Dr. Jimenez, D.C., presents how to prevent atherosclerosis through various therapies that can help reduce the effects of cardiovascular diseases. By understanding the risk factors causing these issues, many specialists associated with cardiovascular disorders can develop a solution to minimize these symptoms that correlate with the vital organs and muscles with a personalized treatment plan. We acknowledge patients to certified providers that provide treatment options for cardiovascular disorders that can restore body functionality and improve a person’s health. We assess each individual and their symptoms by entrusting them to our associated medical providers based on their diagnosis results for a better understanding. We recognize that education is a tremendous way to ask our providers questions about the patient’s knowledge and symptoms. Dr. Jimenez, D.C., implements this information as an educational service. Disclaimer
The Cardiovascular System & Atherosclerosis
Dr. Alex Jimenez, D.C., presents: When the body deals with various issues causing muscle and joint pain, it could be due to overlapping risk profiles affecting the cardiovascular system. In a normal functioning body, the cardiovascular system works with different systems, including the musculoskeletal system, the pulmonary system, the endocrine system, the central nervous system, and the gut system. The heart is one of the main vital organs in the cardiovascular system that supplies oxygen-riched blood to the different muscles, tissues, and organs to function properly. The oxygen-rich blood also carries other items to circulate in the body, like hormones, protein, and nutrients, to be used later. However, when environmental factors start to disrupt the body, they can affect the cardiovascular system and can do serious damage. To that point, it can develop cardiovascular diseases over time and cause body pain. Many studies and research have shown cardiovascular diseases are still the number one in the world that causes mortality and morbidity in the body. They can cause other issues that can affect the body.
One of the cardiovascular diseases that can lead to heart dysfunction is atherosclerosis. Atherosclerosis is a buildup of plaque (fats, cholesterol, and other hard, sticky substances) that builds up over time along the artery walls that can slow down the blood flow, causing less circulation in the arteries. When the circulation becomes obstructed, it can lead to ischemia associated with a blood clot due to the different body areas not getting enough blood and oxygen to function properly.
Inflammation Associated With Atherosclerosis
Dr. Alex Jimenez, D.C., presents: When this happens, there can be an imbalance of LDLs (low-density lipoproteins) which can then develop various symptoms over time that can lead to muscle and joint pain. Some of the most common underlying reasons that can cause LDL imbalances associated with atherosclerosis could include the following:
Chronic inflammation
Immune dysfunction
Oxidative stress in the vascular system
Poor diet
Tobacco exposure
Genetics
Pre-existing cardiovascular disease
When various disruptors can damage LDL, it can become oxidized over time, damage the cardiovascular endothelium wall, and cause macrophage and platelet activation. To that point, once the macrophages start to eat, they form into foam cells and then explode and release peroxidation, which means that they damage the lining of the blood vessel.
Looking closer at the oxidized LDL, it can biotransform into pro-inflammatory markers and is correlated with vascular inflammation. When dealing with vascular inflammation, the body can develop metabolic endotoxemia. Metabolic endotoxemia is where LPS (lipopolysaccharides) levels elevate even though there is a presence of infections in the body. To that point, it can correlate to gut dysbiosis and chronic inflammatory diseases to stimulate the immune system to increase NFkB inflammatory cytokines and cause muscle and joint pain.
When there is an increase in inflammation due to atherosclerosis or any cardiovascular disease an individual may have, the signs and symptoms can vary depending on their environment. Excessive weight gain, hypertension, increased oxidative stress, high triglycerides, low HDLs, etc., can affect the body and make it dysfunctional. These mechanic factors can influence dysbiosis in the cardiovascular and gut systems, leading to chronic conditions like IBS, metabolic syndrome, and cardiovascular diseases.
Treatments To Lower Inflammation
Dr. Alex Jimenez, D.C., presents: So what can we do to reduce the inflammation associated with atherosclerosis causing muscle and joint pain? Well, one of the ways that many people can do this is by eating less refined carbohydrates, and high sugar can lower high glycemic levels in the body can reduce the risk of cardiovascular diseases. Another way is to try the Mediterranean diet, which includes lean proteins, nuts, extra virgin olive oil, heart-healthy vegetables, fresh fruits, and whole grains to reduce inflammatory markers from proceeding further to causing issues in the body. Even supplements and nutraceuticals like glutathione and omega-3s can reduce chronic inflammation and cardiovascular disease complications by enhancing their antioxidant properties to preserve redox homeostasis while regulating oxidative stress in the body.
Another way people can prevent atherosclerosis is by exercising regularly. An exercise routine is an excellent way to keep the heart pumping and allow the muscles to move. Any exercise like yoga, Crossfit, dancing, swimming, walking, and running will allow more oxygen intake to the lungs, allowing the heart to pump out more blood to allow more circulation to the various organs, muscles, and tissues. Plus, any exercise can reduce plaque buildup in the arteries and reduce inflammation in the muscles and joints affecting the body.
Chiropractic Care & Inflammation
Dr. Alex Jimenez, D.C., presents: And finally, treatments like chiropractic care can help restore functionality to the body through spinal manipulation. Now, how does chiropractic care correlate with cardiovascular diseases like atherosclerosis? When the body is dealing with inflammation and chronic stress associated with atherosclerosis, the decrease in blood circulation can cause internal organ dysfunction and disrupt the transmitted signals to reach the brain. So when the transmitted signals become blocked, it can cause spinal subluxation to the spine and invokes pain in the upper, middle, and lower sections of the back, neck, hips, and shoulders. To that point, a chiropractor incorporates mechanical and manual manipulation to realign the spine and allow joint and muscle function back to the body. At the same time, chiropractic care can work with other associated medical providers to develop a personal treatment plan that allows the body to begin its recovery process.
Conclusion
Our goal is to reduce inflammation and oxidative stress in the body to dampen the effects of cardiovascular diseases associated with pain. Covering some of the different ways to prevent atherosclerosis from affecting the cardiovascular system in the body can help the vital organs and muscles from producing more inflammation associated with pain. Incorporating heart-healthy and anti-inflammatory food, taking supplements, exercising, and going to treatments can make big changes to the body. The process may be tedious, but the results will slowly improve the body’s functionality and help the individual stay on the path of health and wellness.
Dr. Alex Jimenez, D.C., presents how the cause and effects of cardiometabolic risk can affect a person’s health and wellness. Cardiometabolic syndrome can affect any person through lifestyle factors and cause pain-like symptoms that can affect their well-being. We refer patients to certified providers that provide cardiovascular treatments associated with metabolic syndrome to relieve issues affecting the body while ensuring optimal wellness for the patient through various treatments. We acknowledge each patient by referring them to our associated medical providers based on their diagnosis to understand better what they are dealing with appropriately. We understand that education is an excellent way to ask our providers various intricated questions to the patient’s knowledge. Dr. Jimenez, D.C., utilizes this information as an educational service. Disclaimer
The Cause & Effects Of Cardiometabolic Risk
Dr. Alex Jimenez, D.C., presents: Now, as we enter this new era, many individuals are trying to find ways of managing cardiometabolic risk. So in this presentation, we will look at the number one killer in many modern countries; cardiovascular disease is defined as a cluster of conditions that affect the heart. Many factors are associated with cardiovascular disease that overlaps with metabolic syndrome. The word cardiometabolic hints that we will discuss something broader than cardiovascular risk.
The goal is to gain perspective on the old conversation about the cardiovascular risk associated with the circulatory system. We all know that the body’s circulatory, respiratory, and skeletal systems have different compartments that have different jobs to make the body functional. The problem is that the body operates in various systems independent of each other. They come together and interconnect like a web.
The Circulatory System
Dr. Alex Jimenez, D.C., presents: So the circulatory system helps transport blood vessels and allows the lymphatic vessels to carry cells and other items like hormones from one place to another. An example would be your insulin receptors moving information throughout your body and your glucose receptors being utilized for energy. And obviously, all other types of communicators govern how transportation happens in the body. Now the body is not a closed fixed circuit connected through the outside. Many factors can influence the body inside and outside that can affect the arterial wall and cause overlapping issues affecting the cardiovascular system. Now, what is happening to the arterial wall causing overlapping matters in the body?
When factors start to affect the arterial wall inside, it can cause plaque to form in the arterial walls and even affect the integrity of the outer walls of the arteries. When this happens, LDL or low-density lipoprotein could grow in size and cause a spike in cholesterol levels. To that point, when the body is dealing with poor lifestyle habits, it can influence the body to be at high cardiovascular risk. When the body is dealing will cardiovascular diseases at high risk, it can cause correlate to high blood pressure, diabetes, or metabolic syndrome. This causes the body to have muscular and joint pain in the back, neck, hips, and chest, to name a few, and can cause the individual to deal with inflammation in the gut, joints, and muscles.
Factors Associated With Cardiometabolic Risk Factors
Dr. Alex Jimenez, D.C., presents: But, interestingly, it’s not until recently that institutions that govern our standard of care are taking this seriously, saying it needs to be a part of the guidelines because the data is so evident that how a person’s lifestyle matters when it comes to their health. The data can range from the correlation of how certain diets, like the Mediterranean diet, can change a person’s nutritional habits. To how stress is associated with cardiometabolic disorders. Or how much exercise or sleep you are getting. These environmental factors correlate to how cardiometabolic risk factors affect the body. By informing patients what is going on with their bodies, they can finally make small changes to their lifestyle habits. Now let’s look at how nutrition can impact a person with cardiometabolic risk profiles.
By having a conversation about nutrition, many people can see the impact of the standard American diet and how it can lead to a caloric increase in central adiposity. When conversing about nutrition, it is best to note what the person is eating, causing cardiometabolic risk issues in their bodies. Doctors work with nutritionists to devise a solution to implement the right amount of protein the individual needs, how much vegetables and fruits they can consume, and what food allergies or sensitivities to avoid. To that point, informing patients about eating healthy, organic, and nutritional food will allow them to understand what they put in their bodies and how to reverse the effects. Now each person is different as certain diets are for some people while others don’t, and it is also important that by advising patients about what they are taking in and consuming but also about timing. Some people do fasting to cleanse their bodies of toxins and allow the body’s cells to find different ways to consume energy.
How Nutrition Plays A Role In Cardiometabolic Syndrome
Dr. Alex Jimenez, D.C., presents: But did you know the quality of calories in the standard American diet can damage our intestinal lining, making it vulnerable to permeability, creating this very common scenario called metabolic endotoxemia that triggers inflammation? The quality and quantity of foods can disrupt our microbiome, leading to dysbiosis as a different mechanism of inflammation. And so you get this immune activation and dysregulation that makes a constant bath in which your genes are bathing. Inflammation can be good or bad depending on the severity of what is happening in the body. If the body suffers from an injury or deals with minor issues, inflammation can help heal. Or if the inflammation is severe, it can cause the intestinal wall lining to become inflamed and leak out toxins and other microbes into the rest of the body. This is known as a leaky gut, potentially leading to muscle and joint pain associated with obesity. So we want to broaden that conversation around nutrition because obesity impacts poor nutrition. It’s commonly said that we are overfed and undernourished as a human population. So we want to be able to mitigate the trends of obesity responsibly. And we want to bring in this larger conversation about social determinants of health. As the years go by, many people are more aware of how their environment and lifestyle play a role in developing cardiovascular or cardiometabolic conditions.
We must recognize that the human body lives in this social ecosystem that determines the health potential. We want to engage the patient to bring awareness to the most potent anti-inflammatory signal into their lives and their lifestyle choice. And we are not discussing fads like putting on spandex and going to the gym once a month; we’re talking about daily movement and how to reduce sedentary behavior associated with the cardiometabolic syndrome. We discussed how even the impact of stress could promote atherosclerosis, arrhythmias, and metabolic dysfunction in the body and cause various issues that can affect a person’s well-being.
Stress & Inflammation’s Role In The Body
Dr. Alex Jimenez, D.C., presents: Stress, like inflammation, can be good or bad, depending on the scenario. So stress can impact a person’s ability to function in the world as we dive into the systems biology dysfunctions that occur from acute and chronic stress and how we can help our patients. We must understand that we should put ourselves in our patient’s shoes by figuring out how to lower chronic stress to reduce cardiometabolic risk factors and improve quality of life.
So by not being so fixated on trying everything at once to reduce cardiometabolic risk factors, taking everything that we learn and incorporating it slowly into our daily lives can make a huge impact on how we look, feel, and what we eat can improve our well-being. Dr. David Jones stated, “If all we do is talk about this and all we do is know this stuff, it doesn’t do the full service we have as an intention for our patients.”
We must get ourselves from the knowing stage into the doing stage because that’s when results will occur. So by looking at the bigger picture, we can take back our health from cardiometabolic syndrome by focusing on where the problem is happening in our bodies and going to various specialists that can develop a treatment plan to lower the stress and inflammation in our bodies that can reduce the effects of cardiometabolic syndrome.
Conclusion
Dr. Alex Jimenez, D.C., presents: So if many people are dealing with cardiometabolic risks, they have these very common systems, biology dysfunctions, whether it’s related to inflammation, oxidative stress, or insulin dysfunction, are all happening under the surface. . In functional medicine, we want to go upstream in this new era of cardiometabolic health. We want to leverage the environment and lifestyle to manipulate the system’s biology so it can be in a favorable setting to allow the epigenetic potential of the patient to be at its highest expression of health.
By providing the right tools for the patients, many functional medicine doctors can educate their patients on how to take back their health a little bit each time. For example, a person is dealing with chronic stress, causing stiffness in their necks and backs, making them unable to move around. Their doctors can devise a plan to incorporate meditation or take a yoga class to ease the stress out of their bodies and become mindful. So by gathering important clinical information about how a person is suffering from cardiometabolic, many doctors can work with their associated medical providers to devise a treatment plan to cater to each suffering from symptoms associated with cardiometabolic.
The chest has the pectoralis major muscle that works with the upper half of the body that provides mobility and power. The pectoralis major also surrounds the clavicle skeletal structure and works with the thoracic spine. The chest allows mobility to the arms and stability to the shoulders while working together with the shoulder and arm muscles. Many individuals utilize the upper body more when working out, lifting, or carrying objects from one place to another. This causes the muscle to become overused and succumb to injuries that can affect the functionality of the chest and invoke pain-like symptoms in the body. One of the chest muscles affected by pain is the pectoralis muscles, especially the pectoralis minor muscle. Today’s article looks at the pectoralis minor muscle, how myofascial pain affects the pectoralis minor, and how to manage myofascial pain associated with the pectoralis minor. We refer patients to certified providers specializing in chest pain therapies to aid many people suffering from trigger point pain affecting the minor muscles of the pectoralis. We brief patients by referring them to our associated medical providers based on their examination when appropriate. We indicate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Pectoralis Minor Muscle
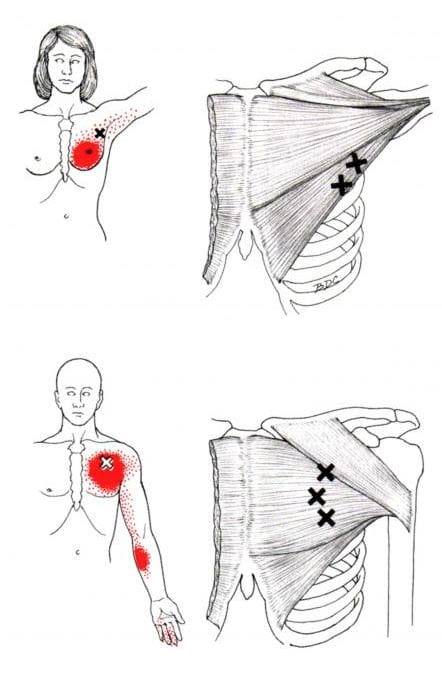
Have you been experiencing pain in your upper-mid back? Do you feel like your chest is feeling compressed constantly? Do you feel the tension in your shoulders that makes it difficult to reach behind your back? Most of these symptoms are signs that many individuals are developing myofascial pain along the pectoralis muscles, especially the pectoralis minor. The pectoralis minor muscle is a thin triangular-shaped muscle below the pectoralis major. It has a crucial part of the chest as it helps stabilize the scapula (the shoulder blades) and is in front of the thoracic wall of the spine. The pectoralis minor is also part of the respiratory muscle group that works with the lungs. The pectoralis minor muscle has many functions for the shoulder blades, which include:
Stabilization
Depression
Abduction or Protraction
Internal Rotation
Downwards Rotation
When environmental factors begin to affect the lungs and cause respiratory issues in the body, the surrounding respiratory muscle group also gets involved, causing the body to be hunched over.
Myofascial Pain Affecting The Pectoralis Minor
When environmental factors begin to affect the lungs, it causes the respiratory muscles to contract and become compressed. This is just one of the many factors that can affect the pectoralis minor muscle. The other factor is that the pectoralis minor muscle may be short in the chest and when individuals try to reach behind their backs. This causes the pectoralis minor muscle to to be overstretched and develop myofascial pain or trigger points along the muscle fibers. The book, “Myofascial Pain and Dysfunction,” written by Dr. Travell, M.D., described the pain from myofascial pain associated with the pectoralis minor to be similar to cardiac pain. This is known as referred pain caused by myofascial pain syndrome and it can be a bit difficult to diagnose since it can mimic other chronic issues. Studies reveal that shortening or any sort of tightness of the pectoralis minor is one of the potential biomechanical mechanisms that is associated with an altered scapular alignment which causes pain and shoulder movement impairments. Overusing the pectoralis minor muscles creates tiny nodules that can affect the stability of the shoulders and causes upper-mid back problems in the thoracic region of the spine.
An Overview Of Trigger Points On The Pectoralis Minor- Video
Have you been experiencing difficulty inreaching behind your back? Do you feeling your body becoming more hunched over than usual? Or have you been experiencing chest pain constantly? These pain-like symptoms are caused by myofascial pain associated with the pectoralis minor muscle. The pectoralis minor muscle helps with the stability of the shoulders and studies reveal that when the presense of myofascial trigger points are linked to shoulder and upper body disorders, it can increase the risk of overlapping conditions that trigger points can mimic. Myofascial trigger points are a common complaint as it can significantly impact a person’s daily activites by causing the taut muscle band to be tender or hypersenitive. When this happens, it can lead to issues of muscle imbalance, weakness and impaired motor function. Thankfully, there are various techniques that can help reduce the pain symptoms and issues in the pectoralis minor muscle, while mananging the trigger points. The video above explainshow to tell when your chest muscles are tight and various tests to know when the pectoralis muscles (both the minor and major) are being affected by trigger points.
Managing Myofacial Pain Associated With Pectoralis Minor
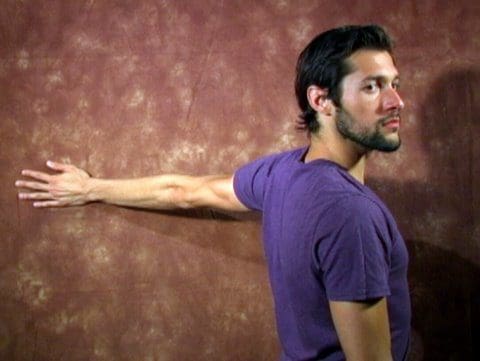
When dealing with chest pains associated with myofascial pain along the pectoralis minor, there are many techniques they can incorporate to prevent myofascial pain from causing further damage to the muscle itself and the surrounding muscles. Various chest stretches can help gently loosen the stiff muscles, warm the pectoralis minor, and improve mobility to the chest and shoulders. Correct posture can help prevent the body from being hunched over constantly and let the surrounding muscles and the pectoralis minor relax. If the pain is unbearable, studies reveal that treatments like dry needling and palpations on the pectoralis minor muscles can help manage the pain caused by trigger points. This kind of treatment allows the muscle to release the trigger point and, combined with a hot or cold pack, can reduce the chances of myofascial pain from forming again in the muscle.
Conclusion
Underneath the pectoralis major muscle, the pectoralis minor is a thin triangular-shaped muscle that helps stabilize the shoulder blades and is located in the front of the thoracic wall of the spine. This tiny muscle is part of the respiratory muscles that have a causal relationship with the lungs and can succumb to environmental factors that can lead to the development of myofascial pain or trigger points on the pectoralis minor. Myofascial pain associated with the pectoralis minor muscle can mimic cardiovascular issues and invoke pain in the muscle. Fortunately, various treatments can help relieve and manage myofascial pain from re-occurring in the pectoralis minor.
References
Bagcier, Fatih, et al. “Three Simple Rules in Pectoral Muscle’s Trigger Point Treatment, Which May Be a Cause of Chest Pain: Position, Palpation, and Perpendicular Needling.” American Board of Family Medicine, American Board of Family Medicine, 1 Nov. 2020, https://www.jabfm.org/content/33/6/1031.long.
Baig, Mirza A, and Bruno Bordoni. “Anatomy, Shoulder and Upper Limb, Pectoral Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 11 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK545241/.
Morais, Nuno, and Joana Cruz. “The Pectoralis Minor Muscle and Shoulder Movement-Related Impairments and Pain: Rationale, Assessment and Management.” Physical Therapy in Sport : Official Journal of the Association of Chartered Physiotherapists in Sports Medicine, U.S. National Library of Medicine, Jan. 2016, https://pubmed.ncbi.nlm.nih.gov/26530726/.
Ribeiro, Daniel Cury, et al. “The Prevalence of Myofascial Trigger Points in Neck and Shoulder-Related Disorders: A Systematic Review of the Literature.” BMC Musculoskeletal Disorders, BioMed Central, 25 July 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6060458/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
The chest in the upper half of the body comprises various structures that each have a job to keep the body functioning. The chest has different large muscles surrounding the ribcage and helps protect the vital organs that allow the host to breathe. The essential organs protected by the ribcage and the chest muscles include the heart and the lungs. These two organs aid the chest with blood circulation, breathing, and digestion to keep the body moving and functional. When injuries or chronic conditions begin to affect the chest, it can cause the muscles surrounding the ribcage to contract and tighten, causing the heart and lungs to work harder and causing various issues to affect the body. This can lead to chronic symptoms in the chest and affect a person’s life. Today’s article looks at the pectoralis major muscle in the chest, how trigger point pain is associated with chest pain, and how to manage trigger points in the chest. We refer patients to certified providers who specialize in chest pain therapies to aid many people suffering from trigger point pain affecting the pectoralis major muscles. We brief patients by referring them to our associated medical providers based on their examination when appropriate. We indicate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., takes note of this information as an educational service only. Disclaimer
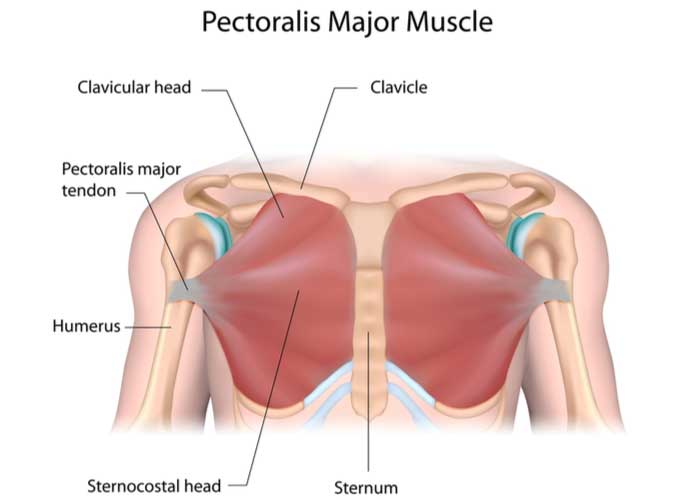
The Pectoralis Major Muscles In The Chest
Have you been experiencing unexplainable chest pains that mimic heart issues? Do you feel muscle stiffness near your clavicle? Or do your chest muscles feel tenser and sorer than usual? Many of these issues affecting the chest could result from trigger points associating with the chest along the pectoralis major muscles. The pectoralis major is the superior and largest muscle in the chest wall’s front area. This muscle looks like a thick fan that surrounds the clavicle and works with the chest and arms to provide mobility and power to the upper body. Studies reveal that the pectoralis major muscle plays an important role in upper limb movements. To that point, it can help with the adduction and medial rotation of the arm, according to the book by Dr. Travell, M.D. “Myofascial Pain and Dysfunction,” the pectoralis muscle works with the rest of the chest muscles while being assisted by the teres major and minor muscles, the anterior and posterior deltoid muscles, the subscapularis muscles, and the tricep muscles. The pectoralis major muscles can also be affected by multiple issues affecting the chest and the rest of the upper half of the body.
Trigger Point Pain Associated With The Chest
When the pectoralis major muscles are affected by various issues, they can mimic other chronic conditions that are causing referred pain in different body areas. This is known as trigger point pain, and it can cause overlapping risk profiles on the pectoralis major muscles that can affect the chest. Trigger points are slightly difficult to diagnose as many factors, like repetitive motions or lifting heavy objects, can cause the affected muscles to develop tiny knots along the muscle fibers and cause pain-like symptoms. Many people with chest pains often complain that something is affecting their heart as they place their hands on their chest and gently rub the affected area. However, when their doctors examine them, the issue is not their hearts but their chest muscles. Studies reveal that trigger points affecting the affected muscle can mimic issues like cardiovascular dysfunction in the heart. To that point, active trigger points in the pectoralis major muscle can cause somato-visceral pain to the heart, mimicking cardiovascular issues like paroxysmal arrhythmia. It can also cause visceral-somatic pain where the heart suffers from cardiovascular problems affecting the pectoralis major muscles.
Trigger Point Therapy On The Pectoralis Major-Video
Have you been dealing with chest pains that cause you to hunch over? Does your chest seem to feel tight when you stretch? Or have your chest muscles feel tender to the touch? These pain symptoms are caused by trigger points affecting the pectoralis muscles. Trigger points are generated when a person overuses their muscles from daily activities or succumbs to muscle injuries that cause referred pain in different body areas. So trigger points affecting the pectoralis major muscle may cause chest pains. The video above explains the pectoralis muscles and where the trigger points are located that cause referred pain to the shoulders and the rest of the upper half of the body. Trigger points associated with the chest along the pectoralis major muscles can be treatable through various treatments and techniques that can reduce the symptoms and prevent trigger points from forming along the affected muscle in the future.
Ways To Manage Trigger Points On The Chest
When trigger points affect the pectoralis major muscles, they can invoke chest pain-like symptoms that resemble a cardiovascular disorder. Fortunately, pain specialists like chiropractors, massage therapists, and physiotherapists can utilize various techniques to help reduce the pain caused by trigger points. Studies reveal that when local and referred pain affects the pectoralis major muscle, multiple massage treatments targeting the trigger points can help alleviate the symptoms causing chest pains. Another way people can manage trigger points is by stretching the pectoralis major muscle to relieve tension and soreness in the chest. Incorporating various stretching techniques to alleviate chest pain can help loosen up the stiff muscles and warm them up before a vigorous workout. This allows the pectoralis muscles to provide optimal output on a person’s health and wellness.
Conclusion
The pectoralis major is a thick fan-shaped muscle located on the chest. This muscle works with the shoulders and upper half of the body while protecting the heart and the lungs from various injuries and chronic conditions. When these muscles become affected by injuries or chronic conditions, they can develop trigger points along the chest, causing referred pain to the pectoralis major muscles. This can lead to somato-visceral and visceral-somatic pain symptoms in the chest and make many individuals miserable. Luckily pain specialists who can help manage trigger points along the affected muscle utilize various techniques to reduce the symptoms and prevent trigger points from forming in the affected muscle again. This allows the individual to continue with their daily activities without worrying about chest pains.
References
Haładaj, Robert, et al. “Anatomical Variations of the Pectoralis Major Muscle: Notes on Their Impact on Pectoral Nerve Innervation Patterns and Discussion on Their Clinical Relevance.” BioMed Research International, Hindawi, 2 Apr. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6466946/.
Moraska, Albert F, et al. “Responsiveness of Myofascial Trigger Points to Single and Multiple Trigger Point Release Massages: A Randomized, Placebo Controlled Trial.” American Journal of Physical Medicine & Rehabilitation, U.S. National Library of Medicine, Sept. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5561477/.
Simons, David G. “Cardiology and Myofascial Trigger Points: Janet G. Travell’s Contribution.” Texas Heart Institute Journal, U.S. National Library of Medicine, 2003, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC152827/.
Solari, Francesca, and Bracken Burns. “Anatomy, Thorax, Pectoralis Major Major.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 26 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK525991/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Everyone wants to be healthier at some point in their lives. Some individuals train to be athletes and must follow procedures to maintain their health. In comparison, others want to get healthier by eating the right food, exercising for at least 30 minutes to an hour, meditating or doing yoga to relieve stress, and maintaining a healthy weight. However, many environmental factors do affect the human body. They can alter how a person looks, weight, levels of physical activity, and how different foods affect the body’s metabolism. When environmental factors start to take hold of a person’s health, it can trigger unwanted issues that affect not only the muscles in the body but the associated internal organs that help provide the functionality to the body. Today’s article focuses on the musculoskeletal system, how different issues affect the musculoskeletal system and associate with other problems in the body, and various treatments to improve musculoskeletal health. We refer patients to certified providers specializing in musculoskeletal therapies that help those with musculoskeletal disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Musculoskeletal System & Its Function
How does the musculoskeletal system play its role in the human body? The body is considered a complex being that consists of various organs, muscles, tissues, ligaments, and joints that help move a person from one place to another, resting while needed, and doing multiple activities in a casual relationship. Studies reveal that the musculoskeletal system is controlled by the central nervous system that interconnects the motor-sensory function for the body’s ability to move and rest.
The three main muscle groups that make up the musculoskeletal system are:
Skeletal muscle- Muscle tendons that are connected to the bones
Cardiac muscle- Muscles associated with the heart
Smooth muscle- Muscles that line with blood vessels and specific organs (ex. intestines)
Each muscle group provides different functions that correlate to how the body moves. Skeletal muscles make the legs and arms move. Cardiac muscles help the heart pump blood to the various muscles, organs, and tissues. Smooth muscles help specific organs (intestines, stomach, and urinary tract) digest, collect nutrients, and eliminate toxins in the body.
Issues That Affect The Musculoskeletal System
These factors are related to different issues that can not only disrupt the musculoskeletal system but can be an overlap of profiles affecting the cardiovascular system, spinal health, and gut system. The different factors that are associated with the musculoskeletal system are:
Obesity
Lack of physical activity
Poor Posture
Inflammation
Unhealthy Diet
How would various factors implicate musculoskeletal issues while triggering different bodily problems? Well, let’s use obesity as an example. Obesity is associated with issues like back and joint pain as studies reveal that these musculoskeletal issues make up pain and disability as a dominant source. A poor diet of processed foods high in fats and sugars can be associated with the risk of developing obesity.
Not only that, but obesity could potentially be involved in the thoracic spine and upper back pain due to the result of physical inactivity and poor dieting. The weight on the body can strain the muscles and ligaments in the back, causing the spinal vertebrae to become misaligned and pressure the nerves exiting the spinal cord. The misalignment of the vertebrae is called a subluxation. When a person is suffering from upper back pain, it can overlap with chest pain, which can be a concerning issue to vital organs like the heart, which potentially involved in the risk of cardiovascular disease. It is related to subluxation that may affect the heart contraction rate, rhythm, and power through the sympathetic efferent pathways originating from the thoracic region.
An Overview Of The Musculoskeletal System-Video
Are you experiencing pain in your upper back or chest? How about cardiac issues associated with shouldering and arming pain? Many of these issues are related to factors that affect the musculoskeletal system that might potentially be involved with chronic issues. The video above summarizes the musculoskeletal system’s role in the body. When environmental factors become a risk of developing musculoskeletal disorders that can potentially be involved in different bodily problems, studies reveal that musculoskeletal disorders associated with abnormal functions may cause a significant impact on regular performances. An example would be a person dealing with bad hip pain and cannot do any exercises triggering heart issues. This is defined as somato-visceral pain where the affected muscle is associated with an internal organ being a pain mediator.
Treatments For Improving Musculoskeletal System
In most treatments, many individuals utilize the following to improve not only the musculoskeletal system but other issues that affect the body:
Exercise
Healthy Diet
Stress Management Treatments
Chiropractic Therapy
No matter what affliction or health problem a person is dealing with, having the best treatment solution possible is a start on a person’s health and wellness journey. The first step is to have a precise diagnosis to the doctor while giving as much information as possible is critical. Providing them with a complete health history is an essential first step. After a manual examination of the issues causing them pain, the primary physician could refer the individual for chiropractic care to relieve issues affecting their musculoskeletal system.
Many people usually only associate chiropractic care with back problems. Still, the reality is that chiropractic therapy can be helpful for the musculoskeletal system and various issues related to the muscles and organs. A chiropractor can provide therapeutic stretches and recommend exercises to individuals to help them avoid the same problems later on. Many chiropractors offer recommendations and nutrition that individuals can utilize to help improve their condition. For the musculoskeletal system, a healthy diet may help achieve and maintain a healthy body weight while reducing the risk of chronic disease. Eating the right amount of healthy greens, fruits, beneficial carbs, and healthy fats can help reduce the risk of developing chronic issues in the body like cardiovascular diseases. However, if primary cardiac problems affect the body, it is best to seek medical attention as soon as possible.
Conclusion
The body is considered a complex being that consists of various organs, muscles, tissues, ligaments, and joints that provide various activities to the host. The musculoskeletal system has three muscle groups: skeletal, cardiac, and smooth muscles provide different functions that correlate to how the body moves. When various factors begin to cause issues to the musculoskeletal system, they can potentially be involved with pain issues that affect more than the body. Treatments like chiropractic care, a healthy diet, exercise, and stress management may be the stepping stones to alleviating various issues that are affecting the musculoskeletal system and a great start in achieving health and wellness.
References
Kennel, Peter J, et al. “Skeletal Muscle Changes in Chronic Cardiac Disease and Failure.” Comprehensive Physiology, U.S. National Library of Medicine, 20 Sept. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6752037/.
Malik, Khalid M, et al. “Musculoskeletal Disorders a Universal Source of Pain and Disability Misunderstood and Mismanaged: A Critical Analysis Based on the U.S. Model of Care.” Anesthesiology and Pain Medicine, Kowsar, 15 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6348332/.
Murphy, Andrew C, et al. “Structure, Function, and Control of the Human Musculoskeletal Network.” PLoS Biology, Public Library of Science, 18 Jan. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5773011/.
Stochkendahl, Mette J, et al. “Diagnosis and Treatment of Musculoskeletal Chest Pain: Design of a Multi-Purpose Trial.” BMC Musculoskeletal Disorders, BioMed Central, 31 Mar. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2315652/.
The heart is a fantastic muscle in the body that allows hormones, oxygenated blood, and nutrients to travel and transport to all the muscles, tissues, and organs, providing functionality to the body. As one of the main components of the cardiovascular system, the heart works together with the lungs to help carry the deoxygenated blood to the pulmonary system to dispose of waste from the body. The human body needs the heart to stay healthy; however, factors like stress, obesity, autoimmune diseases, and unhealthy habits can affect the heart, causing cardiac issues associated with various body problems. Today’s article focuses on coronary heart disease, what are the risks associated with coronary heart disease, and ways to prevent coronary heart disease from progressively getting worse. We refer patients to certified providers specializing in cardiology treatments that help those with issues of coronary heart disease. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Coronary Heart Disease?
Have you been experiencing hypertension in your body or near your heart? How about unexplained chest pains that randomly showed up? Have you experienced pain running down your shoulders and arms? Many of these are signs that you could be experiencing coronary heart disease. Research studies have defined coronary heart disease as a common heart condition with plaque formation in the heart vessels that cuts off the supply of oxygenated blood to the heart and the rest of the body. As part of cardiovascular diseases, coronary heart disease can cause overlapping profile issues over time if it is not treated right away. Many disruptive factors can affect the heart muscle like:
Age and gender
Oxidative stress
Inflammation
Vascular immune dysfunction
Lack of physical activities
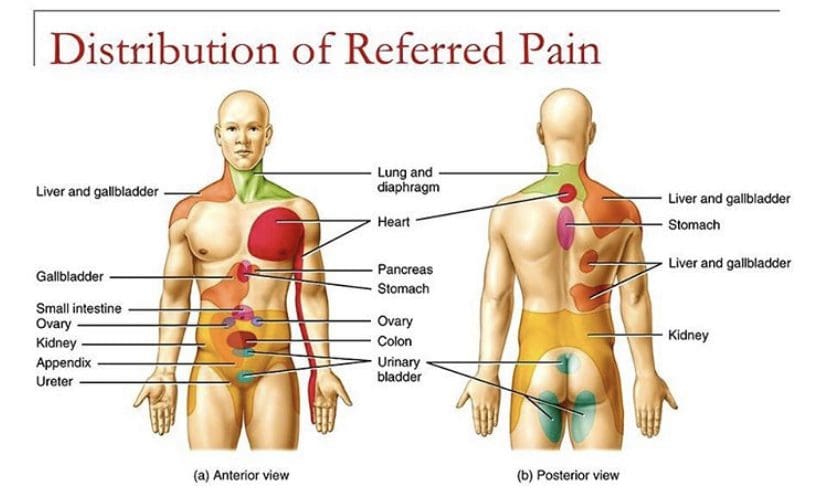
These disruptive factors can increase cardiovascular disease mortality that can affect the heart and be co-morbidities associated with different issues affecting the body. Studies reveal that the mechanisms of cardiac pain are associated with the chest and upper left arm pain. This is defined as referred pain where the sensory input from visceral organs mimics cardiac distress, and the corresponding muscles are affected. But how does this correlate to the heart muscle, and why does the chest experience pain? Visceral pain is a bit trickier to diagnose when cardiovascular disorders overlap the risk profiles associated with other issues affecting the body. For example, you could be experiencing pain in your chest and upper back, but your brain is telling you something is affecting your heart.
An Overview Of CAD-Video
Have you experienced shortness of breath? How about pain located in your chest or radiating from your shoulders and arms? Have you noticed inflammation occurring in your body? Many of these are signs and symptoms of you experiencing coronary artery disease in your body. The video above explains what coronary artery disease is and the risk factors associated with the progression of this common heart disease. Studies reveal that the risk factors can overlap in profiles that contribute to the development of coronary heart disease:
Environmental factors
Lifestyle habits
Diabetes mellitus
Obesity
Symptomatic angina
Smoking
When a person has these risk profiles overlapping different associated issues, their body becomes dysfunctional. Sometimes the symptoms affect other areas of the body, while the brain might be signaled that something is wrong with the heart. Since coronary artery disease progresses slowly over time, many individuals don’t experience the symptoms affecting their heart muscles.
Risk Issues Associated With CHD
Some of these symptoms that overlap in risk profiles may seem like heart issues but may refer to different problems affecting the body. This is defined as viscero-somatic pain, where the pain in the internal organs is associated with the corresponding muscles that share the same nerve. Chest pain associated with heart issues is a perfect example. Studies reveal that chest pains can become indistinguishable from angina, which may result from abnormalities in the thoracic viscera that overlap in profiles with heart issues. So what does it mean? It implies that sensory neurons from different visceral organs might mimic cardiac pain-causing risk-associated problems that affect the thoracic region of the spine triggering neck and upper back issues. Everything is connected as chest pains, dyspnea, and dyspepsia are intertwined with the thoracic anteriority becoming a mediator for cardiovascular diseases.
Ways To Prevent CHD
So let’s visualize a person going to their primary physician due to them experiencing heart issues associated with chest pains after the doctor goes through a manual examination on checking the individual’s heart and chest to see what problems are affecting the body. What does this implicates, and how do chest and back pains correlate with each other if there are heart issues? Studies reveal that the peripheral tissues in the body might be damaged from traumatic events that cause an inflammatory swelling in the cervical and thoracic region of the spine, causing muscle stiffness. Chiropractic care might be the answer to relieving pain and swelling triggering cervical and thoracic pain. Chiropractors use chiropractic adjustments to deliver a non-invasive, gentle treatment that reduces spinal misalignments to enhance the functionality of the musculoskeletal system. This will improve spinal health in the cervical and thoracic regions of the body by decreasing inflammatory swelling associated with heart issues. Chiropractic care, a healthy diet, and exercise also work hand in hand by positively impacting co-morbidities of coronary heart disease and other body problems like obesity to reduce cholesterol, help strengthen the weak muscles along the neck and upper back, and promote blood flow to the heart.
Conclusion
As part of the cardiovascular system, the heart supplies hormones, oxygenated blood, and nutrients throughout the entire body by ensuring that the muscles, tissues, and organs are functioning. When factors like stress, obesity, and unhealthy habits begin to affect the heart, it can develop cardiac issues like coronary heart disease associated with various body problems. Chest pains associated with heart issues that trigger neck and back pain in the body are known as viscero-somatic pain. Available treatments like chiropractic care and changing unhealthy habits work hand in hand to positively impact co-morbidities of coronary heart disease and reduce muscle stiffness along the neck and back muscles of the cervical and thoracic spine.
References
Börjesson, M. “Visceral Chest Pain in Unstable Angina Pectoris and Effects of Transcutaneous Electrical Nerve Stimulation. (TENS). A Review.” Herz, U.S. National Library of Medicine, Apr. 1999, https://pubmed.ncbi.nlm.nih.gov/10372297/.
Foreman, Robert D, et al. “Mechanisms of Cardiac Pain.” Comprehensive Physiology, U.S. National Library of Medicine, Apr. 2015, https://pubmed.ncbi.nlm.nih.gov/25880519/.
Malakar, Arup Kr, et al. “A Review on Coronary Artery Disease, Its Risk Factors, and Therapeutics.” Journal of Cellular Physiology, U.S. National Library of Medicine, Aug. 2019, https://pubmed.ncbi.nlm.nih.gov/30790284/.
Shahjehan, Rai Dilawar, and Beenish S Bhutta. “Coronary Artery Disease – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 9 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK564304/.
In the body, the heart is a vital organ that pumps blood to all the muscles, organs, tissues, and ligaments that require the body to function and move. As part of the cardiovascular system, the heart keeps the body alive by supplying nutrients and disposing of waste and carbon dioxide away from the body. Various factors can affect the body and the heart as well stressful events, unhealthy eating habits, limited physical activities, or autoimmune conditions can cause strain on the heart. Still, they can correlate to different symptoms in the body. This causes an overlap of risk profiles that may feel something is wrong with the heart but might affect another body part. Today’s article focuses on viscero-somatic pain affecting more than the heart muscle, how referred pain is defined, and various ways for treating viscero-somatic pain in the body. We refer patients to certified providers specializing in cardiovascular and chiropractic treatments that help those with issues that affect their hearts. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Visceral-Somatic Pain Affecting More Than The Heart
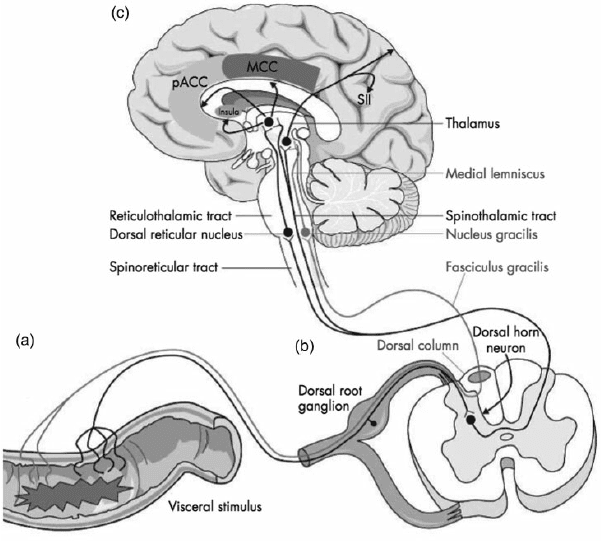
Are you experiencing radiating pain affecting your neck, arms, or back? How about feeling discomfort in your chest? Do gut issues seem to cause a burning sensation affecting your chest? Many of these symptoms overlap in risk profiles that seem like issues in the heart but can refer to something else affecting the body. This is known as viscero-somatic pain, usually defined as pain coming from the internal organs affecting the muscles that share the same nerve. Studies revealed that the autonomic nervous system mediates visceral-somatic pain. For the heart, the parasympathetic innervation comes from the cardiac branches of the vagus nerves connected to the spine and the brain. Since there is extensive autonomic innervation of the heart, the vagus nerve has a minor role in afferent pain transmission signaling.
An example would be having esophageal issues that are causing chest pains in your chest. So how would that correlate to the heart? Think of it as a person experiencing chest pains and whose brain is being signaled that something is wrong with their heart. Then, when they get treated, their results show that it was esophageal issues. Studies have revealed that spinal neurons receive input from a distal esophagus and receive the same information from the heart through viscero-somatic and viscero-visceral convergence. So what does this mean? This means that the sympathetic innervation of the heart is in a casual relationship to the first five thoracic spinal nerves. This indicates that some pain fibers affecting the heart are directly from the upper thoracic spine. Additional studies have mentioned that the vagus nerve connected to the upper thoracic spine can influence harmful afferent signals of the visceral organs to involve pain and joint stiffness in multiple organs and body structures.
Visceral Pain Explained- Video
Do you feel pain occurring on your shoulders or neck? How about severe pressure on your chest that might be something else? Or have you noticed issues that are affecting your heart are affecting your chest? Many of these are signs of visceral pain, where the pain of the damaged organ affects the muscle in a different body location. The video above explains visceral pain and uses an example of the cardiac muscle being affected by visceral pain. Studies reveal that the sensory input from different visceral organs can mimic cardiac pain due to viscero-somatic convergence of the cardiac input affecting the spinothalamic tract neurons in the spine to cause back issues in the thoracic region. So what does this implicates to the body? Well, say a person is experiencing chest and shoulder pains in their body; however, they’re experiencing heart problems that also affect them.
Treating Visceral-Somatic Pain In The Body
So, a person starts experiencing chest pain radiating from heart issues and goes to the doctor to see what is wrong with them. The physicians will begin to check on their hearts to see if anything is wrong or will be looking at their spine and chest through manual examination to see what is the issue that is affecting their bodies. So what does this mean to the body? Well, it could indicate that joint and muscle dysfunction in the neck and thorax is causing non-cardiac issues in the body. The influence of the spinal nerves on the cardiovascular function of the heart, since the afferent and parasympathetic efferents innervation of the heart, could disturb the upper cervical subluxation as the vagus nerve is being compressed. This correlates to other visceral organs mimicking cardiac pain and being the cause of musculoskeletal issues in the back.
Conclusion
In conclusion, the heart is a vital organ in the body that pumps blood to all the muscles, organs, tissues, and ligaments for functionality and nutrients distribution. The heart also share nerves in the parasympathetic innervation that connects to the vagus nerves which connects to the spine and brain to send information. However, various factors like lifestyle habits can affect the heart muscle and cause the individual chest pains that the brain is getting the signals that something is wrong with the heart. This is known a viscero-somatic pain where affected organs can cause muscle issues in the body in a different location. Treatments are available to figure out what the problem is going on with the body to understand better how to alleviate these viscero-somatic issues.
References
Foreman, Robert D, et al. “Mechanisms of Cardiac Pain.” Comprehensive Physiology, U.S. National Library of Medicine, Apr. 2015, https://pubmed.ncbi.nlm.nih.gov/25880519/.
Garrison, David W, et al. “Viscerosomatic Convergence onto Feline Spinal Neurons from Esophagus, Heart and Somatic Fields: Effects of Inflammation.” Pain, U.S. National Library of Medicine, June 1992, https://pubmed.ncbi.nlm.nih.gov/1408304/.
Leach, Austin, and Mike Fisher. “Myocardial Ischaemia and Cardiac Pain – a Mysterious Relationship.” British Journal of Pain, SAGE Publications, Feb. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4590151/.
Soares, Bruno, et al. “Accuracy of Physical Assessment in Nursing for Cervical Spine Joint Pain and Stiffness: Pilot Study Protocol.” JMIR Research Protocols, JMIR Publications, 17 Dec. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8726037/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine