The heart is a fantastic muscle in the body that allows hormones, oxygenated blood, and nutrients to travel and transport to all the muscles, tissues, and organs, providing functionality to the body. As one of the main components of the cardiovascular system, the heart works together with the lungs to help carry the deoxygenated blood to the pulmonary system to dispose of waste from the body. The human body needs the heart to stay healthy; however, factors like stress, obesity, autoimmune diseases, and unhealthy habits can affect the heart, causing cardiac issues associated with various body problems. Today’s article focuses on coronary heart disease, what are the risks associated with coronary heart disease, and ways to prevent coronary heart disease from progressively getting worse. We refer patients to certified providers specializing in cardiology treatments that help those with issues of coronary heart disease. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Coronary Heart Disease?
Have you been experiencing hypertension in your body or near your heart? How about unexplained chest pains that randomly showed up? Have you experienced pain running down your shoulders and arms? Many of these are signs that you could be experiencing coronary heart disease. Research studies have defined coronary heart disease as a common heart condition with plaque formation in the heart vessels that cuts off the supply of oxygenated blood to the heart and the rest of the body. As part of cardiovascular diseases, coronary heart disease can cause overlapping profile issues over time if it is not treated right away. Many disruptive factors can affect the heart muscle like:
Age and gender
Oxidative stress
Inflammation
Vascular immune dysfunction
Lack of physical activities
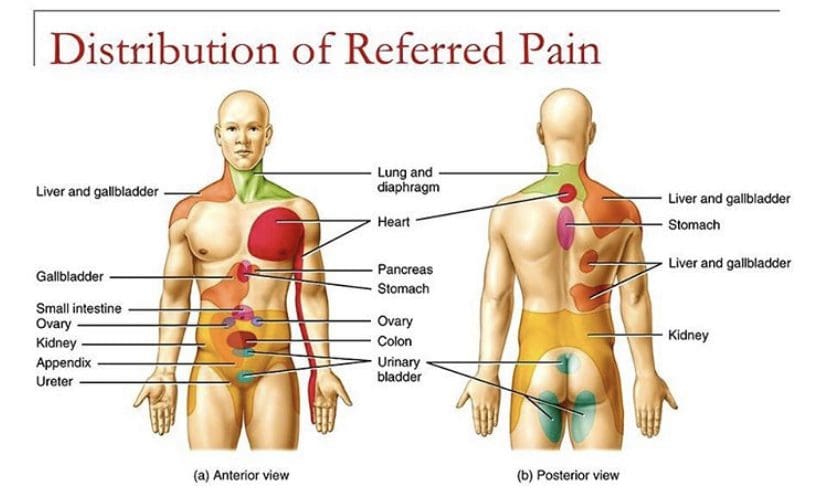
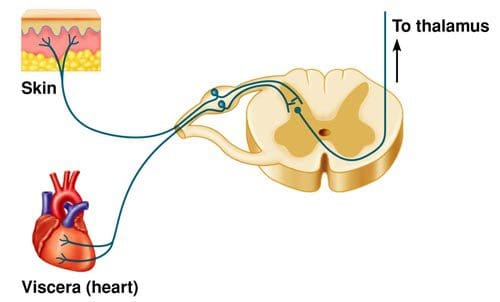
These disruptive factors can increase cardiovascular disease mortality that can affect the heart and be co-morbidities associated with different issues affecting the body. Studies reveal that the mechanisms of cardiac pain are associated with the chest and upper left arm pain. This is defined as referred pain where the sensory input from visceral organs mimics cardiac distress, and the corresponding muscles are affected. But how does this correlate to the heart muscle, and why does the chest experience pain? Visceral pain is a bit trickier to diagnose when cardiovascular disorders overlap the risk profiles associated with other issues affecting the body. For example, you could be experiencing pain in your chest and upper back, but your brain is telling you something is affecting your heart.
An Overview Of CAD-Video
Have you experienced shortness of breath? How about pain located in your chest or radiating from your shoulders and arms? Have you noticed inflammation occurring in your body? Many of these are signs and symptoms of you experiencing coronary artery disease in your body. The video above explains what coronary artery disease is and the risk factors associated with the progression of this common heart disease. Studies reveal that the risk factors can overlap in profiles that contribute to the development of coronary heart disease:
Environmental factors
Lifestyle habits
Diabetes mellitus
Obesity
Symptomatic angina
Smoking
When a person has these risk profiles overlapping different associated issues, their body becomes dysfunctional. Sometimes the symptoms affect other areas of the body, while the brain might be signaled that something is wrong with the heart. Since coronary artery disease progresses slowly over time, many individuals don’t experience the symptoms affecting their heart muscles.
Risk Issues Associated With CHD
Some of these symptoms that overlap in risk profiles may seem like heart issues but may refer to different problems affecting the body. This is defined as viscero-somatic pain, where the pain in the internal organs is associated with the corresponding muscles that share the same nerve. Chest pain associated with heart issues is a perfect example. Studies reveal that chest pains can become indistinguishable from angina, which may result from abnormalities in the thoracic viscera that overlap in profiles with heart issues. So what does it mean? It implies that sensory neurons from different visceral organs might mimic cardiac pain-causing risk-associated problems that affect the thoracic region of the spine triggering neck and upper back issues. Everything is connected as chest pains, dyspnea, and dyspepsia are intertwined with the thoracic anteriority becoming a mediator for cardiovascular diseases.
Ways To Prevent CHD
So let’s visualize a person going to their primary physician due to them experiencing heart issues associated with chest pains after the doctor goes through a manual examination on checking the individual’s heart and chest to see what problems are affecting the body. What does this implicates, and how do chest and back pains correlate with each other if there are heart issues? Studies reveal that the peripheral tissues in the body might be damaged from traumatic events that cause an inflammatory swelling in the cervical and thoracic region of the spine, causing muscle stiffness. Chiropractic care might be the answer to relieving pain and swelling triggering cervical and thoracic pain. Chiropractors use chiropractic adjustments to deliver a non-invasive, gentle treatment that reduces spinal misalignments to enhance the functionality of the musculoskeletal system. This will improve spinal health in the cervical and thoracic regions of the body by decreasing inflammatory swelling associated with heart issues. Chiropractic care, a healthy diet, and exercise also work hand in hand by positively impacting co-morbidities of coronary heart disease and other body problems like obesity to reduce cholesterol, help strengthen the weak muscles along the neck and upper back, and promote blood flow to the heart.
Conclusion
As part of the cardiovascular system, the heart supplies hormones, oxygenated blood, and nutrients throughout the entire body by ensuring that the muscles, tissues, and organs are functioning. When factors like stress, obesity, and unhealthy habits begin to affect the heart, it can develop cardiac issues like coronary heart disease associated with various body problems. Chest pains associated with heart issues that trigger neck and back pain in the body are known as viscero-somatic pain. Available treatments like chiropractic care and changing unhealthy habits work hand in hand to positively impact co-morbidities of coronary heart disease and reduce muscle stiffness along the neck and back muscles of the cervical and thoracic spine.
References
Börjesson, M. “Visceral Chest Pain in Unstable Angina Pectoris and Effects of Transcutaneous Electrical Nerve Stimulation. (TENS). A Review.” Herz, U.S. National Library of Medicine, Apr. 1999, https://pubmed.ncbi.nlm.nih.gov/10372297/.
Foreman, Robert D, et al. “Mechanisms of Cardiac Pain.” Comprehensive Physiology, U.S. National Library of Medicine, Apr. 2015, https://pubmed.ncbi.nlm.nih.gov/25880519/.
Malakar, Arup Kr, et al. “A Review on Coronary Artery Disease, Its Risk Factors, and Therapeutics.” Journal of Cellular Physiology, U.S. National Library of Medicine, Aug. 2019, https://pubmed.ncbi.nlm.nih.gov/30790284/.
Shahjehan, Rai Dilawar, and Beenish S Bhutta. “Coronary Artery Disease – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 9 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK564304/.
In the body, the heart is a vital organ that pumps blood to all the muscles, organs, tissues, and ligaments that require the body to function and move. As part of the cardiovascular system, the heart keeps the body alive by supplying nutrients and disposing of waste and carbon dioxide away from the body. Various factors can affect the body and the heart as well stressful events, unhealthy eating habits, limited physical activities, or autoimmune conditions can cause strain on the heart. Still, they can correlate to different symptoms in the body. This causes an overlap of risk profiles that may feel something is wrong with the heart but might affect another body part. Today’s article focuses on viscero-somatic pain affecting more than the heart muscle, how referred pain is defined, and various ways for treating viscero-somatic pain in the body. We refer patients to certified providers specializing in cardiovascular and chiropractic treatments that help those with issues that affect their hearts. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Visceral-Somatic Pain Affecting More Than The Heart
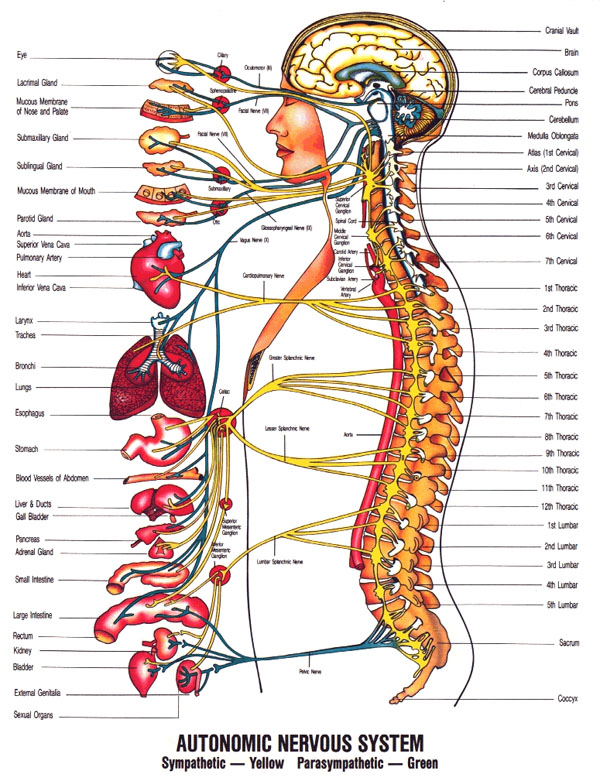
Are you experiencing radiating pain affecting your neck, arms, or back? How about feeling discomfort in your chest? Do gut issues seem to cause a burning sensation affecting your chest? Many of these symptoms overlap in risk profiles that seem like issues in the heart but can refer to something else affecting the body. This is known as viscero-somatic pain, usually defined as pain coming from the internal organs affecting the muscles that share the same nerve. Studies revealed that the autonomic nervous system mediates visceral-somatic pain. For the heart, the parasympathetic innervation comes from the cardiac branches of the vagus nerves connected to the spine and the brain. Since there is extensive autonomic innervation of the heart, the vagus nerve has a minor role in afferent pain transmission signaling.
An example would be having esophageal issues that are causing chest pains in your chest. So how would that correlate to the heart? Think of it as a person experiencing chest pains and whose brain is being signaled that something is wrong with their heart. Then, when they get treated, their results show that it was esophageal issues. Studies have revealed that spinal neurons receive input from a distal esophagus and receive the same information from the heart through viscero-somatic and viscero-visceral convergence. So what does this mean? This means that the sympathetic innervation of the heart is in a casual relationship to the first five thoracic spinal nerves. This indicates that some pain fibers affecting the heart are directly from the upper thoracic spine. Additional studies have mentioned that the vagus nerve connected to the upper thoracic spine can influence harmful afferent signals of the visceral organs to involve pain and joint stiffness in multiple organs and body structures.
Visceral Pain Explained- Video
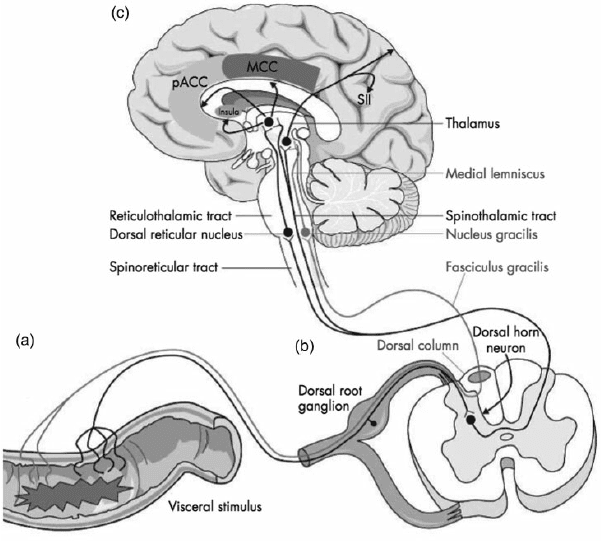
Do you feel pain occurring on your shoulders or neck? How about severe pressure on your chest that might be something else? Or have you noticed issues that are affecting your heart are affecting your chest? Many of these are signs of visceral pain, where the pain of the damaged organ affects the muscle in a different body location. The video above explains visceral pain and uses an example of the cardiac muscle being affected by visceral pain. Studies reveal that the sensory input from different visceral organs can mimic cardiac pain due to viscero-somatic convergence of the cardiac input affecting the spinothalamic tract neurons in the spine to cause back issues in the thoracic region. So what does this implicates to the body? Well, say a person is experiencing chest and shoulder pains in their body; however, they’re experiencing heart problems that also affect them.
Treating Visceral-Somatic Pain In The Body
So, a person starts experiencing chest pain radiating from heart issues and goes to the doctor to see what is wrong with them. The physicians will begin to check on their hearts to see if anything is wrong or will be looking at their spine and chest through manual examination to see what is the issue that is affecting their bodies. So what does this mean to the body? Well, it could indicate that joint and muscle dysfunction in the neck and thorax is causing non-cardiac issues in the body. The influence of the spinal nerves on the cardiovascular function of the heart, since the afferent and parasympathetic efferents innervation of the heart, could disturb the upper cervical subluxation as the vagus nerve is being compressed. This correlates to other visceral organs mimicking cardiac pain and being the cause of musculoskeletal issues in the back.
Conclusion
In conclusion, the heart is a vital organ in the body that pumps blood to all the muscles, organs, tissues, and ligaments for functionality and nutrients distribution. The heart also share nerves in the parasympathetic innervation that connects to the vagus nerves which connects to the spine and brain to send information. However, various factors like lifestyle habits can affect the heart muscle and cause the individual chest pains that the brain is getting the signals that something is wrong with the heart. This is known a viscero-somatic pain where affected organs can cause muscle issues in the body in a different location. Treatments are available to figure out what the problem is going on with the body to understand better how to alleviate these viscero-somatic issues.
References
Foreman, Robert D, et al. “Mechanisms of Cardiac Pain.” Comprehensive Physiology, U.S. National Library of Medicine, Apr. 2015, https://pubmed.ncbi.nlm.nih.gov/25880519/.
Garrison, David W, et al. “Viscerosomatic Convergence onto Feline Spinal Neurons from Esophagus, Heart and Somatic Fields: Effects of Inflammation.” Pain, U.S. National Library of Medicine, June 1992, https://pubmed.ncbi.nlm.nih.gov/1408304/.
Leach, Austin, and Mike Fisher. “Myocardial Ischaemia and Cardiac Pain – a Mysterious Relationship.” British Journal of Pain, SAGE Publications, Feb. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4590151/.
Soares, Bruno, et al. “Accuracy of Physical Assessment in Nursing for Cervical Spine Joint Pain and Stiffness: Pilot Study Protocol.” JMIR Research Protocols, JMIR Publications, 17 Dec. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8726037/.
The body requires the heart in the cardiovascular system to pump oxygen-riched blood to all the muscles, tissues, and organs to keep it functioning. While the heart pumps the blood to the body, the lungs in the pulmonary system help the body by making the host breathe in the fresh air, remove the gases from the body, and helps delivers oxygen to the body cells. When issues begin to affect the lungs and the heart, it can cause the individual to develop cardiovascular disorders and a lung condition known as asthma to disrupt the body and cause pain to the individual. Today’s article looks at what asthma is, how it affects the body, and how somatic issues from asthma can affect the cardiovascular system. We refer patients to certified providers specializing in cardiovascular and pulmonary treatments that help those suffering from asthma attacks. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is Asthma?
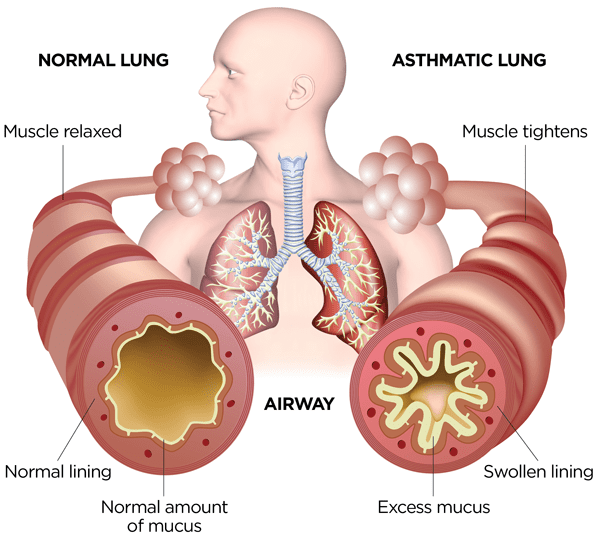
Have you experienced chest pains that are causing issues in your arms? How about the shortness of breath that causes you to have difficulty breathing? Do you have trouble sleeping due to waking up coughing or breathing rapidly? These are the signs and symptoms of you experiencing an asthma attack. Research studies have defined an asthma attack as a chronic disease that causes inflammatory narrowing of the air pathways to the lungs. When a person starts to suffer from an asthma attack, it can cause the lung capacity volume to be weakened and produce an excessive amount of mucus in the airways. Many factors like genetics, allergens, obesity, stress and environmental exposures can trigger a person to have an asthma attack. When these factors begin to affect the lungs, it can cause an overlap of other risk profiles to affect the body.
How Does It Affect The Body?
The lungs help the body intake fresh air and exhale the gases. The lungs provide an autonomic innervation that has a typical casual relationship to the autonomic innervation of the heart. This causal relationship also works with the parasympathetic innervation of the vagus nerve and the prominent sympathetic innervation of the spine’s thoracic region. With the lungs providing the functionality of breathing in the body, it is considered a musculoskeletal act in the service of a visceral system requirement that straddles the somatovisceral interface. Regarding individuals with asthma, research studies have shown that it can cause somatic symptoms like chest pains, cold hands and feet, and blurred vision. These somatic symptoms can affect the lungs and increase the risk associated with cardiovascular diseases.
The Difference Between Somatic & Visceral Pain- Video
Have you noticed chest pain frequently occurring and causing muscle stiffness in your arms? Are you gasping constantly that it irritates your throat? How about the shortness of breath that makes it difficult to sleep? You could be experiencing an asthma attack that can trigger somatovisceral issues that affect the body. The video above explains the difference between somatic and visceral pain affecting the body. Somatic pain is when the muscles trigger the organs, while visceral pain is the opposite, where the internal organs affect the muscles. When asthma affects the airway muscles, it can cause the heart muscles to work extra harder, causing chest and upper-mid back pains in the body.
Asthma Causing Somatic Issues To The Cardiovascular System
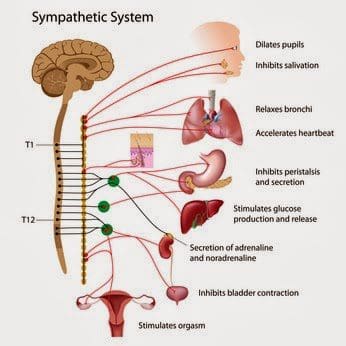
The heart and lungs have a casual relationship as the lungs help the body to breathe in the fresh air, and the heart takes the oxygen-riched blood to supply the rest of the organs, muscles, and tissues in the body. Through the sympathetic system, the heart communicates with the parasympathetic, sympathetic, and sensory pathways that allow the coordination of the cardiac tone, causing the heart to accelerate its beat in the body. When an asthma attack begins to affect the cardiovascular system, research studies have found that the sudden restriction of the airflow pathways from an asthma attack is a development for upcoming cardiovascular issues. The heart muscles will coincidentally begin to strain as the sensory innervations cause immense pain. The sudden constriction of the airways during an asthma attack can also affect the thoracic spine and reach the heart. One of the ways to reduce cardiovascular issues that affect the thoracic spine is spinal manipulation. Research studies have found that manipulating the thoracic spine can help increase the motion of the thoracic cage and enhance the arterial airflow supply to regulate heartbeat and lung capacity.
Conclusion
Asthma is a chronic disorder that causes inflammation and narrows the air pathways that restrict oxygen from entering the heart. The lungs and the heart have a casual relationship to the body, providing oxygen and blood flow to the organs, muscles, and tissues to function correctly. When exposed to environmental factors, it can cause restriction to the airway pathways to the lungs, causing wheezing and coughing motion that can cause somatic visceral dysfunction in the cardiovascular system and the thoracic spine. When this happens, treatments like chiropractic therapy can manipulate the thoracic spine and restore the air pathways to improve cardio and lung capacity.
References
Hashmi, Muhammad F, et al. “Asthma.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 16 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK430901/.
Kaminskyj, Adrienne, et al. “Chiropractic Care for Patients with Asthma: A Systematic Review of the Literature.” The Journal of the Canadian Chiropractic Association, Canadian Chiropractic Association, Mar. 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2829683/.
Pollevick, Matias E, et al. “The Relationship between Asthma and Cardiovascular Disease: An Examination of the Framingham Offspring Study.” Chest, American College of Chest Physicians, Apr. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8501004/.
Ringsberg, K C, et al. “Psychological Differences between Asthmatics and Patients Suffering from an Asthma-like Condition, Functional Breathing Disorder: A Comparison between the Two Groups Concerning Personality, Psychosocial and Somatic Parameters.” Integrative Physiological and Behavioral Science : the Official Journal of the Pavlovian Society, U.S. National Library of Medicine, 1993, https://pubmed.ncbi.nlm.nih.gov/8117581/.
In the body’s upper half, the cardiovascular system’s heart helps pump nutrient-riched oxygenated blood all around the body to the corresponding muscles, tissues, and organs to keep the body functional. The heart is protected by the ribcage and muscles surrounding the heart organ from any external factors that can cause harm to the body. When these factors do cause an effect on the body, it can lead to many issues like thoracic back pain, cardiovascular problems, gut disorders, and even chest pains. These issues affect a person, causing them to feel crummy and dampen their outlook. Today’s article will look at chest pains, how it affects the gut and heart in the body, and how viscerosomatic dysfunction is associated with chest pains. We refer patients to certified, skilled providers specializing in osteopathic and cardiovascular treatments that help those suffering from chest pains and cardiovascular disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Are Chest Pains?
Have you noticed your heart is beating irregularly? How about acid reflux that is affecting your chest constantly? Have you felt muscle stiffness or tenderness in the middle regions of your back? Or have you felt your chest harden and stiffen after something impacted you? Many of these symptoms are tell-tale signs of you experiencing chest pains in your upper body. Research studies have defined chest pains as a common type of visceral pain that is a dull, deep pressure that squeezes the chest. This results in the visceral afferent nerves aggravated as they cause shoulder pain, jaw pain, or thoracic back pain since the nerve root reaches the spinal cord. Additional research studies have found that chest pains can have a variety of cardiac disorders as they can cause dysfunction in the muscles and skeletal joints within the chest walls or the thoracic regions of the spine. When the thoracic region of the spine becomes affected due to chest pains, it can cause herniation on the spinal discs, thus resulting in unwanted pain and discomfort to the individual. Chest pain can even affect the gut system and the heart itself.
How Does It Affect The Gut & The Heart?
Research studies have mentioned that chest pains can affect the gut system and the heart organ itself due to environmental changes that can affect the gut system. The gut microbiota helps metabolize homeostasis in the body for the gut system. When the gut has been impaired, the harmful bacteria travel through the systemic circulation and heighten the inflammatory effects that cause the development of cardiovascular diseases in the heart. At the same time, additional research studies have mentioned that any symptoms accompanying angina pain are conceptualized as a warning to individuals developing coronary artery disease. When this happens, not all ischemic episodes in the heart are indistinguishable when it comes to chest pains and can result from abnormalities of the thoracic regions.
Viscerosomatic Reflexes Overview-Video
Have you experienced irregular chest pains that pop up randomly? How about discomfort in the thoracic regions of your back? Do you feel gastrointestinal inflammatory issues like acid reflux or IBS (irritable bowel syndrome) cause you pain? These symptoms are associated with chest pains in the body due to viscerosomatic dysfunction. Research studies have found that visceral pain is a complex disorder since it can affect one internal organ in the body. In contrast, the corresponding nerve or muscle gets involved as well. Visceral pain is also associated with GI disturbances and changes in the body’s temperature, blood pressure, and heart rate, which are considered autonomic signs that the body is dysfunctioning. The video above gives an insightful overview explanation of what the viscerosomatic reflexes and nerves do when they are not aggravated.
Viscerosomatic Dysfunction Associated With Chest Pains
Since visceral pain is complex and can affect the internal organs, research studies have found that viscerosomatic dysfunction in the thoracic-upper abdominal regions can cause the thoracic and esophagus to become hypersensitive to environmental factors that irritate the airways that connect the entrance of the gut to the esophageal tube. Additional research studies have even found that non-cardiac chest pains are another form of viscerosomatic dysfunction that causes the esophageal opening of the stomach to become dysmotility and hypersensitive causing gastroesophageal reflux disease. This causes many individuals to develop chest pains and can affect a person’s mortality. Adjusting certain habits affecting the chest, gut, or back can reduce the effects that viscerosomatic dysfunction is causing to the person’s body so that they can get their sense of purpose back.
Conclusion
The body’s upper half has the cardiovascular system, where the heart makes sure to pump blood and nutrients to every muscle, tissue, and organ required to keep the body functional. When environmental factors cause issues affecting the body, it can cause various problems in the gut, chest, and heart; this is known as visceral pain and is a complex disorder that can affect the upper abdominal-thoracic region of the body. Visceral pain can cause the gut system to develop gastroesophageal reflux disease, chest pains, and cardiovascular disorders that can make the thoracic region of the spine herniated and stiff if it is not taken care of. When individuals start to take care of themselves and reduce the visceral pain from the affected organ, their bodies will begin to heal naturally and make them continue their health and wellness journey.
References
Brumovsky, P R, and G F Gebhart. “Visceral Organ Cross-Sensitization – an Integrated Perspective.” Autonomic Neuroscience: Basic & Clinical, U.S. National Library of Medicine, 16 Feb. 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2818077/.
Börjesson, M. “Visceral Chest Pain in Unstable Angina Pectoris and Effects of Transcutaneous Electrical Nerve Stimulation. (TENS). A Review.” Herz, U.S. National Library of Medicine, Apr. 1999, https://pubmed.ncbi.nlm.nih.gov/10372297/.
Johnson, Ken, and Sassan Ghassemzadeh. “Chest Pain – StatPearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 1 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK470557/.
Sikandar, Shafaq, and Anthony H Dickenson. “Visceral Pain: The Ins and Outs, the Ups and Downs.” Current Opinion in Supportive and Palliative Care, U.S. National Library of Medicine, Mar. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3272481/.
Stochkendahl, Mette J, et al. “Diagnosis and Treatment of Musculoskeletal Chest Pain: Design of a Multi-Purpose Trial.” BMC Musculoskeletal Disorders, BioMed Central, 31 Mar. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2315652/.
Tang, W H Wilson, et al. “Gut Microbiota in Cardiovascular Health and Disease.” Circulation Research, U.S. National Library of Medicine, 31 Mar. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5390330/.
Heart health and proper function circulate millions of gallons of blood to the entire body. The circulation moves:
Oxygen
Fuel
Hormones
Essential cells
Other compounds
Removes metabolic waste products
If the heart stops, vital functions can fail almost instantly. Family history and genetics play a role in the development of heart disease, but lifestyle choices also play a part. Heart health disease prevention focuses on:
Chiropractic treatment can help improve overall heart health.
Heart Health
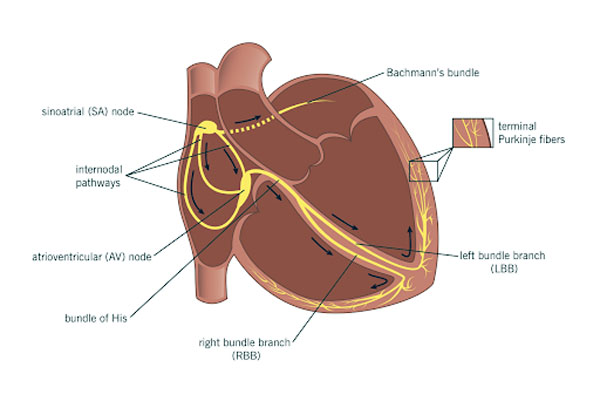
If every nerve was disconnected, the heart would continue to beat. There is a small node of the heart muscle that rhythmically contracts and relaxes inherently, and sets the heartbeat pace. It can be thought of as a natural pacemaker and is called the sinoatrial node.
In an average adult, the node maintains a rhythm of around 70 beats per minute. This natural pacemaker keeps the heart working, while the nerves that accelerate and decelerate (the sympathetic and parasympathetic nerves) can affect the sinoatrial node affecting the heartbeat.
Sympathetic and Parasympathetic Nerves
The sympathetic and parasympathetic nerves are located in the thoracic and upper cervical spine. With chiropractic, any spinal misalignments, pressure, stress, and restrictions are properly addressed, and able to normalize the cardiac rhythm and heart rate. Corrective treatment of the cervical spine will also help lower blood pressure and remove any stress on the cardiovascular system. Heart and spinal health are vital, contact a local chiropractor today.
Healthy Body Composition
Aerobic Training Strengthens The Heart
Aerobic exercise will strengthen the heart, as well as, train the heart to be more efficient in circulating blood. The chamber of the heart that pumps blood to the rest of the body literally gets larger and squeezes out more blood with each pump, meaning the stroke volume gets increased.
This improves cardiac output, which is the quantity of blood pumped by the heart per minute. A strong, efficient heart is the objective to live a long and healthy life. When the heart is stronger and pumps more blood it doesn�t have to beat as much and as rapidly. Lowering the resting heart rate is associated with a reduced risk of cardiovascular disease.
Cardiac adaptations are helped with an increase in blood volume that happens with aerobic exercise training. What happens is the expanded blood volume improves the heart�s contractility/fill capacity pumping more blood per beat. The heart contracts to move blood throughout the body. By making it stronger and more efficient, the heart�s responsibilities are lightened by decreasing the different types of resistance.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Yang, Jian et al. �Physical Exercise Is a Potential “Medicine” for Atherosclerosis.��Advances in experimental medicine and biology�vol. 999 (2017): 269-286. doi:10.1007/978-981-10-4307-9_15
The heart never stops working. The efficiency of the heart and how it operates depends on various factors related to individual health. High blood pressure management can include chiropractic treatment for proper spinal alignment. This promotes improved nervous system function, regulation, and optimal blood flow throughout the body.
High blood pressure is also known as hypertension, often it has no symptoms, and if left untreated, it could lead to heart conditions like heart disease and stroke. Blood pressure is the force the heart exerts on the arteries each time it contracts and relaxes. It is measured with a blood pressure cuff or monitor.
Normal is around 120/80 mmHg
A blood pressure reading of 130/90 mmHg or more, is categorized as high blood pressure.
High blood pressure
Any type of heart condition can place added strain on the body and can lead to poor quality of life, disease, and be fatal. When the body’s ability to pump the proper amount of blood gets compromised the body suffers from a lack of oxygenated blood. These issues can go undiagnosed for years. Often high blood pressure does not get associated with any specific symptoms other than general poor health. When left untreated, high blood pressure can lead to issues like:
Heart attack
Stroke
Kidney disease
Dementia
Prevention and regular monitoring are crucial for staying on top of any potential heart issues.
Heart conditions
Different heart conditions can cause pain in the chest, upper back, and shoulder(s):
Angina is when the heart muscle does not get enough blood causing chest pain.
A heart attack occurs when there is reduced or complete loss of blood supply from the blockage of an artery.
Pericarditisis the inflammation of the thin layers that surround the heart.
Heart conditions are commonly associated with chest pain but remember that chest pain is not always present or severe. Pain-related to the heart can also be felt in other areas, like the shoulder or upper back.
Risk factors
Risk factors associated with high blood pressure include:
An unhealthy diet high full of processed foods, sugar, and salt
The most common treatment for high blood pressure is medication. However, this does not address the root cause of the issue in relation to individual lifestyle and underlying imbalances of the body that include the spine.
Lifestyle
Lifestyle adjustments should be the first line of defense for managing, and reversing heart health issues. High blood pressure management includes:
Focus on nutrition
Exercise
Stress management
Chiropractic
Chiropractic is a specialized approach that focuses on identifying and addressing the root cause of musculoskeletal health issues and optimized organ function through restored impaired nerve function. Spinal misalignment can cause nerve signals to be impaired/damaged which can affect the heart and overall health.
A chiropractic physician can help reduce the strain on the body�s functions by restoring nerve function/energy/blood flow with spinal adjustments that bring the body back into proper alignment. One primary cause of high blood pressure is over-activation of the autonomic nervous system, which regulates the stress response.
When spinal alignment is achieved, there is improved regulation to prevent unnecessary spikes in stress affecting body homeostasis and organ function. Chiropractic can help an individual achieve the best possible heart health. Once the diagnosis is found, an effective customized treatment plan will be developed.
Chiropractor Near Me
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Win, Ni Ni et al. �Effects of Upper and Lower Cervical Spinal Manipulative Therapy on Blood Pressure and Heart Rate Variability in Volunteers and Patients With Neck Pain: A Randomized Controlled, Cross-Over, Preliminary Study.��Journal of chiropractic medicine�vol. 14,1 (2015): 1-9. doi:10.1016/j.jcm.2014.12.005
If you are experiencing any of these situations, then there might be some dysfunction in your body�s system, including the immune system. Why not try the Chinese herb, astragalus to help alleviate the symptoms.
Astragalus
In traditional Chinese medicine, the herb astragalus has been used for thousands of years and has been known to strengthen chi or qi life force in the body. This herb has been known to be typically employed in conditions that are related to general weakness in the body like fatigue, anemia, a poor appetite, cardiovascular diseases, and other conditions that can weaken the body. Surprisingly though, astragalus can be used to optimize kidney health and, with the combination of ginseng and echinacea, can boost up the body’s immune system. There is a variety of astragalus that are native to Northeast Asia, and its roots need to be dried and powdered to be transformed to be consumed as a capsule or as a tea.
Astragalus Beneficial Properties
Studies have found that astragalus�s beneficial pharmacological effects might contain phytochemical components, which include a host of saponins polysaccharides and flavonoids that the body’s immune system needs to function correctly. Another study found that astragalus contains about twenty trace minerals that are highly important for the body. With astragalus extract, it has immune-modulating properties in vivo and in vitro in both animals and humans, and research shows that the herb stimulates and influences on the immune response cytokines while also leaving the inflammatory cytokines unaffected.
Some of the beneficial properties that astragalus can have on the body are still being researched; however, this Chinese herb can help the body to function correctly and are effective.
Improving the Immune System
Studies have shown that astragalus contains some beneficial plant compounds that may enhance the body’s immune system. Studies show that the primary role for the immune system is that it helps protect the body from foreign pathogens like harmful bacteria and viruses that can cause a person to be ill. Research has found out that there is some evidence that astragalus can increase the body�s production of white blood cells, which will help prevent illnesses from entering the body. In other research studies, it has been found that astragalus root has been known to help the body kill bacteria and viruses caused by infections. Even though the research may be limited, there are still studies that show that astragalus can fight off viral infections like the common cold and liver infections in the human body.
Improving the Heart Function
Research shows that astragalus may be able to improve heart function by widening the blood vessels and increasing the amount of blood that is being pumped from the heart. In a clinical research study, it showed that patients were given at least 2.25 grams of astragalus for two weeks and have experienced a more significant improvement in their heart function. In another study, it shows that astragalus may help reduce the symptoms of myocarditis, which is an inflammatory condition in the heart.
Improving Kidney Function
Astragalus can help support kidney health in the body by improving the blood flow to the kidneys and measuring the protein in the urine. A study has shown that proteinuria is a condition where there is an abnormal amount of protein that is found in urine, and it can be a sign that the kidneys are not functioning normally or may be damaged. Surprisingly, there was another study that showed that astragalus could improve proteinuria symptoms in individuals that have kidney disease. Studies have even found that astragalus may also help prevent infections for anyone who has a reduce kidney function and reducing the risk of a kidney disorder known as nephrotic syndrome.
Conclusion
Astragalus is a unique herb that can help the body’s immune system to function correctly. Even though there is a limited amount of research on this herb, but the beneficial properties it provides in the body are truly amazing. Astragalus can be consumed by capsules or even be brewed as a tea, so that way, people can enjoy the beneficial properties and that their body is performing excellently in health and wellness. Some products offer support to the body’s immune system and help target the amino acids that are intended to support the intestines while offering more support to the metabolic system.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Block, Keith I, and Mark N Mead. �Immune System Effects of Echinacea, Ginseng, and Astragalus: a Review.� Integrative Cancer Therapies, U.S. National Library of Medicine, Sept. 2003, www.ncbi.nlm.nih.gov/pubmed/15035888.
Fu, Juan, et al. �Review of the Botanical Characteristics, Phytochemistry, and Pharmacology of Astragalus Membranaceus (Huangqi).� Phytotherapy Research: PTR, U.S. National Library of Medicine, Sept. 2014, www.ncbi.nlm.nih.gov/pubmed/25087616.
Gao, Xing-hua, et al. �Saponin Fraction from Astragalus Membranaceus Roots Protects Mice against Polymicrobial Sepsis Induced by Cecal Ligation and Puncture by Inhibiting Inflammation and Upregulating Protein C Pathway.� Journal of Natural Medicines, U.S. National Library of Medicine, Oct. 2009, www.ncbi.nlm.nih.gov/pubmed/19548065.
Meixner, Makayla. �Astragalus: An Ancient Root With Health Benefits.� Healthline, 31 Oct. 2018, www.healthline.com/nutrition/astragalus.
Nalbantsoy, Ay?e, et al. �Evaluation of the Immunomodulatory Properties in Mice and in Vitro Anti-Inflammatory Activity of Cycloartane Type Saponins from Astragalus Species.� Journal of Ethnopharmacology, U.S. National Library of Medicine, 31 Jan. 2012, www.ncbi.nlm.nih.gov/pubmed/22155389.
Peng, T Q, et al. �Effect and Mechanism of Astragalus Membranaceus on Coxsackie B3 Virus RNA in Mice.� Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi = Chinese Journal of Integrated Traditional and Western Medicine, U.S. National Library of Medicine, Nov. 1994, www.ncbi.nlm.nih.gov/pubmed/7703635.
Piao, Yuan-lin, and Xiao-chun Liang. �Astragalus Membranaceus Injection Combined with Conventional Treatment for Viral Myocarditis: a Systematic Review of Randomized Controlled Trials.� Chinese Journal of Integrative Medicine, U.S. National Library of Medicine, Oct. 2014, www.ncbi.nlm.nih.gov/pubmed/25098261.
Team, DFH. �Astragalus: Funny Name Serious Results.� Designs for Health, 9 Oct. 2018, blog.designsforhealth.com/astragalus-funny-name-serious-results.
Team, NCBI. �Astragalus Membranaceus. Monograph.� Alternative Medicine Review: a Journal of Clinical Therapeutic, U.S. National Library of Medicine, Feb. 2003, www.ncbi.nlm.nih.gov/pubmed/12611564.
Wang, Deqing, et al. �Study of the Effects of Total Flavonoids of Astragalus on Atherosclerosis Formation and Potential Mechanisms.� Oxidative Medicine and Cellular Longevity, Hindawi Publishing Corporation, 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3306992/.
Wu, Hong Mei, et al. �Interventions for Preventing Infection in Nephrotic Syndrome.� The Cochrane Database of Systematic Reviews, John Wiley & Sons, Ltd, 18 Apr. 2012, www.ncbi.nlm.nih.gov/pubmed/22513919.
Yang, Qing-you, et al. �Effects of Astragalus on Cardiac Function and Serum Tumor Necrosis Factor-Alpha Level in Patients with Chronic Heart Failure.� Zhongguo Zhong Xi Yi Jie He Za Zhi Zhongguo Zhongxiyi Jiehe Zazhi = Chinese Journal of Integrated Traditional and Western Medicine, U.S. National Library of Medicine, July 2010, www.ncbi.nlm.nih.gov/pubmed/20929124.
Zhang, Hong Wei, et al. �Astragalus (a Traditional Chinese Medicine) for Treating Chronic Kidney Disease.� The Cochrane Database of Systematic Reviews, U.S. National Library of Medicine, 22 Oct. 2014, www.ncbi.nlm.nih.gov/pubmed/25335553.
The University offers a wide variety of medical professions for functional and integrative medicine. Their goal is to inform individuals who want to make a difference in the functional medical fields with knowledgeable information that they can provide.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine