The hips and the thighs have an established relationship where mobility and stability play a part in the body’s lower extremities. The lower extremities’ main job is to support the upper body’s weight while stabilizing the hips and allowing movement from the thighs to the legs and feet. When it comes to the thighs in the lower body, the various muscle surrounds the thighs and skeletal joints to allow the legs to move from one place to another. One of the muscle groups in the thighs is known as the quadriceps femoris. This muscle group is activated when a person is in motion and can succumb to injuries from trauma or normal factors. When this happens, issues like myofascial pain syndrome can affect the thigh muscle and cause referred pain to travel to the knees. Today’s article focuses on the quadriceps femoris, how myofascial pain syndrome is associated with thigh pain, and trigger point therapy on the quadriceps. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like thigh and hip pain treatments correlating to myofascial pain, to aid individuals dealing with pain symptoms along the quadriceps for muscle. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Are The Quadriceps Femoris?
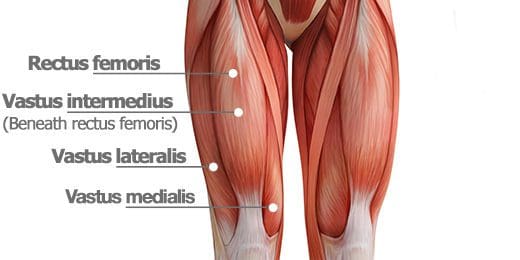
Have you been dealing with knee issues when you are walking? What about muscle tenderness or soreness in your thighs? Or have you been experiencing knee complaints when you are running? These areas of complaint are correlated with trigger points associated with thigh pain along the quadriceps femoris. As one of the most voluminous muscles in the human body, the quadriceps femoris is a group of muscles predominant in the thighs and is extraordinarily important. This muscle group is essential for daily activities like climbing the stairs or getting up from a seated position, allowing repercussions on the knees and hip joints. The quadriceps femoris consist of four thigh muscles to allow extension to the knees:
Vatus medialis
Vatus lateralis
Vatus intermedius
Rectus femoris
Studies reveal that these four different muscles fuse to form the quadricep tendon and stabilize the patella and thigh flexion at the hips and knee extension. This muscle group is highly important for athletes participating in sports events but can succumb to injuries through muscle strain.
Myofascial Pain Syndrome Associated With Tigh Pain
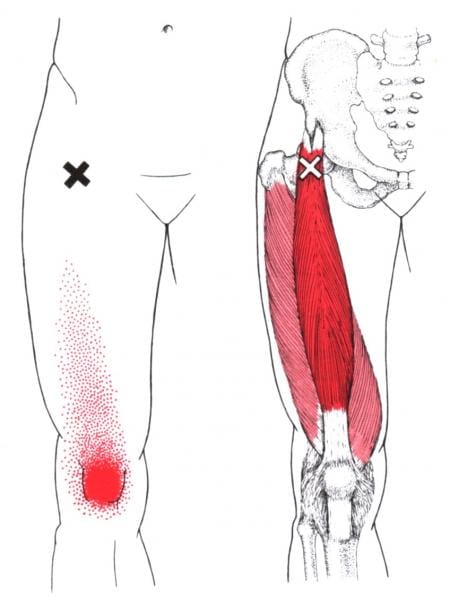
When the thigh muscles, especially the quadriceps femoris, can be overstretched and overused when in motion. Thigh pain is nothing to be alarmed about in its acute form; however, it can develop small nodules along the four muscle fibers that can cause referred pain to the hips and knees. To that point, it can correlate through quadriceps muscle strain to the thighs. Studies reveal that normal factors like kicking, jumping, or a sudden change of direction of running can potentially cause the muscle fibers to be overstretched and develop pain due to localized swelling corresponding to loss of motion from myofascial pain syndrome.
In “Myofascial Pain and Dysfunction,” written by Dr. Janet G. Travell, M.D., the book states that myofascial pain syndrome can invoke referred pain to the affected muscle or muscle group, causing the body to be dysfunctional. Myofascial pain syndrome associated with thigh pain can be managed through various treatments and could allow mobility back to the thighs, legs, knees, and hips. The book even mentions how the four muscles in the quadriceps femoris cause different pain issues in various body parts due to myofascial pain syndrome. For the rectus femoris, many people would complain about knee pain and weakness when climbing stairs. The vatus medialis would initially produce a toothache-like pain deep within the knee joint, often misinterpreted as joint inflammation. The vatus intermedius causes many individuals to have difficulty fully straightening their knees and causes them to develop buckling knee syndrome. And finally, the vatus lateralis could cause many individuals to complain about feeling pain when walking and that the pain is being distributed on the lateral aspect of the thigh, including the knees.
Trigger Point Therapy: Stretching The Quadriceps- Video
Have you been dealing with pain in your thighs and knees? Do you find it difficult to climb up or down the stairs? Or have you been experiencing inflammation in your knee joints? All these symptoms that you are experiencing in your thighs, knees, and hips correlate with trigger points created by myofascial pain syndrome affecting the quadriceps femoris. The quadriceps femoris is a voluminous group of muscles that allows the individual to do daily activities like climbing up or down the stairs, running, jumping, and getting up from a seated position. When various issues can cause the quadricep femoris to become overstretched and overused, it could develop myofascial pain syndrome/trigger points along the muscle fibers to mimic knee pain and cause dysfunction in knee mobility. Even though myofascial pain syndrome is poorly diagnosed, individuals can manage it through various treatments that target myofascial trigger pain. The video above explains where the quadriceps femoris muscles are located on the thigh and where the trigger points are in the muscle fibers. The video also provides various stretching techniques on the quadriceps to reduce pain-like symptoms along the thighs.
Trigger Point Therapy On The Quadriceps
When it comes to releasing myofascial pain syndrome on the quadriceps, treatments like dry needling, acupuncture, or manual stretching can help loosen and lengthen the quadricep muscles from becoming shorten and can reduce myofascial trigger points from causing more issues on the knees and thighs. At the same time, treatment alone can only go so far in rehabilitation unless the person dealing with myofascial pains syndrome associated with thigh pain do some corrective actions to prevent trigger points from reproducing on the quads. Actions like:
Avoid prolonged sitting
Stretching the quads as part of your warm-up
Sleeping with a pillow between the knees
These actions allow the quadriceps to relax and prevent pain-like issues from affecting the knees. To that point, these actions can help many individuals have mobility back to their legs and allow them to bend their knees without feeling pain.
Conclusion
The quadriceps femoris consists of four thigh muscles that fuse to enable mobility functions in the knees without pain. As the most voluminous muscle group in the body, the quadriceps femoris allows the thighs to function when in motion and allow the knees to extend. When various issues cause the quadriceps femoris muscles to be overstretched, it can develop trigger points/myofascial pain syndrome that mimics knee pain and can affect how a person is walking. Thankfully, various treatments specializing in myofascial pain syndrome can reduce the pain symptoms from the quadriceps femoris and bring back knee mobility to the legs.
References
Bordoni, Bruno, and Matthew Varacallo. “Anatomy, Bony Pelvis and Lower Limb, Thigh Quadriceps Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 10 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK513334/.
Kary, Joel M. “Diagnosis and Management of Quadriceps Strains and Contusions.” Current Reviews in Musculoskeletal Medicine, Humana Press Inc, 30 July 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2941577/.
Rozenfeld, Evgeni, et al. “The Prevalence of Myofascial Trigger Points in Hip and Thigh Areas in Anterior Knee Pain Patients.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, 14 May 2019, https://pubmed.ncbi.nlm.nih.gov/31987560/.
Simons, D. G., and L. S. Simons. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Waligora, Andrew C, et al. “Clinical Anatomy of the Quadriceps Femoris and Extensor Apparatus of the Knee.” Clinical Orthopaedics and Related Research, Springer-Verlag, Dec. 2009, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2772911/.
When many individuals begin to work out or start training for an event, they incorporate various muscles to give optimal output and strength when doing a set of exercises. Many athletes or individuals trying to train for an event or to better themselves have to do a pre-workout routine involving various stretches to warm up the muscles before the actual workout and do stretches post-workout again. This ensures that the muscles are ready to give it their all when a person is working out. The body has various parts with different functions and jobs that help the body’s motor function. The upper body has the shoulders, arms, hands, elbows, neck, head, and chest to allow movements and stability. At the same time, the lower body has the hips, low back, thighs, legs, knees, pelvis, and feet to support the upper body’s weight and stabilize the lower extremities from collapsing. When various factors affect the body, it can lead to dysfunction and causes referred pain to different body locations that can mask chronic conditions. Today’s article looks at one of the lower body muscles located at the inner thighs, known as the pectineus muscle, how trigger point pain affects the inner thighs, and various stretches to strengthen the hip adductors. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like thigh and hip pain treatments correlating to trigger point pain, to aid individuals dealing with pain symptoms along the pectineus muscle. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Pectineus Muscle?
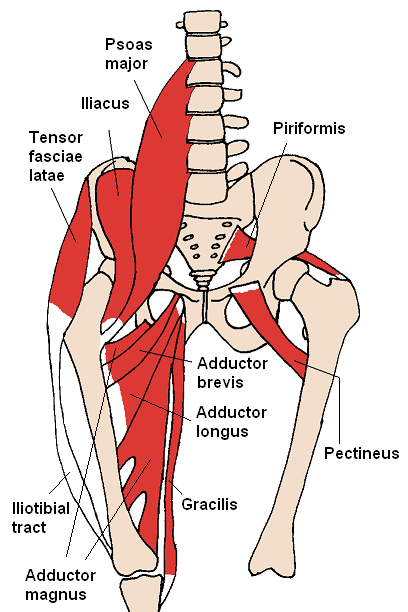
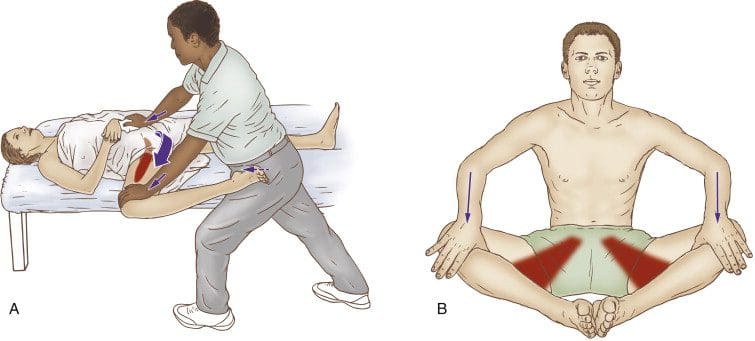
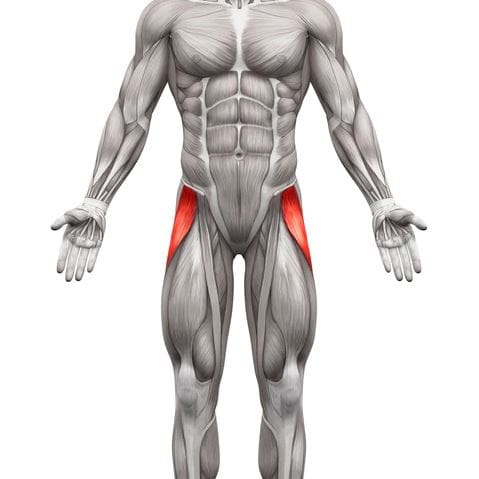
Have you been experiencing pain in your inner thighs? Do you find it difficult to play various sports? Do you feel tenderness or soreness in your thighs or near your groin? Most of these symptoms are associated with trigger point pain along the pectineus muscles that affect the thighs. The pectineus is part of the anterior thigh muscles that extend the leg to the knee joint. The pectineus works with another muscle known as the sartorius and a muscle group known as the quadriceps femoris. The pectineus muscle is responsible for flexion, adduction, and medial rotation since it is a hip adductor for the thighs. This muscle is important for various sports activities like running, skating, soccer, or basketball and can become overused due to overstretching the legs too far, thus developing trigger points in the pectineus muscle.
Trigger Point Pain Affecting The Inner Thighs
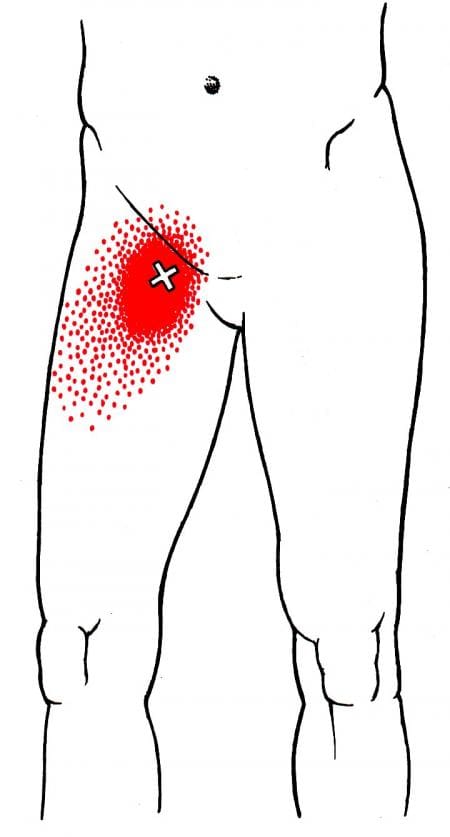
When athletes overuse their legs and overstretch the pectineus muscle, it can cause issues with the thighs, hips, and legs’ mobility causing referred pain to the lower body. This is known as trigger point pain and can be challenging when diagnosing where the pain is located. Studies reveal that trigger point pain affecting the inner thighs, especially the pectineus muscle, can mimic groin and hip pain, causing various symptoms in the lower extremities. The multiple symptoms can include:
Weak adductor muscles
Muscle fatigue
Decreased range of motion
Leg-length discrepancy
Various reasons can lead to the development of trigger point pain associated with the inner thighs along the pectineus; according to “Myofascial Pain and Dysfunction,” written by Dr. Janet G. Travell, M.D., stated that when patients are dealing with pectineus trigger points would complain about the referred pain surrounding the muscle but not the muscle itself. The book also mentioned that nerve entrapment could also be an issue since trigger points like to mimic other chronic conditions. Trigger points along the pectineus muscle can also develop associated with hip joint diseases like advanced osteoarthritis.
Treating Trigger Points In Hip Adductors- Video
Are you experiencing issues when moving around constantly? Do you experience pain in your inner thighs and hips? Or do you have difficulty rotating your thighs or hips? If you have been dealing with these issues throughout your entire life, it could be due to your pectineus muscles being affected by trigger points along your inner thighs. Trigger points (myofascial pain syndrome) develop tiny nodules along the muscle fibers, causing referred pain to the surrounding muscles that can cause dysfunction in the lower extremities. Studies reveal that myofascial trigger points can cause the affected muscles to be intensely sensitive and irritable, predominantly near the reflex muscle. To that point, it causes hip and thigh disability in the lower body. Fortunately, there are ways to reduce the pain and manage the trigger point pain along the pectineus muscle, as shown in the video above. The hip adductor muscles are being stretched and treated for trigger point pain and allowing mobility back to the hips and inner thighs.
Various Stretches To Strengthen Hip Adductor
Since the pectineus muscle is part of the hip adductor muscles, various stretches can reduce the chances of trigger points from future development while minimizing the pain that it is causing along the surrounding muscles. Studies reveal that multiple exercises and stretches for the pectineus muscle can help with hip flexion and stabilization. These stretches can help stretch and strengthen the hip adductor muscles while preventing groin pain associated with trigger points. Incorporating these stretches before and after a workout can reduce trigger points and allow hip mobility and thigh rotation back to the legs. This ensures that the trigger points along the pectineus muscle are managed, and the individual doesn’t have to suffer from referred pain issues on the thighs and can move around without pain.
Conclusion
As part of the hip adductor muscles, the pectineus is a small muscle that extends the leg to the knees and allows the thighs to flex, adduct, and rotate without pain. This muscle is important for many athletes participating in sports and can be easily overstretched to cause referred pain around the thighs. To that point, it can develop trigger points along the pectineus muscles can correlate to groin pain in the lower extremities. All is not lost, as various stretches and exercises can strengthen the hip adductor muscles and improve thigh and hip mobility. This allows athletes and individuals to continue playing the sport they enjoy.
References
Giphart, J Erik, et al. “Recruitment and Activity of the Pectineus and Piriformis Muscles during Hip Rehabilitation Exercises: An Electromyography Study.” The American Journal of Sports Medicine, U.S. National Library of Medicine, July 2012, https://pubmed.ncbi.nlm.nih.gov/22523373/.
Khan, Ayesha, and Abdul Arain. “Anatomy, Bony Pelvis and Lower Limb, Anterior Thigh Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 10 June 2022, https://www.ncbi.nlm.nih.gov/books/NBK538425/.
Kiel, John, and Kimberly Kaiser. “Adductor Strain.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 21 June 2022, https://www.ncbi.nlm.nih.gov/books/NBK493166/.
Simons, D. G., and L. S. Simons. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Wada, Juliano T, et al. “An Anatomical Basis for the Myofascial Trigger Points of the Abductor Hallucis Muscle.” BioMed Research International, Hindawi, 22 Jan. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6998759/.
The lower body extremities help provide stability to the various body parts, including the hips, thighs, pelvis, legs, knees, and feet. The hips and thighs comprise multiple muscles and nerves that provide mobility to the lower half and allow the host to move around in different locations. While the hip muscles act on the thigh muscles at the hip joint and stabilize the pelvis, the thigh muscles allow the lower body to bend, flex and rotate while bearing most of the upper body’s weight and keeping alignment with the hips and legs. One of the thigh muscles is the sartorius muscle, and if it becomes overused and injured can lead to complications in the form of myofascial pain syndrome. Today’s article post examines the sartorius muscle, how myofascial trigger pain is associated with the sartorius, and the effectiveness of myofascial pain treatment on the thighs. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like thigh pain treatments correlating to myofascial pain syndrome, to aid individuals dealing with pain symptoms along the sartorius muscle. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Sartorius Muscle?
Are you experiencing pain in the upper, mid, or lower parts of your thighs? Do you have difficulty walking for long periods? Or do your knees hurt more than usual? Most of these issues correlate with myofascial trigger pain associated with the sartorius muscle. As the longest muscle that spans from the hips to the knee joints, the sartorius muscle, or the “tailor muscle,” serves as both a hip and knee flexor while working with other muscles that allow hip mobility. The sartorius shares its origin location with the TFL (tensor fascia latae) muscle at the anterior superior iliac spine and is responsible for internal rotation at the hips. In the book, “Myofascial Pain and Dysfunction,” the author Dr. Janet G. Travell, M.D., mentioned that the sartorius muscle assists the iliacus and the TFL muscles in hip flexion while assisting the short head of the bicep femoris in the knees for knee flexion, allowing the individual to walk for long distances. Even though this long muscle assists in hip and knee flexion, it can succumb to injuries and create issues with the hips and knees in the lower body.
Myofascial Trigger Pain Associated With The Sartorius Muscle
When traumatic forces or normal factors begin to affect the sartorius muscle, the surrounding muscles on the thighs and hips are also affected. The sartorius muscle allows the individual to move around and allows flexion to the hips and knees when injuries or the muscle is being overused; it can cause pain-like symptoms that correlate with hip and knee issues associated with myofascial trigger pain. Myofascial trigger pain along the sartorius muscle doesn’t usually occur in the muscle but can occur in conjunction with trigger point involvement in the surrounding muscles. Studies reveal that myofascial trigger pain is found in the hip muscles and can cause issues in the lumbopelvic-hip muscles of the lower body. This causes referred pain on the sartorius to be more diffused and superficial to the knees. When myofascial trigger pain is associated with the sartorius, many individuals often mistake it for knee pain. To that point, myofascial trigger pain could affect how a person walks and bends at the knees.
Anatomy & Palpation Of The Sartorius Muscle- Video
Are you experiencing issues when you are walking? Do your knees hurt constantly? Or are you experiencing tenderness or pain in your thighs? Most of these issues correlate with myofascial trigger pain associated with the sartorius muscle. The sartorius is a long muscle that connects the hips and spans to the knee joints to provide hip and knee flexion. The sartorius muscle works with the other muscles in the thighs and hips, allowing hip mobility and motor function to the legs. When multiple issues affect the sartorius and the surrounding muscles, it can develop into myofascial trigger pain and cause overlapping risk profiles to the knees and hips. To that point, it causes referred pain issues in the hips and knees, making the individual have difficulty walking from place to place. However, there are available treatments to reduce the pain in the hips and knees and manage the myofascial trigger pain from affecting the sartorius muscle on the thighs. The video above explains the anatomy of the sartorius muscle location and how palpation is used to locate the muscle to see if it is tight or could be affected by trigger points along the muscle fibers. This is one of the techniques that is used when a person is dealing with myofascial trigger pain associated with the sartorius muscle.
The Effectiveness Of Myofascial Pain Treatment On The Thighs
When a person is dealing with myofascial trigger pain in their thighs, and it is affecting the sartorius, many will often try to find available treatments to alleviate the pain. Treatments like dry needling are one of the various myofascial pain treatments that can reduce pain and related disability on the thighs, hips, and knees. Studies reveal that dry needling treatments can help manage knee pain syndrome associated with trigger points on the thighs. However, treatment alone can not be the only solution to reduce myofascial trigger pain in the thighs. Various hip stretches can loosen up tight hip flexors and help elongate the sartorius muscles to break up the nodules and improve mobility function to the hips and knees. People can even utilize self-ischemic compression to allow a more effective stretch on the sartorius muscle.
Conclusion
As the longest muscle in the thighs, the sartorius helps provide a service to hip and knee flexion while working with various muscles to keep the legs moving. When the sartorius muscles become overused and start to cause referred pain to the hips and knees, it can develop into myofascial trigger pain along the sartorius muscle. This can make many individuals believe they are suffering from knee pain when it’s their thigh muscle. However, myofascial trigger pain is treatable through treatments and corrective actions that people can incorporate into their daily activities to prevent pain from escalating and manage trigger points along the sartorius muscle. This can allow people to get back their mobility in their legs.
References
Rahou-El-Bachiri, Youssef, et al. “Effects of Trigger Point Dry Needling for the Management of Knee Pain Syndromes: A Systematic Review and Meta-Analysis.” Journal of Clinical Medicine, MDPI, 29 June 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7409136/.
Samani, Mahbobeh, et al. “Prevalence and Sensitivity of Trigger Points in Lumbo-Pelvic-Hip Muscles in Patients with Patellofemoral Pain Syndrome.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, 15 Oct. 2019, https://pubmed.ncbi.nlm.nih.gov/31987531/.
Simons, D. G., and L. S. Simons. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Walters, Benjamin B, and Matthew Varacallo. “Anatomy, Bony Pelvis and Lower Limb, Thigh Sartorius Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 29 Aug. 2022, https://www.ncbi.nlm.nih.gov/books/NBK532889/.
The thighs in the lower half of the body work together with the hips to stabilize the legs when the body is in motion. The thighs and the hips also support the weight of the upper half of the body and are surrounded by muscles, ligaments, and nerve roots to supply blood and sensory-motor function to the legs. One of the thigh muscles that work with the hips is the tensor fasciae latae (TFL) muscle. When the thigh muscles are being overused or suffer from injuries, tiny nodules known as trigger points (myofascial pain syndrome) can affect a person’s ability to function worldwide. Today’s article examines what the tensor fasciae latae muscles do, how myofascial pain syndrome affects the thighs, and various stretches/techniques for the thighs. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like thigh pain treatments correlating to trigger points, to aid individuals dealing with pain symptoms along the tensor fasciae latae muscle. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Does The Tensor Fasciae Latae Muscle Do?
Do you have difficulty walking for a long period? So you feel that your hips feel unstable when you move? Or do you feel radiating pain down from your thighs to your knees? Thigh pain associated with these symptoms can affect a person’s ability to move around from one location to another due to trigger points affecting the tensor fasciae latae muscle. The tensor fasciae latae (TFL) muscles are located at the proximal anterolateral thigh and originate from the anterior superior iliac spine. The TFL muscle is between the superficial and deep muscle fibers of the iliotibial (IT) band, as its attachment assists with knee flexion and lateral rotation. The TFL muscles also work together with the gluteus muscles in various hip movements. Studies reveal that the primary function of the TFL muscles is providing balance to the body’s weight and the non-weight-bearing leg to walk. The TFL muscles allow the individual to walk, run, and assist with movement and stabilization to the hips and knees without pain inflicted on the joints and muscles.
Myofascial Pain Syndrome Affecting The Thighs
Since the TFL muscles allow the person to walk and run, this muscle can become overused and strained through repetitive motions causing many issues to the hips, knees, and thighs. When these issues affect the TFL muscles, they can develop nodules along the muscle fibers known as trigger points or myofascial pain syndrome. Myofascial pain syndrome is a musculoskeletal disorder that can invoke referred pain in one location of the body while affecting the surrounding muscles in a different body location. Myofascial pain syndrome associated with the TFL muscles can cause issues to the hips, thighs, and knees while affecting a person’s ability to walk. Studies reveal that the prevalence of myofascial pain syndrome on the TFL muscles correlates to pain and disability in the thighs. When myofascial pain syndrome affects the TFL muscles, it can mimic chronic knee osteoarthritis.
Even though myofascial pain syndrome is challenging to diagnose, it is treatable through various stretches and techniques. In Dr. Janet G. Travell, M.D.’s book, “Myofascial Pain and Dysfunction,” it mentioned that when patients have active trigger points in their TFL muscles, they become aware of the referred pain affecting their hip joints and are unable to lie comfortably on their sides due to the body-weight pressure pressing on the affected TFL muscle. The book also points out that when pain is referred to from trigger points associated with the TFL muscles, it can be mistaken for pain in the glutes.
Trigger Point Of The Week: Tensor Fasciae Latae- Video
Have you been experiencing difficulty walking from one location to another? Do you feel pain in your thighs or knees? Or do you have a problem lying down on your side that is causing you pain? If you have been dealing with walking issues, it could be due to myofascial trigger pain in your tensor fasciae latae (TFL) muscles affecting your ability to walk. The TFL muscles help provide stability to the hips and thighs and assist with knee flexion and lateral rotation. This muscle also allows people to walk and run without any pain inflicted on the joints and muscles. When repetitive motions start to cause the TFL muscles to become overused and strained, it can lead to myofascial pain syndrome or trigger points developing, causing referred pain to the thighs. The video above explains where the TFL muscles are located and where the trigger points on the TFL muscles are causing pain to the thighs. Myofascial pain syndrome can mimic other chronic conditions like knee osteoarthritis, which causes pain and disability to the lower half of the body.
Various Stretches & Techniques For The Thighs
Now myofascial pain syndrome is challenging to diagnose in an examination due to the referred pain affecting one location of the body than the actual source of where the pain is coming. However, it is treatable through various techniques and stretches for the thighs to restore leg mobility. Studies reveal that direct stretching of the TFL (tensor fasciae latae) muscles can reduce long-term pain effects on the hips, thighs, and lower back and improve hip and thigh mobility. Various stretches like hip extensions and laterally rotating the hips can break the myofascial trigger points in the TFL muscle. Using a foam roller on the hips can gently stretch and loosen the muscle fibers on the TFL and help warm up the muscle before working out. Sitting down correctly in a chair can help the hips from causing more muscle strain to the thighs and prevent the TFL muscles from being shortened. Incorporating these stretches and techniques can improve hip and thigh mobility in the legs, allowing the individual to walk or run without pain.
Conclusion
The TFL (tensor fasciae latae) muscles are located on the proximal anterolateral thigh between the IT (iliotibial) band, which assists with knee flexion and lateral rotation. The TFL muscle also works with the gluteal muscles and allows the person to walk, run, and help with stability movement to the hips and knees with inflicted pain on the joints and surrounding muscles. When the TFL muscles become overused, they can develop myofascial trigger pain on the TFL, causing referred hip, knee, and thigh pain. This can cause the individual not to be able to walk for long periods and think they might have osteoarthritis in the knees. Fortunately, people can incorporate various stretches and techniques to reduce the pain in the thighs and hips while managing myofascial trigger pain along the TFL muscles. These various stretches and techniques allow mobility back to the hips and thighs so the individual can walk without pain.
References
Gottschalk, F, et al. “The Functional Anatomy of Tensor Fasciae Latae and Gluteus Medius and Minimus.” Journal of Anatomy, U.S. National Library of Medicine, Oct. 1989, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1256751/.
Ohtsuki, Keisuke. “A 3-Month Follow-up Study of the Long-Term Effects of Direct Stretching of the Tensor Fasciae Latae Muscle in Patients with Acute Lumbago Using a Single-Case Design.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, May 2014, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4047246/.
Simons, D. G., and L. S. Simons. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Sánchez Romero, Eleuterio A, et al. “Prevalence of Myofascial Trigger Points in Patients with Mild to Moderate Painful Knee Osteoarthritis: A Secondary Analysis.” Journal of Clinical Medicine, MDPI, 7 Aug. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7464556/.
Trammell, Amy P, et al. “Anatomy, Bony Pelvis and Lower Limb, Tensor Fasciae Muscle – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 8 Aug. 2022, https://www.ncbi.nlm.nih.gov/books/NBK499870/.
The lumbar region of the spine has various muscles and nerve roots that work together with the lower body extremities, like the hips, buttocks, legs, knees, and feet, for mobility and walking function. The various muscles in the buttock region include the gluteal muscles. They have a casual relationship with the hip muscles as they work together for hip mobility and erect good posture in the body. These various muscles and nerves also supply sensory-motor function for the legs to be mobile and provide hip mobility. The piriformis is one of the muscles assisting in the hips and buttock region. When this muscle becomes overused, it can cause mobility issues in the legs and affect a person’s ability to walk. Today’s article looks at the piriformis muscle, how trigger points are associated with piriformis syndrome, and how to manage piriformis syndrome associated with trigger points. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like sciatic pain and piriformis syndrome treatments related to trigger points, to aid individuals dealing with pain symptoms along the piriformis muscle. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Piriformis Muscle?
Have you been having issues walking from one place to another? Do you feel muscle tightness in your hips or buttock region? Or are you experiencing radiating pain traveling to your knees and feet? These pain symptoms are correlated with trigger points affecting the piriformis muscle. The piriformis is a flat, pear-shaped muscle, one of the six short rotator muscle groups in the gluteal region of the hips and thighs. The rotator muscle groups consist of the following:
Gemelli
Quadratus Femoris
Obturator Internus
Obturator Externus
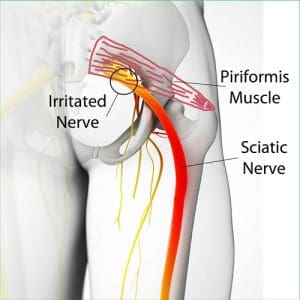
This muscle is parallel to the posterior margins of the gluteus medius and deep into the gluteus maximus. This muscle is very important to the body as it provides lower-body movement by stabilizing the hip joint and can lift and rotate the thighs away from the body. The piriformis muscle also surrounds the sciatic nerve, as this long nerve runs deep beneath the piriformis and enters the gluteal region of the rear. When the piriformis muscle becomes overused or suffers from associated traumatic factors, it can aggravate the sciatic nerve and even develop tiny nodules known as trigger points, causing mobility issues.
Trigger Points Associated With Piriformis Syndrome
When abnormal factors affect the piriformis muscles, they can develop into trigger points associated with piriformis syndrome and cause issues in the pelvic and hip regions of the body. According to Dr. Janet G. Travell, M.D., “Myofascial Pain and Dysfunction,” trigger points can be activated when repetitive strain affects the piriformis muscle and causes symptoms of muscle weakness and pain in the hips. This causes overlapping issues in the surrounding muscles and the sciatic nerve, making diagnosing tricky for trigger points. Studies reveal that trigger points associated with piriformis syndrome may potentially cause muscle spasms or an inflammatory process to irritate the sciatic nerve that may be presented as identical to lumbar disk syndrome without neurological findings. Trigger points associated with piriformis syndrome may mimic chronic issues like fibromyalgia. Even though trigger points are tricky to pinpoint in a thorough examination, there are various ways to reduce the pain and prevent trigger points from affecting the piriformis muscle causing sciatic nerve pain.
Trigger Point Of The Week: Piriformis Muscle- Video
Have you been dealing with sciatic nerve pain? Have you found it difficult to walk for a short period? Or are you dealing with muscle tenderness or soreness in your buttock or hips? People experiencing these symptoms could be dealing with piriformis syndrome associated with trigger points. The piriformis is a small, fan-shaped muscle, one of the six short rotator muscle groups that help with hip and thigh mobility through stabilization. The piriformis muscles also surround the sciatic nerve and can succumb to injuries. When traumatic forces affect the hips and thighs, the piriformis muscle develops nodules known as trigger points, causing the muscle to irritate the sciatic nerve and cause pain in the legs. The video above shows where the piriformis muscle is located and how trigger points can mimic sciatic nerve pain in the leg without neurological findings. Studies reveal that trigger points could be a rare anatomical variation that can correlate with piriformis syndrome associated with sciatica. However, there is some good news, as there are ways to manage piriformis syndrome associated with trigger points.
Managing Piriformis Syndrome Associated With Trigger Points
Various techniques can help manage piriformis syndrome associated with trigger points to relieve the piriformis muscle. Studies reveal that Kinesio tape on the piriformis muscle can help reduce pain and improve many individuals’ hip joint range of motion. Other techniques like stretching or deep tissue massage can help loosen up the stiff muscles and relieve trigger points from forming on the piriformis. For sciatica pain associated with trigger points along the piriformis muscle, decompression therapy can help the piriformis muscle lay off pressure on the sciatic nerve and reduce aggravated pain. These techniques can help improve hip joint mobility and increase the range of motion to the hips and lower extremities.
Conclusion
The piriformis is a small muscle that provides hip and thigh mobility. This small muscle surrounds the sciatic nerve, which helps give motor function to the legs. When traumatic factors affect the piriformis muscle, it can develop trigger points and cause sciatic pain in the hips. This causes mobility issues and pain around the hips. Various treatments are provided to help reduce the trigger points along the piriformis muscle and reduce sciatic nerve pain from causing more problems to the hips and legs mobility.
References
Chang, Carol, et al. “Anatomy, Bony Pelvis and Lower Limb, Piriformis Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 3 Oct. 2022, https://www.ncbi.nlm.nih.gov/books/NBK519497/.
Pfeifer, T, and W F Fitz. “[The Piriformis Syndrome].” Zeitschrift Fur Orthopadie Und Ihre Grenzgebiete, U.S. National Library of Medicine, 1989, https://pubmed.ncbi.nlm.nih.gov/2618150/.
R;, Hashemirad F;Karimi N;Keshavarz. “The Effect of Kinesio Taping Technique on Trigger Points of the Piriformis Muscle.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, 8 Feb. 2016, https://pubmed.ncbi.nlm.nih.gov/27814861/.
Ro, Tae Hoon, and Lance Edmonds. “Diagnosis and Management of Piriformis Syndrome: A Rare Anatomic Variant Analyzed by Magnetic Resonance Imaging.” Journal of Clinical Imaging Science, Medknow Publications & Media Pvt Ltd, 21 Feb. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843966/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The buttock and the lower back have a casual relationship to the body, as the lower back has various muscles and nerves surrounding the spinal column. In contrast, the buttock region has multiple muscles and the sciatic nerve to keep the body upright. The sciatic nerve travels from the lumbar region of the spine across the gluteus muscles and down to the legs. The gluteus muscles include the Maximus, medius, and minimus, and they work with the sciatic nerve regarding good posture. When normal or traumatic factors begin to affect the body, like sciatica or poor posture, it can lead to developing trigger points associated with the gluteus minimus affecting the sciatic nerve. Today’s article examines the gluteus minimus, how trigger points mimic sciatic pain on the gluteus minimus, and various treatments to relieve sciatic nerve pain. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like sciatic pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the gluteus medius muscles associated with sciatica. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Gluteus Minimus?
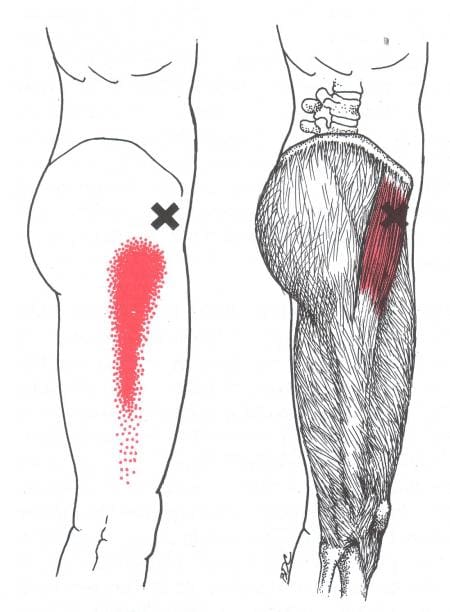
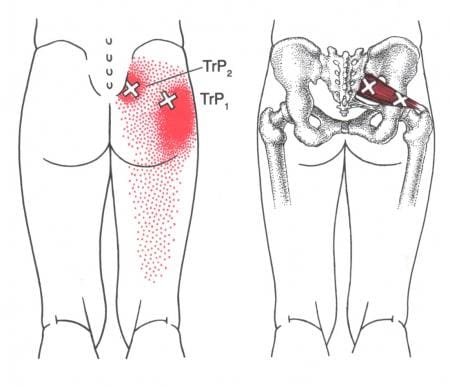
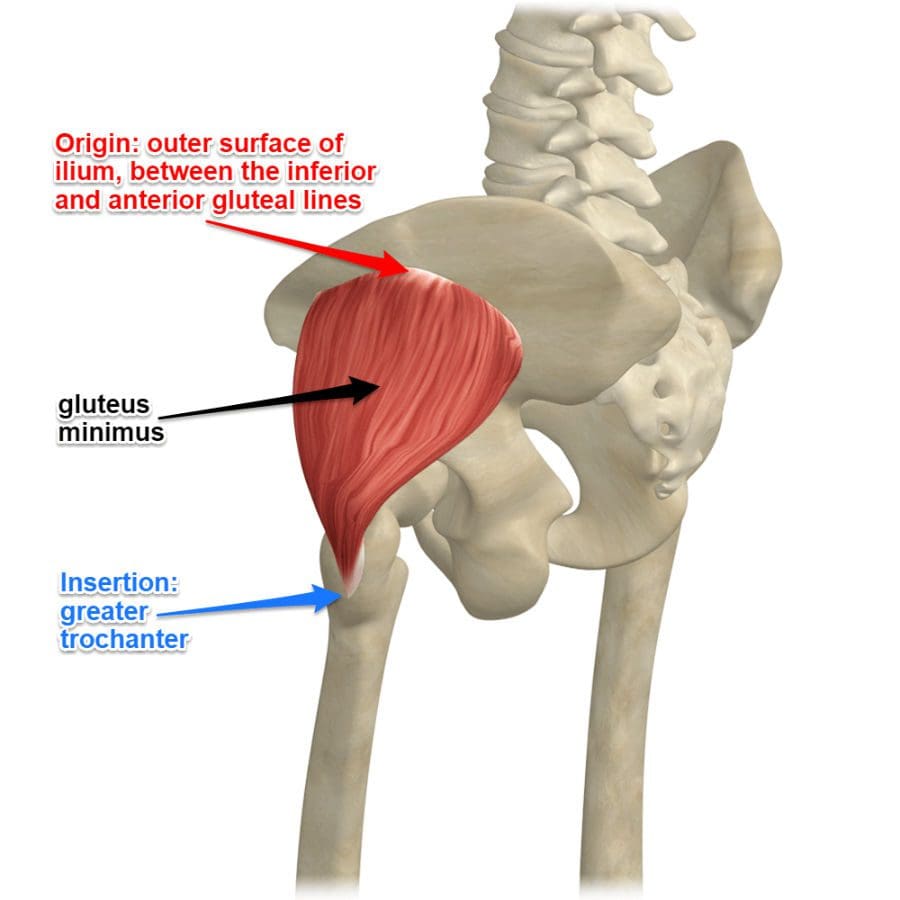
Have you been experiencing radiating pain traveling down to your leg? Do you have difficulty walking or sitting down? Do you feel tenderness or referred pain near your buttock region? Some of the issues correlate with trigger points affecting the gluteus minimus, causing pain in the sciatic nerve. As the smallest muscle in the gluteal region of the buttock, the gluteus minimus shares similar characteristics to the gluteus medius while being located beneath the medius muscle. One of the primary functions of the gluteus minimus is that it predominantly acts as a hip stabilizer and abductor. The nerves from the gluteal muscles include the sciatic nerve, which is on top of the gluteus muscles and the other nerves help supply the muscles to function in the posterior region of the body. Studies reveal that the structural integrity of the gluteus minimus muscles is the key to the lateral hip muscle, which contributes to pelvic stability and lower extremity function. However, when issues affect the gluteal muscles’ posterior region could trigger point pain mimicking sciatica.
How Trigger Points Mimic Sciatic Pain On The Gluteus Minimus?
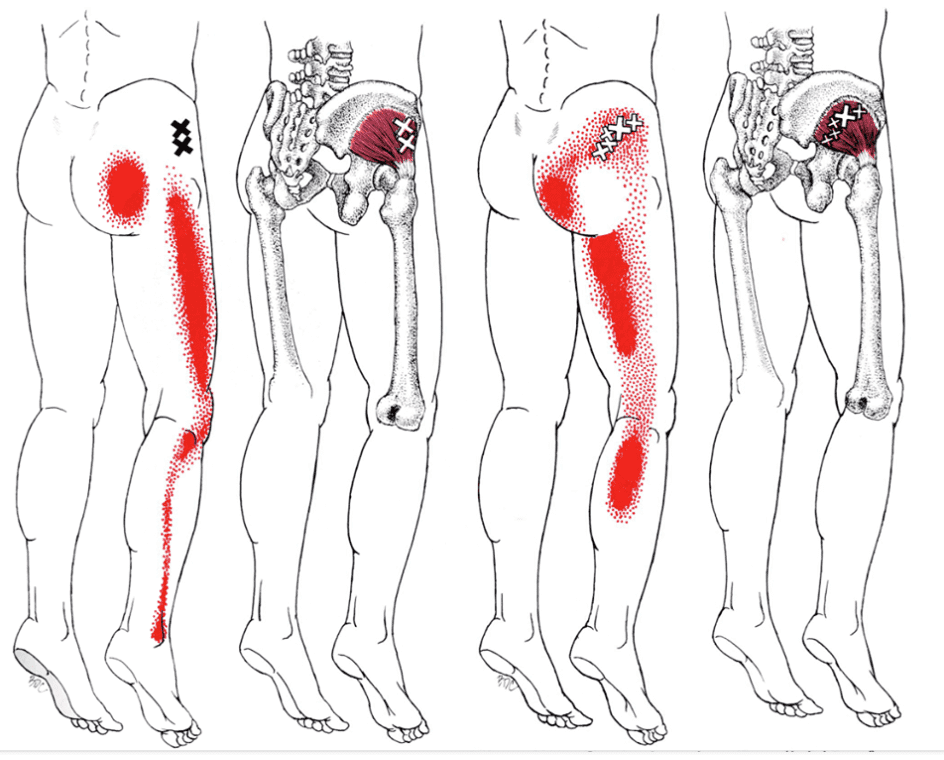
When the lower body extremities begin to suffer from multiple issues that cause the individual to have mobility dysfunction, various factors could correlate to the dysfunction. When the gluteus minimus muscles have been overused or been through a traumatic experience, they can develop trigger points along the muscle fibers and even cause nerve entrapment along the sciatic nerve. Trigger points along the gluteus minimus can mimic sciatic nerve pain down to the back or even the side of the legs that causes excruciating and deep pain in the posterior region. Studies reveal that pain in the buttock region is a deep gluteal syndrome caused by non-discogenic pain that causes sciatic nerve entrapment.
The book, “Myofascial Pain and Dysfunction,” written by Dr. Janet G. Travell, M.D., states that many patients with active trigger points located in their gluteus minimus would complain about hip pain that could cause them to limp-walk when they are going to places. The pain caused by the active trigger points can make it difficult to stand up from a seated position due to the painful movements. The associated pain that the trigger points are causing to the gluteus minimus can be constant and excruciating; even small stretches can not alleviate the pain. The book also mentioned that trigger points could cause referred pain to the gluteus minimus that can cause various somato-visceral issues to the hips, legs, and knees if the pain worsens.
Sciatic Type Pain: Gluteus Minimus Trigger Points- Video
Are you dealing with pain in your hips, low back, and legs? Do you find it difficult to walk or stand up constantly? Or are you experiencing sciatic nerve pain that is radiating down your leg? All these pain-like symptoms are associated with trigger points along the gluteus minimus affecting the sciatic nerve. The gluteus minimus is the smallest of the gluteal muscles with the same function as the gluteus medius and predominately acts as the hip’s stabilizer and abductor. When the gluteus minimus muscles have been overused from traumatic events or normal factors, they can develop trigger points in the muscle fibers, entrap the sciatic nerve and irritate the nerve causing sciatica. The video above explain where the gluteus minimus is located and pinpoints where the trigger points are in the muscle fibers. Trigger points along the gluteus minimus can mimic sciatica by causing referred pain to travel down the leg. This can cause the individual to be unable to walk or even stand up due to the excruciating pain that they are in. Luckily, trigger points are treatable even though they are tricky to diagnose.
Various Treatments To Release Sciatic Nerve Pain
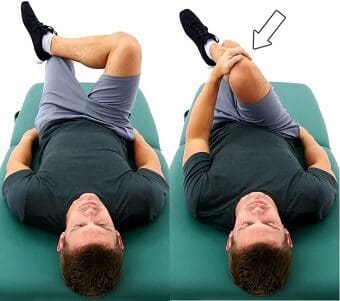
Even though trigger points along the gluteus minimus are tricky to diagnose, they are treatable through various treatments to alleviate the pain that the person is experiencing and can reduce sciatic nerve pain from causing more issues in the legs. Studies reveal that the effectiveness of active soft tissue release and trigger point block treatments combined can release entrapped nerves from the gluteus minimus and reduce low back and sciatic pain from the lower extremities. Now the treatments alone can only do so much to the individual, as many doctors tell their patients to take corrective actions or techniques to reduce the chances of trigger points from forming again on the gluteus minimus. Techniques like glute stretches, ischemic compressions, or using a foam roller can break the myofascial triggers from the gluteus minimus muscles and reduce the pain in the glutes and legs. This will help bring mobility back to the lower extremities.
Conclusion
As the smallest muscle in the body’s gluteal region, the gluteus minimus is the lower body’s predominant hip stabilizer and abductor. The gluteus minimus contributes to pelvic stability and lower extremity functionality that can be overused and can develop trigger points associated with sciatica. Trigger points along the gluteus minimus can cause referred pain to the legs and lower back while mimicking sciatic nerve pain. Thankfully various treatments and techniques can help reduce the chances of trigger points forming along the gluteus minimus and release nerve entrapment from the aggravated muscles pressing on the sciatic nerve, bringing back lower extremity mobility to the body.
References
Greco, Anthony J, and Renato C Vilella. “Anatomy, Bony Pelvis and Lower Limb, Gluteus Minimus Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 29 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK556144/.
Kameda, Masahiro, and Hideyuki Tanimae. “Effectiveness of Active Soft Tissue Release and Trigger Point Block for the Diagnosis and Treatment of Low Back and Leg Pain of Predominantly Gluteus Medius Origin: A Report of 115 Cases.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6382483/.
Martin, Hal David, et al. “Deep Gluteal Syndrome.” Journal of Hip Preservation Surgery, Oxford University Press, July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4718497/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Whiler, Lisa, et al. “Gluteus Medius and Minimus Muscle Structure, Strength, and Function in Healthy Adults: Brief Report.” Physiotherapy Canada. Physiotherapie Canada, University of Toronto Press, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5963550/.
Many individuals utilize the lower half of their bodies to go to different places and use the various surrounding muscles that provide stability on the hips and low back while supporting the upper body’s weight. Along the lower back is the buttock region, where the gluteal muscles help stabilize the pelvis, extend the hips, and rotate the thighs. The gluteal muscles also help shape and support the spine and have an erect posture in the body. One of the gluteal muscles that support the lower body is the gluteus medius, which can succumb to injuries and strain when overused or strained. This leads to developing trigger points that can cause various issues in the lower extremities and lead to corresponding chronic conditions. Today’s article focuses on the gluteus medius muscles, how the lumbago is associated with gluteus medius trigger pain, and various techniques to manage trigger points along the gluteus medius muscle. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like butt and low back pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the gluteus medius muscles near and surrounding the body’s lower extremities. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Gluteus Medius?
Have you been experiencing pain near your buttock and lower back? Have you been feeling unstable when you are walking? What about feeling pain in your tailbone that makes it unbearable to sit down? Many of these issues are associated with referred pain caused by trigger points affecting the gluteus medius. As part of the gluteal muscle region, the gluteus medius lies between the gluteus maximus and minimus is a flat, triangular muscle and is the primary hip abductor. The gluteus medius and minimus work together for internal rotation for the thighs and lateral rotation for the knees when they are extended. The gluteus medius muscles also help stabilize the pelvis, while the trunk maintains an upright position when the legs are in motion. Studies reveal that the gluteus medius is a key lateral hip muscle that correlates with muscle function with other muscle groups like the quadriceps and abdominal muscles. When injuries or not activating the gluteal muscles often, various muscle issues can cause problems to the gluteus medius muscles.
Lumbago Associated With Gluteus Medius Trigger Pain
Dysfunction in the hips can lead to various issues that can either be acute or chronic, depending on how severely the muscles have been overused or injured. Studies reveal that low back pain has been identified as the leading contributor to disability and when there is dysfunction in the lumbopelvic-hip complex, causing a reduction in gluteus medius strength. When the gluteus medius muscles have become overused or injured through trauma, it can develop trigger points on the muscle causing low back pain issues. When trigger points affect the gluteus medius, additional studies reveal that latent trigger points along the gluteus medius muscles may cause joint movement limitation while causing overload by affecting muscle activation from the hips.
According to Dr. Janet G. Travell, M.D.’s book, “Myofascial Pain and Dysfunction: The Trigger Point Manual,” patients with active trigger points along their gluteus medius complain of pain when they are doing normal actions like walking or sitting. The pressure from the trigger points along the gluteus medius causes the individual to be in a slumped position, causing them to be uncomfortable. This causes instability in the hips and lower body extremities, making many people miserable. The book also explains that the referred pain patterns caused by gluteus medius trigger points can overlap other chronic conditions like sacroiliac joint dysfunction, low back pain, and inflammation of the subgluteus medius bursa.
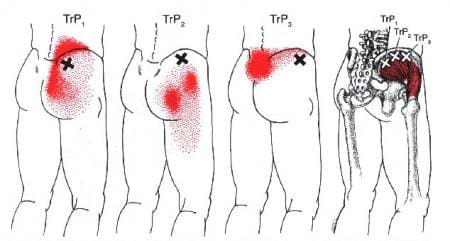
Trigger Point Of The Week: Gluteus Medius- Video
Have you been dealing with hip pain? Do you feel uncomfortable pain when walking or sitting down? Or Do you feel muscle stiffness or tenderness near your tailbone constantly? If you have been experiencing these painful symptoms constantly in your lower back or your hips, it could be due to your gluteus medius muscles being affected by trigger points. The video above overviews the gluteus medius location and how trigger points or myofascial pain syndrome causes referred pain to the lower back and hips. When trigger points affect the gluteus medius, the referred pain can overlap and correlate to low back and hip pain, thus causing various issues to the muscles surrounding the low back and buttock region. Regarding trigger points affecting the gluteus medius, they can be treatable through multiple techniques specific to the low back, buttocks, and hips.
Various Techniques For Managing Trigger Pain Along The Gluteus Medius
When issues of low back or hip pain begin to cause a problem in the lower extremities, the gluteus muscles can invoke pain-like symptoms in the affected muscle regions, thus developing trigger points. Even though trigger points are tricky to diagnose, they can be treated with various techniques that many people can incorporate into their daily lives. Exercises like resistance training on the gluteus medius can help improve hip abductor functionality and increase the strength of the gluteus medius. To manage trigger points along the gluteus medius, many people must do these corrective actions to reduce the pain that they may be causing to their glutes. When people are putting on pants, it is best to sit down and then put on their pants to prevent muscle strain on their hips and gluteus medius. Another corrective action is to move around after sitting down for a prolonged period to avoid trigger pain from developing. These corrective actions and techniques can help strengthen the lower body extremities and improve hip mobility.
Conclusion
As part of the gluteal muscle region, the gluteus medius lies between the gluteus maximus and minimus by being a primary hip abductor. The gluteus medius helps with pelvic stabilization and helps the trunk maintain an upright position when the legs are in motion. When normal or traumatic factors affect the gluteus medius, it can develop trigger points on the muscle fibers, causing referred pain to the hips and lower back. Trigger points along the gluteus medius are manageable through various techniques that people can use to prevent hip and low back issues. These techniques can minimize the trigger points and strengthen the gluteus medius muscles in the glutes.
References
Bagcier, Fatih, et al. “The Relationship between Gluteus Medius Latent Trigger Point and Muscle Strength in Healthy Subjects.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, Jan. 2022, https://pubmed.ncbi.nlm.nih.gov/35248262/.
Sadler, Sean, et al. “Gluteus Medius Muscle Function in People with and without Low Back Pain: A Systematic Review.” BMC Musculoskeletal Disorders, BioMed Central, 22 Oct. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6805550/.
Shah, Aashin, and Bruno Bordoni. “Anatomy, Bony Pelvis and Lower Limb, Gluteus Medius Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 Jan. 2022, https://www.ncbi.nlm.nih.gov/books/NBK557509/.
Stastny, Petr, et al. “Strengthening the Gluteus Medius Using Various Bodyweight and Resistance Exercises.” Strength and Conditioning Journal, Strength and Conditioning Journal, June 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4890828/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Whiler, Lisa, et al. “Gluteus Medius and Minimus Muscle Structure, Strength, and Function in Healthy Adults: Brief Report.” Physiotherapy Canada. Physiotherapie Canada, University of Toronto Press, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5963550/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine