Food is more than just energy. Diets have a profound effect on everything in an individual’s life. Some foods can help the body heal or interfere with the recovery/healing process from injury/s and/or conditions that include sciatica. Making changes to a diet plays a significant factor in the recovery/rehabilitation phase, and adding certain foods will improve and expedite the healing process. A fully functional sciatic nerve nutrition diet plan must be personalized to each individual’s needs.
Sciatic Nerve Nutrition
Sciatica can cause numbness, tingling, electrical shock-type pain, or a combination in the back, hip, outer side of the leg, and the foot. Clinical nutrition is a powerful tool when combating sciatica. Enzymes in certain foods can help reduce the inflammation associated with sciatica. A high percentage of individuals dealing with sciatica can enhance pain relief by adjusting their diets. Quick recommendations include:
Oily fish like salmon and halibut are rich in omega-three fatty acids that decrease inflammation in the body and the sciatic nerve.
Fresh pineapples and berries are anti-inflammatories that aid in healing and increase immune system function.
2-3 cups of green tea contain antioxidants that help control peripheral sensations and help manage pain.
Turmeric, ginger, and garlic contain anti-inflammatory agents that relieve swelling by reducing levels of inflammation-stimulating enzymes.
B-Vitamins are essential to maintain normal nerve function and can be found in green peas, spinach, navy beans, nuts, and bananas.
Magnesium-rich foods can ensure the body is not deficient and help control muscle spasms.
Sciatica can also be triggered by a poor diet that causes constipation that can place pressure on the nerve. Therefore it is recommended to incorporate fiber-rich foods that include plenty of fruits and vegetables to prevent constipation.
Foods That Make Sciatica Worse
Inflammatory foods to avoid:
Sugar and high-fructose corn syrup.
Trans fats include margarine and any hydrogenated/solidified or partially hydrogenated oils.
Refined vegetable oils – These are vegetable, nut, or seed oils that have been highly processed. Cut down on french fries, chips, or other foods fried in these oils.
Refined carbohydrates – Carbohydrates that have fiber removed increase the growth of inflammatory gut bacteria. These include white flour, refined corn products, white rice, and various commercial cereals and sugars.
Excessive alcohol – Moderate amounts of alcohol can provide health benefits, but higher amounts increase inflammation.
Processed meats – are often processed at high temperatures, creating chemicals/substances associated with inflammation.
Avoid Surgery
References
Davis D, Maini K, Vasudevan A. Sciatica. [Updated 2022 Feb 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507908/
Garfin, SR et al. “Spinal nerve root compression.” Spine vol. 20,16 (1995): 1810-20. doi:10.1097/00007632-199508150-00012
Kumar, M. Epidemiology, pathophysiology and symptomatic treatment of sciatica: A review. nt. J. Pharm. Bio. Arch. 2011, 2.
Safari, Mir Bahram, et al. “Efficacy of a Short-Term Low-Calorie Diet in Overweight and Obese Patients with Chronic Sciatica: A Randomized Controlled Trial.” Journal of alternative and complementary medicine (New York, N.Y.) vol. 26,6 (2020): 508-514. doi:10.1089/acm.2019.0360
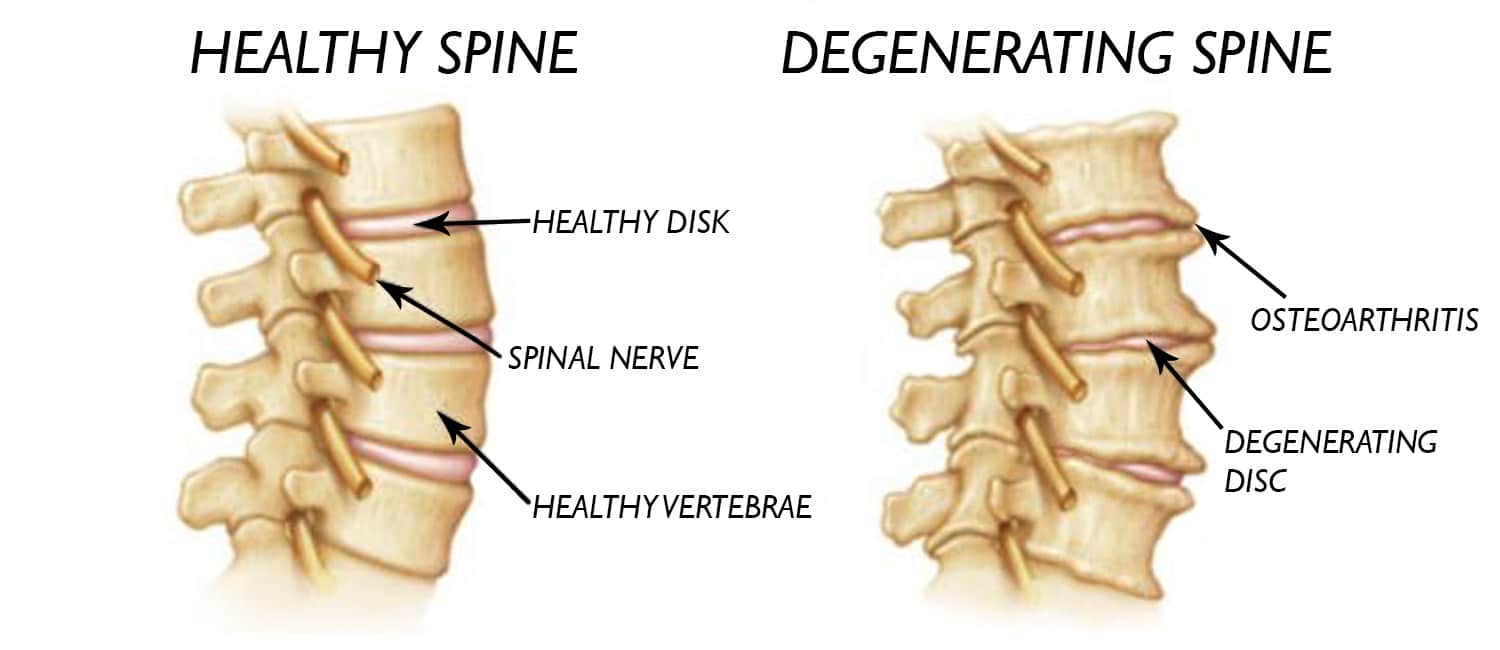
Everyone worldwide has suffered from some reasonable amount of injuries in their spine. The spine is part of the musculoskeletal system that holds muscles, tissues, ligaments, and spinal cavities. In the spine, round, cushion-like discs are sectioned in each vertebra that helps protect the spine and spinal cord. As the body ages, so do the spine, causing the cushion-like disc to become stiff and compressed until they start to crack the outer layer. This crack allows the inner layer of the spinal disc to leak out and bulge out of the spine. This bulge then starts to press on the spinal nerve roots connected to the spinal cord causing the person to feel pain. When this happens, non-surgical treatments are available to help restore the spinal disc to the spine and allow the irritated nerve root to relax and repair itself. Today’s article explains how to take care of our spine, what happens when disc herniation is, and how decompression therapy can restore spinal discs and increase their height in the spine. Referring patients to qualified and skilled providers who specialize in spinal decompression therapy. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is essential for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
Taking Care Of Your Spine
Feeling wear and tear on your back? Do you feel stiffness in your joints as you twist and turn? How about aches and pains in random places in the lumbar or cervical area of the body? When something like this happens to the body, it could be how you take care of your spine. In many previous articles, the spine is an S-shaped curve part of the musculoskeletal system that allows the body to do everyday movements that help a person move around. When a person injures their back, their spine usually takes damage in pulled muscles, stiff joints, a momentary sense of instability when getting up, and low back pain. Research studies have stated that when there are spine disorders in the back, it can involve the entire intervertebral disc, joints, and tissues that are connected to the spine.
Spine disorders are also associated with low back pain issues, causing them to lower the quality of life in a person and, if not treated right away, hinder their ability to move around. Additional information has mentioned that contributing factors affect when acute or repetitive trauma starts to cause low back pain issues. Compressing the spinal disc repeatedly through overtwisting and turning can increase the chances of internal disc disruptors and disc instability. When this happens, disc herniation does occur in the cervical and lumbar regions of the spine.
Disc Herniation
When there are spine disorders associated with low back pain, disc herniation is one of the factors for back sufferers. Studies have defined that disc herniation occurs in the cervical and lumbar regions of the spine, causing the spinal disc’s outer layer to crack and expose the inner walls to bulge out, causing the spinal nerve roots that are neck to them to be irritated and compressed. When the nerves start to become affected, it can cause pain and dysfunction in the spinal cord. Disc herniation can also progress to severe causes like loss of sensory and motor functions to the lower half of the body and lower back, causing muscle weakness. More research studies have stated that since disc herniation is so common for many people, it can be the pathogenesis of sciatica to develop. All is not lost, as there are treatments that provide the necessary relief for the spine and restore the intervertebral disc back to its original function.
Disc Height & Decompression- Video
Have you been experiencing numbness around some regions of your back? How about muscle stiffness that is occurring around your neck and lower back? Does it hurt when you stretch, and the pain radiates down your leg? Experiencing these symptoms is due to disc herniation and can cause severe spinal issues that affect the back and the spine. The best way to restore the spine is through spinal decompression therapy. The video above describes how spinal decompression can help improve spinal functionality by increasing the disc height and reducing the pain signals through gentle traction on the spinal disc leaving the nerve roots alone. This will allow the individual receiving spinal decompression therapy to have their sensory and motor functions back in their lower back and legs. Suppose you want to learn more about decompression and how it can benefit you in providing relief from disc herniation? This link will explain what decompression offers optimal comfort for disc herniation in the spine.
Decompression Therapy Helps Increase Disc Height
Since disc herniation has been associated with issues affecting the cervical and lumbar regions of the spine, some treatments are available to help with disc restoration, and it is none other than decompression therapy. Research studies have shown that when individuals go in for decompression therapy, they are first lying down on a traction table and are strapped in. This allows the provider to adjust and change the direction where the opposing force will begin to reduce the pressure that the herniated disc has caused on the irritable nerve root while increasing the hydration back to the cracked outer layer of the spinal disc. The continuous effects of spinal decompression allow the intervertebral disc to increase its height between the spinal columns and reduce the herniated material. Spinal decompression therapy can also help alleviate other low back and neck pain symptoms that a person could be suffering from.
Conclusion
Utilizing treatments to take care of the body can allow it to live longer and reduce other ailments that can hinder one’s functionality. Overall, spinal decompression therapy can help restore spinal disc herniation by causing anti-gravitational or negative pressure on the spinal canals and help restore the functionality of the spine. Incorporating decompression therapy as part of a wellness lifestyle can benefit most people who suffer from low back and neck pain. Without it, many people will suffer from chronic pain and spinal issues that can cause them to become miserable
References
Choi, Jioun, et al. “Influences of Spinal Decompression Therapy and General Traction Therapy on the Pain, Disability, and Straight Leg Raising of Patients with Intervertebral Disc Herniation.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4339166/.
Dydyk, Alexander M, et al. “Disc Herniation – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 18 Jan. 2022, https://www.ncbi.nlm.nih.gov/books/NBK441822/.
Raciborski, Filip, et al. “Disorders of the Spine. A Major Health and Social Problem.” Reumatologia, Narodowy Instytut Geriatrii, Reumatologii i Rehabilitacji w Warszawie, 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5090028/.
Tariq, Rayhan A, et al. “Back Safety – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 29 Nov. 2021, https://www.ncbi.nlm.nih.gov/books/NBK519066/.
Vialle, Luis Roberto, et al. “Lumbar Disc Herniation.” Revista Brasileira De Ortopedia, Elsevier, 16 Nov. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4799068/.
As part of the musculoskeletal system located in the middle of the back, the spine helps the body stay up and provides everyday movements that a person goes from one place to another. Ligaments, soft tissue muscles, nerve roots, and other components help protect the spinal cord and spine from significant injuries like auto accidents, a slip, fall, work injuries, or acute injuries like a slipped disc or degeneration, herniation, pulled back muscles. These damages can affect the back in multiple ways and cause most people to suffer from pain. Thus many people start trying to find ways to relieve the pain in their spine or back. Today’s article immerses us in how degenerative disc starts to affect the spine and how treatments like decompression can help reduce the pain affecting the back and the spine. Referring patients to qualified and skilled providers who specialize in spinal decompression therapy. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is essential for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
The Spine Can Degenerate Naturally
Feeling tired and aching after a long workday? Do you think a variety range of pain starting to affect either your neck or lower back? How about feeling the wear and tear on your back due to normal activities? It is expected that the body naturally ages over time, causing muscles, joints, and even ligaments not to work correctly. For the spine, though, the spinal discs, which are located in-between the spinal joints, can also age and cause pain to the body. Studies have mentioned that degenerative disc disrupts the structure of the disc itself. In a healthy, average, functioning body, the spine allows mobility and stability to the person doing any activities without feeling discomfort. When habits and lifestyle choices begin to affect the body, it can develop over time into degeneration in the spinal joints, causing the spine to be afflicted. Other research studies have provided that disc degeneration on the spine affects not only the lumbar area but also the cervical area as it causes three stages during the degenerative process:
Dysfunction
Instability
Stabilization
These stages gradually affect the lumbar and cervical area over time; it causes spinal issues like osteoarthritis and spinal nerve root pressure in the back. When the spinal nerve roots become pressurized, it radiates pain that promotes muscle weakness in some back regions.
How Does It Affect The Back?
Since the spine does age naturally, causing disc degeneration, other symptoms in the lumbar regions of the back will begin to show up over time. Symptoms of low back pain seem to work hand-in-hand with disc degeneration as research studies have found that degenerative discs are irreversible in the spine. In contrast, low back pain can have adverse effects on many individuals. Low back pain exerts an enormous burden on the back’s lumbar region while promoting long-term disability. Anytime low back pain is associated with degenerative discs on the spine, the body loses the necessary sensory and motor functions such as movement limitations, balance issues, pain, muscle weakness, and reflex issues will hinder a person’s quality of life; studies have concluded.
An Overview On Degenerative Disc-Video
Feeling pain along your spine? How about aches and discomfort in the lower regions of your back? How about muscle stiffness and discomfort around the cervical and lumbar region of the spine? Experiencing disc degeneration is no laughing matter; why not try non-surgical decompression to alleviate the severe symptoms of disc degeneration. The video above provides an overview of disc degeneration and how non-surgical treatments like spinal decompression can help promote relief to the spine. Decompression promotes traction through gentle pulling to elongate spinal disc height while releasing the compressed discs off the aggravated nerve roots causing low back and neck pain. Suppose you want to learn more about decompression and how it can benefit you in providing relief from disc degeneration and other low back conditions? This link will explain what decompression offers optimal comfort for disc degeneration in the spine.
How Decompression Treats Degenerative Disc
Since both the spine and body can age, naturally, many unwanted symptoms can pop up over time in random locations in the back. With disc degeneration, the spinal discs help cushion the spine from any injuries that it succumbs to. Treatments like decompression can help with low back pain and disc degeneration. Research studies have proven that decompression treatments allow the space in-between the spinal joints to be vertically expanded while lessening the pressure and restoring disc height to the spine. Utilizing decompression enables the spine to restore the natural beneficial substances for the spinal discs while loosening the muscles connected to the spine.
Conclusion
Overall, the spine can age naturally, causing issues like disc degeneration to occur and causes unwanted symptoms like low back pain to cause long-term disability to many people. Disc degeneration is irreversible, causing sensory and motor dysfunction to the body, making it unstable, have muscle weakness in certain areas in the back, and affecting a person’s quality of life. Treatments like decompression therapy allow the spine to be decompressed while elongating disc height, causing relief to the individual while restoring spinal health. These types of treatments are perfect for many individuals that are looking to reclaim their health and wellness.
References
Apfel, Christian C, et al. “Restoration of Disk Height through Non-Surgical Spinal Decompression Is Associated with Decreased Discogenic Low Back Pain: A Retrospective Cohort Study.” BMC Musculoskeletal Disorders, BioMed Central, 8 July 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912793/.
Fakhoury, Jordan, and Thomas J Dowling. “Cervical Degenerative Disc Disease – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK560772/.
Jandrić, Slavica, and Branislav Antić. “[Low Back Pain and Degenerative Disc Disease].” Medicinski Pregled, U.S. National Library of Medicine, 2006, https://pubmed.ncbi.nlm.nih.gov/17345822/.
Kirnaz, Sertac, et al. “Pathomechanism and Biomechanics of Degenerative Disc Disease: Features of Healthy and Degenerated Discs.” International Journal of Spine Surgery, International Society for the Advancement of Spine Surgery, Apr. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8092938/.
Zheng, Chang-Jiang, and James Chen. “Disc Degeneration Implies Low Back Pain.” Theoretical Biology & Medical Modelling, BioMed Central, 9 Nov. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4640162/.
Anyone that has dealt with low back pain can describe it in various ways. Some may describe it as a mild, dull ache that can be a gradual nuisance throughout the day, while others describe it as sudden throbbing, burning pain that can radiate pain that travels down to the feet. Either way, having low back pain is horrible, and it could be developed more if people don’t change their habits to relieve back pain. Some of the risk factors can be poor lifestyle choices, common factors like looking down at your phone or lifting heavy objects, while others can be due to stress and anxiety. These risk factors can cause more pressure on the lower back; however, there are a variety of treatments that can help alleviate low back pain. Today’s article focuses on the differences between two non-surgical treatments, traction therapy and decompression therapy, and how they can relieve low back pain in their unique way. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is essential for asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
The Difference Between Traction & Decompression Therapy
Are you feeling a wide variety of pain in your lower back? Has the pain been a dull gradual ache that causes you to place your hand on your lower back? Or is it a sudden throbbing pain that hinders your ability to do any errands? This type of pain is called low back pain, and trying out either traction therapy or decompression therapy could be the answer you are looking for low back relief. Say you want to try traction therapy. Well, research studies have mentioned that traction therapy can be both manually and mechanically used to gently pulls on the spine to increase the spinal disc height while reducing the internal pressure. This allows the pain-sensitive fibers surrounding the outer layer of the spinal disc to relax. Traction therapy also allows the physical function of the spine to recover and return to normal posture; plus decreases the pain and improves the biomechanic function of the spine’s mobility. Other research studies have found that when individuals try traction therapy, the positive results show that traction therapy can help alleviate leg pain conditions like sciatica and relieve nerve root tension.
If traction therapy is not suitable for you, decompression therapy can help. As research has stated, Decompression therapy is a treatment that helps reduce the pressure off the irritated spinal nerve roots that are sending out pain signals throughout the entire lower half of the body. Decompression helps compressed, bulging discs that are touching pinched nerve roots retract back to the spine and cause the relief to the individual. That allows the reduction of muscular back spasms and loosens tense soft tissues. Additional information has been provided that decompression works well with physical therapy by restoring lumbar functionality on the spine and enhancing muscle endurance on the back. Decompression even provides relief for individuals suffering from other back pain conditions such as herniation, slipped disc, poor posture, and pinched nerves.
An Overview Of Lumbar Traction-Video
Feeling aches and pains all over your back? How about stiff muscles on your lower back when you stretch side to side? Does the pain come in a gradual or sudden throbbing way? These can be issues of low back pain and decompression, along with traction therapy can help you. The above explains what traction does while using the Chatanooga Trition machine. The machine helps many people suffering from low back pain issues and helps alleviate other chronic problems like sciatica, bulging disc, lumbar scoliosis, and pinched nerves in the lumbar region. People will feel instant relief after going in for a treatment to relieve low back pain. Suppose you want to learn more about decompression or traction therapy and how it can benefit you in relieving low back pain and other low back conditions? This link will explain what these two therapies do for the lower back.
How Both Traction & Decompression Therapy Alleviate Low Back Pain
Both traction and decompression therapy have unique ways of alleviating low back pain as both are non-surgical treatments. Research studies have demonstrated that the effects of both these treatments have increased back muscle activities through muscle endurance from the torso. Traction and decompression therapy can also provide valuable information in relieving low back pain due to degenerative changes in the spinal discs, as studies have concluded. Both treatments are excellent for many people suffering from lumbar, cervical, and leg pain, restricting their quality of life. Non-surgical treatments help people worldwide recuperate from suffering so long with back pain and help them utilize non-surgical therapy as part of their path to recovery.
Conclusion
Overall, even though traction and decompression therapy has unique functions to help alleviate pain, they both have one thing in common: they are used in non-surgical treatments to ease low back pain for many individuals. Integrating non-surgical treatments for a person’s health and wellness journey can help them live longer, develop new habits, and even help supply relief to their back. While traction therapy increases spinal disc height and decompression relieves pressure off irritated, pinched nerves, having low back pain is no laughing matter when it stops a person’s quality of life. Knowing that there are treatments for low back pain can help many individuals in the long run with their health and wellness.
References
Alrwaily, Muhammad, et al. “Assessment of Variability in Traction Interventions for Patients with Low Back Pain: A Systematic Review.” Chiropractic & Manual Therapies, BioMed Central, 17 Sept. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6139896/.
Amjad, Fareeha, et al. “Effects of Non-Surgical Decompression Therapy in Addition to Routine Physical Therapy on Pain, Range of Motion, Endurance, Functional Disability and Quality of Life versus Routine Physical Therapy Alone in Patients with Lumbar Radiculopathy; a Randomized Controlled Trial.” BMC Musculoskeletal Disorders, BioMed Central, 16 Mar. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8924735/.
Apfel, Christian C, et al. “Restoration of Disk Height through Non-Surgical Spinal Decompression Is Associated with Decreased Discogenic Low Back Pain: A Retrospective Cohort Study.” BMC Musculoskeletal Disorders, BioMed Central, 8 July 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2912793/.
Horseman, Ian, and Mark W Morningstar. “Radiographic Disk Height Increase after a Trial of Multimodal Spine Rehabilitation and Vibration Traction: A Retrospective Case Series.” Journal of Chiropractic Medicine, Elsevier, Dec. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2697595/.
Kang, Jeong-Il, et al. “Effect of Spinal Decompression on the Lumbar Muscle Activity and Disk Height in Patients with Herniated Intervertebral Disk.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Nov. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5140813/.
Oh, Hyunju, et al. “The Impact of Manual Spinal Traction Therapy on the Pain and Oswestry Disability Index of Patients with Chronic Back Pain.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6279706/.
Massage is the manipulation of the body’s muscles and tissues using controlled force, gentle and slow kneading, and assisted instrumentation. Decompression Massage Centertailors treatment plans to the individual’s health needs to help expedite recovery. A medical decompression massage can:
Bring pain relief
Relieve stress
Relieve muscle aches and tension
Release knotted or cramped muscles
Improve sleep
Improve mental/emotional state
Accelerate injury rehabilitation
Strengthen the musculoskeletal system
Release toxins
Boost the immune system
Trained professionals perform massage therapy in a clinical or hospital setting to find and focus on problem areas. The therapeutic massage involves focused work on the body’s:
Soft tissues
Muscles
Tendons
Ligaments
Discomfort and Pain Relief
A massage therapist works on several medical issues that are either chronic or acute, which include:
Overuse/Repetitive stress injuries.
Neck pain
Whiplash.
Migraines.
Tension headaches, cluster headaches, and sinus headaches.
Shoulder pain.
Back pain.
Radiating pain.
Strains and sprains.
Tendonitis.
Post-surgical scar tissue rehabilitation with a doctor’s clearance.
Decompression Massage
A therapeutic decompression massage is more profound, with individuals experiencing more tenderness as the therapist works through the tissue using various techniques and instruments that could incorporate:
A decompression massage could be recommended as an extended part of a treatment plan. Spot work focuses on areas of concern for a shorter period while enhancing the decompression treatment. Focused massage techniques will:
Alleviate pain
Increase range of motion
Restore movement and function
Assist in healing faster
Spinal DRX9000
References
Demirel, Aynur, et al. “Regression of lumbar disc herniation by physiotherapy. Does non-surgical spinal decompression therapy make a difference? A double-blind, randomized controlled trial.” Journal of back and musculoskeletal rehabilitation vol. 30,5 (2017): 1015-1022. doi:10.3233/BMR-169581
Keller, Glenda. “The effects of massage therapy after decompression and fusion surgery of the lumbar spine: a case study.” International journal of therapeutic massage & bodywork vol. 5,4 (2012): 3-8. doi:10.3822/ijtmb.v5i4.189
Menard, Martha Brown. “Immediate Effect of Therapeutic Massage on Pain Sensation and Unpleasantness: A Consecutive Case Series.” Global advances in health and medicine vol. 4,5 (2015): 56-60. doi:10.7453/gahmj.2015.059
Zainuddin, Zainal, et al. “Effects of massage on delayed-onset muscle soreness, swelling, and recovery of muscle function.” Journal of athletic training vol. 40,3 (2005): 174-80.
As the world moves, so does the body. When the body does everyday movements like running, jumping, and walking without feeling pain. When people incorporate daily habits to live longer and have healthier bodies, the body will not succumb to injuries and pain. However, when certain circumstances like stress, anxiety, and unhealthy habits start to take hold of the person’s body, it can lead to complications like obesity, chronic inflammatory responses, and low back pain affecting the body. Treatments like physical therapy and decompression therapy have been used to help many individuals trying to get their lives back together. Today’s article focuses on how obesity is associated with low back pain, how it affects the body, and how decompression therapy can help weight loss patients experiencing low back pain. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
Obesity and Low Back Pain
Feeling sluggish after walking around all day long? Do you feel shortness of breath? How about aches on your lower back? Experiencing any of these symptoms could result from obesity and low back pain affecting you. Research studies have mentioned that low back pain and obesity are the most common concerns for everybody worldwide. Since low back pain is the most musculoskeletal health concern and obesity is a health problem, many individuals will have an increased risk of lumbar radicular pain. This is due to the mass body index affecting the person’s body, as research studies have mentioned that obesity can have both biomechanical and meta-inflammatory effects on the spine. Since both male and female bodies are different in fat composition, it is more likely that female bodies tend to have more fat masses stored around the torso area, causing lower back pain issues than male bodies. In regards to that, lifestyle habits and changes can also cause obesity to progress further in both male and female bodies causing low back pain issues to develop further.
How Does It Affect The Body
When obesity and low back pain start to affect the body, research studies have shown that chronic conditions like diabetes and hypertension are associated with obesity and can influence the path for diseases in the tendons and ligaments of the body. As the body goes through the natural aging process, this can lead to low back pain and cause many overweight individuals to be at risk of osteoarthritis. The excess weight starts putting more pressure on the knees, hips, feet, and lower back when this happens. This causes the pelvis to pull forward in the body, causing the lower back muscles to become strained. All is not lost as there are treatments to lose weight and alleviate the symptoms of low back pain.
DRX9000 Decompression Therapy-Video
Do you feel aches and strains on your lower back? How about feeling out of breath from walking? Do you feel the weight bearing down onto your legs and feet? Your weight could be affecting your back, and non-surgical treatments like physical therapy and decompression therapy might be able to help you out. The video above shows how the DRX9000 decompression machine can help alleviate low back pain by gently stretching the spine to elongate the disc height and loosen up the lower back muscles. While decompression therapy helps with low back pain, research studies have found that physical therapy can help promote weight loss. Losing the excess weight can alleviate low back symptoms that are causing the muscles and joints to relax and take the stress off the spine. Suppose you want to learn more about decompression and how it can benefit you in relieving low back pain and other low back pain conditions? This link will explain what it does for the lower back.
How Decompression Can Help Weightloss Individuals
As stated in a previous article, physical therapy and decompression go hand in hand in alleviating low back pain. For individuals suffering from obesity, physical therapy can help get them back in shape. With the right motivation to exercise, lose weight, and eat healthier, individuals will begin to see the excess weight be taken off and take the pressure off their lower backs. Research studies have mentioned that individuals who lose weight are allowed to do spinal decompression therapy. After a person starts to lose weight, the residual low back pain is still there and can be a nuisance to the back. Luckily, that is where decompression therapy comes in, and as research shows, decompression therapy can help relieve low back pain and reduce the symptoms of leg pain. This is beneficial for weight loss individuals as both of these therapies can help improve a person’s quality of life and help them on their weight loss journey.
Conclusion
Overall, obesity and low back pain can cause a person to become miserable and be in pain. When a person is obese, the excess weight around the torso can pressure the lower back, hips, knees, and feet. If a person is suffering from lower back issues, it can cause them to develop other back problems that can cause them to lean and find relief. Incorporating physical therapy and decompression therapy is a match made in heaven as many individuals lose weight and start to take the pressure off their lower back. Eating healthy foods, exercising, and changing certain lifestyles can help promote a healthy body without pain, and many individuals can benefit from that.
References
Chou, Louisa, et al. “The Association between Obesity and Low Back Pain and Disability Is Affected by Mood Disorders: A Population-Based, Cross-Sectional Study of Men.” Medicine, Wolters Kluwer Health, Apr. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4839843/.
Frilander, Heikki, et al. “Role of Overweight and Obesity in Low Back Disorders among Men: A Longitudinal Study with a Life Course Approach.” BMJ Open, BMJ Publishing Group, 21 Aug. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4550727.
Frisco, Donald. “Weight Loss for Back Pain Relief.” Spine, Spine-Health, 2 Nov. 2004, https://www.spine-health.com/wellness/nutrition-diet-weight-loss/weight-loss-back-pain-relief.
Kakiuchi, Masaaki, et al. “Relief of Low Back Pain after Posterior Decompression for Lumbar Spinal Stenosis.” Spine, U.S. National Library of Medicine, 15 Sept. 2021, https://pubmed.ncbi.nlm.nih.gov/34435987/.
Mirtz, Timothy A, and Leon Greene. “Is Obesity a Risk Factor for Low Back Pain? an Example of Using the Evidence to Answer a Clinical Question.” Chiropractic & Osteopathy, BioMed Central, 11 Apr. 2005, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1151650/.
Ross, Donald A, et al. “Trends in Weight and Body Mass Index after Spinal Surgery for Degenerative Disease.” International Journal of Spine Surgery, International Society for the Advancement of Spine Surgery, Aug. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8375684/.
The central nervous system in the body controls every muscle, tissue, organ, and nerve all over the entire structure. Since the nervous system in the body contains two main parts that keep the body functioning: the central nervous system and the peripheral nervous system, these two systems work hand in hand as the central nervous system is composed of the brain and the spinal cord. In contrast, the peripheral nervous system is composed of all the nerves branched out from the spinal cord and extended throughout the entire body. One of these nerves is the sciatic nerve, and when it gets irritated, it can send hot, burning pain from the lower back down to the feet. Luckily, non-surgical treatments like decompression can help alleviate sciatic nerve pain for many suffering individuals. For today’s article, we will be discussing the sciatic nerve, what happens when it gets affected and how decompression therapy can help alleviate sciatic nerve pain. By referring patients to qualified and skilled providers specializing in spinal decompression therapy. To that end, and when appropriate, we advise our patients to refer to our associated medical providers based on their examination. We find that education is the key to asking valuable questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions, please call Dr. Jimenez at 915-850-0900.
What Is The Sciatic Nerve?
Are you feeling a searing, burning pain traveling from your buttocks to your feet? Has this pain felt uncomfortable when you try to stretch it out? Or does this pain hinders your ability to walk around to relieve the symptoms? It could be due to your sciatic nerve becoming irritated. Research shows that the sciatic nerve is the largest in the human body, originating from the lower back and traveling down to the feet. This nerve is part of the peripheral nervous system and is an important nerve that allows the legs to function like generally walking, running, and even standing so the body doesn’t fall over, as research shows. The sciatic nerve in the body provides two functions for the legs: motor function, which makes the leg’s muscles move from one place to another, and sensory function, which helps the person feel the sensations on their feet. When there are factors that cause the sciatic nerve to become irritated, it can lead to unwanted pain that can affect either side of the legs causing sciatica to form.
What Happens When The Sciatic Nerve Gets Affected?
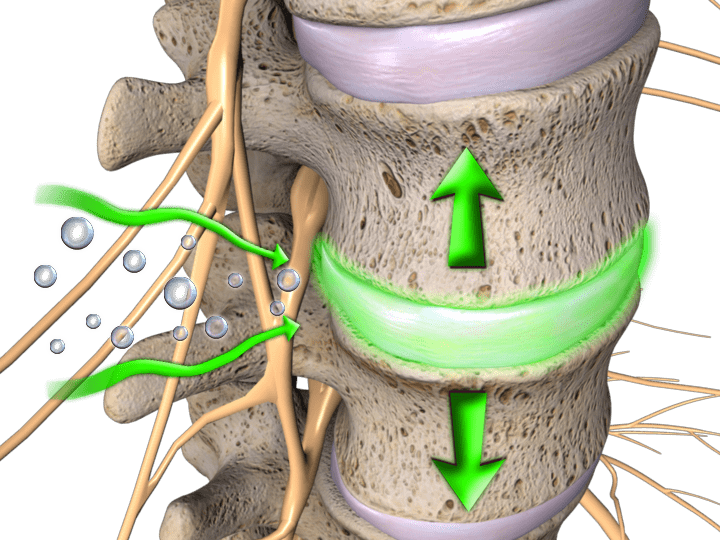
When the sciatic nerve is being affected by numerous factors, research studies have stated that irritation, compression, and inflammatory factors affecting the lower back portion of the body also affect the sciatic nerve. This causes a symptom known as sciatica, and it can affect the lower half of the body down to the feet, affecting one side of the body in either leg. Research studies have found that sciatica usually starts to affect the legs through a herniated disc in the spine that pinches the sciatic nerve, causing searing, burning pain radiating down the back of the leg. Fortunately, there are treatments available to help sciatic nerve pain from progressing further and can even help alleviate other issues affecting the lumbar area of the back. When it is not treated right away, sciatica can cause permanent nerve damage to the lower half of the body.
Decompression Benefiting The Sciatic Nerve- Video
Feeling agonizing, burning pain emitting from the buttocks down to the feet? Does it hurt to walk a short distance? How about feeling low back pain on top of leg pain? You could be experiencing sciatic nerve pain, and decompression might give you the relief you are searching for. The video above explains the top 3 ways to apply traction or decompression to the spine and how it can help relieve back issues like sciatic nerve pain. Decompression helps the spine by taking the compressed spinal disc pressure off the irritated sciatic nerve root. This allows instant relief to individuals suffering from sciatica and alleviates other back and leg issues that make them miserable. Suppose you want to learn more about decompression and how it can benefit you in relieving sciatic nerve pain or even sciatica in the lower half of the body? This link will explain what it does for the sciatic nerve and the lower back.
Decompression Can Help Alleviate Sciatic Nerve Pain
Many beneficial treatments can help alleviate sciatic nerve pain and relieve many individuals suffering. Treatments like surgical decompression can help ease sciatic nerve pain. Research studies have found that endoscopic sciatic nerve decompression is helpful to help take the pressure off the sciatic nerve and improve the person’s hip function. This type of surgical decompression can help reduce the sciatic nerve pain associated with deep gluteal syndrome entrapping the sciatic nerve and causing radicular pain. Other treatments that can help with sciatic nerve pain are non-surgical decompression. Research studies have shown that non-surgical decompression can help increase the space of the intervertebral discs that are compressed and reduces the pressure off the irritated sciatic nerve root. Non-surgical decompression allows the lower half of the body to feel relieved by decreasing the mechanical stress it’s been under, improves mobility in the lower half, and reduces muscle spasms in the legs. Decompression treatments are beneficial to anyone that wants relief from sciatic nerve pain in their legs.
Conclusion
Therefore, the sciatic nerve is the largest in the peripheral nervous system, located in the lower back, and travels down to the feet. This nerve has two primary functions that help the legs be in motion and feel sensations occurring in the feet. When unwanted factors start to affect the lower back, it can either irritate, compress, or inflame the sciatic nerve causing symptoms like sciatica to affect the legs. Treatments like decompression therapy can help take the pressure off the irritated sciatic nerve and relieve the individual from low back and leg pain. Incorporating decompression therapy is beneficial for many individuals that want to be pain-free on their health and wellness journey.
References
Giuffre, Brittney A, and Rebecca Jeanmonod. “Anatomy, Sciatic Nerve.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 29 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK482431/.
Ham, Dong Hun, et al. “Effectiveness of Endoscopic Sciatic Nerve Decompression for the Treatment of Deep Gluteal Syndrome.” Hip & Pelvis, Korean Hip Society, Mar. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5861023/.
Medical Professionals, Cleveland Clinic. “Sciatic Nerve: What Is, Anatomy, Function & Conditions.” Cleveland Clinic, 15 June 2021, https://my.clevelandclinic.org/health/body/21618-sciatic-nerve-and-sciatica.
Staff, Mayo Clinic. “Sciatica.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 1 Aug. 2020, https://www.mayoclinic.org/diseases-conditions/sciatica/symptoms-causes/syc-20377435.
Wegner, Inge, et al. “Traction for Low-Back Pain with or without Sciatica.” The Cochrane Database of Systematic Reviews, John Wiley & Sons, Ltd, 19 Aug. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6823219/.
Yeomans, Steven. “Sciatic Nerve and Sciatica.” Spine, Spine-Health, 7 June 2019, https://www.spine-health.com/conditions/sciatica/sciatic-nerve-and-sciatica.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine