A migraine is commonly identified by a moderate to severe throbbing pain or a pulsing sensation, usually on one side of the head, often accompanied by nausea, vomiting and extreme sensitivity to light and sound. Migraine headache pain can last for hours to even days and the symptoms can become so severe they may be disabling. Many doctors can treat varying intensities of head pain, however, the use of drugs and/or medications may only temporarily relieve the painful symptoms. Evidence-based research studies like the one described below, have determined that chiropractic spinal manipulative therapy may effectively improve migraine headaches. The purpose of the article is to educate patients on migraine headache chiropractic treatment.
A Twelve Month Clinical Trial of Chiropractic Spinal Manipulative Therapy for Migraine
Abstract
Objective: To assess the efficacy of Chiropractic spinal manipulative therapy (SMT) in the treatment of migraine.
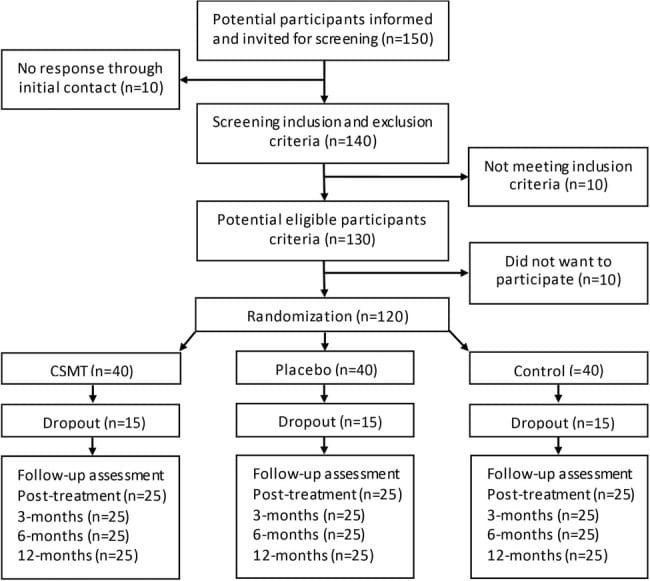
Design: A prospective clinical trial of twelve months duration. The trial consisted of 3 stages: two month pre- treatment, two month treatment, and two months post treatment. Comparison of outcomes to the initial baseline factors was made and also 6 months after the cessation of the study.
Setting: Chiropractic Research Centre of Macquarie University
Participants: Thirty two volunteers, between the ages of 20 to 65 were recruited through media advertising. The diagnosis of migraine was based on a self reported detailed questionnaire, with minimum of one migraine per month.
Interventions: Two months of chiropractic SMT at vertebral fixations determined by the practitioner, through orthopedic and chiropractic testing.
Main Outcome Measures: Participants completed diaries during the entire trial noting the frequency, intensity (visual analogue score), duration, disability, associated symptoms and use of medication for each migraine episode.
Results: The initial 32 participants showed statistically significant (p < 0.05) improvement in migraine frequency, VAS, disability, and medication use, when compared to initial baseline levels. A further assessment of outcomes after a six month follow up (based on 24 participants), continued to show statistically significant improvement in migraine frequency (p < 0.005), VAS (p < 0.01), disability (p < 0.05), and medication use (p < 0.01), when compared to initial baseline levels. In addition, information was collected regarding any changes in neck pain following chiropractic SMT. The results indicated that 14 participants (58%) reported no increase in neck pain as a consequence of the two months of SMT. Five participants (21%) reported a slight increase, three participants (13%) reported mild pain, and two participants (8%) reported moderate pain.
Conclusion: The results of this study support the hypothesis that Chiropractic SMT is an effective treatment for migraine, in some people. However, a larger controlled study is required.
The cervical spine as a cause of headache has been well described in the literature (1,2). The Headache Classification Committee of the International Headaches Society, has defined cervicogenic headache, in addition to the other types of headaches, including migraine and tension type headache (3).
However, the role of spinal conditions (especially the cervical spine) and their associated treatment for migraine does not have a well established causal relationship or clear aetiological pathway (4-7). In addition, migraine often has uncertain or overlapping diagnostic criteria thus making the role of the cervical spine as an aetiological factor even more uncertain (8,9).
Migraines are a common and debilitating conditions yet because of this uncertain aetiology, the most appropriate long term treatment has not been established (9,10). Most aetiological models relate to vascular causes of migraine, where episodes seem to be initiated by a decreased blood flow to the cerebrum followed by extracranial vasodilatation during the headache phase (11,12). However, other aetiological models seem connected with vascular changes related to neurological causes and associated serotonergic disturbances (10). Therefore, previous treatments have focused on pharmacological modification of blood flow or serotonin antagonist block (11).
This paper will evaluate the efficacy of chiropractic spinal manipulative treatment during a prospective clinical trial of twelve months duration.
Chiropractic Treatment
Chiropractic SMT is defined as a passive manual manoeuvre during which the three joint complex is carried beyond the normal physiological range of movement without exceeding the boundaries of anatomical integrity (4). SMT requires a dynamic force in a specific direction, usually with a short amplitude to correct a problem of reduced vertebral motion or positional fault. Treatment usually consists of short amplitude, high velocity spinal manipulative thrusts (diversified technique), on areas of vertebral fixation determined by a clinical history and physical examinations.
The most commonly used factors to locate vertebral fixation (denoted vertebral subluxation complex by�chiropractors) are a clinical history relating to mechanical pain patterns and medical details to excluded possible non- mechanical causes (4). These findings would then be confirmed by a thorough physical examination, by assessing which tests/signs (orthopaedic and chiropractic) were able to reproduce the presenting symptom (7).
Studies in effectiveness and cost-effectiveness of treatment for back pain have found significant benefit for chiropractic spinal manipulative therapy (SMT). These studies have been detailed in a previous publication by this author on chiropractic in the workers compensation system (13). In addition, numerous studies have identified improvement in neck pain and headache following chiropractic SMT (4,7,14-17).
This paper will test an hypothesis that spinal conditions appear to contribute to the aetiology and morbidity of migraine.
Methodology
The study was twelve month prospective clinical trial which involved 32 subjects who received a two month course of chiropractic SMT. Treatment consisted of short amplitude, high velocity spinal manipulative thrusts (chiropractic adjustive technique), on areas of vertebral subluxation determined by the physical examination.
Participants were recruited via the radio and newspapers in the Sydney region. Applicants completed a previously reported questionnaires, and were selected according to responses in the following symptoms. The participants needed to a minimum of 5 of the following IHS indicators: reaction to pain requiring cessation of activities, the need to seek a quiet dark area, unilateral pain located parieto- temporal, pain described as pulsating/throbbing, associated symptoms of nausea &/or vomiting, photophobia &/or phonophobia, migraine aggravated by head or neck movements, and a family history of migraine (3).
Inclusion was also based on participants experiencing at least one migraine a month. Exclusion was based on non- migraine indicators of a daily migraine or the initiating factor being trauma. Participants were also excluded from the study if there were contra-indications to SMT, such as meningitis or cerebral aneurysm. In addition, participants with temporal arteritis, benign intracranial hypertension or space occupying lesions were also excluded due to safety aspects.
Participants completed diaries during the initial six month trial noting the frequency, VAS, duration, disability, associated symptoms and use of medication for each migraine episode. Participants were instructed how to complete the diary which contained a table and an�instruction sheet. Participants had to note the date of the migraine, an intensity score based on a visual analogue scale, the hours the migraine lasted and the time before they could return to normal activities. In addition, participants noted associated symptoms using a letter abbreviation and they noted the type and strength of medication for each migraine episode.
Patient’s blinding was achieved by participants being informed that they may be randomly assigned to a control group which would receive a placebo (non effective) treatment. Concurrently, the practitioners were “blinded” to previous treatment results, assignment of control procedures and other outcome measures.
The first aspect of the trial was conducted over six months, and consisted of 3 stages: two months pre-treatment, two months treatment, and two months post treatment. Participants were contacted by the author a further six months after the initial trial and asked to complete another questionnaire regarding their current migraine episodes for comparison to baseline data. The follow up questionnaire sought information on the same outcome measures, as detailed in the diaries described above.
Comparison was made to initial baseline outcome measurements of migraine preceding commencement of SMT, data at the end of the two months post SMT, and to the six month follow up data. Statistical analysis involved comparing the changes of the different outcome measurements of frequency, VAS, duration, disability, and medication use throughout the trial. Statistical tests employed were a paired t test to test for significant difference between each group and a one way analysis of variance (ANOVA) to test for changes for all groups.
Dr. Alex Jimenez’s Insight
“How can chiropractic spinal manipulative therapy help manage my migraine headache pain?”�Although researchers today don’t know the definitive cause behind these complex headaches, many healthcare professionals believe migraines are often the result of an underlying issue along the cervical spine, or neck. If you suffer from migraine headache pain, chiropractic treatment can help correct spinal misalignments, or subluxations, in the cervical spine to improve the severity of the headache and decrease their frequency. It’s not necessary to rely on drugs and/or medications to relieve the painful symptoms, however, these may be used if properly directed by a healthcare professional. Rather than focusing on the head pain alone, a doctor of chiropractic will target the source of the issue and help improve your overall health and wellness.
Results
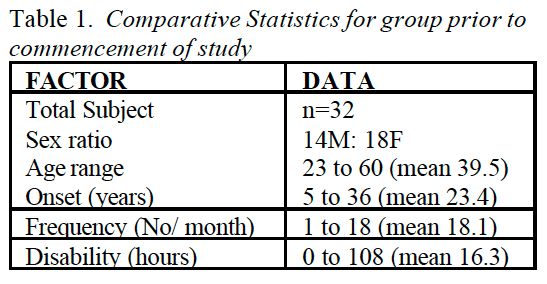
Thirty two participants, between the ages of 23 to 60, joined the study with there being 14 males and 18 females. Table 1 gives the comparative descriptive statistics for the group. The length of time the person had migraines ranged between 5 to 36 years for the group, with the average being 18.1 years. The duration of a typical migraine episode ranged between 0.75 to 108 hours for the group, with the average being 23.3 hours. The disability (length of time before the person could return to normal activities) of a typical migraine ranged between 0 to 108 hours for the group, with the average being 25.0 hours.
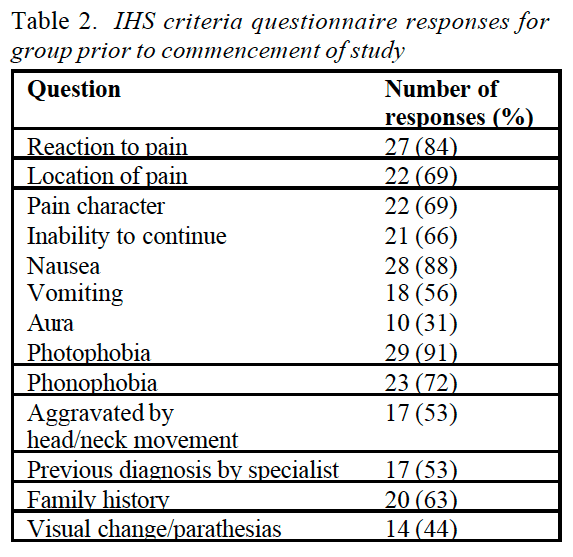
The percentage response for each of the diagnostic criteria of the IHS guidelines is detailed in table 2 (Table 2). The highest responses were for photophobia (91%), nausea (88%), reaction to pain requiring the person to seek a quiet dark area (84%), phonophobia (72%), throbbing pain characteristic (69%), parieto-temporal pain location (69%), inability to continue normal activities (66%), and family history (63%).
The IHS diagnostic criteria with the lowest responses were aura (31%), migraines aggravated by head or neck movement (53%), and vomiting (56%). A moderate number (44%) of people did not indicate aura as a feature, however, they described either homonymous visual changes or parasthesias. Therefore, the number of people experiencing migraine with aura (MA) for this group was twenty four (75%) of a total group of thirty two.
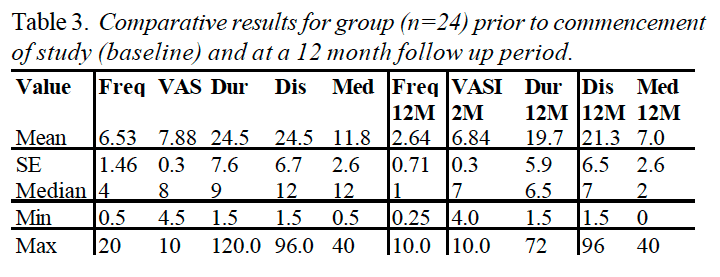
The group showed statistically significant improvement (p < 0.05) in migraine frequency, VAS, duration and disability, when compared to initial baseline levels. The frequency rates reduced by 46% for the group, severity reduced by 12%, duration reduced by 20%, disability reduced by 14% only one participant (3.1 %) reported that their migraine episodes were worse after the two months of SMT, but this was not sustained at the two month post treatment follow up period. Table 3 demonstrates variate scores in each of the six diary categories for the three phases of the trial.
From the initial thirty two participants who entered the study, four participants failed to complete the entire trial, one due to alteration in work situation, one due to a fractured ankle, one due to soreness after SMT, and one ACO�following a perceived worsening of their migraine due to chiropractic SMT. In addition, four people failed to return their six month follow up data, and were excluded from the assessment. Therefore the assessment of changes in migraine at the twelve month period was based on 24 participants. Table 4 gives the comparative statistics for this group at the end of the 12 month period.
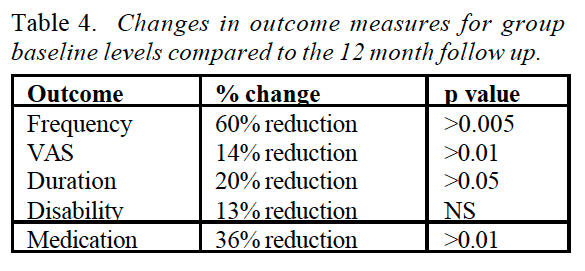
The average response at twelve months (n=24) showed statistically significant improvement in migraine frequency (p < 0.005), VAS (p < 0.01), duration (p < 0.05), and medication use (p < 0.01), when compared to initial baseline levels (Figure ????). The greatest area for improvement was with the frequency of episodes (60% reduction), and the associated severity of each migraine (14% reduction). In addition, the duration of the migraine (20% reduction) and the use of medication, reduced significantly following the SMT intervention (36% reduction). Table 3 shows mean variate scores for the three phases of the trial and statistical significance by analysis of variance (ANOVA).
Another additional result related to associated neck pain. Fourteen participants (58%) reported no increase in neck pain as a consequence of the two months of SMT. Five participants (21%) reported slight pain, three participants (13%) reported mild pain, and two participants (8%) reported moderate pain.
Discussion
The majority of participants were chronic migraine sufferers, on average they had experienced migraines for 18.1 years. However, the results have demonstrated a significant (p< 0.005) reduction in their migraine episodes and their associated disability. The mean number of migraines per month reduced from 7.6 to 2.6 episodes.
A twelve month study gives the results substantial significance because a criticism of early studies were that the length of the trial was too short to allow for the cyclical nature of migraines (18). However, the study was limited in the sample size and the fact that the trial was a pragmatic study which did not consider what aspects of chiropractic SNIT had contributed to the improvement in the migraines.
In addition, the study was limited due to the lack of a control group. However, it could be argued that participants acted as their own form of control, due to the�baseline two months data collection, especially given the fact that this group were chronic migraine sufferers.
A further limitation of this study, as with other studies of migraine or headaches was that there is substantial overlap in diagnosis and classification of migraines. The questionnaire used in this study proved to have good reliability, however, there is strong suggestion that many headache sufferers may have more than one type of headache (6-9). An advantage with the design of this study is that regardless of the exact “diagnosis” of the migraine, self reported improvement of outcome measures allow assessment of the validity of the therapy in question (4).
This study appears to confirm that there are a number of precipitating or aggravating factors involved in migraine episodes and therefore a single treatment regime may prove ineffective in the long term (4,5,9,15).
Practitioners need to be aware of the various treatment strategies and their relative advantages or limitations.
Importantly, many of the associated symptoms suffered by participants on the trial were reported to be decreased following the SMT. The associated symptoms which decreased following the trial included nausea (41% of participants felt reduction), photophobia (31 % felt reduction), vomiting (25% felt reduction), and phonophobia (25% felt reduction). Commonly reported side effects which often increase following pharmaceutical trials include nausea, vomiting, fatigue, chest pain, paraesthesia, somnolence, syncope, vertigo and less commonly atrial fibrillation. In addition, recent evidence has identified sumatriptan to be a potential cause of birth defects and myocardial infarction (19,20).
Whilst not a factor noted by the IHS, stress as either an aggravating or precipitating factor was cited by 73% of participants. In addition, 66% of people reported neck pain at the time of the migraine, with a further 31 % of people reporting upper back pain (some people noted both simultaneously).
Interestingly, five people at the end of the 12 months followup had no migraines and had decreased need for medication by 100% following chiropractic SMT. No patients reported that their migraines had increased as a result of the SMT trial.
Conclusion
The results of this study support the hypothesis that Chiropractic SMT is an effective treatment for migraine, in some people. However, due to the multifactorial nature of migraine, and the finding that episodes usually reduce following any intervention, further larger controlled study is required.
A prospective randomised controlled trial utilising detuned EPT (interferential), a sham manipulation group and an SMT group is nearing conclusion. It is anticipated this trial will provide further information of the efficacy of Chiropractic SMT in the treatment of migraine with aura.
In conclusion,�because migraine headache pain can be significantly debilitating, it’s essential for patients who suffer from this complex type of head pain to understand the effectiveness of chiropractic spinal manipulative therapy. According to the results of the research study above, migraine headache chiropractic treatment can be effectively used to as migraine treatment. Regardless of the results of the twelve month clinical trial, further research studies are still required. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Bogduk N. Cervical causes of headache and dizziness. In: Greive GP (ed) Modern manual therapy of the vertebral column. 2nd ed 1994. Churchill Livingstone, Edinburgh. p3l7-31.
2. Jull GA. Cervical Headache: a review. In: Greive GP (ed) Modem manual therapy of the vertebral column. 2nd ed 1994. Churchill Livingstone, Edinburgh. p 333-34,6
3. Headache Classification Committee of the International Headache, Society. Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalgia 1988, 9. Suppl. 7: 1-93.
4. Tuchin PJ. The efficacy of chiropractic spinal manipulative therapy (SMT) in the treatment of migraine – a pilot study. Aust Chiro & Osteo 1997; 6: 41-7.
5. Milne E. The mechanism and treatment of migraine and other disorders of cervical and postural dysfunction. Cephaigia 1989; 9, Suppi 10: 381-2.
6. Kidd R, Nelson C. Musculoskeletal dysfunction of the neck in migraine and tension headache. Headache 1993; 33: 566-9.
7. Tuchin PJ, Bonello R. Classic migraine or not classic migraine, that is the question. Aust Chiro & Osteo 1996; 5: 66-74.
8. Marcus DA. Migraine and tension type headaches: the questionable validity of current classification systems. 1992; Pain 8: 28-36.
9. Rasmussen BK, Jensen R, Schroll M, Olsen J. Interactions between migraine and tension type headaches in the general population. Arch Neurol 1992; 49: 914-8.
10. Lance JW. A concept of migraine and the search for the ideal headache drug. Headache 1990; 1: 17-23.
11. Dalassio D. The pathology of migraine. Clin J Pain 1990 6: 235-9.
12. Moskowitz MA. Basic mechanisms in vascular headache. Neurol Clin 1990; 16: 157-68
13. Tuchin PJ, Bonello R. Preliminary Findings of Analysis of Chiropractic Utilisation and Cost in the Workers Compensation System of New South Wales. J Manipulative Physiol Ther 1995; lg: 503-11.
14. Tuchin PJ, Scwafer T, Brookes M. A Case Study of Chronic Headaches. Aust Chiro & Osteo 1996; 5: 47-53.
15. Parker GB, Tupling H, Pryor DS. A Controlled Trial of Cervical Manipulation for Migraine. Aust NZ J Med 1978; 8: 585-93.
16. Young K, Dharmi M. The efficacy of cervical manipulation as opposed to pharmacological therapeutics in the treatment of migraine patients. Transactions of the Consortium for Chiropractic Research. 1987.
17. Vernon H, Steiman I, Hagino C. Cervicogenic dysfunction in muscle contraction headache and migraine: a descriptive study. J Manipulative Physiol Ther 1992; 15: 418-29
18. Parker GB, Tupling H, Pryor DS. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine. Aust NZ J Med 1980; 10: 192-8.
19. Ottervanger JP, Stricker BH. Cardiovascular adverse reactions to sumatriptan: cause for concern? CNS Drugs 1995; 3: 90-8.
20. Simmons VE, Blakeborough P. The safety profile of sumatriptan. Rev Contemp Pharmacother 1994; 5: 319-28.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Infraspinatus
Assessment of Shortness in the Infraspinatus
Infraspinatus shortness test (a) The patient is asked to reach upwards, backwards and across to touch the upper border of the opposite scapula, so producing external rotation of the humeral head. If this effort is painful infraspinatus shortness should be suspected.
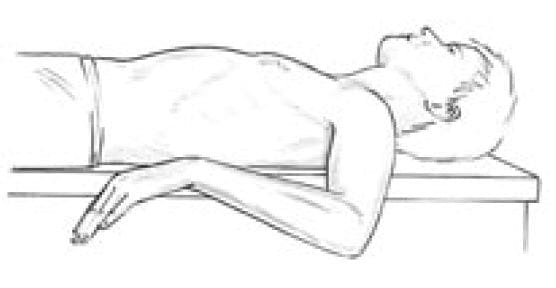
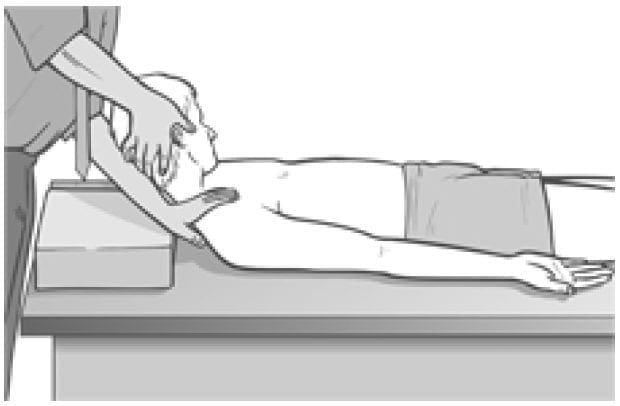
Infraspinatus shortness test (b) (see Fig. 4.37 below) Visual evidence of shortness is obtained by having the patient supine, upper arm at right angles to the trunk, elbow flexed so that lower arm is parallel with the trunk, pointing caudad with the palm downwards. This brings the arm into internal rotation and places infraspinatus at stretch. The practitioner ensures that the shoulder remains in contact with the table during this assessment by means of light compression.
Figure 4.37 Assessment and self-treatment position for infraspinatus. If the upper arm cannot rest parallel to the floor, possible shortness of infraspinatus is indicated.�If infraspinatus is short, the lower arm will not be capable of resting parallel with the floor, obliging it to point somewhat towards the ceiling.
Assessment for Infraspinatus Weakness
The patient is seated. The practitioner stands behind. The patient�s arms are flexed at the elbows and held to the side, and the practitioner provides isometric resistance to external rotation of the lower arms (externally rotating them and also the humerus at the shoulder). If this effort is painful, an indication of probable infraspinatus shortening exists.
The relative strength is also judged. If weak, the method discussed by Norris (1999) should be used to increase strength (isotonic eccentric contraction performed slowly).
NOTE: In this as in other tests for weakness there may be a better degree of cooperation if the practitioner applies the force, and the patient is asked to resist as much as possible. Force should always be built slowly and not suddenly.
MET Treatment of Infraspinatus
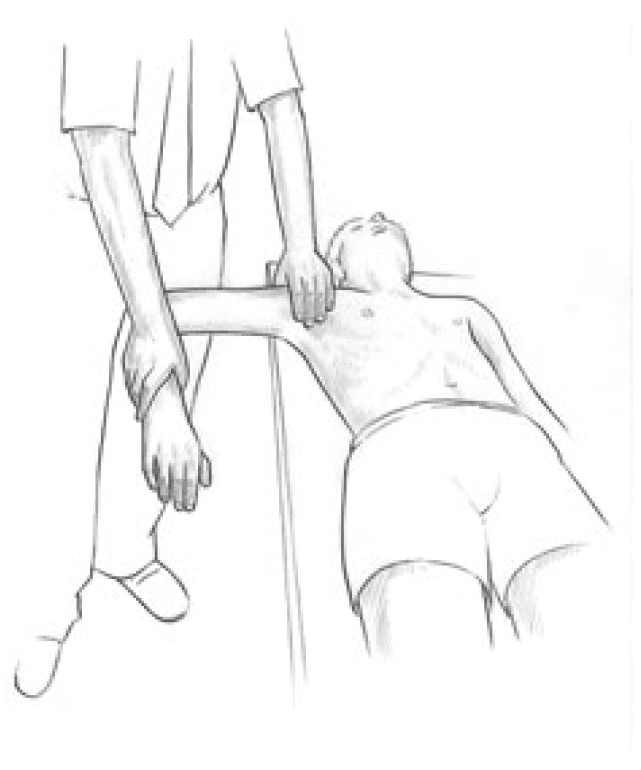
Figure 4.38 MET treatment of infraspinatus. Note that the practitioner�s left hand maintains a downward pressure to stabilise the shoulder to the table during this procedure.
The patient is supine, upper arm at right angles to the trunk, elbow flexed so that lower arm is parallel with the trunk, pointing caudad with the palm downwards. This brings the arm into internal rotation and places infraspinatus at stretch.
The practitioner ensures that the posterior shoulder remains in contact with the table by means of light compression. The patient slowly and gently lifts the dorsum of the wrist towards the ceiling, against resistance from the practitioner, for 7�10 seconds.
After this isometric contraction, on relaxation, the forearm is taken towards the floor (combined patient and practitioner action), so increasing internal rotation at the shoulder and stretching infraspinatus (mainly at its shoulder attachment).
Care needs to be taken to prevent the shoulder from rising from the table as rotation is introduced, so giving a false appearance of stretch in the muscle. In order to initiate stretch of infraspinatus at the scapular attachment, the patient is seated with the arm (flexed at the elbow) fully internally rotated and taken into full adduction across the chest. The practitioner holds the upper arm and applies sustained traction from the shoulder in order to prevent subacromial impingement.
The patient is asked to use a light (20% of strength) effort to attempt to externally rotate and abduct the arm, against resistance offered by the practitioner, for 7�10 seconds.
After this isometric contraction, and with the traction from the shoulder maintained, the arm is taken into increased internal rotation and adduction (patient and practitioner acting together) where the stretch is held for at least 20 seconds.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
A migraine is characterized as a moderate to severe headache, often accompanied by nausea and sensitivity to light and sound. Nearly 1 in 4 United States households include someone who suffers from migraine. As a matter of fact, migraine is considered to be the 3rd most prevalent condition in the world. Researchers haven’t identified a definitive cause for migraines, however, several factors are believed to trigger the complex headache pain, including a misalignment in the cervical spine. Chiropractic care is a well-known alternative treatment option used to help treat migraine headaches and improve the symptoms. The purpose of the following case study is to demonstrate the effects of chiropractic care on migraine pain management.
A Case of Chronic Migraine Remission After Chiropractic Care
Abstract
Objective: To present a case study of migraine sufferer who had a dramatic improvement after chiropractic spinal manipulative therapy (CSMT).
Clinical features: The case presented is a 72-year�old woman with a 60-year history of migraine headaches, which included nausea, vomiting, photophobia, and phonophobia.
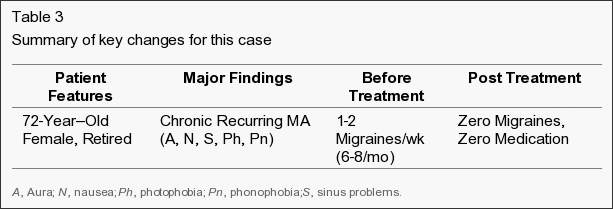
Intervention and outcome: The average frequency of migraine episodes before treatment was 1 to 2 per week, including nausea, vomiting, photophobia, and phonophobia; and the average duration of each episode was 1 to 3 days. The patient was treated with CSMT. She reported all episodes being eliminated after CSMT. The patient was certain there had been no other lifestyle changes that could have contributed to her improvement. She also noted that the use of her medication was reduced by 100%. A 7-year follow-up revealed that the person had still not had a single migraine episode in this period.
Conclusion: This case highlights that a subgroup of migraine patients may respond favorably to CSMT. While a case study does not represent significant scientific evidence, in context with other studies conducted, this study suggests that a trial of CSMT should be considered for chronic, nonresponsive migraine headache, especially if migraine patients are nonresponsive to pharmaceuticals or prefer to use other treatment methods.
Migraine remains a common and debilitating condition.[1, 2] It has an estimated incidence of 6% in males and 18% in females.[2] A study in Australia found the cost to industry to be an estimated $750 million.[3] Lipton et al found that migraine is one of the most frequent reasons for consultations with general practitioners, affecting between 12 million and 18 million people each year in the United States.[4] The estimated cost in the United States is $25 billion in lost productivity due to 156 million full-time work days being lost each year.[5] Recent information has suggested that these older figures above are still current, but also underestimated, because of many sufferers not stating their problem because of a perceived poor social stigma.[6]
The Brain Foundation in Australia notes that 23% of households contain at least one migraine sufferer. Nearly all migraine sufferers and 60% of those with tension-type headache experience reductions in social activities and work capacity. The direct and indirect costs of migraine alone would be about $1 billion per annum.[3]
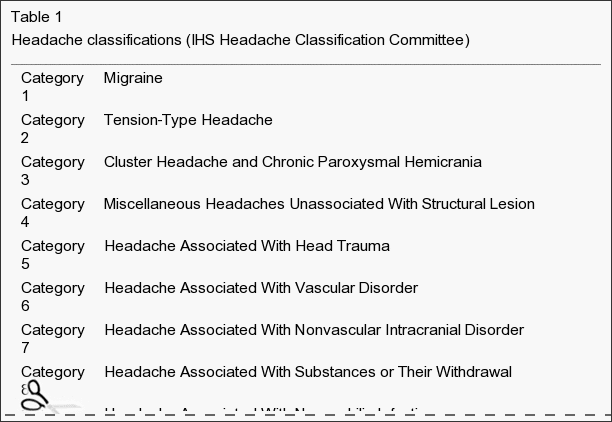
The Headache Classification Committee of the International Headache Society (IHS) defines migraines as having the following: unilateral location, pulsating quality, moderate or severe intensity, and aggravated by routine physical activity. During the headache, the person must also experience nausea and/or vomiting, photophobia, and/or phonophobia.[7] In addition, there is no suggestion either by history or by physical or neurologic examination that the person has a headache listed in groups 5 to 11 of their classification system.[7] Groups 5 to 11 of the classification system include headache associated with head trauma, vascular disorder, nonvascular intracranial disorder, substances or their withdrawal, noncephalic infection, or metabolic disorder, or with disorders of cranium, neck, eyes, nose, sinuses, teeth, mouth, or other facial or cranial structures.
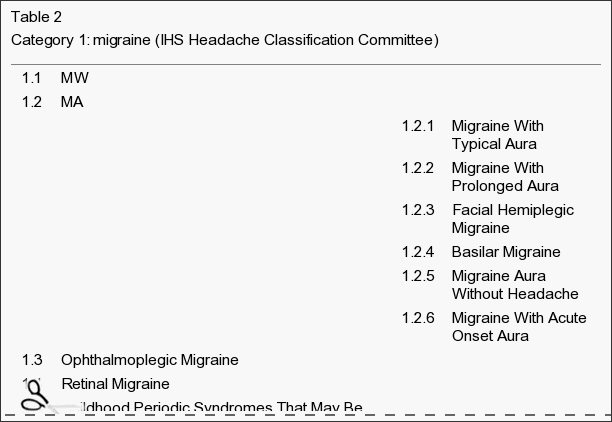
Some confusion relates to the �aura� feature that distinguishes migraine with aura (MA) and migraine without aura (MW). An aura usually consists of homonymous visual disturbances, unilateral paresthesias and/or numbness, unilateral weakness, aphasia, or unclassifiable speech difficulty.[7] Some migraineurs describe the aura as an opaque object, or a zigzag line around a cloud; even cases of tactile hallucinations have been recorded.[8] The new terms MA and MW replace the old terms classic migraine and common migraine, respectively.
The IHS diagnostic criteria for MA (category 1.2) is at least 3 of the following:
One or more fully reversible aura symptoms indicating focal cerebral cortex and/or brain stem dysfunction.
At least 1 aura symptom develops gradually over more than 4 minutes or 2 or more symptoms occurring in succession.
No aura symptom lasts more than 60 minutes.
Headache follows aura with a free interval of less than 60 minutes.
Migraine is often still nonresponsive to treatment.[9] However, several studies have demonstrated statistically significant reduction in migraines after chiropractic spinal manipulative therapy (CSMT).[10-15]
This article will discuss a patient presenting with MW and her response after CSMT. The discussion will also outline specific diagnostic criteria for migraine and other headaches relevant to chiropractors, osteopaths, or other health practitioners.
Case Report
A 72-year�old 61-kg white woman presented with migraine headaches that had commenced in early childhood (approximately 12 years old). The patient could not relate anything to the commencement of her migraines, although she believed there was a family history (father) of the condition. During the history, the patient stated that she suffered regular migraine headaches (1-2 per week) with which she also experienced nausea, vomiting, vertigo, and photophobia. She needed to cease activities to alleviate the symptoms, and she often required acetaminophen and codeine medication (25 mg) or sumatriptan succinate for pain relief. The patient was also taking verapamil (calcium ion antagonist, for essential hypertension), calcitriol (calcium uptake, for osteoporosis), pnuemenium on a daily basis, and carbamazipine (antiepileptic, neurotropic medication) twice daily.
The patient reported that an average episode lasted 1 to 3 days and that she could not perform activities of daily living for a minimum of 12 hours. In addition, a visual analogue scale score for an average episode was 8.5 out of a possible maximum score of 10, corresponding to a description of �terrible� pain. The patient noted that stress or tension would precipitate a migraine and that light and noise aggravated her condition. She described the migraine as a throbbing head pain located in the parietotemporal region and was always left-sided.
The patient had a previous history of a pulmonary embolism (2 years before treatment) and had a partial hysterectomy 4 years before treatment. She also stated she had hypertension that was controlled. She was a widow with 2 children, and she had never smoked. The patient had tried acupuncture, physiotherapy, substantial dental treatment, and numerous other medications; but nothing had changed her migraine pattern. She stated that she had never had previous chiropractic treatment. The patient also stated that she had been treated by a neurologist for �migraines� over many years.
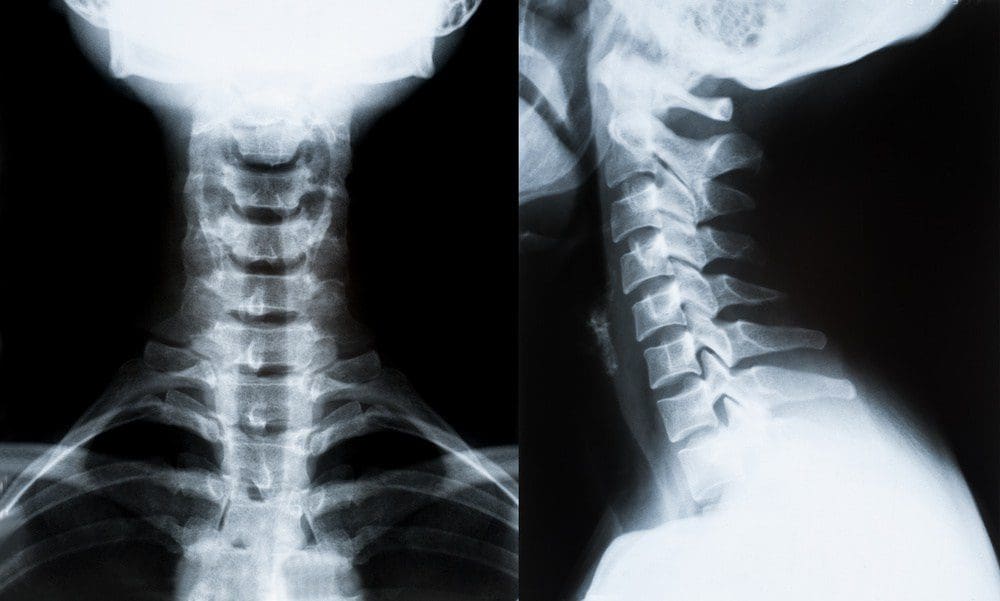
On examination, she was found to have very sensitive suboccipital and upper cervical musculature and decreased range of motion at the joint between the occiput and first cervical vertebra (Occ-C1), coupled with pain on flexion and extension of the cervical spine. She also had significant reduction in thoracic spine motion and a marked increase in her thoracic kyphosis.
Blood pressure testing revealed she was hypertensive (178/94), which the patient reported was an average result (stage 2 hypertension using the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure 7 guidelines).
Based on the IHS Headache Classification Committee classification and diagnostic criteria, the patient had an MW�category 1.1, previously called common migraine (Table 1). This appeared secondary to moderate cervical segmental dysfunction with mild to moderate suboccipital and cervical paraspinal myofibrosis.
The patient received CSMT (diversified chiropractic �adjustments�) to her Occ-C1 joint, upper thoracic spine (T2 through T7), and the affected hypertonic musculature. Hypertonic muscles were released through gentle massage and stretching. An initial course of 8 treatments was conducted at a frequency of twice a week for 4 weeks. The treatment program also included recording several features for every migraine episode. This included frequency, visual analogue scores, episode duration, medication, and time before they could return to normal activities.
The patient reported a dramatic improvement after her first treatment and noticed a reduction in the intensity of her head and neck pain. This continued with the patient reporting having no migraines in the initial month course of treatment. Further treatment was recommended to increase her range of motion, increase muscle tone, and reduce suboccipital muscle tension. In addition, monitoring of her migraine symptoms was continued. A program of treatment at a frequency of once a week for a further 8 weeks was instigated. After the next phase of treatment, the patient noted much less neck tension, better movement, and no migraine. In addition, she no longer used pain-relieving medication (acetaminophen, codeine, and sumatriptan succinate) and noted that she did not experience nausea, vomiting, photophobia, or phonophobia (Table 2). The patient continued treatment at 2-weekly intervals and stated that, after 6 months, her migraine episodes had disappeared completely. In addition, she was no longer experiencing neck pain. Examination revealed no pain on active neck movement; however, a passive motion restriction at the C1-2 motion segment was still present.
The patient is currently having treatment every 4 weeks, and she still reports no return of her migraine episodes or neck pain. The patient has now not experienced any migraines for a period of more than 7 years since her last episode, which was immediately before her having her first chiropractic treatment.
Dr. Alex Jimenez’s Insight
Migraine pain is a debilitating symptom which can be effectively managed with chiropractic care. Chiropractic treatment provides a wide selection of services which can help patients with a variety of injuries and/or conditions, including symptoms of chronic pain, limited range of motion and many other health issues. Chiropractic care can also help control stress associated with migraine. Our staff is determined to treat patients by focusing on the source of the issue rather than temporarily relieving the symptoms using drugs and/or medications. The purpose of the article is to demonstrate evidence-based results on the improvement of migraine using chiropractic care and to educate patients on the best type of treatment for their specific health issues. Chiropractic treatment offers relief from migraine pain as well as overall health and wellness.
Discussion
Case studies do not form high levels of scientific data. However, some cases do present significant findings. For example, cases with long (chronic) and/or severe symptomatology can highlight alternative treatment options. With case studies such as this, there is always a possibility that the symptoms spontaneously resolved, with no effective from the treatment. The case presented highlights a potential alternative treatment option. A 7-year follow-up revealed that the person had still not had a single migraine episode in this period. The patient was certain that there had been no other lifestyle changes that could have contributed to her improvement. She also noted that the migraines had stopped after her first treatment.
The average frequency of her migraines before treatment was 1 to 2 per week, with episodes that always included nausea, vomiting, photophobia, and phonophobia. In addition, the average duration of each episode was 1 to 3 days before her receiving CSMT. The person also noted that the use of her pain-relieving medication was also reduced by 100% (Table 3).
Table 3: Summary of key changes for this case
Migraines are a common and debilitating condition; yet because they have an uncertain etiology, the most appropriate treatment regime is often unclear.[16] Previous etiological models described vascular causes of migraine, where episodes seem to be initiated by a decreased blood flow to the cerebrum followed by extracranial vasodilation during the headache phase.[8] However, other etiological models seem connected with vascular changes related to neurologic changes and associated serotonergic disturbances.[9] Therefore, previous treatments have focused on pharmacological modification of blood flow or serotonin antagonist block.[17]
Studies examining the role of the cervical spine to headache (ie, �cervicogenic headache�) have been well described in the literature.[18-30] However, the relation of the cervical spine to migraine is less well documented.[10-15] Previous studies by this author have demonstrated an apparent reduction in migraines after CSMT.[10, 11] In addition, other studies have suggested that CSMT may be an effective intervention for migraine.[14, 15] Although, previous studies have some limitations (inaccurate diagnosis, overlapping symptoms, inadequate control groups), the level of evidence gives support for CSMT in migraine treatment.[11] However, practitioners need to be critically aware of potential overlap of diagnoses when reviewing migraine research or case studies on effectiveness of their treatment.[18-22] This is especially important in comparison of migraine patients who may be suitable for chiropractic manipulative therapy.[23-28]
Between 40% and 66% of patients with migraine, particularly those with severe or frequent migraine attacks, do not seek help from a physician.[29] Among those who do, many do not continue regular physician visits.[30] This may be due to patients’ perceived lack of empathy from the physician and a belief that physicians cannot effectively treat migraine. In a 1999 British survey, 17% of 9770 migraineurs had not consulted a physician because they believed their condition would not be taken seriously; and 8% had not seen a physician because they believed existing migraine medications were ineffective.[30] The most common reason for not seeking a physician’s advice (cited by 76% of patients) was the patients’ belief that they did not need a physician’s opinion to treat their migraine attacks.
The case was presented to assist practitioners making a more informed decision on the treatment of choice for migraines. The outcome of this case is also relevant in relation to other research that concludes that CSMT is a very effective treatment for some people. Practitioners could consider CSMT for migraine based on the following:
Limitation of passive neck movements.
Changes in neck muscle contour, texture, or response to active and passive stretching and contraction.
Abnormal tenderness of the suboccipital area.
Neck pain before or at the onset of the migraine.
Initial response to CSMT.
As with all case reports, results are limited in application to larger populations. Careful clinical decision making should be used when applying these results to other patients and clinical situations.
Conclusion
This case demonstrates that some migraine sufferers may respond well with manual therapies, which includes CSMT. Therefore, migraine patients who have not received a trial of CSMT should be encouraged to consider this treatment and assess any potential response. Where there are no contraindications to CSMT, an initial trial of treatment may be warranted. Following evidence-based medicine guidelines, medical practitioners should discuss CSMT with migraine patients as an option for treatment.[31, 32] Subsequent studies should address this issue and the role that CSMT has in migraine management.
In conclusion, migraine pain is a common condition which affects a large number of the population. Although the cause of migraines is not fully understood, treatment for the complex head pain can ultimately help manage the symptoms. Chiropractic spinal manipulative therapy, or CSMT, may improve migraine in patients and may be a valuable treatment option to consider. However, further research studies are required to demonstrate further results. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Bigal M.E., Lipton R.B., Stewart W.F. The epidemiology and impact of migraine. Curr Neurol Neurosci Rep. 2004;4(2):98�104. [PubMed]
2. Lipton R.B., Stewart W.F., Diamond M.L., Diamond S., Reed M. Prevalence and burden of migraine in the United States: data from the American Migraine Study 11. Headache. 2001;41:646�657. [PubMed]
3. Alexander L. Migraine in the workplace. Brainwaves. Australian Brain Foundation; Hawthorn, Victoria: 2003. pp. 1�4.
4. Lipton R.B., Bigal M.E. The epidemiology of migraine. Am J Med. 2005;118(Suppl 1):3S�10S. [PubMed]
5. Lipton R.B., Bigal M.E. Migraine: epidemiology, impact, and risk factors for progression. Headache. 2005;45(Suppl 1):S3�S13. [PubMed]
6. Stewart W.F., Lipton R.B. Migraine headache: epidemiology and health care utilization. Cephalalgia. 1993;13(suppl 12):41�46. [PubMed]
7. Headache Classification Committee of the International Headache, Society Classification and diagnostic criteria for headache disorders, cranial neuralgias and facial pain. Cephalgia. 2004;24(Suppl. 1):1�151. [PubMed]
8. Goadsby P.J., Lipton R.B., Ferrari M.D. Migraine�current understanding and treatment. N Engl J Med. 2002;346:257�263. [PMID 11807151] [PubMed]
9. Goadsby P.J. The scientific basis of medication choice in symptomatic migraine treatment. Can J Neurol Sci. 1999;26(suppl 3):S20�S26. [PubMed]
10. Tuchin P.J., Pollard H., Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine. J Manipulative Physiol Ther. 2000;23:91�95. [PubMed]
11. Tuchin P.J. The efficacy of chiropractic spinal manipulative therapy (SMT) in the treatment of migraine�a pilot study. Aust Chiropr Osteopath. 1997;6:41�47. [PMC free article][PubMed]
12. Tuchin P.J., Bonello R. Classic migraine or not classic migraine, that is the question. Aust Chiropr Osteopath. 1996;5:66�74. [PMC free article][PubMed]
13. Tuchin P.J., Scwafer T., Brookes M. A case study of chronic headaches. Aust Chiropr Osteopath. 1996;5:47�53. [PMC free article][PubMed]
14. Nelson C.F., Bronfort G., Evans R., Boline P., Goldsmith C., Anderson A.V. The efficacy of spinal manipulation, amitriptyline and the combination of both therapies for the prophylaxis of migraine headache. J Manipulative Physiol Ther. 1998;21:511�519. [PubMed]
15. Parker G.B., Tupling H., Pryor D.S. A controlled trial of cervical manipulation for migraine. Aust NZ J Med. 1978;8:585�593. [PubMed]
16. Dowson A.J., Lipscome S., Sender J. New guidelines for the management of migraine in primary care. Curr Med Res Opin. 2002;18:414�439. [PubMed]
17. Ferrari M.D., Roon K.I., Lipton R.B. Oral triptans (serotonin 5-HT1B/1D agonists) in acute migraine treatment: a meta-analysis of 53 trials. Lancet. 2001;358:1668�1675. [PubMed]
18. Sjasstad O., Saunte C., Hovdahl H., Breivek H., Gronback E. Cervical headache: an hypothesis. Cephalgia. 1983;3:249�256.
19. Vernon H.T. Spinal manipulation and headache of cervical origin. J Manipulative Physiol Ther. 1989;12:455�468. [PubMed]
20. Sjasstad O., Fredricksen T.A., Stolt-Nielsen A. Cervicogenic headache, C2 rhizopathy, and occipital neuralgia: a connection. Cephalgia. 1986;6:189�195. [PubMed]
21. Bogduk N. Cervical causes of headache and dizziness. In: Greive G.P., editor. Modern manual therapy of the vertebral column. 2nd ed. Edinburgh; Churchill Livingstone: 1994. pp. 317�331.
22. Jull G.A. Cervical headache: a review. In: Greive GP, editor. Modern manual therapy of the vertebral column. 2nd ed. Edinburgh; Churchill Livingstone: 1994. pp. 333�346.
23. Boline P.D., Kassak K., Bronfort G. Spinal manipulations vs. amitriptyline for the treatment of chronic tension-type headaches: a randomized clinical trial. J Manipulative Physiol Ther. 1995;18:148�154. [PubMed]
24. Vernon H., Steiman I., Hagino C. Cervicogenic dysfunction in muscle contraction headache and migraine: a descriptive study. J Manipulative Physiol Ther. 1992;15:418�429. [PubMed]
25. Kidd R., Nelson C. Musculoskeletal dysfunction of the neck in migraine and tension headache. Headache. 1993;33:566�569. [PubMed]
26. Whittingham W., Ellis W.S., Molyneux T.P. The effect of manipulation (Toggle recoil technique) for headaches with upper cervical joint dysfunction: a case study. J Manipulative Physiol Ther. 1994;17:369�375. [PubMed]
27. Jull G., Trott P., Potter H., Zito G., Shirley D., Richardson C. A randomized controlled trial of exercise and spinal manipulation for cervicogenic headache. Spine. 2002;27:1835�1843. [PubMed]
28. Bronfort G, Nilsson N, Assendelft WJJ, Bouter L, Goldsmith C, Evans R, et al. Non-invasive physical treatments for chronic headache (a Cochrane review). In: The Cochrane Library Issue 2 2003. Oxford: Update Software.
29. Dowson A., Jagger S. The UK migraine patient survey: quality of life and treatment. Curr Med Res Opin. 1999;15:241�253. [PubMed]
30. Solomon G.D., Price K.L. Burden of migraine: a review of its socioeconomic impact. Pharmacoeconomics. 1997;11(Suppl 1):1�10. [PubMed]
31. Bronfort G., Assendelft W.J.J., Evans R., Haas M., Bouter L. Efficacy of spinal manipulation for chronic headache: a systematic review. J Manipulative Physiol Ther. 2001;24:457�466. [PubMed]
32. Vernon H.T. Spinal manipulation in the management of tension-type migraine and cervicogenic headaches: the state of the evidence. Top Clin Chiropr. 2002;9:14�21.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Levator Scapulae (As Seen on Fig. 4.36 Below)
Assessment of the Levator Scapulae
Levator scapula �springing� test (a) The patient lies supine with the arm of the side to be tested stretched out with the supinated hand and lower arm tucked under the buttocks, to help restrain movement of the shoulder/scapula. The practitioner�s contralateral arm is passed across and under the neck to cup the shoulder of the side to be tested, with the forearm supporting the neck. 11 The practitioner�s other hand supports the head. The forearm is used to lift the neck into full pain-free flexion (aided by the other hand). The head is placed fully towards side-flexion and rotation, away from the side being treated.
Figure 4.36 MET test (a) and treatment position for levator scapula (right side).
With the shoulder held caudally and the head/ neck in the position described (each at its resistance barrier) stretch is being placed on levator from both ends.
If dysfunction exists and/or levator scapula is short, there will be discomfort reported at the attachment on the upper medial border of the scapula and/or pain reported near the levator attachment on the spinous process of C2.
The hand on the shoulder gently �springs� it caudally.
If levator is short there will be a harsh, wooden feel to this action. If it is normal there will be a soft feel to the springing pressure.
Levator scapula observation test (b) A functional assessment involves applying the evidence we have seen (see Ch. 2) of the imbalances which commonly occur between the upper and lower stabilisers of the scapula. In this process shortness is noted in pectoralis minor, levator scapulae and upper trapezius (as well as SCM), while weakness develops in serratus anterior, rhomboids, middle and lower trapezius � as well as the deep neck flexors.
Observation of the patient from behind will often show a �hollow� area between the shoulder blades, where interscapular weakness has occurred, as well as an increased (over normal) distance between the medial borders of the scapulae and the thoracic spine, as the scapulae will have �winged� away from it.
Levator scapula test (c) To see the imbalance described in test (b) in action, Janda (1996) has the patient in the press-up position (see Fig. 5.15). On very slow lowering of the chest towards the floor from a maximum push-up position, the scapula(e) on the side(s) where stabilisation has been compromised will move outwards, laterally and upwards � often into a winged position � rather than towards the spine.
This is diagnostic of weak lower stabilisers, which implicates tight upper stabilisers, including levator scapulae, as inhibiting them.
MET Treatment of Levator Scapula (Fig. 4.36)
Treatment of levator scapulae using MET enhances the lengthening of the extensor muscles attaching to the occiput and upper cervical spine. The position described below is used for treatment, either at the limit of easily reached range of motion, or a little short of this, depending upon the degree of acuteness or chronicity of the dysfunction.
The patient lies supine with the arm of the side to be tested stretched out alongside the trunk with the hand supinated. The practitioner, standing at the head of the table, passes his contralateral arm under the neck to rest on the patient�s shoulder on the side to be treated, so that the practitioner�s forearm supports the patient�s neck. The practitioner�s other hand supports and directs the head into subsequent movement (below).
The practitioner�s forearm lifts the neck into full flexion (aided by the other hand). The head is turned fully into side-flexion and rotation away from the side being treated.
With the shoulder held caudally by the practitioner�s hand, and the head/neck in full flexion, sideflexion and rotation (each at its resistance barrier), stretch is being placed on levator from both ends.
The patient is asked to take the head backwards towards the table, and slightly to the side from which it was turned, against the practitioner�s unmoving resistance, while at the same time a slight (20% of available strength) shoulder shrug is also asked for and resisted.
Following the 7�10 second isometric contraction and complete relaxation of all elements of this combined contraction, the neck is taken to further flexion, sidebending and rotation, where it is maintained as the shoulder is depressed caudally with the patient�s assistance (�as you breathe out, slide your hand towards your feet�). The stretch is held for 20�30 seconds.
The process is repeated at least once.
CAUTION: Avoid overstretching this sensitive area.
Facilitation of Tone in Lower Shoulder Fixators Using Pulsed MET (Ruddy 1962)
In order to commence rehabilitation and proprioceptive re-education of a weak serratus anterior:
The practitioner places a single digit contact very lightly against the lower medial scapula border, on the side of the treated upper trapezius of the seated or standing patient. The patient is asked to attempt to ease the scapula, at the point of digital contact, towards the spine (�press against my finger with your shoulder blade, towards your spine, just as hard [i.e. very lightly] as I am pressing against your shoulder blade, for less than a second�).
Once the patient has learned to establish control over the particular muscular action required to achieve this subtle movement (which can take a significant number of attempts), and can do so for 1 second at a time, repetitively, they are ready to begin the sequence based on Ruddy�s methodology (see Ch. 10, p. 75).
The patient is told something such as �now that you know how to activate the muscles which push your shoulder blade lightly against my finger, I want you to try do this 20 times in 10 seconds, starting and stopping, so that no actual movement takes place, just a contraction and a stopping, repetitively�.
This repetitive contraction will activate the rhomboids, middle and lower trapezii and serratus anterior � all of which are probably inhibited if upper trapezius is hypertonic. The repetitive contractions also produce an automatic reciprocal inhibition of upper trapezius, and levator scapula.
The patient can be taught to place a light finger or thumb contact against their own medial scapula (opposite arm behind back) so that home application of this method can be performed several times daily.
Treatment for Eye Muscles (Ruddy 1962)
Ruddy�s treatment method for the muscles of the eye is outlined in the notes below.
Ruddy�s Treatment for the Muscles of the Eye (Ruddy 1962)
Osteopathic eye specialist Dr T. Ruddy described a practical treatment method for application of MET principles to the muscles of the eye:
The pads of the practitioner�s index, middle and ring finger and the thumb are placed together to form four contacts into which the eyeball (eye closed) can rest (middle finger is above the cornea and the thumb pad below it).
These contacts resist the attempts the patient is asked to make to move the eyes downwards, laterally, medially and upwards � as well as obliquely between these compass points � up and half medial, down and half medial, up and half lateral, down and half lateral, etc.
The fingers resist and obstruct the intended path of eye motion.
Each movement should last for a count �one� and then rest between efforts for a similar count, and in each position there should be 10 repetitions before moving on around the circuit. Ruddy maintained the method released muscle tension, permitted better circulation, and enhanced drainage. He applied the method as part of treatment of many eye problems.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
Several types of headaches can affect the average individual and each may result due to a variety of injuries and/or conditions, however, migraine headaches can often have a much more complex reason behind them. Many healthcare professionals and numerous evidence-based research studies have concluded that a subluxation in the neck, or a misalignment of the vertebrae in the cervical spine, is the most common reason for migraine headaches. Migraine is characterized by severe head pain typically�affecting one side of the head, accompanied by nausea and disturbed vision. Migraine headaches can be debilitating. The information below describes a case study regarding the effect of atlas vertebrae realignment on patients with migraine.
Effect of Atlas Vertebrae Realignment in Subjects with Migraine: An Observational Pilot Study
Abstract
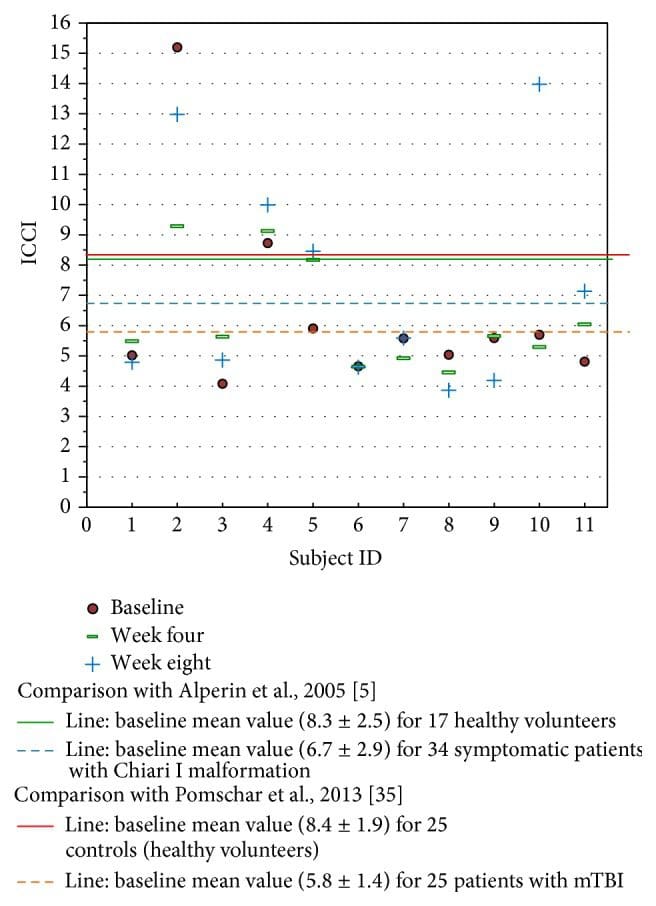
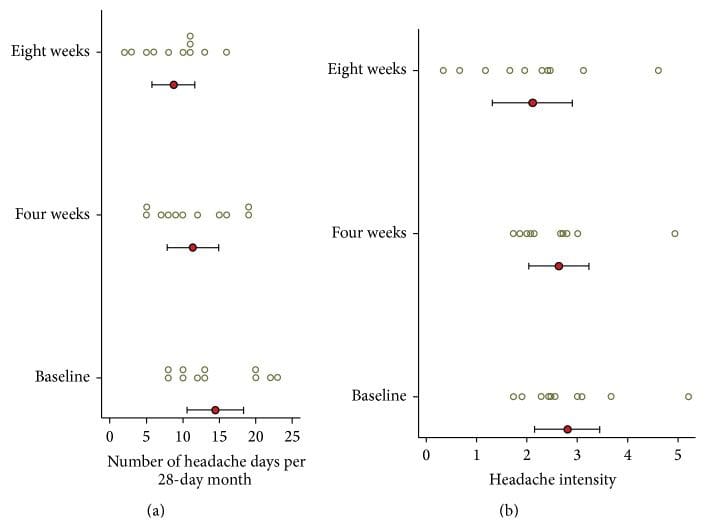
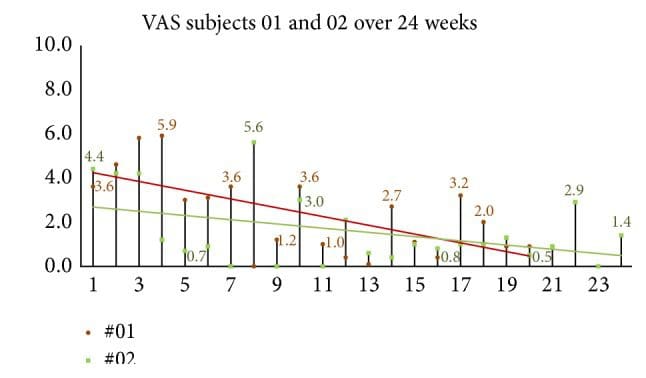
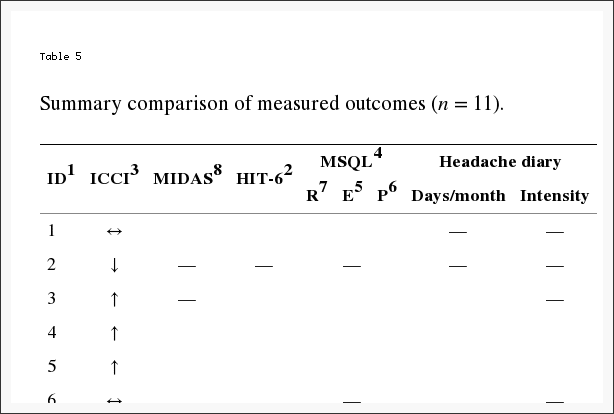
Introduction. In a migraine case study, headache symptoms significantly decreased with an accompanying increase in intracranial compliance index following atlas vertebrae realignment. This observational pilot study followed eleven neurologist diagnosed migraine subjects to determine if the case findings were repeatable at baseline, week four, and week eight, following a National Upper Cervical Chiropractic Association intervention. Secondary outcomes consisted of migraine-specific quality of life measures. Methods. After examination by a neurologist, volunteers signed consent forms and completed baseline migraine-specific outcomes. Presence of atlas misalignment allowed study inclusion, permitting baseline MRI data collection. Chiropractic care continued for eight weeks. Postintervention reimaging occurred at week four and week eight concomitant with migraine-specific outcomes measurement. Results. Five of eleven subjects exhibited an increase in the primary outcome, intracranial compliance; however, mean overall change showed no statistical significance. End of study mean changes in migraine-specific outcome assessments, the secondary outcome, revealed clinically significant improvement in symptoms with a decrease in headache days. Discussion. The lack of robust increase in compliance may be understood by the logarithmic and dynamic nature of intracranial hemodynamic and hydrodynamic flow, allowing individual components comprising compliance to change while overall it did not. Study results suggest that the atlas realignment intervention may be associated with a reduction in migraine frequency and marked improvement in quality of life yielding significant reduction in headache-related disability as observed in this cohort. Future study with controls is necessary, however, to confirm these findings. Clinicaltrials.gov registration number is NCT01980927.
Introduction
It has been proposed that a misaligned atlas vertebra creates spinal cord distortion disrupting neural traffic of brain stem nuclei in the medulla oblongata encumbering normal physiology [1�4].
The objective of the National Upper Cervical Chiropractic Association (NUCCA) developed atlas correction procedure is restoration of misaligned spinal structures to the vertical axis or gravity line. Described as the �restoration principle,� realignment aims to reestablish a patient’s normal biomechanical relationship of the upper cervical spine to the vertical axis (gravity line). Restoration is characterized as being architecturally balanced, being capable of unrestricted range of motion, and allowing a significant decrease in gravitational stress [3]. The correction theoretically removes the cord distortion, created by an atlas misalignment or atlas subluxation complex (ASC), as specifically defined by NUCCA. Neurologic function is restored, specifically thought to be in the brain stem autonomic nuclei, which affect the cranial vascular system that includes Cerebrospinal Fluid (CSF) [3, 4].
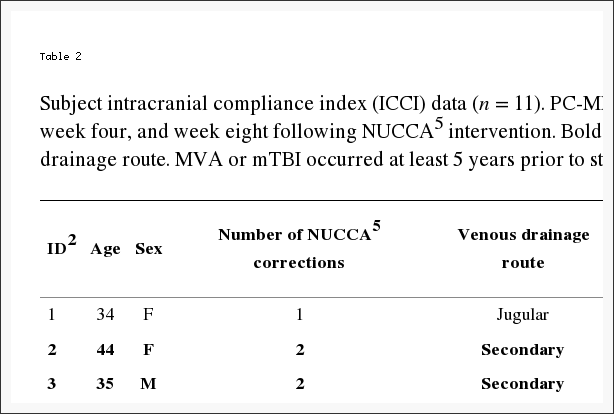
The intracranial compliance index (ICCI) appears to be a more sensitive assessment of changes made in craniospinal biomechanical properties in symptomatic patients than the local hydrodynamic parameters of CSF flow velocities and cord displacement measurements [5]. Based on that information, previously observed relationships of increased intracranial compliance to marked reduction in migraine symptoms following atlas realignment provided incentive for using the ICCI as the study objective primary outcome.
ICCI affects the ability of the Central Nervous System (CNS) to accommodate physiologic volume fluctuations that occur, thereby avoiding ischemia of underlying neurologic structures [5, 6]. A state of high intracranial compliance enables any volume increase to occur in the intrathecal CNS space without causing an intracranial pressure increase that occurs primarily with arterial inflow during systole [5, 6]. Outflow occurs in the supine position via the internal jugular veins or when upright, via paraspinal or secondary venous drainage. This extensive venous plexus is valveless and anastomotic, allowing blood to flow in a retrograde direction, into the CNS through postural changes [7, 8]. Venous drainage plays an important role in regulating the intracranial fluid system [9]. Compliance appears to be functional and dependent on the free egress of blood via these extracranial venous drainage pathways [10].
Head and neck injury could create abnormal function of the spinal venous plexus that may impair spinal venous drainage, possibly because of autonomic dysfunction secondary to spinal cord ischemia [11]. This decreases accommodation of volume fluctuations within the cranium creating a state of decreased intracranial compliance.
Damadian and Chu describe return of a normal CSF outflow measured at mid-C-2, exhibiting a 28.6% reduction of the measured CSF pressure gradient in the patient where the atlas had been optimally realigned [12]. The patient reported freedom from symptoms (vertigo and vomiting when recumbent) consistent with the atlas remaining in alignment.
A hypertension study using the NUCCA intervention suggests a possible mechanism underlying the blood pressure decrease could be resultant from changes in cerebral circulation in relation to atlas vertebrae position [13]. Kumada et al. investigated a trigeminal-vascular mechanism in brain stem blood pressure control [14, 15]. Goadsby et al. have presented compelling evidence that migraine originates via a trigeminal-vascular system mediated through the brain stem and upper cervical spine [16�19]. Empirical observation reveals significant reduction of migraine patients’ headache disability after application of the atlas correction. Using migraine-diagnosed subjects seemed ideal for investigating proposed cerebral circulation changes following atlas realignment as originally theorized in the hypertension study conclusions and seemingly supported by a possible brain stem trigeminal-vascular connection. This would further advance a developing working pathophysiologic hypothesis of atlas misalignment.
Results from an initial case study demonstrated substantial increase in ICCI with decrease in migraine headache symptoms following the NUCCA atlas correction. A 62-year-old male with neurologist diagnosed chronic migraine volunteered for a before-after intervention case study. Using Phase Contrast-MRI (PC-MRI), changes in cerebral hemodynamic and hydrodynamic flow parameters were measured at baseline, 72 hours, and then four weeks after the atlas intervention. The same atlas correction procedure used in the hypertension study was followed [13]. 72 hours after study revealed a noteworthy change in the intracranial compliance index (ICCI), from 9.4 to 11.5, to 17.5 by week four, after intervention. Observed changes in venous outflow pulsatility and predominant secondary venous drainage in the supine position warranted additional investigation further inspiring a study of migraine subjects in this case series.
The possible effects of the atlas misalignment or ASC on venous drainage are unknown. Careful examination of intracranial compliance in relation to effects of an atlas misalignment intervention may provide insight into how the correction might influence migraine headache.
Using PC-MRI, this current study’s primary objective, and primary outcome, measured ICCI change from baseline to four and eight weeks following a NUCCA intervention in a cohort of neurologist selected migraine subjects. As observed in the case study, the hypothesis supposed that a subject’s ICCI would increase following the NUCCA intervention with a corresponding decrease in migraine symptoms. If present, any observed changes in venous pulsatility and drainage route were to be documented for further comparison. To monitor migraine symptoms response, the secondary outcomes included patient reported outcomes to measure any related change in Health Related Quality of Life (HRQoL), similarly used in migraine research. Throughout the study, subjects maintained headache diaries documenting the decrease (or increase) in the number of headache days, intensity, and medication used.
Conducting this observational case series, pilot study, allowed for additional investigation into aforementioned physiologic effects in further development of a working hypothesis into the pathophysiology of an atlas misalignment. Data required for estimation of statistically significant subject sample sizes and resolving procedural challenges will provide needed information for developing a refined protocol to conduct a blinded, placebo controlled migraine trial using the NUCCA correction intervention.
Methods
This research maintained compliance with the Helsinki Declaration for research on human subjects. The University of Calgary and Alberta Health Services Conjoint Health Research Ethics Board approved the study protocol and subject informed consent form, Ethics ID: E-24116. ClinicalTrials.gov assigned the number NCT01980927 after registration of this study (https://clinicaltrials.gov/ct2/show/NCT01980927).
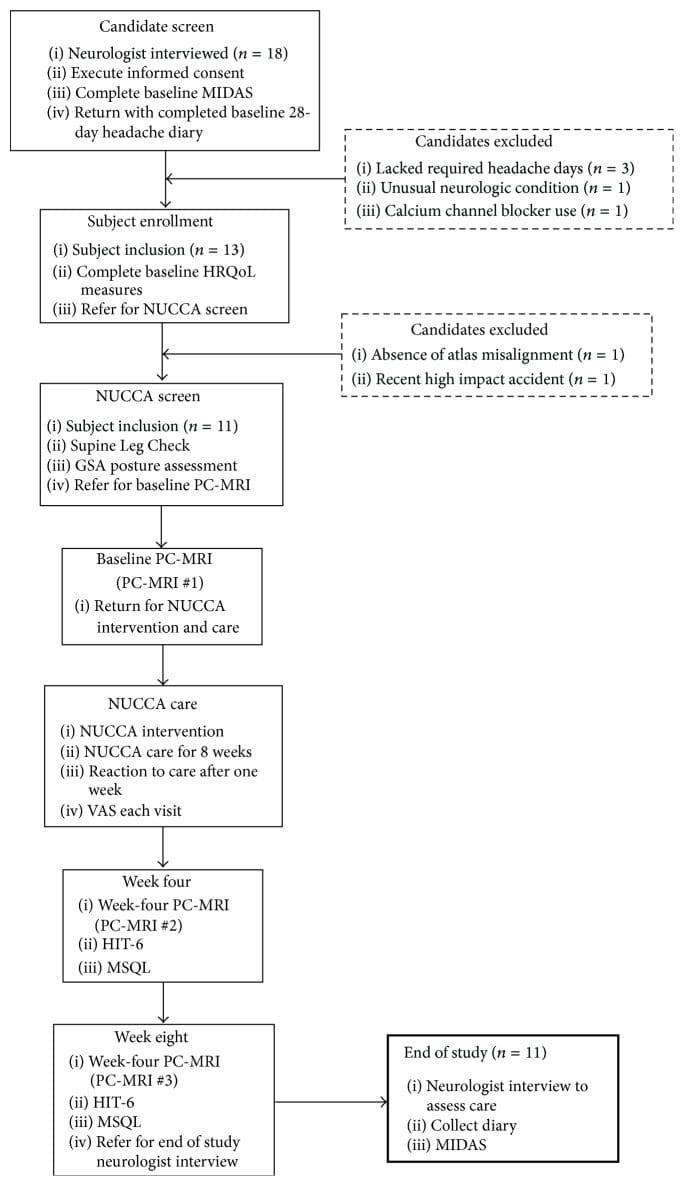
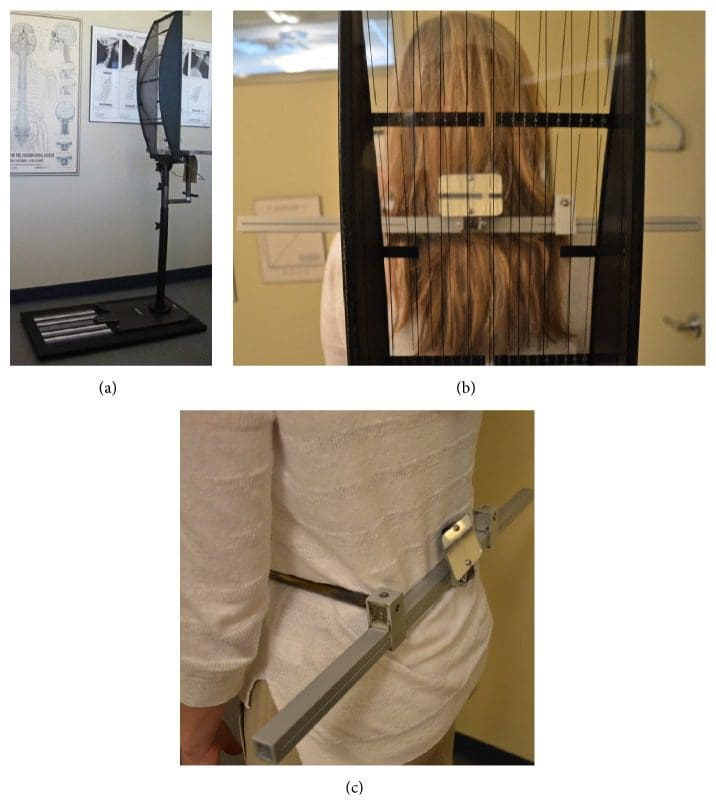
Subject recruitment and screening occurred at the Calgary Headache Assessment and Management Program (CHAMP), a neurology-based specialist referral clinic (see Figure 1, Table 1). CHAMP evaluates patients resistant to standard pharmacotherapy and medical treatment for migraine headache that no longer provides migraine symptom relief. Family and primary care physicians referred potential study subjects to CHAMP making advertising unnecessary.
Figure 1: Subject disposition and study flow (n = 11). GSA: Gravity Stress Analyzer. HIT-6: Headache Impact Test-6. HRQoL: Health Related Quality of Life. MIDAS: Migraine Disability Assessment Scale. MSQL: Migraine-Specific Quality of Life Measure. NUCCA: National Upper Cervical Chiropractic Association. PC-MRI: Phase Contrast Magnetic Resonance Imaging. VAS: Visual Analog Scale.
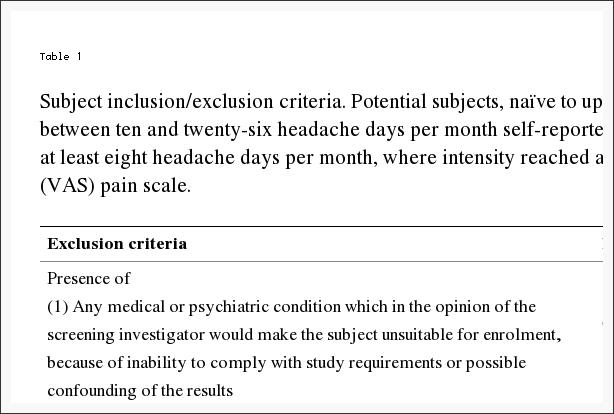
Table 1: Subject inclusion/exclusion criteria. Potential subjects, na�ve to upper cervical chiropractic care, demonstrated between ten and twenty-six headache days per month self-reported over the previous four months. Requisite was at least eight headache days per month, where intensity reached at least four, on a zero to ten Visual Analog Scale (VAS) pain scale.
Study inclusion required volunteers, between the ages of 21 and 65 years, that satisfy specific diagnostic criteria for migraine headache. A neurologist with several decades of migraine experience screened applicants utilizing the International Classification of Headache Disorders (ICHD-2) for study inclusion [20]. Potential subjects, na�ve to upper cervical chiropractic care, must have demonstrated through self-report between ten and twenty-six headache days per month over the previous four months. At least eight headache days per month had to reach an intensity of at least four on a zero to ten VAS pain scale, unless treated successfully with a migraine-specific medication. At least four separate headache episodes per month separated by at least a 24-hour pain-free interval were required.
Significant head or neck trauma occurring within one year prior to study entry excluded candidates. Further exclusion criteria included acute medication overuse, a history of claustrophobia, cardiovascular or cerebrovascular disease, or any CNS disorder other than migraine. Table 1 describes the complete inclusion and exclusion criteria considered. Using an experienced board certified neurologist to screen potential subjects while adhering to the ICHD-2 and guided by the inclusion/exclusion criteria, the exclusion of subjects with other sources of headache such as muscular tension and medication overuse rebound headache would increase the likelihood of successful subject recruitment.
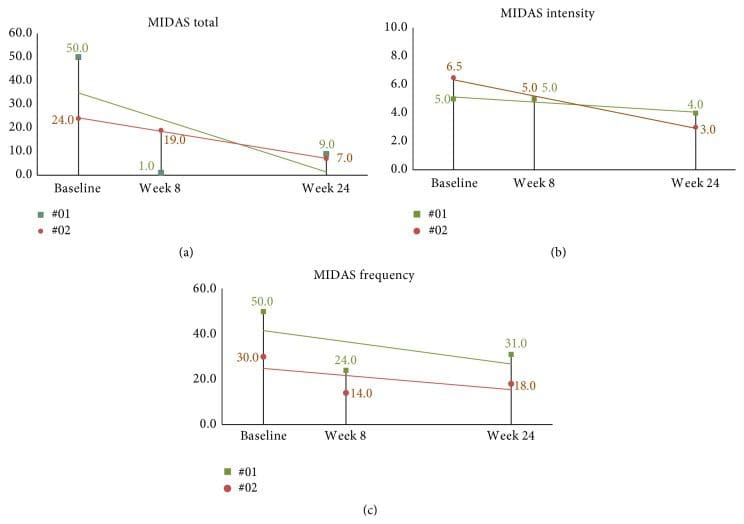
Those meeting initial criteria signed informed consent and then completed a baseline Migraine Disability Assessment Scale (MIDAS). The MIDAS requires twelve weeks to demonstrate clinically significant change [21]. This allowed adequate time to pass to discern any possible changes. Over the next 28 days, candidates recorded a headache diary providing baseline data while confirming the number of headache days and intensity required for inclusion. After the four weeks, the diary check diagnostic substantiation permitted administration of remaining baseline HRQoL measures:
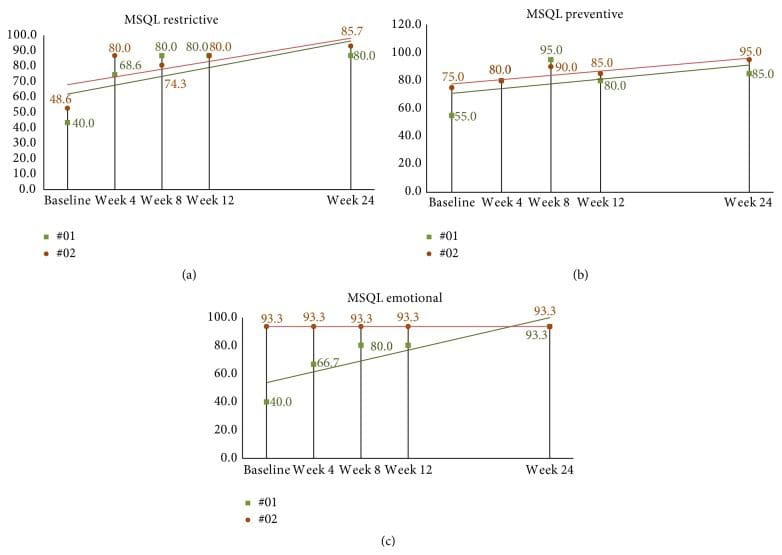
Migraine-Specific Quality of Life Measure (MSQL) [22],
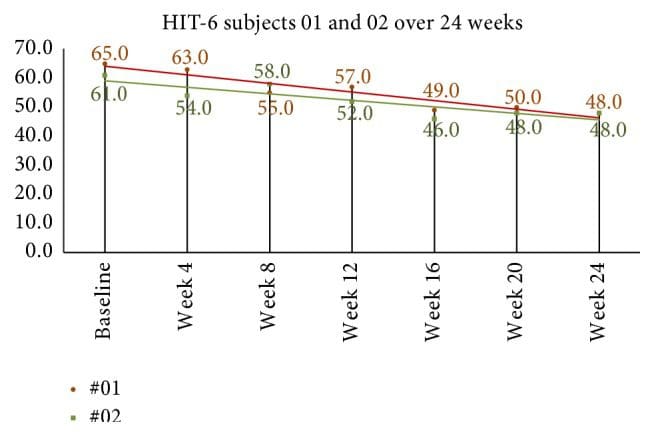
Headache Impact Test-6 (HIT-6) [23],
Subject current global assessment of headache pain (VAS).
Referral to the NUCCA practitioner, to determine presence of atlas misalignment, confirmed need for intervention finalizing a subject’s study inclusion?exclusion. Absence of atlas misalignment indicators excluded candidates. After scheduling appointments for NUCCA intervention and care, qualified subjects obtained baseline PC-MRI measures. Figure 1 summarizes subject disposition throughout the study.
The initial NUCCA intervention required three consecutive visits: (1) Day One, atlas misalignment assessment, before-correction radiographs; (2) Day Two, NUCCA correction with after-correction assessment with radiographs; and (3) Day Three, after-correction reassessment. Follow-up care occurred weekly for four weeks, then every two weeks for the remainder of the study period. At each NUCCA visit, subjects completed a current assessment of headache pain (please rate your headache pain on average over the past week) using a straight edge and pencil in marking a 100?mm line (VAS). One week after the initial intervention, subjects completed a �Possible Reaction to Care� questionnaire. This assessment has past been used for successfully monitoring adverse events related to various upper cervical correction procedures [24].
At week four, PC-MRI data were obtained and subjects completed an MSQL and HIT-6. End of study PC-MRI data were collected at week eight followed by a neurologist exit interview. Here, subjects completed final MSQOL, HIT-6, MIDAS, and VAS outcomes and headache diaries were collected.
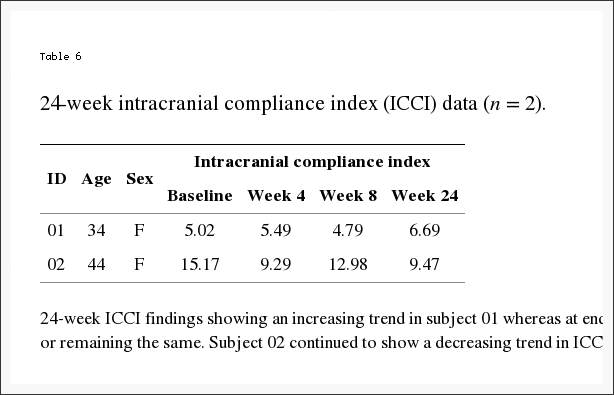
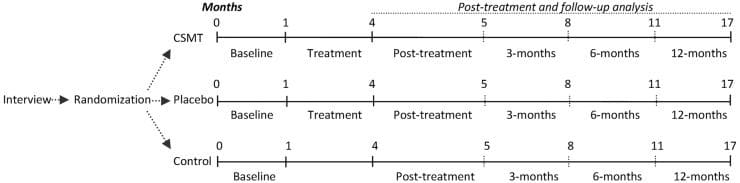
At the week-8 neurologist visit, two willing subjects were offered a long-term follow-up opportunity for a total study period of 24 weeks. This involved further NUCCA reassessment monthly for 16 weeks after completion of the initial 8-week study. The purpose of this follow-up was to help determine if headache improvement continued contingent upon maintenance of atlas alignment while observing for any long-term effect of NUCCA care on ICCI. Subjects desiring to participate signed a second informed consent for this phase of study and continued monthly NUCCA care. At the end of 24 weeks from the original atlas intervention, the fourth PC-MRI imaging study occurred. At the neurologist exit interview, final MSQOL, HIT-6, MIDAS, and VAS outcomes and headache diaries were collected.
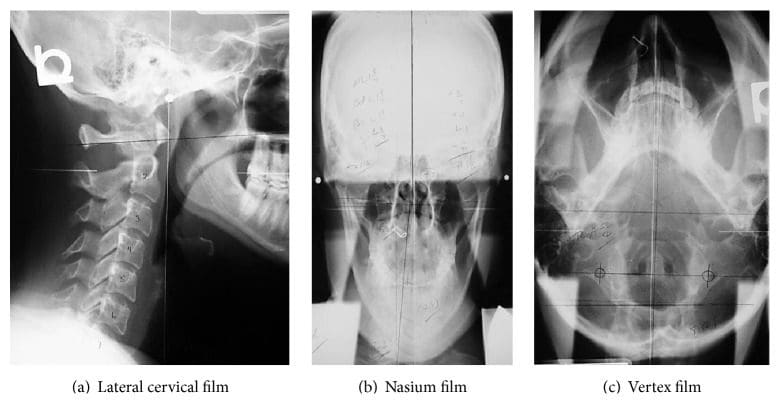
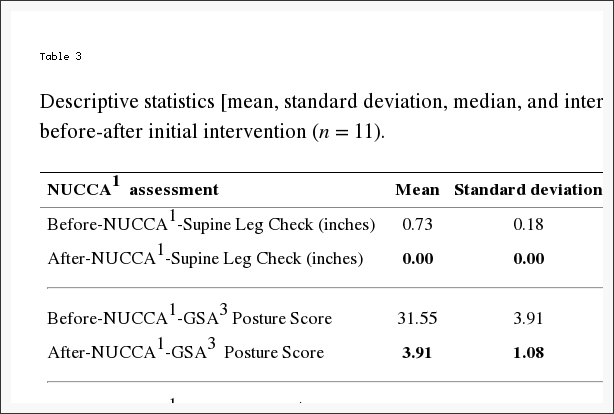
The same NUCCA procedure as previously reported was followed using the established protocol and standards of care developed through NUCCA Certification for assessment and atlas realignment or correction of the ASC (see Figures ?Figures22�5) [2, 13, 25]. Assessment for the ASC includes screening for functional leg-length inequality with the Supine Leg Check (SLC) and examination of postural symmetry using the Gravity Stress Analyzer (Upper Cervical Store, Inc., 1641 17 Avenue, Campbell River, BC, Canada V9W 4L5) (see Figures ?Figures22 and 3(a)�3(c)) [26�28]. If SLC and postural imbalances are detected, a three-view radiographic exam is indicated to determine the multidimensional orientation and degree of craniocervical misalignment [29, 30]. A thorough radiographic analysis provides information to determine a subject specific, optimal atlas correction strategy. The clinician locates anatomic landmarks from the three-view series, measuring structural and functional angles that have deviated from established orthogonal standards. The degree of misalignment and atlas orientation are then revealed in three dimensions (see Figures 4(a)�4(c)) [2, 29, 30]. Radiographic equipment alignment, reduction of collimator port size, high-speed film-screen combinations, special filters, specialized grids, and lead shielding minimize subject radiation exposure. For this study, average total measured Entrance Skin Exposure to subjects from the before-after-correction radiographic series was 352 millirads (3.52 millisieverts).
Figure 2: Supine Leg Check Screening Test (SLC). Observation of an apparent �short leg� indicates possible atlas misalignment. These appear even.
Figure 3: Gravity Stress Analyzer (GSA). (a) Device determines postural asymmetry as a further indicator of atlas misalignment. Positive findings in the SLC and GSA indicate need for NUCCA radiographic series. (b) Balanced patient with no postural asymmetry. (c) Hip calipers used to measure pelvis asymmetry.
Figure 4: NUCCA radiograph series. These films are used to determine atlas misalignment and developing a correction strategy. After-correction radiographs or postfilms ensure the best correction has been made for that subject.
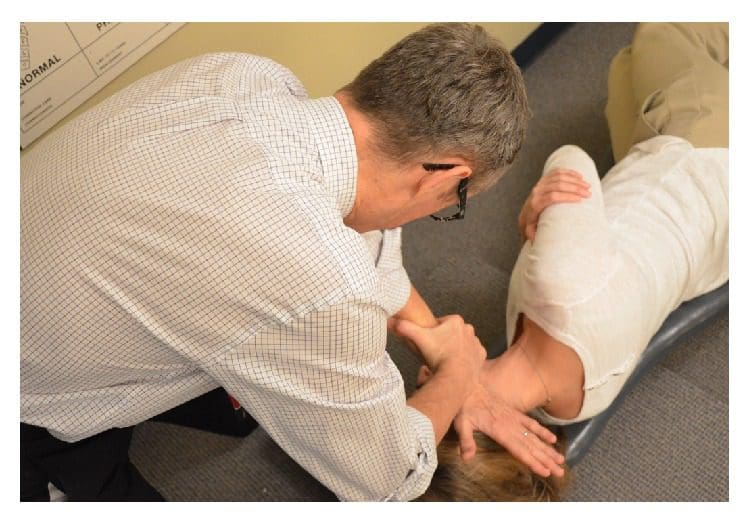
Figure 5: Making a NUCCA correction. The NUCCA practitioner delivers a triceps pull adjustment. The practitioner’s body and hands are aligned to deliver an atlas correction along an optimal force vector using information obtained from radiographs.
The NUCCA intervention involves a manual correction of the radiographically measured misalignment in the anatomical structure between the skull, atlas vertebra, and cervical spine. Utilizing biomechanical principles based on a lever system, the doctor develops a strategy for proper
subject positioning,
practitioner stance,
force vector to correct the atlas misalignment.
Subjects are placed on a side-posture table with the head specifically braced using a mastoid support system. Application of the predetermined controlled force vector for the correction realigns the skull to the atlas and neck to the vertical axis or center of gravity of the spine. These corrective forces are controlled in depth, direction, velocity, and amplitude, producing an accurate and precise reduction of the ASC.
Using the pisiform bone of the contact hand, the NUCCA practitioner contacts the atlas transverse process. The other hand encircles the wrist of the contact hand, to control the vector while maintaining the depth of force generated in application of the �triceps pull� procedure (see Figure 5) [3]. By understanding spinal biomechanics, the practitioner’s body and hands are aligned to produce an atlas correction along the optimal force vector. The controlled, nonthrusting force is applied along the predetermined reduction pathway. It is specific in its direction and depth to optimize the ASC reduction assuring no activation in the reactive forces of the neck muscles in response to the biomechanical change. It is understood that an optimal reduction of the misalignment promotes long-term maintenance and stability of spinal alignment.
Following a short rest period, an after-assessment procedure, identical to the initial evaluation, is performed. A postcorrection radiograph examination uses two views to verify return of the head and cervical spine into optimum orthogonal balance. Subjects are educated in ways to preserve their correction, thus preventing another misalignment.
Subsequent NUCCA visits were comprised of headache diary checks and a current assessment of headache pain (VAS). Leg length inequality and excessive postural asymmetry were used in determining the need for another atlas intervention. The objective for optimal improvement is for the subject to maintain the realignment for as long as possible, with the fewest number of atlas interventions.
In a PC-MRI sequence, contrast media are not used. PC-MRI methods collected two data sets with different amounts of flow sensitivity acquired by relating gradient pairs, which sequentially dephase and rephase spins during the sequence. The raw data from the two sets are subtracted to calculate a flow rate.
An on-site visit by the MRI Physicist provided training for the MRI Technologist and a data transfer procedure was established. Several practice scans and data transfers were performed to ensure data collection succeeded without challenges. A 1.5-tesla GE 360 Optima MR scanner (Milwaukee, WI) at the study imaging center (EFW Radiology, Calgary, Alberta, Canada) was used in imaging and data collection. A 12-element phased array head coil, 3D magnetization-prepared rapid-acquisition gradient echo (MP-RAGE) sequence was used in anatomy scans. Flow sensitive data were acquired using a parallel acquisition technique (iPAT), acceleration factor 2.
To measure blood flow to and from the skull base, two retrospectively gated, velocity-encoded cine-phase-contrast scans were performed as determined by individual heart rate, collecting thirty-two images over a cardiac cycle. A high-velocity encoding (70?cm/s) quantified high-velocity blood flow perpendicular to the vessels at the C-2 vertebra level includes the internal carotid arteries (ICA), vertebral arteries (VA), and internal jugular veins (IJV). Secondary venous flow data of vertebral veins (VV), epidural veins (EV), and deep cervical veins (DCV) were acquired at the same height using a low-velocity encoding (7�9?cm/s) sequence.
Subject data were identified by Subject Study ID and imaging study date. The study neuroradiologist reviewed MR-RAGE sequences to rule out exclusionary pathologic conditions. Subject identifiers were then removed and assigned a coded ID permitting transfer via a secured tunnel IP protocol to the physicist for analysis. Using proprietary software volumetric blood, Cerebrospinal Fluid (CSF) flow rate waveforms and derived parameters were determined (MRICP version 1.4.35 Alperin Noninvasive Diagnostics, Miami, FL).
Using the pulsatility-based segmentation of lumens, time-dependent volumetric flow rates were calculated by integrating the flow velocities inside the luminal cross-sectional areas over all thirty-two images. Mean flow rates were obtained for the cervical arteries, primary venous drainage, and secondary venous drainage pathways. Total cerebral blood flow was obtained by summation of these mean flow rates.
A simple definition of compliance is a ratio of volume and pressure changes. Intracranial compliance is calculated from the ratio of the maximal (systolic) intracranial volume change (ICVC) and pressure fluctuations during the cardiac cycle (PTP-PG). Change in ICVC is obtained from momentary differences between volumes of blood and CSF entering and exiting the cranium [5, 31]. Pressure change during the cardiac cycle is derived from the change in the CSF pressure gradient, which is calculated from the velocity-encoded MR images of the CSF flow, using the Navier-Stokes relationship between derivatives of velocities and the pressure gradient [5, 32]. An intracranial compliance index (ICCI) is calculated from the ratio of ICVC and pressure changes [5, 31�33].
Statistical analysis considered several elements. ICCI data analysis involved a one-sample Kolmogorov-Smirnov test revealing a lack of normal distribution in the ICCI data, which were therefore described using the median and interquartile range (IQR). Differences between baseline and follow-up were to be examined using a paired t-test.
NUCCA assessments data were described using mean, median, and interquartile range (IQR). Differences between baseline and follow-up were examined using a paired t-test.
Depending on the outcome measure, baseline, week four, week eight, and week twelve (MIDAS only) follow-up values were described using the mean and standard deviation. MIDAS data collected at initial neurologist screening had one follow-up score at the end of twelve weeks.
Differences from baseline to each follow-up visit were tested using a paired t-test. This resulted in numerous p values from two follow-up visits for each outcome except the MIDAS. Since one purpose of this pilot is to provide estimates for future research, it was important to describe where differences occurred, rather than to use a one-way ANOVA to arrive at a single p value for each measure. The concern with such multiple comparisons is the increase in Type I error rate.
To analyze the VAS data, each subject scores were examined individually and then with a linear regression line that adequately fits the data. Use of a multilevel regression model with both random intercepts and random slope provided an individual regression line fitted for each patient. This was tested against a random intercept-only model, which fits a linear regression line with a common slope for all subjects, while intercept terms are allowed to vary. The random coefficient model was adopted, as there was no evidence that random slopes significantly improved the fit to the data (using a likelihood ratio statistic). To illustrate the variation in the intercepts but not in the slope, the individual regression lines were graphed for each patient with an imposed average regression line on top.
Results
From initial neurologist screening, eighteen volunteers were eligible for inclusion. After completion of baseline headache diaries, five candidates did not meet inclusion criteria. Three lacked the required headache days on baseline diaries to be included, one had unusual neurological symptoms with persistent unilateral numbness, and another was taking a calcium channel blocker. The NUCCA practitioner found two candidates ineligible: one lacking an atlas misalignment and the second with a Wolff-Parkinson-White condition and severe postural distortion (39�) with recent involvement in a severe high impact motor vehicle accident with whiplash (see Figure 1).
Eleven subjects, eight females and three males, average age forty-one years (range 21�61 years), qualified for inclusion. Six subjects presented chronic migraine, reporting fifteen or more headache days a month, with a total eleven-subject mean of 14.5 headache days a month. Migraine symptom duration ranged from two to thirty-five years (mean twenty-three years). All medications were maintained unchanged for the study duration to include their migraine prophylaxis regimens as prescribed.
Per exclusion criteria, no subjects included received a diagnosis of headache attributed to traumatic injury to the head and neck, concussion, or persistent headache attributed to whiplash. Nine subjects reported a very remote past history, greater than five years or more (average of nine years) prior to neurologist screen. This included sports-related head injuries, concussion, and/or whiplash. Two subjects indicated no prior head or neck injury (see Table 2).
Table 2: Subject intracranial compliance index (ICCI) data (n = 11). PC-MRI6 acquired ICCI1 data reported at baseline, week four, and week eight following NUCCA5 intervention. Bolded rows signify subject with secondary venous drainage route. MVA or mTBI occurred at least 5 years prior to study inclusion, average 10 years.
Individually, five subjects demonstrated an increase in ICCI, three subject’s values remained essentially the same, and three showed a decrease from baseline to end of study measurements. Overall changes in intracranial compliance are seen in Table 2 and Figure 8. The median (IQR) values of ICCI were 5.6 (4.8, 5.9) at baseline, 5.6 (4.9, 8.2) at week four, and 5.6 (4.6, 10.0) at week eight. Differences were not statistically different. The mean difference between baseline and week four was ?0.14 (95% CI ?1.56, 1.28), p = 0.834, and between baseline and week eight was 0.93 (95% CI ?0.99, 2.84), p = 0.307. These two subject’s 24-week ICCI study results are seen in Table 6. Subject 01 displayed an increasing trend in ICCI from 5.02 at baseline to 6.69 at week 24, whereas at week 8, results were interpreted as consistent or remaining the same. Subject 02 demonstrated a decreasing trend in ICCI from baseline of 15.17 to 9.47 at week 24.
Figure 8: Study ICCI data compared to previously reported data in the literature. The MRI time values are fixed at baseline, week 4, and week 8 after intervention. This study’s baseline values fall similar to the data reported by Pomschar on subjects presenting only with mTBI.
Table 6: 24-week ICCI findings showing an increasing trend in subject 01 whereas at end of study (week 8), results were interpreted as consistent or remaining the same. Subject 02 continued to show a decreasing trend in ICCI.
Table 3 reports changes in NUCCA assessments. The mean difference from before to after the intervention is as follows: (1) SLC: 0.73 inches, 95% CI (0.61, 0.84) (p < 0.001); (2) GSA: 28.36 scale points, 95% CI (26.01, 30.72) (p < 0.001); (3) Atlas Laterality: 2.36 degrees, 95% CI (1.68, 3.05) (p < 0.001); and (4) Atlas Rotation: 2.00 degrees, 95% CI (1.12, 2.88) (p < 0.001). This would indicate that a probable change occurred following the atlas intervention as based on subject assessment.
Table 3: Descriptive statistics [mean, standard deviation, median, and interquartile range (IQR2)] of NUCCA1 assessments before-after initial intervention (n = 11).
Headache diary results are reported in Table 4 and Figure 6. At baseline subjects had mean 14.5 (SD = 5.7) headache days per 28-day month. During the first month following NUCCA correction, mean headache days per month decreased by 3.1 days from baseline, 95% CI (0.19, 6.0), p = 0.039, to 11.4. During the second month headache days decreased by 5.7 days from baseline, 95% CI (2.0, 9.4), p = 0.006, to 8.7 days. At week eight, six of the eleven subjects had a reduction of >30% in headache days per month. Over 24 weeks, subject 01 reported essentially no change in headache days while subject 02 had a reduction of one headache day a month from study baseline of seven to end of study reports of six days.
Figure 6: Headache days and headache pain intensity from diary (n = 11). (a) Number of headache days per month. (b) Average headache intensity (on headache days). Circle indicates the mean and the bar indicates the 95% CI. Circles are individual subject scores. A significant decrease in headache days per month was noticed at four weeks, almost doubling at eight weeks. Four subjects (#4, 5, 7, and 8) exhibited a greater than 20% decrease in headache intensity. Concurrent medication use may explain the small decrease in headache intensity.
At baseline, mean headache intensity on days with headache, on a scale of zero to ten, was 2.8 (SD = 0.96). Mean headache intensity showed no statistically significant change at four (p = 0.604) and eight (p = 0.158) weeks. Four subjects (#4, 5, 7, and 8) exhibited a greater than 20% decrease in headache intensity.
Quality of life and headache disability measures are seen in Table 4. The mean HIT-6 score at baseline was 64.2 (SD = 3.8). At week four after NUCCA correction, mean decrease in scores was 8.9, 95% CI (4.7, 13.1), p = 0.001. Week-eight scores, compared to baseline, revealed mean decrease by 10.4, 95% CI (6.8, 13.9), p = 0.001. In the 24-week group, subject 01 showed a decrease of 10 points from 58 at week 8 to 48 at week 24 while subject 02 decreased 7 points from 55 at week 8 to 48 at week 24 (see Figure 9).
Figure 9: 24-week HIT-6 scores in long-term follow-up subjects. Monthly scores continued to decrease after week 8, end of first study. Based on Smelt et al. criteria, it can be interpreted that a within-person minimally important change occurred between week 8 and week 24. HIT-6: Headache Impact Test-6.
MSQL mean baseline score was 38.4 (SD = 17.4). At week four after correction, mean scores for all eleven subjects increased (improved) by 30.7, 95% CI (22.1, 39.2), p < 0.001. By week eight, end of study, mean MSQL scores had increased from baseline by 35.1, 95% CI (23.1, 50.0), p < 0.001, to 73.5. The follow-up subjects continued to show some improvement with increasing scores; however, many scores plateaued remaining the same since week 8 (see Figures 10(a)�10(c)).
Figure 10: ((a)�(c)) 24-week MSQL scores in long-term follow-up subjects. (a) Subject 01 has essentially plateaued after week 8 throughout to end of the second study. Subject 02 shows scores increasing over time demonstrating minimally important differences based on Cole et al. criteria by week 24. (b) Subject scores seem to peak by week 8 with both subjects showing similar scores reported at week 24. (c) Subject 2 scores remain consistent throughout the study while subject 01 shows steady improvement from baseline to the end of week 24. MSQL: Migraine-Specific Quality of Life Measure.
Mean MIDAS score at baseline was 46.7 (SD = 27.7). At two months after NUCCA correction (three months following baseline), the mean decrease in subject’s MIDAS scores was 32.1, 95% CI (13.2, 51.0), p = 0.004. The follow-up subjects continued to show improvement with decreasing scores with intensity showing minimal improvement (see Figures 11(a)�11(c)).
Figure 11: 24-week MIDAS scores in long-term follow-up subjects. (a) Total MIDAS scores continued a decreasing trend over the 24-week study period. (b) Intensity scores continued improvement. (c) While 24-week frequency was higher than at week 8, improvement is observed when compared to baseline. MIDAS: Migraine Disability Assessment Scale.
Assessment of current headache pain from VAS scale data is seen in Figure 7. The multilevel linear regression model showed evidence of a random effect for the intercept (p < 0.001) but not for the slope (p = 0.916). Thus, the adopted random intercept model estimated a different intercept for each patient but a common slope. The estimated slope of this line was ?0.044, 95% CI (?0.055, ?0.0326), p < 0.001, indicating that there was a significant decrease in the VAS score of 0.44 per 10 days after baseline (p < 0.001). The mean baseline score was 5.34, 95% CI (4.47, 6.22). The random effects analysis showed substantial variation in the baseline score (SD = 1.09). As the random intercepts are normally distributed, this indicates that 95% of such intercepts lie between 3.16 and 7.52 providing evidence of substantial variation in the baseline values across patients. VAS scores continued showing improvement in the 24-week two-subject follow-up group (see Figure 12).
Figure 7: Subject global assessment of headache (VAS) (n = 11). There was substantial variation in baseline scores across these patients. The lines show individual linear fit for each of eleven patients. The thick dotted black line represents the average linear fit across all eleven patients. VAS: Visual Analog Scale.
Figure 12: 24-week follow-up group global assessment of headache (VAS). When subjects were queried, �please rate your headache pain on average over the past week� VAS scores continued showing improvement in the 24-week two-subject follow-up group.
The most obvious reaction to the NUCCA intervention and care reported by ten subjects was mild neck discomfort, rated an average of three out of ten on pain assessment. In six subjects, pain began more than twenty-four hours after the atlas correction, lasting more than twenty-four hours. No subject reported any significant effect on their daily activities. All subjects reported satisfaction with NUCCA care after one week, median score, ten, on a zero to ten rating scale.
Dr. Alex Jimenez’s Insight
“I’ve been experiencing migraine headaches for several years now. Is there a reason for my head pain? What can I do to decrease or get rid of my symptoms?”�Migraine headaches are believed to be a complex form of head pain, however, the reason for them is much the same as any other type of headache. A traumatic injury to the cervical spine, such as that of whiplash from an automobile accident or a sports injury, can cause a misalignment in the neck and upper back, which may lead to migraine. An improper posture can also cause neck issues which could lead to head and neck pain. A healthcare professional who specializes in spinal health issues can diagnose the source of your migraine headaches. Furthermore, a qualified and experienced specialist can perform spinal adjustments as well as manual manipulations to help correct any misalignments of the spine which could be causing the symptoms. The following article summarizes a case study based on the improvement of symptoms after atlas vertebrae realignment in participants with migraine.
Discussion
In this limited cohort of eleven migraine subjects, there was no statistically significant change in ICCI (primary outcome) after the NUCCA intervention. However, a significant change in HRQoL secondary outcomes did occur as summarized in Table 5. The consistency in the magnitude and direction of improvement across these HRQoL measures indicates confidence in enhancement of headache health over the two-month study following the 28-day baseline period.
Table 5: Summary Comparison of Measured Outcomes
Based on the case study results, this investigation hypothesized a significant increase in ICCI after the atlas intervention which was not observed. Use of PC-MRI allows quantification of the dynamic relationship between arterial inflow, venous outflow, and CSF flow between the cranium and the spinal canal [33]. Intracranial compliance index (ICCI) measures the brain’s ability to respond to incoming arterial blood during systole. Interpretation of this dynamic flow is represented by a monoexponential relationship existing between CSF volume and CSF pressure. With increased or higher intracranial compliance, also defined as good compensatory reserve, the incoming arterial blood can be accommodated by the intracranial contents with a smaller change in intracranial pressure. While a change in intracranial volume or pressure could occur, based on the exponential nature of the volume-pressure relationship, a change in after-intervention ICCI may not be realized. An advanced analysis of the MRI data and further study are required for pinpointing practical quantifiable parameters to use as an objective outcome sensitive for documenting a physiologic change following atlas correction.
Koerte et al. reports of chronic migraine patients demonstrate a significantly higher relative secondary venous drainage (paraspinal plexus) in the supine position when compared to age- and gender-matched controls [34]. Four study subjects exhibited a secondary venous drainage with three of those subjects demonstrating notable increase in compliance after intervention. The significance is unknown without further study. Similarly, Pomschar et al. reported that subjects with mild traumatic brain injury (mTBI) demonstrate an increased drainage through the secondary venous paraspinal route [35]. The mean intracranial compliance index appears significantly lower in the mTBI cohort when compared to controls.
Some perspective may be gained in comparison of this study’s ICCI data to previously reported normal subjects and those with mTBI seen in Figure 8 [5, 35]. Limited by the small number of subjects studied, the significance these study’s findings may have in relation to Pomschar et al. remains unknown, offering only speculation of possibilities for future exploration. This is further complicated by the inconsistent ICCI change observed in the two subjects followed for 24 weeks. Subject two with a secondary drainage pattern exhibited a decrease in ICCI following intervention. A larger placebo controlled trial with a statistically significant subject sample size could possibly demonstrate a definitive objectively measured physiologic change after application of the NUCCA correction procedure.
HRQoL measures are used clinically to assess the effectiveness of a treatment strategy to decrease pain and disability related to migraine headache. It is expected that an effective treatment improves patient perceived pain and disability measured by these instruments. All HRQoL measures in this study demonstrated significant and substantial improvement by week four following the NUCCA intervention. From week four to week eight only small improvements were noted. Again, only small improvements were noted in the two subjects followed for 24 weeks. While this study was not intended to demonstrate causation from the NUCCA intervention, the HRQoL results create compelling interest for further study.
From the headache diary, a significant decrease in headache days per month was noticed at four weeks, almost doubling at eight weeks. However, significant differences in headache intensity over time were not discernable from this diary data (see Figure 5). While the number of headaches decreased, subjects still used medication to maintain headache intensity at tolerable levels; hence, it is supposed that a statistically significant difference in headache intensity could not be determined. Consistency in the headache day numbers occurring in week 8 in the follow-up subjects could guide future study focus in determining when maximum improvement occurs to help in establishing a NUCCA standard of migraine care.
Clinically relevant change in the HIT-6 is important for completely understanding observed outcomes. A clinically meaningful change for an individual patient has been defined by the HIT-6 user guide as ?5 [36]. Coeytaux et al., using four different analysis methods, suggest that a between-group difference in HIT-6 scores of 2.3 units over time may be considered clinically significant [37]. Smelt et al. studied primary care migraine patient populations in developing suggested recommendations using HIT-6 score changes for clinical care and research [38]. Dependent on consequences resulting from false positives or negatives, within-person minimally important change (MIC) using a �mean change approach� was estimated to be 2.5 points. When using the �receiver operating characteristic (ROC) curve analysis� a 6-point change is needed. Recommended between-group minimally important difference (MID) is 1.5 [38].
Using the �mean change approach,� all subjects but one reported a change (decrease) greater than ?2.5. The �ROC analyses� also demonstrated improvement by all subjects but one. This �one subject� was a different person in each comparison analysis. Based on Smelt et al. criteria, the follow-up subjects continued to demonstrate within-person minimally important improvement as seen in Figure 10.
All subjects but two showed improvement on the MIDAS score between baseline and three-month results. The magnitude of the change was proportional to the baseline MIDAS score, with all subjects but three reporting an overall fifty percent or greater change. The follow-up subjects continued to show improvement as seen in continued decrease in scores by week 24; see Figures 11(a)�11(c).
Use of the HIT-6 and MIDAS together as a clinical outcome may provide a more complete assessment of headache-related disability factors [39]. The differences between the two scales can predict disability from headache pain intensity and headache frequency, by providing more information on factors related to the reported changes than either outcome used alone. While the MIDAS appears to change more by headache frequency, headache intensity seems to affect HIT-6 score more than the MIDAS [39].
How migraine headache affects and limits patient perceived daily functioning is reported by the MSQL v. 2.1, across three 3 domains: role restrictive (MSQL-R), role preventive (MSQL-P), and emotional functioning (MSQL-E). An increase in scores indicates improvement in these areas with values ranging from 0 (poor) to 100 (best).
MSQL scales reliability evaluation by Bagley et al. report results to be moderately to highly correlated with HIT-6 (r = ?0.60 to ?0.71) [40]. Study by Cole et al. reports minimally important differences (MID) clinical change for each domain: MSQL-R = 3.2, MSQL-P = 4.6, and MSQL-E = 7.5 [41]. Results from the topiramate study report individual minimally important clinical (MIC) change: MSQL-R = 10.9, MSQL-P = 8.3, and MSQL-E = 12.2 [42].
All subjects except one experienced an individual minimally important clinical change for MSQL-R of greater than 10.9 by the week-eight follow-up in MSQL-R. All but two subjects reported changes of more than 12.2 points in MSQL-E. Improvement in MSQL-P scores increased by ten points or more in all subjects.
Regression analysis of VAS ratings over time showed a significant linear improvement over the 3-month period. There was substantial variation in baseline scores across these patients. Little to no variation was observed in the rate of improvement. This trend appears to be the same in the subjects studied for 24 weeks as seen in Figure 12.
Many studies using pharmaceutical intervention have shown a substantial placebo effect in patients from migrainous populations [43]. Determining possible migraine improvement over six months, using another intervention as well as no intervention, is important for any comparison of results. The investigation into placebo effects generally accepts that placebo interventions do provide symptomatic relief but do not modify pathophysiologic processes underlying the condition [44]. Objective MRI measures may help in revealing such a placebo effect by demonstrating a change in physiologic measurements of flow parameters occurring after a placebo intervention.
Use of a three-tesla magnet for MRI data collection would increase the reliability of the measurements by increasing the amount of data used to make the flow and ICCI calculations. This is one of the first investigations using change in ICCI as an outcome in evaluating an intervention. This creates challenges in interpretation of MRI acquired data to base conclusions or further hypothesis development. Variability in relationships between blood flow to and from the brain, CSF flow, and heart rate of these subject-specific parameters has been reported [45]. Variations observed in a small three-subject repeated measures study have led to conclusions that information gathered from individual cases be interpreted with caution [46].
The literature further reports in larger studies significant reliability in collecting these MRI acquired volumetric flow data. Wentland et al. reported that measurements of CSF velocities in human volunteers and of sinusoidally fluctuating phantom velocities did not differ significantly between two MRI techniques used [47]. Koerte et al. studied two cohorts of subjects imaged in two separate facilities with different equipment. They reported that intraclass correlation coefficients (ICC) demonstrated a high intra- and interrater reliability of PC-MRI volumetric flow rate measurements remaining independent of equipment used and skill-level of the operator [48]. While anatomic variation exists between subjects, it has not prevented studies of larger patient populations in describing possible �normal� outflow parameters [49, 50].
Being based solely on patient subjective perceptions, there are limitations in using patient reported outcomes [51]. Any aspect affecting a subject’s perception in their quality of life is likely to influence the outcome of any assessment used. Lack of outcome specificity in reporting symptoms, emotions, and disability also limits interpretation of results [51].
Imaging and MRI data analysis costs precluded use of a control group, limiting any generalizability of these results. A larger sample size would allow for conclusions based on statistical power and reduced Type I error. Interpretation of any significance in these results, while revealing possible trends, remains speculation at best. The big unknown persists in the likelihood that these changes are related to the intervention or to some other effect unknown to the investigators. These results do add to the body of knowledge of previously unreported possible hemodynamic and hydrodynamic changes after a NUCCA intervention, as well as changes in migraine HRQoL patient reported outcomes as observed in this cohort.
The values of collected data and analyses are providing information required for estimation of statistically significant subject sample sizes in further study. Resolved procedural challenges from conducting the pilot allow for a highly refined protocol to successfully accomplish this task.
In this study, the lack of robust increase in compliance may be understood by the logarithmic and dynamic nature of intracranial hemodynamic and hydrodynamic flow, allowing individual components comprising compliance to change while overall it did not. An effective intervention should improve subject perceived pain and disability related to migraine headache as measured by these HRQoL instruments used. These study results suggest that the atlas realignment intervention may be associated with reduction in migraine frequency, marked improvement in quality of life yielding significant reduction in headache-related disability as observed in this cohort. The improvement in HRQoL outcomes creates compelling interest for further study, to confirm these findings, especially with a larger subject pool and a placebo group.
Acknowledgments
The authors acknowledge Dr. Noam Alperin, Alperin Diagnostics, Inc., Miami, FL; Kathy Waters, Study Coordinator, and Dr. Jordan Ausmus, Radiography Coordinator, Britannia Clinic, Calgary, AB; Sue Curtis, MRI Technologist, Elliot Fong Wallace Radiology, Calgary, AB; and Brenda Kelly-Besler, RN, Research Coordinator, Calgary Headache Assessment and Management Program (CHAMP), Calgary, AB. Financial support is provided by (1) Hecht Foundation, Vancouver, BC; (2) Tao Foundation, Calgary, AB; (3) Ralph R. Gregory Memorial Foundation (Canada), Calgary, AB; and (4) Upper Cervical Research Foundation (UCRF), Minneapolis, MN.
Abbreviations
ASC: Atlas subluxation complex
CHAMP: Calgary Headache Assessment and Management Program
CSF: Cerebrospinal Fluid
GSA: Gravity Stress Analyzer
HIT-6: Headache Impact Test-6
HRQoL: Health Related Quality of Life
ICCI: Intracranial compliance index
ICVC: Intracranial volume change
IQR: Interquartile range
MIDAS: Migraine Disability Assessment Scale
MSQL: Migraine-Specific Quality of Life Measure
MSQL-E: Migraine-Specific Quality of Life Measure-Emotional
MSQL-P: Migraine-Specific Quality of Life Measure-Physical
MSQL-R: Migraine-Specific Quality of Life Measure-Restrictive
NUCCA: National Upper Cervical Chiropractic Association
PC-MRI: Phase Contrast Magnetic Resonance Imaging
SLC: Supine Leg Check
VAS: Visual Analog Scale.
Conflict of Interests
The authors declare that there are no financial or any other competing interests regarding the publication of this paper.
Authors’ Contribution
H. Charles Woodfield III conceived the study, was instrumental in its design, helped in coordination, and helped to draft the paper: introduction, study methods, results, discussion, and conclusion. D. Gordon Hasick screened subjects for study inclusion/exclusion, provided NUCCA interventions, and monitored all subjects on follow-up. He participated in study design and subject coordination, helping to draft the Introduction, NUCCA Methods, and Discussion of the paper. Werner J. Becker screened subjects for study inclusion/exclusion, participated in study design and coordination, and helped to draft the paper: study methods, results and discussion, and conclusion. Marianne S. Rose performed statistical analysis on study data and helped to draft the paper: statistical methods, results, and discussion. James N. Scott participated in study design, served as the imaging consultant reviewing scans for pathology, and helped to draft the paper: PC-MRI methods, results, and discussion. All authors read and approved the final paper.
In conclusion, the case study regarding the improvement of migraine headache symptoms following atlas vertebrae realignment demonstrated an increase in the primary outcome, however, the average results of the research study also demonstrated no statistical significance. Altogether, the case study concluded that patients who received atlas vertebrae realignment treatment experienced considerable improvement in symptoms with decreased headache days. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Magoun H. W. Caudal and cephalic influences of the brain stem reticular formation. Physiological Reviews. 1950;30(4):459�474. [PubMed]
2. Gregory R. Manual of Upper Cervical Analysis. Monroe, Mich, USA: National Upper Cervical Chiropractic Association; 1971.
3. Thomas M., editor. NUCCA Protocols and Perspectives. 1st. Monroe, Mich, USA: National Upper Cervical Chiropractic Association; 2002.
4. Grostic J. D. Dentate ligament-cord distortion hypothesis. Chiropractic Research Journal. 1988;1(1):47�55.
5. Alperin N., Sivaramakrishnan A., Lichtor T. Magnetic resonance imaging-based measurements of cerebrospinal fluid and blood flow as indicators of intracranial compliance in patients with Chiari malformation. Journal of Neurosurgery. 2005;103(1):46�52. doi: 10.3171/jns.2005.103.1.0046. [PubMed][Cross Ref]
6. Czosnyka M., Pickard J. D. Monitoring and interpretation of intracranial pressure. Journal of Neurology, Neurosurgery and Psychiatry. 2004;75(6):813�821. doi: 10.1136/jnnp.2003.033126. [PMC free article][PubMed][Cross Ref]
7. Tobinick E., Vega C. P. The cerebrospinal venous system: anatomy, physiology, and clinical implications. MedGenMed: Medscape General Medicine. 2006;8(1, article 153) [PubMed]
8. Eckenhoff J. E. The physiologic significance of the vertebral venous plexus. Surgery Gynecology and Obstetrics. 1970;131(1):72�78. [PubMed]
9. Beggs C. B. Venous hemodynamics in neurological disorders: an analytical review with hydrodynamic analysis. BMC Medicine. 2013;11, article 142 doi: 10.1186/1741-7015-11-142. [PMC free article][PubMed][Cross Ref]
10. Beggs C. B. Cerebral venous outflow and cerebrospinal fluid dynamics. Veins and Lymphatics. 2014;3(3):81�88. doi: 10.4081/vl.2014.1867. [Cross Ref]
11. Cassar-Pullicino V. N., Colhoun E., McLelland M., McCall I. W., El Masry W. Hemodynamic alterations in the paravertebral venous plexus after spinal injury. Radiology. 1995;197(3):659�663. doi: 10.1148/radiology.197.3.7480735. [PubMed][Cross Ref]
12. Damadian R. V., Chu D. The possible role of cranio-cervical trauma and abnormal CSF hydrodynamics in the genesis of multiple sclerosis. Physiological Chemistry and Physics and Medical NMR. 2011;41(1):1�17. [PubMed]
13. Bakris G., Dickholtz M., Meyer P. M., et al. Atlas vertebra realignment and achievement of arterial pressure goal in hypertensive patients: a pilot study. Journal of Human Hypertension. 2007;21(5):347�352. doi: 10.1038/sj.jhh.1002133. [PubMed][Cross Ref]
14. Kumada M., Dampney R. A. L., Reis D. J. The trigeminal depressor response: a cardiovascular reflex originating from the trigeminal system. Brain Research. 1975;92(3):485�489. doi: 10.1016/0006-8993(75)90335-2. [PubMed][Cross Ref]
15. Kumada M., Dampney R. A. L., Whitnall M. H., Reis D. J. Hemodynamic similarities between the trigeminal and aortic vasodepressor responses. The American Journal of Physiology�Heart and Circulatory Physiology. 1978;234(1):H67�H73. [PubMed]
16. Goadsby P. J., Edvinsson L. The trigeminovascular system and migraine: studies characterizing cerebrovascular and neuropeptide changes seen in humans and cats. Annals of Neurology. 1993;33(1):48�56. doi: 10.1002/ana.410330109. [PubMed][Cross Ref]
17. Goadsby P. J., Fields H. L. On the functional anatomy of migraine. Annals of Neurology. 1998;43(2, article 272) doi: 10.1002/ana.410430221. [PubMed][Cross Ref]
18. May A., Goadsby P. J. The trigeminovascular system in humans: pathophysiologic implications for primary headache syndromes of the neural influences on the cerebral circulation. Journal of Cerebral Blood Flow and Metabolism. 1999;19(2):115�127. [PubMed]
19. Goadsby P. J., Hargreaves R. Refractory migraine and chronic migraine: pathophysiological mechanisms. Headache. 2008;48(6):799�804. doi: 10.1111/j.1526-4610.2008.01157.x. [PubMed][Cross Ref]
20. Olesen J., Bousser M.-G., Diener H.-C., et al. The international classification of headache disorders, 2nd edition (ICHD-II)�revision of criteria for 8.2 medication-overuse headache. Cephalalgia. 2005;25(6):460�465. doi: 10.1111/j.1468-2982.2005.00878.x. [PubMed][Cross Ref]
21. Stewart W. F., Lipton R. B., Whyte J., et al. An international study to assess reliability of the Migraine Disability Assessment (MIDAS) score. Neurology. 1999;53(5):988�994. doi: 10.1212/wnl.53.5.988. [PubMed][Cross Ref]
22. Wagner T. H., Patrick D. L., Galer B. S., Berzon R. A. A new instrument to assess the long-term quality of life effects from migraine: development and psychometric testing of the MSQOL. Headache. 1996;36(8):484�492. doi: 10.1046/j.1526-4610.1996.3608484.x. [PubMed][Cross Ref]
23. Kosinski M., Bayliss M. S., Bjorner J. B., et al. A six-item short-form survey for measuring headache impact: the HIT-6. Quality of Life Research. 2003;12(8):963�974. doi: 10.1023/a:1026119331193. [PubMed][Cross Ref]
24. Eriksen K., Rochester R. P., Hurwitz E. L. Symptomatic reactions, clinical outcomes and patient satisfaction associated with upper cervical chiropractic care: a prospective, multicenter, cohort study. BMC Musculoskeletal Disorders. 2011;12, article 219 doi: 10.1186/1471-2474-12-219. [PMC free article][PubMed][Cross Ref]
25. National Upper Cervical Chiropractic Association. NUCCA Standards of Practice and Patient Care. 1st. Monroe, Mich, USA: National Upper Cervical Chiropractic Association; 1994.
26. Gregory R. A model for the supine leg check. Upper Cervical Monograph. 1979;2(6):1�5.
27. Woodfield H. C., Gerstman B. B., Olaisen R. H., Johnson D. F. Interexaminer reliability of supine leg checks for discriminating leg-length inequality. Journal of Manipulative and Physiological Therapeutics. 2011;34(4):239�246. doi: 10.1016/j.jmpt.2011.04.009. [PubMed][Cross Ref]
28. Andersen R. T., Winkler M. The gravity stress analyzer for measuring spinal posture. Journal of the Canadian Chiropractic Association. 1983;2(27):55�58.
29. Eriksen K. Subluxation X-ray analysis. In: Eriksen K., editor. Upper Cervical Subluxation Complex�A Review of the Chiropractic and Medical Literature. 1st. Philadelphia, Pa, USA: Lippincott Williams & Wilkins; 2004. pp. 163�203.
30. Zabelin M. X-ray analysis. In: Thomas M., editor. NUCCA: Protocols and Perspectives. 1st. Monroe: National Upper Cervical Chiropractic Association; 2002. p. p. 10-1-48.
31. Miyati T., Mase M., Kasai H., et al. Noninvasive MRI assessment of intracranial compliance in idiopathic normal pressure hydrocephalus. Journal of Magnetic Resonance Imaging. 2007;26(2):274�278. doi: 10.1002/jmri.20999. [PubMed][Cross Ref]
32. Alperin N., Lee S. H., Loth F., Raksin P. B., Lichtor T. MR-intracranial pressure (ICP). A method to measure intracranial elastance and pressure noninvasively by means of MR imaging: baboon and human study. Radiology. 2000;217(3):877�885. doi: 10.1148/radiology.217.3.r00dc42877. [PubMed][Cross Ref]
33. Raksin P. B., Alperin N., Sivaramakrishnan A., Surapaneni S., Lichtor T. Noninvasive intracranial compliance and pressure based on dynamic magnetic resonance imaging of blood flow and cerebrospinal fluid flow: review of principles, implementation, and other noninvasive approaches. Neurosurgical Focus. 2003;14(4, article E4) [PubMed]
34. Koerte I. K., Schankin C. J., Immler S., et al. Altered cerebrovenous drainage in patients with migraine as assessed by phase-contrast magnetic resonance imaging. Investigative Radiology. 2011;46(7):434�440. doi: 10.1097/rli.0b013e318210ecf5. [PubMed][Cross Ref]
35. Pomschar A., Koerte I., Lee S., et al. MRI evidence for altered venous drainage and intracranial compliance in mild traumatic brain injury. PLoS ONE. 2013;8(2) doi: 10.1371/journal.pone.0055447.e55447 [PMC free article][PubMed][Cross Ref]
36. Bayliss M. S., Batenhorst A. S. The HIT-6 A User’s guide. Lincoln, RI, USA: QualityMetric Incorporated; 2002.
37. Coeytaux R. R., Kaufman J. S., Chao R., Mann J. D., DeVellis R. F. Four methods of estimating the minimal important difference scores were compared to establish a clinically significant change in Headache Impact Test. Journal of Clinical Epidemiology. 2006;59(4):374�380. doi: 10.1016/j.jclinepi.2005.05.010. [PubMed][Cross Ref]
38. Smelt A. F. H., Assendelft W. J. J., Terwee C. B., Ferrari M. D., Blom J. W. What is a clinically relevant change on the HIT-6 questionnaire? An estimation in a primary-care population of migraine patients. Cephalalgia. 2014;34(1):29�36. doi: 10.1177/0333102413497599. [PubMed][Cross Ref]
39. Sauro K. M., Rose M. S., Becker W. J., et al. HIT-6 and MIDAS as measures of headache disability in a headache referral population. Headache. 2010;50(3):383�395. doi: 10.1111/j.1526-4610.2009.01544.x. [PubMed][Cross Ref]
40. Bagley C. L., Rendas-Baum R., Maglinte G. A., et al. Validating migraine-specific quality of life questionnaire v2.1 in episodic and chronic migraine. Headache. 2012;52(3):409�421. doi: 10.1111/j.1526-4610.2011.01997.x. [PubMed][Cross Ref]
41. Cole J. C., Lin P., Rupnow M. F. T. Minimal important differences in the Migraine-Specific Quality of Life Questionnaire (MSQ) version 2.1. Cephalalgia. 2009;29(11):1180�1187. doi: 10.1111/j.1468-2982.2009.01852.x. [PubMed][Cross Ref]
42. Dodick D. W., Silberstein S., Saper J., et al. The impact of topiramate on health-related quality of life indicators in chronic migraine. Headache. 2007;47(10):1398�1408. doi: 10.1111/j.1526-4610.2007.00950.x. [PubMed][Cross Ref]
43. Hr�bjartsson A., G�tzsche P. C. Placebo interventions for all clinical conditions. Cochrane Database of Systematic Reviews. 2010;(1)CD003974 [PubMed]
44. Meissner K. The placebo effect and the autonomic nervous system: evidence for an intimate relationship. Philosophical Transactions of the Royal Society B: Biological Sciences. 2011;366(1572):1808�1817. doi: 10.1098/rstb.2010.0403. [PMC free article][PubMed][Cross Ref]
45. Marshall I., MacCormick I., Sellar R., Whittle I. Assessment of factors affecting MRI measurement of intracranial volume changes and elastance index. British Journal of Neurosurgery. 2008;22(3):389�397. doi: 10.1080/02688690801911598. [PubMed][Cross Ref]
46. Raboel P. H., Bartek J., Andresen M., Bellander B. M., Romner B. Intracranial pressure monitoring: invasive versus non-invasive methods-A review. Critical Care Research and Practice. 2012;2012:14. doi: 10.1155/2012/950393.950393 [PMC free article][PubMed][Cross Ref]
47. Wentland A. L., Wieben O., Korosec F. R., Haughton V. M. Accuracy and reproducibility of phase-contrast MR imaging measurements for CSF flow. American Journal of Neuroradiology. 2010;31(7):1331�1336. doi: 10.3174/ajnr.A2039. [PMC free article][PubMed][Cross Ref]
48. Koerte I., Haberl C., Schmidt M., et al. Inter- and intra-rater reliability of blood and cerebrospinal fluid flow quantification by phase-contrast MRI. Journal of Magnetic Resonance Imaging. 2013;38(3):655�662. doi: 10.1002/jmri.24013. [PMC free article][PubMed][Cross Ref]
49. Stoquart-Elsankari S., Lehmann P., Villette A., et al. A phase-contrast MRI study of physiologic cerebral venous flow. Journal of Cerebral Blood Flow and Metabolism. 2009;29(6):1208�1215. doi: 10.1038/jcbfm.2009.29. [PubMed][Cross Ref]
50. Atsumi H., Matsumae M., Hirayama A., Kuroda K. Measurements of intracranial pressure and compliance index using 1.5-T clinical MRI machine. Tokai Journal of Experimental and Clinical Medicine. 2014;39(1):34�43. [PubMed]
51. Becker W. J. Assessing health-related quality of life in patients with migraine. Canadian Journal of Neurological Sciences. 2002;29(supplement 2):S16�S22. doi: 10.1017/s031716710000189x. [PubMed][Cross Ref]
Headaches can be a real aggravating issue, especially if these begin to occur more frequently. Even more so, headaches can become a bigger problem when the common type of head pain becomes a migraine. Head pain is often a symptom resulting from an underlying injury and/or condition along the cervical spine, or upper back and neck. Fortunately, a variety of treatment methods are available to help treat headaches. Chiropractic care is a well-known alternative treatment option which is commonly recommended for neck pain, headaches and migraines. The purpose of the following research study is to determine the effectiveness of chiropractic spinal manipulative therapy for migraine.
Chiropractic Spinal Manipulative Therapy for Migraine: a Study Protocol of a Single-Blinded Placebo-Controlled Randomised Clinical Trial
Abstract
Introduction
Migraine affects 15% of the population, and has substantial health and socioeconomic costs. Pharmacological management is first-line treatment. However, acute and/or prophylactic medicine might not be tolerated due to side effects or contraindications. Thus, we aim to assess the efficacy of chiropractic spinal manipulative therapy (CSMT) for migraineurs in a single-blinded placebo-controlled randomised clinical trial (RCT).
Method and Analysis
According to the power calculations, 90 participants are needed in the RCT. Participants will be randomised into one of three groups: CSMT, placebo (sham manipulation) and control (usual non-manual management). The RCT consists of three stages: 1?month run-in, 3?months intervention and follow-up analyses at the end of the intervention and 3, 6 and 12?months. The primary end point is migraine frequency, while migraine duration, migraine intensity, headache index (frequency x duration x intensity) and medicine consumption are secondary end points. Primary analysis will assess a change in migraine frequency from baseline to the end of the intervention and follow-up, where the groups CSMT and placebo and CSMT and control will be compared. Owing to two group comparisons, p values below 0.025 will be considered statistically significant. For all secondary end points and analyses, a p value below 0.05 will be used. The results will be presented with the corresponding p values and 95% CIs.
Ethics and Dissemination
The RCT will follow the clinical trial guidelines from the International Headache Society. The Norwegian Regional Committee for Medical Research Ethics and the Norwegian Social Science Data Services have approved the project. Procedure will be conducted according to the declaration of Helsinki. The results will be published at scientific meetings and in peer-reviewed journals.
Trial Registration Number
NCT01741714.
Keywords:Statistics & Research Methods
Strengths and Limitations of this Study
The study will be the first three-armed manual therapy randomised clinical trial (RCT) assessing the efficacy of chiropractic spinal manipulative therapy versus placebo (sham manipulation) and control (continue usual pharmacological management without receiving manual intervention) for migraineurs.
Strong internal validity, since a single chiropractor will conduct all interventions.
The RCT has the potential to provide a non-pharmacological treatment option for migraineurs.
Risk for dropouts is increased due to strict exclusion criteria and 17?months duration of the RCT.
A generally accepted placebo has not been established for manual therapy; thus, there is a risk for unsuccessful blinding, while the investigator who provides the interventions cannot be blinded for obvious reasons.
Background
Migraine is a common health problem with substantial health and socioeconomic costs. On the recent Global Burden of Disease study, migraine was ranked as the third most common condition.[1]
About 15% of the general population have migraine.[2, 3] Migraine is usually unilateral with pulsating and moderate/severe headache which is aggravated by routine physical activity, and is accompanied by photophobia and phonophobia, nausea and sometimes vomiting.[4] Migraine exists in two major forms, migraine without aura and migraine with aura (below). Aura is reversible neurological disturbances of the vision, sensory and/or speech function, occurring prior to the headache. However, intraindividual variations from attack to attack are common.[5, 6] The origin of migraine is debated. The painful impulses may originate from the trigeminal nerve, central and/or peripheral mechanisms.[7, 8] Extracranial pain sensitive structures include the skin, muscles, arteries, periosteum and joints. The skin is sensitive to all usual forms of pain stimuli, while temporal and neck muscles may especially be sources for pain and tenderness in migraine.[9�11] Similarly, the frontal supraorbital, superficial temporal, posterior and occipital arteries are sensitive to pain.[9, 12]
Notes
The International Classification of Headache Disorders-II Diagnostic Criteria for Migraine
Migraine without Aura
A. At least five attacks fulfilling criteria B�D
B. Headache attacks lasting 4�72?h (untreated or unsuccessfully treated)
C. Headache has at least two of the following characteristics:
1. Unilateral location
2. Pulsating quality
3. Moderate or severe pain intensity
4. Aggravated by or causing avoidance of routine physical activity
D. During headache at least one of the following:
1. Nausea and/or vomiting
2. Photophobia and phonophobia
E. Not attributed to another disorder
Migraine with aura
A. At least two attacks fulfilling criteria B�D
B. Aura consisting of at least one of the following, but no motor weakness:
1. Fully reversible visual symptoms including positive features (ie, flickering lights, spots or lines) and/or negative features (ie, loss of vision). Moderate or severe pain intensity
2. Fully reversible sensory symptoms including positive features (ie, pins and needles) and/or negative features (ie, numbness)
2. At least one aura symptom develops gradually over ?5?min and/or different aura symptoms occur in succession over ?5?min
3. Each symptom lasts ?5 and ?60?min
D. Headache fulfilling criteria B-D for 1.1 Migraine without aura begins during the aura or follows the aura within 60?min
E. Not attributed to another disorder
Pharmacological management is the first treatment option for migraineurs. However, some patients do not tolerate acute and/or prophylactic medicine due to side effects or contraindications due to comorbidity of other diseases or due to a wish to avoid medication for other reasons. The risk of medication overuse due to frequent migraine attacks represents a major health hazard with direct and indirect cost concerns. The prevalence of medication overuse headache (MOH) is 1�2% in the general population,[13�15] that is, about half the population suffering chronic headache (15 headache days or more per month) have MOH.[16] Migraine causes loss of 270 workdays per year per 1000 persons from the general population.[17] This corresponds to about 3700 work years lost per year in Norway due to migraine. The economic cost per migraineur was estimated to be $655 in USA and �579 in Europe per year.[18, 19] Owing to the high prevalence of migraine, the total cost per year was estimated to be $14.4 billion in the USA and �27 billion in the EU countries, Iceland, Norway and Switzerland at that time. Migraine costs more than neurological disorders such as dementia, multiple sclerosis, Parkinson’s disease and stroke.[20] Thus, non-pharmacological treatment options are warranted.
The Diversified technique and the Gonstead method are the two most commonly used chiropractic manipulative treatment modalities in the profession, used by 91% and 59%, respectively,[21, 22] along with other manual and non-manual interventions, that is, soft tissue techniques, spinal and peripheral mobilisation, rehabilitation, postural corrections and exercises as well as general nutrition and dietetic advice.
A few spinal manipulative therapy (SMT) randomised controlled trials (RCTs) using the Diversified technique have been conducted for migraine, suggesting an effect on migraine frequency, migraine duration, migraine intensity and medicine consumption.[23�26] However, common for previous RCTs are the methodological shortcomings such as inaccurate headache diagnosis, that is, questionnaire diagnoses used are imprecise,[27] inadequate or no randomisation procedure, lack of placebo group, and primary and secondary end points not prespecified.[28�31] In addition, previous RCTs did not consequently adhere to the recommended clinical guidelines from the International Headache Society (IHS).[32, 33] At present, no RCTs have applied the Gonstead chiropractic SMT (CSMT) method. Thus, considering the methodological shortcomings in previous RCTs, a clinical placebo-controlled RCT with improved methodological quality remains to be conducted for migraine.
The SMT mechanism of action on migraine is unknown. It is argued that migraine might originate from a complexity of nociceptive afferent responses involving the upper cervical spine (C1, C2 and C3), leading to a hypersensitivity state of the trigeminal pathway conveying sensory information for the face and much of the head.[34, 35] Research has thus suggested that SMT may stimulate neural inhibitory systems at different spinal cord levels, and might activate various central descending inhibitory pathways.[36�40] However, although the proposed physiological mechanisms are not fully understood, there are most likely additional unexplored mechanisms which could explain the effect SMT has on mechanical pain sensitisation.
The objective of this study is to assess the efficacy of CSMT versus placebo (sham manipulation) and controls (continue usual pharmacological management without receiving manual intervention) for migraineurs in an RCT.
Method and Design
This is a single-blinded placebo-controlled RCT with three parallel groups (CSMT, placebo and control). Our primary hypothesis is that CSMT gives at least 25% reduction in the average number of migraine days per month (30?days/month) as compared to placebo and control from baseline to the end of intervention, and we expect the same reduction to be maintained at 3, 6 and 12?months follow-up. If the CSMT treatment is effective, it will be offered to participants who received placebo or control after study completion, that is, after 12?months follow-up. The study will adhere to the recommended clinical trial guidelines from the IHS,32 33 and the methodological CONSORT and SPIRIT guidelines.[41, 42]
Patient Population
Participants will be recruited in the period January to September 2013 through the Akershus University Hospital, through general practitioners and media advertisement, that is, posters with general information will be put up at general practitioners� offices along with oral information in the Akershus and Oslo counties, Norway. Participants will receive posted information about the project followed by a short telephone interview. Those recruited from the general practitioners� offices will have to contact the clinical investigator whose contact details have been provided on the posters in order to obtain extensive information about the study.
Eligible participants are between 18 and 70?years of age and have at least one migraine attack per month. Participants are diagnosed according to the diagnostic criteria of the International Classification of Headache Disorders (ICHD-II) by a neurologist at the Akershus University Hospital.[43] They are only allowed to have co-occurrence of tension-type headache and not other primary headaches.
Exclusion criteria are contraindication to SMT, spinal radiculopathy, pregnancy, depression and CSMT within the previous 12?months. Participants whom during the RCT receive any manual interventions by physiotherapists, chiropractors, osteopaths or other health professionals to treat musculoskeletal pain and disability, including massage therapy, joint mobilisation and manipulation,[44] changed their prophylactic headache medicine or pregnancy will be withdrawn from the study at that time and be regarded as dropouts. They are allowed to continue and change their usual acute migraine medication throughout the trial.
In response to initial contact, participants fulfilling the inclusion criteria will be invited to further assessment by the chiropractic investigator. The assessment includes an interview and a physical examination with special emphasis on the whole spinal column. Oral and written information about the project will be provided in advance and oral and written consent will be obtained from all accepted participants during the interview and by the clinical investigator. In accordance with good clinical practice, all patients will be informed about the harms and benefits as well as possible adverse reactions of the intervention primarily including local tenderness and tiredness on the treatment day. No serious adverse events have been reported for the chiropractic Gonstead method.[45, 46] Participants randomised into active or placebo interventions will undergo a full spine radiographic examination and be scheduled for 12 intervention sessions. The control group will not be exposed to this assessment.
Clinical RCT
The clinical RCT consists of a 1?month run-in and 3?months intervention. Time profile will be assessed from baseline to the end of follow-up for all end points (Figure 1).
The participants will fill in a validated diagnostic paper headache diary 1?month prior to intervention which will be used as baseline data for all participants.[47, 48] The validated diary includes questions directly related to the primary and secondary end points. X-rays will be taken in standing position in the anterioposterior and lateral planes of the entire spine. The X-rays will be assessed by the chiropractic investigator.
Randomisation
Prepared sealed lots with the three interventions, that is, active treatment, placebo and the control group, will be subdivided into four subgroups by age and gender, that is, 18�39 and 40�70?years of age and men and women, respectively. Participants will be equally allocated to the three groups by allowing the participant to draw one lot only. The block randomisation will be administrated by an external trained party with no involvement from the clinical investigator.
Intervention
Active treatment consists of CSMT using the Gonstead method,[21] that is, a specific contact, high-velocity, low-amplitude, short-lever spinal with no postadjustment recoil directed to spinal biomechanical dysfunction (full spine approach) as diagnosed by standard chiropractic tests.
The placebo intervention consists of sham manipulation, that is, a broad non-specific contact, low-velocity, low-amplitude sham push manoeuvre in a non-intentional and non-therapeutic directional line. All the non-therapeutic contacts will be performed outside the spinal column with adequate joint slack and without soft tissue pretension so that no joint cavitations occur. In some sessions, the participant lay either prone on a Zenith 2010 HYLO bench with the investigator standing at the participant’s right side with his left palm placed on the participant’s right lateral scapular edge with the other hand reinforcing. In other sessions, the investigator will stand at the participant’s left side and place his right palm over the participant’s left scapular edge with the left hand reinforcing, delivering a non-intentional lateral push manoeuvre. Alternatively, the participant lay in the same side posture position as the active treatment group with the bottom leg straight and the top leg flexed with the top leg’s ankle resting on the bottom leg’s knee fold, in preparation for a side posture push move, which will be delivered as a non-intentional push in the gluteal region. The sham manipulation alternatives will be equally interchanged among the placebo participants according to protocol during the 12-week treatment period to strengthen the study validity. The active and the placebo groups will receive the same structural and motion assessment prior to and after each intervention. No additional cointerventions or advice will be given to participants during the trial period. The treatment period will include 12 consultations, that is, twice per week in the first 3?weeks followed by once a week in the next 2?weeks and once every second week until 12?weeks are reached. Fifteen minutes will be allocated per consultation for each participant. All interventions will be conducted at the Akershus University Hospital and administered by an experienced chiropractor (AC).
The control group will continue usual care, that is, pharmacological management without receiving manual intervention by the clinical investigator. The same exclusion criteria apply for the control group during the whole study period.
Blinding
After each treatment session, the participants who receive active or placebo intervention will complete a de-blinding questionnaire administrated by an external trained independent party with no involvement from the clinical investigator, that is, providing a dichotomous �yes� or �no� answer as to whether active treatment was received. This response was followed by a second question regarding how certain they were that active treatment was received on a 0�10 numeric rating scale (NRS), where 0 represents absolutely uncertain and 10 represents absolutely certainty. The control group and the clinical investigator can for obvious reasons not be blinded.[49, 50]
Follow-Up
Follow-up analysis will be conducted on the end points measured after the end of intervention and at 3, 6 and 12?months follow-up. During this period, all participants will continue to fill in a diagnostic paper headache diary and return it on a monthly basis. In the case of unreturned diary or missing values in the diary, the participants will be contacted immediately on detection to minimise recall bias. Participants will be contacted by phone to secure compliance.
Primary and Secondary End Points
The primary and secondary end points are listed below. The end points adhere to the recommended IHS clinical trial guidelines.[32, 33] We define number of migraine days as the primary end point and expect at least a 25% reduction in average number of days from baseline to the end of intervention, with the same level of reduction being maintained at follow-up. On the basis of previous reviews on migraine, a 25% reduction is considered to be a conservative estimate.[30] A 25% reduction is also expected in secondary end points from baseline to the end of intervention, retaining at follow-up for migraine duration, migraine intensity and headache index, where the index is calculated as number of migraine days (30?days)�average migraine duration (hours per day)�average intensity (0�10 NRS). A 50% reduction in medication consumption from baseline to the end of intervention and to follow-up is expected.
Notes
Primary and Secondary End Points
Primary End Points
1. Number of migraine days in active treatment versus placebo group.
2. Number of migraine days in active treatment versus control group.
Secondary End Points
3. Migraine duration in hours in active treatment versus placebo group.
4. Migraine duration in hours in active treatment versus control group.
5. Self-reported VAS in active treatment versus placebo group.
6. Self-reported VAS in active treatment versus control group.
7. Headache index (frequency x duration x intensity) in active treatment versus placebo group.
8. Headache index in active treatment versus control group.
9. Headache medication dosage in active treatment versus placebo group.
10. Headache medication dosage in active treatment versus control group.
*The data analysis is based on the run-in period versus end of intervention. Point 11�40 will be duplicate of point 1�10 above at 3, 6 and 12?months follow-up, respectively.
Data Processing
A flow chart of the participants is shown in Figure 2. Baseline demographic and clinical characteristics will be tabulated as means and SDs for continuous variables and proportions and percentages for categorical variables. Each of three groups will be described separately. Primary and secondary end points will be presented by suitable descriptive statistics in each group and for each time point. Normality of end points will be assessed graphically and transformation will be considered if necessary.
Change in primary and secondary end points from baseline to the end of intervention and to follow-up will be compared between the active and placebo groups and the active and control groups. The null hypothesis states that there is no significant difference between the groups in average change, while the alternative hypothesis states that a difference of at least 25% exists.
Owing to the follow-up period, repeated recordings of primary and secondary end points will be available, and analyses of trend in primary and secondary end points will be of main interest. Intra-individual correlations (cluster effect) are likely to be present in data with repeated measurements. Cluster effect will thus be assessed by calculating intraclass correlation coefficient quantifying the proportion of total variation attributable to the intraindividual variations. The trend in end points will be assessed by a linear regression model for longitudinal data (linear mixed model) to correctly account for the possible cluster effect. The linear mixed model handles unbalanced data, enabling all available information from randomised patients to be included, as well as from dropouts. Regression models with fixed effects for time component and group allocation as well as the interaction between the two will be estimated. The interaction will quantify possible differences between groups regarding time trend in the end points and serve as an omnibus test. Random effects for patients will be included to adjust the estimates for intraindividual correlations. Random slopes will be considered. The linear mixed models will be estimated by the SAS PROC MIXED procedure. The two pairwise comparisons will be performed by deriving individual time point contrasts within each group with the corresponding p values and 95% CIs.
Both per-protocol and intention-to-treat analyses will be conducted if relevant. All analyses will be performed by a statistician, blinded for group allocation and participants. All adverse effects will also be registered and presented. Participants who experience any sort of adverse effects during the trial period will be entitled to call the clinical investigator on the project cell phone. The data will be analysed with SPSS V.22 and SAS V.9.3. Owing to two group comparisons in the primary end point, p values below 0.025 will be considered statistically significant. For all secondary end points and analyses, a significance level of 0.05 will be used. Missing values might appear in incomplete interview questionnaires, incomplete headache diaries, missed intervention sessions and/or due to dropouts. The pattern of missingness will be assessed and missing values handled adequately.
Power Calculation
Sample size calculations are based on the results in a recently published group comparison study on topiramate.[51] We hypothesise that the average difference in reduction of number of days with migraine per month between the active and the placebo groups is 2.5?days. The same difference is assumed between the active and control groups. SD for reduction in each group is assumed to be equal to 2.5. Under the assumption of, on average, 10 migraine days per month at baseline in each group and no change in the placebo or control group during the study, 2.5?days reduction corresponds to a reduction by 25%. Since primary analysis includes two group comparisons, we set a significance level at 0.025. A sample size of 20 patients is required in each group to detect a statistically significant average difference in reduction of 25% with 80% power. To allow for dropouts, the investigators plan to recruit 120 participants.
Dr. Alex Jimenez’s Insight
“I’ve been recommended to seek chiropractic care for my migraine-type headaches. Is chiropractic spinal manipulative therapy effective for migraine?”�Many different types of treatment options can be utilized to effectively treat migraine, however, chiropractic care is one of the most popular treatment approaches for naturally treating migraine. Chiropractic spinal manipulative therapy�is the traditional high-velocity low-amplitude (HVLA) thrust. Also known as spinal manipulation, a chiropractor performs this chiropractic technique by applying a controlled sudden force to a joint while the body is positioned in a specific way. According to the following article, chiropractic spinal manipulative therapy can effectively help treat migraine.
Discussion
Methodological Considerations
Current SMT RCTs on migraine suggest treatment efficacy regarding migraine frequency, duration and intensity. However, a firm conclusion requires clinical single-blinded placebo-controlled RCTs with few methodological shortcomings.[30] Such studies should adhere to the recommended IHS clinical trial guidelines with migraine frequency as the primary end point and migraine duration, migraine intensity, headache index and medication consumption as secondary end points.[32, 33] The headache index, as well as a combination of frequency, duration and intensity, gives an indication of the total level of suffering. Despite the lack of consensus, the headache index has been recommended as an accepted standard secondary end point.[33, 52, 53] The primary and secondary end points will be collected prospectively in a validated diagnostic headache diary for all participants in order to minimise recall bias.[47, 48] To the best of our knowledge, this is the first prospective manual therapy in a three-armed single-blinded placebo-controlled RCT to be conducted for migraine. The study design adheres to the recommendations for pharmacological RCTs as far as possible. RCTs that include a placebo group and a control group are advantageous to pragmatic RCTs that compare two active treatment arms. RCTs also provide the best approach for producing safety as well as efficacy data.
Unsuccessful blinding is a possible risk to the RCT. Blinding is often difficult as there is no single validated standardised chiropractic sham intervention which can be used as a control group for this date. It is, however, necessary to include a placebo group in order to produce a true net effect of the active intervention. Consensus about an appropriate placebo for a clinical trial of SMT among experts representing clinicians and academics has, however, not been reached.[54] No previous studies have, to the best of our knowledge, validated a successful blinding of a CSMT clinical trial with multiple treatment sessions. We intend to minimise this risk by following the proposed protocol for the placebo group.
The placebo response is furthermore high in pharmacological and assumed similarly high for non-pharmacological clinical studies; however, it might even be higher in manual therapy RCTs were attention and physical contact is involved.[55] Similarly, a natural concern with regard to attention bias will be involved for the control group as it is not being seen by anyone or not seen as much by the clinical investigator as the other two groups.
There are always risks for dropouts due to various reasons. Since the trial duration is 17?months with a 12?month follow-up period, the risk for loss to follow-up is thus enhanced. Co-occurrence of other manual intervention during the trial period is another possible risk, as those who receive manipulation or other manual physical treatments elsewhere during the trial period will be withdrawn from the study and regarded as dropouts at the time of violation.
The external validity of the RCT might be a weakness as there is only one investigator. However, we found that advantageous to multiple investigators, in order to provide similar information to participants in all three groups and manual intervention in the CSMT and the placebo groups. Thus, we intend to eliminate inter-investigator variability which might be present if there are two or more investigators. Although the Gonstead method is the second most commonly used technique among chiropractors, we do not see an issue of concern when it comes to generalisability and external validity. Furthermore, the block randomisation procedure will provide a homogeneous sample across the three groups.
The internal validity is, however, strong by having one treating clinician. It reduces the risk of potential selection, information and experimental biases. Furthermore, the diagnosis of all participants is performed by experienced neurologists and not by questionnaires. A direct interview has higher sensitivity and specificity as compared to a questionnaire.[27] Individual motivational factors which can influence a participant’s perception and personal preferences when treating are both reduced by having one investigator. In addition, the internal validity is further strengthened by a concealed validated randomisation procedure. Since age and genders may play a role in migraine, block randomisation was found necessary to balance arms by age and gender in order to reduce possible age-related and/or gender-related bias.
X-rays demonstrating loss of cervical lordosis as a possible cause for migraine.
Conducting X-rays prior to the active and placebo interventions was found to be applicable in order to visualise posture, joint and disc integrity.[56, 57] Since the total X-ray radiation dose varies from 0.2�0.8?mSv, the radiation exposure was considered low.[58, 59] X-ray assessments were also found to be necessary in order to determine if full spine X-rays are useful in future studies or not.
Since we are unaware of the mechanisms of possible efficacy, and both spinal cord and central descending inhibitory pathways have been postulated, we see no reasons to exclude a full spine treatment approach for the intervention group. It has furthermore been postulated that pain in different spinal regions should not be regarded as separate disorders but rather as a single entity.[60] Similarly, including a full spine approach limits the differentiations between the CSMT and the placebo groups. Thus, it might strengthen the likelihood of successful blinding in the placebo group being achieved. In addition, all the placebo contacts will be performed outside the spinal column, thus minimising a possible spinal cord afferent input.
Innovative and Scientific Value
This RCT will highlight and validate the Gonstead CSMT for migraineurs, which has not previously been studied. If CSMT proves to be effective, it will provide a non-pharmacological treatment option. This is especially important as some migraineurs do not have efficacy of prescript acute and/or prophylactic medications, while others have non-tolerable side effects or comorbidity of other diseases that contradict medication while others wish to avoid medication for various reasons. Thus, if CSMT works, it can really have an impact on migraine treatment. The study also bridges cooperation between chiropractors and physicians, which is important in order to make healthcare more efficient. Finally, our method might be applied in future chiropractic and other manual therapy RCTs on headache.
Ethics and Dissemination
Ethics
The study has been approved by the Norwegian Regional Committee for Medical Research Ethics (REK) (2010/1639/REK) and the Norwegian Social Science Data Services (11�77). The declaration of Helsinki is otherwise followed. All data will be anonymised while participants must give oral and written informed consent. Insurance is provided through �The Norwegian System of Compensation to Patients� (NPE), which is an independent national body set up to process compensation claims from patients who have suffered an injury as a result of treatment under the Norwegian health service. A stopping rule was defined for withdrawing participants from this study in accordance with recommendations in the CONSORT extension for Better Reporting of Harms.[61] If a participant reports to their chiropractor or research staff a severe adverse event, he or she will be withdrawn from the study and referred to their general practitioner or hospital emergency department depending on the nature of the event. The final data set will be available to the clinical investigator (AC), the independent and blinded statistician (JSB) and Study Director (MBR). Data will be stored in a locked cabinet at the Research Centre, Akershus University Hospital, Norway, for 5?years.
Dissemination
This project is due for completion 3?years after the start. Results will be published in peer-reviewed international scientific journals in accordance with the CONSORT 2010 Statement. Positive, negative, as well as inconclusive results will be published. In addition, a written lay summary of the results will be available to study participants on request. All authors should qualify for authorship according to the International Committee of Medical Journal Editors, 1997. Each author should have participated sufficiently in the work to take public responsibility for the content. The final decision on the order of authorship will be decided when the project has been finalised. The results from the study may, moreover, be presented as posters or oral presentations at national and/or international conferences.
Acknowledgments
Akershus University Hospital kindly provided research facilities. Chiropractor Clinic1, Oslo, Norway, performed X-ray assessments.
Footnotes
Contributors: AC and PJT had the original idea for the study. AC and MBR obtained funding. MBR planned the overall design. AC prepared the initial draft and PJT commented on the final version of the research protocol. JSB performed all the statistical analyses. AC, JSB, PJT and MBR were involved in the interpretation and assisted in the revision and preparation of the manuscript. All authors have read and approved the final manuscript.
Funding: The study has received funding from Extrastiftelsen (grant number: 2829002), the Norwegian Chiropractic Association (grant number: 2829001), Akershus University Hospital (grant number: N/A) and University of Oslo in Norway (grant number: N/A).
Competing interests: None declared.
Patient consent: Obtained.
Ethics approval: The Norwegian Regional Committee for Medical Research Ethics approved the project (ID of the approval: 2010/1639/REK).
Provenance and peer review: Not commissioned; externally peer reviewed.
A Randomized Controlled Trial of Chiropractic Spinal Manipulative Therapy for Migraine
Abstract
Objective: To assess the efficacy of chiropractic spinal manipulative therapy (SMT) in the treatment of migraine.
Design: A randomized controlled trial of 6 months’ duration. The trial consisted of 3 stages: 2 months of data collection (before treatment), 2 months of treatment, and a further 2 months of data collection (after treatment). Comparison of outcomes to the initial baseline factors was made at the end of the 6 months for both an SMT group and a control group.
Setting: Chiropractic Research Center of Macquarie University.
Participants: One hundred twenty-seven volunteers between the ages of 10 and 70 years were recruited through media advertising. The diagnosis of migraine was made on the basis of the International Headache Society standard, with a minimum of at least one migraine per month.
Interventions: Two months of chiropractic SMT (diversified technique) at vertebral fixations determined by the practitioner (maximum of 16 treatments).
Main Outcome Measures: Participants completed standard headache diaries during the entire trial noting the frequency, intensity (visual analogue score), duration, disability, associated symptoms, and use of medication for each migraine episode.
Results: The average response of the treatment group (n = 83) showed statistically significant improvement in migraine frequency (P < .005), duration (P < .01), disability (P < .05), and medication use (P< .001) when compared with the control group (n = 40). Four persons failed to complete the trial because of a variety of causes, including change in residence, a motor vehicle accident, and increased migraine frequency. Expressed in other terms, 22% of participants reported more than a 90% reduction of migraines as a consequence of the 2 months of SMT. Approximately 50% more participants reported significant improvement in the morbidity of each episode.
Conclusion: The results of this study support previous results showing that some people report significant improvement in migraines after chiropractic SMT. A high percentage (>80%) of participants reported stress as a major factor for their migraines. It appears probable that chiropractic care has an effect on the physical conditions related to stress and that in these people the effects of the migraine are reduced.
In conclusion, chiropractic spinal manipulative therapy can be used effectively to help treat migraine, according to the research study. Furthermore, chiropractic care improved the individual’s overall health and wellness. The well-being of the human body as a whole is believed to be one of the biggest factors as to why chiropractic care is effective for migraine. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Vos T, Flaxman AD, Naghavi M et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990�2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2163�96. doi:10.1016/S0140-6736(12)61729-2[PubMed]
2. Russell MB, Kristiansen HA, Saltyte-Benth J et al. A cross-sectional population-based survey of migraine and headache in 21,177 Norwegians: the Akershus sleep apnea project. J Headache Pain 2008;9:339�47. doi:10.1007/s10194-008-0077-z[PMC free article][PubMed]
3. Steiner TJ, Stovner LJ, Katsarava Z et al. The impact of headache in Europe: principal results of the Eurolight project. J Headache Pain 2014;15:31 doi:10.1186/1129-2377-15-31[PMC free article][PubMed]
4. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013;33:629�808. doi:10.1177/0333102413485658[PubMed]
5. Russell MB, Iversen HK, Olesen J. Improved description of the migraine aura by a diagnostic aura diary. Cephalalgia 1994;14:107�17. doi:10.1046/j.1468-2982.1994.1402107.x[PubMed]
6. Russell MB, Olesen J. A nosographic analysis of the migraine aura in a general population. Brain 1996;119(Pt 2):355�61. doi:10.1093/brain/119.2.355[PubMed]
7. Olesen J, Burstein R, Ashina M et al. Origin of pain in migraine: evidence for peripheral sensitisation. Lancet Neurol 2009;8:679�90. doi:10.1016/S1474-4422(09)70090-0[PubMed]
8. Amin FM, Asghar MS, Hougaard A et al. Magnetic resonance angiography of intracranial and extracranial arteries in patients with spontaneous migraine without aura: a cross-sectional study. Lancet Neurol 2013;12:454�61. doi:10.1016/S1474-4422(13)70067-X[PubMed]
9. Wolff HGF. Headache and other head pain. 2nd edn Oxford: Oxford University Press, 1963.
10. Jensen K. Extracranial blood flow, pain and tenderness in migraine. Clinical and experimental studies. Acta Neurol Scand Suppl 1993;147:1�8. doi:10.1111/j.1748-1716.1993.tb09466.x[PubMed]
11. Svensson P, Ashina M. Human studies of experimental pain from muscles. In: Olesen J, Tfelt-Hansen P, Welch KMA et al., eds Headache. 3rd edn Lippincott Williams & Wilkins, 2006:627�35.
12. Ray BS, Wolff HG. Experimental studies on headache. Pain sensitive structures of the head and their significance in headache. Arch Surg 1940;41:813�56. doi:10.1001/archsurg.1940.01210040002001
13. Grande RB, Aaseth K, Gulbrandsen P et al. Prevalence of primary chronic headache in a population-based sample of 30- to 44-year-old persons. The Akershus study of chronic headache. Neuroepidemiology 2008;30:76�83. doi:10.1159/000116244[PubMed]
14. Aaseth K, Grande RB, Kvaerner KJ et al. Prevalence of secondary chronic headaches in a population-based sample of 30�44-year-old persons. The Akershus study of chronic headache. Cephalalgia 2008;28:705�13. doi:10.1111/j.1468-2982.2008.01577.x[PubMed]
16. Lundqvist C, Grande RB, Aaseth K et al. Dependence scores predict prognosis of medication overuse headache: a prospective cohort from the Akershus study of chronic headache. Pain 2012;153:682�6. doi:10.1016/j.pain.2011.12.008[PubMed]
17. Rasmussen BK, Jensen R, Olesen J. Impact of headache on sickness absence and utilisation of medical services: a Danish population study. J Epidemiol Community Health 1992;46:443�6. doi:10.1136/jech.46.4.443[PMC free article][PubMed]
18. Hu XH, Markson LE, Lipton RB et al. Burden of migraine in the United States: disability and economic costs. Arch Intern Med 1999;159:813�18. doi:10.1001/archinte.159.8.813[PubMed]
20. Andlin-Sobocki P, Jonsson B, Wittchen HU et al. Cost of disorders of the brain in Europe. Eur J Neurol 2005;12(Suppl 1):1�27. doi:10.1111/j.1468-1331.2005.01202.x[PubMed]
24. Parker GB, Pryor DS, Tupling H. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine. Aust NZ J Med 1980;10:192�8. doi:10.1111/j.1445-5994.1980.tb03712.x[PubMed]
25. Nelson CF, Bronfort G, Evans R et al. The efficacy of spinal manipulation, amitriptyline and the combination of both therapies for the prophylaxis of migraine headache. J Manipulative Physiol Ther 1998;21:511�19. [PubMed]
26. Tuchin PJ, Pollard H, Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine. J Manipulative Physiol Ther 2000;23:91�5. doi:10.1016/S0161-4754(00)90073-3[PubMed]
28. Vernon HT. The effectiveness of chiropractic manipulation in the treatment of headache: an exploration in the literature. J Manipulative Physiol Ther 1995;18:611�17. [PubMed]
29. Fernandez-de-las-Penas C, Alonso-Blanco C, San-Roman J et al. Methodological quality of randomized controlled trials of spinal manipulation and mobilization in tension-type headache, migraine, and cervicogenic headache. J Orthop Sports Phys Ther 2006;36:160�9. doi:10.2519/jospt.2006.36.3.160[PubMed]
31. Chaibi A, Russell MB. Manual therapies for primary chronic headaches: a systematic review of randomized controlled trials. J Headache Pain 2014;15:67 doi:10.1186/1129-2377-15-67[PMC free article][PubMed]
32. Tfelt-Hansen P, Block G, Dahlof C et al. International Headache Society Clinical Trial Subcommittee. Guidelines for controlled trials of drugs in migraine: second edition. Cephalalgia 2000;20:765�86. doi:10.1046/j.1468-2982.2000.00117.x[PubMed]
33. Silberstein S, Tfelt-Hansen P, Dodick DW et al. , Task Force of the International Headache Society Clinical Trial Subcommittee . Guidelines for controlled trials of prophylactic treatment of chronic migraine in adults. Cephalalgia 2008;28:484�95. doi:10.1111/j.1468-2982.2008.01555.x[PubMed]
34. Kerr FW. Central relationships of trigeminal and cervical primary afferents in the spinal cord and medulla. Brain Res 1972;43:561�72. doi:10.1016/0006-8993(72)90408-8[PubMed]
36. McLain RF, Pickar JG. Mechanoreceptor endings in human thoracic and lumbar facet joints. Spine (Phila Pa 1976) 1998;23:168�73. doi:10.1097/00007632-199801150-00004[PubMed]
37. Vernon H. Qualitative review of studies of manipulation-induced hypoalgesia. J Manipulative Physiol Ther 2000;23:134�8. doi:10.1016/S0161-4754(00)90084-8[PubMed]
38. Vicenzino B, Paungmali A, Buratowski S et al. Specific manipulative therapy treatment for chronic lateral epicondylalgia produces uniquely characteristic hypoalgesia. Man Ther 2001;6:205�12. doi:10.1054/math.2001.0411[PubMed]
39. Boal RW, Gillette RG. Central neuronal plasticity, low back pain and spinal manipulative therapy. J Manipulative Physiol Ther 2004;27:314�26. doi:10.1016/j.jmpt.2004.04.005[PubMed]
40. De Camargo VM, Alburquerque-Sendin F, Berzin F et al. Immediate effects on electromyographic activity and pressure pain thresholds after a cervical manipulation in mechanical neck pain: a randomized controlled trial. J Manipulative Physiol Ther 2011;34:211�20. doi:10.1016/j.jmpt.2011.02.002[PubMed]
41. Moher D, Hopewell S, Schulz KF et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c869 doi:10.1136/bmj.c869[PMC free article][PubMed]
42. Hoffmann TC, Glasziou PP, Boutron I et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348:g1687 doi:10.1136/bmj.g1687[PubMed]
43. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia 2004;24(Suppl 1):9�10. doi:10.1111/j.1468-2982.2003.00824.x[PubMed]
44. French HP, Brennan A, White B et al. Manual therapy for osteoarthritis of the hip or knee – a systematic review. Man Ther 2011;16:109�17. doi:10.1016/j.math.2010.10.011[PubMed]
45. Cassidy JD, Boyle E, Cote P et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine (Phila Pa 1976) 2008;33(4Suppl):S176�S83. doi:10.1097/BRS.0b013e3181644600[PubMed]
47. Russell MB, Rasmussen BK, Brennum J et al. Presentation of a new instrument: the diagnostic headache diary. Cephalalgia 1992;12:369�74. doi:10.1111/j.1468-2982.1992.00369.x[PubMed]
48. Lundqvist C, Benth JS, Grande RB et al. A vertical VAS is a valid instrument for monitoring headache pain intensity. Cephalalgia 2009;29:1034�41. doi:10.1111/j.1468-2982.2008.01833.x[PubMed]
49. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials 2004;25:143�56. doi:10.1016/j.cct.2003.10.016[PubMed]
51. Silberstein SD, Neto W, Schmitt J et al. Topiramate in migraine prevention: results of a large controlled trial. Arch Neurol 2004;61:490�5. doi:10.1001/archneur.61.4.490[PubMed]
52. Bendtsen L, Jensen R, Olesen J. A non-selective (amitriptyline), but not a selective (citalopram), serotonin reuptake inhibitor is effective in the prophylactic treatment of chronic tension-type headache. J Neurol Neurosurg Psychiatry 1996;61:285�90. doi:10.1136/jnnp.61.3.285[PMC free article][PubMed]
53. Hagen K, Albretsen C, Vilming ST et al. Management of medication overuse headache: 1-year randomized multicentre open-label trial. Cephalalgia 2009;29:221�32. doi:10.1111/j.1468-2982.2008.01711.x[PubMed]
54. Hancock MJ, Maher CG, Latimer J et al. Selecting an appropriate placebo for a trial of spinal manipulative therapy. Aust J Physiother 2006;52:135�8. doi:10.1016/S0004-9514(06)70049-6[PubMed]
55. Meissner K, Fassler M, Rucker G et al. Differential Effectiveness of Placebo Treatments: A Systematic Review of Migraine Prophylaxis. JAMA Inter Med 2013;173:1941�51. doi:10.1001/jamainternmed.2013.10391[PubMed]
56. Taylor JA. Full-spine radiography: a review. J Manipulative Physiol Ther 1993;16:460�74. [PubMed]
57. International Chiropractic Assocoation Practicing Chiropractors� Committee on Radiology Protocols (PCCRP) for biomechanical assessment of spinal subluxation in chiropractic clinical practice. Secondary International Chiropractic Assocoation Practicing Chiropractors� Committee on Radiology Protocols (PCCRP) for biomechanical assessment of spinal subluxation in chiropractic clinical practice 2009. http://www.pccrp.org/
58. Cracknell DM, Bull PW. Organ dosimetry in spinal radiography: a comparison of 3-region sectional and full-spine techniques. Chiropr J Austr 2006;36:33�9.
59. Borretzen I, Lysdahl KB, Olerud HM. Diagnostic radiology in Norway trends in examination frequency and collective effective dose. Radiat Prot Dosimetry 2007;124:339�47. doi:10.1093/rpd/ncm204[PubMed]
60. Leboeuf-Yde C, Fejer R, Nielsen J et al. Pain in the three spinal regions: the same disorder? Data from a population-based sample of 34,902 Danish adults. Chiropr Man Ther 2012;20:11 doi:10.1186/2045-709X-20-11[PMC free article][PubMed]
61. Ioannidis JP, Evans SJ, Gotzsche PC et al. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Ann Intern Med 2004;141:781�8. doi:10.7326/0003-4819-141-10-200411160-00009[PubMed]
Defeat Chronic Pain: If you are one of the estimated 50 to 100 million Americans who struggles with Chronic Pain, you are aware of just how miserable and life-altering it can be. There is not a single area of you life that remains unaffected. You no longer sleep well. Your SEX LIFE is non-existent. Everyday activities have become your own personal �Mount Everest �. You cannot concentrate because the pain IS ALWAYS ON YOUR MIND. It is wearing you out, physically, mentally, and emotionally. It’s sapping your ability to think clearly or make decisions. In short we’re here to defeat chronic pain.
People can see the pain on your face and in your eyes. Chronic Pain and the inability to do the things you love, is making you feel DEPRESSED (not the other way around like your doctor may have suggested). Recent studies have even shown that brains of people suffering with Chronic Pain, show patterns of atrophy that are virtually indistinguishable from what is seen in patients with dementia or ALZHEIMER’S. In fact, a recent study from a prominent Canadian University showed that Chronic Pain causes the brain to degenerate at almost 10 times the rate of someone without pain!
Although Chronic Pain may seem hopeless, there are some things that you can do to help yourself � even though your doctor undoubtedly failed to educate you in this regard. Some of the most basic of these include eating only healthy foods (I recommend a PALEO DIET), taking only WHOLE FOOD SUPPLEMENTS, drinking more WATER, giving up the CIGARETTES, and EXERCISING to the degree that you can (difficult when suffering with Chronic Pain or FIBROMYALGIA).
Although DOING THESE SIMPLE THINGS will certainly help a large percentage who suffer and be able to defeat chronic pain; there is a significant percentage of you whose pain is not greatly diminished by these measures. It is for you that I created this website. But before we move on to treatment of Chronic Pain, you must first understand what Chronic Pain is and how it really works.
Defeat Chronic Pain: It Works Like This
For years, neuro-scientists have known that Chronic Pain can cause brain atrophy (shrinkage) that is indistinguishable from Alzheimer�s or Dementia. More recently, the prestigious Journal of Neuroscience reported research from McGill University showing that, “The longer the individual has had Fibromyalgia, the greater the gray matter loss, with each year of Fibromyalgia being equivalent to 9.5 times the loss in normal aging”. Think about this statement for a moment. Every single year you live with some sort of CHRONIC PAIN SYNDROME (or syndromes as the case may be) is the equivalent of nearly 10 times the brain loss seen in the normal aging process. Re-read this paragraph until the urgency of your situation sinks in!
Although there are several types of pain (the study of Chronic Pain can get extremely complex), we are going to try and keep this as simple as possible. For our purposes, there are two types of Chronic Pain. It has to do with where the pain comes from. Chronic Pain originates in one of the two following areas.
The Central Nervous System
The Body
As we will discuss shortly, Chronic Pain that arises in the CNS is frequently ‘learned’ pain. Let me explain. In order to learn how to SHOOT FREE THROWS, use chop sticks, PLAY THE PIANO, speak Swahili, you have to practice. Everyone remembers the old adage; Practice makes Perfect. If you stimulate pain pathways in the Brain & Nervous System long enough, or are exposed to enough stressors in your life (CHEMICAL, AUTOIMMUNE, EMOTIONAL, DIETARY, FOOD SENSITIVITIES, PHYSICAL, BACTERIAL, VIRAL, PARASITIC, FUNGAL, MOLD, ELECTROMAGNETIC, etc), you can alter the way your Brain and Central Nervous System function.
Hopefully your pain, even though severe, is still Type II (THE THREE TYPES OF PAIN). As people start losing control of numerous areas of physiology (DIGESTION, HORMONAL, IMMUNITY, BLOOD SUGAR REGULATION, HYPERSENSITIVITY, DYSBIOSIS, etc), the problems ramp up. Over time this pain can (will) become locked into the brain. Although pathological Pain Syndromes arising from a malfunctioning CNS are not the most common causes of Chronic Pain, if this is where you are at, you are going to have to find a way to deal with these underlying issues (FUNCTIONAL NEUROLOGY can be a fantastic starting point). Although I provide information that helps many people help themselves with the severe metabolic and neurological problems, this website is chiefly devoted to defeat chronic Pain that is not locked into the Brain, but is instead originating from the body (Type II Pain).
Defeat Chronic Pain: Nociception
“Simple Nociception” is the most basic type of pain. If someone steps on your toe, it hurts. This is normal, and means that your nervous system is functioning properly. Get the person off your toe, and the pain goes away — almost immediately. Simple. There are several different types of Nociceptive Pain, but the one that we are most concerned about on this website is the one that has to do with ‘deep’ musculoskeletal pain, otherwise known as Deep Somatic Pain (Greek �Soma� = body). Deep Somatic Pain is pain that originates in tissues that are considered to be ‘deep’ in the body. Although we do not always think of many of these tissue types as being deep, this category includes things like LIGAMENTS, TENDONS, MUSCLES, FASCIA, blood vessels, and bones. There are two main types of Nociceptors, chemical and mechanical.
I. Chemical Nociception
The Chemical Nociceptors are stimulated by noxious chemicals. The chief of these are the chemicals we collectively refer to as INFLAMMATION (bear in mind that once Inflammation is involved, we begin moving away from Type I pain and into Type II pain — Nociception is still involved, but so is the Inflammatory Cascade). Inflammation is actually made up of a large group of chemicals manufactured within your body as part of the normal Immune System response. They have names like prostaglandins, leukotrienes, histamines, cytokines, kinins, etc, etc, etc. When these chemicals are out of increased beyond what’s needed for normal tissue repair, the result will be a whole host of health problems —- and Chronic Pain.
Although “SYSTEMIC INFLAMMATION” is at the root of the vast majority of America’s health problems (DIABETES, CANCER, FIBROMYALGIA, THYROID PROBLEMS, ARTHRITIS, HEART DISEASE, and numerous others), you will soon see that even though Inflammation is always involved with the tissues of the “Deep Soma,” it sometimes gets more credit than it deserves. However, you also have to be aware that exposing MICROSCOPIC SCAR TISSUE to chronic inflammation can potentially hyper-sensitize nerves. This hypersensitization makes the nerves within Scar Tissue as much as 1,000 times more pain sensitive than normal (the work of the famous neurologist, DR. CHAN GUNN).
INCREASED TISSUE ACIDITY (usually caused by hypoxia — diminished tissue oxygen levels) is another common form of Chemical Nociception. This frequently occurs as the result of a JUNKY DIET, but is also caused by relentless Mechanical / Neurological / Immune System Dysfunction. It is a big reason that my Decompression Protocols utilize OXYGEN THERAPY extensively.
II. Mechanical Nociception
As you can imagine, Mechanical Dysfunction stimulates the Mechanical Nociceptors. This group of nociceptors (pain receptors) is stimulated by constant mechanical stress in the tissues of the Deep Soma — particularly ligaments, tendons, and fascia. Mechanical tension, mechanical deformation, mechanical pressure, etc are the things that cause Mechanical Nociception, which can in turn, cause pain — chronic, unrelenting, pain. Remove the offending mechanical stressor, and you can oftentimes remove the pain. Sounds simple, doesn�t it? Unfortunately, nothing is ever quite as simple as it initially appears.
Be aware that Nociceptive Pain can actually become Brain-Based over time. This is called ‘Supersensitivity’ and is caused by alterations in the Brain and Central Nervous System that perpetuate the pain cycle (many in the medical community are calling it CENTRALIZATION OR CENTRAL SENSITIZATION. In Mechanical Nociception, even though the injured tissue has, according to all of the medical tests, HEALED, it has healed improperly; i.e. microscopic scar tissue and tissue adhesion — particularly in the FASCIA. I probably do not need to tell you that this can be really really bad news — particularly because it is a significant feature of what I call “CHRONIC PAIN’S PERFECT STORM“.
As nerve function and PROPRIOCEPTION become increasingly fouled up, degenerative arthritis and joint deterioration begin to set in (HERE). Because of involvement in the Brain or Central Nervous System, this kind of pain is often referred to as Neuropathic Pain or Neruogenic Pain. Sometimes people end up with HYPERALGIA (Extreme sensitivity to pain. Stimulus that should cause a little pain, causes extraordinary amounts of pain). Or they end up with ALLODYNIA (Stimulus which do not normally elicit any pain at all, now causes pain). Sometimes these two overlap. Stay with me and you will begin to understand why.
Defeat Chronic Pain: Hypersensitized Nerves Relationship To Injured Or Damaged Fascia
Think of nerve endings as the twigs at the very end of a tree limb. Nerves (just like a tree) begin with a large trunk, which splits / divides into smaller and smaller branches until eventually you arrive at the end � the tiny twig (or nerve ending) at the end of the very smallest branches.
If you have ever seen a �topped� tree, you can understand what happens to nerve endings that are found in microscopic scar tissue. Professional Tree Trimmers cut (or �top�) the largest branches just above where the trunk splits into two or three limbs. What happens to these stubs? Instead of having limbs that continue to branch out and divide into ever-smaller limbs in a normal fashion, you get a stub or stump, that in a short matter of time, swells up and has hundreds of tiny twig-like limbs growing from it. �Topping� stimulates the growth of twigs from the stump. The injured nerves found in microscopic scar tissue act in much the same way.
As the larger nerves that are found in soft tissues are injured, you end up with an inordinate number of immature nerve endings (twigs) growing out of an inflamed nerve �stump�. As you might imagine, extra pain receptors are never a good thing! And because there in Inflammation present, this often leads to Microscopic Scar Tissue, which, even though it is up to 1,000 times more pain-sensitive than normal tissue, cannot be seen with even the most technologically advance imaging techniques such as CT / MRI (HERE). This is a commonly seen phenomenon in Facial Adhesions, and is why even though the people living this nightmare believe that because their pain is so severe that it should make their MRI “Glow Red”, it shows nothing. This tends to lead to deer-in-the-headlight looks when you ask your doctor what might be causing your pain, not to mention accusations of malingering, drug seeking, or attempting to get on Disability.
Defeat Chronic Pain: Nerves Are Like Tree Branches
Uninjured Nerves
Photo by Stephen McCulloch
Injured Nerves
Photo by Linda Bailey
Defeat Chronic Pain: Fascial Adhesions
Microscopic Scar Tissue & Chronic Pain
One of the biggest revelations for many people suffering with Chronic Pain is the absurd numbers of CHRONIC PAINSYNDROMES brought on by microscopic scarring of the FASCIA. It gets even worse once you realize that this Fascia is the most pain-sensitive tissue in the body —- yet it does not show up on even the most technologically advanced imaging techniques, including MRI. Simply read our “Fascia” page to see why microscopic scarring of this specific “Connective Tissue” is at the root of all sorts of Chronic Pain Cases — not to mention ILL HEALTH.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine