Live Pain-Free: Chiropractic and Integrative Care for Injury Recovery at El Paso Back Clinic
In the vibrant heart of El Paso, Texas, where desert trails beckon and hardworking days define our community, injuries can derail your active lifestyle. From car accidents to workplace strains or sports mishaps, overexertion and trauma often lead to pain, stiffness, or chronic issues that linger without proper care. These setbacks can limit your ability to work, play, or enjoy El Paso’s unique spirit. At El Paso Back Clinic, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, chiropractic and integrative care offer a path to recovery. Through spinal adjustments, soft tissue therapy, and neuromuscular re-education, the clinic accelerates healing, restores flexibility, enhances balance, and boosts heart and lung function. With holistic nutrition and stress management plans, Dr. Jimenez’s team crafts personalized strategies to prevent future injuries, empowering El Pasoans to live pain-free and thrive.
This article explores how injuries arise, the benefits of integrative care, and how El Paso Back Clinic delivers top-tier recovery solutions.
The Impact of Overuse and Accidents: Why Pain Persists
El Paso’s dynamic lifestyle—hiking the Franklin Mountains, working long shifts, or driving busy roads—can strain the body. Overexertion from repetitive tasks like lifting or intense workouts causes sprains, strains, or joint issues. Motor vehicle accidents (MVAs) bring sudden trauma, with 60% of cases leading to lingering pain if untreated (Jimenez, n.d.). Even minor falls at home can spark chronic discomfort.
Dr. Alexander Jimenez, a chiropractor and nurse practitioner with over 30 years of experience, sees these patterns daily. “Our dual-scope diagnostics, combining chiropractic and nursing insights, uncover how trauma or overuse triggers pain cycles,” he shares on his clinic’s site (Jimenez, n.d.). Using advanced neuromusculoskeletal imaging, his team pinpoints root causes, from workplace injuries to MVA trauma. Ignoring early signs, such as stiffness or fatigue, can lead to reduced mobility, increased stress, and sleep disturbances. El Paso Back Clinic’s integrative approach breaks this cycle, restoring health naturally.
Everyday Injuries: From Crashes to Chronic Strains
Injuries vary but share a common impact: they disrupt your life. MVAs cause neck and back pain, limiting movement. Work-related strains, like those from lifting or repetitive tasks, create nagging discomfort. Sports injuries, such as twisted ankles or knees, sideline active El Pasoans. Personal falls at home can lead to shoulder or hip pain, while untreated stress may cause chronic conditions like joint stiffness.
Dr. Jimenez’s clinic tackles these with precision. “We connect injury origins—crashes, work tasks, or sports—to customized treatments,” he explains. MVAs receive urgent care with legal documentation for claims. Work injuries get rehab to restore function, and sports or personal injuries benefit from targeted plans to prevent recurrence. Without care, these issues worsen, lowering the quality of life. El Paso Back Clinic’s chiropractic and integrative methods pave the way to recovery.
Realigning for Relief: The Power of Spinal Adjustments
Spinal adjustments are the foundation of chiropractic care at El Paso Back Clinic. These precise, hands-on techniques realign vertebrae, easing nerve pressure and restoring balance to the body. Injuries from accidents or overuse misalign the spine, causing pain and impaired movement. Adjustments can boost blood flow, reduce inflammation, and alleviate pain by up to 25% in as little as a few weeks (Trident Health Chiropractic, n.d.).
For MVA patients, adjustments relieve neck stiffness, restoring mobility. Work injury patients regain strength for daily tasks. Dr. Jimenez’s approach is unique: “We use imaging to guide adjustments, targeting issues from trauma or strains,” he says. Legal reports ensure MVA patients have clear records for claims. From athletes to office workers, adjustments help El Pasoans move freely and heal quickly.
Healing Muscles: Soft Tissue Therapy for Recovery
Injuries tighten muscles, creating knots that misalign joints and prolong pain. Soft tissue therapy, like massage or myofascial release, targets these areas, breaking up scar tissue and boosting circulation. This delivers nutrients to damaged tissues, speeding recovery. A single session can significantly reduce healing time, getting you back to work or play faster (Yoder Chiropractic Center, n.d.).
Picture a construction worker with shoulder pain from heavy lifting. Therapy loosens tightness, improving arm range. MVA patients find relief from neck strain. Dr. Jimenez’s team pairs therapy with imaging for precision. “We treat trauma from accidents or sports non-surgically,” he notes. Legal documentation tracks progress for claims, prioritizing natural healing. Patients feel relaxed, move more easily, and recover more quickly.
Injuries disrupt nerve-muscle communication, resulting in shaky balance or impaired movements. Neuromuscular re-education uses exercises like balance drills or resistance training to retrain these pathways, reducing fall risks and boosting confidence. A soccer player with a sprained ankle, for example, regains stability, thereby lowering the odds of re-injury (Integrative Chiropractic, n.d.).
Dr. Jimenez’s clinic excels here. “We link nerve issues to injury histories, guiding re-education for MVA, work, or sports recovery,” he says. A retail worker with back pain learns core-strengthening moves; an MVA patient rebuilds neck control. Legal reports detail progress for claims, ensuring comprehensive care. This sharpens coordination, making daily tasks and active pursuits feel natural again.
Faster Healing, Better Mobility: Recovery and Flexibility Gains
Chiropractic care at El Paso Back Clinic speeds healing by optimizing body systems. Adjustments and therapy reduce swelling, allowing tissues to mend faster—often in weeks, not months (Abundant Life Chiropractor, n.d.). Flexibility improves as tight muscles and joints stretch safely. A warehouse worker lifts without strain; an accident victim moves freely again.
Dr. Jimenez’s holistic plans amplify results. “Targeted exercises and adjustments build lasting mobility, preventing chronic issues,” he says. Nutrition tips, like anti-inflammatory foods, fuel healing. MVA and work cases get legal-grade documentation, aligning care with claims. El Pasoans recover quickly, staying active in our vibrant community.
Balance and coordination are key to preventing injuries and enhancing daily function. Re-education drills steady wobbly steps, helping MVA victims or athletes avoid falls. A delivery driver navigates uneven terrain easily post-care. Chiropractic also boosts stamina by freeing the spine for deeper breaths, improving oxygen flow and endurance (ASR Sports Medicine, n.d.).
Jimenez’s integrative approach shines: “Acupuncture and massage enhance flow, boosting stamina for work or sports.” Virtual coaching reinforces gains, and legal support ensures MVA patients have clear records. Patients work longer, play harder, and live stronger.
Whole-Person Healing: Nutrition, Stress, and Custom Plans
El Paso Back Clinic’s functional medicine approach goes beyond physical fixes. Nutrition advice—like omega-3s or antioxidant-rich fruits—fights inflammation and boosts energy. Stress management, such as mindfulness or breathing exercises, eases tension, aiding sleep and recovery. Personalized plans fit your injury, lifestyle, and goals.
Dr. Jimenez leads the way. “We uncover root causes—poor diet, stress—and craft plans with acupuncture or massage,” he says. MVA or work injuries get detailed reports for legal cases, prioritizing natural healing. Patients receive plans tailored to their El Paso lives, ensuring lasting wellness.
El Paso Back Clinic: Your Trusted Recovery Partner
At El Paso Back Clinic, Dr. Alexander Jimenez combines chiropractic and nursing expertise for exceptional care. Awarded from 2015 to 2024, his team treats MVAs, work strains, sports injuries, and personal falls with precision. “Our imaging and dual expertise catch hidden issues,” he says. A crash victim drives pain-free in weeks. A nurse lifts patients again. Legal documentation supports MVA and work cases, while virtual coaching and nutrition webinars empower long-term health.
Patients praise the results: “Dr. Jimenez restored my mobility and energy,” one shares. From veterans to families, his care transforms lives, helping El Pasoans thrive.
Preventing Future Pain: A Strategy for Lifelong Wellness
Prevention keeps you active. Regular chiropractic checkups spot misalignments early, cutting injury risks by 20% (Erie Chiro, n.d.). Holistic habits—such as balanced diets, stress relief, and smart exercise—build resilience. Dr. Jimenez’s team creates plans for workers, athletes, or retirees. “We flag risks like posture or stress early, ensuring lasting health,” he notes.
With care, education, and documentation, El Pasoans live pain-free, embracing our city’s vibrant spirit.
Feeling drained? Relying on caffeine or sugar-packed energy drinks may give you a quick lift—but they don’t fix the real problem. These quick fixes can raise blood pressure, worsen sleep, and even contribute to more serious long-term health issues. El Paso Back Clinic takes a different approach: one that uncovers root causes and restores vitality naturally. (elpasobackclinic.com)
Your Nervous System = Your Power Source
The nervous system controls every important bodily function, from heartbeat to digestion. Spinal misalignment—due to poor posture, injuries, or birth trauma—can block nerve signals, leading to fatigue, pain, and even organ dysfunction. Chiropractic care realigns the spine and restores this vital communication. (elpasobackclinic.com)
Fatigue Fix: Circulation, Alignment, and Sleep
Chronic stress and misalignment often lead to poor sleep, brain fog, weakness, and digestive complaints. At El Paso Back Clinic, chiropractic + functional medicine work together to:
Align the spine for better nerve function
Improve circulation and oxygen delivery
Support restful sleep and reduce stress-related fatigue
Your body is like a car—it runs poorly on bad fuel. Proper nutrition makes a huge difference. El Paso Back Clinic emphasizes the importance of macronutrients and micronutrients that support recovery and energy. A poor diet can hinder healing and prolong fatigue. (elpasobackclinic.com)
Acupuncture: Energy Boost from Ancient Wisdom
Tired and worn out? Acupuncture may help. Studies show that it can improve both physical and mental fatigue, resulting in a better overall quality of life, reduced pain, improved sleep, and even enhanced gut health. For athletes, acupuncture aided faster metabolic recovery than rest alone. (elpasobackclinic.com)
Supplements That Help You Recover Smarter
Certain supplements speed recovery:
Protein & BCAAs rebuild muscle and reduce soreness
Fatty acids (MCTs, Omega-3s) deliver energy and reduce inflammation
Creatine, Citrulline Malate, and Magnesium support energy, muscle recovery, and blood flow
These can significantly shorten recovery and reduce fatigue. (elpasobackclinic.com)
Move Right: Exercise with Purpose
Routine activities like walking, stretching, and posture-aware movement strengthen the body and increase stamina. These simple practices improve endurance and productivity—especially when paired with chiropractic adjustments. (elpasobackclinic.com)
Dr. Jimenez’s Dual-Licensed Advantage
At El Paso Back Clinic, Dr. Alex Jimenez blends chiropractic precision with the diagnostic power of a board-certified nurse practitioner. This means:
Expert spinal alignment and pain relief
Comprehensive health diagnostics
Personalized treatment plans that address symptoms and root causes
Functional Medicine + Chiropractic = Full Recovery
Your pain relief plan includes more than adjustments. At El Paso Back Clinic, a functional medicine lens helps identify imbalances—such as inflammation or nutrient deficiencies—that interfere with recovery. Chiropractic adjustments, supplements, and targeted therapies then help the body heal and stay energized. (elpasobackclinic.com)
Beating Fatigue at El Paso Back Clinic
Here’s how the clinic restores vitality through an integrative approach:
Nervous system blockages → Bio-Chiropractic alignment → Improved nerve signaling
Poor circulation and sleep issues → Spinal realignment + functional support → Enhanced energy and mood
Stress and poor posture → Chiropractic adjustments + lifestyle coaching → Better rest and mental clarity
Inflammation → Nutrition plans, supplements, and acupuncture → Reduced fatigue and pain
Weak muscles → Movement therapy + targeted nutrients → Greater strength and endurance
Complex health problems → Functional medicine testing + chiropractic → Root-cause healing
Closing Thoughts
El Paso Back Clinic offers more than just a quick fix for fatigue. By combining nervous system alignment, functional nutrition, therapeutic movement, and Dr. Jimenez’s dual-licensed expertise, the clinic helps patients reclaim energy, vitality, and better health for the long haul.
Discover effective chiropractic care options for sports injuries & sciatica to support your healing journey.
Sciatica Pain and Sports Injuries: A Comprehensive Guide to Chiropractic Care and Recovery
Introduction: The Sciatica Struggle and the Sports Connection
Imagine this: you’re sprinting down the soccer field, weaving through defenders like a pro, when suddenly a sharp, electric jolt shoots down your leg. Or maybe you’re just sitting at your desk, minding your own business, and a nagging pain in your lower back decides to throw a party that radiates all the way to your toes. Welcome to the world of sciatica—a condition that can make even the toughest athletes feel like they’ve been tackled by an invisible linebacker. Sciatica isn’t just a pain in the… well, you know where. It’s a complex musculoskeletal issue that can stem from various causes, including sports injuries, and it affects millions of people worldwide.
At El Paso Back Clinic, led by the esteemed Dr. Alexander Jimenez, DC, APRN, FNP-BC, patients find hope through advanced chiropractic care and integrative treatments tailored to alleviate sciatica pain and restore mobility. Whether you’re an athlete sidelined by a sports injury or someone dealing with the aftermath of a car accident, understanding sciatica and its connection to the musculoskeletal system is key to recovery. In this comprehensive guide, we’ll dive into the causes of sciatica, explore how sports injuries contribute to it, and highlight how chiropractic care, combined with non-surgical treatments, can help you get back on your feet. Plus, we’ll sprinkle in a bit of humor to keep things light—because nobody likes a blog post that’s as stiff as a bad back!
What Is Sciatica? Understanding the Basics
Sciatica isn’t just one thing—it’s a symptom of an underlying issue affecting the sciatic nerve, the longest nerve in your body, which runs from your lower back through your hips, buttocks, and down each leg. When this nerve gets irritated or compressed, it can cause pain, numbness, tingling, or weakness that radiates along its path. Think of it like a garden hose with a kink: the water (or in this case, nerve signals) can’t flow properly, and the result is discomfort that can range from mildly annoying to downright debilitating.
Common Symptoms of Sciatica
Pain: A sharp, burning, or aching sensation that starts in the lower back or buttocks and travels down one leg.
Numbness or Tingling: That “pins and needles” feeling, like your leg fell asleep but decided to stay that way.
Weakness: Difficulty moving your leg or foot, making you feel like you’re auditioning for a role as a wobbly penguin.
One-Sided Symptoms: Sciatica typically affects only one side of the body, though it can occasionally be bilateral (both sides).
Causes of Sciatica
Sciatica can be triggered by various conditions, many of which involve the musculoskeletal system. Some of the most common culprits include:
Lumbar Disc Herniation: When the soft inner material of a spinal disc bulges or ruptures, it can press on the sciatic nerve roots (Wang et al., 2022).
Piriformis Syndrome: The piriformis muscle in the buttocks can irritate the sciatic nerve if it becomes tight or inflamed (Hicks et al., 2021).
Spinal Stenosis: Narrowing of the spinal canal can compress nerve roots, leading to sciatica symptoms.
Degenerative Arthritis: Wear and tear on the spine can cause bone spurs or disc degeneration, irritating the nerve.
Trauma or Injury: Sports injuries, car accidents, or even a bad fall can damage the spine or surrounding tissues, contributing to sciatica (El Paso Back Clinic, n.d.).
Hicks, B. L., Lam, J. C., & Varacallo, M. (2021). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 20(2), 97–102. https://pubmed.ncbi.nlm.nih.gov/33560090/
Wang, Y., Chen, J., & Chen, L. (2022). Association between chiropractic spinal manipulation and lumbar discectomy in adults with lumbar disc herniation and radiculopathy: Retrospective cohort study using United States’ data. BMJ Open, 12(12), e068262. https://pubmed.ncbi.nlm.nih.gov/36523295/
The Musculoskeletal System and Sciatica: A Complex Relationship
The musculoskeletal system—your bones, muscles, ligaments, and tendons—works together like a well-oiled machine to keep you moving. But when one part of this system gets out of whack, it can throw everything off balance, including the sciatic nerve. Let’s break down how the musculoskeletal system plays a role in sciatica and why sports injuries can be a major contributing factor.
How the Musculoskeletal System Contributes to Sciatica
The sciatic nerve is surrounded by muscles, bones, and connective tissues, all of which can influence its function. Here’s how:
Spinal Misalignment: When vertebrae in the lumbar spine are misaligned, they can compress nerve roots, leading to sciatica. This is often seen in conditions like spondylolisthesis, where one vertebra slips over another.
Muscle Imbalances: Tight or weak muscles, such as the piriformis or hamstrings, can put pressure on the sciatic nerve or alter spinal alignment.
Joint Dysfunction: Stiff or hypermobile joints in the spine or pelvis can disrupt normal biomechanics, irritating the nerve.
Inflammation: Injuries or overuse can cause inflammation in surrounding tissues, which can compress or irritate the sciatic nerve (Jensen et al., 2023).
Sports Injuries and Sciatica: The Connection
Athletes, whether weekend warriors or seasoned pros, are no strangers to musculoskeletal injuries. Sports like football, soccer, running, or even yoga can put significant stress on the body, leading to injuries that may trigger or exacerbate sciatica. Here’s how sports injuries can contribute:
Direct Trauma: A hard tackle in football or a fall during a basketball game can cause pelvic fractures or spinal injuries, which may compress the sciatic nerve (El Paso Back Clinic, n.d.).
Overuse Injuries: Repetitive motions, like running or cycling, can lead to muscle tightness or inflammation, such as piriformis syndrome, which irritates the sciatic nerve (Hicks et al., 2021).
Poor Biomechanics: Improper form during weightlifting or running can strain the spine or pelvis, leading to disc herniation or misalignment.
Pelvic Injuries: A broken pelvis, as discussed in El Paso Back Clinic’s article, can directly affect the sciatic nerve due to its proximity to the nerve’s path (El Paso Back Clinic, n.d.).
For example, imagine a runner who pushes through a tight hamstring without stretching properly. Over time, this tightness can pull on the pelvis, misalign the spine, and irritate the sciatic nerve. Or picture a soccer player who takes a hard fall, bruising their lower back and causing inflammation that pinches the nerve. These scenarios highlight how sports injuries can set the stage for sciatica.
Hicks, B. L., Lam, J. C., & Varacallo, M. (2021). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 20(2), 97–102. https://pubmed.ncbi.nlm.nih.gov/33560090/
Jensen, R. K., Kongsted, A., Kjaer, P., & Koes, B. (2023). Surgical versus non-surgical treatment for sciatica: Systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://pubmed.ncbi.nlm.nih.gov/37019468/
Sports Injury Rehabilitation- Video
Risk Factors for Sciatica: Why Athletes Are at Risk
Sciatica doesn’t discriminate—it can affect anyone, from desk jockeys to elite athletes. However, certain factors increase the likelihood of developing sciatica, particularly in those who engage in sports. Let’s explore these risk factors and why athletes might be more susceptible.
Key Risk Factors
Obesity: Excess weight puts extra pressure on the spine, increasing the risk of disc herniation and sciatica (Cao et al., 2021).
Sedentary Lifestyle: Prolonged sitting or inactivity weakens core muscles, leading to poor spinal support and nerve compression.
Age: As we age, degenerative changes in the spine, like arthritis or disc wear, become more common, increasing sciatica risk.
Occupational Hazards: Jobs or activities involving heavy lifting, twisting, or prolonged sitting can strain the spine.
Sports Injuries: High-impact or repetitive sports activities can cause trauma or overuse injuries, leading to sciatica (El Paso Back Clinic, n.d.).
Poor Posture: Slouching or improper body mechanics during sports or daily activities can misalign the spine, irritating the sciatic nerve.
Why Athletes Are Vulnerable
Athletes often push their bodies to the limit, which can lead to musculoskeletal issues that trigger sciatica. For instance:
High-Impact Sports: Football, rugby, or gymnastics involve jarring movements that can stress the spine or pelvis.
Repetitive Motions: Runners or cyclists may develop muscle imbalances or overuse injuries that affect the sciatic nerve.
Inadequate Recovery: Skipping rest days or neglecting proper warm-ups and cool-downs can lead to chronic inflammation or injury.
Improper Equipment: Worn-out running shoes or an ill-fitting bike saddle can alter biomechanics, contributing to sciatica.
Think of an athlete’s body like a finely tuned race car: it performs beautifully until a single misaligned part causes the whole system to sputter. That’s where chiropractic care comes in to realign the wheels and get you back on the track.
References
Cao, H., Zhang, Z., & Lu, T. (2021). Causal associations of obesity with the intervertebral degeneration, low back pain, and sciatica: A two-sample Mendelian randomization study. Frontiers in Endocrinology, 12, 740746. https://pubmed.ncbi.nlm.nih.gov/34956081/
Chiropractic Care: A Non-Surgical Solution for Sciatica
Chiropractic care is like the superhero of non-surgical treatments for sciatica—it swoops in to save the day without the need for scalpels or long recovery times. At El Paso Back Clinic, Dr. Alexander Jimenez and his team use a variety of chiropractic techniques to address the root causes of sciatica, helping patients regain mobility and reduce pain.
How Chiropractic Care Helps
Chiropractic care focuses on restoring proper alignment and function to the musculoskeletal system, which can alleviate pressure on the sciatic nerve. Here’s how it works:
Spinal Adjustments: Gentle manipulations correct misalignments in the spine, reducing nerve compression and improving biomechanics (Wang et al., 2022).
Soft Tissue Therapy: Techniques like myofascial release or trigger point therapy relax tight muscles, such as the piriformis, that may be irritating the nerve (Hicks et al., 2021).
Joint Mobilization: Restoring mobility to stiff joints in the spine or pelvis can reduce strain on the sciatic nerve.
Postural Correction: Chiropractors assess and correct posture issues that contribute to sciatica, ensuring long-term relief.
Benefits of Chiropractic Care for Sciatica
Pain Reduction: By addressing the root cause, chiropractic care can significantly reduce sciatica pain without relying on medications.
Improved Mobility: Restoring joint and muscle function helps patients move more freely, whether they’re athletes or office workers.
Non-Invasive: Unlike surgery, chiropractic care avoids the risks and recovery time associated with invasive procedures (Jensen et al., 2023).
Holistic Approach: Chiropractors often combine adjustments with lifestyle advice, exercises, and nutrition to support overall health.
Dr. Jimenez’s approach at El Paso Back Clinic is particularly effective because it integrates advanced diagnostic tools, like imaging and biomechanical assessments, to pinpoint the exact cause of sciatica. This precision ensures that treatments are tailored to each patient’s unique needs, whether their sciatica stems from a sports injury, a car accident, or a broken pelvis.
References
Hicks, B. L., Lam, J. C., & Varacallo, M. (2021). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 20(2), 97–102. https://pubmed.ncbi.nlm.nih.gov/33560090/
Jensen, R. K., Kongsted, A., Kjaer, P., & Koes, B. (2023). Surgical versus non-surgical treatment for sciatica: Systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://pubmed.ncbi.nlm.nih.gov/37019468/
Wang, Y., Chen, J., & Chen, L. (2022). Association between chiropractic spinal manipulation and lumbar discectomy in adults with lumbar disc herniation and radiculopathy: Retrospective cohort study using United States’ data. BMJ Open, 12(12), e068262. https://pubmed.ncbi.nlm.nih.gov/36523295/
Integrative Non-Surgical Treatments for Sciatica
While chiropractic care is a cornerstone of sciatica treatment, combining it with other non-surgical therapies can enhance outcomes, especially for athletes recovering from sports injuries. Dr. Jimenez and his team at El Paso Back Clinic incorporate a variety of integrative approaches to address sciatica and its overlapping symptoms.
Complementary Therapies
Acupuncture: This ancient practice involves inserting thin needles into specific points to reduce pain and inflammation. Studies show acupuncture can be effective for sciatica, particularly when tailored to neuropathic pain mechanisms (Li et al., 2020; Zhang et al., 2019).
Massage Therapy: Therapeutic massage can relax tight muscles, improve circulation, and reduce inflammation, complementing chiropractic adjustments.
Nutritional Support: A diet rich in anti-inflammatory foods, like omega-3s and antioxidants, can support recovery by reducing systemic inflammation (El Paso Back Clinic, n.d.).
Durable Medical Equipment: Braces or supports can stabilize the spine or pelvis during recovery, especially after injuries like a broken pelvis.
Acupuncture for Sciatica: A Closer Look
Acupuncture deserves a special mention because of its growing evidence base. Research suggests that acupuncture can modulate pain pathways and reduce inflammation, making it a valuable tool for sciatica management. For example, a randomized controlled pilot study found that acupuncture provided significant pain relief for sciatica patients, with effects varying based on the “dose” of treatment (Zhang et al., 2019). By combining acupuncture with chiropractic care, patients can address both the structural and neurological components of sciatica.
The Role of Nutrition
Nutrition plays a critical role in musculoskeletal recovery. After a sports injury or accident, inflammation can exacerbate sciatica symptoms. Dr. Jimenez emphasizes a diet that includes:
Anti-Inflammatory Foods: Fish, nuts, leafy greens, and berries to reduce inflammation.
Hydration: Proper fluid intake to support tissue repair and disc health.
Supplements: Omega-3 fatty acids or turmeric may help manage inflammation, though patients should consult a professional before starting supplements.
By integrating these therapies, El Paso Back Clinic creates a comprehensive treatment plan that addresses the multifaceted nature of sciatica, helping patients recover faster and more effectively.
Li, Q., Liu, R., & Zhao, J. (2020). The management of sciatica by acupuncture: An expert consensus using the improved Delphi survey. Evidence-Based Complementary and Alternative Medicine, 2020, 8565987. https://pubmed.ncbi.nlm.nih.gov/32595769/
Zhang, W., Liu, Y., & Yu, L. (2019). Therapeutic efficacy and the impact of the “dose” effect of acupuncture to treat sciatica: A randomized controlled pilot study. Journal of Pain Research, 12, 351–360. https://pubmed.ncbi.nlm.nih.gov/30666157/
Dr. Alexander Jimenez: A Leader in Personal Injury Care in El Paso
In El Paso, Dr. Alexander Jimenez stands out as a distinguished practitioner for victims of personal injuries, including those with sciatica caused by sports injuries or motor vehicle accidents. With his credentials as a Doctor of Chiropractic (DC), Advanced Practice Registered Nurse (APRN), and Family Nurse Practitioner-Board Certified (FNP-BC), Dr. Jimenez brings a unique blend of expertise to patient care. His practice at El Paso Back Clinic is renowned for its integrative approach, combining advanced diagnostics with holistic treatments.
Dr. Jimenez’s Approach to Personal Injury Cases
Personal injury cases, such as those involving car accidents or sports injuries, often require meticulous documentation and medical expertise to ensure patients receive proper care and legal support. Dr. Jimenez excels in this area by:
Advanced Imaging: Using X-rays, MRIs, or CT scans to identify structural issues like disc herniation or pelvic fractures that may cause sciatica (El Paso Back Clinic, n.d.).
Diagnostic Evaluations: Conducting thorough physical exams and biomechanical assessments to pinpoint the root cause of pain.
Dual-Scope Procedures: Combining chiropractic adjustments with medical interventions, such as injections or referrals to specialists, when needed.
Legal Liaison: Providing detailed medical reports and collaborating with legal teams to document injuries accurately, ensuring patients receive fair compensation.
Dr. Jimenez’s ability to bridge medical and legal needs makes him a trusted advocate for personal injury victims in El Paso. His work ensures that patients not only recover physically but also have the documentation needed to navigate insurance claims or legal proceedings.
Small Changes, Big Impact: Lifestyle Tips for Sciatica Prevention
Preventing sciatica or managing its symptoms doesn’t always require major interventions. Dr. Jimenez emphasizes that small, intentional changes in daily routines can make a significant difference. Here are some practical tips, infused with a touch of humor to keep you smiling:
Stay Active, But Smart: Regular exercise strengthens core muscles, but don’t go full Hulk mode without warming up. Gentle stretches before and after workouts can prevent muscle tightness.
Mind Your Posture: Slouching is the sciatic nerve’s archenemy. Sit up straight, like you’re trying to impress your high school crush at a reunion.
Ergonomic Workspace: Adjust your chair and desk to support your spine. Think of your office chair as a throne, not a torture device.
Stretch Like a Cat: Incorporate daily stretches for your hamstrings, piriformis, and lower back. Channel your inner feline and make stretching a ritual.
Stay Hydrated: Your spinal discs love water like a plant loves sunlight. Drink up to keep them plump and healthy.
Proper Footwear: Athletes, ditch those worn-out sneakers. Good shoes are like loyal friends—they support you through every step.
By making these small tweaks, you can reduce the risk of sciatica and support your musculoskeletal health, whether you’re hitting the gym or just navigating daily life.
The Role of Advanced Diagnostics in Sciatica Treatment
One of Dr. Jimenez’s strengths is his use of advanced diagnostics to create personalized treatment plans. Sciatica can have multiple causes, and pinpointing the exact source is crucial for effective treatment. At El Paso Back Clinic, patients benefit from:
Imaging Studies: X-rays, MRIs, or CT scans to visualize disc herniation, spinal stenosis, or pelvic injuries.
Electromyography (EMG): Tests to assess nerve function and identify compression sites.
Biomechanical Assessments: Evaluating posture, gait, and joint mobility to identify underlying dysfunctions.
These tools allow Dr. Jimenez to develop targeted interventions, whether it’s chiropractic adjustments, acupuncture, or physical therapy, ensuring that patients receive the most effective care for their specific condition.
To bring this all together, let’s consider a hypothetical case study inspired by real-world scenarios at El Paso Back Clinic. Meet Sarah, a 30-year-old avid runner who developed sciatica after a minor fall during a trail race. The impact caused a pelvic misalignment, which irritated her sciatic nerve, leading to burning pain down her left leg. Initially, Sarah thought it was just a pulled muscle, but the pain persisted, affecting her ability to run or even sit comfortably.
Sarah visited El Paso Back Clinic, where Dr. Jimenez conducted a thorough evaluation. An X-ray revealed a subtle pelvic tilt, and a physical exam confirmed piriformis tightness. Dr. Jimenez developed a treatment plan that included:
Chiropractic Adjustments: To correct pelvic and spinal alignment.
Acupuncture: To reduce inflammation and modulate pain signals.
Physical Therapy: To strengthen core muscles and improve running form.
Nutritional Counseling: To support tissue repair with an anti-inflammatory diet.
Within weeks, Sarah’s pain decreased significantly, and she was back to running with proper form and better shoes. Her case highlights how sports injuries can trigger sciatica and how an integrative approach can lead to lasting recovery.
Sciatica can be a challenging condition, but with the right care, recovery is within reach. At El Paso Back Clinic, Dr. Alexander Jimenez and his team offer a beacon of hope for those struggling with sciatica, whether it’s caused by sports injuries, car accidents, or other musculoskeletal issues. By combining chiropractic care, acupuncture, physical therapy, and nutritional support, patients can address the root causes of their pain and regain their quality of life. Dr. Jimenez’s expertise in personal injury cases also ensures that patients receive the medical and legal support they need to navigate complex situations.
Disclaimer: This blog post is intended for informational purposes only and should not be considered medical advice. Always consult a qualified healthcare professional, such as Dr. Alexander Jimenez at El Paso Back Clinic, for a proper diagnosis and treatment plan tailored to your specific condition. Sciatica and musculoskeletal injuries require individualized care, and self-treatment without professional guidance may worsen symptoms.
References
Cao, H., Zhang, Z., & Lu, T. (2021). Causal associations of obesity with the intervertebral degeneration, low back pain, and sciatica: A two-sample Mendelian randomization study. Frontiers in Endocrinology, 12, 740746. https://pubmed.ncbi.nlm.nih.gov/34956081/
Hicks, B. L., Lam, J. C., & Varacallo, M. (2021). Piriformis syndrome: A cause of nondiscogenic sciatica. Current Sports Medicine Reports, 20(2), 97–102. https://pubmed.ncbi.nlm.nih.gov/33560090/
Jensen, R. K., Kongsted, A., Kjaer, P., & Koes, B. (2023). Surgical versus non-surgical treatment for sciatica: Systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://pubmed.ncbi.nlm.nih.gov/37019468/
Li, Q., Liu, R., & Zhao, J. (2020). The management of sciatica by acupuncture: An expert consensus using the improved Delphi survey. Evidence-Based Complementary and Alternative Medicine, 2020, 8565987. https://pubmed.ncbi.nlm.nih.gov/32595769/
Vickers, A. J., & Vertosick, E. A. (2021). Extra-spinal sciatica and sciatica mimics: A scoping review. Pain Medicine, 22(1), 70–81. https://pubmed.ncbi.nlm.nih.gov/32951055/
Wang, Y., Chen, J., & Chen, L. (2022). Association between chiropractic spinal manipulation and lumbar discectomy in adults with lumbar disc herniation and radiculopathy: Retrospective cohort study using United States’ data. BMJ Open, 12(12), e068262. https://pubmed.ncbi.nlm.nih.gov/36523295/
Zhang, W., Liu, Y., & Yu, L. (2019). Therapeutic efficacy and the impact of the “dose” effect of acupuncture to treat sciatica: A randomized controlled pilot study. Journal of Pain Research, 12, 351–360. https://pubmed.ncbi.nlm.nih.gov/30666157/
El Paso Back Clinic®: Your Path to Wellness and Recovery
At El Paso Back Clinic®, we believe in empowering our patients to live pain-free, active lives through comprehensive chiropractic care and integrative medicine. Led by Dr. Alex Jimenez, DC, APRN, FNP-BC, our clinic in El Paso, TX, specializes in treating a wide range of injuries, from motor vehicle accidents (MVAs) to sports mishaps, with a focus on restoring mobility, flexibility, and overall wellness. By addressing posture, spinal health, and musculoskeletal issues, we help patients recover from injuries, manage pain, and prevent future complications. This article explores how our holistic approach, combining chiropractic care, nutrition, and advanced therapies, transforms lives at El Paso Back Clinic®.
The Role of Posture in Wellness and Recovery
Good posture is the foundation of a healthy body, especially when recovering from injuries or managing chronic pain. Poor posture, often caused by accidents or prolonged sitting, can lead to muscle strain, joint stress, and increased discomfort. At El Paso Back Clinic®, we prioritize correcting posture to improve spinal alignment, which enhances mobility and reduces the risk of further injury. Proper posture allows the body to distribute weight evenly, supporting natural healing and optimal function (Optimal Spine Chiro, 2023).
Our chiropractic adjustments focus on restoring spinal alignment, relieving pressure on nerves, and improving overall body mechanics. This is particularly important for patients recovering from MVAs or sports injuries, where misalignments can worsen pain or delay recovery. By addressing posture, we help patients move better, feel better, and stay active (Zaker Chiropractic, 2023).
Dr. Alex Jimenez: Leading Wellness Care in El Paso
Dr. Alex Jimenez, a chiropractor and nurse practitioner, brings a unique combination of medical and chiropractic expertise to El Paso Back Clinic®. With years of experience treating severe pain, sciatica, whiplash, and sports injuries, Dr. Jimenez uses advanced diagnostics and integrative therapies to create personalized treatment plans. His dual training allows him to address both the structural and medical aspects of injuries, ensuring comprehensive care (Jimenez, 2025).
Advanced Diagnostics for Precise Treatment
At El Paso Back Clinic®, we use state-of-the-art diagnostic tools, such as X-rays and MRIs, to identify the root causes of pain and injury. Dr. Jimenez employs techniques like motion palpation and static palpation to assess spinal and joint function, ensuring treatments are tailored to each patient’s needs. This approach is critical for conditions like whiplash or spinal misalignments caused by MVAs, where precise diagnosis leads to faster recovery (El Paso Back Clinic, 2023).
Supporting Legal and Medical Needs
In personal injury cases, such as those from car accidents, Dr. Jimenez provides detailed medical reports to support insurance claims or legal proceedings. His ability to navigate both medical and legal aspects ensures patients can focus on healing while their cases are handled effectively. This expertise is especially valuable for injuries like back pain or joint dislocations, where documentation is key (Personal Injury Doctor, 2017).
El Paso Back Clinic® specializes in treating musculoskeletal injuries caused by MVAs, workplace accidents, sports, and daily activities. Our non-invasive, drug-free approach focuses on restoring function and relieving pain through chiropractic care and integrative therapies.
Whiplash and Neck Pain
Whiplash, common in car accidents, results from sudden neck jolts that strain muscles and misalign the spine. Our clinic uses gentle spinal adjustments, trigger point therapy, and corrective exercises to reduce inflammation and restore mobility. These treatments help patients recover quickly and avoid chronic neck pain (El Paso Back Clinic, 2023).
Back Pain and Spinal Injuries
Back injuries, such as herniated discs or spinal misalignments, are frequent after MVAs or heavy lifting. Dr. Jimenez employs spinal manipulation and decompression techniques to alleviate pain and promote healing. We also incorporate mobility exercises to strengthen supporting muscles, ensuring long-term spinal health (El Paso Back Clinic, 2023).
Sports and Joint Injuries
Athletes trust El Paso Back Clinic® for recovery from injuries like ACL tears, sprains, or joint dislocations. Our integrative approach combines chiropractic adjustments with physical therapy and nutritional guidance to restore strength and enhance performance. By improving posture and alignment, we help athletes return to their sport stronger than before (Square One Health, 2023).
Our clinic’s strength lies in combining chiropractic care with integrative therapies to address the whole person, not just the injury. This holistic approach promotes natural healing, reduces pain, and prevents long-term complications.
Targeted Exercise and Physical Therapy
Customized exercise programs are central to our treatment plans. These exercises strengthen muscles, improve flexibility, and support spinal health, helping patients recover from injuries like fractures or sprains. For example, after an 18-wheeler accident, we design specific stretches to restore mobility without aggravating spinal trauma (El Paso Back Clinic, 2023).
Massage Therapy and Acupuncture
Massage therapy relieves muscle tension and boosts circulation, aiding recovery from soft tissue injuries. Acupuncture reduces inflammation and stimulates natural pain relief, complementing chiropractic care. These therapies work together to provide comprehensive pain relief and support healing (Mountain Movement Center, 2023).
Nutritional Support for Healing
Nutrition is a key component of recovery at El Paso Back Clinic®. Dr. Jimenez provides dietary recommendations, such as anti-inflammatory foods and supplements, to support tissue repair and reduce pain. This approach strengthens the body’s ability to heal after MVAs or sports injuries, promoting long-term wellness (El Paso Back Clinic, 2023).
Preventing Long-Term Complications with Integrative Care
Untreated injuries can lead to chronic pain, reduced mobility, or conditions like degenerative arthritis. At El Paso Back Clinic®, our integrative approach prevents these issues by addressing the root causes of pain and injury. Regular chiropractic adjustments maintain spinal alignment, while therapies like acupuncture and exercise reduce inflammation and strengthen the body. This comprehensive care ensures patients recover fully and maintain optimal health (Current Physical Therapy, 2025).
For athletes, this means returning to their sport with improved performance and less risk of re-injury. For accident victims, it means reclaiming their daily lives without pain. Our focus on wellness empowers patients to live active, healthy lives long after their treatment ends (Tigard Chiropractic Auto Injury, 2023).
El Paso Back Clinic®, under the leadership of Dr. Alex Jimenez, is dedicated to helping patients achieve wellness through chiropractic care and integrative medicine. By focusing on posture, spinal health, and holistic therapies, we treat injuries from MVAs, sports, and daily life, while preventing long-term complications. Whether you’re recovering from whiplash, back pain, or a sports injury, our personalized approach ensures you return to a pain-free, active life. Visit El Paso Back Clinic® to start your journey to optimal health today.
Nutrition and Integrative Care for Mobility and Injury Recovery at El Paso Back Clinic®
In El Paso, TX, maintaining mobility and flexibility is essential for an active lifestyle, whether you’re recovering from an injury or managing chronic pain. At El Paso Back Clinic®, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, a well-balanced diet and targeted supplementation are combined with chiropractic care to support joint health, reduce inflammation, and enhance muscle and bone function. Nutrients like omega-3 fatty acids, collagen, and vitamins D and K, alongside supplements such as glucosamine, chondroitin, and turmeric, are key to improving movement and promoting healing. Dr. Jimenez’s integrative approach, incorporating massage therapy, acupuncture, and functional medicine, helps patients recover from motor vehicle accidents, work injuries, sports injuries, and chronic conditions, ensuring natural healing and long-term wellness.
Nutrition for Joint Health and Recovery
A nutrient-dense diet is critical for supporting joint health and aiding recovery, especially for El Pasoans dealing with injuries from accidents or physical strain. Omega-3 fatty acids, found in foods like salmon, chia seeds, and walnuts, reduce inflammation, helping to alleviate joint pain and improve flexibility (StretchIt App, 2023). This is particularly important for those recovering from motor vehicle accidents or sports injuries, where inflammation can prolong discomfort.
Collagen, a primary component of cartilage and tendons, strengthens joints and supports repair. Consuming collagen-rich foods like bone broth or taking supplements can aid recovery from injuries common in El Paso’s active community (Nature’s Best, 2023). Vitamins D and K are vital for bone health, providing stability to joints. Vitamin D, sourced from fortified dairy or El Paso’s sunny environment, enhances calcium absorption, while vitamin K, found in leafy greens like spinach, supports bone mineralization (BetterYou, 2023).
Protein is essential for muscle repair, acting as a protective layer for joints during movement. Foods like eggs, lean meats, and lentils provide amino acids to rebuild muscle tissue, crucial for those healing from work or sports injuries (Nature’s Best, 2023). Hydration is also key, as water lubricates joint cartilage, reducing wear and supporting smooth motion (Spinal Rehab and Chiro Center, 2023).
Supplements can amplify the benefits of a healthy diet, particularly for those recovering from injuries or managing chronic pain. Glucosamine and chondroitin support cartilage health, with glucosamine aiding cartilage production and chondroitin helping joints retain water, improving mobility (VoltaGel, 2023). At El Paso Back Clinic®, Dr. Jimenez often recommends these for patients with joint wear from auto accidents or repetitive work tasks.
Turmeric, with its active compound curcumin, is a potent anti-inflammatory supplement that reduces joint pain, aiding recovery for El Paso’s active residents (ZoharyogaFlex, 2023). Magnesium supports muscle relaxation and flexibility, helping prevent stiffness after injuries (BetterYou, 2023). Collagen supplements strengthen connective tissues, speeding up recovery from sprains or strains, common in sports or workplace injuries (NutritionX, 2023).
Patients are advised to consult Dr. Jimenez or a healthcare professional before starting supplements, especially if they have existing conditions or take medications (MVSU, 2023).
At El Paso Back Clinic®, Dr. Alexander Jimenez, a chiropractor and nurse practitioner, specializes in treating injuries from motor vehicle accidents, work incidents, sports mishaps, and chronic conditions like arthritis or back pain. His dual-scope approach combines chiropractic adjustments with medical evaluations, using advanced diagnostics like X-rays and MRIs to identify issues such as herniated discs or nerve compression (Jimenez, 2023a). This ensures precise, personalized treatment plans for conditions causing pain, numbness, or reduced mobility.
Dr. Jimenez’s ability to provide detailed medical and legal documentation is a key asset for personal injury cases, supporting insurance claims or legal proceedings in El Paso’s vibrant community (Jimenez, 2023b). His focus on addressing the root causes of pain, such as spinal misalignments or soft tissue damage, promotes lasting recovery and improved quality of life.
Integrative Therapies for Comprehensive Rehabilitation
El Paso Back Clinic® offers a holistic approach to recovery, combining chiropractic care, massage therapy, acupuncture, and nutritional guidance. Chiropractic adjustments correct spinal and joint misalignments, relieving pressure and restoring mobility for conditions like whiplash or lower back pain (Jimenez, 2023a). Massage therapy reduces muscle tension and improves blood flow, aiding recovery from soft tissue injuries common in auto accidents or sports (Jimenez, 2023c).
Acupuncture targets pain and inflammation with precise needle placements, making it effective for chronic pain or post-injury recovery (Jimenez, 2023d). Nutritional guidance, including anti-inflammatory diets and supplements like omega-3s or collagen, supports joint and muscle repair, addressing underlying causes and preventing complications like chronic pain or joint degeneration (El Paso Back Clinic, 2023).
This integrative approach promotes natural healing, helping El Paso patients recover from a wide range of injuries while minimizing long-term issues.
At El Paso Back Clinic®, Dr. Jimenez and his team provide personalized care plans that integrate nutrition, chiropractic care, and integrative therapies to address pain and promote wellness. Whether recovering from a car accident, work injury, or sports trauma, the clinic’s holistic approach ensures optimal outcomes. Nutritional strategies, such as incorporating omega-3-rich foods or collagen supplements, support joint health and recovery (El Paso Back Clinic, 2023).
The clinic’s commitment to El Paso’s community is evident in its mission to help patients live pain-free, active lives. Always consult a healthcare professional before making dietary changes or starting supplements to ensure they align with your specific health needs (MVSU, 2023).
At El Paso Back Clinic®, Dr. Alexander Jimenez combines nutrition, supplementation, and integrative therapies to support mobility, flexibility, and injury recovery. A diet rich in omega-3s, collagen, and vitamins D and K, paired with supplements like glucosamine and turmeric, enhances joint health and reduces inflammation. Dr. Jimenez’s expertise in chiropractic care, massage therapy, acupuncture, and functional nutrition provides a comprehensive approach to healing injuries from auto accidents, work, or sports, while preventing long-term complications. The clinic helps El Pasoans live vibrant, pain-free lives. Consult a healthcare professional before starting new dietary or supplement regimens to ensure they suit your needs.
Get insights into chiropractic care and see how it can facilitate recovery and help you regain your strength from ACL tears.
Introduction
Imagine twisting your knee during a soccer game, hearing a dreaded “pop,” and suddenly finding yourself unable to walk without pain. This is the reality for many who suffer an anterior cruciate ligament (ACL) injury, a common yet debilitating condition that can derail daily routines and athletic pursuits. With an estimated 150,000 ACL injuries annually in the United States, resulting in approximately $500 million in healthcare expenses, the impact is substantial (The Joint Chiropractic, 2017). While surgery and physical therapy are standard treatments, chiropractic care offers a complementary, non-invasive approach that may enhance recovery and restore function.
This comprehensive guide explores the clinical rationale for using chiropractic care to manage ACL injuries, drawing on evidence and insights from Dr. Alexander Jimenez, a distinguished chiropractor and family practice nurse practitioner in El Paso, Texas. We’ll explore how ACL injuries impact daily life, the role of chiropractic interventions, and Dr. Jimenez’s distinctive contributions, particularly in personal injury cases. With a touch of dark humor to lighten the mood—because who hasn’t felt like their knee is staging a mutiny?—this post aims to inform and engage readers at a high school reading level. However, the conclusion will adopt a serious tone, emphasizing the importance of professional care and including a disclaimer for clarity.
Understanding ACL Injuries
What Is the ACL?
The anterior cruciate ligament (ACL) is one of four major ligaments in the knee, connecting the femur (thigh bone) to the tibia (shin bone). It prevents excessive forward movement of the tibia and provides rotational stability, which is crucial for activities such as running, jumping, or pivoting (Vale Health Clinic, 2021). The knee joint also includes the patella (kneecap), the fibula, tendons, and cartilage (menisci), all of which work together to ensure smooth motion and stability.
Causes and Risk Factors
ACL injuries often result from sudden, high-stress movements, such as:
Sudden Stops or Changes in Direction: Common in sports like soccer, basketball, and skiing.
Jumping and Landing Incorrectly: A misstep can overstress the ligament.
Direct Trauma: Such as a collision in contact sports or accidents like car crashes.
Women are 7-8 times more likely to suffer ACL injuries due to anatomical differences, hormonal influences, and neuromuscular control variations (Vale Health Clinic, 2021). Everyday activities, like slipping on ice or tripping, can also cause ACL tears, making them relevant beyond athletics.
Symptoms and Diagnosis
An ACL tear typically presents with:
A popping sensation at the time of injury.
Severe pain and swelling within hours.
Instability or a feeling that the knee “gives out.”
Difficulty walking or bearing weight.
Diagnosis involves physical exams, such as the Lachman’s Test, Pivot Shift Test, and Anterior Drawer Test, which assess knee stability (Vale Health Clinic, 2021). Imaging, like X-rays to rule out fractures or an MRI to confirm ligament damage, is often used. Arthroscopy, a minimally invasive procedure, may provide a detailed view of the injury.
Impact on Daily Life
An ACL injury can turn simple tasks into Herculean challenges. Walking becomes a wobbly adventure, climbing stairs feels like scaling Everest, and sports may be sidelined indefinitely. For non-athletes, routine activities like carrying groceries or playing with kids become painful obstacles. Emotionally, the loss of mobility can lead to frustration or depression, especially for active individuals. Untreated, ACL injuries may lead to chronic instability, bone friction, and osteoarthritis, underscoring the need for effective treatment (Tri State Clinic North Chiropractic, 2018).
For complete ACL tears, particularly in active individuals or athletes, surgical reconstruction is often recommended. This involves replacing the torn ligament with a graft, typically from the patient’s patellar tendon, hamstring, or a donor. Surgery aims to restore knee stability and function but carries risks like infection, graft failure, or anesthesia complications. Recovery typically spans 6 to 12 months, requiring extensive rehabilitation (Physiopedia, n.d.).
Physical Therapy
For both post-surgical and non-surgical cases, physical therapy is crucial. It focuses on:
Restoring Range of Motion: Gentle exercises to regain flexibility.
Strengthening Muscles: Targeting quadriceps, hamstrings, and calves to support the knee.
Improving Proprioception: Balance and coordination training to prevent re-injury.
Physical therapy is effective but can be time-intensive, and some patients experience persistent pain or incomplete recovery.
Limitations of Traditional Approaches
While effective, traditional treatments have challenges:
Surgical Risks: Complications can delay recovery or affect outcomes.
Long Recovery Time: It may take up to a year to return to full activity.
Persistent Symptoms: Some patients report ongoing pain or instability.
Cost and Accessibility: Surgery and prolonged therapy can be expensive and inaccessible for some.
These limitations highlight the potential role of complementary therapies, such as chiropractic care, in enhancing recovery and addressing residual issues.
The Role of Chiropractic Care in ACL Injury Recovery
Chiropractic Techniques for ACL Injuries
Chiropractic care offers non-invasive methods to support ACL injury recovery, either as a standalone treatment for partial tears or as a complement to surgery. Key techniques include:
Chiropractic manipulation involves adjustments to the knee and surrounding joints (e.g., hip, ankle) to restore alignment and mobility, thereby reducing stiffness and improving function (Vale Health Clinic, 2021).
Therapeutic Ultrasound: Uses sound waves to generate heat, stimulating blood flow and promoting tissue healing.
Soft Tissue Therapy: Techniques such as massage or Active Release Technique help relieve muscle tension and break down scar tissue, thereby enhancing circulation (Kaizo Health, 2023).
Cold Laser Therapy: Reduces inflammation and accelerates tissue repair by stimulating cellular activity.
Enhancing Nervous System Function: Chiropractic adjustments optimize nervous system communication, which controls healing processes (The Joint Chiropractic, 2017).
For post-surgical patients, chiropractic care can accelerate recovery by addressing scar tissue and restoring joint mechanics, as demonstrated in a case study where a patient regained full function after completing a 12-week multimodal chiropractic program (Solecki & Herbst, 2011).
Benefits of Chiropractic Care
Non-Invasive: Avoids surgical risks and drug side effects.
Cost-Effective: Often covered by insurance with shorter wait times (Vale Health Clinic, 2021).
Holistic Approach: Addresses the whole body, not just the knee.
Prevention Focus: Reduces the risk of re-injury through biomechanical corrections.
However, the effectiveness of chiropractic care depends on the severity of the injury. Severe tears typically require surgical intervention, and chiropractic care is most beneficial as a complementary or preventative approach.
A notable case involved a 25-year-old man who suffered a complete ACL rupture, medial meniscus tear, and lateral meniscus tear after a basketball injury. Following surgical reconstruction, he underwent a 12-week chiropractic rehabilitation program including Active Release Technique, Graston Technique, and Kinesio Taping. Outcomes included:
Pain Relief: Numeric Pain Scale score dropped to 0/10.
Functional Recovery: Full restoration of range of motion and muscle strength.
Return to Activity: Resumed sports without complications.
Long-Term Success: No pain reported at one-year follow-up (Solecki & Herbst, 2011).
This case demonstrates the potential of chiropractic care in post-surgical recovery, particularly when a multimodal approach is employed.
Supporting Research
Knee Injury Management: A study in the Journal of Manipulative and Physiological Therapeutics found that chiropractic manipulation and soft tissue therapy reduced pain and improved function in patients with knee injuries, including ACL tears (Haldeman et al., 2008).
Muscle Activation: Research on gluteal muscle activation during walking suggests that strengthening supporting muscles, a common chiropractic focus, can enhance pelvic and knee stability, aiding recovery (Bullock-Saxton et al., 1993).
Preventative Benefits: Chiropractic care that addresses muscular imbalances and movement patterns may reduce the risk of ACL injuries (MSK Centre, 2023).
While the evidence is promising, more large-scale studies are needed to confirm the efficacy of chiropractic care for ACL injuries, particularly for non-surgical cases.
References
Bullock-Saxton, J. E., Janda, V., & Bullock, M. I. (1993). Reflex activation of gluteal muscles in walking: An approach to restoration of muscle function for patients with low-back pain. Spine, 18(6), 704-708. https://pubmed.ncbi.nlm.nih.gov/8516698/
Haldeman, S., Kohlbeck, F. J., & McGregor, M. (2008). Unpredictability of cerebrovascular ischemia associated with cervical spine manipulation therapy: A review of sixty-four cases after cervical spine manipulation. Journal of Manipulative and Physiological Therapeutics, 31(1), 1-12.
MSK Centre. (2023, September 18). Minimize risks: Proven ACL injury prevention. https://mskcentre.ca/treatments/chiropractic/acl-injury-prevention/
Solecki, T. J., & Herbst, E. M. (2011). Chiropractic management of a postoperative complete anterior cruciate ligament rupture using a multimodal approach: A case report. Journal of Chiropractic Medicine, 10(1), 47-53. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3110400/
Insights from Dr. Alexander Jimenez
Background and Expertise
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a dual-licensed chiropractor and family practice nurse practitioner based in El Paso, Texas, with over 25 years of experience. His clinic, Injury Medical & Chiropractic Clinic, specializes in treating musculoskeletal conditions, including sports injuries like ACL tears. Dr. Jimenez’s unique qualifications allow him to integrate chiropractic care with advanced medical diagnostics, offering a holistic approach to recovery (A4M, n.d.).
Approach to ACL Injuries
While specific protocols for ACL injuries are not detailed on his website, Dr. Jimenez’s practice emphasizes:
Advanced Diagnostics: Using imaging (e.g., MRI, X-rays) and dual-scope procedures to assess injury severity and tailor treatments.
Multimodal Treatments: Combining chiropractic adjustments, soft tissue therapies, and rehabilitative exercises to address pain, mobility, and stability.
Functional Medicine: Incorporating nutrition and lifestyle changes to support healing and reduce inflammation.
Patient-Centered Care: Creating individualized plans based on the patient’s activity level and goals.
His focus on sports injuries suggests that he applies techniques, such as those described earlier, including manipulation, ultrasound, and Kinesio Taping, to ACL cases (Dr. Alex Jimenez, 2020).
Patient Testimonials
Patients praise Dr. Jimenez for his transformative care. One testimonial noted, “After my ACL surgery, I was struggling with persistent pain and stiffness. Dr. Jimenez’s chiropractic care helped me regain my strength and get back to my normal activities much faster than I expected” (Dr. Alex Jimenez, 2023). His ability to address complex injuries makes him a trusted provider in El Paso.
In El Paso, personal injury cases, such as those from car accidents or workplace incidents, often involve musculoskeletal injuries like ACL tears. Chiropractic care is a valuable option for these patients, offering non-invasive pain relief and functional restoration. Dr. Jimenez’s clinic is a go-to resource for personal injury victims, providing comprehensive care that addresses both immediate symptoms and long-term recovery (Dr. Alex Jimenez, 2019).
Dr. Jimenez’s Role as a Liaison
Dr. Jimenez’s dual licensure enables him to:
Provide Accurate Diagnoses: Using advanced imaging and diagnostic evaluations to document injuries thoroughly.
Offer Comprehensive Treatment: Combining chiropractic care with medical management for optimal outcomes.
Support Legal Documentation: Providing detailed medical reports is crucial for insurance claims and legal proceedings.
This makes him an invaluable ally for personal injury victims navigating the complex interplay of medical and legal systems (A4M, n.d.).
Case Example
Consider a car accident victim with an ACL sprain. Dr. Jimenez might use diagnostic imaging to confirm the injury, apply chiropractic adjustments to restore knee alignment, and prescribe exercises to strengthen supporting muscles. Simultaneously, he provides detailed medical records to help the patient’s legal claim, ensuring they receive appropriate compensation and care.
Correcting Muscle Imbalances: Strengthening weaker muscles like hamstrings to balance quadriceps dominance.
Improving Biomechanics: Adjusting joints to ensure proper movement patterns during activities like jumping or pivoting.
Enhancing Flexibility: Increasing joint range of motion to reduce stress on the ACL (MSK Centre, 2023).
Dr. Jimenez emphasizes preventative strategies, offering education on proper techniques and regular check-ups to catch issues early (Dr. Alex Jimenez, 2016).
Long-Term Knee Health
Regular chiropractic care supports long-term knee health by:
Maintaining Joint Alignment: Preventing undue stress on ligaments.
Strengthening Supporting Muscles: Enhancing stability through targeted exercises.
Promoting Overall Wellness: Integrating nutrition and lifestyle changes to reduce inflammation and support joint function.
For athletes, these interventions can enhance performance and resilience, allowing them to stay active safely.
ACL injuries can be a major setback, turning everyday tasks into painful challenges and sidelining athletes from their passions. Chiropractic care offers a promising complement to traditional treatments, utilizing techniques such as joint manipulation, therapeutic ultrasound, and rehabilitative exercises to alleviate pain, restore function, and facilitate recovery. Dr. Alexander Jimenez, with his dual expertise and integrative approach, stands out as a leading practitioner in El Paso, Texas, helping patients navigate both medical and legal aspects of their injuries.
For those facing an ACL injury, whether from sports or an accident, consulting a chiropractor like Dr. Jimenez can be a game-changer. His clinic, Injury Medical & Chiropractic Clinic, is dedicated to holistic healing, offering personalized care plans that address the root causes of pain and dysfunction. Contact the clinic at 915-850-0900 to explore how chiropractic care can support your recovery journey.
Disclaimer: This blog post is for informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of a qualified healthcare provider, such as an orthopedic specialist or chiropractor, for any questions regarding an ACL injury or other medical condition. Do not disregard professional medical advice or delay seeking it because of information in this post.
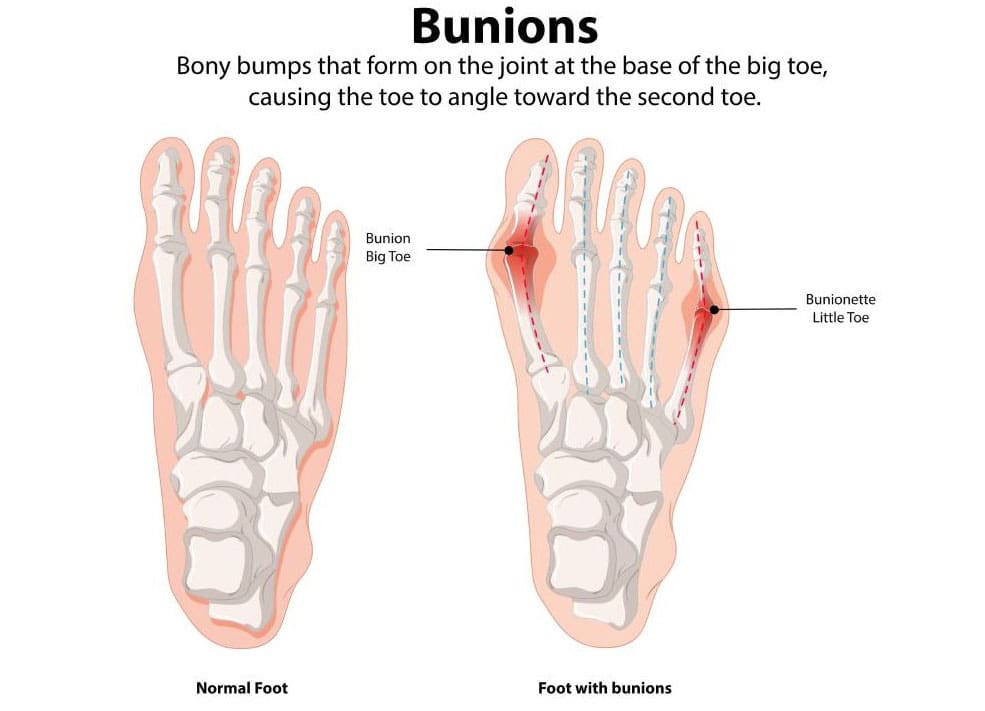
How can one effectively manage the early signs of bunions?
Bunions
A bunion, also known as hallux valgus, is a bony, often painful protrusion on the side of the big toe. The most common cause of bunions is a misalignment of the big toe. Early symptoms of a bunion include redness, thicker skin, edema, and discomfort around the big toe joint. While you can’t stop a bunion from growing, you can manage the symptoms along the way. Early indicators of bunions include pain management measures and treatment choices. (MedlinePlus, 2024)
Early Visual Signs
Bunions are initially minor and don’t result in many noticeable issues. The following symptoms may be present in the early stages of a bunion around the metatarsophalangeal (MTP) joint, which joins the base of your big toe to the rest of your foot. (American Academy of Orthopaedic Surgeons, 2022)
Redness
Skin that is darker and swollen
Skin that has gotten thicker and harder
There is a bony bump
A bump where the big toe goes toward the second toe or even under it
Corns and calluses
Early Physical Signs
While bunions may not be visible immediately, they can cause discomfort even in the early stages. Here are some early physical indicators of a developing bunion. (MedlinePlus, 2024)
Pain in the foot and big toe
This pain is especially noticeable when walking or wearing tight, narrow-toed shoes.
Decreased movement of the big toe
Tenderness
Inflammation
Swelling
Stiffness
Heat
Stages
Bunions often worsen over time, a condition known as progressive. You could have problems if you don’t do anything to stop your bunions from getting bigger. Bunions in later stages might cause the following symptoms: (American Academy of Orthopaedic Surgeons, 2022)
Long-lasting, intense pain in and around the MTP joint and the sides and bottom of your foot
Bursitis causes a sac full of fluid to form at the bottom of your big toe.
The big toe bends toward and even crosses over the second toe.
Too much bone development on the side of your big toe
Not being able to wear your regular shoes
Hard to walk
Abnormalities known as “hammer toe” occur when your second, third, or fourth toes bend upward in the middle, resembling a hammer or claw.
Hallux rigidus is a form of arthritis affecting the big toe.
Manage the Progression
Bunions tend to remain in place once they start to develop. However, there are several steps you can take to prevent them from worsening or causing additional problems. These are some of them: (American Academy of Orthopaedic Surgeons, 2022)
Place spacers between your toes to prevent friction and chafing.
Use over-the-counter (OTC) pads made of felt, silicone, or foam to cover the bunion.
You should also stretch your calf muscles to improve joint alignment.
Managing Pain
Advil and Motrin (ibuprofen) are two examples of non-steroidal anti-inflammatory medicines (NSAIDs) that can aid with bunion pain. Studies also show that injecting Botox into the muscles in the forefoot can help with pain. (Hurn, S. E., et al., 2022)
Nonsurgical Early Stage Treatment
If your bunions continue to worsen despite using the self-care procedures listed above, you may need to consult a podiatrist (a foot expert) or another healthcare provider. A healthcare provider may recommend.
Orthotics, or foot orthoses
Foot orthoses, also known as orthotics, are customized inserts that help alleviate bunion pain and prevent chafing.
Splints
Bunion splints are orthotic devices that can help straighten out your toes. People typically use them at night. (Aebischer, A. S., & Duff, S. 2020)
Physical Therapy
A physical therapist can help you by giving you exercises that will help your feet and joints line up better. They might also do manual therapy to help with pain. (Hurn, S. E., et al., 2022)
Podiatrist
A podiatrist is a medical doctor (M.D.) who specializes in treating health problems that affect the feet, ankles, and lower legs. If you want help with your bunion issues, ask your doctor for a referral to a podiatrist. (American Podiatric Medical Association, 2025)
Chiropractic Treatment
Chiropractors and nurse practitioners (NPs) have distinct roles in managing bunions, which are bony bumps at the base of the big toe caused by joint misalignment, often resulting in pain, swelling, and restricted movement. Here’s how each can help:
Chiropractors:
Focus: Chiropractors primarily address musculoskeletal issues through manual adjustments and manipulations.
Bunion Support:
Foot Adjustments: They may perform adjustments to improve foot alignment and joint mobility, which can potentially reduce bunion-related discomfort.
Soft Tissue Therapy: Techniques such as massage or myofascial release can help alleviate tension in surrounding muscles and tissues.
Orthotics or Taping: Some chiropractors recommend custom orthotics or use taping to support proper foot mechanics.
Exercise Guidance: They may suggest stretches or exercises to strengthen foot muscles and improve alignment.
Limitations: Chiropractors don’t prescribe medications or perform surgeries, so severe cases requiring these interventions would need referral to a podiatrist or orthopedic specialist.
Evidence: While some patients report relief from chiropractic care for foot issues, evidence specifically for bunions is limited, and results vary.
Nurse Practitioners:
Focus: NPs are advanced practice registered nurses with broad medical training, able to diagnose, treat, and prescribe medications within their scope of practice.
Bunion Support:
Diagnosis and Assessment: NPs can evaluate bunion severity, often using physical examinations or ordering imaging, such as X-rays, to assess joint damage.
Pain Management: They may prescribe anti-inflammatory medications (e.g., ibuprofen) or corticosteroid injections for pain and swelling.
Conservative Treatments: NPs can recommend padding, splints, or orthotic devices to reduce pressure and improve alignment.
Lifestyle Advice: They provide guidance on footwear (such as wide-toed shoes) and weight management to reduce stress on the bunion.
Referrals: For severe cases, NPs can refer patients to podiatrists or orthopedic surgeons for surgical options, such as bunionectomies.
Scope: NPs offer a medical approach, bridging conservative care and coordination with specialists.
Key Differences:
Chiropractors focus on non-invasive, manual techniques and alignment, while NPs can incorporate medications and broader medical management.
NPs are more likely to coordinate with other healthcare providers for comprehensive care, whereas chiropractors tend to work more independently.
General Notes:
Both can assist in managing mild to moderate bunion symptoms, but neither can “cure” bunions, particularly if the structural deformity has progressed.
Consult a podiatrist or an orthopedic specialist for persistent or worsening symptoms, as severe cases may require surgical intervention.
Always verify the provider’s credentials and experience in treating bunions.
Injury Medical Chiropractic and Functional Medicine Clinic
Dr. Jimenez, a nurse practitioner, treats a wide range of conditions using a combination of medical knowledge and chiropractic care. The clinic offers personalized care plans that incorporate functional medicine, acupuncture, electroacupuncture, and sports medicine. The clinic treats chronic pain syndromes and injuries, focusing on strength, agility, and flexibility. Comprehensive care plans, when paired with in-person and virtual health coaching, offer personalized treatment and wellness outcomes for patients of all ages and abilities.
Enhance Your Performance with Functional Foot Orthotics
References
MedlinePlus (2024). Bunions. U.S. Department of Health and Human Services.
American Academy of Orthopaedic Surgeons. (2022). “Bunions.” OrthoInfo. from https://orthoinfo.aaos.org/en/diseases–conditions/bunions/.
Hurn, S. E., Matthews, B. G., Munteanu, S. E., & Menz, H. B. (2022). Effectiveness of Nonsurgical Interventions for Hallux Valgus: A Systematic Review and Meta-Analysis. Arthritis care & research, 74(10), 1676–1688. https://doi.org/10.1002/acr.24603
Aebischer, A. S., & Duff, S. (2020). Bunions: A review of management. Australian Journal of General Practice, 49(11), 720–723. https://doi.org/10.31128/AJGP-07-20-5541
American Podiatric Medical Association. (2025). “What is a podiatrist?” Advancing foot and ankle medicine and surgery. from https://www.apma.org/patients-and-the-public/what-is-a-podiatrist/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine