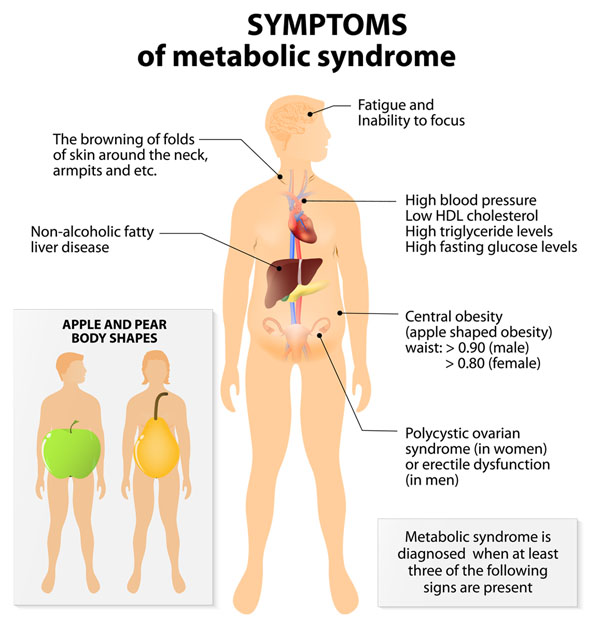
Metabolic syndrome is the term for a group of risk factors like heart disease, diabetes, along with other health issues. The number of individuals dealing with the condition could be as high as 1 in 4. An individual can have one risk factor but most have several in combination. When there are three of these risk factors it becomes metabolic syndrome. The syndrome is a collection of conditions, that culminate in a correlative diagnosis. Risk factors/Symptoms include some or all of the following:
If left untreated and continued poor life choices that include unhealthy diet, lack of physical activity/exercise, and habit formation an individual can die from complications of the syndrome. The condition requires clinical treatment and medical assistance, however, chiropractic has been seen as a viable way to help treat the syndrome.
Causes
The syndrome can have several causes that progress together:
Age the risk goes up as an individual gets older
Genetics and family history
Weight issues
Physical inactivity
Insulin resistance, a condition where the body can’t use insulin properly
The resistance can lead to high blood sugar levels
Individuals with metabolic syndrome tend to have excessive blood clotting and inflammation throughout the body. However, research has not shown whether these conditions cause the syndrome or worsen it.
Chiropractic
Chiropractic�s role is to stabilize the spine and the body. Too much weight leads to spinal dislocation and vertebral compression issues. This can lead to nerve impingement and disc problems. Even a small subluxation can turn into an extreme condition/s with widespread symptoms. Individuals that are overweight require a spinal realignment in order to gain proper stability. A chiropractor will administer corrective adjustments to generate the body’s natural healing process in the affected areas.
Restoring the nerve pathways will promote better blood flow and nutrient delivery to and through the spine. Chiropractic will set the tone for a metabolic syndrome reversal. The second phase of treatment will look at diet and exercise. This serves a dual purpose of introducing proper nutrition to the body, encouraging weight loss, and conditioning the individual’s mindset for the lifestyle adjustments/changes. A healthy/balanced spine will help those with metabolic syndrome get a proper foothold on turning their poor lifestyle into a healthy one.
Reversal
The syndrome can be reversed with the right treatment approach. Usually, this begins with weight loss. Once the weight begins to reduce the secondary benefits kick in. This includes a reduction in blood pressure and a decrease in triglycerides. Once an individual’s spine is stable, they will then be educated on how to adapt and apply a long-term plan to maintain healthy habits for diet, physical activity, sleep, and stress relief strategies. As chiropractors focus on whole-body wellness, treatment plans will also look at:
Remember, the spine is the root of the body. The key to wellness is total body balance. All-natural chiropractic medicine can help achieve optimal health.
Weight Loss Doctor of Chiropractic
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Samson, Susan L, and Alan J Garber. �Metabolic syndrome.��Endocrinology and metabolism clinics of North America�vol. 43,1 (2014): 1-23. doi:10.1016/j.ecl.2013.09.009
Fructose is one of the main components of added sugar. It is a simple type of sugar that makes up about 50 percent of table sugar or sucrose. Table sugar is also made up of glucose or the main energy source of the human body. However, fructose needs to be turned into glucose by the liver before it can be used as fuel for energy by our cells. Fructose, sucrose, and glucose are all naturally found in fruits, vegetables, dairy products, and whole grains as well as in many processed foods. The effects of this simple sugar on our health have been a controversial topic for many years. Research studies are starting to demonstrate the connection between fructose and obesity, diabetes, and even cancer.
What is Fructose?
Fructose, also referred to as fruit sugar, is a monosaccharide or simple sugar like glucose. It’s naturally found in fruits, most root vegetables, agave, and honey. Moreover, it’s commonly added to processed foods as high-fructose corn syrup. The fructose used in high-fructose corn syrup mainly comes from corn, sugar beets, and sugar cane. High-fructose corn syrup is made from cornstarch and it has more of this simple sugar than glucose, compared to regular corn syrup. Fructose has the sweetest taste of the three sugars. It is digested and absorbed differently by the human body. Because monosaccharides are simple sugars, they don’t need to be broken down to be used as fuel for energy by our cells.
Natural foods that are high in fructose can include:
apples
apple juice
pears
prunes
dry figs
sorghum
asparagus
Jerusalem artichokes
chicory roots
leeks
onions
caramel
licorice
molasses
agave syrup
honey
Similar to glucose, fructose is absorbed directly into the bloodstream through the small intestine. Healthcare professionals have found that fructose has the least impact on blood sugar levels. It increases blood sugar levels much more gradually than glucose does and it doesn’t seem to immediately affect insulin levels. However, although this simple sugar has the least impact on blood sugar levels than any of the other simple types of sugars, it may ultimately cause more long-term negative effects on the human body. Fructose needs to be turned into glucose by the liver before it can be used as fuel for energy by our cells. Eating excess fructose can increase triglycerides and lead to metabolic syndrome.
Why is Fructose Bad for You?
When people eat a diet that is high in calories and processed foods with lots of high-fructose corn syrup, the liver can become overwhelmed and start turning fructose into fat. Research studies are starting to demonstrate the connection between this simple sugar and an increased risk of developing a variety of health issues, including obesity, type 2 diabetes, and even cancer. Many healthcare professionals also believe that eating excess fructose is one of the main causes of metabolic disorders. However, there currently isn’t enough evidence to demonstrate the full extent to which fructose can contribute to these health issues. Nevertheless, numerous research studies have justified these controversial concerns.
Research studies have demonstrated that eating excess fructose can increase LDL or bad cholesterol which may lead to fat accumulation around the organs and heart disease. As a result, evidence showed that the deposition of fat in the liver due to the negative effects of this simple sugar can also result in non-alcoholic fatty liver disease. Eating excess fructose may also affect body fat regulation. Other research studies have demonstrated that because fructose doesn’t suppress appetite as much as other types of sugars do, it can promote overeating which may lead to obesity, insulin resistance, and type 2 diabetes. Furthermore, evidence has demonstrated that fructose can increase uric acid levels and cause gout.
For information regarding if fructose is bad for your health, please review the following article:
AS PREVIOUSLY MENTIONED IN THE FOLLOWING ARTICLE, FRUCTOSE IS ONE OF THE MAIN COMPONENTS OF ADDED SUGAR. IT IS A SIMPLE SUGAR THAT MAKES UP APPROXIMATELY 50 PERCENT OF TABLE SUGAR OR SUCROSE. TABLE SUGAR ALSO CONSISTS OF GLUCOSE OR THE MAIN ENERGY SOURCE OF THE HUMAN BODY. HOWEVER, FRUCTOSE NEEDS TO BE CONVERTED INTO GLUCOSE BY THE LIVER BEFORE IT CAN BE UTILIZED AS FUEL FOR ENERGY BY OUR CELLS. FRUCTOSE, SUCROSE, AND GLUCOSE ARE ALL NATURALLY FOUND IN SEVERAL FRUITS, VEGETABLES, DAIRY PRODUCTS, AND WHOLE GRAINS AS WELL AS IN MANY PROCESSED FOODS. THE EFFECTS OF THIS SIMPLE SUGAR ON OUR HEALTH HAVE BEEN A CONTROVERSIAL TOPIC FOR MANY YEARS. RESEARCH STUDIES ARE STARTING TO DEMONSTRATE THE CONNECTION BETWEEN FRUCTOSE AND OBESITY, DIABETES, AND EVEN CANCER. IN THE FOLLOWING ARTICLE, WE DISCUSS IF FRUCTOSE IS BAD FOR YOUR HEALTH. DRINKING SMOOTHIES ADD A HEALTHY NUTRITIONAL BOOST.� -�DR. ALEX JIMENEZ D.C., C.C.S.T. INSIGHTS
Sweet and Spicy Juice
Servings: 1 Cook time: 5-10 minutes
� 1 cup honeydew melons
� 3 cups spinach, rinsed
� 3 cups Swiss chard, rinsed
� 1 bunch cilantro (leaves and stems), rinsed
� 1-inch knob of ginger, rinsed, peeled, and chopped
� 2-3 knobs whole turmeric root (optional), rinsed, peeled, and chopped
Juice all ingredients in a high-quality juicer. Best served immediately.
Red peppers have almost 2.5 times more vitamin C than oranges
Citrus fruits like oranges are a great source of vitamin C, however, there are other fruits and vegetables that offer an even better boost of this essential nutrient. Just half a red pepper, eaten raw, offers more than your requirement of vitamin C for the day, according to healthcare professionals. Cut it into crudit�s for a healthy mid-morning or afternoon snack. Red peppers are also rich in a variety of other essential nutrients, including vitamin A, B6, folate, and antioxidants!
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas*& New Mexico*�
Curated by Dr. Alex Jimenez D.C., C.C.S.T.
References:
Gunnars, Kris. �Is Fructose Bad for You? The Surprising Truth.� Healthline, Healthline Media, 23 Apr. 2018, www.healthline.com/nutrition/why-is-fructose-bad-for-you#section1.
Nall, Rachel. �Is Fructose Bad for You? Benefits, Risks, and Other Sugars.� Medical News Today, MediLexicon International, 28 Nov. 2018, www.medicalnewstoday.com/articles/323818.
Groves, Melissa. �Sucrose vs Glucose vs Fructose: What’s the Difference?� Healthline, Healthline Media, 8 June 2018, www.healthline.com/nutrition/sucrose-glucose-fructose.
Rizkalla, Salwa W. �Health Implications of Fructose Consumption: A Review of Recent Data.� National Center for Biotechnology Information, BioMed Central, 4 Nov. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC2991323/.
Daniluk, Julie. �5 Health Benefits of Red Peppers. Plus, Our World’s Healthiest Pizza Recipe.� Chatelaine, 26 Feb. 2016, www.chatelaine.com/health/healthy-recipes-health/five-health-benefits-of-red-peppers/.
If you are experiencing any of these situations, then you might want to try astaxanthin.
The body needs specific vitamins, minerals, and supplements from food, in order to function correctly. The variety of these nutrients can be found in healthy foods like fruits, vegetables, lean meats, and whole grains are precisely what the body needs. One of the essential nutrients that the body needs is antioxidants. Antioxidants help the body get rid of free radicals that can cause the body to become overly stressed and leading it to develop chronic illnesses. There is an antioxidant that can help the body and can be found in berries and pomegranates, and it is called astaxanthin.
Astaxanthin
Astaxanthin is a xanthophyll carotenoid that can be found in various microorganisms and marine animals. Astaxanthin is common for humans to apply and consume into the body while also being different. This red, fat-soluble pigment is quite different from the other kinds of food that contain carotenoids. Astaxanthin surprising does not contain vitamin A like all the other food containing carotenoids, and astaxanthin is an impressive antioxidant. Studies have shown that astaxanthin can not only be beneficial for the eyes but can provide nutritional support as well as having potential health-promoting effects in preventing and treating various diseases that can harm the body. Some of the various diseases that can harm the body when there is an excessive amount of free radicals can include:
Various cancers
Chronic inflammatory diseases
Metabolic syndrome
Diabetes
Gastrointestinal diseases
Another study found that astaxanthin was superior to fish oil due to astaxanthin having the ability to enhance the body’s immune response and thus lowering the risk of vascular and infectious diseases that can harm the body, causing it to dysfunction.
A Powerful Antioxidant
There are some fantastic beneficial properties that astaxanthin can provide for the body and help improve the body�s systems as well.
Astaxanthin is a powerful antioxidant since various chronic diseases are rooted in a disproportionate balance of reactive oxygen and nitrogen species to antioxidants. Studies have shown�that astaxanthin has been known to scavenge free radicals more effectively out of the body than beta-carotene. There was another study showing how the body�s DNA was damage due to low plasma 8 -OHdG (8-hydroxy-2′-deoxyguanosine) levels.
Boosts the Immune System
The publication of the immunomodulatory effects of astaxanthin is not getting enough attention as they should be. A test study has reported that dietary astaxanthin was able to stimulate mitogen-induced lymphocyte proliferation. This will help increase the natural killer cell cytotoxicity and even delay the hypersensitivity response in the body while also increasing the numbers of total T and B cells in the peripheral blood in the body. Another study showed how astaxanthin could help significantly enhanced lymphocyte proliferation in vitro and ex vivo. The studies also found that astaxanthin can be consumed in high concentrations without the risk of cytotoxicity.
Controls Glucose and Lipids
Surprisingly there has been new research that has been revealing about another unique but vital role that astaxanthin has. The studies show that it can modulate peroxisome proliferator-activated receptors or PPARs. What this function does is that it may have various applications in human health, including producing glucose and lipid homeostasis. Since PPARs are members of the nuclear hormone receptors in the body, they are a superfamily that plays roles in the expression of many genes that are regulating cellular differentiation and many other functions in the body.
There are at least three subtypes of PPARs that helps the major organs and help the metabolism of glucose and lipids. PPAR? can primarily be expressed in the liver, kidney, heart, and skeletal muscle, where it can be involved in lipid metabolism and insulin sensitivity to the body. Another subtype of PPARs is PPAR?, which plays a role in glucose and lipid homeostasis but also is the site of action in the adipose tissue in the body. When astaxanthin is being involved, astaxanthin is a PPAR? agonist but can act as either an agonist or antagonist to PPAR? receptors. Studies have found that PPAR? agonist and PPAR? antagonist in astaxanthin can decrease cholesterol and triglycerides in loaded HepG2 cells, while changing several enzymes expressions that are being involved in lipid and glucose metabolism pathways, thus resulting in a hypolipidemic effect in the body.
Exercise Enhancement
Surprisingly astaxanthin can be used to prevent exercise-induced free radical production and is a lesser-known application. Astaxanthin can enhance exercise performance and even improve the recovery process. The increase in the reactive oxygen and nitrogen species or RONS are being produced during an exercise regime is deleterious to the health. It is often combated with a matching increase in the endogenous antioxidant enzymes. However, when a person is doing excessive exercises, it can cause RONS to rise above the body’s natural capacity to eliminate them. This will cause an increased risk of oxidative damage in lipids, protein, and DNA molecules. In a review study, it showed the ability of astaxanthin to squelch the RONS generating during exercising. It reported that the antioxidant effects of astaxanthin could provide a variety of benefits to athletes.
Conclusion
Astaxanthin is a powerful immunomodulatory antioxidant that can support numerous biological pathways that are in the body. It can dampen the effects of a variety of chronic diseases and illnesses that can harm the body. Astaxanthin is useful for being a therapeutic and powerful nutraceutical while also being an excellent addition for someone who needs supplements to support their general health and well-being. Some of the products here are beneficial to the body as they help support the immune system while providing more excellent stability.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Ambati, Ranga Rao, et al. �Astaxanthin: Sources, Extraction, Stability, Biological Activities and Its Commercial Applications–a Review.� Marine Drugs, MDPI, 7 Jan. 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC3917265/.
Brown, Daniel R, et al. �Astaxanthin in Exercise Metabolism, Performance and Recovery: A Review.� Frontiers in Nutrition, Frontiers Media S.A., 18 Jan. 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5778137/.
Brown, Daniel R, et al. �Astaxanthin in Exercise Metabolism, Performance and Recovery: A Review.� Frontiers in Nutrition, Frontiers Media S.A., 18 Jan. 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5778137/.
Choi, Chang-Ik. �Astaxanthin as a Peroxisome Proliferator-Activated Receptor (PPAR) Modulator: Its Therapeutic Implications.� Marine Drugs, MDPI, 23 Apr. 2019, www.ncbi.nlm.nih.gov/pmc/articles/PMC6521084/.
Lin, Kuan-Hung, et al. �Astaxanthin, a Carotenoid, Stimulates Immune Responses by Enhancing IFN-? and IL-2 Secretion in Primary Cultured Lymphocytes in Vitro and Ex Vivo.� International Journal of Molecular Sciences, MDPI, 29 Dec. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4730289/.
Park, Jean Soon, et al. �Astaxanthin Decreased Oxidative Stress and Inflammation and Enhanced Immune Response in Humans.� Nutrition & Metabolism, BioMed Central, 5 Mar. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC2845588/?report=reader.
Team, DFH. �Applications of the Antioxidant, Astaxanthin.� Designs for Health, 27 June 2019, blog.designsforhealth.com/node/1047.
Yuan, Jian-Ping, et al. �Potential Health-Promoting Effects of Astaxanthin: a High-Value Carotenoid Mostly from Microalgae.� Molecular Nutrition & Food Research, U.S. National Library of Medicine, Jan. 2011, www.ncbi.nlm.nih.gov/pubmed/21207519.
The University offers a wide variety of medical professions for functional and integrative medicine. Their goal is to inform individuals who want to make a difference in the functional medical fields with knowledgeable information that they can provide.
The ketogenic diet also referred to as the keto diet, is a low-carbohydrate, high-fat diet that has been demonstrated to have a variety of health benefits, especially for people with metabolic syndrome. Several research studies found that the ketogenic diet can help promote weight loss and improve overall wellness. Researchers also found that the keto diet may even be beneficial against diabetes, epilepsy, Alzheimer’s disease, and cancer, among others.
What is the Ketogenic Diet?
As previously mentioned, the keto diet is a low-carb, high-fat diet similar to the Atkins diet, as well as other low-carbohydrate diets. The primary goal of the ketogenic diet is to considerably decrease the consumption of carbohydrates and replace them with “good” fats. Reducing carb intake will allow the body to enter a metabolic state, known as ketosis. During ketosis, the body becomes tremendously efficient at burning fat in order to turn it into energy for fuel. It will also produce ketones in the liver to be used as energy by the brain. The ketogenic diet can greatly improve high blood sugar levels and insulin resistance.
Metabolic syndrome is commonly characterized by 5 risk factors. People with 3 our of 5 risk factors may have metabolic syndrome, including:
Excess waist fat (> 40 inches in men, and > 35 inches in women)
High blood pressure (130/85 mm Hg)
Hight blood sugar or glucose levels (100 mg/dL or greater)
High triglyceride levels (150 mg/dL or greater)
Low HDL cholesterol (< 40 mg/dL in men or < 50 mg/dL in women)
Metabolic syndrome can increase the risk of a variety of health issues, including diabetes, stroke, and heart disease. Fortunately, the keto diet can help improve the risk factors associated with metabolic syndrome, such as increased HDL cholesterol as well as decreased blood pressure and blood sugar levels. In a controlled 12-week research study, people with metabolic syndrome following a calorie-restricted ketogenic diet lost 14 percent of their body fat. The research study also found that the participants had decreased triglycerides by more than 50 percent and experienced several other health benefits.
How the Keto Diet Helps Improve Metabolic Syndrome
The ketogenic diet has been demonstrated to help improve the risk factors associated with metabolic syndrome. As a low-carbohydrate, high- fat diet, the keto diet is effective in decreasing high blood sugar levels and improving insulin resistance by having the body break down body fat into ketones for energy. Metabolic syndrome is a cluster of signs that are associated with various health issues, including diabetes, stroke, and heart disease. The signs of metabolic syndrome include excess waist fat, high blood pressure, high blood sugar, high triglyceride levels, and low HDL or “good” cholesterol.
A research study conducted by researchers at Bethel University, Minnesota, USA, compared the health of three groups of adults with metabolic syndrome. The first group followed the ketogenic diet without exercise, the second group followed the standard American diet without exercise, and the third group followed the standard American diet with 30 minutes of exercise or physical activity for three to five days per week. The findings showed that the ketogenic diet without exercise was much more effective than the other groups at promoting weight loss, decreasing body fat and reducing HbA1c.
According to a variety of other research studies like the one above, the ketogenic diet may help improve a variety of other health issues, including:�
Type 2 Diabetes
Although there’s a variety of research studies on what is the best type of diet for people with type 2 diabetes to promote weight loss and improve insulin resistance, healthcare professionals recommend following the keto diet. The keto diet lowers carb intake which causes high blood glucose levels to drop, producing less insulin, burning fat, and potentially improving insulin sensitivity. Research studies suggest that the keto diet may be helpful for people with type 2 diabetes. Several hospitals have comprehensive programs dedicated to using the nutritional approach to help treat type 2 diabetes.
Obesity
Excess weight and obesity increase the risk of developing type 2 diabetes. A small research study published in December 2016 in the journal Endocrine involved 45 obese participants either on a very-low-calorie ketogenic diet or a standard low-calorie diet. After two years, the participants following the keto diet lost approximately 27 pounds on average compared with less than 10 pounds in the low-calorie participants. The participants following the keto diet also lost more belly fat. The ketogenic diet also helped keep lean body mass during weight loss which prevented a metabolic slowdown.
Metabolic Syndrome
Metabolic syndrome is a collection of risk factors, including excess waist fat, high blood pressure, high blood sugar, high triglyceride levels, and low HDL cholesterol, according to the American Heart Association. Improving insulin resistance may also reduce the risk of developing metabolic syndrome. One small research study on 30 adults found that adults with metabolic syndrome who followed the ketogenic diet for 10 weeks lost more weight and body fat as well as lowered their A1C levels compared with participants who followed a standard American diet, even with or without exercise.
About 23 percent of adults in the United States have metabolic syndrome. Although the risk factors for developing the collection of signs are significant, there are good news. Many of the risk factors associated with metabolic syndrome can be addressed through diet and lifestyle modifications, such as the ketogenic diet as well as exercise and physical activity. By making these changes, people can considerably reduce their risks of developing a variety of other health issues, including diabetes, stroke, and heart disease. Although metabolic syndrome can be a serious health issue, people can reduce their risks by reducing their weight; increasing exercise and physical activity; eating a heart-healthy diet that’s rich in fruits, vegetables, whole grains, and fish; as well as working with a healthcare professional to regulate blood pressure, blood sugar, blood cholesterol. In the following article, we will discuss how the ketogenic diet can help improve metabolic syndrome and its risk factors. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The ketogenic diet also referred to as the keto diet, is a low-carbohydrate, high-fat diet that has been demonstrated to have a variety of health benefits, especially for people with metabolic syndrome. Several research studies found that the ketogenic diet can help promote weight loss and improve overall wellness. Researchers also found that the keto diet may even be beneficial against diabetes, epilepsy, Alzheimer’s disease, and cancer, among others.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
Mawer, Rudy. �The Ketogenic Diet: A Detailed Beginner’s Guide to Keto.� Healthline, Healthline Media, 30 July 2018, www.healthline.com/nutrition/ketogenic-diet-101#weight-loss.
Spritzler, Franziska. �15 Health Conditions That May Benefit From a Ketogenic Diet.� Healthline, Healthline , 12 Sept. 2016, www.healthline.com/nutrition/15-conditions-benefit-ketogenic-diet.
Migala, Jessica. �Can Keto Cure You? 11 Conditions It May Help and 6 It Won’t: Everyday Health.� Everyday Health, Everyday Health Media, 28 Dec. 2018, www.everydayhealth.com/ketogenic-diet/diet/health-conditions-it-may-help-and-definitely-wont/.
Dr. Alex Jimenez Podcast: Metabolic Syndrome
Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL or good cholesterol levels are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines, such as the ketogenic diet or the keto diet, as well as demonstrate the biochemical and chemical pathways that the body goes through during ketosis to help people with metabolic syndrome improve their overall health and wellness. From eating good fats and staying hydrated to exercise and better sleep, Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas discuss how diet and lifestyle modifications, such as the ketogenic diet or keto diet, can help improve the 5 risk factors associated with metabolic syndrome to prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. – Podcast Insight
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
Eating sweets does not relieve the craving for sugar?
If you are experiencing any of these situations, then you might be experiencing an imbalance of your blood glucose. Why not try adding berberine into your daily diet and lifestyle.
For many individuals reclaiming their health, the incidence of metabolic syndrome, and type 2 diabetes along with many other conditions that can be related to insulin resistance. Many local healthcare practitioners need all the tools to inform their patients as a powerful supplement that has been receiving recognition for its efficacy in improving the multiple parameters for metabolic health and improving glycemic control. This supplement is known as berberine, and the studies have shown that berberine is as effective as metformin and can help patients who have type 2 diabetes.
What Is Berberine?
Berberine is an alkaloid compound that is found in several plants like goldenseal, barberry, and tree turmeric. When berberine is crushed, it has a yellow color hue that is similar to curcumin and has been part of Chinese and Ayurvedic traditional medicine that has been used for thousands of years. Surprisingly berberine has worked in multiple ways and has been able to make some changes within the body�s cells and metabolic system. There has been research showing that berberine can transport in the bloodstream once it has been ingested and can activate the AMPK (AMP-activated protein kinase) enzyme. Once this happens, the enzyme is referred to as a “metabolic master switch” and can help regulate the significant organs and regulating the body’s metabolism.
The Health Benefits from Berberine
Research shows that berberine can provide many health benefits to the body, especially those who have been affected with type 2 diabetes and have metabolic syndrome. Here are some of the health benefits that berberine has to offer.
Bacterial Infections
Studies have found that berberine is an active antimicrobial agent. Studies have shown that berberine can enhance the inhibitory efficacy of antibiotics against the bacteria Staphylococcus aureus. This type of bacteria can cause many health problems in the body, like sepsis, pneumonia, and meningitis. There is even another study that shows that when a person consumes a high concentration of berberine could kill the Staphylococcus aureus bacteria more quickly. The berberine effects can dissociate the bacteria protein into individual chains and separate them into their molecular weight.
Regulates Blood Glucose
Type 2 diabetes is a common disease that can make a person’s blood sugar to either rise or fall, causing them to DKA (diabetic ketoacidosis). With berberine, it can help regulate blood glucose in the body. Studies have shown that type 2 diabetes has become a worldwide health threat for people, and finding treatment for this disease is limited due to the availability of effective medications that can help control the blood glucose levels. With berberine, it can help reduce insulin resistance and surprisingly, regulate the blood glucose to healthy levels like metformin. The research even shows that berberine can also help regulate the body�s lipid metabolism as well.
More results showed that berberine could do the following:
Lower the insulin resistance to make the blood sugar to lower the hormone insulin more effectively.
It helps increase the glycolysis so the body can break down the sugars.
Decease the sugar produced in the liver.
It helps break down the carbohydrates in the gut microbiome.
It helps increase the beneficial bacteria in the gut to prevent inflammation.
Help Losing Weight
Studies have shown that berberine is an effective weight loss supplement for anyone who may be obese. There was a twelve-week study that showed that the participates took about 500 mg of berberine, and they lost about five pounds of body fat. While another study stated that about 37 participants that have metabolic syndrome took about 300 mg of berberine, and the results showed that the participants have dropped their BMI (body mass index) levels go from obese to overweight in three months. The participants even improved many of their health markers and lose their belly fat.
Many researchers believed that when people take berberine and see that they are losing their excess weight, it can help improve their fat-regulating hormones like insulin, adiponectin, and leptin in their body. There is still more research being done about berberine and how its beneficial weight loss effects can help anyone with metabolic syndrome and might be overly obese.
Conclusion
Berberine is a compound that is found in plants like tree turmeric, goldenseal, and barberry. It has a yellow color cue and has many beneficial properties. Berberine can help anyone who has type 2 diabetes and metabolic syndrome. For the beneficial properties, berberine can help regulate the body�s glucose hormones and has the same effects as the pharmaceutical drug, metformin. When people consume berberine, their metabolic system will begin to function correctly and begun to live a healthier life. Some products can help the metabolic system and the immune system by supporting sugar metabolism as well as reducing the glutathione for providing more excellent stability, bioavailability, and digestive comfort in the body.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Berry, Jennifer. �Everything You Need to Know about Berberine.� MedicalNewsToday, 19 July 2019, www.medicalnewstoday.com/articles/325798.php.
Chu, Ming, et al. �Role of Berberine in the Treatment of Methicillin-Resistant Staphylococcus Aureus Infections.� Scientific Reports, Nature Publishing Group, 22 Apr. 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4840435/.
Gunnars, Kris. �Berberine � A Powerful Supplement With Many Benefits.� Healthline, 14 Jan. 2017, www.healthline.com/nutrition/berberine-powerful-supplement.
Hu, Yueshan, et al. �Lipid-Lowering Effect of Berberine in Human Subjects and Rats.� Phytomedicine, Urban & Fischer, 25 June 2012, www.sciencedirect.com/science/article/abs/pii/S0944711312001870.
Li, Zheng, et al. �Antioxidant and Anti-Inflammatory Activities of Berberine in the Treatment of Diabetes Mellitus.� Evidence-Based Complementary and Alternative Medicine, Hindawi, 11 Feb. 2014, www.hindawi.com/journals/ecam/2014/289264/.
Peng, Lianci, et al. �Antibacterial Activity and Mechanism of Berberine against Streptococcus Agalactiae.� International Journal of Clinical and Experimental Pathology, e-Century Publishing Corporation, 1 May 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4503092/.
Team, DFH. �Berberine: Boon for Metabolic Syndrome.� Designs for Health, 5 Jan. 2018, blog.designsforhealth.com/berberine-boon-for-metabolic-syndrome.
Yang, Jing, et al. �Berberine Improves Insulin Sensitivity by Inhibiting Fat Store and Adjusting Adipokines Profile in Human Preadipocytes and Metabolic Syndrome Patients.� Evidence-Based Complementary and Alternative Medicine: ECAM, Hindawi Publishing Corporation, 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3310165/.
Yin, Jun, et al. �Efficacy of Berberine in Patients with Type 2 Diabetes Mellitus.� Metabolism: Clinical and Experimental, U.S. National Library of Medicine, May 2008, www.ncbi.nlm.nih.gov/pmc/articles/PMC2410097/.
The University offers a wide variety of medical professions for functional and integrative medicine. Their goal is to inform individuals who want to make a difference in the functional medical fields with knowledgeable information that they can provide.
Metabolic syndrome is caused by having more than one condition. Metabolic syndrome often leaves individuals with headaches, joint pain, fatigue, and more! Metabolic syndrome is an epidemic all over the world, but in the US, we are seeing this condition all too often.
Metabolic Syndrome can be defined as having two or more of the conditions listed below:
Women with abdominal fat or a waistline greater than 35
Men with abdominal fat or a waistline greater than 40
Individuals with high blood pressure ( 130/85 or higher)
Patients with triglycerides higher than 150
A fasting glucose of 100 or greater
Low HDL ( good cholesterol ) less than 40 in men and 50 for women
These symptoms are often associated with inflammation. Many people believe inflammation is just something that occurs in the joints and on the skin, but inflammation can occur to the organs inside the body and create havoc.
Metabolic syndrome does not target a specific population but can affect anyone who has an overlap of the factors listed above. Those who have an “apple” or “pear” body shape, are likely to have higher abdominal fat, and therefore are more at risk.
As individuals age, their chances of developing metabolic syndrome increases. On top of age, previously having or having a history of diabetes in one’s family also increases their risk of developing metabolic syndrome.
Speaking from personal experience, and having Type 1 Diabetes myself, I can say that metabolic syndrome really takes a toll on one’s body. With experiencing these symptoms first hand, it can leave your body feeling exhausted. When the blood glucose level in the body rises, it causes the blood to become thick due to the excess sugar in the blood. This then causes the heart to work harder and raise the body’s blood pressure due to the effort needed to pump. From here, the body responds with a hard and heavy headache, nausea, occasional vomiting, increased thirst, increased urination, and blurred vision. Recovering from a day of high blood sugars can leave you feeling defeated and similar to feeling like you are recovering from the flu.
One of the things that occur within the body when an individual has metabolic syndrome is their insulin sensitivity decreases. Insulin is the hormone produced that helps to turn the food you eat into fuel for the body or store it as fat. When the insulin sensitivity becomes decreased, it means not enough glucose in the body is being absorbed.� Leading to high blood glucose levels and increases the risk for Type 2 Diabetes.
For those who are suffering from metabolic syndrome, or have one or more of the above risk factors there are ways to take charge. The benefits of taking charge and preventing metabolic syndrome from getting worse or returning means getting back the energy you thought was lost. By decreasing your symptoms and increasing your energy, you could be feeling better than you remembered.
The best diet to quickly gain control of blood sugars and raise HDL is the ketogenic diet. This diet works by eating low carb, high-fat foods. In turn, this makes the body burn fat as fuel rather than carbohydrates. It starts by burning the fat around the pancreas and liver and then starts to burn the intramuscular fat ( excess abdominal weight ). By eliminating most carbs and increasing water intake, individuals can see a decrease in depression, brain fog, their risk of stroke, and blood pressure. All while seeing an increase in sleep and energy.
One of the best ways to reach your goals and stay healthy is to work with a team who understands them and is willing to educate you. We provide 1:1 coaching, scales to track weight that also reports the water weight and BMI of the individual, wrist bands to track caloric activity, and education. The education will help you understand why you are following a specific diet or food guidelines, how that food is breaking down to help you, and what foods to avoid. We will never leave a patient confused or with unanswered questions.
Speaking from personal experience, it is best to get a handle on these symptoms before they cause permanent damage. There are ways and things to do to help reduce your risk. I highly recommend seeing us, or a local doctor to start to build your plan. We can create personalized plans that will help you reach your goals, lower your risk, and work with your lifestyle. Take it from me, you do not want to be stuck feeling the side effects metabolic syndrome comes with.� -Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
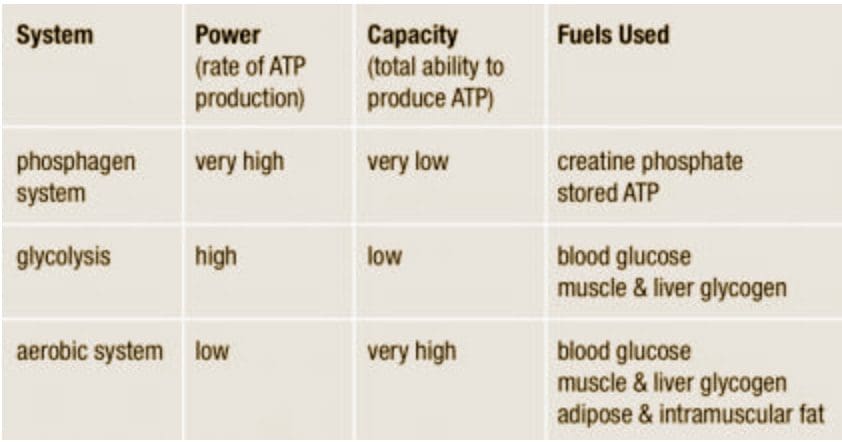
We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect?
Albert Einstein, in his infinite wisdom, discovered that the total energy of an object is equal to the mass of the object multiplied by the square of the speed of light. His formula for atomic energy, E = mc2, has become the most recognized mathematical formula in the world. According to his equation, any change in the energy of an object causes a change in the mass of that object. The change in energy can come in many forms, including mechanical, thermal, electromagnetic, chemical, electrical or nuclear. Energy is all around us. The lights in your home, a microwave, a telephone, the sun; all transmit energy. Even though the solar energy that heats the earth is quite different from the energy used to run up a hill, energy, as the first law of thermodynamics tells us, can be neither created nor destroyed. It is simply changed from one form to another.
ATP Re-Synthesis
The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP.
Like many other animals, humans produce ATP through three metabolic pathways that consist of many enzyme-catalyzed chemical reactions: the phosphagen system, glycolysis and the aerobic system. Which pathway your clients use for the primary production of ATP depends on how quickly they need it and how much of it they need. Lifting heavy weights, for instance, requires energy much more quickly than jogging on the treadmill, necessitating the reliance on different energy systems. However, the production of ATP is never achieved by the exclusive use of one energy system, but rather by the coordinated response of all energy systems contributing to different degrees.
1. Phosphagen System
During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.
2. Glycolysis
Glycolysis is the predominant energy system used for all-out exercise lasting from 30 seconds to about 2 minutes and is the second-fastest way to resynthesize ATP. During glycolysis, carbohydrate�in the form of either blood glucose (sugar) or muscle glycogen (the stored form of glucose)�is broken down through a series of chemical reactions to form pyruvate (glycogen is first broken down into glucose through a process called�glycogenolysis). For every molecule of glucose broken down to pyruvate through glycolysis, two molecules of usable ATP are produced (Brooks et al. 2000). Thus, very little energy is produced through this pathway, but the trade-off is that you get the energy quickly. Once pyruvate is formed, it has two fates: conversion to lactate or conversion to a metabolic intermediary molecule called acetyl coenzyme A (acetyl-CoA), which enters the mitochondria for oxidation and the production of more ATP (Robergs & Roberts 1997). Conversion to lactate occurs when the demand for oxygen is greater than the supply (i.e., during anaerobic exercise). Conversely, when there is enough oxygen available to meet the muscles� needs (i.e., during aerobic exercise), pyruvate (via acetyl-CoA) enters the mitochondria and goes through aerobic metabolism.
When oxygen is not supplied fast enough to meet the muscles� needs (anaerobic glycolysis), there is an increase in hydrogen ions (which causes the muscle pH to decrease; a condition called acidosis) and other metabolites (ADP, Pi�and potassium ions). Acidosis and the accumulation of these other metabolites cause a number of problems inside the muscles, including inhibition of specific enzymes involved in metabolism and muscle contraction, inhibition of the release of calcium (the trigger for muscle contraction) from its storage site in muscles, and interference with the muscles� electrical charges (Enoka & Stuart 1992; Glaister 2005; McLester 1997). As a result of these changes, muscles lose their ability to contract effectively, and muscle force production and exercise intensity ultimately decrease.
3. Aerobic System
Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�
The aerobic system�which includes the�Krebs cycle�(also called the�citric acid cycle or TCA cycle) and the�electron transport chain�uses blood glucose, glycogen and fat as fuels to resynthesize ATP in the mitochondria of muscle cells (see the sidebar �Energy System Characteristics�). Given its location, the aerobic system is also called�mitochondrial respiration.�When using carbohydrate, glucose and glycogen are first metabolized through glycolysis, with the resulting pyruvate used to form acetyl-CoA, which enters the Krebs cycle. The electrons produced in the Krebs cycle are then transported through the electron transport chain, where ATP and water are produced (a process called�oxidative phosphorylation) (Robergs & Roberts 1997). Complete oxidation of glucose via glycolysis, the Krebs cycle and the electron transport chain produces 36 molecules of ATP for every molecule of glucose broken down (Robergs & Roberts 1997). Thus, the aerobic system produces 18 times more ATP than does anaerobic glycolysis from each glucose molecule.
Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).
Following acetyl-CoA formation, fat metabolism is identical to carbohydrate metabolism, with acetyl-CoA entering the Krebs cycle and the electrons being transported to the electron transport chain to form ATP and water. The oxidation of free fatty acids yields many more ATP molecules than the oxidation of glucose or glycogen. For example, the oxidation of the fatty acid palmitate produces 129 molecules of ATP (Brooks et al. 2000). No wonder clients can sustain an aerobic activity longer than an anaerobic one!
Understanding how energy is produced for physical activity is important when it comes to programming exercise at the proper intensity and duration for your clients. So the next time your clients get done with a workout and think, �I have a lot of energy,� you�ll know exactly where they got it.
Energy System Characteristics
Energy System Workouts
Have clients warm up and cool down before and after each workout.
Phosphagen System
An effective workout for this system is short, very fast sprints on the treadmill or bike lasting 5�15 seconds with 3�5 minutes of rest between each. The long rest periods allow for complete replenishment of creatine phosphate in the muscles so it can be reused for the next interval.
2 sets of 8 x 5 seconds at close to top speed with 3:00 passive rest and 5:00 rest between sets
5 x 10 seconds at close to top speed with 3:00�4:00 passive rest
Glycolysis
This system can be trained using fast intervals lasting 30 seconds to 2 minutes with an active-recovery period twice as long as the work period (1:2 work-to-rest ratio).
8�10 x 30 seconds fast with 1:00 active recovery
4 x 1:30 fast with 3:00 active recovery
Aerobic System
While the phosphagen system and glycolysis are best trained with intervals, because those metabolic systems are emphasized only during high-intensity activities, the aerobic system can be trained with both continuous exercise and intervals.
60 minutes at 70%�75% maximum heart rate
15- to 20-minute tempo workout at lactate threshold intensity (about 80%�85% maximum heart rate)
5 x 3:00 at 95%�100% maximum heart rate with 3:00 active recovery
Brooks, G.A., et al. 2000.�Exercise Physiology: Human Bioenergetics and Its Applications.Mountain View, CA: Mayfield.
Enoka, R.M., & Stuart, D.G. 1992. Neurobiology of muscle fatigue.�Journal of Applied Physiology, 72�(5), 1631�48.
Glaister, M. 2005. Multiple sprint work: Physiological responses, mechanisms of fatigue and the influence of aerobic fitness.�Sports Medicine, 35�(9), 757�77.
Hochachka, P.W., Gunga, H.C., & Kirsch, K. 1998. Our ancestral physiological phenotype: An adaptation for hypoxia tolerance and for endurance performance?�Proceedings of the National Academy of Sciences, 95,�1915�20.
Hochachka, P.W., & Monge, C. 2000. Evolution of human hypoxia tolerance physiology.�Advances in Experimental and Medical Biology, 475,�25�43.
McLester, J.R. 1997. Muscle contraction and fatigue: The role of adenosine 5′-diphosphate and inorganic phosphate.�Sports Medicine, 23�(5), 287�305.
Robergs, R.A. & Roberts, S.O. 1997.�Exercise Physiology: Exercise, Performance, and Clinical Applications.�Boston: William C. Brown.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine




















 We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect?
We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect? The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP.
The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP. During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.
During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.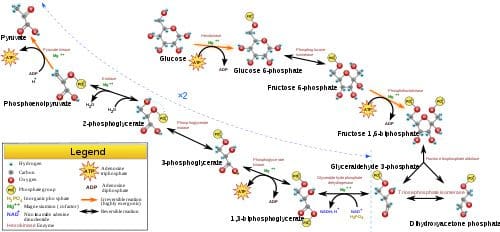 Glycolysis is the predominant energy system used for all-out
Glycolysis is the predominant energy system used for all-out  Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�
Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�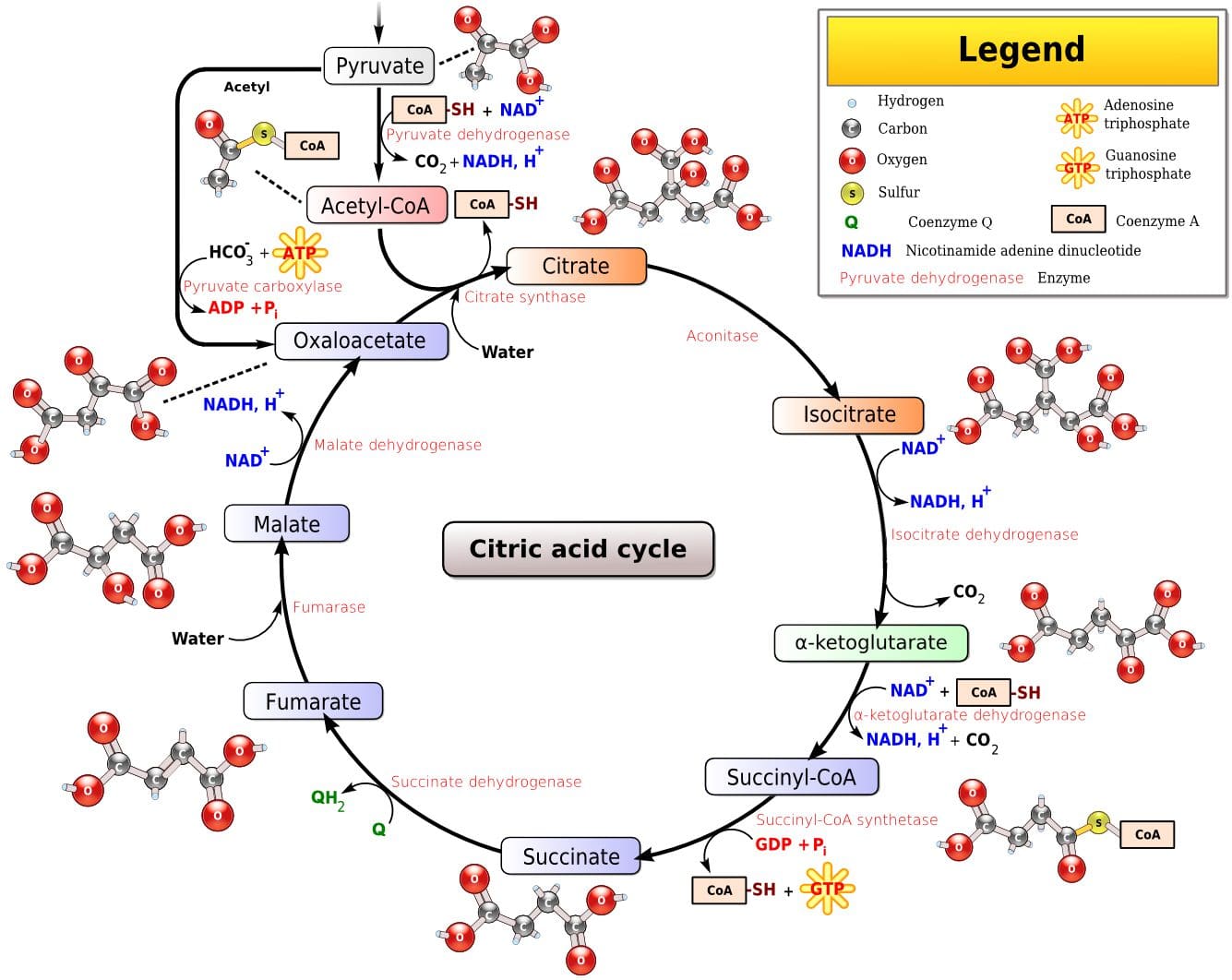 Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).
Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).