As the “backbone” of the body, the thoracic region of the back has various muscles that help support the ribcage and protect the heart and lungs from injuries. The thoracic spine’s main function is providing respiration and maintaining good posture. However, various habits can cause issues to the muscles in the thoracic spine, which leads to upper back pain and the development of trigger points. One of the thoracic muscles affected by trigger points is the serratus posterior inferior muscle. Today’s article looks at the serratus posterior inferior muscle, how trigger points affect the thoracic region of the back, and how to manage thoracic back pain associated with trigger points. We refer patients to certified providers who provide different techniques in thoracic back pain therapies associated with trigger points to aid many suffering from pain-like symptoms along the serratus posterior inferior muscle along the back. We encourage patients by referring them to our associated medical providers based on their examination when it is appropriate. We designate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
What Is The Serratus Posterior Inferior Muscle?
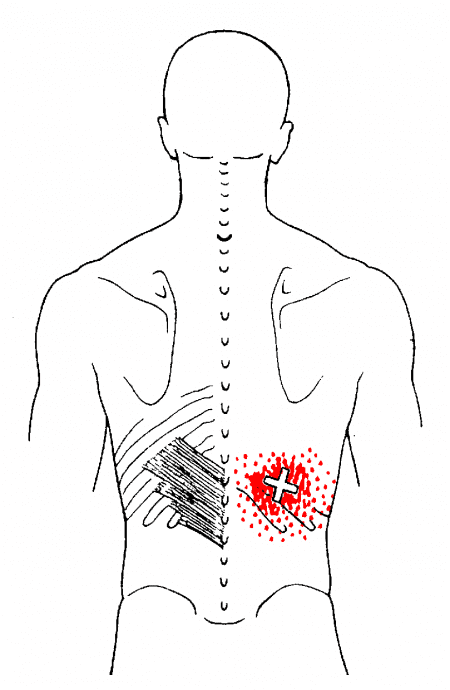
Have you felt aches and pain when bending down to pick something up? What about feeling tenderness near your lower back? Or have you experienced muscle stiffness when stretching? Many of these symptoms are associated with back pain that correlates to overusing the thoracic muscles, which includes the serratus inferior posterior muscles. The serratus posterior muscles (superior and inferior) are accessory breathing muscles as part of the extrinsic muscles. The serratus posterior inferior helps with the chest cavity’s expiration, while the superior help with inspiration. Some of the functionalities that the serratus posterior inferior provides are that in a bilateral action, the inferior works with the superior muscles to reduce the extension of the thoracic vertebrae.
In contrast, the unilateral action for the serratus posterior inferior muscle helps rotate the spine to the opposite sides. Studies reveal that based on the attachment of the serratus, the posterior inferior and superior are generally considered insignificant muscles. Since the serratus posterior muscles help aid respiration to the thoracic region, it can be succumbed to trigger points or myofascial pain syndrome that can affect the thoracic part of the back.
How Trigger Points Affect The Thoracic Region?
When the serratus posterior muscles in the thoracic region are affected by myofascial pain syndrome or trigger points, it correlates to the various activities the person has been doing that cause muscle strain along the serratus inferior posterior muscle. The book, “Myofascial Pain & Dysfunction” explains that when individuals feel a nagging ache in the lower thoracic region of the back, it correlates to residual backache associated with trigger points. Studies reveal that trigger points or myofascial pain syndrome are musculoskeletal pain disorder that affects one or multiple muscles in the body. Since back pain is common, trigger points can cause hyperirritability in the muscle’s taut band due to various factors that can cause strain on the affected muscle. When it comes to the serratus posterior inferior muscle developing active trigger points, it’s due to overload strain from combined movements like lifting, turning, and reaching for items that can also affect the surrounding muscles in the thoracic region of the back.
Trigger Point Of The Week: Serratus Posterior Inferior- Video
Have you been dealing with pain in your upper back in the thoracic region? Do you experience tenderness or soreness near your ribcage? Or have you felt a twinge of pain when turning your torso? Most of these symptoms are common signs that the thoracic region is affected by trigger points along the serratus posterior inferior muscle. The video explains where the serratus posterior inferior is located while pinpointing where the trigger points are located in the thoracic region of the back. Trigger points associated with thoracic back pain mimic other chronic conditions that can cause muscle tension and strain on the upper back. Studies reveal that latent and active trigger points affecting the upper thoracic area muscles can make many individuals feel more pain than they can tolerate. This can affect how a person functions and can make them feel inadequate. However, it is possible to incorporate a variety of treatments to reduce the pain and manage trigger points from progressing further in the thoracic region of the back.
Managing Thoracic Back Pain Associated With Trigger Points
Various treatments are available to reduce the pain affecting the thoracic region of the back and even manage trigger points associated with the serratus posterior inferior muscle. Many individuals often go to a chiropractor to relieve their back pain. Chiropractors utilize their hands and various techniques to manipulate the spine and can even pinpoint where the trigger points affect the multiple muscles in the thoracic region. Chiropractors even work with other pain specialists to devise a treatment procedure to reduce the symptoms while managing thoracic back pain associated with trigger points. Studies reveal that by when pain specialists like chiropractors begin identifying proper treatment strategies for managing thoracic back pain associated with trigger points, it might be able to reduce pain and improve function for many people dealing with thoracic back pain.
Conclusion
The thoracic region of the back has various muscles that help support the ribcage and protect vital organs, which include the heart and the lungs. One of the muscles in the thoracic region is the serratus posterior inferior muscle, an accessory breathing muscle that helps with the chest cavity expiration and helps reduce the extension of the thoracic vertebrae. When the inferior muscle becomes overused by various movements, it can develop trigger points along the inferior muscle, causing thoracic back pain. Trigger points along the serratus inferior posterior muscles can mimic other chronic conditions that can cause symptoms of muscle tension and strain on the upper back. Luckily, various treatments have been available to reduce pain symptoms and manage thoracic back pain associated with trigger points. These treatments can bring back mobility to the thoracic region of the back without the individual being in pain.
References
Chen, Chee Kean, and Abd Jalil Nizar. “Myofascial Pain Syndrome in Chronic Back Pain Patients.” The Korean Journal of Pain, The Korean Pain Society, June 2011, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3111556/.
Dor, Adi, et al. “Proximal Myofascial Pain in Patients with Distal Complex Regional Pain Syndrome of the Upper Limb.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, July 2019, https://pubmed.ncbi.nlm.nih.gov/31563368/.
Mitchell, Brittney, et al. “Anatomy, Back, Extrinsic Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 Aug. 2022, https://www.ncbi.nlm.nih.gov/books/NBK537216/.
Ortega-Santiago, Ricardo, et al. “Widespread Pressure Pain Sensitivity and Referred Pain from Trigger Points in Patients with Upper Thoracic Spine Pain.” Pain Medicine (Malden, Mass.), U.S. National Library of Medicine, 1 July 2019, https://pubmed.ncbi.nlm.nih.gov/30821833/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Vilensky , J A, et al. “Serratus Posterior Muscles: Anatomy, Clinical Relevance, and Function.” Clinical Anatomy (New York, N.Y.), U.S. National Library of Medicine, July 2001, https://pubmed.ncbi.nlm.nih.gov/11424195/.
The upper body works because it provides stability for the body and motor-sensory functions to the arms, neck, shoulders, and chest. The muscles surrounding each body section have different roles and outputs that have specific jobs for body functionality. For the chest body area, the various muscles are there to support the shoulders and arms while protecting the chest cavity and the internal organs inside. Some of the different chest muscles even support the internal organs and the rest of the muscles. One of those muscles is known as the serratus anterior muscle. Today’s article looks at this muscle, how trigger points affect the serratus anterior muscle, and various actions to manage trigger points along the serratus anterior. We refer patients to certified providers who provide different techniques in pain therapies associated with trigger points to aid many suffering from pain-like symptoms along the serratus anterior muscle along the ribcage. We encourage patients by referring them to our associated medical providers based on their examination when it is appropriate. We designate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
What Is The Serratus Anterior?
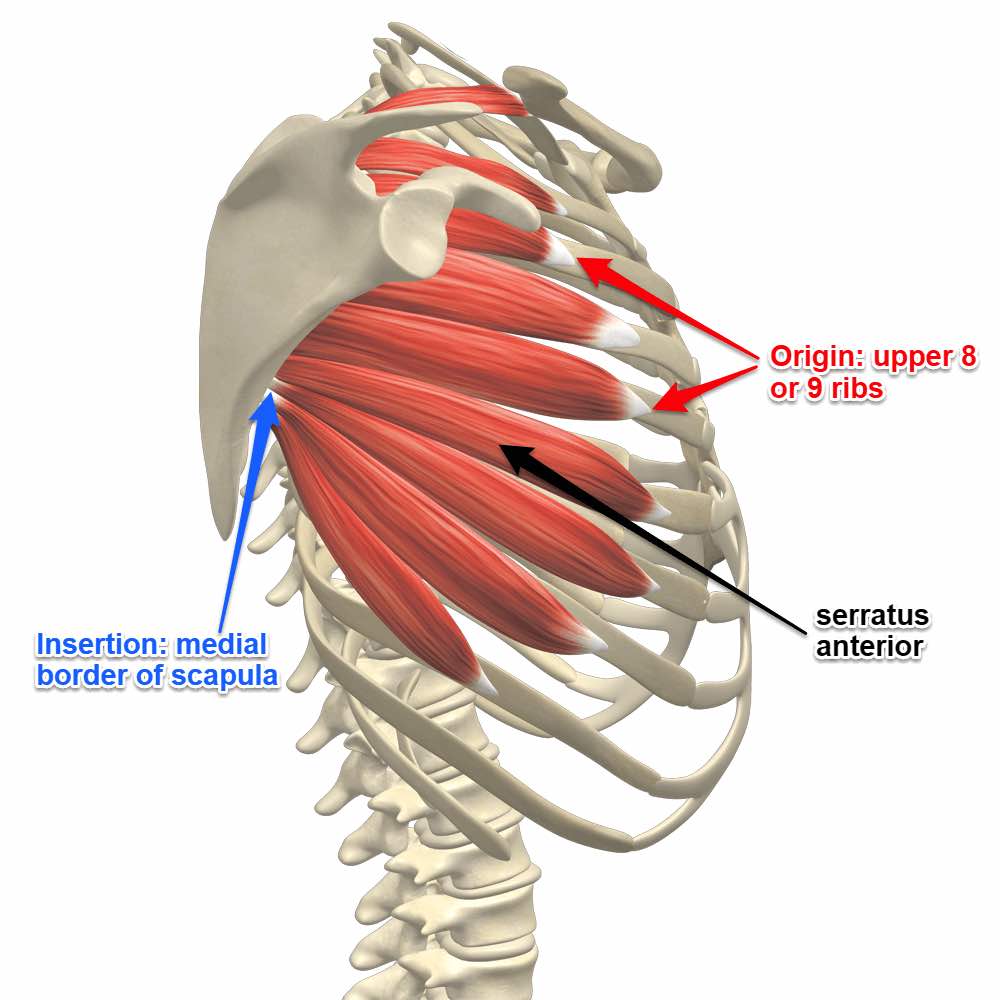
Have you been experiencing pain in your sides? Do you notice that your shoulders feel stiff when rotating backward? Or are you experiencing any cardiovascular disorders that are causing you pain? Pain can come in many forms and affect a person differently, as most of these symptoms are associated with trigger points affecting the serratus anterior muscle along the side of the ribs. The serratus anterior muscles work in the body because this muscle is located deep within the scapula (shoulder blades) and the pectoral muscles. Some of the functions that the serratus anterior provides are that it helps pull the shoulder blades forward around the thorax by allowing anteversion and protraction of the arms.
A great example is when a boxer is throwing a punch. This motor action is done with the long thoracic nerve. The long thoracic nerve originated from the C-5 and C-6 regions of the cervical spine and is the motor nerve for the serratus anterior muscle to allow an anterolateral motion for the shoulder blades that allows arm elevation. Another function of the serratus anterior is that it helps lift the ribs and provide assistance with respiration. The serratus anterior muscle also helps protect the side of the ribcage.
Trigger Points Affecting The Anterior Serratus Muscle
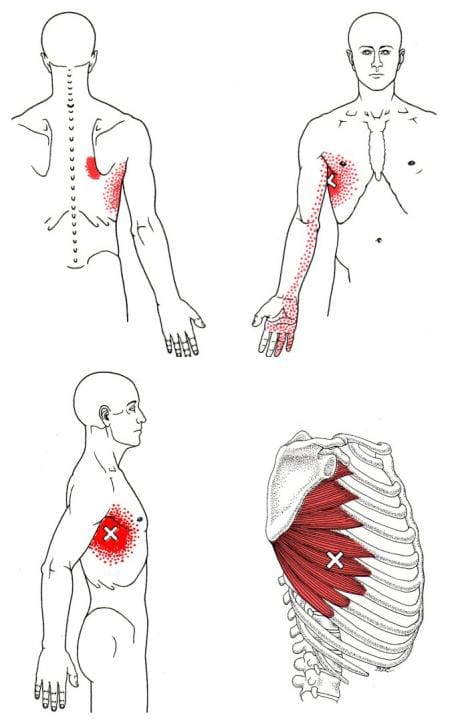
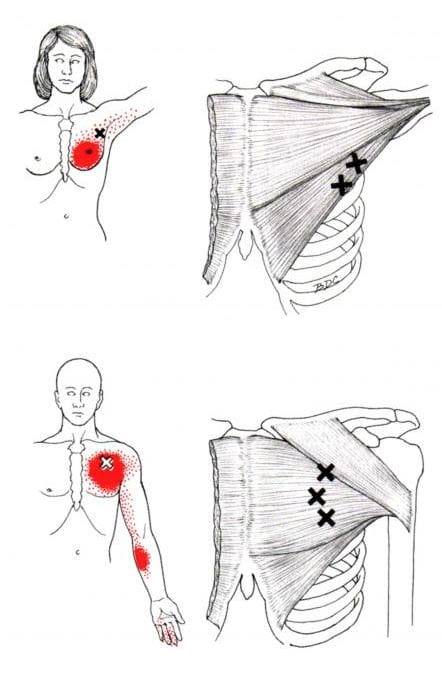
The serratus anterior muscle and the long thoracic nerve work hand-in-hand to provide motor function to the arms but can succumb to various injuries that can cause the development of trigger points or myofascial pain syndrome in the anterior serratus muscle. According to Dr. Travell, M.D.’s book, “Myofascial Pain & Dysfunction,” trigger points may be activated when the serratus anterior muscle has been overused and strained from excessive exercises like prolonged running, pushups, or heavy weight lifting or even extreme coughing from respiratory diseases. Other studies reveal that trigger points affecting the serratus anterior muscle can cause radiating pain along the anterior chest wall that can mimic radiculopathy and often be confused with chronic mechanical neck pain, instability in the glenohumeral, and even shoulder impingement syndrome. Trigger points are often difficult to diagnose due to the referred pain in the affected muscle. The various factors that contribute to the development of trigger points can be simple, like an overused muscle or even a slightly poor posture stance that can cause an imbalance in the body.
Trigger Point Release On The Serratus Anterior- Video
Have you been dealing with pain in the side of your ribs? What about experiencing stiffness or pain when throwing a punch? Do you feel any aches or soreness when adjusting your posture? These symptoms you are experiencing could contribute to the development of trigger points affecting the serratus anterior muscle. The serratus anterior covers the side of the ribcage and lies deep within the scapula and pectoral muscle. This muscle allows the motor function to the arms as it pulls the scapula forward around the thorax when someone throws a punch. However, when the muscle is overused, it can develop trigger points along the serratus anterior muscle and mimic chronic issues in the chest cavity. This causes referred pain to travel from the side of the ribs down to the hand, causing pain-like symptoms to the ring and pinky fingers. Fortunately, various treatments help manage trigger points in the serratus anterior muscle. The video above shows where the trigger points are located in the serratus anterior and how to release the trigger points from the affected muscle to relieve the pain and manage trigger points from returning to the muscle.
Various Actions To Manage Trigger Points Along The Serratus Anterior
When the serratus anterior is affected by trigger points, many people will often feel pain along their sides and complain about their chest hurting for an unknown reason. When this happens, they would be referred to a pain specialist like a chiropractor or a massage therapist to manage trigger points associated with the serratus anterior through various techniques. Studies reveal that techniques like intramuscular neural distribution of the serratus anterior muscle can help reduce the effects of trigger points in the affected muscle to reduce pain-like symptoms. Other methods like thoracic spinal manipulation, dry-needling, acupuncture, or stretching the muscle group can help loosen the stiff muscles and lower trigger points from forming. However, other actions that many people should consider are modifying or avoiding strenuous activities that can reactivate the serratus anterior muscle trigger points. Even when the person is sleeping, putting a pillow under to support the arm can prevent the scapula from falling forward.
Conclusion
The serratus anterior muscle is located at the side of the ribs and is deep within the scapula (the shoulder blades) and the poster muscles. The serratus anterior muscle works with the long thoracic nerve by providing motor function to the arms by allowing anterolateral motion. This allows the individual to throw a punch in a boxing match while lifting the ribs and assisting with respiration. When the serratus anterior muscle succumbs to injuries or has been overused, it can develop into trigger points and cause various issues affecting the body’s chest cavity. Trigger points are treatable through multiple therapies that can manage trigger points while reducing the pain effects rendered in the serratus anterior muscles. These therapies return mobility and motor function to the arms and the serratus anterior muscles.
References
Bautista, Alexander, et al. “Serratus Anterior Muscle Pain Syndrome: A Diagnostic Conundrum.” OUP Academic, Oxford University Press, 11 Feb. 2017, https://academic.oup.com/painmedicine/article/18/8/1600/2990174?login=false.
Long, Kirsten, and Forshing Lui. “Anatomy, Thorax, Long Thoracic Nerve.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 31 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK535396/.
The upper back is part of the thoracic region of the spine, surrounded by various muscles that protect the thoracic joints and help assist with respiratory functionality for the lungs. The upper back muscles consist of the rhomboids and the trapezoid muscles that provide functionality to the scapula or shoulder blades. Other superficial muscles offer assistance to the thoracic spine. The serratus posterior muscle is one of the superficial muscles that helps the thoracic spine and, like all superficial muscles, can succumb to injuries that can lead to the development of overlapping referred pain symptoms known as trigger points. Today’s article focuses on the serratus posterior muscle function in the back, how trigger points are causing upper back pain, and various techniques to manage trigger points in the upper back. We refer patients to certified providers who are diverse in upper back pain therapies to aid many people suffering from myofascial pain syndrome or trigger points associated with the serratus posterior muscle along the upper back. We advised patients by referring them to our associated medical providers based on their examination when appropriate. We indicate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Serratus Posterior Muscle Function In The Back
Have you been dealing with constant upper back pain? Do you feel soreness at the base of your neck? Or are you having difficulty breathing? Most of the symptoms cause pain in the serratus posterior muscles that can lead to the development of myofascial pain syndrome or trigger points along the upper back. The serratus posterior has various roles in the upper back as it is not only part of the extrinsic muscles but also part of the accessory breathing muscle. The serratus posterior muscle helps with inspiration, which causes the chest cavity to expand as it is a superficial muscle attached to the ribs and is less commonly known. Studies show that the serratus posterior muscle is deep within the rhomboid muscles and is superficial. Even though this muscle is superficial when it has been overused through various activities, that can cause hypertrophy in the accessory respiratory muscles. Additional studies reveal that the serratus posterior superior muscle is considered clinically insignificant but has been impaired by myofascial pain syndrome or trigger points that can lead to upper back pain.
Trigger Points Causing Upper Back Pain
As stated earlier, the upper back is part of the thoracic region of the spine, and when various factors begin to affect the body, the back muscles tend to be involved. Studies reveal numerous sources of spinal pain in the thoracic spine. One is a myofascial pain syndrome affecting the serratus posterior muscles causing referred upper back pain. Myofascial pain syndrome or trigger points can be activated when the serratus posterior muscle is overloaded from thoracic respiratory issues like coughing due to pneumonia, asthma, or chronic emphysema. When respiratory problems affect the muscles in the thoracic region of the back, it leads to the development of trigger points, leading to overlapping issues like referred pain, motor dysfunction, and autonomic phenomena. According to Dr. Travell, M.D., in the upper back, trigger points can make the serratus posterior muscle cause overlapping risk profiles along the shoulder blades and have referred pain travel to the hands. This can make many individuals suffer from serious pain-like symptoms, causing them to be miserable.
Releasing Trigger Points Related Tension In The Upper Back-Video
Have you been dealing with respiratory issues causing you to be hunched over constantly? Do you feel soreness or tenderness at the base of your neck? Or are you suffering from upper back pain? These symptoms are associated with trigger points that are affecting the serratus posterior muscles causing upper back pain. Trigger points, or myofascial pain syndrome, is a musculoskeletal disorder that causes tenderness along the affected muscle that causes referred pain to the surrounding muscles in the body. Trigger points associated with the serratus posterior muscles can cause referred pain in the upper back and mimic various chronic conditions. Trigger point pain is difficult to diagnose but can be manageable with treatment. The video above gives examples of how to treat trigger points to relieve tension in the upper back.
Various Techniques To Manage Trigger Points In The Upper Back
When it comes to upper back pain, many individuals will go to pain specialists like massage therapists or chiropractors to relieve any issues affecting the upper back. These pain specialists utilize various techniques like stretching, spinal manipulation, massages, and ischemic compression to alleviate pain and manage trigger points from forming further in the affected muscle. Pain specialists like massage therapists or chiropractors are excellent for locating pain-like symptoms associated with trigger points. Even though treatment can help manage symptoms associated with trigger points, many people can still incorporate these techniques, like deep breathing or correcting their posture, to prevent the upper back muscles from becoming strained and causing more issues than before.
Conclusion
The serratus posterior muscles have various roles in the upper back region of the body. These superficial muscles are extrinsic and accessory breathing muscles that help expand the chest cavity. When multiple issues affect the upper back muscles, like strenuous activities or respiratory problems, it can develop trigger points along the serratus posterior muscles and invoke pain-like symptoms to travel down to the hand, causing mobility issues. Thankfully, various techniques that pain specialists like chiropractors and massage therapists use can help manage trigger points from escalating and can bring upper back mobility to the body once again.
References
Altafulla, Juan J, et al. “An Unusual Back Muscle Identified Bilaterally: Case Report.” Cureus, Cureus, 15 June 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6093753/.
Briggs, Andrew M, et al. “Thoracic Spine Pain in the General Population: Prevalence, Incidence and Associated Factors in Children, Adolescents and Adults. A Systematic Review.” BMC Musculoskeletal Disorders, BioMed Central, 29 June 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2720379/.
Mitchell, Brittney, et al. “Anatomy, Back, Extrinsic Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 4 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK537216/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Vilensky, J A, et al. “Serratus Posterior Muscles: Anatomy, Clinical Relevance, and Function.” Clinical Anatomy (New York, N.Y.), U.S. National Library of Medicine, July 2001, https://pubmed.ncbi.nlm.nih.gov/11424195/.
The chest in the body has many functions: it helps provide stability on the shoulders, helps protect the heart and lungs, and bears most of the weight of the rest of the upper body. The chest is home to the pectoralis (major and minor) and the serratus anterior muscles, providing mobility and compression to the chest. As the chest muscles protect the heart and lungs, the other muscles, known as the accessory muscles, aid the heart and lungs regarding respiratory and ventilation. In contrast, the primary chest muscles can not provide that function. The sternalis muscle is one accessory muscle that assists the heart and the lungs. Today’s article examines the sternalis muscle in the chest, how myofascial pain syndrome is associated with the sternalis muscle, and various techniques for managing myofascial pain syndrome on the sternalis muscle. We refer patients to certified providers specializing in chest pain therapies to aid many people suffering from myofascial pain syndrome associated with the sternalis muscle along the chest. We brief patients by referring them to our associated medical providers based on their examination when appropriate. We indicate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Sternalis Muscle In The Chest
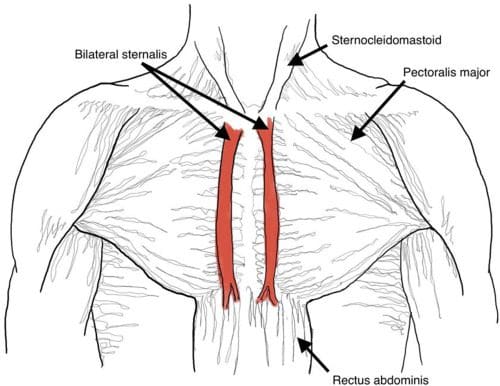
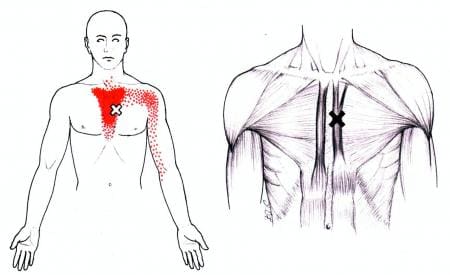
Have you been experiencing respiratory issues that are affecting your chest? What about feeling muscle tightness in the middle of your chest? Or are you experiencing radiating pain traveling down your elbow? These symptoms are often associated with pain caused by trigger points along the chest affecting the sternalis muscle. Studies reveal that the sternalis muscle is an anatomical variant along the anterior thoracic region of the body. The sternalis muscle is located right in the middle of the chest and is toward the end of the pectoralis muscles. “Myofascial Pain and Dysfunction,” written by Dr. Janet G. Travell, M.D., explained that the sternalis muscle often occurs bilaterally or unilaterally in the body and may attach itself either in the pectoralis muscle or the sternocleidomastoid. The sternalis muscle could even become a continuation of these muscles as well.
One of the unique functions of the sternalis muscle for the body is that it is an accessory muscle. An accessory muscle refers to various muscles that assist the breathing muscles. Since the sternalis muscle assists the other muscles as an accessory muscle, this muscle help opens the airways to allow more oxygen to the lungs. This muscle is extremely useful when it comes to exercising the body. However, this muscle is superficial and can succumb to various issues that affect the chest and internal organs.
Myofascial Pain Syndrome Associated With The Sternalis Muscle
Since the sternalis muscle is superficial, many issues can affect the middle of the chest and invoke pain-like symptoms that overlap and develop myofascial pain syndrome or trigger points in the sternalis. The symptoms associated with myofascial pain syndrome affecting the sternalis muscle are intense, deep pain that can occasionally cause soreness in the sternum. Studies reveal that since the sternalis is an accessory muscle, it can be overlooked, and symptomatic incidences can affect the chest and surrounding organs. To that point, symptoms like muscular imbalances, overuse tendinopathies, or neural compression syndromes can cause the sternalis muscle to ache and activate trigger points. When active trigger points affect the sternalis muscle, it correlates with myocardial infarction or angina pectoris mimicking cardiovascular disorders. Myofascial pain syndrome is tricky to diagnose, but it is treatable with various techniques that can manage the pain.
Massage Techniques For The Sternalis Muscle-Video
Have you been experiencing pain in the middle of your chest? Are you experiencing symptoms of cardiovascular disorders? Or does your chest hurts when you’re coughing? Myofascial pain syndrome or trigger points affecting the sternalis muscle are associated with many symptoms. Myofascial pain syndrome is a condition that affects the musculoskeletal system by causing the affected muscles to be overused and causing referred pain. Studies reveal that issues like myofascial pain syndrome begin to affect the chest wall cavity of the body; many patients think they have a cardiac disease causing greater impairment in their daily activities, causing emotional stress and a higher level of anxiety. All is not lost, though, as there are various techniques to reduce the pain and other chronic symptoms while managing myofascial pain syndrome on the sternalis muscle. The video above explains the sternalis muscle and shows different approaches to stretching and massaging the sternalis muscle on the chest.
Various Techniques For Managing Myofascial Pain Syndrome On The Sternalis Muscle
When a doctor examines the sternalis muscle, many individuals will often complain about experiencing chest and heart pain since the muscle is located in the front-middle of the chest. However, all is not lost, as various techniques can help relieve the pain along the sternalis muscle while managing myofascial pain syndrome. As stated earlier, trigger points can mimic other chronic conditions that can affect not only the muscle itself but the surrounding organs. Gently stretching the chest can help reduce the aches in the surrounding muscles and trigger point formation. Another technique that many people can incorporate is ischemic compression on the sternalis muscle combined with moist heat. The ischemic compression allows a sense of discomfort, but no pain should be inflicted to reduce pain symptoms and manage myofascial pain syndrome.
Conclusion
The sternalis muscle is located in the middle of the chest and helps the surrounding muscles to breathe and expand. This muscle works together with the pectoralis and the sternocleidomastoid muscle by attaching itself to these muscles in a unilateral or bilateral muscle. When traumatic forces or events affect the chest, this superficial muscle can be affected and develop myofascial pain syndrome that mimics cardiovascular disorders. Fortunately, various techniques like gentle chest stretch and ischemic compression can help manage trigger points and reduce pain in the chest.
References
Bell, Daniel J. “Accessory Muscles of Respiration: Radiology Reference Article.” Radiopaedia Blog RSS, Radiopaedia.org, 23 July 2022, https://radiopaedia.org/articles/accessory-muscles-of-respiration?lang=us.
Raikos, Athanasios, et al. “Sternalis Muscle: An Underestimated Anterior Chest Wall Anatomical Variant.” Journal of Cardiothoracic Surgery, BioMed Central, 16 May 2011, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3117696/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Verdon, François, et al. “Chest Wall Syndrome among Primary Care Patients: A Cohort Study.” BMC Family Practice, BioMed Central, 12 Sept. 2007, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2072948/.
The chest has the pectoralis major muscle that works with the upper half of the body that provides mobility and power. The pectoralis major also surrounds the clavicle skeletal structure and works with the thoracic spine. The chest allows mobility to the arms and stability to the shoulders while working together with the shoulder and arm muscles. Many individuals utilize the upper body more when working out, lifting, or carrying objects from one place to another. This causes the muscle to become overused and succumb to injuries that can affect the functionality of the chest and invoke pain-like symptoms in the body. One of the chest muscles affected by pain is the pectoralis muscles, especially the pectoralis minor muscle. Today’s article looks at the pectoralis minor muscle, how myofascial pain affects the pectoralis minor, and how to manage myofascial pain associated with the pectoralis minor. We refer patients to certified providers specializing in chest pain therapies to aid many people suffering from trigger point pain affecting the minor muscles of the pectoralis. We brief patients by referring them to our associated medical providers based on their examination when appropriate. We indicate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., notes this information as an educational service only. Disclaimer
The Pectoralis Minor Muscle
Have you been experiencing pain in your upper-mid back? Do you feel like your chest is feeling compressed constantly? Do you feel the tension in your shoulders that makes it difficult to reach behind your back? Most of these symptoms are signs that many individuals are developing myofascial pain along the pectoralis muscles, especially the pectoralis minor. The pectoralis minor muscle is a thin triangular-shaped muscle below the pectoralis major. It has a crucial part of the chest as it helps stabilize the scapula (the shoulder blades) and is in front of the thoracic wall of the spine. The pectoralis minor is also part of the respiratory muscle group that works with the lungs. The pectoralis minor muscle has many functions for the shoulder blades, which include:
Stabilization
Depression
Abduction or Protraction
Internal Rotation
Downwards Rotation
When environmental factors begin to affect the lungs and cause respiratory issues in the body, the surrounding respiratory muscle group also gets involved, causing the body to be hunched over.
Myofascial Pain Affecting The Pectoralis Minor
When environmental factors begin to affect the lungs, it causes the respiratory muscles to contract and become compressed. This is just one of the many factors that can affect the pectoralis minor muscle. The other factor is that the pectoralis minor muscle may be short in the chest and when individuals try to reach behind their backs. This causes the pectoralis minor muscle to to be overstretched and develop myofascial pain or trigger points along the muscle fibers. The book, “Myofascial Pain and Dysfunction,” written by Dr. Travell, M.D., described the pain from myofascial pain associated with the pectoralis minor to be similar to cardiac pain. This is known as referred pain caused by myofascial pain syndrome and it can be a bit difficult to diagnose since it can mimic other chronic issues. Studies reveal that shortening or any sort of tightness of the pectoralis minor is one of the potential biomechanical mechanisms that is associated with an altered scapular alignment which causes pain and shoulder movement impairments. Overusing the pectoralis minor muscles creates tiny nodules that can affect the stability of the shoulders and causes upper-mid back problems in the thoracic region of the spine.
An Overview Of Trigger Points On The Pectoralis Minor- Video
Have you been experiencing difficulty inreaching behind your back? Do you feeling your body becoming more hunched over than usual? Or have you been experiencing chest pain constantly? These pain-like symptoms are caused by myofascial pain associated with the pectoralis minor muscle. The pectoralis minor muscle helps with the stability of the shoulders and studies reveal that when the presense of myofascial trigger points are linked to shoulder and upper body disorders, it can increase the risk of overlapping conditions that trigger points can mimic. Myofascial trigger points are a common complaint as it can significantly impact a person’s daily activites by causing the taut muscle band to be tender or hypersenitive. When this happens, it can lead to issues of muscle imbalance, weakness and impaired motor function. Thankfully, there are various techniques that can help reduce the pain symptoms and issues in the pectoralis minor muscle, while mananging the trigger points. The video above explainshow to tell when your chest muscles are tight and various tests to know when the pectoralis muscles (both the minor and major) are being affected by trigger points.
Managing Myofacial Pain Associated With Pectoralis Minor
When dealing with chest pains associated with myofascial pain along the pectoralis minor, there are many techniques they can incorporate to prevent myofascial pain from causing further damage to the muscle itself and the surrounding muscles. Various chest stretches can help gently loosen the stiff muscles, warm the pectoralis minor, and improve mobility to the chest and shoulders. Correct posture can help prevent the body from being hunched over constantly and let the surrounding muscles and the pectoralis minor relax. If the pain is unbearable, studies reveal that treatments like dry needling and palpations on the pectoralis minor muscles can help manage the pain caused by trigger points. This kind of treatment allows the muscle to release the trigger point and, combined with a hot or cold pack, can reduce the chances of myofascial pain from forming again in the muscle.
Conclusion
Underneath the pectoralis major muscle, the pectoralis minor is a thin triangular-shaped muscle that helps stabilize the shoulder blades and is located in the front of the thoracic wall of the spine. This tiny muscle is part of the respiratory muscles that have a causal relationship with the lungs and can succumb to environmental factors that can lead to the development of myofascial pain or trigger points on the pectoralis minor. Myofascial pain associated with the pectoralis minor muscle can mimic cardiovascular issues and invoke pain in the muscle. Fortunately, various treatments can help relieve and manage myofascial pain from re-occurring in the pectoralis minor.
References
Bagcier, Fatih, et al. “Three Simple Rules in Pectoral Muscle’s Trigger Point Treatment, Which May Be a Cause of Chest Pain: Position, Palpation, and Perpendicular Needling.” American Board of Family Medicine, American Board of Family Medicine, 1 Nov. 2020, https://www.jabfm.org/content/33/6/1031.long.
Baig, Mirza A, and Bruno Bordoni. “Anatomy, Shoulder and Upper Limb, Pectoral Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 11 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK545241/.
Morais, Nuno, and Joana Cruz. “The Pectoralis Minor Muscle and Shoulder Movement-Related Impairments and Pain: Rationale, Assessment and Management.” Physical Therapy in Sport : Official Journal of the Association of Chartered Physiotherapists in Sports Medicine, U.S. National Library of Medicine, Jan. 2016, https://pubmed.ncbi.nlm.nih.gov/26530726/.
Ribeiro, Daniel Cury, et al. “The Prevalence of Myofascial Trigger Points in Neck and Shoulder-Related Disorders: A Systematic Review of the Literature.” BMC Musculoskeletal Disorders, BioMed Central, 25 July 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6060458/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
The chest in the upper half of the body comprises various structures that each have a job to keep the body functioning. The chest has different large muscles surrounding the ribcage and helps protect the vital organs that allow the host to breathe. The essential organs protected by the ribcage and the chest muscles include the heart and the lungs. These two organs aid the chest with blood circulation, breathing, and digestion to keep the body moving and functional. When injuries or chronic conditions begin to affect the chest, it can cause the muscles surrounding the ribcage to contract and tighten, causing the heart and lungs to work harder and causing various issues to affect the body. This can lead to chronic symptoms in the chest and affect a person’s life. Today’s article looks at the pectoralis major muscle in the chest, how trigger point pain is associated with chest pain, and how to manage trigger points in the chest. We refer patients to certified providers who specialize in chest pain therapies to aid many people suffering from trigger point pain affecting the pectoralis major muscles. We brief patients by referring them to our associated medical providers based on their examination when appropriate. We indicate that education is a great solution to asking our providers profound and complex questions at the patient’s request. Dr. Alex Jimenez, D.C., takes note of this information as an educational service only. Disclaimer
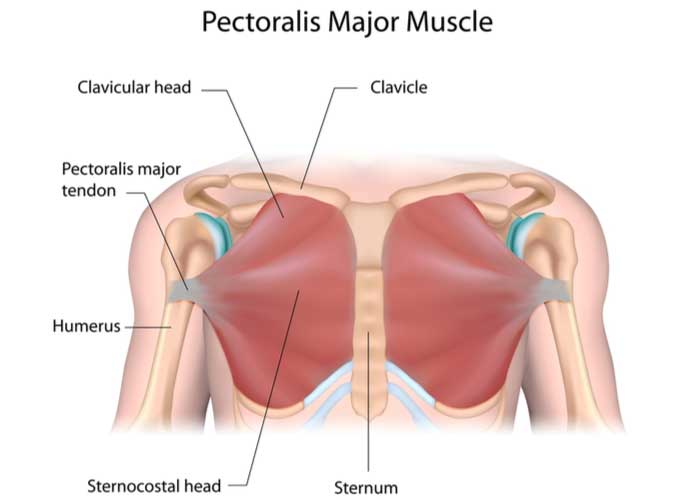
The Pectoralis Major Muscles In The Chest
Have you been experiencing unexplainable chest pains that mimic heart issues? Do you feel muscle stiffness near your clavicle? Or do your chest muscles feel tenser and sorer than usual? Many of these issues affecting the chest could result from trigger points associating with the chest along the pectoralis major muscles. The pectoralis major is the superior and largest muscle in the chest wall’s front area. This muscle looks like a thick fan that surrounds the clavicle and works with the chest and arms to provide mobility and power to the upper body. Studies reveal that the pectoralis major muscle plays an important role in upper limb movements. To that point, it can help with the adduction and medial rotation of the arm, according to the book by Dr. Travell, M.D. “Myofascial Pain and Dysfunction,” the pectoralis muscle works with the rest of the chest muscles while being assisted by the teres major and minor muscles, the anterior and posterior deltoid muscles, the subscapularis muscles, and the tricep muscles. The pectoralis major muscles can also be affected by multiple issues affecting the chest and the rest of the upper half of the body.
Trigger Point Pain Associated With The Chest
When the pectoralis major muscles are affected by various issues, they can mimic other chronic conditions that are causing referred pain in different body areas. This is known as trigger point pain, and it can cause overlapping risk profiles on the pectoralis major muscles that can affect the chest. Trigger points are slightly difficult to diagnose as many factors, like repetitive motions or lifting heavy objects, can cause the affected muscles to develop tiny knots along the muscle fibers and cause pain-like symptoms. Many people with chest pains often complain that something is affecting their heart as they place their hands on their chest and gently rub the affected area. However, when their doctors examine them, the issue is not their hearts but their chest muscles. Studies reveal that trigger points affecting the affected muscle can mimic issues like cardiovascular dysfunction in the heart. To that point, active trigger points in the pectoralis major muscle can cause somato-visceral pain to the heart, mimicking cardiovascular issues like paroxysmal arrhythmia. It can also cause visceral-somatic pain where the heart suffers from cardiovascular problems affecting the pectoralis major muscles.
Trigger Point Therapy On The Pectoralis Major-Video
Have you been dealing with chest pains that cause you to hunch over? Does your chest seem to feel tight when you stretch? Or have your chest muscles feel tender to the touch? These pain symptoms are caused by trigger points affecting the pectoralis muscles. Trigger points are generated when a person overuses their muscles from daily activities or succumbs to muscle injuries that cause referred pain in different body areas. So trigger points affecting the pectoralis major muscle may cause chest pains. The video above explains the pectoralis muscles and where the trigger points are located that cause referred pain to the shoulders and the rest of the upper half of the body. Trigger points associated with the chest along the pectoralis major muscles can be treatable through various treatments and techniques that can reduce the symptoms and prevent trigger points from forming along the affected muscle in the future.
Ways To Manage Trigger Points On The Chest
When trigger points affect the pectoralis major muscles, they can invoke chest pain-like symptoms that resemble a cardiovascular disorder. Fortunately, pain specialists like chiropractors, massage therapists, and physiotherapists can utilize various techniques to help reduce the pain caused by trigger points. Studies reveal that when local and referred pain affects the pectoralis major muscle, multiple massage treatments targeting the trigger points can help alleviate the symptoms causing chest pains. Another way people can manage trigger points is by stretching the pectoralis major muscle to relieve tension and soreness in the chest. Incorporating various stretching techniques to alleviate chest pain can help loosen up the stiff muscles and warm them up before a vigorous workout. This allows the pectoralis muscles to provide optimal output on a person’s health and wellness.
Conclusion
The pectoralis major is a thick fan-shaped muscle located on the chest. This muscle works with the shoulders and upper half of the body while protecting the heart and the lungs from various injuries and chronic conditions. When these muscles become affected by injuries or chronic conditions, they can develop trigger points along the chest, causing referred pain to the pectoralis major muscles. This can lead to somato-visceral and visceral-somatic pain symptoms in the chest and make many individuals miserable. Luckily pain specialists who can help manage trigger points along the affected muscle utilize various techniques to reduce the symptoms and prevent trigger points from forming in the affected muscle again. This allows the individual to continue with their daily activities without worrying about chest pains.
References
Haładaj, Robert, et al. “Anatomical Variations of the Pectoralis Major Muscle: Notes on Their Impact on Pectoral Nerve Innervation Patterns and Discussion on Their Clinical Relevance.” BioMed Research International, Hindawi, 2 Apr. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6466946/.
Moraska, Albert F, et al. “Responsiveness of Myofascial Trigger Points to Single and Multiple Trigger Point Release Massages: A Randomized, Placebo Controlled Trial.” American Journal of Physical Medicine & Rehabilitation, U.S. National Library of Medicine, Sept. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5561477/.
Simons, David G. “Cardiology and Myofascial Trigger Points: Janet G. Travell’s Contribution.” Texas Heart Institute Journal, U.S. National Library of Medicine, 2003, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC152827/.
Solari, Francesca, and Bracken Burns. “Anatomy, Thorax, Pectoralis Major Major.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 26 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK525991/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
Many people use their hands when going to work or doing normal things in their daily lives. The hands correlate with the five finger digits that provide grip strength when holding onto items in various sizes and weights that the hand muscles can handle. The hands have multiple muscles, tendons, and ligaments that travel past the wrist and forearms. These three components in the upper body have a casual relationship with the shoulders to provide stability and mobilization to the upper extremities. When the various muscles, tendons, and ligaments succumb to traumatic forces or injuries that cause pain to the forearms, wrists, and hands, it can develop myofascial pain syndrome or trigger points to generate overlapping risk profiles that mask other symptoms. Today’s article looks at the thumb muscles, how myofascial trigger pain affects the thumb, and how to prevent and manage the trigger thumb from occurring further in the hands. We refer patients to certified providers specializing in hand and wrist pain therapies to aid many people suffering from trigger thumb and fingers affecting their hands. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
A Look At The Thumb Muscles
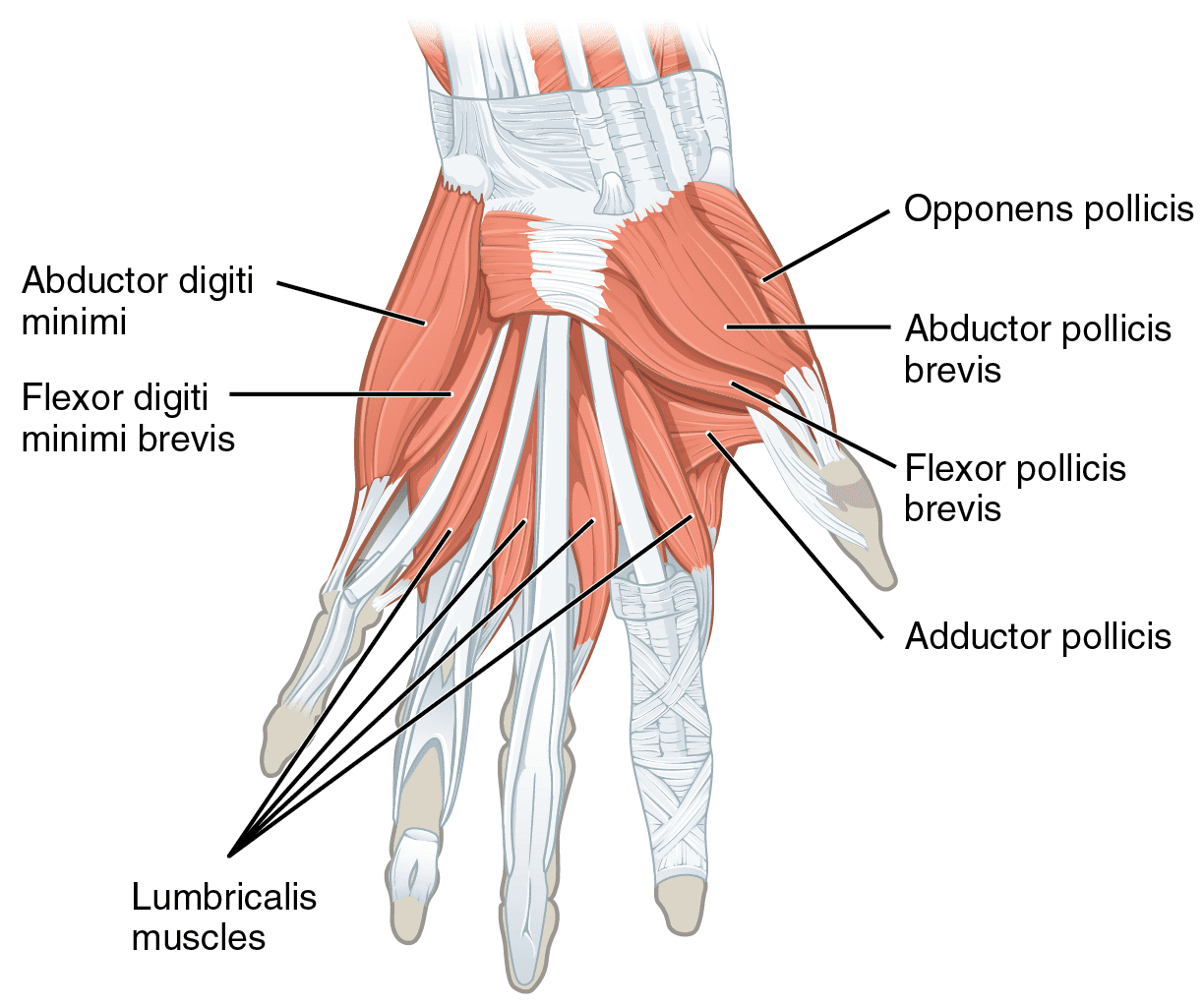
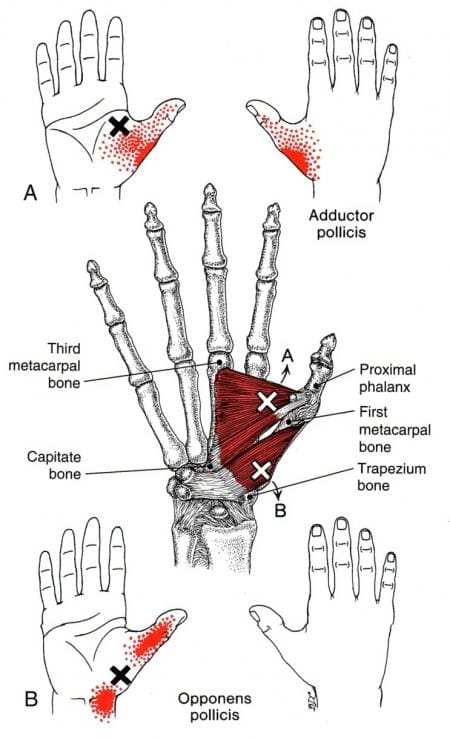
Have you been experiencing a strong decrease in your grip when holding something? What about hearing popping or snapping sounds when moving your fingers or thumb? Or have you experienced pain near your wrist or at the palm of your hands? When people are experiencing pain along their fingers, especially thumbs, it can develop into myofascial trigger pain along the thumb. As part of the hand, the thumb has muscles that provide movement and motor skills to make the thumb mobile. The two muscles: the adductor pollicis and the opponens pollicis, allow the thumb to move and touch each of the other finger digits. The adductor pollicis in the hand has deep, intricate, superimposed layers of muscles, tendons, and fascial compartments that work together to be versatile to the thumb. This muscle is triangular-shaped with a two-headed structure, and its main function is to adduct the thumb. This means that the adductor pollicis allows the thumb to move, touch the palm, and be close to the index finger. To that point, this muscle provides the thumb pinching and gripping movements.
The other muscle is known as the opponens pollicis, and this muscle helps provides small hand movements for the thumb by allowing it to touch the tips of each of the digits. The opponens pollicis muscle works together with the adductor pollicis muscle as it allows the hand to cup objects while also making the pinching grip possible for the hand. The oppponens pollicis muscle also works with the various muscles, nerves, and bones to be in sync in providing movement to the hands and provide mobility strength.
How Myofascial Trigger Pain Affects The Thumb
The adductor and oppenens pollicis muscles can provide gripping and pinching motions to the hands without causing pain; however, when the thumb muscle ligaments have been overused or been through trauma, they can develop into myofascial trigger pain along the thumb muscles, causing trigger thumb. Studies reveal that causes for the trigger thumb to form are repetitive gripping motions and overusing of the thumb muscle. This causes the flexor tendon sheath to narrow along the thumb joint and causes clicking or popping sensations when the thumb is trying to extend, thus leading to the development of myofascial trigger pain. According to the book, “Myofascial Pain and Dysfunction: The Trigger Point Manual,” written by Dr. Janet G. Travell, M.D., when myofascial trigger pain begins to affect the hand’s functionality, it can make many individuals lose the pinching motion in their hands as they aren’t able to hold the object they are using. Even simple actions like pulling weeds in the garden can cause stress on the thumb and cause tenderness to the affected muscle.
An Overview Of Trigger Finger & Trigger Thumb-Video
Are you having difficulty holding items in your hands? Do you feel like your fingers are locking up constantly? Or does it hurt when you extend your thumb or fingers? If you have been experiencing these pain symptoms in your hands and fingers, it could be due to myofascial trigger pain associated with the thumb and fingers along the hands. Trigger fingers or trigger thumbs is a common ailment that affects the mobility function of the hands and can invoke pain in the affected joints causing them to lock up. The video above explains what trigger fingers and trigger thumbs, the symptoms and causes, and how to treat and manage the pain. When pain is associated with the hands and fingers, causing trigger points to form along the affected muscle, many individuals begin to feel hopeless when they aren’t able to hold items. Thankfully, there are various ways to manage trigger thumb and prevent pain from causing further damage.
How To Manage & Prevent Trigger Thumb
When trigger thumb begins to affect a person’s ability to grasp objects, it can cause them to feel miserable and can greatly affect their quality of life. All is not lost, as there are various ways to manage trigger thumbs and prevent future pain symptoms from continuously affecting a person’s mobility in their hands. Studies show that multiple treatments like splinting can help gain mobility back to the thumb and prevent the joint from locking up, causing pain. Other therapies like hand and wrist stretches can help loosen up the stiff tendons and muscles and even bring back mobility strength to the hands. Many doctors advise their patients to start using different hand and wrist exercises to relax the aching muscles and get circulation back to the hands. Another way to prevent the trigger thumb from affecting the hands is to do stretch exercises for the adductor and opponens pollicis muscles with heat to relax and loosen the stiff muscles while also restoring flexion and extension to the thumb.
Conclusion
The thumbs provide the functionality to the hands by allowing gripping and pinching motions when people pick up objects. The two muscles that provide this motion are the adductor and oppnens pollicis muscles. When traumatic forces begin to affect these two muscles in the thumb, it can develop a trigger thumb associated with pain. This causes the thumb to lock up and invoke pain when someone tries to extend their thumbs. Trigger thumbs occur when individuals overuse the thumb muscles and causes the grip strength to weaken. Luckily, available treatments can help restore mobility to the thumb and prevent it from locking up.
Reference
Acosta, Jonathan R, et al. “Anatomy, Shoulder and Upper Limb, Hand Adductor Pollicis.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 11 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK526059/.
Akhtar, Sohail, et al. “Management and Referral for Trigger Finger/Thumb.” BMJ (Clinical Research Ed.), BMJ Publishing Group Ltd., 2 July 2005, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC558536/.
Nguyen, John D, and Hieu Duong. “Anatomy, Shoulder and Upper Limb, Hand Opponens Pollicis Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 11 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK546603/.
Pencle, Fabio J, et al. “Trigger Thumb.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 20 July 2022, https://www.ncbi.nlm.nih.gov/books/NBK441854/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 1:Upper Half of Body. Williams & Wilkins, 1999.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine