[00:00:08] Welcome to the Dr. J. Hour with our crew here and our entire staff. We’re gonna be talking today about basal metabolic rate, BMI, and BIA. What does BIA stand for?
[00:00:33] BIA is a bioelectrical impedance analysis. Right. And we’re gonna be talking about weight analysis and figuring things out. We got a couple of guests online. We have Alexander Jimenez. Which is going to come in, pop him in, please. Let’s hear and as you can see him here on the line there. He’s on the corner side of the HDMI. So on the HDMI, you can actually see him. Hey, Alex, how are you doing? Where are you calling from? Where are we getting in with you?
[00:00:58] I’m doing good. I’m calling here from Lombard, Illinois. And what is it you do, Alexander? Right now I’m going to school for chiropractic and ND, which is naturopathic doctor, kind of doing a little bit of a dual degree program here up north.
[00:01:11] All right. That sounds good. We also have on the line here we have Kenna Vaughn, who is the senior health coach over at our domain. We also have two wonderful individuals. We have Truide who is basically the director and the patient flow analysis individual. And we have Astrid, who is the chief editor at Injury Medical Clinic, where she writes and documents everything according to that. Can everyone hear okay? Yeah, yeah, yeah. All right. We’re all live. All right. So what we’re gonna be discussing today is the basal metabolic index. Okay. And one of the things that we do here is we’re gonna be able to assess the findings. Ok, so our goal today is to determine exactly what the primary assessment is and the assessment. So stay on me. Stay on me. You know you got that. And what we want to do is we want to see what BMI is and why is it useful? Ok. The main topics are what we’ve used to assess body fat analysis and determine the indications and the reasons…
[00:02:11] We use BMI alongside BIA, along with we got waist circumference variables allows also with waist-hip circumference variables and what it means because what we’re finding today is that these are great analysis tools that can be used to determine nature’s kind of a healthy cadence. It’s like blood pressure. We can kind of assess it. Then as long as we have other assessments and other evaluations, we can come up with a plan to kind of comparative. Now, all of them have their issues and we’re gonna discuss each one of them in the costs and what’s the easiest and most cost-effective methods that we can use. But one of the things that we can do is to see, why would we do this and what are the purposes. Now, there are quite a few reasons for this now in terms of it, what I’ve noticed is I’d like for you to, let’s look at the HDMI, we have the assessments here and we can actually see on the live the origination of this. We can see that there are different types over the history of BMI. We’ve gone from calipers that were just a method of measuring behind the arm, behind the waist, along with kind of in the thigh region. We would come up with a measurement of which we were probably about five to 10 percent away from accuracy. But in that process, even using those as long as you did use it on a consistent basis, you had a comparative accuracy and a method of kind of determining a change in your body dynamics and composition. It may not be accurate, but it was accurately inaccurate if that makes sense. Right. So what we did here is we’ve looked at here on our graph here. We have one thing that’s called the underwater way. But that was the standard. It is a research method. It is one of the most important things. And to determine actually what your body metabolism is we have to use things of oxygen consumption because that’s what determines the great spot of metabolism. The metabolism is controlled by the amount of cellular activity that is happening in the body. So calculating how much oxygen debt and how much oxygen use is a great way of researchers finding it out. But we don’t always have a laboratory that has I’d say, you know, one hundred million dollars of stuff and like a university. So it’s pretty much used in a research setting, the DEXA test, you may have heard it because it’s used as the clinical standard to look at bone density specifically on the hip side and the lumbar spine. We use that to determine things such as osteoporosis, osteopenia. We get a variable number and based on that number we can calculate the changes in bone density. There are certain types of medications we use to determine a better outcome for those that have estrogen deficiency. Some people have radical hysterectomy where they do remove all of both ovaries at a young age for whatever the reason is and the estrogen level is changed at that point a DEXA test every few years is determinable. The standard of care for the DEXA is one every two to three years after the age of about 50 to determine the changes in bone density. Now the skin fold that we just looked at here and you can actually, as I kind of draw it out, forgive me that I’m not drawing this, but we can actually see that the BIA and the skin fold tests are other tests that are easy to find, but as we discussed, are inaccurate. The Body Pod test, as you see here, you can see the cost of it, it’s about thirty to forty thousand. It’s extremely accurate and it allows for your body to relax. Each one of these tests has certain standards. One of the things that we have to do is prep for a BIA test or a BMI test. Now, the BMI is something that calculates an easy way of figuring out just height versus weight. However, someone like Alexander, you are how tall Alex? I am 5′ 8″. So a 5’8″ individual. How much do you weigh when you were at your deep competition and you were at your healthiest. Probably around 195 to 197. If you have a person that is 5′ 8 and 187 and I’ve seen him range from 210 and he’s still shredded as can be, he would be having a very high and he would characteristically show as minimally obese. Now you can tell that he’s not obese. So in essence, the BMI has flaw issues and bone density issues. Also, there are other disorders that sometimes fool you like sarcopenia, which is muscle wasting, and you wouldn’t be able to see the differences between those on the BMI. So what clinical assessments have determined is that the BMI and the BIA can be used together. But we have led a new technological world where we actually measure impedance. Impedance is kind of like the filtering or the kind of slowing of electrons or how fast and how quickly they go through. If electrons travel faster or something, there is low impedance or if it goes slowly through it or takes a longer time, there’s higher impedance or actually a lower flow, which allows us to understand that fat is not good a good conductor.
[00:07:03] So the more fat you have, the indirect relationship is, the slower the electrical current goes, therefore it’s less healthy. So using these electronic methods and what we have used in recent technology, we’ve used different companies such as Tanita, also InBody has an awesome system. We will be discussing those that assess the BIA in a way that it’s the most accurate if the most accurate is underwater weighing. And let’s give that relative value of 1.0 the actual BIA test are so accurate they are at .98. OK, so once we see that ratio, we can see that we’re the closest with the BIA test, specifically with an eight-point contact. Now any point contact means with your fingers, your palm of your hand, that’s two, both hands before. And then you have two points of the foot that can actually hit on each foot and that would be four from the feet if you can send that electrical current through the body. In that way, the BIA assessments such as done by the InBody design, we can actually determine a much more accurate assessment. So as we look at these tests, we can actually see what’s actually going on. So one of the things is we’re going to start looking at different companies and we can actually look at what a BMI is looked at. So BMI is used so you can look at it from a relative number. And it’s measuring kilograms per meter squared. And it’s measuring basically the height of the body, base of the body weight. Right. So the higher the number, as you can see, 25 to 29, you’re going to notice that the person is pretty much overweight. OK. I would venture to say that Alex would just because he’s in a situation where he would actually rate because he’s a much more muscular guy. He would not be healthy. He would basically almost reach close to 30 just because he has a large size and weight. But it’s clearly measuring only height and weight. So in order to determine the true health, that’s where the BIA and its bioelectrical impedance analysis, okay. Right. I should remember the words. So this is very typical. So one of the things is I like to show you here on these things, what kind of, Astrid, show a copy of what a BIA, kind of machine would look like. Okay. We have like here, here we have bioelectrical impedance analysis and this is what it looks like. If you notice, you’ll be able to see. And I’ll kinda take you through here and we can kind of see the ability to look at this particular region. You can see that the palm of the hand has one and you’ll notice the two points on each foot. What we’re missing is the final contact, but it’s eight and it takes only 15 seconds to be .98 versus one. Accuracy is a pretty efficient way.
[00:09:48] It also takes seconds to do this and not 45 minutes to do something like the Body Pod. So one of the things that we have to do is ask ourselves, why would someone do these kinds of things? Why would we do this? There are more accurate, more powerful ones, such as the 550 model, which we do not have in our office. And the model that we have is the 770 in our office. So you can see it’s much more accurate and we’re gonna discuss exactly what goes on. But one of the things we want to do is how could someone do something at home that is logical? Kenna, you got some thoughts on how someone could check out their basic health by doing some measurements? What are those measurements?
[00:10:25] Right. So one thing that’s really easy to do at home is gonna be to check your waist circumference, which is relatively cheap. You just need one of those flexible tape measurers you can get at the dollar store or it comes in almost all your basic sewing kits. And what you’re going to do is just gonna stand up nice and straight and you’re going to take that tape measurer, you’re going to want to make sure that you have no bulky clothes on. It’s best done just right on the skin. And you’re going to take it and you’re gonna fold it around where your belly button lies because that’s generally the largest part of your waist. So you’re just gonna wrap it around. You don’t want it to be too tight where it’s squeezing you or anything like that, because that’s going to give you inaccurate results. Take a deep breath in and on your exhale. That’s when you’re gonna get the best measurement and it’s best to do it about three times that way you make sure you’re really getting that accurate read.
[00:11:12] And what is that going to give us in terms of, what’s the circumference going to give us in terms of the assessment?
[00:11:18] What will we get from measuring our girth. That’s gonna help to see if you’re high risk for cardiovascular disease or type 2 diabetes. If you hold more of your fat around your abdomen, it shows that individuals are at higher risk for developing these later on in their life.
[00:11:34] Got it. Got it. There’s another one that we’ve used that most people can use at home.
[00:11:40] It’s a really simple one, which is that one? That one’s gonna be the waist to hip ratio. So you are going to start with that waist ratio that I just explained. But in addition to that measurement, you’re going to go ahead and also take your hip circumference.
[00:11:53] Alexander, one of the things that you did when you did your competition, when you were doing your stuff as a competitor, one of the things that you were doing is you were competing and weight was very important. Tell us what how that kind of stuff affected you and how could the BIA be useful in the world of, let’s say high-performance collegiate wrestling?
[00:12:15] So when it came to wrestling, there were a couple of different things that you just do to strategically approach the season, so the season is around six months. Most of the time wrestlers tend to gain weight in the offseason. So you do a couple of different things at the beginning of the season, they would have you use a caliper by a trained individual and they would measure your body fat and do a pretty much a calculation to see how much weight you could lose in a timely manner that was considered healthy for an average individual. And these individuals were allowed to cut a certain amount of weight within that time frame. So you kind of they pretty much gave you a plan of what you could and could not cut. I think the lowest I was ever allowed to cut was 184. And kind of just showing you kind of what’s going on here. So what they would do is kind of show you what your BMI is. I’m going to switch over to my screen here and you can kind of see just kind of just the reference ranges here. So below 18.5, they have underweight 18.5 to the rest of this kind of going into those reference ranges. And like Kenna was saying, they were doing an analysis depending on what type you had. So there’s a couple you have, your android, which is more of that apple-shaped and then your pear, which is gynoid. So they would measure for females and males completely different. So as your approach, you would either take a couple different dietary regimens and kind of approach to a different aspect of how you would go to cutting weight. So whether it was certain people did better just doing fats and protein. Some people did better just managing their carbs. Some people did better just lowering their caloric intake. So by having that BMI, you can see what your total calorie output for the day for living costs is a good way of saying it. So what’s the cost of living for every day for all your cells to function and what or how much exercise you would do. So most of us were burning between 1000 to 1800 calories between running in the morning or working out and then a two and a half hour to three-hour wrestling practice, which is all cardio intensive training. So as the month went on, we were allowed to cut weight and they would measure the weight that we were cutting at each tournament. So we were kind of scanned in, in a way to allow for us to cut weight correctly. One thing that they did start implementing when I joined, when I started wrestling in high school, was morning weigh-ins, which prevented people from really cutting weight the wrong way and not having a good benefit, because before you could cut all this amount of weight and you’d still have a 15, 16-hour window to replenish all those glycogen storages and gain 15 to 20 pounds depending on how dehydrated you are. So it was not a very healthy approach to cutting weight in that sense. So now with everything that’s going on, athletes are training smarter.
[00:15:01] They’re cutting weight better. They’re managing pretty much themselves a lot better in that aspect.
[00:15:07] So this is a great example of when you use these assessments. I remember as we’ve done a lot with the wrestling, one of the way that the university got involved and they do BIAs for people, but for the athletes, they start them out with the standard specific gravity test and that’s a urine test to determine which protein is within their urine. Also, there are electrolytes such as potassium, sodium, calcium. If the person is highly dehydrated, what happens is the specific gravity rises and they also measure specific gravity. In the beginning, it’s something to be able to measure. And we can say that the kid who weighs 200 pounds, his specific gravity is a certain amount. Right. So we don’t want a kid cutting down with the specific gravity of their body concentration. Blood constriction is too high because that means they’re dehydrated. Those individuals can, once we got that number, we can assess the person, not just with body weight, but we can use BIA to follow them through the season in a much more accurate way. So that allows a very expensive test, which is a specific gravity to go through the BIAs. We also have issues and we’re going to touch upon these. But there are other special dynamics that parents can be involved and parents like Truide, you’re a parent of an athlete. What would you want to know in a BIA?
[00:16:22] Well, I have two athletes. Well, basically, I guess at what point is it safe with children to start watching, you know, and being concerned about, you know, BIA? Because certainly as young adolescents, you don’t want them prone to having eating disorders or being so self-conscious about their body composition that then you have other types of side effects of psychological approaches. So that will be one of my concerns. When is it safe from a parental stand to be watching about BIA and BMI?
[00:16:59] You know, that’s a very good question. And I guess what we would want to know is that we know that our kids are healthy when they’re with us, but when they’re going through certain dynamic changes. We want to follow up. We want to see when is it getting too concentrated? When is the kid losing too much protein? When is the child running the risk of hurt because we do have the stories of the 180 pounder cutting down to 135. That individual is not only running themselves at risk. But in the world that they’re wrestling someone, their own body weight, they’re running the risk of being injured. So as a parent, I see that very important. The BIA offers us the ability to be able to quantify and to see the measurable changes as the child goes through the process. Now, if you can look at these areas, now there are other areas. And one of the things that we have here, our chief editor has found out some really interesting dynamics, specifically how assessing BMI actually has other consequences and things that we can assess for those things. Astrid, one of the things that you’ve seen in the process when you have gone through the process, tell us a little bit about what you’ve found out about the BMI and BIA in terms of brain health.
[00:18:09] OK. So there are actually quite a few research studies that have been conducted on pretty much the importance of BMI and BIA and why it’s, you know, we all want to know these, I guess, these values so that, you know, because obesity or having excess weight, you know, which you use BMI and BIA to determine, you know, it can affect a variety of functions. And like you said, research studies have actually found that obesity can actually affect your brain health. And there’s actually like probably one of the biggest things like there are several things that obesity, can affect brain health because it increases inflammation in your body and it could even speed up the neurodegeneration process like your brain ages a lot faster.
[00:19:09] Wait a second. Wait a second. So, it actually makes your brain kind of lose its intelligence.
[00:19:15] I wouldn’t say it makes you lose your intelligence. It just makes it work slower. Slower. Yes. Ok.
[00:19:21] So brains that get smaller. Or let’s say dementia. Well, let’s say the brain becomes, loses its size and dimension.
[00:19:29] So those things we could, are correlated to BMI as well.
[00:19:34] Well, you want to know your, it’s important to know your BMI or your BIA.
[00:19:39] You know, interchangeably like depending on what would it be more important to know or the person? Because like research studies have found that if you have excess weight or if you have obesity, that it can actually change the size of your brain and it can decrease or just alter the gray matter and the white matter of the brain and that can age your brain a lot faster and it can slow down your cognitive functions and it can even affect your memory. And you’ll have a harder time remembering things simply by having excess weight.
[00:20:25] I read something today that said even dopamine is affected by, the production of dopamine potentially is correlatable or associated with BMI values.
[00:20:36] Ok. So what scientists have found is that if you have a lot of excess weight, you know, if you’re overweight or if you have, you’re a person with obesity.
[00:20:49] The thing is that.
[00:20:52] Excess weight or obesity, it can go as far as affecting what’s known as your pleasure and reward center of the brain. And that is, it’s pretty much the region of the brain that controls the release of dopamine. Just being like having obesity in itself could even cause your brain to release less amount of dopamine. And that can cause a variety of mental health issues. And it could even lead to depression just by having excess weight.
[00:21:26] So BMI, you know, let’s pop it up first to Alexander, make his screen bigger, let’s go to the HDMI. He’s noticed some things here. Alex, can you tell us a bit about what you’re actually putting up on there?
[00:21:36] Perfect. So you guys can see my screen right there? Yes, we sure can. Awesome. So like Astrid was saying that adipose tissue does have an effect on certain things.
[00:21:46] We have to take a look at adipose tissue at the cellular level. Normally, adipose tissue, large amounts in certain areas were meant for producing hormones and not all adipose tissue is created equally. So we could see that, here’s the average individual that would have what people call a beer gut. And here’s the pear-shaped as what a normal individual would have as well, for most females. So we could see that we have pear, which would be gynoid, and android, which would be apple. But we could see that males who tend to have these tend to produce a little bit more estrogen, affects the males differently. We can also see the ratio of significant health risks. So males have a 95 percent increase in percentage for developing other health risks while females are different. Now, when it comes to losing this type of way, we have to keep in mind that not all adipose tissue is created equally, as my professor likes to say. So we can see that even though we have the same amount of adipose tissue in both areas, they’re in completely different areas.
[00:22:48] So most of the time you’ll hear the saying that some women have trouble losing weight, which is correct because of their adipose tissue located in different areas. It’s not as metabolically active, which is good for them because they don’t produce as much hormones from it. They don’t get much stress from it. Now, on the other hand, the visceral fat releases hormones and this is the one that is problematic to individuals but can also be reduced a lot quicker. So when you’re kind of coming down to the breakdown of the main macromolecules of the bodies, we could see there were 5 percent minerals, calcium, 15 percent fat, 1 percent carbs, and 60 percent water mostly. So we can kind of see what the reference ranges are here for the reference man aged 20 to 24 years and the reference woman 20 to 24. And coming back to Mrs. Truide when she was mentioning what is the safe and recommended way? Well, it’s hit and miss. It’s different from males and females. For males you want to keep anywhere between always stay above 3 percent body fat, anything below that becomes detrimental and your body starts to break down. But for females, on the other hand, we can see that once they start dropping below 15 percentage, they actually will miss their period if it drops below that. So if a female athlete or a tri triathlete does this, it will, honestly. So there’s been cases where female athletes develop osteoporosis just because they produce less estrogen, only because they drop below that 15 percent body weight. And females need more adipose tissue than men. It’s just the way we came through evolution and we were designed and it’s just the way it is and needs to be. So for females, as long as they’re above 15 percent body fat, they’re always gonna be healthy. For males, it’s a long as long as it’s above 3 percent, they’re always going to be healthy. It’s very hard to attain 3 percent for males, but as long as they usually stay between this, you can kind of see what body masses, lean body masses muscle on kind of the breakdown of everything from there.
[00:24:48] Answering the question regarding Truide’s particular question, cause that’s the bottom line is, what is the 25-year-old mom? What is the mom that’s 27, 28 years old with a five year old little boy, with a 10 year old little boy. What is she got to do? Go ahead and put up the 550 up there for me. What we’re looking at here is we want to be able to quantify these things. And one of the things I’d like to show you that is available in today’s research is the ability to determine certain things. Body composition analysis takes a lot of different studies and a lot of different dynamics in its research. We’ve been able to look at questions that are more specific for someone like Truide and her child to be able to assess the variable changes, body composition. And we’re going to follow up with the follow up videos discussing this particular issue. But the studies today, we can actually see in this particular area that we can assess muscle body fat analysis and the ranges versus the total body fat. We can look at obesity analysis and we can measure the ranges, Ok? We can look at percent body fat. We can look at extremity segmental lean body analysis versus one arm versus the other. This particularly comes in and true because let’s assume someone has an ACL injury on the right leg or left leg. You’ll notice that there will be a variation of body mass changes and to be able to determine if the body protein in that leg is getting more developed, in a leg that has noted atrophy there will be obvious changes in terms of the amount of protein or the amount of difference in percent body fat as well as water retention in that area. If someone has a swollen knee, you can also see the difference. Now the total area and the body weight, we can start measuring and just start noticing this. This is what helps mother Truide’s around the world understand the continuous. You’ll notice down here on the bottom that there are reference dates here where we can actually see the changes as time goes by. And once you see the changes as time goes by, it gives you a lot better tools. Now, the other thing that we’ve noticed here in terms of this particular area is the awareness that we can actually do visceral body fat that Alexander referred to. We want to be able to see what is inside the body. Now, visceral body fat is if you open a body up, there’s fat that surrounds each area, like the liver, the intestines. We call it the peritoneal area, Pernille, area that basically holds the body fat and holds the amount of tissue to protect it. And that’s how nature has done it. But we want to know how much it is. And if it does produce hormones that are bad like cortisol or produces hormones, that we know about that for a different video, we can see that that would mean not good. So the person with fat that’s around the viscera is at higher risk. So that analysis and to be able to give a point and see the changes is very important. So one of the things is that we can do. And as we talked about here, you can actually see the impedance by the individual depending on which extremity it is. So the tests on a regular basis, those simple as that may be standing on a thing. They’re very complex and very accurate. So it does bode well for someone that really needs it, that has a family that is going through these kinds of techniques so that we can reassess. Initially, you can start someone with a, to be real detailed and to be accountable to the individual by specific gravity to determine the concentration of body, metabolites in the body, and the proteins, and the level of dehydration the person may have. Then you can follow up with a BIA repetitively through the history of a season and you can really get a lot of information as to how your child is going if it’s a healthy form of weight loss. So, Alex, I notice that you put up some things up there. Can you open that up? And you’re putting up some interesting dynamics there. What is it that you’re noticing there? What did you put there?
[00:28:32] So we can see that these are some of the graphs that I just got from classes here so we can see that correlation is not cause for causation, but it does correlate to the data of many individuals. This was taken from a study. And what they found is that people with a higher body mass index tend to have a higher risk for certain diseases, such as cardiovascular disease or cancer or all other causes, just illnesses in general. And we also have to keep in mind that women do have more receptors for those hormones produced by adipose tissue. So they are more susceptible to cancers. So we have to ask ourselves, what is the point of, you know, losing weight besides just the cancer thing? So we come down here, we can just see the correlation of the lifestyle of individuals just if they lose 10 percent body weight. So if their obesity is decreased, their life expectancy increases for about seven years. But not only that, but you can see where the circle of lifestyle changes for this individual who not only begins to change their lifestyle but also operates those healthy choices into their daily environment.
[00:29:42] Makes sense. So these are very, very important things to assess on a regular basis. So what I’ve learned is the BIA, BMI, in general, is a very important method to be able to assess the overall health and the progression of health. So we want to get a better BMI and we want to get a better, be able to assess the regions of the body and to assess the dynamics of what someone can do to monitor their true health. We’re going to be following through with follow-up studies and the follow-up information and on these follow-up programs to teach about what we use here in our little town of El Paso, which is a big town. But we’re gonna be bringing families. We’re gonna be bringing athletes to discuss those things. We’re gonna get real technical right on the screen right now. We have a real interesting dynamics to the level that we’re gonna be pushing the knowledge of. Can you pull back to the screen? You actually can see it right there. You can actually see biochemistry. And we have our resident and biochemistry expert right there. Alexander, tell us what we’re looking at there.
[00:30:46] So here we’re kind of going through the synthesis of cholesterol and what it takes to actually produce cholesterol. So it’s kind of a very complex pathway. But we can also see that it takes your body a lot of stress to really produce high cholesterol levels as well as cortisol levels. So kind of coming into the main breakdown of what kind of goes down, if you have a very increased dietary cholesterol intake, not only are you putting more stress on the liver, but you’re also increasing more LDL. LDL just tends to be bad in general because the LDL is…
[00:31:23] I’m sorry, Alex was is LDL?
[00:31:25] Low-density lipoprotein. Got it. So the problem with the low-density lipoproteins is that their main job is to drop off the correct cholesterol to the proper levels. Now if they turn into LDLs, the problem is that if they don’t get reabsorbed by the liver or a good way, I think of it as, they are thought of as a suicide bomber. Pretty much so. What they do is they deposit. If they don’t deposit and don’t get absorbed by the liver because the liver is being bombarded by too much cholesterol, they will actually deposit themselves into other tissues, specifically the epithelial lining of the extracellular part of capillaries. Then at that point macrophages will actually try to eat them up and create these things called foam cells. Foam cells tend to aggregate and they’re really large cells that have no purpose other than to aggregate within the layers of the capillaries.
[00:32:24] Is that what the protective mechanism, is that what the body does?
[00:32:27] It pretty much just tries to seal it off so it can’t affect anything else. But in doing so, it clogs arteries.
[00:32:33] Okay. So BMI would be able to determine the overall health of the body and fat. So it would tend to, we would tend to say that a person with a, let’s say a high BMI, extremely high BMI and the obese level would have more of this action happening. Right?
[00:32:49] Exactly. But we also have to take a look at a different thing. So let’s say this person is already morbidly obese and their cholesterol is high. So they go to an M.D., their M.D. gives them a statin. So statins are good to an extent. So, yes, they’re going to decrease the level of cholesterol, but they’re also going to decrease. See if I can find it here. The levels of all these other hormones being produced because cholesterol is the driving force for all these hormones. So if you are decreasing your cholesterol, you are decreasing for women their progesterone for men, their testosterone, their dihydrotestosterone was kind of what people describe as the old man’s strength. As you get older, you produce more DHT, but you’re also decreasing these. Not only are you decreasing cholesterol, but you’re also decreasing by 50 percent coenzyme-Q. Coenzyme-Q it was the main electron transporter for the electron transport chain and it transports electrons that certain parts in the pathway which we won’t go into. But if you decrease that by 50 percent, most of these people feel tired all the time. And what’s the tissue that has the most mitochondria in the entire body? Muscle. The heart. Oh, okay. So the heart. So not only are they decreasing their energy levels, they’re decreasing the ability of their actual lifeline, pretty much, their heart to produce and pump blood and get energy. So by just decreasing body weight, decreasing cholesterol intake in a moderate amount because cholesterol is good, we need it for everything. Too much of one thing can kill you, though. So within moderate amounts, exercise, dietary regimens, you won’t need to be put on statins and you can be weaned off of those in time as your cholesterol levels get to an appropriate level.
[00:34:37] That’s amazing, Alex. So that’s at the microscopic level. At the macroscopic level, we can assess that by visceral fat. So the more visceral fat you got, the more hormones you got going haywire. And it’s fair to say that we have a situation where you’re less healthy with visceral fat. Ok. So does anyone else have any input in here? Any other questions that you would want to know about Mrs. Truide as a mom of athletes?
[00:35:02] No, I guess just the woman on a side note, if all of this is very complex. The bottom line is if you’re having to lay down in your bed to tie your jeans, you’re not having a healthy BMI.
[00:35:14] That’s very true. Right. So basically, if your gut hangs over, you’re in trouble, right? So that’s where you can use the simple tests of the waist circumference or the waist-hip balance. And if pretty much the belly is three inches bigger than the hips, you are probably at a BMI that you shouldn’t have. So I hope. OK, go ahead. Astrid, you want to say something.
[00:35:36] So essentially, it’s just super important to find out your, I guess, your BMI or your BIA interchangeably pretty much for overall health, because just having excess weight, as we’ve found out here, it can affect a whole variety of functions. Brain health, cardiovascular, health, and finding your BMI and your BIA seems like such an easy, you know, like an easy way to kind of find out if your weight is like at a healthier range. And it all kind of goes like hand-in-hand with all these things, as you’ve explained and as Alex explained. Pretty much like being, having obesity or excess weight, it can just disrupt our entire body, our entire system.
[00:36:37] Exactly. Kenna. Any other comments in terms of specifics on questions?
[00:36:43] Not for questions, just for that waist to hip ratio. We’re gonna want to make sure that for women, they’re under one. And the same thing for males. So you’re gonna divide your waist by your hip ratio to get that number. Right.
[00:36:58] So the numerator hopefully won’t be too bigger than the denominator, right? Yeah. So that would be the numerator would be the waist and the denominator would be the hip. Right. So we want to keep those in line. So all those kinds of things are very important. We’ve learned a lot today. We’re going to come back with a much more elaborate and we’re gonna splice this up in many ways. I want to thank Alexander for coming in from Illinois at the National University of Health Sciences way out there. This probably about 2000 miles away. We have Truide, Mrs. Truide who’s giving us a point of view. We have Astrid who’s given us the scientific approach of the brain and dopamine connection. But we also need to know that there’s a lot of reasons why the BMI. As we learn every day through the NCBI research institutes of information, that there are lots of reasons why to keep a BMI low and also to make sure you watch your BIAs in time. So we look forward to bringing it to you. And we thank you for watching us and we look forward to giving more information. Alexander, thank you so much for coming from a distance and making it real cool for us all.
[00:38:01] Ok, thank you. Thank you for having me. You’re welcome. Appreciate it. Thanks.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
[00:00:10] You know what keeps them moving and growing and living? Tell me. It’s other catfish or that predator. So, if we never had predators in our lives. We’d stay stuck and we progress nothing. So every time we ask, “God, take away the stress, God, take away this issue,” we’re asking God to make us weaker, not stronger.
[00:00:33] Because instead of asking like, “Hey, God, make me more creative, make me more passionate, make me more patient”. We ask, “Hey, take away this”.
[00:00:45] But then we still want everything else that comes along with it. How does that work?
[00:00:49] It’s easy. I don’t know. I mean, if you think about it, you know, from the first time we’re born, Danny. It’s not easy. Right. You’ve got to be one in a trillion sperm, really, and only to God, it’s very, very clear that, if you don’t get to that egg first? Done. Right. You’re done. So from the moment we’re given a chance, we’re on the point of destruction from the beginning. Exactly. So, in essence, why did that sperm get to that egg? Right. So you asked. It fought through. Fought through, right.
[00:01:27] So, when you think of everything else as far as people complain, how people say, “oh, you know, I want more money, I want this”. But they don’t look at everybody’s backstory, the back end. And then behind the curtains, they think, “oh, man, Dr. Jimenez, you’re a doctor”. Sure, you don’t know how many times you’ve lost and rebuilt your practice or you’re a gym owner and you have it made. You don’t know how many times you have to go in at 4:00 in the morning to get a work out because you have to train people all day long to ensure that this business stays afloat. You know? Right. People don’t see that back end. Right. You know, they’re quick to say, “oh, it must be easy”. No, it’s not easy until you step into the person’s shoes because you’re the one that has to sign the checks. You’re the one that has to stay up at night and figure out payroll. You’re the one who has to be creative and figure out how you’re going to make ends meet. You’re the one that constantly has to be on it. You know, as much as you want to kick back and say whatever and do this. Well, I would love to work out four to five hours a day. That my passion. Is it your passion? It’s my passion. And do we? No, no. Right. What do we have to do? We have to be meticulous. We have to be disciplined. And we have to keep, I’m sure, we have to keep a proper order to ensure that we stay on top of schedule. Yes or no? Absolutely. Exactly. You know, so I’m saying at the end of the day is, if you don’t have something chasing you, you become fat and dormant and you become lazy.
[00:02:54] I think nature is designed to eliminate you. Alex would say, you know, it’s survival of the fittest limiting the species or whatever he’d call it when he’s in biochemistry. You know, I got to tell you, it’s not easy to be a business owner. It’s not. It’s not easy when you have no sleep.
[00:03:15] Ever since I’ve known you, you’ve put time in from early hours and you’re here from 430 in the morning and here. What time is it now? You’re here. You’re here. And we’re here sharing some stories. You know, it’s one of those things where it’s going to be nonstop all our lives.
[00:03:29] But here’s the thing. If you don’t do it, it doesn’t stimulate you to become good at what you do. Right. You become lethargic and everything goes bad. Literally, you slowly begin the process of ceasing to exist. Right.
[00:03:45] So, we all need rest. Right? Right. To rejuvenate. Get creative. It’s scientifically proven. You need that to reset. You have to. Otherwise, you burn out. Right? Right. But after how many days of rest? One. Two. Where you just get, disconnected, spastic. You know, you’re kind of like, “All right, cool. I rested enough. I’m good”. You don’t stay stuck there.
[00:04:12] No, no, no, no. And I pray for vacation. Right. And when I get it, after about three days, I’m like, OK. Right. All right. I’m done. Let’s go. Yeah, OK. What am I going to break? What am I going to do? That’s how we are. Exactly. But that’s what makes you so successful, right? Yeah, well, it drives us. And it drives us in creating who we are. And it also gives us a vision as to what we’re going to do. You know, Danny, when we start these podcasts, we want to get a little bit or tell the people a little bit about the story of what you do. And tell them about, you know, where you’ve been and what’s been happening with you. OK. So for me, it’s very important to share with the people what is actually happening.
[00:04:59] I’ve always been one to say, you know, I see how hard you work. And I see how much effort you put into things. But I’d like to know a little bit about you as to what actually made you and what kind of makes you click a little bit. When I actually discuss these things, I want to ask you what made you begin PUSH, what made you start this massive, massive organization.
[00:05:25] I want to reach the masses of people and help people.
[00:05:33] So, in all reality.
[00:05:39] My sister, my brother-in-law, my brother. We’ve all come from platforms, as far as, speaking, preaching, singing. Whatever it is. I was always, kind of the black sheep, so to speak, and I mean that like in a good way because I wasn’t treated differently. I just was very much a rebel. If that makes any sense.
[00:06:00] I wanted to create my own. So if my family went right, I’d go left. The people go right. I’d go left. I was always trying to find a different way. And I was just stubborn like that. But I think that’s what allowed me to become the most successful. But that’s what allowed me to create this place so I can reach the masses of people and have my own platform of changing people’s lives.
[00:06:23] Let me ask you. When you first started PUSH. What was the reason you started it out? You know? Did you? You were always in the fitness. Ever since I’ve known you, you’ve always been into a deep understanding. You know, I love sharing that story with people about when I first met you. You were driven. I mean, you were this kid, it’s just like you were hunting for knowledge. You were trying to figure out what it was that made people tick. And you wanted to teach people. A little cocky. I’d say. But being 18 years old, I mean, who isn’t? Right. At that age? You haven’t even thumped in the head a couple of times, but you did and you shared it with people and you did that. But what made you, what drove you? Because I got to tell you, I’m a big believer, Danny. About like, when you evaluate families, I see how hard your dad works. I see how your mom is incredible in terms of what she does. She just, she wins these crossfit competitions just on mere, literally, you have to turn off the lights to get her off the wall because she just keeps on going. Right? I mean, what is it that you feel drove you and what started the whole philosophy of trying to help people out?
[00:07:32] I mean, like you put it, in my my parents work ethic. They just never stop. They still don’t stop. They still try to move forward despite what life throws at them and they’re successful in their own way. They never stop working towards their marriage, towards their love, towards serving each other. The biggest thing they showed me is that, well, we always have to serve people and they serve each other. They serve at the church, they serve wherever they go. My dad, it doesn’t matter where it is. He’s always trying to, if it’s not your house. It doesn’t matter. Try to take out your trash, clean your table, whatever it is. You’ve got to tell him, “Hey day, just chill. But that’s where I learned it from. You don’t just go anywhere and just be. Wherever you go, you always serve. And that’s my sense of faith mentality. You know, it’s biblical. You know? Wherever you are, we are supposed to serve people. As husbands and wives, we’re supposed to serve each other. That’s what makes us so successful. You know, you look at Jesus in the Bible and he’s, “What do you do? You serve people.
[00:08:44] He helped people.
[00:08:47] Not the norm. The most unorthodox non-religious people, you know, other people that needed the most help, not the most religious. And I think that’s what I love to do. I love helping the people that need the most help. The unconventional. Not the people that are already athletic. I mean, don’t get me wrong. I do love helping them, but I guess I like helping the unorthodox, so to speak.
[00:09:17] Yeah. You know what? When you mentioned that about your dad, one of things I noticed is that I came here to work out around 6:00 in the morning and it was freezing outside, literally freezing.
[00:09:29] You had a flat tire. Your dad was lifting the car by himself to get that tire up. Yeah. It was crazy. I go, you know, by the time I got there, I was like, there’s this guy working on that. There was no jack. He’s actually picking up the car himself. He’s pushing that thing up and lifting the car to fit the tire on. I was like, you gotta be kidding me. You didn’t even know. I told you and you go, man, my dad never asked or, you know, he just does it. That’s one of the things you said. And that’s who we are. We are our parents. We eventually become our parents to some extent. And that’s very much how you are. Your philosophies that have guided the PUSH fitness, you know, entourage and the people that come here have been like extreme athletes. Tell me a little bit about that. In terms of what actually drove you to pick athleticism as your way of serving.
[00:10:20] I think seeing the potential of.
[00:10:24] Well, what people can be pushed to if you believe in them. A lot of times people, you know, do believe in themselves but it’s amazing what you see people become or individuals or athletes when you say, hey, I believe you. Someone that, not your mom not your dad, because it’s kind of like, it’s expected, sister, relatives, you know. And you know, not that they have to tell you that but, you know, it’s kind of sometimes expected. Yes, exactly. But then you have this stranger saying, I believe in you genuinely, wholeheartedly. And it brings out that much more of you. I know. That’s how I was. I still remember various times where you tapped me on the shoulder and said, you know.
[00:11:15] What are you doing? You can, and I’m very different.
[00:11:20] I don’t need someone to preach to me. To tell me how to run the place it’s kind of like a little, just a little hug. A kick, a get going. And that gets you going to move on to the next level of the mountain. And that’s what allowed, that’s what I love seeing as a potential that you could bring out in all individuals. When you see that pretty much you’ve been able to see everyone crack.
[00:11:45] What is it you look for when you see them kind of hit that wall? When you start working with an individual with a specific set, whatever sport they’re in or whatever their dreams are, a weight loss or whatever it is. What is it you look for?
[00:11:59] To see the reason why they’re quitting. They’re genuinely tired or have they’ve been?
[00:12:07] Babied so much by society that they don’t know how to push themselves anymore, and it’s really a sensitive society nowadays you can’t, you know, push kids because they get their feelings hurt or they feel this way or that way, and sometimes it’s like.
[00:12:25] Dude, you got to wake your ass up.
[00:12:28] If not, you’re not making it in this life. Nothing comes easy. And then we’re all expecting for things to become easy because we’re, you know, a microwave generation, everything we do we want to do so quick. So I look for the reason as to why they’re quitting. This genuinely like, the why, they’re tired and they’re gonna throw up. Oh, alright. But you remember firsthand when I worked out with you, I went to go to the restroom, threw up. I came right back. Why? Because it’s what you build with that person, that respect. You know, why would you want someone to quit on you when it gets hard, you know? Yeah. That’s exanctly right. How are you gonna count on them. I know you depend on them. No, when it gets tough. You know, they’re just gonna jump the wagon. That’s it. You’re left alone.
[00:13:18] You know, you’re given a responsibility, a huge one, with a lot of the El Paso kids in whatever sports they do, in whatever the sport, whether it be agility sport based or just some sort of sport based system where where they’re just kind of, you know, let’s say hockey or even things like tennis or golf.
[00:13:37] But they all have a moment of trying to reach within. I love the way you do that in terms of, you can go ahead and see the depths of what is wrong with them and you can actually connect with them like no other. I’ve seen that every single time, my own kids too when you train them. You asked why? So really like that boats to the point? No one cares what you know. They care that you care. And that caring really allows them to open up, huh?
[00:14:04] Right. Yeah, definitely it does. You know, it makes them see like I do have it in me. I, you know, need to quit babying myself. Right. And I need to get up and get after this because no one’s gonna give it to me. I gotta get up after it and work for it, period.
[00:14:20] When I would tell my daughter, when they would come in, I’d say, you know what? You know, I’m not coming and, you know, I’m not going today. Right. I’d say, all right let me call, Danny. No, no. They’d feel like they have a, well.
[00:14:34] They sense the obligation that and the trust that you have put into their hearts like no other. Because that’s what they want. They want someone to believe in them. Exactly. You know, push them. That’s why the push. Push. You know, there’s the added edge of the push. You know, these are very important points. What got you into, do you have to deal with, like the mind-stuff and like work? How do you work on developing a child or working them through their own mental impediments or their own mental kind of dynamics to make them better of who they are? If that makes sense.
[00:15:13] You have to build a foundation with them first. You have to build trust with them. You can’t just go in and yell at them. Hey, let’s go, let’s go. Like, move your ass. Don’t be a little, bitch. You know, you can’t just do that. You have to build a relationship first, have them trust you and have them understand why you’re pushing them. And then when they’re at the brink of giving up, you yell at their ass and they know why you’re yelling at them. A good parent, after they discipline their kid or ground them, they’ll tell them the reason why they did that. But they don’t stop loving them. They appreciate because they know they’re wrong.
[00:15:48] Same concept here. Obviously I don’t hit them. But I do yell at them after they know like hey. Yeah, I was sucking and I need to stop feeling sorry for myself and get after it. Right?
[00:16:01] You know, in my own experience with what you did. You know, you have a lot of moms watching you train their kids. Moms are really sharp. There’s nothing smarter than a mother in this world. Right.
[00:16:14] And they intuitively understand and they feel the depths of the change in the child. Right. So when they see the depths of the change in the child, they trust you. And this is in mass because I have like a whole wall of families of moms, dads. They bring their kids no matter what. Tired, cold, sleet, rain, snow. They bring their kids here to train with you and the entire crew with the philosophies of pushing to those limits. You know, how does that feel when you see those kids, you know, kind of, excel?
[00:16:54] Proud.
[00:16:57] Completely, pretty much over the moon because you see the hard work that you took to instill that time into them and make sure their full potential came out. So it’s well, it’s rewarding. It’s inexplicable.
[00:17:11] Let me ask you this. You’ve been now, you know, you’re not young, like 16 years more. You’re in your 30s, which is a very young age. However, you’ve lived long enough to see some of these kids go on and do their their thing.
[00:17:27] Tell me how that feels in terms of you watching them develop, in terms of who they are and what they are, what they develop because of the foundation or at least influenced by the foundation of just don’t give up and keep on pushing through it. How does it feel? What do you think?
[00:17:45] It feels very, in a lot of sense, a lot of pride, because you can see what they could have been and what they couldn’t have been. A lot of times some kids do come from poor or poor extremities. And so to see them excel, believe in themselves, to go to college, to get a successful job, to be something of a higher profession, that other wise they thought they couldn’t build or settling for less and not letting them settle for less is really amazing. It’s of most, that’s why I keep doing what I’m doing.
[00:18:26] These kids keep on calling you? They talk to you personally?
[00:18:30] Yeah, they do. They still kind of keep up with me as far as like what they’re doing, how they’re doing, the’ll come in work out. Still, you know, to chat with me, everything. It’s fun. You build that long lasting relationship.
[00:18:43] If you could come up with a couple of words vindicating what makes PUSH unique and you can look deep inside your heart and figure out what it would be. Say you were to had an obituary being read about you. What would they say about PUSH and you? What would you want them to say?
[00:19:04] Honestly.
[00:19:06] That they have somebody other than their parents believe in them.
[00:19:11] That’s amazing. That’s really a huge component to everything that’s going on. When do you think someone should actually be coming out to this place and enjoying the kind of lifestyle that this place, you know, helps enhance their lives with? When is that time?
[00:19:29] Whenever. Whenever you want to be a better version of yourself.
[00:19:33] Ok. Ok.
[00:19:34] What do you think people sometimes think about, you know, why shouldn’t they come in? What should not be an impediment? Of them coming in here?
[00:19:43] Their image, that they can’t do it. That they’re not athletic enough. That they’re obese. That they have any problems, low back problems. That they look foolish. You know, the whole thing is that at the day, we all look foolish to one extent or another.
[00:19:56] But the point is that if I always assume what others thought and paid attention to how I felt, as far as being embarrased and not being good enough, then I wouldn’t be where I’m at.
[00:20:11] I tell you, I’ve learned a lot from you, and if anything, my kids have learned a lot from you by just your persistence. You know, I can honestly tell you that my son is better as an athlete because of his relationship with you.
[00:20:29] But let me ask you, in terms of what kind of physical changes as well as emotional changes have happened with you in terms of watching your clients attain their goals?
[00:20:43] Hearing people say you saved me from.
[00:20:48] From diabetes, medications, diabetic medications, I mean you hear people say like.
[00:20:55] I would have died being in this obese state. You saved my life. Man. How do you not get emotional with things like that?
[00:21:04] How do you not get emotional? People saying like, you know, I thought I couldn’t walk or had this muscle imbalance or muscle type of. How do you say?
[00:21:18] I have this one client that couldn’t build muscle. I can’t remember terminology, but the fact that she can build muscle now where the doctor told her she wouldn’t be able to squat a bar and now she’s squatting over one hundred and thirty five pounds, that’s phenomenal.
[00:21:31] How does that not keep you motivated and getting up every single day when you don’t feel like getting up, you know, and I’ll say it again. I am in the King David. You know, when you had to encourage yourself, because somebody is not always going to be there to encourage you. You do have to encourage yourself so you can be the best or somebody else that needs it more than you. Ultimately, at the end of the day, someone has it harder than you and you can always help somebody under you.
[00:22:01] Oh, Danny, you’ve basically said it in very short and very important keywords. You know, we appreciate you. We’re here at the PUSH Fitness Center. You know, we’ve got some information there that you can use to find Mr. Alvarado, the PUSH Fitness Center is a monster center with a lot of people that care and make changes in people’s lives.
[00:22:25] If you guys have any questions, any comments, any ideas in terms of what we do for people, let us know. And we’re here to serve as Danny is. Danny, thank you very much, brother. And I appreciate everything you’ve done.
[00:22:38] And God bless, brother. God bless. Thank you.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
Nutraceuticals can help relieve several different types of chronic pain, including sciatica or sciatic nerve pain. Stephen DeFelice, MD, coined the term in 1989, which is a combination of the words nutrition and pharmaceutical. He defined nutraceuticals as food that offers a variety of health benefits as well as prevention and/or treatment of health issues. Although these foods are considered to be natural products, it’s essential to discuss nutraceutical options for chronic pain, including sciatica or sciatic nerve pain, with a healthcare professional to avoid any side-effects or interactions with drugs/medications.
Several nutraceuticals are also considered to be dietary supplements. According to the Dietary Supplement Health and Education Act (DSHEA) is a product that is taken orally in pill, capsule, tablet, or liquid form which is made-up of any chemical ingredient that adds to what a person normally gets in their diet, including vitamins, minerals, amino acids, and herbs as well as substances made from organs or glands and enzymes. Dietary supplements can also be an extract or concentrate. Several examples of dietary supplements include vitamin C, vitamin D, calcium, and fish oil, best known as omega-3 fatty acids.
Nutraceuticals aren’t only limited to dietary supplements, as Dr. Stephen DeFelice previously described. It can also include genetically engineered food, such as food with added antioxidants, vitamins, and minerals. Nutraceuticals offer people extra nutrients that the body needs to use as fuel for energy. Nutrients, such as proteins, fats, and carbohydrates are broken down by the body’s metabolism, a process that uses energy to regulate breathing and heartbeat, among other essential bodily functions. In the following article, we will discuss how nutraceuticals can help improve sciatica or sciatic nerve pain.
How Nutraceuticals Can Help Improve Sciatica
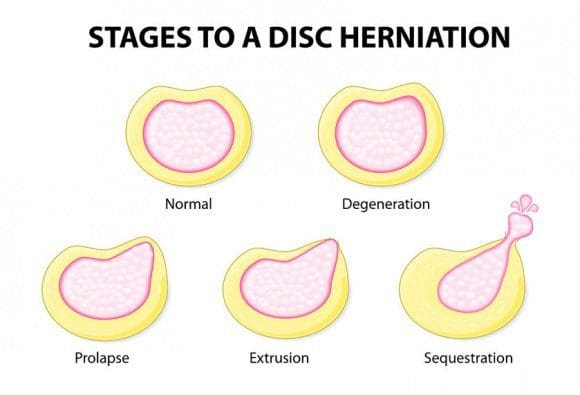
When people have chronic pain, including sciatica or sciatic nerve pain, the body will generally require more nutrients to repair itself. Nutraceuticals can help supplement the nutrients people are already getting from their diet by giving the body more nutrients to use. According to several research studies, nutraceuticals can help reduce pain and inflammation associated with low back pain and other health issues. Sciatica or sciatic nerve pain is a collection of symptoms, rather than a single condition, which is caused by a variety of health issues, including a bulging disk, herniated disk, or degenerative disk disease.
“Nutraceuticals, as well as dietary supplements, work best when used in combination with proper diet, regular exercise or physical activity, and stress management”, stated Carrie Bowler, DO, a physician with One Medical Group in New York. Although these foods are considered to be natural products, it’s essential to discuss nutraceutical options for chronic pain, including sciatica or sciatic nerve pain, with a healthcare professional to avoid any side-effects or interactions with drugs/medications. Below, we will discuss several nutraceuticals that can ultimately help improve sciatica or sciatic nerve pain.
Nutraceuticals for Sciatica
Vitamin D
According to researchers, vitamin D deficiency can make sciatica or sciatic nerve pain worse. One research study published in Pain Physician in 2013 found that chronic pain may be associated with an increased prevalence of vitamin D deficiency in people with spinal stenosis in their lumbar spine or low back, a common cause of sciatica or sciatic nerve pain. A healthcare professional will determine an individual’s recommended dosage of vitamin D based on their individual needs and requirements. Sunlight exposure and vitamin D-fortified foods, such as vitamin D milk, may also help supply the nutrient.
Omega-3 Fatty Acids
Healthcare professionals recommend increasing the intake of omega-3 fatty acids to help reduce inflammation that can ultimately cause chronic pain. Many dietary supplements are available in pill, capsule, tablet, or liquid form. Make sure to talk with your healthcare professional about the proper dosage of omega-3 fatty acids because increased doses of this nutrient can increase the risk of bleeding and other complications. It can also interfere with any blood-thinning drugs and/or medications. You can also increase the intake of omega-3 fatty acids by eating tuna, salmon, sardines, and dark leafy greens.
Glucosamine and Chondroitin
Glucosamine and chondroitin are organic compounds that are naturally produced in the body. According to the U.S. National Library of Medicine, glucosamine can be found in the fluid around the joints while chondroitin can be found in the cartilage surrounding the joints. Navid Farahmand, MD, an interventional pain management physician with the Brain and Spine Institute of California in Newport Beach, stated that, although there aren�t many research studies on the effectiveness of glucosamine and chondroitin for people with back pain, others have shown a meaningful impact on chronic knee pain.
Turmeric or Curcumin
Turmeric or curcumin, the active ingredient in the yellow-ish plant, is one of the most recommended dietary supplements for chronic pain, including sciatica or sciatic nerve pain. The spice, which is commonly used in Indian curry dishes, can be taken as a powder in capsules, mixed into tea, or as a liquid extract. The National Center for Complementary and Alternative Medicine (NCAAM) reports that turmeric is considered safe for most adults but prolonged use could cause an upset stomach. As a dietary supplement, it’s not recommended for people with gallbladder disease because it can make the condition worse.
Nutraceuticals can help relieve several different types of chronic pain, including sciatica or sciatic nerve pain. Nutraceuticals are foods that offers a variety of health benefits. It’s essential to discuss nutraceutical options for sciatica or sciatic nerve pain with a healthcare professional to avoid any side-effects or interactions with drugs/medications. Several nutraceuticals are also considered to be dietary supplements. Several examples of dietary supplements include vitamin C, vitamin D, calcium, and fish oil, best known as omega-3 fatty acids. Nutraceuticals can also include genetically engineered food. Nutraceuticals offer people extra nutrients that the body needs to use as fuel for energy to regulate breathing and heartbeat, among other essential bodily functions. In this article, we will discuss how nutraceuticals can help improve sciatica or sciatic nerve pain.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Nutraceuticals can help relieve several different types of chronic pain, including sciatica or sciatic nerve pain. Stephen DeFelice, MD, coined the term in 1989, which is a combination of the words nutrition and pharmaceutical. He defined nutraceuticals as food that offers a variety of health benefits as well as prevention and/or treatment of health issues. Although these foods are considered to be natural products, it’s essential to discuss nutraceutical options for chronic pain, including sciatica or sciatic nerve pain, with a healthcare professional to avoid any side-effects or interactions with drugs/medications.
Several nutraceuticals are also considered to be dietary supplements. According to the Dietary Supplement Health and Education Act (DSHEA) is a product that is taken orally in pill, capsule, tablet, or liquid form which is made-up of any chemical ingredient that adds to what a person normally gets in their diet, including vitamins, minerals, amino acids, and herbs as well as substances made from organs or glands and enzymes. Dietary supplements can also be an extract or concentrate. Several examples of dietary supplements include vitamin C, vitamin D, calcium, and fish oil, best known as omega-3 fatty acids.
Nutraceuticals aren’t only limited to dietary supplements, as Dr. Stephen DeFelice previously described. It can also include genetically engineered food, such as food with added antioxidants, vitamins, and minerals. Nutraceuticals offer people extra nutrients that the body needs to use as fuel for energy. Nutrients, such as proteins, fats, and carbohydrates are broken down by the body’s metabolism, a process that uses energy to regulate breathing and heartbeat, among other essential bodily functions. In the article above, we ultimately discussed how nutraceuticals can help improve sciatica or sciatic nerve pain.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
Tennant, Forest. �Nutraceuticals for Chronic Pain.� Practical Pain Management, 18 July 2016, www.practicalpainmanagement.com/patient/treatments/nutraceuticals/nutraceuticals-chronic-pain.
Mosenthal, William P. �Sciatica Pain, Symptoms, Causes, Diagnosis, and Treatment.� SpineUniverse, 9 Jan. 2020, www.spineuniverse.com/conditions/sciatica/sciatica-pain-symptoms-causes-diagnosis-treatment.
Theobald, ByMikel. �Photo Gallery: 7 Supplements That Help Back Pain.� EverydayHealth.com, 22 Jan. 2015, www.everydayhealth.com/pictures/best-worst-supplements-help-back-pain/.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
Here are some tips that you can use throughout the year but are especially useful during the holidays. So give yourself the gift of spending happy holidays with less stress, neck and back pain. Christmas is a time of excitement, growth, family, friends mixed with stress.
Now there is good stress that we all use when we need it, but when everything just starts to close in all around you, that’s the bad kind of stress that we want to prevent and avoid. For people with chronic back or neck pain, the strain of getting your to-do list done can take the joy of the season right out and replace it with pain and misery. �Therefore plan ahead so you can get your holiday chores done without pain.
Five tips for making the holidays more enjoyable and comfortable
Tip 1 – Shop Simple
Back and leg pain, along with sciatica, can make walking at a shopping mall almost impossible. Instead of doing a lot of walking maybe pick up gift cards or go online. This way the family and friends get to pick whatever they want and you avoid lifting and carrying shopping bags. But, if you do buy personalized gifts, go online. Everything gets shipped straight to wherever you want.
Tip 2 – Plan Before Cooking
If you’re expecting a large crowd, prepare all you can ahead of time. Example: pies can be baked the day before.
Before you start cooking, look at the kitchen. Is there room for everyone to fit while helping, conversing, etc? If not, set up the space so people can flow easily around each other and get things done.
Use your counter-top to lean on every now and then for a few minutes and take the pressure off your back. Do not stay in any one position for an extended period. To help you not forget, set a timer to remind you to sit, rest, or stand. Also, let your guests help with serving and clean up so any stress on the body is reduced.
Tip 3 – Make Decorating a Group Activity
Don�t decorate by yourself. Especially when moving heavy objects. Get help so everyone is involved. This will prevent repetitive injuries when reaching or twisting and reduce stress to you and your family’s backs.
Tip 4: Make Time for Yourself
During the holidays we can get tempted to forget about our regular eating and exercise routines.
Stay focused, as you need strength and flexibility to be able to accomplish these tasks. So stretch out and continue your exercise regimen no matter how hectic it gets.
Stretching will help keep you limber and reduce the risk of a sprain or strain.
If there is no time for your regular exercise routine, don�t just drop it. Adapt and break up the exercises into little segments throughout the day.
Continue to eat the regular healthy meals you’re used to. Gaining weight will make back pain worse. Staying on track isn�t easy during the holidays. Take a look online for healthy strategies before the holiday parties begin.
Here are some examples:
Eat breakfast to prevent overeating later in the day.
At the party, fill up with low-calorie foods like vegetables, leafy green salads, and lean proteins.
Try to stay out of easy reach of nuts, chips or candies, cookies, etc.
If you’re going to have some high-calorie food have some, but don’t overdo it.
And if you�re going to indulge try something that doesn’t come around all the time, like a piece of your aunt�s pie, cookies, cake, ham, tamales, that you only get once a year.
Tip 5 – Look to the Future
Look ahead to the future and look up some simple ways to improve your back or neck pain. Setting some goals like adding a 5-minute walk break to your day that you could gradually increase to ten, fifteen minutes and so on. Signing up for a yoga/fitness class could be another idea. This could also be the year to replace your mattress. Whatever the case, take it all in, look at the options and figure out what works for you.
How to eliminate Back Pain naturally | (2020) Foot Levelers |El Paso, Tx
NCBI Resources
There are 3 major categories of stress: bodily, environmental and emotional.
Bodily stress: Caused by lack of sleep, disease, trauma or injury, and improper nutrition.
Environmental stress:�Caused by loud noises (sudden or sustained), pollution and world events, such as war and politics.
Emotional stress:�Caused by a variety of life events, such as moving homes, starting a new job and regular personal interactions. In contrast to the other two categories of stress, however, people can have some control over their emotional stress. Such can depend on the individual�s own attitude.
A pain specialist is a medical or osteopathic doctor that treats pain caused by disease, disorder, and trauma. Also known as interventional pain management specialists, these doctors are often anesthesiologists or physiatrists.
Pain medicine involves multi-disciplines and team effort with a patient’s primary physician, other doctors, and specialists in radiology, psychiatry, oncology, nursing, chiropractic/physical therapy, alternative medicine, etc.
Education and Training
Upon completion of medical school and a one-year internship, the specialist enters a residency program in anesthesiology, physical medicine or other fields like neurology. Upon residency completion, the doctor completes a one-year fellowship for advanced training in pain medicine.
Pain medicine specialists continue medical training and education throughout their careers.
Pain Management Goals
Pain medicine is aimed at managing acute or chronic pain through pain frequency and intensity reduction and ultimately alleviation.
Multidisciplinary treatment programs are utilized to address functional goals and normal day to day chores and activities.
A pain treatment plan’s goal is to regain well-being, increasing your level of activities like returning to work, school, etc and eliminate medication dependency.
Pain Types & Treatment
Specialists treat all types of pain.
Acute pain is severe/sharp and can signal something is wrong.
Touching a hot stove or slamming a finger in a door are examples of acute pain.
Chronic pain lasts 6 months or longer.
This type varies from mild to severe and is constant.
Spinal arthritis (spondylosis) is an example of chronic pain.
It can be difficult to manage, but combining a variety of treatments can show positive results. The pain types include:
Degenerative disease
Facet joint pain
Sciatica
Cervical and lumbar spinal stenosis
Spondylolisthesis
Vertebral compression fracture
Whiplash
An appointment consists of
These are like most medical visits. The focus is on the pain, the cause, what factors are contributing, and creating an optimal treatment management plan.
A physical examination
Neurological examination
Review of medical history particularly pain history.
Questions can include:
From zero to 10, 10 being the worst, where’s your pain at?
When did it start?
What were you doing when it started?
Does it spread or radiate out other areas of the body?
Is the intensity constant?
Is it worse at different times of the day or night?
What helps relieve the pain?
What worsens the pain?
What types of treatments have you tried?
Did it work and to what degree?
Do you take and what types of, over-the-counter medications, vitamins, and herbal supplements?
Do you take prescription medications?
A drawing of the body could be used to mark where the pain is felt, as well as indicate pain spread and type.
Diagnosis
Diagnosing the cause of pain is paramount to creating the proper management treatment plan. If the wrong diagnosis is made and the wrong treatment is initiated it might exacerbate the condition and/or create new injuries.
This can mean getting:
X-ray’s
CT scan
MRI
These imaging types help confirm the origin of the pain. When treating spine pain, arm, leg and foot symptoms may also be present. Therefore the correct diagnosis is essential to a successful treatment plan.
Spinal disorder pain treatment usually involves other specialists, like a primary care physician, neurosurgeon, orthopedic surgeon, radiologists, oncologists, nurses, chiropractors, physical therapists, and alternative medicine practitioners.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural and use the body�s own ability to achieve goals of improvement, rather than introducing harmful chemicals, controversial hormone replacement, surgery, or addictive drugs.
We want you to live a life that is fulfilled with more energy, a positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life. I have made a life of taking care of every one of my patients.
I assure you, I will only accept the best for you�
Back Pain Chiropractic Care El Paso, Texas
NCBI Resources
If you have low back pain�or have had it, you are not alone. Experts estimate that around�80% of people�will experience some type of back problem at some point in their lives.�The Global Burden of Disease 2010�lists low back pain as the number one cause of disability worldwide. The good news is the majority of back pain is mechanical in origin or is not organic.
Q: My primary healthcare provider recently diagnosed me with a herniated disc in the lumbar spine. They referred me to get chiropractic treatment, but I�m nervous because it’s new to me and I’m afraid of being adjusted wrong, paralyzed, etc. Can I trust chiropractic treatment to work?
A: It�s normal to be nervous about going to a chiropractic clinic.
If you’re not sure whether chiropractic is for you, there is scientific evidence that shows how chiropractic techniques like spinal manipulation/spinal adjustment and forms of manual/mechanical therapy are safe and effective for relieving pain and other musculoskeletal pain, conditions, and symptoms.
I encourage everyone to try chiropractic treatment as a non-surgical treatment option for a herniated disc.
It Is Your Decision
At the first appointment, a chiropractor will take a medical history and perform a thorough exam to determine the nature of the symptoms and their possible causes, which include a herniated disc.
Sometimes with a herniated disc, there may be no symptoms at all.
But usually a herniated disc causes:
Back pain
Referred pain or pain that is felt in other parts of the body like the legs, feet, etc.
An irritated spinal nerve can cause symptoms in the legs
This can lead to neurological symptoms like:
Tingling
Numbness
Weakness in the legs
Once the chiropractor determines your symptoms, they may use one or several techniques to relieve the back pain and other symptoms.
Techniques used by chiropractors for disc-related problems include:
Specific self-treatment exercises to improve motion & decrease back pain
Cox technique like spinal traction using special tables
Spinal manipulation
Hands-on techniques that relieve pain and restore movement to the spine and body
These techniques have been proven to be very safe. There are other techniques a chiropractor can recommend for various conditions, as each has their own style and method.
A chiropractic treatment plan will also include:
Education
Self-management instructions
This is to teach you how to control/eliminate pain with proper posture and proper body mechanics.
Whichever treatment the chiropractor recommends, he or she will discuss it with you, including the benefits and risks.
Although the treatments listed above will most likely be a part of your treatment plan, your chiropractor will answer your questions and work with you to select a treatment that meets your specific goals and preferences.
Don’t Be Nervous A Chiropractor Monitors Treatment Progress
If symptoms do not improve within a reasonable time frame, then a chiropractor may refer the patient to other treatments to manage disc-related pain, including:
Physical therapy
Acupuncture
Spinal injections
Surgery
Fortunately, self-management and time can be the best treatment. Allowing the body to heal itself is the way to go. But if rest is not enough then chiropractic treatment may be just what is needed to kick in the body’s self-healing function.
If you decide to give chiropractic treatment a try, don’t be nervous, as a chiropractor will monitor progress throughout the treatment.
In any case, chiropractors are qualified to discuss the benefits and risks of other treatments, depending on the condition.
Hopefully, this article has given you the basics of chiropractic medicine and how it works so you can make the best choice for your herniated disc/s.
Low Back Pain Management El Paso, TX Chiropractor
Denise suffered an auto accident injury which resulted in back pain. When she realized she could not sit, walk or sleep for lengthy periods of time without having painful symptoms, Denise found chiropractic care with Dr. Alex Jimenez at El Paso, TX. Once she received therapy for her automobile accident injuries, Denise experienced relief from her symptoms and she was able to execute her regular tasks once again. Thanks to the education and maintenance Dr. Alex Jimenez supplied, Denise regained her initial health and health.
Back pain is more most common, with roughly nine out of ten adults undergoing it at some time in their lifetime, and five functioning adults developing it annually. Some quote around 95 percent of Americans will experience back pain at some time in their lifetime. It is undoubtedly the typical cause of chronic pain since it’s also a substantial contributor to missed work and handicap. In the United States alone, acute cases of lower back pain are the fifth most frequent reason for doctor visits and cause 40% of missed days off work. What’s more, it is the leading cause of disability worldwide.
NCBI Resources
A herniated disc is a common spinal condition that typically affects the cervical spine (neck region) or the lumbar spine (lower back), although it can occur in any part of the spine. Most often, a herniated disc happens at the L4 � L5 and the L5 � S1.� This is because this portion of the spine, the lumbar region, bears the bulk of the body�s weight.
FDA recognizes and approves spinal decompression and its ability to eliminate herniated discs.
On the verge of back surgery, a mason discovered the non-surgical solution to work-related chronic back pain.
A new male patient who works in construction came to see me as a last resort to lessen his back pain brought on from damaged/herniated discs.
His primary caregiver recommended back surgery, but that would have put him on disability for months.
Fortunately, before saying yes to the surgery, a co-worker recommended chiropractic care.
Bricklayers/masons have the highest rate of back injuries with non-paid sick leave.
Constant bending over, even with a back brace, takes its toll on the spine, which in this case resulted in two herniated discs.
Pain medications helped in the beginning but with constant use, put him in a constant brain fog state, along with the expense, which took its toll on the family budget.
Disc Injury & Back Surgery
The doctor did not discuss spinal decompression therapy
�A non-surgical back treatment that slowly and gently stretches the spine.
This stretching lessens the pressure on the compressed nerve root (herniated disc) and results in less and even complete alleviation.
The patient came twice a week with myself and the team working on him over the course of a month, however, every case is different so treatments vary depending on the condition.
With each treatment, the two herniated discs were slowly reverted back to their natural position. This is able to be achieved with less pressure between the discs.
Towards the end of treatment, the patient’s pain was gone by about 90%.
With two weeks of rest, the patient was able to return to work.
The best part was that there was no surgery, pain medications, disability, and hospital bills.
Spine treatment alternative
Chiropractic/Decompression therapy is way less expensive than medication and surgery. It is:
Non-surgical
Recovery time is faster
Completely drug-free
People suffering every day with herniated/injured discs should consider the chiropractic decompression option. You do not have to learn to live with chronic back pain.
If you suffer from:
Herniated discs
Bulging discs
Degenerative disc disease
I encourage you to discuss the condition with an experienced chiropractor. There are many proven alternatives to back surgery and pain meds. People need to be aware of these alternatives for chronic back pain. The right-back pain treatment can definitely improve the quality of life.
Herniated Disc El Paso, TX
Sandra Rubio developed two herniated discs and a bulging disc after suffering from an accident at a young age, which caused her intense pain throughout her youth.
When she became a mother, her symptoms became severe.
After visiting doctors without results, Sandra found chiropractor Dr. Alex Jimenez and found relief from her sciatica and migraines.
The herniated disc treatment she received from Dr. Alex Jimenez was non-surgical.
A herniated disc, also known as a slipped disc, is a medical condition in which:
Atear from the outer intervertebral disc allows the soft, central area to bulge out beyond the outer rings.
Disc herniation is usually a result of:
Degeneration (wear/tear)
Trauma (auto accident/sports injury)
Lifting injuries
Straining movement
The tear can release the compounds, which cause inflammation and can cause severe pain even if the nerve root not compressed.
A physical examination is usually the first step in diagnosing a herniated disc. The chiropractor will examine the spine while the patient is standing, and while they’re lying down. Depending on the severity and location of the herniation, they may note a decrease in spine curvature.
Radicular pain will be assessed, when the spine is:
Unmoving
In motion
With pressure applied
Other tests may be administered.
X-rays may also be taken, but an MRI is usually more accurate and shows more detail.
Chiropractic has been very effective in helping patients manage their pain and regain their mobility so they can return to their normal life. Therefore, it should be your first option for treatment before you go down the road with drugs or surgery.
NCBI Resources
It is often referred to as a ruptured disc or slipped disc and occurs when the disc moves or slips out of place. It can also be the result of a disc that has a small tear and is leaking the jelly-like substance that is inside. This can put pressure on the surrounding nerves, causing pain and discomfort.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine