Do you experience chronic gut health issues? Research studies have found that Parkinson’s disease (PD) may be associated with the gut-brain connection. Evidence in a group of mice demonstrated that PD can actually start in the gut, which may explain why patients with PD have constipation and other gut health issues. Scientists have also found that patients with Parkinson’s disease report having gut health issues up to 10 years before experiencing tremors and other symptoms. According to other research studies, patients with PD may even have different biodiversity of gut bacteria than other healthy adults. �
Outcome measures in the group of mice showed that the “harmful” alpha-synuclein fibers that build-up in the nerve cell endings of patients with Parkinson’s disease can immediately affect neurons in the brain. Scientists found this by identifying the spread of alpha-synuclein fibers in the nerve cell endings of the affected neurons in the brain of patients with PD. Alpha-synuclein is a fat-soluble substance, generally found in healthy neurons, however, alpha-synuclein molecules can clump together and damage brain cells. Scientists also found that patients can have a build-up of alpha-synuclein fibers in their gut. �
The Gut-Brain Connection
A collection of fibers, known as the vagus nerve, which starts in the brain stem and extends to the major organs, including the gut, is believed to be the main source of PD associated with the gut-brain connection. Recent research studies of vagotomy patients demonstrated a reduced risk of developing Parkinson’s disease. Scientists have also found that alpha-synuclein fibers injected into the digestive system of a group of mice can reach the brain through the vagus nerve. If alpha-synuclein molecules can reach the brain from the gut, why does the fat-soluble substance build-up in the gut in the first place? �
Scientists believe that alpha-synuclein develops in the gastrointestinal (GI) tract to help combat pathogens and other “harmful” components. Michael Zasloff, a professor at Georgetown University, and his colleagues reported that alpha-synuclein molecules developed in healthy children after having an infection and alpha-synuclein seemed to trigger immune cells. Scientists also believe that alpha-synuclein can build-up in the GI tract due to the gut microbiome itself. Evidence in a group of mice demonstrated that bacteria can ultimately activate the development of alpha-synuclein in the gut and brain. �
Research studies have started to understand how the gut microbiome may be associated with Parkinson’s disease. Scientists have found that patients with Parkinson’s disease have a unique biodiversity of gut bacteria and scientists have also found that fecal microbe transplants from patients into a group of mice may increase alpha-synuclein in the brain and worsen symptoms in patients with PD. Other research studies have also shown that alpha-synuclein molecules seem to trigger microglial cells. This substance may send a signal through the vagus nerve or penetrate it completely through the bloodstream. �
Inflammation and Parkinson’s Disease
According to several research studies, inflammation caused by an abnormal gut microbiome may also cause the development of Parkinson’s disease. In one research study, Inga Peter, a genetic epidemiologist at the Icahn School of Medicine at Mount Sinai, and her colleagues analyzed the relationship between inflammatory bowel syndrome (IBS) and Parkinson’s disease. The analysis compared 144,018 participants with ulcerative colitis or Crohn’s disease and 720,090 healthy controls where PD was 28 percent higher in people with IBS than in those in the control group, supporting previous research study findings. �
Inflammation is believed to increase the risk of developing Parkinson’s disease because it may increase alpha-synuclein as well as increase intestinal and blood-brain barrier (BBB) permeability. Inflammation may also increase cytokines, molecules which can increase inflammation in the body. Moreover, an abnormal gut microbiome can also cause inflammation. However, because not all patients with Parkinson’s disease will have inflammatory bowel syndrome or any other gut health issues, further evidence is still required to determine how the gut-brain connection can ultimately be associated with PD. �
If this is indeed true, however, it will allow scientists to develop new interventions for the treatment of Parkinson’s disease that targets the gut instead of the brain. Several research studies have already started to analyze the effects of these new interventions. In 2015, Michael Zasloff and his colleagues started a company, known as Enterin, which is currently testing a substance that decreases the development of alpha-synuclein molecules in the gastrointestinal (GI) tract. Although the treatment is intended to reduce constipation, the scientists hope that they will be able to prevent or even restore the effects of PD. �
Although many research studies and evidence support the hypothesis that Parkinson�s disease may be much closely associated with the gut-brain axis than we thought, the question of how early the digestive system changes may occur is still unknown. Furthermore, other scientists still suggest that PD may start elsewhere in the body. �I believe that there�s possibly various sites of origin for Parkinson�s disease,� stated Viviane Labrie, a neuroscientist at the Van Andel Research Institute in Michigan. �For several people, it might be the gut while for several people, it might simply be something that occurs in the brain.�
�
Parkinson’s disease (PD) is a movement disorder that affects the central nervous system. PD can cause various, well-known symptoms, including tremors, slowed movements, stiffness, and loss of balance, among others. Research studies have demonstrated that nerve cell damage in the brain can decrease dopamine, a neurotransmitter and/or hormone, that can cause Parkinson’s disease. However, scientists have found that the gut-brain connection may ultimately be associated with PD. Inflammation caused by an abnormal gut microbiome as well as gut health issues like irritable bowel syndrome (IBS) is also believed to be one of the main factors for PD associated with the gut-brain connection.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Johns Hopkins University School of Medicine. �New Research Shows Parkinson’s Disease Origins in the Gut.� Medical Xpress – Medical Research Advances and Health News, Medical Xpress, 26 June 2019, medicalxpress.com/news/2019-06-parkinson-disease-gut.html.
CureParkinsonsTrust. �New Evidence Suggests Parkinson’s Might Not Start in The Brain.� The Cure Parkinson’s Trust, 28 Nov. 2019, www.cureparkinsons.org.uk/news/parkinsons-starts-in-gut.
Kwon, Diana. �Does Parkinson’s Begin in the Gut?� Scientific American, Scientific American, 8 May 2018, www.scientificamerican.com/article/does-parkinsons-begin-in-the-gut/.
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
� XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
�
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparallel experience at the National University of Health Sciences to be able to help restore the natural integrity of the patient and define the future of modern integrated medicine. �
Waking up tired even after getting six or more hours of sleep?
Under a high amount of stress?
If you are experiencing any of these situations, then it might be due to your melatonin and cortisol levels affecting your body and circadian rhythm.
Across the world, millions of people have trouble sleeping. In the United States, there are roughly about 50-70 million people who have a poor quality of sleep. When a person has slept for less than eight hours, they become tired, and many problems can come to them, especially if their lives are hectic. With a hectic lifestyle and poor sleep, it can cause the body to have low energy to get any task done, the cortisol stress hormone will be raised, and diseases like high blood pressure and diabetes can cause problems that can be chronic if it is not treated.
In functional endocrinology, melatonin and cortisol are hormones that the body produces naturally. The cortisol hormone or the stress hormone helps the body be in a state of “fight or flight” mode, which can be a good thing for anyone who is doing a project or going for a job interview. Although when cortisol hormone levels are high, it can lead the body to have complications like inflammation, chronic oxidative stress, and high blood pressure.
The Melatonin Circadian Rhythm
With the melatonin hormone, this hormone tells the body when it is time to sleep. Sometimes though, people do have a hard time sleeping, and taking melatonin supplements can actually relax the body and thus making the person fall asleep. Since the pineal gland produces melatonin from the brain, it can also be found in the eyes, the bone marrow, and the gut to relax the body and making the person fall asleep naturally. Some studies show that the circadian rhythm of the pineal gland that is producing melatonin. By doing this, the research shows that the administration of melatonin can:
One: induce sleep on individuals who have trouble falling asleep.
Two: inhibits the body to wake up naturally from the circadian pacemaker.
Three: shift the circadian biological clocks to increase sleep intake when a person is trying to sleep at an earlier time to get the full eight-hour benefits of sleep.
When a person is working at a 9 to 5 job, they are rising with their bodies and relaxing their bodies after a hard day at work. Studies found out that the melatonin and cortisol hormones help regulate the 24-hour pattern of the body’s function and responses tremendously. With the body’s hormone production cycle, it can be disturbed if the person is staying awake late at night or sleeping during the day. When this happens, the person can get disruptive disorders like mood swings, dizziness, be irritable and depressed, and have metabolic disorders. Not only that, but the body’s immune system and its endocrine system can also be damaged as well, causing the body to be a host to infections and diseases.
There have been more studies on the circadian rhythms in the body, as the studies show how people who work in the night shift have been associated with a vast number of adverse health problems that attack the cardiovascular and gastrointestinal system as well as disturbing the metabolic system. Anyone who has worked the night shift has to change their sleep schedule and adapt to the rapid reorientation in their sleep/wake schedule to go to work and do their job. Since everyone is working at a shift schedule, it can be stressful and can affect a worker’s body performance as well as affecting melatonin and cortisol secretion.
Ways To Support Cortisol and Melatonin
Surprisingly though, there are ways to lower cortisol levels and make sure that melatonin levels are working correctly for the body to function. For cortisol levels to be lowered, a person should do meditative practices, find an enjoyable hobby, and, most importantly, try deep breathing exercises to relax the body from unwanted stress. With deep breathing exercises, it can help the body to release any tension that a person is holding, and the muscles in the body began to relax, and the blood starts to flow. With the melatonin levels, they work together with the body’s circadian rhythm and make sure the body knows when it is time to wake up, sleep and eat. The melatonin hormone can also help regulate the body’s temperature, blood pressure, and hormone levels to make sure it is functioning correctly. When there are high levels of these systems, it can cause the body to develop chronic illnesses and harm the body in the process.
Research shows that melatonin hormones can bind to neurological receptors in the body, thus promoting relaxation. Since melatonin binds to neurological receptors, it can also reduce nerve activity and dopamine levels to make the eyes heavy, thus making the person fall asleep.
Conclusion
With the body being able to naturally produce melatonin and cortisol levels to make sure that the body does not get overly stressed throughout the entire day. Since melatonin is partnered with the body’s circadian rhythm, the body knows when to stay up and fall asleep. Since everyone has a hectic schedule, it is essential to take time and relax and get on a healthy sleep schedule so the body can be healthy and functioning. Some products are here to make sure that the endocrine system is functioning properly and supporting the adrenal glands and sugar metabolism.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Cajochen, C, et al. �Role of Melatonin in the Regulation of Human Circadian Rhythms and Sleep.� Journal of Neuroendocrinology, U.S. National Library of Medicine, Apr. 2003, www.ncbi.nlm.nih.gov/pubmed/12622846.
James, Francine O, et al. �Circadian Rhythms of Melatonin, Cortisol, and Clock Gene Expression during Simulated Night Shift Work.� Sleep, Associated Professional Sleep Societies, LLC, Nov. 2007, www.ncbi.nlm.nih.gov/pmc/articles/PMC2082093/.
Monteleone, P, et al. �Temporal Relationship between Melatonin and Cortisol Responses to Nighttime Physical Stress in Humans.� Psychoneuroendocrinology, U.S. National Library of Medicine, 1992, www.ncbi.nlm.nih.gov/pubmed/1609019.
Raman, Ryan. �How Melatonin Can Help You Sleep and Feel Better.� Healthline, Healthline Media, 3 Sept. 2017, www.healthline.com/nutrition/melatonin-and-sleep.
Zamanian, Zahra, et al. �Outline of Changes in Cortisol and Melatonin Circadian Rhythms in the Security Guards of Shiraz University of Medical Sciences.� International Journal of Preventive Medicine, Medknow Publications & Media Pvt Ltd, July 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3775223/.
By informing individuals about how the National University of Health Sciences provides knowledge for future generations who want to make a difference in the world. The University offers a wide variety of medical professions for functional and integrative medicine.
If you are experiencing any of these situations, then your collagen peptides might be low.
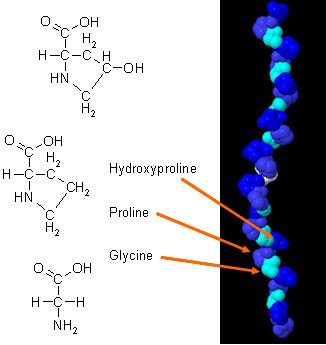
There have been new studies on how collagen can improve body composition when it is combined with daily exercises. Collagen in the body has a unique amino acid composition that plays an essential role in the body’s anatomy. Collagen protein is a concentrated source of glycine, proline, and hydroxyproline, and when it is being compared to all the other dietary proteins, it makes collagen a potential practical choice as a structural protein.
In a 2015 study, researchers have demonstrated how efficient collagen supplements can improve body composition in active males. The results show how each male individuals are participating in weight training at least three times a week and have to supplement with at least 15 grams of collagen peptides to achieve maximum health. The assessments that the test provide are strength test, bioimpedance analysis (BIA), and muscle biopsies. These tests make sure that the male individuals are performing well after taking the collagen supplements, and the results show how their body mass had an increase of fat-free body mass. Another study showed how collagen protein supplementation when it is combined with resistance training that can increase muscle mass and muscle strength with the elderly as well as people with sarcopenia.
Beneficial Properties With Collagen
There are many beneficial properties that collagen supplements can provide to the body when it is consumed. There are hydrolyzed collagen and gelatin and can help improve a person’s skin structure. Even though there are not many studies on collagen supplements, there are excellent promises for the areas on the body. They are:
Muscles mass: Collagen supplements, when combined with strength training, can increase muscle mass and strength in the body.
Arthritis: Collagen supplements can help people with osteoarthritis. Studies show that when people osteoarthritis take collagen supplements, they discovered a massive decline in the pain they were experiencing.
Skin elasticity: In a 2014 study, it stated that women who took collagen supplements and has shown improvements in skin elasticity. Collagen can also be used in topical treatments to help improve the appearance of a person�s skin by minimizing fine lines and wrinkles.
Not only collagen supplements provide beneficial properties to the specific areas on the body, but there are the four main types of collagen and what is their roles in the human body as well as their functions:
Type 1: Type 1 collagen took account of 90% of the body’s collagen and made up of densely packed fibers that provide structures to the skin, bones, connective tissues, and teeth that are in the body.
Type 2: Type 2 collagen is made up of loosely packed fibers that are found in the elastic cartilage, which helps cushion the joints in the body.
Type 3: Type 3 collagen helps support the structure of the muscles, organs, and arteries that make sure that the body is functioning correctly.
Type 4: Type 4 collagen is found in the layers of everyone�s skin and helps with the filtration in the body.
Since these four types of collagen are in the body, it is essential to know that collagen can naturally decrease over time with age since the body will produce a lesser lower quality of collagen. One of the visible signs of decrease collagen is when the skin on the human body becomes less firm and supple as well as weaken cartilage due to aging.
Factors That Can Damage Collagen
Even though collagen can decrease naturally with age, many factors can destroy collagens that are harmful to the skin. The harmful factors can include:
Sugar and Carbs: Refined sugars and carb can interfere with collagen�s ability to repair itself on the skin. So by minimizing sugar and carb consumption in the body, it can reduce the effects of vascular, renal, and cutaneous tissue dysfunction.
Sun Exposure: Even though getting enough sun can help a person enjoy the day, however, being exposed to the sun for an extended period can cause damaged to the skin and destroy collagen peptides. The effects of overexposure of the sun can cause the skin to photo age and produce oxidative stress in the body.
Smoking: When a person smokes, it can reduce collagen production in the body, causing the body to have premature wrinkles, and if the body is wounded, the healing process will be slower and can lead to ailments in the body.
Autoimmune Diseases: Some autoimmune diseases can also damage collagen production like lupus.
Conclusion
Collagen is vital for the body as it helps the skin be gentle and firm. Naturally, it will decrease as a person gets older, so taking collagen supplements can make sure that the body can function correctly. When harmful factors are affecting the body, they can stop or even damage collagen production and accelerate the process of premature wrinkles from forming, making a person look older than they are. Some products can help the body’s cellular activity by providing more excellent stability, bioavailability, and digestive comfort.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Bosch, Ricardo, et al. �Mechanisms of Photoaging and Cutaneous Photocarcinogenesis, and Photoprotective Strategies with Phytochemicals.� Antioxidants (Basel, Switzerland), MDPI, 26 Mar. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4665475/.
Danby, F William. �Nutrition and Aging Skin: Sugar and Glycation.� Clinics in Dermatology, U.S. National Library of Medicine, 2010, www.ncbi.nlm.nih.gov/pubmed/20620757.
Jennings, Kerri-Ann. � Collagen – What Is It and What Is It Good For?� Healthline, 9 Sept. 2016, www.healthline.com/nutrition/collagen.
Jurgelewicz, Michael. �New Study Demonstrates the Benefits of Collagen Peptides for Improving Body Composition Combined with Exercise.� Designs for Health, 31 May 2019, blog.designsforhealth.com/node/1031.
Knuutinen, A, et al. �Smoking Affects Collagen Synthesis and Extracellular Matrix Turnover in Human Skin.� The British Journal of Dermatology, U.S. National Library of Medicine, Apr. 2002, www.ncbi.nlm.nih.gov/pubmed/11966688.
Proksch, E, et al. �Oral Supplementation of Specific Collagen Peptides Has Beneficial Effects on Human Skin Physiology: a Double-Blind, Placebo-Controlled Study.� Skin Pharmacology and Physiology, U.S. National Library of Medicine, 2014, www.ncbi.nlm.nih.gov/pubmed/23949208.
Schauss, Alexander G, et al. �Effect of the Novel Low Molecular Weight Hydrolyzed Chicken Sternal Cartilage Extract, BioCell Collagen, on Improving Osteoarthritis-Related Symptoms: a Randomized, Double-Blind, Placebo-Controlled Trial.� Journal of Agricultural and Food Chemistry, U.S. National Library of Medicine, 25 Apr. 2012, www.ncbi.nlm.nih.gov/pubmed/22486722.
Zdzieblik, Denise, et al. �Collagen Peptide Supplementation in Combination with Resistance Training Improves Body Composition and Increases Muscle Strength in Elderly Sarcopenic Men: a Randomised Controlled Trial.� The British Journal of Nutrition, Cambridge University Press, 28 Oct. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4594048/.
By informing individuals about how the National University of Health Sciences provides the knowledge for future generations, the University offers a wide variety of medical professions for functional medicine.
Movement disorders are health issues that can cause abnormal and involuntary body movements. Many common movement disorders are frequently caused by problems in the transmission signals of the brain and they can ultimately affect quality, fluency, speed, and ease of movement. Movement disorders are also referred to as conversion disorders and/or psychogenic movement disorders. Damage, injuries or underlying conditions of the brain, spinal cord, and nervous system don’t necessarily cause movement disorders. We will discuss the most common movement disorders, including: �
Tremor: also known as an essential tremor or a resting tremor.
Ataxia: characterized by “jerky” movements and coordination problems.
Dystonia: characterized by abnormal, involuntary, and prolonged muscle contractions.
Huntington’s disease: also known as chronic progressive chorea.
Parkinson’s disease: one of the most “well-known” movement disorders, associated with tremor.
Multiple system atrophies: also known as Shy-Drager syndrome.
Myoclonus: characterized by rapid, brief, and irregular movements.
Tourette’s syndrome: another “well-known” movement disorder, associated with repetitive or unwanted sounds and movements.
Wilson’s disease: also known as an inherited health issue, associated with common symptoms and liver disease.
Progressive supranuclear palsy: also known as a rare health issue that affects movement.
Tremor
Tremor is a common movement disorder that is characterized by abnormal and/or involuntary shaking or “trembling”. It can generally affect single or multiple limbs and it can also frequently worsen with simple movements. Tremor affects approximately five million people in the United States. According to the U.S. National Library of Medicine, tremors most commonly develop in older adults, specifically in those over 65 years of age. It is commonly caused by problems in the regions of the brain that regulate and manage movement. Tremor is not associated with damage, injury, or an underlying condition.
Ataxia
Ataxia is a well-known movement disorder that affects the brain and/or spinal cord. Ataxia can cause common symptoms, such as instability, imbalance, clumsiness, tremor, and/or a lack of coordination. Normal movements associated with ataxia generally aren’t smooth and they may appear to be “jerky” or disjointed. People with ataxia may also fall down frequently due to an unsteady gait or walking cycle. Ataxia also can affect speech and eye movement.
Dystonia
Dystonia is a common movement disorder that is characterized by abnormal and/or involuntary muscle spasms. Dystonia is caused by basal ganglia dysfunction, a region of the brain that regulates and manages movement coordination to control the fluency and speed of movement and avoid unwanted movement. Dystonia can cause common symptoms, such as repetitive, abnormal and/or involuntary movements of any part of the body. General dystonia can ultimately affect the whole body while focal dystonias can ultimately affect a single area of the body, most commonly affecting the neck, known as spasmodic torticollis, eyelids, known as blepharospasm, lower face, known as Meige syndrome, or hand, known as writer’s cramp or limb dystonia.
Huntington’s Disease
Huntington’s disease is another well-known movement disorder that gradually deteriorates the brain cells. It can also often be fatal. Huntington’s disease affects approximately one in every 10,000 people in the United States and generally develops between 35 and 50 years of age, progressing without remission through 10 to 25 years. A juvenile form of the movement disorder affects approximately 16 percent of all cases and generally develops in people less than 20 years of age. Huntington’s disease can cause common symptoms, such as jerky, abnormal and/or involuntary movements of the face, limbs, and trunk, gradual brain dysfunction as well as mental health issues. Moreover, Huntington’s disease is well-known as a hereditary movement disorder.
Parkinson’s Disease
Parkinson’s disease is another commonly well-known movement disorder caused by the deterioration of the brain cells in the area, known as the substantia nigra, that regulates and manages movement. The brain cells can become damaged and die, ultimately affecting their capability to create an essential substance known as dopamine. Parkinson’s disease can cause common symptoms, such as tremor, muscle stiffness, gradual loss of movement, gradual brain dysfunction, decreased facial expressions and/or voice changes, decreased blinking, swallowing frequency, and drooling, a stooped, flexed posture, unsteady gait or walking cycle, mental health issues, and/or dementia. According to the Parkinson’s Disease Foundation, approximately 60,000 new cases of Parkinson’s disease are diagnosed each year. Approximately four percent of people with Parkinson’s disease are diagnosed before 50 years of age.
Multiple System Atrophies (MSA)
Multiple system atrophies (MSA) are gradual movement disorders that can affect blood pressure, movement, and other structures and functions. Because of the different ranges of symptoms, MSAs were initially characterized as three different health issues, including Shy-Drager syndrome, striatonigral degeneration, and olivopontocerebellar atrophy. All of these health issues are currently characterized as MSA. Common symptoms include stiffness, slowed movements, instability, loss of balance, loss of coordination, a considerable decrease in blood pressure associated with dizziness, lightheadedness, fainting or blurred vision, known as orthostatic hypotension, male impotence, urinary problems, constipation, as well as speech and swallowing difficulties.
Myoclonus
Myoclonus is a common movement disorder characterized by abnormal or involuntary twitching or muscle spasms. There are several different forms of myoclonus. Cortical myoclonus develops in a region of the brain known as the sensorimotor cortex and it may be caused by a variety of health issues. Subcortical myoclonus affects various muscle groups and may be caused by unusually low levels of oxygen in the brain, known as hypoxia, or by a metabolic process, such as liver or kidney failure. Spinal myoclonus may be caused by damage, injury, or an underlying condition of the spine, such as multiple sclerosis, syringomyelia, ischemic myelopathy or an infection like herpes zoster, Lyme disease, E. coli or HIV. Peripheral myoclonus may be caused by the compression of a facial nerve or it may occur for no apparent reason. Furthermore, several other health issues associated with myoclonus can ultimately include celiac disease, Angelman syndrome, Huntington’s disease, Rett syndrome, Creutzfeldt-Jakob disease, and Alzheimer’s disease.
Tourette’s Syndrome
Tourette Syndrome is a hereditary movement disorder characterized by repetitive, abnormal, and/or involuntary movements and sounds known as tics. This health issue commonly develops between six and 15 years of age, however, it may develop as early as two years of age or as late as 20 years of age. Common symptoms include abnormal and/or involuntary movements of the face and body. Tics are generally frequent, repetitive, and quick. Verbal tics, known as vocalizations, generally occur with the movements and/or may replace single or multiple movement tics. Vocalizations can include grunting, throat clearing, and shouting, among others. Verbal tics may also include the abnormal and/or involuntary utilization of obscene, socially unacceptable words and phrases, known as coprolalia,� as well as obscene gestures, known as copropraxia. Tics disappear in about 70 percent of cases.
Wilson’s Disease
Wilson’s Disease is a common movement disorder that causes excess copper to accumulate in the brain or liver. Although copper can accumulate since birth, common symptoms can develop between six and 40 years of age. Wilson’s Disease affects approximately one in 30,000 people in the world. Wilson’s disease is also associated with mental health issues as well as liver disease. Other common symptoms can include jaundice, abdominal pain and swelling, vomiting, tremor as well as walking, talking or swallowing difficulties, suicidal or homicidal behavior, depression, and aggression, among others.
Progressive Supranuclear Palsy (PSP)
Progressive supranuclear palsy (PSP) is a rare but well-known movement disorder that causes gradual loss of certain brain cells, slowed movement, and balance, walking, swallowing, speech and eye movement difficulties. It may also affect cognition and personality, causing emotional outbursts and a decrease in intellectual capabilities. PSP commonly affects people between 40 to 60 years of age and it can generally run its full terminal course throughout six to 10 years. PSP is occasionally misdiagnosed as Parkinson’s disease because the symptoms are very similar. Although the cause of PSP is unknown, healthcare professionals understand that a protein, known as tau, can accumulate in unusual clumps in certain brain cells of people with PSP.
Common movement disorders are characterized as health issues that can cause common symptoms, such as abnormal and involuntary movements. Common movement disorders, such as Parkinson’s disease, tremor, ataxia, and dystonia, among others, are caused by problems in the transmitting signals of the brain and they can ultimately affect quality, fluency, speed, and ease of movement. Common movement disorders are also frequently referred to as conversion disorders and/or psychogenic movement disorders. In the following article, we discussed several of the most common movement disorders. Understanding common movement disorders and their common symptoms is fundamental for diagnosis and treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Movement disorders are health issues that can cause abnormal and involuntary body movements. Many common movement disorders are frequently caused by problems in the transmission signals of the brain and they can ultimately affect quality, fluency, speed, and ease of movement. Movement disorders are also referred to as conversion disorders and/or psychogenic movement disorders. Damage, injuries or underlying conditions of the brain, spinal cord, and nervous system don’t necessarily cause movement disorders. In the article above, we discussed the most common movement disorders.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
Stanford Health Care (SHC) – Stanford Medical Center. �Functional Movement Disorders.� Stanford Health Care (SHC) – Stanford Medical Center, stanfordhealthcare.org/medical-conditions/brain-and-nerves/functional-movement-disorders.html.
Swierzewski, Stanley J. �Movement Disorders Overview.� Movement Disorders Overview – Movement Disorders – HealthCommunities.com, 1 Jan. 2000, www.healthcommunities.com/movement-disorders/overview-of-movement-disorders.shtml.
[wp-embedder-pack width=”100%” height=”1050px” download=”all” download-text=”” attachment_id=”52657″ /]
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download* All of the above XYMOGEN policies remain strictly in force.
Stomach pain, burning, or aching 1-4 hours after eating?
Is waist girth equal to or larger than hip girth?
Tired/sluggish?
Mental sluggish?
If you are experiencing any of these situations, then try to detox your body for the new year as part of your resolutions.
With the start of the new year comes the numerous ads on T.V. for detox programs and cleanses that will help people who are trying to get healthier as their new year�s resolution. The detox programs and cleanses that are shown as commercials and online ads will make anyone believe that lemon water, apple cider vinegar, and green juices can help detox the body and boost the metabolism. Even though these detox programs and cleanses are alluring and may reel in unsuspected individuals. The truth is that the endocrine system helps the body runs its detoxification process all day with natural, efficient, and effective essential nutrients that are critical for each of the endocrine functions.
Naturally Detox Foods and Nutrients
If someone enjoys eating superfruits like goji or a�ai berries, there is nothing wrong with that because these berries have antioxidant properties for the body. Studies show that animal foods such as beef, pork, poultry, and many other animal products have contributed vital amino acids for liver detoxification and provide a rich source of sulfur that the body needs. With many commercial detox programs and �cleanses� that claims that it will temporarily eliminate the animal protein, however, this is not a requirement for a healthy detox. Any plant foods from the cruciferous and allium families are beneficial and crucial for the body due to sulfation via sulfotransferase enzymes for phase 2 detoxification.
There is also something else that plays a critical role in the biotransformation and detoxification of harmful compounds out of the body is none other than glutathione. Since glutathione is called the “master antioxidant,” it is a tripeptide, which is a molecule that is made up of three amino acids. Research shows that any foods can provide nutrients to help support glutathione production, especially a large proportion of animal foods like beef, pork, eggs, turkey, chicken, and lamb can provide nutrients for the body. With these nutrients contributing to the body, some of them are not found exclusively, even though they are strongly being represented but are being underscored. It is not necessary to eliminate animal foods; a person can still eat both plant foods and animal foods to help support healthy detoxification for the body.
Kidney Detoxification
Surprisingly, detoxing is not always about the liver. The kidneys need to detox as well since they are the liver�s assistants in the detoxification process of harmful toxins in the body. Since the liver can convert the fat-soluble toxins into water-soluble compounds, it makes it easier for the body to excrete the urine out of the body easily as the kidneys are regulating the detoxification.
The kidneys may be small, but they are very hardworking organs that are less than 0.5% of the body mass. In a healthy body, the filtration rate for the kidneys is about 150 quarts of blood daily. According to the information given by the National Kidney Foundation, it states that when there is frequent dehydration, it can lead to permanent kidney damage. By staying hydrated, this can prevent bad kidney function from happening and eliminating the harmful toxins out of the body.
Although this does not mean that a person should be guzzling water every day, even though it is recommended for a person to drink six to eight glasses of water, a day turns out to be a myth. In general, it is fine to use thirst as a reminder to drink water and to consume coffee and tea even counts even though there are diuretics. The research found in the Mayo Clinic found out that any foods like iceberg lettuce and cucumbers have high water content and can contribute to total water intake.
Sleep Is Very Important
Regarding detoxification, sleep is something that does not get too much attention. With the body trying to detoxify throughout the entire day, some factors can upregulate during the sleep period. Studies show that sleep or even a quick power nap is universal to all humans and animals. Not everyone exactly knows why sleep is essential, but there are many possibilities that when a person is sleeping, it is time for the brain to do a bit of cleaning for the body. This is because the brain has an easier time to process everything when the individual is not awake, and their attention is not on a hundred different things.
A recent discovery has found that the brain has a unique system called the glymphatic system, and that system is activated when a person is asleep. The glymphatic system can also clear beta-amyloid, which is the potential harmful protein that is associated with Alzheimer’s disease. Studies even show that the glymphatic system can clear beta-amyloid twice as effective when a person is sleeping than when they are awake. If a person wants to have a healthier year, then they should be aware of the importance of good quality sleep.
Conclusion
So for the new year, adding these detoxifying methods can help boost the body system and promote wellness. By adding nutritious foods that are filled with antioxidants and detoxifying properties that are beneficial to the body, getting enough sleep and staying hydrated is highly crucial for healthy body detoxification. Some products have advance detoxification properties that can help support the immune system and are designed for greater stability bioavailability, and digestive comfort for the body.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Publishing, Harvard Health. �The Dubious Practice of Detox.� Harvard Health, 2008, www.health.harvard.edu/staying-healthy/the-dubious-practice-of-detox.
Hodges, Romilly E, and Deanna M Minich. �Modulation of Metabolic Detoxification Pathways Using Foods and Food-Derived Components: A Scientific Review with Clinical Application.� Journal of Nutrition and Metabolism, Hindawi Publishing Corporation, 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4488002/.
Jessen, Nadia Aalling, et al. �The Glymphatic System: A Beginner’s Guide.� Neurochemical Research, U.S. National Library of Medicine, Dec. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4636982/.
Labos, Christopher. �The Water Myth.� Office for Science and Society, 14 Aug. 2018, www.mcgill.ca/oss/article/health-nutrition/water-myth.
Masters, M, and R A McCance. �The Sulphur Content of Foods.� The Biochemical Journal, U.S. National Library of Medicine, Aug. 1939, www.ncbi.nlm.nih.gov/pmc/articles/PMC1264524/.
Mendelsohn, Andrew R, and James W Larrick. �Sleep Facilitates Clearance of Metabolites from the Brain: Glymphatic Function in Aging and Neurodegenerative Diseases.� Rejuvenation Research, U.S. National Library of Medicine, Dec. 2013, www.ncbi.nlm.nih.gov/pubmed/24199995.
Purves, Dale. �Why Do Humans and Many Other Animals Sleep?� Neuroscience. 2nd Edition., U.S. National Library of Medicine, 1 Jan. 1970, www.ncbi.nlm.nih.gov/books/NBK11108/.
Rasmussen, Martin Kaag, et al. �The Glymphatic Pathway in Neurological Disorders.� The Lancet. Neurology, U.S. National Library of Medicine, Nov. 2018, www.ncbi.nlm.nih.gov/pubmed/30353860.
Staff, Mayo Clinic. �Water: How Much Should You Drink Every Day?� Mayo Clinic, Mayo Foundation for Medical Education and Research, 6 Sept. 2017, www.mayoclinic.org/healthy-lifestyle/nutrition-and-healthy-eating/in-depth/water/art-20044256.
Team, DFH. �A New Year Is Upon Us � It’s Detox Time!� Designs for Health, 31 Dec. 2019, blog.designsforhealth.com/node/923.
Team, NIDDKD. �Your Kidneys & How They Work.� National Institute of Diabetes and Digestive and Kidney Diseases, U.S. Department of Health and Human Services, 1 June 2018, www.niddk.nih.gov/health-information/kidney-disease/kidneys-how-they-work.
Team, NKF. �Can Dehydration Affect Your Kidneys?� National Kidney Foundation, 16 Apr. 2018, www.kidney.org/newsletter/can-dehydration-affect-your-kidneys.
Modern Integrative Wellness
By informing individuals about how the National University of Health Sciences provides the knowledge for future generations, the University offers a wide variety of medical professions for functional medicine.
Part of understanding the body and treating symptoms such as fatigue, headaches, joint pain, and overall discomfort is realizing that the body is an intricate system that functions as one. In modern medicine, we have become used to seeing different specialists for different body systems ( i.e the endocrine system, the nervous system, etc.). However, in all reality, the body is made up of all these systems to work together to maintain homeostasis.
Wellness is best defined by the National Wellness Institute as, ” An active process through which people become aware of, and make a choice toward, a more successful existence (The Six Dimensions Of Wellness)”.
In general, wellness is applied in one’s life to incorporate all aspects of health. Similar to the systems in the body, wellness is not just isolated to one part. The National Wellness Institute has promoted and defined there to be six dimensions of wellness.
Emotional
Occupational
Physical
Social
Intellectual
Spiritual
These dimensions dive deep to incorporate mental health and physical health. Mental and physical health are closely intertwined and often times relate to each other. By applying the six dimensions of wellness into your life, you are treating the body as a whole and allowing yourself to embrace the mind-body connection for optimal wellness.
Emotional:
The ability to be alone and have your own feelings and thoughts not overwhelm you, expressing emotions in a healthy way, and to be able to be compassionate towards others’ emotional state.
Occupational:�
The work you put in every day and understanding that it has a purpose and point to fulfill not only the necessary job duties but also the soul.
Physical:
The practice of regular physical activity, healthy eating/nutrition, and a regular healthy sleep schedule. These are essential elements to fuel life and heal the body.
Social:
To be able to regularly socialize and react with others. This includes interacting with people in all aspects of life and engaging in a healthy living environment.
Intellectual:
Not only referring to education, but allowing the mind to open up and connect to the lively world around.� Intellectual wellness has a main focus of creativity while exploring problem-solving and critical thinking.
Spiritual:
Knowing that there is a purpose in life that the life you are living is meaningful.
Essentially, by applying these six dimensions of wellness into everyday life, a person becomes more aware of how each dimension is connected to another and how they contribute to healthy living. Emotional health has a lot to do with mental health. By aligning emotional health with mental health, the physical health the body receives is less inflammation, a healthier gut, and more mental clarity.
Similarly speaking, occupational health has a lot to do with physical health. If the occupation one has is constantly exhausting them and causing high levels of stress, the hormones in their body will start to become off balance. This will affect their health in the way that they will not be sleeping as well, causing fatigue and the body to react with inflammation because it is not getting an adequate amount of rest to properly heal.
Physical health is important because by incorporating regular physical activity into one’s life, endorphins will be released more often. Physical activity is used to treat many mental health disorders as well as prevent many physical disabilities.
Often times, anxiety or stomach issues can be brought on by social events. Social wellness works on healthy communications with others around you while also being able to be comfortable and confident.
Intellectual wellness happens as individuals explore and connect with others. If one is not complete or working on the intellectual wellness side of things, this can cause depression and poor health due to not being stimulated and interactive.
The last dimension of wellness is spiritual.� Spiritual wellness does not mean that you believe in a specific thing, but rather that your life has a meaning and you have a purpose.
By incorporating these six dimensions, it allows the human body to connect with itself. by opening up the communication between the systems, a new level of wellness can be achieved.
The six dimensions of wellness is a more holistic approach to healthy living. These dimensions will help individuals reach their full potential while learning and acknowledging their strengths and weaknesses when it comes to health. I highly recommend incorporating the six dimensions of wellness into everyone’s life as the healing benefits it can bring are remarkable. Treating the body as a whole and realizing that your gut health is related to your brain health is eye-opening and creates a lot of room for potential healing. – Kenna Vaughn, Senior Health Coach�
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Movement disorders are characterized as health issues that cause abnormal and involuntary body positions or movements. Many neurological conditions are caused by brain signal problems and they can ultimately affect quality, fluency, speed, and ease of movement. Dyskinesia is characterized as abnormal and involuntary fluency and/or speed of movement while hyperkinesia is characterized as excessive movement and hypokinesia is characterized as slow or absent, abnormal and involuntary movements. Movement disorders are also referred to as conversion disorders and/or psychogenic movement disorders. � Injuries or underlying conditions to the brain, spinal cord, and nervous system don’t always cause movement disorders. Movement disorders can include: �
Tics, characterized as abnormal and/or involuntary contractions of the muscles,
Tremor, also referred to as a resting tremor or essential tremor,
Ataxia, characterized by “jerky” movements and coordination problems,
Dystonia, characterized as abnormal and/or involuntary, generally prolonged contractions of the muscles,
Huntington’s disease, also referred to as chronic progressive chorea,
Parkinson’s disease, a well-known movement disorder, including tremors,
Multiple system atrophies, also referred to as Shy-Drager syndrome,
Restless legs syndrome (RLS) and reflex sympathetic dystrophy/periodic limb movement disorder (RSD/PLMD),
Myoclonus, characterized by rapid, brief, irregular movements,
Tourette’s syndrome, another well-known movement disorder, including repetitive or unwanted sounds and movements,
Wilson disease, known as an inherited health issue that causes a variety of symptoms and liver disease, and
Progressive supranuclear palsy, characterized as a rare health issue that affects movement.
As previously mentioned in the list above, tics are a well-known, movement disorder characterized by abnormal and/or involuntary contractions of the muscles that can ultimately affect an individual’s regular physical activities as well as their overall quality of life. Tics are generally triggered by a powerful urge or sensation that is temporarily relieved after the contraction of the muscles. Several examples of common tics can involve the following, including: �
Twitching of the face,
Clearing of the throat,
Grunting,
Sighing,
Blinking, and/or
Shrugging of the shoulders.
Dystonia can include spasmodic torticollis, characterized by abnormal and/or involuntary movements of the eyelids, face, head, neck, and blepharospasm. � Tourette’s syndrome is another well-known movement disorder characterized as a health issue that causes a variety of vocal and motor tics or repetitive contractions of the muscles. Common symptoms of Tourette’s syndrome generally manifest during childhood and/or early adolescence and they can commonly vary in severity and frequency. Patients diagnosed with Tourette’s syndrome can also ultimately develop a variety of other behavioral problems, including inattention, hyperactivity, impulsivity, compulsions, and obsessions. A diagnosis is necessary to determine the presence of Tourette’s syndrome. �
What are the Symptoms of Movement Disorders?
Movement disorders are characterized by abnormal and involuntary movements. But, patients may also experience a variety of other symptoms, including: �
Jerky movements or twitching,
Spasms and/or contractures, characterized as limbs “freezing” in an abnormal or involuntary body position,
Tremors, characterized by abnormal or involuntary movement of a limb, can range from moderate to severe and occasional or constant, and
Gait problems, characterized as walking problems that can ultimately cause difficulty while standing or unsteady walking.
The symptoms of the movement disorders previously mentioned above can be treated. Treatment can help improve the symptoms of movement disorders. �
What are the Treatments for Movement Disorders?
Movement disorders can cause stress and ultimately affect an individual’s overall quality of life. Qualified and experienced healthcare professionals that specialize in a variety of movement disorders can help diagnose as well as develop a treatment program for every patient’s unique needs and symptoms. The goal of a doctor is to help improve the quality of life of patients with movement disorders through the use of lifestyle modifications, therapy, and medicines. According to the diagnosis, the healthcare professional will ultimately suggest treatments and possible referrals to other specialists, including: �
Referral to neurobehavioral healthcare professionals,
Physical therapy,
Chiropractic care,
Medication
Movement disorders are ultimately characterized as a variety of neurological health issues that can also generally cause various abnormal and involuntary body positions or movements. Many other neurological health issues are commonly caused by problems in the transmitting signals of the brain and they can ultimately affect quality, fluency, speed, and ease of movement. Movement disorders are also frequently referred to as conversion disorders and/or psychogenic movement disorders. Treatment of the symptoms of movement disorders will ultimately depend on the diagnosis of the patient. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Movement disorders are characterized as health issues that cause abnormal and involuntary body positions or movements. Many neurological conditions are caused by brain signal problems and they can ultimately affect quality, fluency, speed, and ease of movement. Dyskinesia is characterized as abnormal and involuntary fluency and/or speed of movement while hyperkinesia is characterized as excessive movement and hypokinesia is characterized as slow or absent, abnormal and involuntary movements. Movement disorders are also referred to as conversion disorders and/or psychogenic movement disorders. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Stanford Health Care (SHC) – Stanford Medical Center. �Functional Movement Disorders.� Stanford Health Care (SHC) – Stanford Medical Center, stanfordhealthcare.org/medical-conditions/brain-and-nerves/functional-movement-disorders.html.
Stanford Health Care (SHC) – Stanford Medical Center. �Symptoms.� Stanford Health Care (SHC) – Stanford Medical Center, stanfordhealthcare.org/medical-conditions/brain-and-nerves/functional-movement-disorders/symptoms.html.
Stanford Health Care (SHC) – Stanford Medical Center. �Treatments.� Stanford Health Care (SHC) – Stanford Medical Center, stanfordhealthcare.org/medical-conditions/brain-and-nerves/functional-movement-disorders/treatments.html.
Swierzewski, Stanley J. �Movement Disorders Overview.� Movement Disorders Overview – Movement Disorders – HealthCommunities.com, 1 Jan. 2000, www.healthcommunities.com/movement-disorders/overview-of-movement-disorders.shtml.
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine