older/.
Gunnars, Kris. �20 Common Reasons Why You’re Not Losing Weight.� Healthline, 20 Aug. 2018, www.healthline.com/nutrition/20-reasons-you-are-not-losing-weight.
Lawler, Moira. �5 Reasons It’s Harder to Lose Weight With Age.� EverydayHealth.com, 27 June, 2019, www.everydayhealth.com/weight/weight-gain-and-aging.aspx.
Santilli, Valter, et al. �Clinical Definition of Sarcopenia.� Clinical Cases in Mineral and Bone Metabolism: the Official Journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases, CIC Edizioni Internazionali, Sept. 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4269139/.
Walston, Jeremy D. �Sarcopenia in Older Adults.� Current Opinion in Rheumatology, U.S. National Library of Medicine, Nov. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC4066461/.
Health coaches are becoming more and more crucial as modern and naturopathic medicine continues to improve. More than ever, the healthcare field is progressing at high speeds and professionals do not always have the time available that some patients desire. Here is where health coaches get involved. Basically, the position of a health coach was produced to fulfill the emptiness in several doctor offices. Many physicians contribute but don’t have the time or tools to help each individual and assist in constructing healthy habits on a day to day basis. But, health coaches are available to be a supportive mentor who guides and assists patients in making healthy lifestyle changes. Many patients who seek assistance to change their lifestyle are those afflicted by some kind of chronic pain, headaches, or joint swelling.
In the previous weeks, we have defined and explained what a health coach is and what they really do, as well as the first four steps a health coach might take with a patient. Throughout this article, the fifth and sixth steps will be broken down and analyzed.
Need a refresher? No problem!
Health Coaching in El Paso: Part 1 can be found by clicking�here
Health Coaching in El Paso: Part 2 can be found by clicking�here
Health coaching in El Paso: Part 3 can be found by clicking�here
Step 5: Visualizing Your Best Self
�
This step is extremely crucial. The reason being, without a vision of where an individual wants to be, they can easily get lost on their way to achieving a goal. A vision statement is not intended to be a specific sentence, but rather a loose description of what / who the patient is trying to become.
In order to create this statement, a health coach will work with the patient to clearly identify their skills, interests, and strengths. These are oftentimes similar to the items listed on the values sheet the patient filled out while the health coach was working with them back in�step 1. Other times, the health coach will assist the patient with their vision statement by asking things like:
What are you naturally good at?
What have you always wanted to see, do, or create?
What would help you feel more fulfilled?
In addition to these questions,� the health coach might encourage the individual by steering the conversation in a way that is related to their best self. With the help from a health coach, the patient can reflect and describe their best self as well as the emotions connected to their best self (thinking, feeling, and doing). A coach will also provide critical thinking questions related to a patient’s best self such as:
How do you know you’re there?
How do you know you’re not there?
How can you remember to be your best self and not slip back into the old ways of being?
Step 6: Creating A Plan For Resiliency
It is simply human nature that all people react to stressful situations differently.� However, one thing that is guaranteed is people will need a plan to get back on track. Undergoing life changes is not a simple task, but having a plan is.�An approach for building resilience must be tailored to the specific individual. A health coach will ensure the individuals that falling off track is natural, but how you get back on track is what counts. It starts with reflecting, seeking support, and making a plan to move forward.
When a patient is placed in a stressful situation, it is key they take a moment to recognize the situation and think about how they are feeling. During the moment, it may be difficult but with practice, reflection, and help from a health coach, the process becomes easier.
The best tips when it comes to addressing resiliency are to develop connections, set daily intentions, reflect on experiences, practice self-care, and be proactive.
A health coach may encourage a journal to help patients celebrate small victories and take responsibility for their own happiness. In addition to this, there are other resources available the patients may utilize such as books, self-help support groups, and asking themselves, “What do I typically find helpful in a stressful situation?”.
By utilizing a health coach and implementing these 6 steps into one’s life, the benefits are unbelievable. Identifying values, determining goals, building a plan for action, tracking progress and results, visualizing the best self, and creating a plan for resiliency will help individuals reach their health goals better than before.
By working with a health coach and remembering these exercises, individuals are extremely likely to be successful. Not only do they have someone for accountability, but they are learning ways to become more independent and thoughtful when it comes to their health. A positive community offers support that many individuals need to thrive. Naturopathic medicine and functional approaches are becoming more recognized for their ability to work on a variety of individuals. Take advantage of all the resources around that are there to help you.�– Kenna Vaughn, Senior Health Coach�
All information and resources for this post came from an Integrative Practioner article titled, “A Six-Step Approach To Health And Wellness Coaching: A Toolkit for Practice Implementation” and can be found by clicking�here; as well as listed below in the proper bibliography.
*The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900.
Miller, W. and Rose, G. (1991). Motivational Interviewing: Preparing People to Change Addictive Behavior. Guilford Publications.
Pecoraro, Wendy. �A Six-Step Approach to Health and Wellness Coaching: A Toolkit for Practice Implementation.��Official Media Integrative Practitioner, 17 Oct. 2019, www.integrativepractitioner.com/resources/e-books/a-six-step-approach-to-health-and-wellness-coaching-a-toolkit-for-practice-implementation.
Trzeciak, S. and Mazzarelli, A. (2019). Compassionomics. Studer Group.
If you are experiencing any of these situations, then you might want to consider seeing a chiropractor.
Transgender Discrimination
Going to get a routine checkup from either the doctor or the dentist is stressful enough for individuals. For transgender individuals, going to get a routine checkup is even more stressful for them as they are more often getting mistreated or even denied care that they needed. In a 2009 survey, around 70% of transgender and gender-nonconforming individuals have reported experience the following:
Refusal of health care
Healthcare professional refusing to touch or use precautions to individuals
Healthcare professionals using unnecessary abusive language
Blamed for their own health wellness
Healthcare professionals being abusive to the patients
Additional surveys also revealed that transgender health care is discriminated and has kept at least one-third of transgender individuals from seeking medical help for any illnesses or injuries that they may have encountered. It is especially startling that many transgender patients have educated their doctors about transgender health.
Transgender is defined as �an individual who feels that their gender identity does not match their physical body and is different from the gender they are born in.� A 2016 data analysis by The Williams Institute, found out that about 1.4 million American individuals that identify as transgender.
Transgender individuals are beginning to speak about their problems and issues. They talk about the concerns about how office staff are feeling betrayed during their transitional status, all the way to others discriminating in the health care they are receiving. Transgender individuals are providing medical professionals what they can and should do to make sure that they feel safe in the medical professional’s care. Without awareness and education, the healthcare providers are not doing; these issues are more likely to escalate with the growing transgender population.
What Practitioners Need To Do
In March 2019, two individuals Emma Vosicky and Jaime Pagano, addressed to the students and faculty at the National University of Health Sciences (NUHS) Pride Medical Alliance (PMA) club about the challenges they faced. These two individuals were worried about how they would be treated differently by the office staff and were in fear of those who would betray them by sharing their information. These transgender speakers went ahead and discussed the difficult challenges that went beyond the physical transformations that they and many others have faced when seeking medical care.
Vosicky went ahead and discussed how necessary it was to “out” herself to a medical professional when they were asking her about the medication she was taking or discussing the previous medical history that did not match her appearance. Both speakers suggested that healthcare providers should consider different ways that they can let their patients know that they are non-discriminatory to them.
Pagano discussed how he felt much safer when he sees an intake form that included different sex options in a doctor’s lobby. Terms that are in the intake form includes gender non-conforming, non-binary, trans-female, and trans male, alongside with male and female. He said that this feels helpful to the provider he was seeing to be aware and cognizant that everyone is not living in a male/female only world. Pagano also mentioned that he feels more confident that his provider will be more clinically aware of his needs.
The NUHS faculty member Jamine Blesoff, ND, has worked with transgender youth and stressed that it is vital for physicians to ensure that their patients’ care is essential throughout each stage of their transitions.� Dr. Blesoff noted that health practitioners still must provide a PAP test for men who are transitioning from being female as well as a prostate exam for pre-surgical women. Dr. Blesoff expresses concern that some doctors will not provide any type of service to transgender patients.
“It is a universal requirement that healthcare practitioners adhere to HIPAA laws and to make sure that their transgender patients are treated with dignity, respect, and above all else, ensuring that they receive the needed medical care that they deserve like everyone else.”-Dr. Alex Jimenez D.C., C.C.S.T. Insight
Being Gender Neutral
Healthcare professionals should always build trust with any patients that walks through the door. Healthcare providers have to make sure that the intake forms provide space for patient�s gender identity. In addition to the patient’s physical status, transgender patients can indicate their preferred identity, and healthcare professionals can ask what pronouns the patients preferred like he/she/they and uses them throughout their visit.
Speak Respectfully
Doctors should consider using their patient�s chosen name instead of their �real� name if it does not show up in their records and ask the patient if a different name is listed. Healthcare professionals should politely apologize if they use the individual’s wrong name or identity. Even though it may be a bit challenging for long-time patients, but as long as healthcare professionals are making an effort, it will become a way of demonstrating respect not only to the patient but to the doctors as well.
“I always believe that intent matters more than words,” Sam Brinton said, who is the Head of Advocacy and Government Affairs at The Trevor Project. Brinton also mentioned, “There is a difference between ‘I cannot’ and ‘I am trying.’ If you intend to hurt me by not using my pronouns, that matters more than any words you say.”
Recognize the Physical Discomfort
For transgender patients to feel safe and that they are getting the medical care that they need, doctors should take care of them and be respectful to their patient�s needs. For transgender patients, it is already stressful enough for them to get a routine check. When doctors are respectful of their patient’s needs and not to continue procedures to them, that will cause them shame and physical discomfort.
Treat the Ailments Only
Healthcare professionals should consider what kind of information or examination that they are giving to their patients the care they needed. So providing necessary medical care like back pains, stomach problems, immune disorders, or a general checkup is essential.
Educate the Staff
All medical staff that interacts with patients must educate themselves on how to provide comfort and care when they are dealing with transgender patients. Medical providers and medical staff must apply the knowledge of interacting with patients on a day to day basis.
Conclusion
Transgender healthcare is a necessity for these individuals that are trying to get the same benefits that everyone else is getting. Healthcare professionals must be respectful and provide the best care to offer for patients with different identities and backgrounds. Educating and being aware of what the patient is going through is part of the doctor’s job to assist not only themselves better but also inform the patient a solution while making them feel comfortable. Some products are here to support anyone’s ailments and provide support to the intestines, gastrointestinal function, and muscular system.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Flores, Andrew R., et al. �How Many Adults Identify As Transgender In The United States?� The William Institute, June 2016, williamsinstitute.law.ucla.edu/wp-content/uploads/How-Many-Adults-Identify-as-Transgender-in-the-United-States.pdf.
Marshall, Tari. �Transgender Health Care: How to Meet Their Needs.� Transgender Health Care: How to Meet Their Needs, 20 Nov. 2019, blog.nuhs.edu/the-future-of-integrative-health/transgender-health-care-how-to-meet-their-needs.
Marshall, Tari. �When He/She May Be They/Them.� LinkedIn, 13 Feb. 2018, www.linkedin.com/pulse/when-heshe-may-theythem-tari-marshall?trk=portfolio_article-card_title.
Team, Lambda. �Lambda Legal Releases Health Care Discrimination Survey Results; More Than Half of LGBT and HIV Positive Respondents Report Discrimination.� Lambda Legal, 4 Feb. 2010, www.lambdalegal.org/news/ny_20100204_lambda-releases-health.
Team, NUHS. �Pride Club Program Addresses Transgender Experiences with Medical Professionals: National University of Health Sciences Illinois & Florida.� Earn a Degree Chiropractic, Naturopathy, and Acupuncture Medicine |�National University of Health Sciences, 13 Mar. 2019, www.nuhs.edu/news/2019/3/pride-club-program-addresses-transgender-experiences-with-medical-professionals/.
Team, The Trevor Project. �Saving Young LGBTQ Lives.� The Trevor Project, 2019, www.thetrevorproject.org/#sm.00013irq131dh2e6qpejz1qoa103y.
If you are experiencing any of these situations, then you might have a magnesium deficiency.
Good health is one of the things to be thankful for. Unfortunately, 84 million adults in the U.S. are living with prediabetes, while another 27 to 28 million adults are affected with type 2 diabetes, so good health is not a given for everyone. According to the National Osteoporosis Foundation, 10 million Americans have osteoporosis, and another 44 million have low bone density, putting them at an increased risk. From the body to the brain, psychological and mood issues like depression and anxiety plague people. There is something that may be beneficial for all of these issues and is a workhorse nutrient that does not get its share of the spotlight. It has been regulated to the shadows behind the flashier and more buzzworthy compounds that get recognition than this nutrient. Magnesium is the critically essential, time-tested, go-to reliable nutrient that everybody needs.
The human body contains about 25 grams of magnesium, which is needed for over 300 enzymes to react. The data from the NHANES (National Health and Nutrition Examination Survey) indicated that the majority of Americans from all ages consume less that than their respective EARs (estimated average requirements) on magnesium. It is a massive problem because magnesium deficiency plays a role in hypertension, cardiovascular diseases, type 2 diabetes, osteoporosis, and migraine headaches.
Magnesium and Glucose Levels
Magnesium is required for several enzymes in glycolysis, which is the first process in glucose metabolism in the body, and it may explain why it is such an essential factor for blood sugar regulation in the body. Epidemiological evidence indicates that magnesium intake is inversely correlated with the risk of type 2 diabetes. Studies have shown that higher magnesium intakes may help reduce the risk of type 2 diabetes as much as 17%, and 48% of people with type 2 diabetes may have hypomagnesemia.
The inverse correlations have been observed between circulating magnesium levels, fasting blood glucose, and insulin level. There is even a response to an OGTT (oral glucose tolerance test) for those with type 2 diabetes. Research shows that higher magnesium intakes are also associated with reducing the risk for cardiovascular mortality, particularly in women as it is estimated that 100 mg/day increase in dietary magnesium may confer as much as 25% reduction in the risk of cardiovascular mortality. Researchers have called subclinical magnesium deficiency “principal dicer of cardiovascular disease and a public health crisis,” so naturopathic practitioners suggesting adding magnesium-rich foods to a person’s diet is beneficial to prevent magnesium deficiency from happening.
Magnesium and Mental Health
In regards to mental health, evidence has suggested that magnesium deficiency may play a role in the etiology of depression and that high-dose supplementation of magnesium may improve this condition. Studies found that other issues that have responded favorably to magnesium supplementation include irritability, insomnia, postpartum depression, and substance abuse in the body. There is some suggestive but inconclusive evidence that indicates that magnesium supplementation may be beneficial for individuals with mild anxiety and possibly owing to its role as a natural relaxing agent.
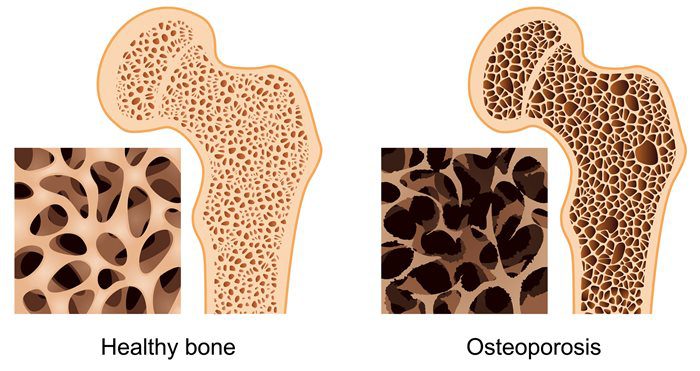
Magnesium and Osteoporosis
For osteoporosis, calcium gets all the attention when it comes to bone mineral density; however, magnesium is an essential component for the physical structure of bone density as well. There is about 60% of the body’s magnesium stored in the bones, and considering the high prevalence of suboptimal magnesium intake in North America, the concurrent high prevalence of osteoporosis is unsurprising. Concerning bone health, low magnesium status may interfere with the efficacy of vitamin D supplementation. In the Journal of the American Osteopathic Association, a review was covered in which researchers affirmed that vitamin D could not be metabolized without the sufficient levels of magnesium.
Adding Magnesium-rich Food To Your Feast
With Thanksgiving coming around the corner, there is a way to bring magnesium to the holiday table. The good news is that this crucial mineral fits perfectly into Thanksgiving entertainment. People can serve mixed nuts as part of appetizers or hors d’oeuvres while their guests are socializing. Mixed nuts can provide a substantial amount of magnesium. They can be an excellent addition to turkey stuffing/dressing or a whole grain salad, which can provide even more magnesium that the body needs. Serving leafy greens like chard and spinach are reliable sources of magnesium, as well as certain beans like black beans and kidney beans are filled with magnesium.
Since nuts, seeds, and beans are high in phytic acid, which is a compound that binds to the minerals. So in order to increase the bioavailability of magnesium in these foods, soaking nuts, seeds, and beans is a traditional preparation method to neutralize some of this problematic molecule.
For dessert, adding chocolate is an excellent way to get magnesium in the body. Since the cocoa powder is a rich source of magnesium, research has been speculating that the chocolate cravings might be the body’s way of crying for magnesium. Not to mention, when foods are much higher in magnesium, they are not the usual subjects for intense cravings like chocolate.
“So for Thanksgiving, adding magnesium-rich foods can help cut back the sodium and carb intake of the holiday feast can be beneficial to your body to function correctly and good for your health.”-Dr. Alex Jimenez D.C., C.C.S.T. Insight
Conclusion
Magnesium is an excellent and beneficial nutrient for anyone to add to their Thanksgiving dinner. The nutrient plays many roles in the body like regulating blood sugar, improving mental health as a natural relaxing agent, and preventing osteoporosis from occurring. Adding this nutrient and some products can help the body metabolize and stable the blood sugar levels to their normal range for beneficial results.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Boyle, Neil Bernard, et al. �The Effects of Magnesium Supplementation on Subjective Anxiety and Stress-A Systematic Review.� Nutrients, MDPI, 26 Apr. 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5452159/.
Bruinsma, K, and DL Taren. “Chocolate: Food or Drug?” Journal of the American Dietetic Association, U.S. National Library of Medicine, Oct. 1999, www.ncbi.nlm.nih.gov/pubmed/10524390.
Castiglioni, Sara, et al. �Magnesium and Osteoporosis: Current State of Knowledge and Future Research Directions.� Nutrients, MDPI, 31 July 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3775240/.
DiNicolantonio, James J, et al. �Subclinical Magnesium Deficiency: a Principal Driver of Cardiovascular Disease and a Public Health Crisis.� Open Heart, BMJ Publishing Group, 13 Jan. 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5786912/.
Eby, George A, and Karen L Eby. �Rapid Recovery from Major Depression Using Magnesium Treatment.� Medical Hypotheses, U.S. National Library of Medicine, 2006, www.ncbi.nlm.nih.gov/pubmed/16542786.
Fang, Xin, et al. �Dose-Response Relationship between Dietary Magnesium Intake and Cardiovascular Mortality: A Systematic Review and Dose-Based Meta-Regression Analysis of Prospective Studies.� Journal of Trace Elements in Medicine and Biology: Organ of the Society for Minerals and Trace Elements (GMS), U.S. National Library of Medicine, Dec. 2016, www.ncbi.nlm.nih.gov/pubmed/27053099.
Fang, Xin, et al. �Dose-Response Relationship between Dietary Magnesium Intake and Risk of Type 2 Diabetes Mellitus: A Systematic Review and Meta-Regression Analysis of Prospective Cohort Studies.� Nutrients, MDPI, 19 Nov. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC5133122/.
Higdon, Jane. �Magnesium.� Linus Pauling Institute, 14 Oct. 2019, lpi.oregonstate.edu/mic/minerals/magnesium#structural-roles.
Serefko, Anna, et al. �Magnesium and Depression.� Magnesium Research, U.S. National Library of Medicine, 1 Mar. 2016, www.ncbi.nlm.nih.gov/pubmed/27910808.
Spiga, Rosangela, et al. �Are Circulating Mg2+ Levels Associated with Glucose Tolerance Profiles and Incident Type 2 Diabetes?� Nutrients, U.S. National Library of Medicine, 14 Oct. 2019, www.ncbi.nlm.nih.gov/pubmed/31615167.
Team, DFH. �Preparing Beans and Legumes � What to Know.� Designs for Health, 9 Oct. 2018, blog.designsforhealth.com/preparing-beans-and-legumes.
Team, DFH. �Put Magnesium on the Menu at Thanksgiving.� Designs for Health, 19 Nov. 2019, blog.designsforhealth.com/node/1151.
Team, NOF. �Https://Cdn.nof.org/Wp-Content/Uploads/2015/12/Osteoporosis-Fast-Facts.pdf.� National Osteoporosis Foundation, 2015.
Unknown, Unknown. �Diabetes Statistics.� National Institute of Diabetes and Digestive and Kidney Diseases, U.S. Department of Health and Human Services, 1 Sept. 2017, www.niddk.nih.gov/health-information/health-statistics/diabetes-statistics.
Unknown, Unknown. �Office of Dietary Supplements – Magnesium.� NIH Office of Dietary Supplements, U.S. Department of Health and Human Services, 11 Oct. 2019, ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/#h4.
Unknown, Unknown. �Office of Dietary Supplements – Magnesium.� NIH Office of Dietary Supplements, U.S. Department of Health and Human Services, 11 Oct. 2019, ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/#h7.
Uwitonze, Anne Marie, and Mohammed S. Razzaque. �Role of Magnesium in Vitamin D Activation and Function.� The Journal of the American Osteopathic Association, American Osteopathic Association, 1 Mar. 2018, jaoa.org/article.aspx?articleid=2673882.
Waanders, Femke, et al. �Hypomagnesaemia and Its Determinants in a Contemporary Primary Care Cohort of Persons with Type 2 Diabetes.� Endocrine, U.S. National Library of Medicine, 24 Oct. 2019, www.ncbi.nlm.nih.gov/pubmed/31650393.
Yanovski, Susan. �Sugar and Fat: Cravings and Aversions.� OUP Academic, Oxford University Press, 1 Mar. 2003, academic.oup.com/jn/article/133/3/835S/4688015.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine