Origin: The most common cause of�migraines/headaches�can relate to neck complications. From spending excessive time looking down at a laptop, desktop, iPad, and even from constant texting, an incorrect posture for extended periods of time can begin to place pressure on the neck and upper back leading to problems that can cause headaches. The majority of these type of headaches occurs as a result of tightness between the shoulder blades, which in turn causes the muscles on the top of the shoulders to also tighten and radiate pain into the head.
Arteriovenous malformations and expanding aneurysms
Lupus cerebritis
Venous sinus thrombosis
Cervical fracture or malformation
Fracture or dislocation
Occipital neuralgia
Vertebral artery dissection
Chiari malformation
Metabolic
Hypoglycemia
Hypercapnea
Carbon monoxide
Anoxia
Anemia
Vitamin A toxicity
Glaucoma
Subarachnoid Hemorrhage
Usually due to ruptured aneurysm
Sudden onset of severe pain
Often vomiting
Patient appears ill
Often nuchal rigidity
Refer for CT and possibly lumbar puncture
Meningitis
Patient appears ill
Fever
Nuchal rigidity (except in elderly and young children)
Refer for lumbar puncture – diagnostic
Neoplasms
Unlikely cause of HA in average patient population
Mild and nonspecific head pain
Worse in the morning
May be elicited by vigorous head shaking
If focal symptoms, seizures, focal neurologic signs, or evidence of increased intracranial pressure are present rule our neoplasm
Subdural Or Epidural Hemorrhage
Due to hypertension, trauma or defects in coagulation
Most often occurs in the context of acute head trauma
Onset of symptoms may be weeks or months after an injury
Differentiate from the common post-concussion headache
Post-Concussive HA may persist for weeks or months after an injury and be accompanied by dizziness or vertigo and mild mental changes, which will all subside
Exquisite tenderness and/or swelling over the temporal or occipital arteries
Evidence of arterial insufficiency in the distribution of branches of the cranial vessels
High ESR
Cervical Region HA
Neck trauma or with symptoms or signs of cervical root or cord compression
Order MR or CT cord compression due to fracture or dislocation
Cervical instability
Order cervical spine x-rays lateral flexion and extension views
Ruling Out Dangerous HA
Rule our history of serious head or neck injury, seizures or focal neurologic symptoms, and infections that may predispose to meningitis or brain abscess
Check for fever
Measure blood pressure (concern if diastolic >120)
Ophthalmoscopic exam
Check neck for rigidity
Auscultate for cranial bruits.
Complete neurologic examination
If needed order complete blood cell count, ESR, cranial or cervical imaging
Episodic Or Chronic?
<15 days per month = Episodic
>15 days per month = Chronic
Migraine HA
Generally due to dilation or distension of cerebral vasculature
Serotonin In Migraine
AKA 5-hydroxytryptamine (5-HT)
Serotonin becomes depleted in migraine episodes
IV 5-HT can stop or reduce severity
Migraine With Aura
History of at least 2 attacks fulfilling the following criteria
One of the following fully reversible aura symptoms:
Visual
Somatic sensory
Speech or language difficulty
Motor
Brain stem
2 of the following 4 characteristics:
1 aura symptom spreads gradually over ?5 min, and/or 2 symptoms occur in succession
Each individual aura symptom lasts 5-60 min
1 aura symptom is unilateral
Aura accompanied or followed in <60 min by headache
Not better accounted for by another ICHD-3 diagnosis, and TIA excluded
Migraine Without Aura
History of at least 5 attacks fulfilling the following criteria:
Headache attacks lasting 4-72 h (untreated or unsuccessfully treated)
Unilateral pain
Pulsing/pounding quality
Moderate to severe pain intensity
Aggravation by or causing avoidance of routine physical activity
During headache nausea and/or sensitivity to light and sound
Not better accounted for by another ICHD-3 diagnosis
Cluster Headache
Severe unilateral orbital, supraorbital and/or temporal pain
�Like an ice pick stabbing me the eye�
Pain lasts 15-180 minutes
At least one of the following on the side of headache:
Conjunctival injection
Facial sweating
Lacrimation
Miosis
Nasal congestion
Ptosis
Rhinorrhea
Eyelid edema
History of similar headaches in the past
Tension Headache
Headache pain accompanied by two of the following:
Pressing/tightening (non-pulsing) quality
�Feels like a band around my head�
Bilateral location
Not aggravated by routine physical activity
Headache should be lacking:
Nausea or vomiting
Photophobia and phonophobia (one or the other may be present)
History of similar headaches in the past
Rebound Headache
Headache occurring on ?15 days a month in a patient with a pre-existing headache disorder
Regular overuse for >3 months of one or more drugs that can be taken for acute and/or symptomatic treatment of headache
Due to medication overuse/withdrawal
Not better accounted for by another ICHD-3 diagnosis
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
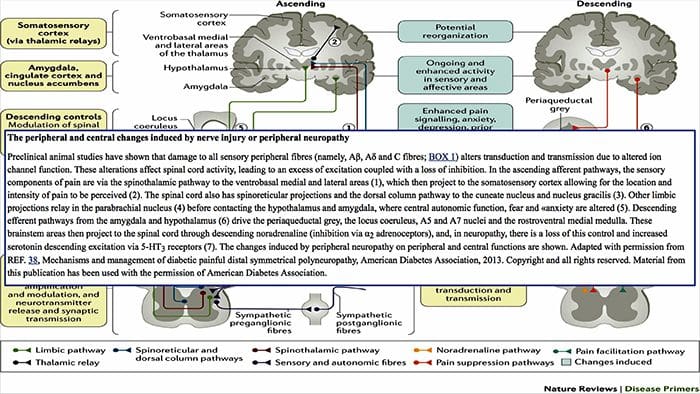
When the sensory system is affected by injury or disease, the nerves within that system can’t work properly to transmit sensations and feelings into the brain. This frequently contributes to a feeling of numbness, or lack of sensation. However, in certain cases, when this system is damaged, people may experience pain in the affected area.
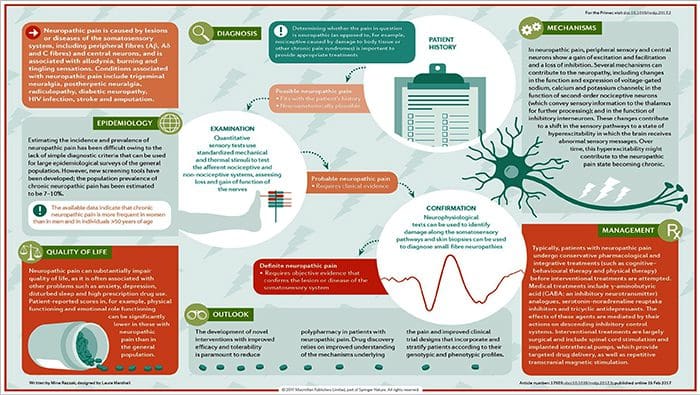
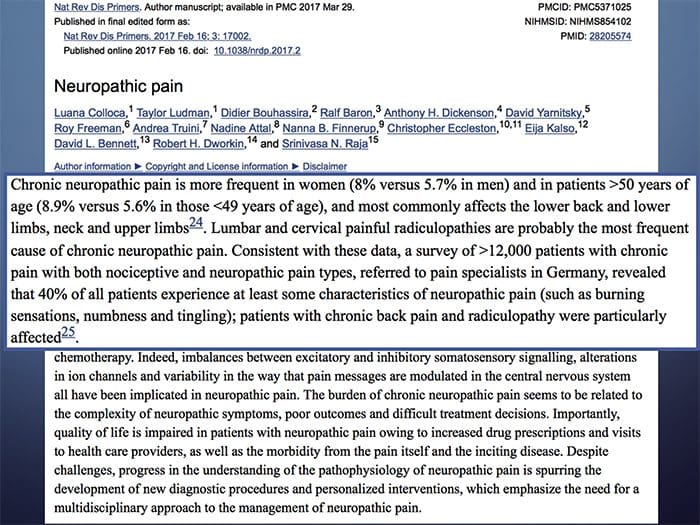
Neuropathic pain does not start abruptly or resolve quickly; it’s a chronic pain condition which leads to persistent pain symptoms. For most individuals, the intensity of their symptoms may wax and wane throughout the day. Although neuropathic pain is supposed to be related to peripheral nerve health issues, like neuropathy caused by diabetes or spinal stenosis, injuries to the brain or spinal cord may also lead to chronic neuropathic pain. Neuropathic pain is also referred to as nerve pain.
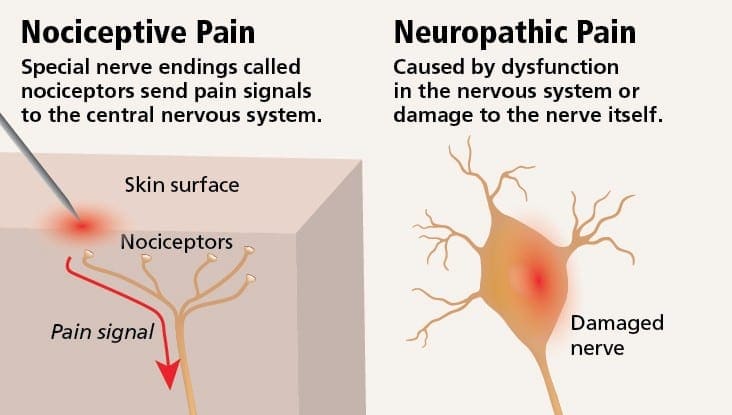
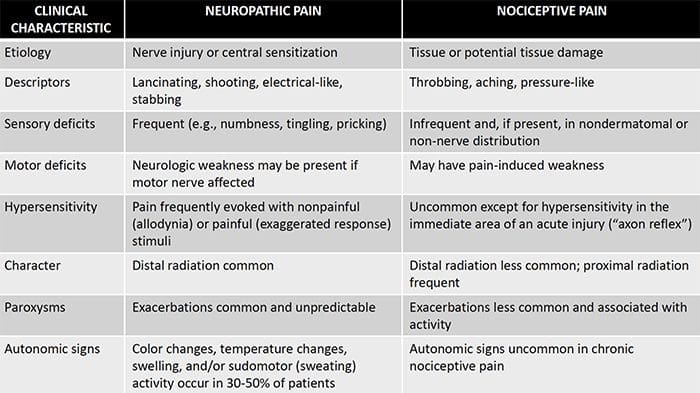
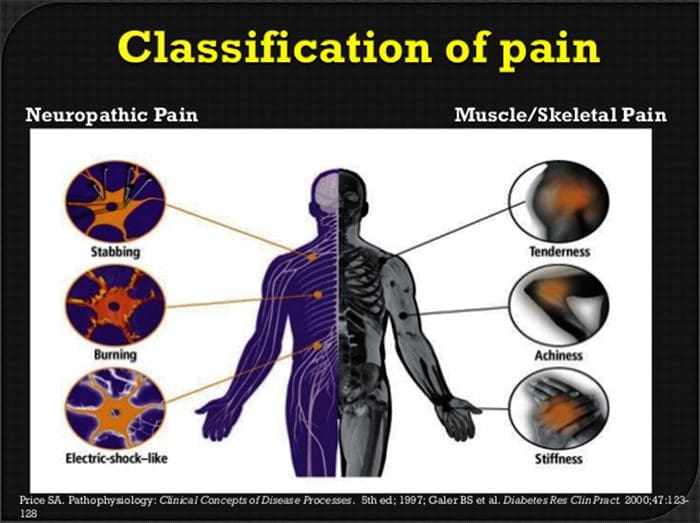
Neuropathic pain may be contrasted to nociceptive pain. Neuropathic pain does not develop to any specific circumstance or outside stimulus, but rather, the symptoms occur simply because the nervous system may not be working accordingly. As a matter of fact, individuals can also experience neuropathic pain even when the aching or injured body part is not actually there. This condition is called phantom limb pain, which may occur in people after they’ve had an amputation.
Nociceptive pain is generally acute and develops in response to a specific circumstance, such as when someone experiences a sudden injury, like hammering a finger with a hammer or stubbing a toe when walking barefoot. Moreover, nociceptive pain tends to go away once the affected site heals. The body contains specialized nerve cells, known as nociceptors, which detect noxious stimuli that could damage the body, such as extreme heat or cold, pressure, pinching, and exposure to chemicals. These warning signals are then passed along the nervous system to the brain, resulting in nociceptive pain.
What are the Risk Factors for Neuropathic Pain?
Anything that contributes to a lack of function within the sensory nervous system can lead to neuropathic pain. As such, nerve health issues from carpal tunnel syndrome, or similar conditions, can ultimately trigger neuropathic pain. Trauma, resulting in nerve injury, may lead to neuropathic pain. Other conditions which could predispose individuals to developing neuropathic pain include: diabetes, vitamin deficiencies, cancer, HIV, stroke, multiple sclerosis, shingles, and even some cancer treatments.
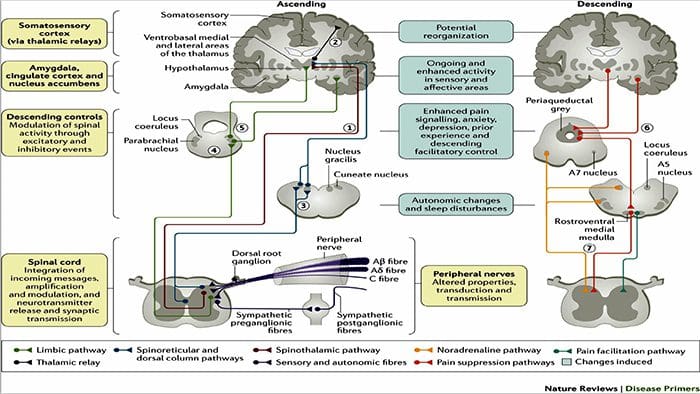
What are the Causes of Neuropathic Pain?
There are many causes from which individuals may develop neuropathic pain. But on a cellular level, one explanation is an increased release of certain receptors that indicate pain, together with a diminished ability of the nerves to modulate these signals, leads to the sensation of pain originating from the affected region. Additionally, in the spinal cord, the region which exerts painful signs is rearranged with corresponding changes in hormones and loss of normally-functioning mobile bodies. Those alterations result in the perception of pain in the absence of external stimulation. In the brain, the ability to block pain can be affected following an injury, such as stroke or trauma from an injury. As time passes, additional cell damage happens and the feeling of pain continues. Neuropathic pain is also related to diabetes, chronic alcohol intake, certain cancers, vitamin B deficiency, diseases, other nerve-related diseases, toxins, and specific drugs.
What are the Symptoms of Neuropathic Pain?
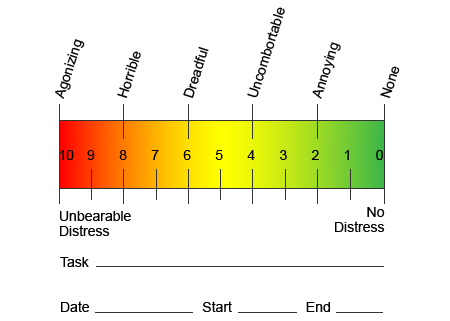
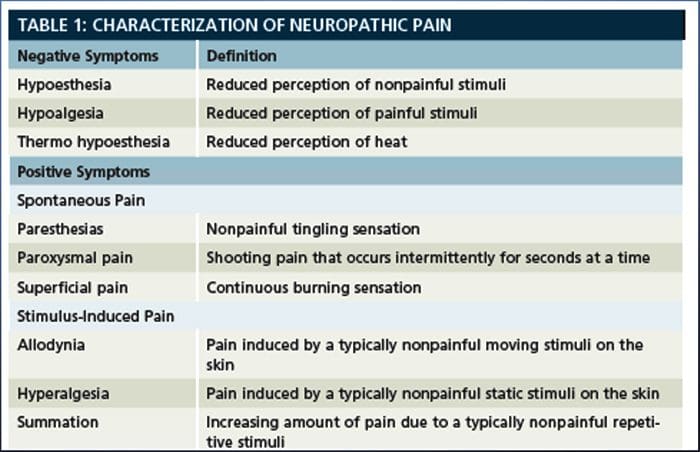
Contrary to other neurological conditions, identification of neuropathic pain can be challenging. However, several, if any, objective signals may be present. Healthcare professionals have to decipher and translate an assortment of words which patients use to describe their pain. Patients may describe their symptoms as sharp, dull, hot, cold, sensitive, itchy, deep, stinging, burning, among a variety of other descriptive terms. Additionally, some patients may experience pain through light touch or pressure.
In an effort to help identify how much pain patients could be undergoing, different scales are often used. Patients are asked to rate their pain according to a visual scale or numerical graph. Many examples of pain scales exist, such as the one demonstrated below. Often, pictures of faces depicting a variety of levels of pain may be helpful when individuals have a difficult time describing the quantity of pain they are experiencing.
Chronic Pain and Mental Health
For many, the impact of chronic pain may not be limited to the pain ; it may also negatively influence their mental state. New research studies conducted by scientists at the Northwestern University in Chicago can explain why individuals who have chronic pain also suffer with seemingly unrelated health issues, such as depression, stress, lack of sleep and difficulty concentrating.
The evaluation demonstrated that people with chronic pain show different regions of the brain which are always active, most specifically, the area associated with mood and attention. This continuous action rewires nerve connections from the brain and leaves chronic pain sufferers at greater risk for psychological problems. Researchers suggested that getting pain signals constantly could result in mental rewiring that adversely affects the mind. The rewiring compels their brains to devote mental resources differently to deal with everyday tasks, from mathematics, to recalling a shopping list, to feeling happy.
The pain-brain connection has been well recorded, at least anecdotally, and lots of healthcare professionals say they’ve seen first-hand the way the patient’s mental state can go downhill when they endure chronic pain. Misconceptions about the pain-brain connection may have emerged from a lack of evidence that pain has a measurable, lasting influence on the brain. Researchers expect that with additional research into the mechanisms of how chronic pain makes people more susceptible to mood disorders, people are going to have the ability to better manage their overall well-being.
Culture and Chronic Pain
Many things contribute to the way we experience and express pain, however, it has also been recently suggested by researchers that culture relates directly into the expression of pain. Our upbringing and societal values affect how we express pain and also its own nature, intensity and length. However, these variables aren’t as obvious as socio-psychological values, such as age and sex.
Research states that chronic pain is a multifaceted process and the concurrent interplay between pathophysiology, cognitive, affective, behavioral and sociocultural factors summate to what is referred to as the chronic pain experience. It’s emerged that chronic pain is experienced differently among patients of varied cultures and ethnicities.
Some cultures encourage the expression of pain, particularly in the southern Mediterranean and Middle East. Other individuals suppress it, as in the many lessons to our kids about behaving bravely and not crying. Pain is recognized as part of the human experience. We are apt to assume that communication about pain will seamlessly cross cultural boundaries. But people in pain are subject to the manners their civilizations have trained them to experience and express pain.
Both individuals in pain and healthcare professionals experience difficulties communicating pain across ethnic borders. In a matter like pain, where effective communication can have far-reaching implications for medical care, quality of life and potentially survival, the role of culture in pain communicating remains under-evaluated. Persistent pain is a multidimensional, a composite encounter formed by interweaving and co-influencing biological and psychosocial factors. Knowing the culmination of these factors is critical to understanding the differences of its manifestation and management.
How is Neuropathic Pain Diagnosed?
The diagnosis of neuropathic pain relies upon additional evaluation of an individual’s history. If underlying nerve damage is suspected, then analysis of the nerves together with testing may be justified. The most common means to assess whether or not a nerve is injured is using electrodiagnostic medicine. This medical subspecialty utilizes techniques of nerve conduction studies with electromyelography (NCS/EMG). Clinical evaluation may show evidence of loss of work, and can include evaluation of light touch, the capacity to differentiate sharp out of dull pain and the ability to discern temperature, as well as the evaluation of vibration.
After a thorough clinical examination is completed, the electrodiagnostic analysis could be planned. These studies are conducted by specially trained neurologist and physiatrists. If neuropathy is suspected, a hunt for reversible causes ought to be accomplished. This can include blood function for vitamin deficiencies or thyroid problems, and imaging studies to exclude a structural lesion affecting the spinal cord. Depending on the results of this testing, there might be a means to decrease the intensity of the neuropathy and possibly reduce the pain that a patient is undergoing.
Regrettably, in many conditions, even good control of the underlying cause of the neuropathy can’t reverse the neuropathic pain. This is commonly seen in patients with diabetic neuropathy. In rare instances, there may be signs of changes in the skin and hair growth pattern in an affected region. These alterations may be associated with changes in perspiration. If present, these changes can help identify the likely presence of neuropathic pain related to a condition known as complex regional pain syndrome.
Dr. Alex Jimenez’s Insight
Neuropathic pain is a chronic pain condition which is generally associated with direct damage or injury to the nervous system or nerves. This type of pain is different from nociceptive pain, or the typical sensation of pain. Nociceptive pain is an acute or sudden sensation of pain which causes the nervous system to send signals of pain immediately after the trauma occurred. With neuropathic pain, however, patients may experience shooting, burning pain without any direct damage or injury. Understanding the possible causes of the patient’s neuropathic pain versus any other type of pain, can help healthcare professionals find better ways to treat chronic pain conditions.
What is the Treatment for Neuropathic Pain?
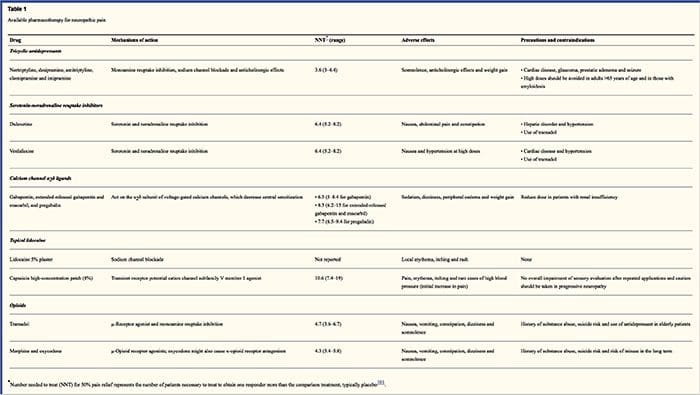
Various medicines are used in an attempt to treat neuropathic pain. The majority of these drugs are utilized off-label, which means that the medicine was approved by the FDA to treat different conditions and was then recognized as being advantageous to treat neuropathic pain. Tricyclic antidepressants, such as amitriptyline, nortriptyline and desipramine, have been prescribed for management of neuropathic pain for several years.
Some individuals find that these may be very effective in giving them relief. Other kinds of antidepressants have been shown to offer some relief. Selective serotonin reuptake inhibitors, or SSRIs, such as paroxetine and citalopram, and other antidepressants , such as venlafaxine and bupropion, have been utilized in certain patients. Another frequent treatment of neuropathic pain incorporates antiseizure medications, including carbamazepine, phenytoin, gabapentin, lamotrigine, and others.
In acute cases of painful neuropathy which don’t respond to first-line brokers, drugs typically utilized to treat heart arrhythmias may be of some benefit; however, these can lead to significant side effects and often have to be monitored closely. Medications applied directly to the skin can offer modest to perceptible benefit for some patients. The forms commonly used include lidocaine (in patch or gel type) or capsaicin.
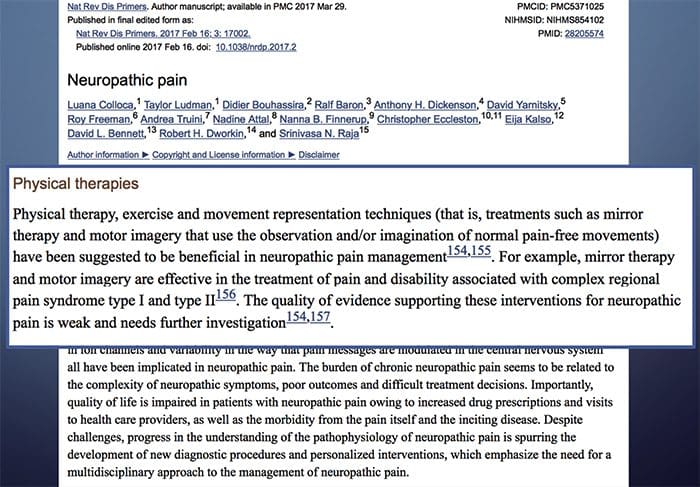
Treating neuropathic pain is dependent on the underlying cause. If the cause is reversible, then the peripheral nerves can regenerate and the pain will abate; nonetheless, this reduction in pain may take several months to years. Several other alternative treatment options, including chiropractic care and physical therapy, may also be utilized in order to help relieve tension and stress along the nerves, ultimately helping to improve painful symptoms.
What is the Prognosis for Neuropathic Pain?
Many individuals with neuropathic pain are able to get some measure of aid, even when their pain persists. Although neuropathic pain isn’t dangerous to a patient, the presence of chronic pain can negatively affect quality of life. Patients with chronic nerve pain might suffer from sleep deprivation or mood disorders, including depression, anxiety and stress, as previously mentioned above. Because of the inherent alopecia and lack of sensory feedback, patients are at risk of developing injury or infection or unknowingly causing an escalation of a present injury. Therefore, it’s essential to seek immediate medical attention and follow specific guidelines directed by a healthcare professional for safety and caution.
Can Neuropathic Pain be Prevented?
The best way to prevent neuropathic pain is to avoid the development or progression of neuropathy. Monitoring and changing lifestyle options, including restricting the use of alcohol and tobacco; keeping a healthy weight to lower the chance of diabetes, degenerative joint disease, or stroke; and having great ergonomic form at work or when practicing hobbies to lower the risk of repetitive stress injury are strategies to decrease the probability of developing neuropathy and potential neuropathic pain. Make sure to seek immediate medical attention in the case of any symptoms associated with neuropathic pain in order to proceed with the most appropriate treatment approach.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Tension headaches are the most prevalent types of headaches, occurring more often in women than in men. Research shows that 48 percent of women and 38 percent of men suffer from tension headaches.
Each year, patients spend more than $2 billion on over the counter headache medications. In fact, people spend a lot of money and effort seeking remedies for headaches. From prescription medication to over the counter drugs to alternative headache treatments like meditation, acupuncture, and chiropractic.
In fact, chiropractic is a proven treatment for these types headaches, but there is more to it than just adjustments. Chiropractic offers a whole body approach to treatment that can not only relieve the pain of these headaches, but help prevent them as well.
What Are Tension Headaches?
The most common type of headache is the tension headache which is described as pain ranging from mild to moderate that feels like a tight band is wrapped around the head. While stress can be a factor in the cause of these headaches, it still isn�t well understood how these headaches originate. Symptoms of a tension headache include:
Aching, dull pain in the head
Sensation of pressure or tightness on the back and sides of the head or across the forehead
Tenderness in the shoulder muscles, neck, and scalp
There are two categories of tension headaches: chronic and episodic. There are two primary factors that identify each type. The length of the headache and the frequency can help you determine which type of tension headache you have.
Chronic Tension Headaches
Length of Headache � hours and can be continuous
Frequency of Headache � occur 15 days or more a month for three or more months
Episodic Tension Headaches
Length of Headache – half hour to a week
Frequency of Headache � occur less than 15 days a month for three or more months
There are two primary risk factors for tension headaches:
Women � Research shows that nearly 90 percent of women will experience tension headaches throughout the course of their life. Only 70 percent of men will experience tension headaches in their lifetime.
Middle Age � Tension headaches increase as people approach 40 and peak at middle age, or when a person is in their 40s. However, anyone can get a tension headache, regardless of age.
Lifestyle Changes To Treat Tension Headaches
A chiropractor can treat tension headaches through traditional spinal manipulation and adjustments, but they also provide advice on lifestyle and nutrition. Several things that your chiropractor may suggest include applying heat or ice to the area around your neck, shoulders, or head. A warm bath or shower may also help.
Stress management is another way that you can learn to manage and prevent tension headaches. This is typically a combination of minimizing stress in your life and learning relaxation techniques. Your chiropractor may also help you improve your posture. Poor posture is a very common contributing factor for many types of headaches.
Chiropractic for Tension Headaches
Your Doctor of Chiropractic will sit down with you to discuss your history, including your headaches. He or she will conduct diagnostic tests including x-rays, MRIs and other to determine if there are underlying causes for your headaches. They will recommend various lifestyle changes including dietary changes and exercises that you can do.
Your doctor may also perform chiropractic adjustments, or spinal manipulation which will help return the body to proper balance, improving spinal function and alleviating stress on the body and system. This helps to relieve pain as an immediate treatment, but when performed consistently, chiropractic can also help prevent tension headaches, allowing you to live pain free.
Injury Medical Clinic: Migraine Treatment & Recovery
If the sensory system becomes impacted by injury or disease, the nerves in that system can’t function in the transmitting of sensation to the brain. This can lead to a sensation of numbness, or lack of sensation. In some cases when the sensory system is injured, individuals can experience pain in the affected region. Neuropathic pain does not start quickly or ends quickly. It’s a chronic condition that leads to�symptoms of persistent pain. For many, the intensity of the symptoms can come and go throughout a day. Neuropathic pain is thought to be associated with peripheral nerve problems, i.e. neuropathy caused by diabetes, spinal stenosis, injury to the brain or spinal cord can also lead to chronic neuropathic pain.
NEUROPATHIC PAIN
Objectives:
What is it?
What is the pathophysiology behind it?
What are the causes
What are some of the pathways
How can we fix it?
NEUROPATHIC PAIN
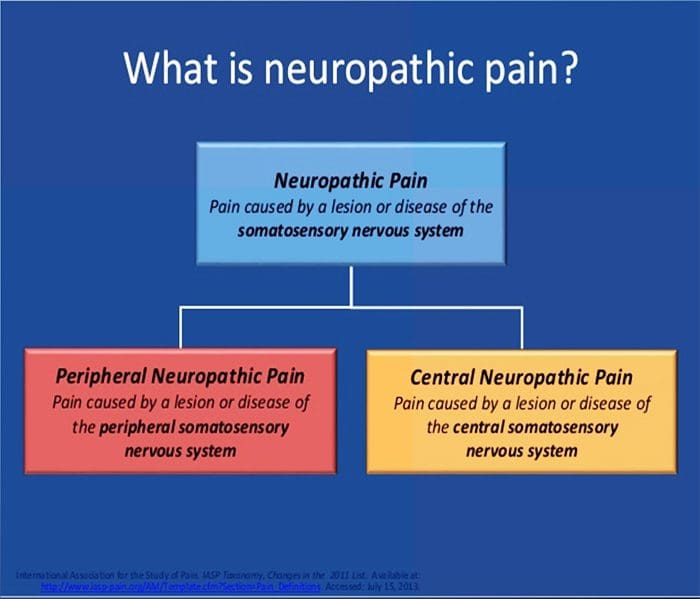
Pain initiated or caused by a primary lesion or dysfunction in the somatosensory nervous system.
Neuropathic pain is usually chronic, difficult to treat and often resistant to standard analgesic management.
PATHOGENESIS OF NEUROPATHIC PAIN
PERIPHERAL MECHANISMS
After a peripheral nerve lesion, neurons become more sensitive and develop abnormal excitability and elevated sensitivity to stimulation
This is known as…Peripheral Sensitization!
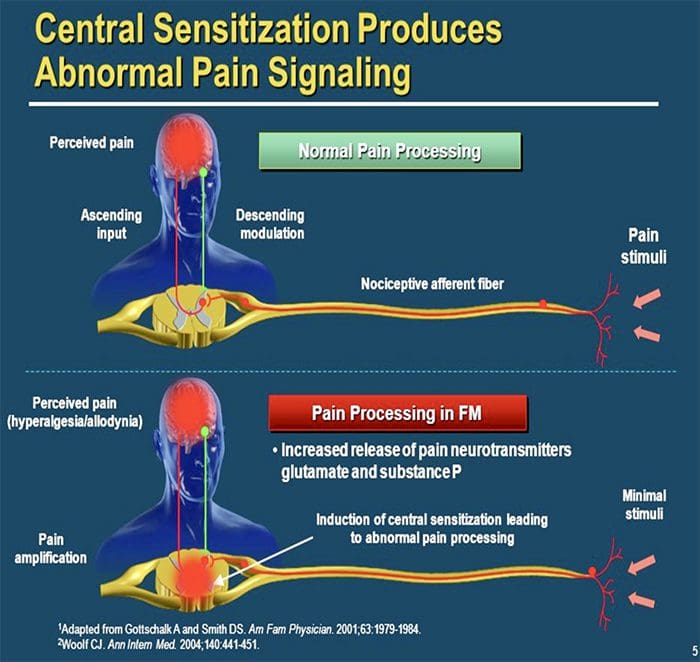
CENTRAL MECHANISMS
As a consequence of ongoing spontaneous activity arising in the periphery, neurons develop an increased background activity, enlarged receptive fields and increased responses to afferent impulses, including normal tactile stimuli
This is known as…Central Sensitization!
COMMON CAUSES
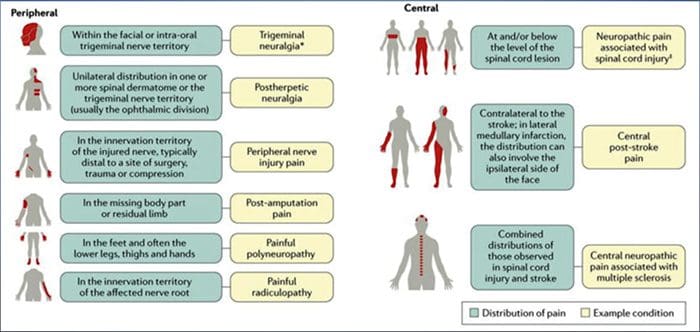
Lesions or diseases of the somatosensory nervous system can lead to altered and disordered transmission of sensory signals into the spinal cord and the brain; common conditions associated with neuropathic pain include:
Postherpetic neuralgia
Trigeminal neuralgia
Painful radiculopathy
Diabetic neuropathy
HIV infection
Leprosy
Amputation
Peripheral nerve injury pain
Stroke (in the form of central post-stroke pain)
PHANTOM LIMB PAIN & AUGMENTED REALITY
Phantom Limb Pain and AR
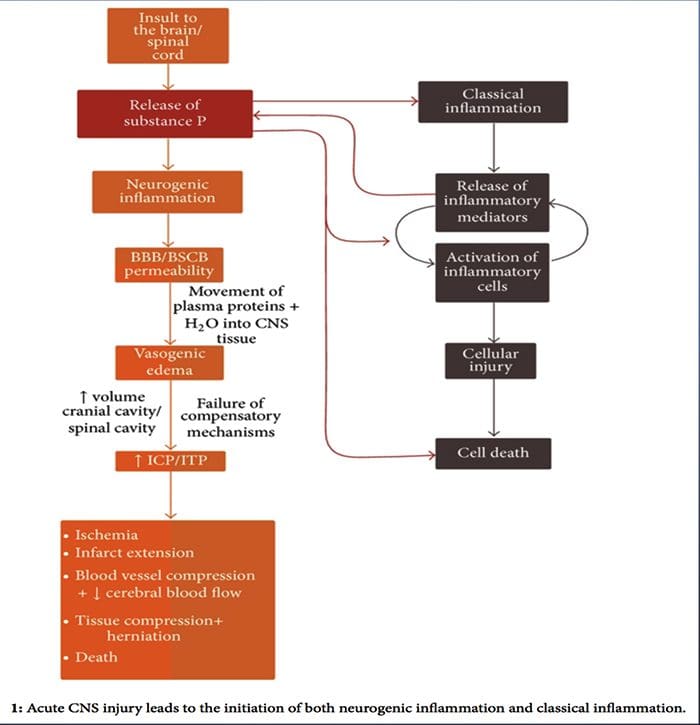
NEUROGENIC INFLAMMATION
Objectives:
What is it?
What is the pathophysiology behind it?
What are the causes
How can we fix it?
NEUROGENIC INFLAMMATION
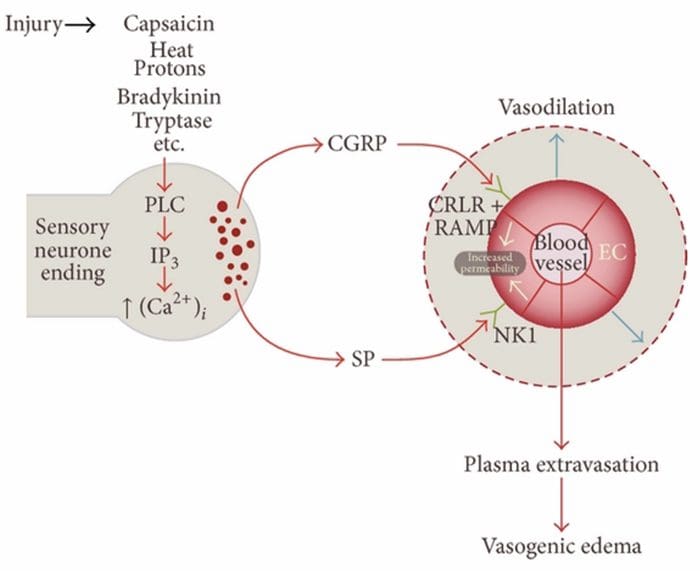
Neurogenic inflammation is a neurally elicited, local inflammatory response characterized by vasodilation, increased vascular permeability, mast cell degranulation, and the release of neuropeptides including SP and calcitonin gene-related peptide (CGRP)
It appears to play an important role in the pathogenesis of numerous disease including migraine, psoriasis, asthma, fibromyalgia, eczema, rosacea, dystonia and multiple chemical sensitivity
COMMON CAUSES
There are multiple pathways by which neurogenic inflammation may be initiated. It is well documented, using both animal models and isolated neurons in vitro, that capsaicin, heat, protons, bradykinin, and tryptase are upstream regulators of the intracellular calcium influx, which results in inflammatory neuropeptide release. In contrast, it is thought that prostaglandins E2 and I2, cytokines, interleukin-1, interleukin-6, and tumor necrosis factor do not cause neurotransmitter release themselves, but rather excite sensory neurons and thus lower the threshold for firing and cause augmented release of neuropeptides.
While neurogenic inflammation has been extensively studied and well documented in peripheral tissues, until recently the concept of neurogenic inflammation within the CNS has remained largely unexplored. Given the capacity for neurogenic inflammation to influence vascular permeability and lead to the genesis of edema, it has now been widely investigated for its potential to influence BBB permeability and vasogenic edema within the brain and spinal cord under varying pathological conditions.
Headaches are very common health issues, and lots of people treat themselves by using basic painkillers, drinking additional water, with rest, or by simply waiting for the headache to go away on its own. As a matter of fact, a headache is among the most common reasons for doctor office visits.
Just about everyone will experience a headache sometime during their life. Most headaches are not caused by serious or sinister conditions. However, people understandably worry if headaches feel different, whether they’re especially severe, particularly frequent or unusual in any other manner. But, the most common concern is whether the headache may be a symptom of an underlying health issue, such as a brain tumor.
The following article discusses headaches generally. It explains the various types of headaches you may experience and describes those very rare situations where a headache may be a symptom of a serious disease.
Types of Headaches
Headaches can be categorized as primary, or they can be classified as secondary, meaning they are a side-effect of another injury or condition.
A healthcare professional can usually determine the possible cause of your headaches from speaking to you and examining you. When they have found the cause then you’ll have the ability to decide the best treatment approach for your head pain symptoms. This may involve taking drugs only when you get the headaches, taking daily medication to stop them altogether, and/or even stopping medication you’re already taking. Very occasionally, headaches may need further diagnosis to rule out more serious underlying causes. Chiropractic care and physical therapy are also commonly utilized to help treat headaches. Below, we will discuss the different types of headaches.
Primary Headaches
The most common types of headaches, by far, are tension headaches and migraines.
Tension Headaches
Tension headaches are generally felt as a band around the forehead. They may last for many days. They may be tiring and uncomfortable, but they don’t normally disturb sleep. Most people can carry on working with a tension headache. These often have a tendency to worsen as the day progresses, however, they aren’t usually made worse with physical activities, though it’s not strange to be somewhat sensitive to bright light or noise.
Migraines
Migraines are also very common types of headaches. A typical migraine is described as a throbbing sensation. Headaches which are one-sided, headaches which throb and headaches that make you feel sick are more inclined to be migraines compared to anything else. Migraines are often severe enough to be disabling. Some individuals will need to go to bed to sleep off their aggravation.
Cluster Headaches
Cluster headaches are extremely severe headaches, sometimes called “suicide headaches”. They occur in clusters, often every day for a number of days or maybe weeks. Then they vanish for weeks on end. These types of headaches are rare and often occur particularly in adult male smokers. They’re intense, one-sided headaches, which are very disabling, meaning they stop routine activity. People often describe them as the worst pain they have ever felt. Cluster headaches are typically one-sided. Patients frequently have a red watery eye on the other hand, a stuffy runny nose and a droopy eyelid.
Chronic Tension Headaches
Chronic tension headaches (or chronic daily headache) is generally caused by muscle tension in the back of the neck and affects women more frequently than men. Chronic means that the problem is persistent and ongoing. These headaches can develop due to neck injuries or tiredness and may worsen with drug/medication overuse. A headache that occurs virtually every day for 3 weeks or more is known as a chronic daily headache or a chronic tension headaches.
Medication-Overuse Headaches
Medication-overuse headaches or medication-induced aggravation, is an unpleasant and long-term headache. It’s brought on by taking painkillers usually meant for headaches. Unfortunately, when painkillers are taken regularly for headaches, the body reacts by creating additional pain sensors in the brain. Finally, the pain sensors are so many that the head becomes super-sensitive and the headache won’t go away. Individuals who have these headaches often take an increasing number of painkillers to attempt and feel much better. But, the painkillers may have regularly long ceased to work. Medication-overuse headaches are the most common cause of secondary headache.
Exertional Headaches/Sexual Headaches
Exertional headaches are headaches associated with physical activity. They may get severe very quickly following a strenuous activity like coughing, running, with intercourse, and straining with bowel movements. They’re more commonly experienced by patients that also have migraines, or who have relatives with migraine.
Headaches associated with sex particularly worry patients. They can occur as sex starts, at orgasm, or following sex. Headaches at orgasm would be the most common type. They are generally acute, at the back of the head, behind the eyes or all around. They last about twenty minutes and aren’t usually an indication of any other underlying health issues or problems.
Exertional and sexual intercourse-related headaches aren’t typically an indication of serious underlying problems. Very occasionally, they can be a sign that there is a leaky blood vessel on the surface of the brain. As a result, if they are marked and repeated, it’s sensible to talk about them with your healthcare professional.
Primary Stabbing Headaches
Primary traumatic headaches are sometimes called “ice-pick headaches” or “idiopathic stabbing headache”. The term “idiopathic” is used by doctors for something that comes without a clear cause. These are brief, stabbing headaches that are extremely sudden and severe. They generally last between 5 and 30 seconds and they occur at any time of the day or night. They feel as though a sharp object, like an ice pick, is being stuck into your head. They frequently occur in or just behind the ear and they are sometimes quite frightening. Even though they aren’t migraines they’re more prevalent in those who suffer from migraines, nearly half of individuals who experience migraines have principal stabbing headaches.
They are often felt at the place on the head where the migraines have a tendency to happen. Primary stabbing headaches are too brief to take care of, even though migraine prevention medications may reduce their number.
Hemicrania Continua
Hemicrania continua is a major chronic daily headache. It typically induces a continuous but shifting pain on one side of the brain. The pain is generally continuous with episodes of severe pain, which can last between 20 minutes and several days. During those episodes of severe pain there may be other symptoms, such as watering or redness of the eye, runny or blocked nose, and drooping of the eyelid, around precisely the same side as the aggravation. Similar to a migraine, there may also be sensitivity to light, feeling sick, such as nausea, and being sick, such as vomiting. The headaches do not go away but there may be periods when you don’t have any headaches. Hemicrania continua headaches respond to medicine called indometacin.
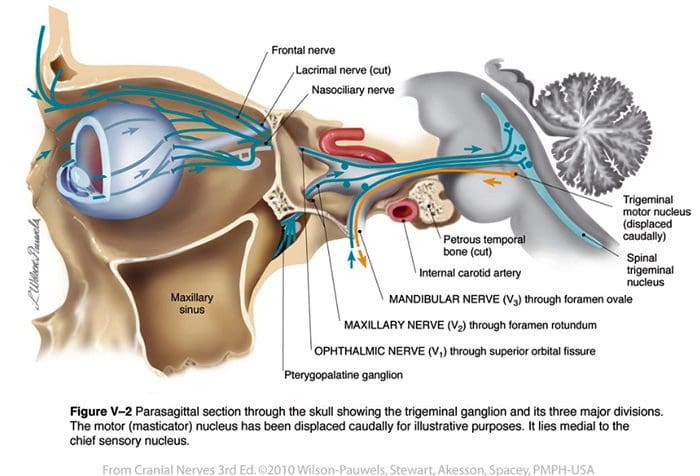
Trigeminal Neuralgia
Trigeminal neuralgia causes facial pain. The pain consists of very short bursts of electric shock-like sensations in the face, particularly at the area of the eyes, nose, scalp, brow, lips or limbs. It’s usually one-sided and is more common in people over age 50. It may be triggered by touch or a light breeze on the surface area.
Headache Causes
Occasionally, headaches have underlying causes, and treatment of the headache involves treating the cause. Individuals often fear that headaches are caused by serious illness, or by high blood pressure. Both of these are extremely uncommon causes of headache, really increased blood pressure usually causes no symptoms in any way.
Chemicals, Drugs and Substance Withdrawal
Headaches can be because of a substance, or its withdrawal, for example:
Carbon monoxide, that is made by gas heaters which aren’t properly ventilated
Drinking alcohol, with headache often experienced the morning afterwards
Deficiency of body fluid or dehydration
Headaches Due to Referred Pain
Some headaches may be caused by pain in some other portion of the head, such as ear or tooth pain, pain in the jaw joint and pain in the neck.
Sinusitis is also a frequent cause of headaches. The sinuses are “holes” in the skull which are there to stop it from becoming too heavy for the neck to transport around. They are lined with mucous membranes, such as the lining of the nose, and this creates mucus in response to colds or allergy. The liner membranes also swell and can block the drainage of the mucus out of the space. It subsequently becomes cracked and infected, resulting in headache. The headache of sinusitis is often felt at the front of the head and also in the face or teeth.
Frequently the face feels tender to tension, particularly just below the eyes beside the nose. You might have a stuffy nose and the pain is often worse when you bend forwards. Acute sinusitis is the kind that comes on fast in conjunction with a cold or abrupt allergy. You may have a temperature and be generating a lot of mucus. Chronic sinusitis may be caused by allergy, by overusing decongestants or with the acute sinusitis that doesn’t settle. The sinuses become chronically infected and the nasal linings chronically swollen. The contents of this uterus may be thick but frequently not infected.
Acute glaucoma can cause severe headaches. In this condition, the pressure inside the eyes goes up suddenly and this causes a surprisingly, very severe headache behind the eye. Even the eyeball can feel really hard to touch, the eye is red, the front part of the eye, or cornea, can seem cloudy and the eyesight is generally blurred.
What Types of Headaches are Dangerous or Serious?
All headaches are unpleasant and some, such as headache from medication abuse, are serious in the sense that if not treated correctly they might never go away. But a few headaches are indications of serious underlying issues. These are uncommon, in many cases very rare. Dangerous headaches often occur suddenly, and also eventually become increasingly worse over time. They are more common in elderly people. They comprise of the following:
Bleeding Around the Brain (Subarachnoid Haemorrhage)
Subarachnoid haemorrhage is a really serious condition which occurs when a tiny blood vessel pops on the surface of the brain. Patients develop a serious headache and stiff neck and may become unconscious. This is a rare cause of acute headache.
Meningitis and Brain Infections
Meningitis is infection of the tissues around and on the surface of the brain and encephalitis is infection of the brain itself. Brain infections can be caused by germs called bacteria, viruses or parasites and they are thankfully rare. They cause a severe, disabling headache. Normally, patients may feel sick or vomit and can’t bear bright lights, something known as photophobia. Often they have a rigid neck, too stiff for your physician to have the ability to bend the head down so that the chin touches the chest, even in the event that you attempt to relax. Patients are generally also unwell, experiencing hot, sweaty and overall sick sensations.
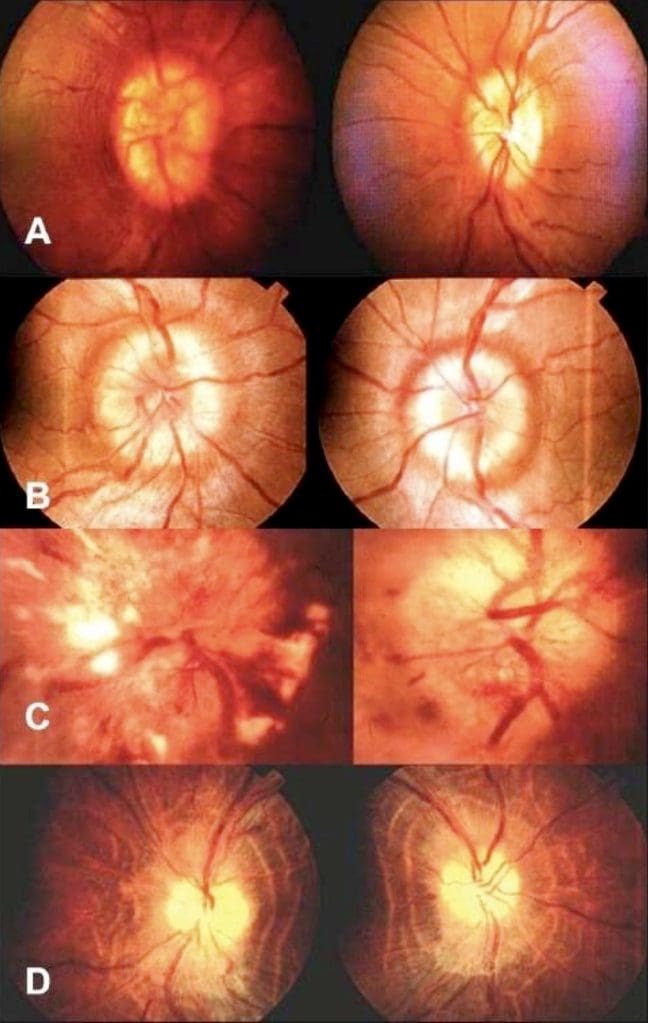
Giant Cell Arteritis (Temporal Arteritis)
Giant cell arteritis (temporal arteritis) is, generally, just seen in people over the age of 50. It is due to swelling, or inflammation, of the arteries at the temples and behind the eye. It causes a headache behind the forehead, also referred to as a sinus headache. Typically the blood vessels at the forehead are tender and individuals detect pain from the scalp when they comb their own hair. Frequently the pain gets worse with chewing. Temporal arteritis is severe because if it’s not treated it can cause sudden loss of eyesight. Treatment is with a course of steroids. The need to keep these steroids is generally monitored by the GP through blood tests, and they are typically needed for several months.
Brain Tumors
Brain tumors are a very uncommon cause of headache, although most patients with long-term, severe or persistent headaches start to worry that this might be the reason. Brain tumors can lead to headaches. Usually the aggravation of brain tumors exists on waking in the morning, is worse on sitting up, and becoming steadily worse in the day to day, never easing and never disappearing. It can sometimes be worse on coughing and sneezing, as may sinus headaches and migraines.
When Should I Worry About a Headache?
Most headaches do not have a serious underlying cause. However, healthcare professionals are trained to ask you about the signs and symptoms that might suggest your headache needs further diagnosis, just to make certain it’s nothing serious.
The things which would suggest to your physician and nurse that your headache may need additional evaluation include the following. They don’t mean that your headache is severe or sinister, but they imply that the healthcare professional may wish to do some additional evaluations to make sure if:
You have had a substantial head injury in the previous three months.
Your headaches are worsening and accompanied with high temperature or fever.
Your headaches begin extremely unexpectedly.
You’ve developed problems with speech and balance as well as headache.
You’ve developed problems with your memory or changes in your behavior or personality in addition to headache.
You’re confused or muddled along with your headache.
Your headache started when you coughed, sneezed or strained.
Your headache is much worse when you sit or stand.
Your headache is associated with red or painful eyes.
Your headaches are not like anything you’ve ever experienced before.
You have unexplained nausea together with the aggravation.
You have low immunity, for instance, when you have HIV, or are about oral steroid medicine or immune suppressing drugs.
You have or have had a type of cancer that can spread throughout the body.
Dr. Alex Jimenez’s Insight
Headaches are extremely common health issues which affect a wide range of the population around the world. Although frequent, a headache which is described to be like no other ever experienced before, may often become a concern. There are several types of headaches which can be caused by a variety of injuries and/or underlying conditions. As a healthcare professional, it’s essential to be able to determine between sinister or dangerous types of headaches and benign types of headaches, in order to decide the best treatment approach. By properly diagnosing the source of a patient’s headaches, both benign and sinister types of headaches can be treated accordingly.
Overview
Many headaches, whilst unpleasant, are harmless and react to a variety of treatments, including chiropractic care. Migraine, tension headaches and medication-overuse headaches are very common. The majority of the populace will experience one or more of these. Working out exactly the underlying cause of any headaches through discussion with your doctor is often the best method to resolve them. It is possible to develop a persistent or chronic and constant headache through taking drugs and/or medications that you took to get rid of your headache. Your physician can support you through the practice of quitting painkillers when that is the case.
Headaches are, quite infrequently, an indication of a serious or sinister underlying illness, and many headaches go away on their own.
If you have a headache which is uncommon for you then you need to discuss it with your doctor. You should also speak to your doctor about headaches which are particularly severe or that affect your regular activities, those that are associated with other symptoms, such as tingling or weakness, and those which make your own scalp tender, especially if you’re over 50 years old. Finally, always speak to a healthcare professional when you have an unremitting morning headache which is present for at least three days or is becoming gradually worse.
Remember that headaches are not as likely to occur in people who:
Handle their anxiety levels well.
Eat a balanced, regular diet.
Take balanced routine exercise.
Focus on posture and core muscles.
Sleep on two pillows or fewer.
Drink loads of water.
Have plenty of sleep.
Anything that you can do to enhance one or more of these aspects of your life will improve your health and well-being and cut back the number of headaches you experience. Make sure to seek the appropriate medical attention from a qualified and experienced healthcare professional in the event of a severe headache unlike anything you’ve ever experienced before. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Bulging disc is often thought of as a normal part of the aging process. It causes pain and decreases mobility. Athletes and people who have jobs that are very physical are often prone to bulging discs and other disc problems. Smoking tobacco can also be a contributing factor in spinal discs deteriorating and weakening. Chiropractic has been proven to be an effective treatment to heal a bulging disc and the associated pain.
What Is A Bulging Disc?
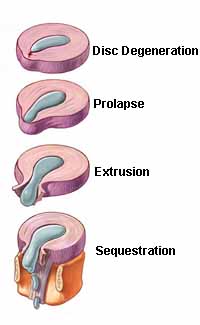
Bulging discs are often thought to be the same as herniated discs but that is incorrect. A herniated disc involves a crack in the disc�s outer layer. This is called an annulus. Typically, a small part of the disc is affected, allowing the soft material that makes up the nucleus pulposus to protrude. This is different from a bulging disc because, unlike a herniated disc, there is no crack. The disc bulges out of the space but it doesn�t crack and no material protrudes. It also affects more area of the disc than a herniated disc.
While a herniated disc is likely more painful, a bulging disc can also cause pain that can increase over time. Symptoms of a bulging disc include:
Tingling, numbness, or muscle weakness in one or both legs
Changes in bowel or bladder function
Hyper reflexivity in one or both legs
Paralysis below the waist
Deep pain over the shoulder blade or in the shoulder area
Radiating pain in the fingers, forearm, and upper arm
A bulging disc is often diagnosed by a combination of several methods. A physical exam, along with a full history of the problem will often lead to tests like MRI, x-ray, and myelogram with CT scan. From there, your doctor will work with you to find the best course of treatment.
Chiropractic To Help Heal A Bulging Disc
Chiropractic is a preferred treatment method for many patients with bulging disc because it is non-invasive and does not involve drugs or injections. Once you have your diagnosis, you and your chiropractor can work together to find the best way to treat your condition.
Your chiropractor will want to verify your diagnosis so you may go through questions about your medical history, a physical examination, and tests that involve nerve function, reflexes, and muscle tone. Your chiropractor may also order MRI or x-ray as well as other diagnostic testing in order to get a better picture of what is going on.
One of the most popular features of chiropractic care is the whole body approach to wellness. Your chiropractor will look at your entire spine, not just the area that is painful. They will treat your entire spine and provide self-care direction, exercise, and nutritional recommendations so that you can continue to progress and live pain free. Your pain and spinal problems could be the result of spinal misalignment so your chiropractor will seek to get to the root of the problem and treat your entire spine so that you have less pain, your spine can heal, and you have better mobility.
Through focused chiropractic adjustments, your chiropractor will gently use low force techniques to relieve the painful symptoms by manipulating your spine around and at the disc that is bulging. They may use other types of treatments depending on your specific condition and other issues that may be exacerbating your problem.
Chiropractic for bulging discs is safe, effective, and long lasting. If you are having back pain from a bulging disc, you owe it to yourself to seek quality chiropractic care so that you can enjoy less pain, improved mobility, and better quality of life.
Pablo Mena and his son, Pablo Alonso Mena, started receiving chiropractic care and physical therapy with Dr. Alex Jimenez and the trainers at Push after Pablo Mena (father) injured his lower back. Ever since Pablo Mena and his son started treatment and rehab, they have seen tremendous improvements in their overall health and wellness. Pablo Alonso Mena (son) has also benefitted from chiropractic care and physical therapy. Both father and son recommend Dr. Alex Jimenez as the non-surgical choice for lower back pain treatment.
Lower Back Pain Chiropractic Treatment
Chiropractic care is a medical profession devoted to the non-surgical treatment of disorders of the nervous system and/or the musculoskeletal system. Normally, chiropractors maintain an exceptional focus on spinal manipulation for surrounding structures. A number of studies have concluded that massage treatments commonly used by physicians are usually effective for the treatment of lower back pain, as well as for treatment of lumbar herniated disc for radiculopathy and neck pain, among other conditions. In reality, when patients with non invasive chronic low back pain are treated by chiropractors, the long-term outcome is improved by obtaining maintenance spinal manipulation.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine
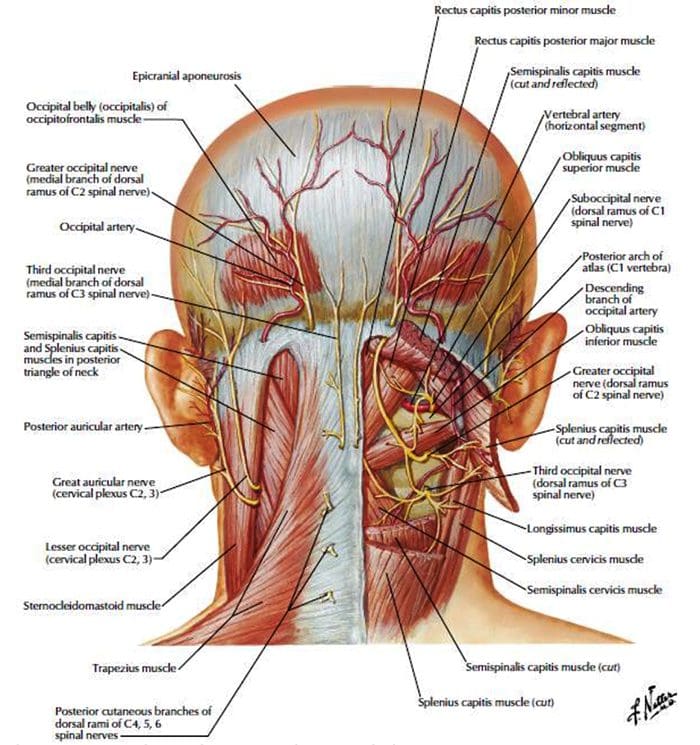 http://dailymedfact.com/neck-anatomy-the-suboccipital-triangle/
http://dailymedfact.com/neck-anatomy-the-suboccipital-triangle/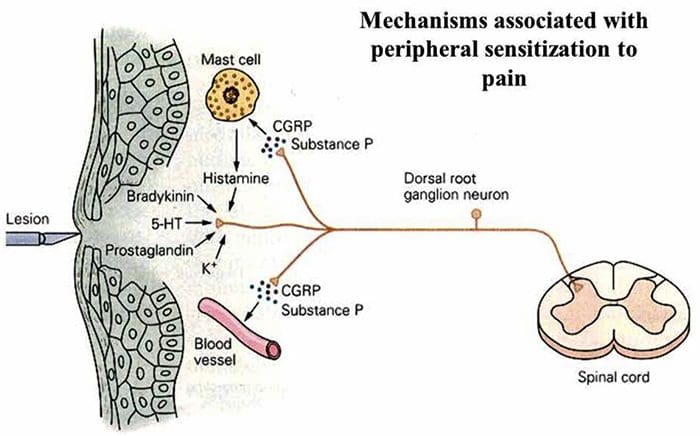





 PATHOGENESIS OF NEUROPATHIC PAIN
PATHOGENESIS OF NEUROPATHIC PAIN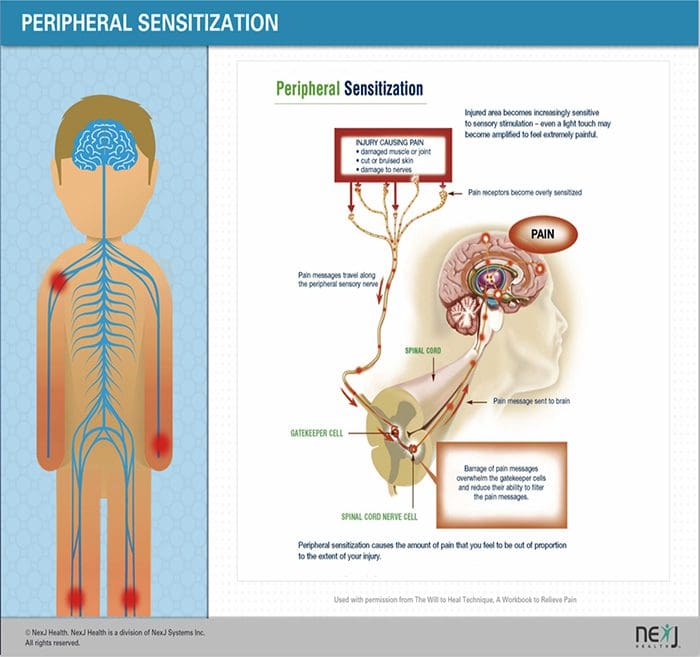
 COMMON CAUSES
COMMON CAUSES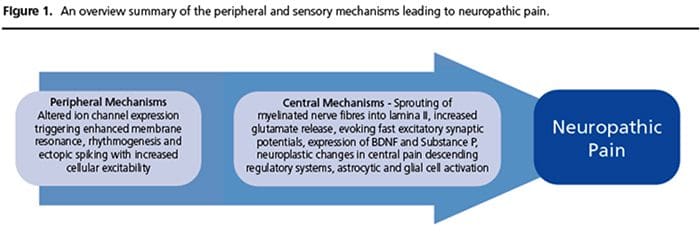
 PHANTOM LIMB PAIN & AUGMENTED REALITY
PHANTOM LIMB PAIN & AUGMENTED REALITY
 COMMON CAUSES
COMMON CAUSES