Can healthcare providers help many individuals with lumbar disc degeneration find relief through spinal decompression treatments?
Introduction
Many individuals often do everyday motions that can allow the spine to bend, twist, and turn in various ways without feeling pain and discomfort. However, as the body ages, so does the spine, as the spinal discs begin the natural process of degeneration. Since the spinal discs in the spinal column absorb the vertical pressure weight, it stabilizes the upper and lower extremities and provides motion. To that point, when many individuals suffer from various injuries or environmental factors that cause the spinal disc to be compressed, it can lead to low back issues that cause pain and discomfort when a person is doing an activity. Since low back pain is one of the three most common problems that many people worldwide have dealt with, it can become a socio-economic issue that can lead to a life of disability and misery. Low back pain is often correlated with disc degeneration, and the surrounding ligaments and muscle tissues can affect the upper and lower extremities. This causes referred pain to the different musculoskeletal groups, causing many people to seek treatment that can not only be affordable but also effective in reducing the pain. Today’s article looks at the anatomy of the lumbar disc, how disc degeneration affects the lumbar spine, and how spinal decompression can reduce lumbar disc degeneration from causing more pain to the lower back. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to ease the pain-like symptoms associated with lumbar disc degeneration causing low back pain. We also inform our patients that there are non-surgical options to reduce these pain-like issues correlated with disc degeneration and restore lumbar mobility to the body. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the lower back. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
The Anatomy Of The Lumbar Disc
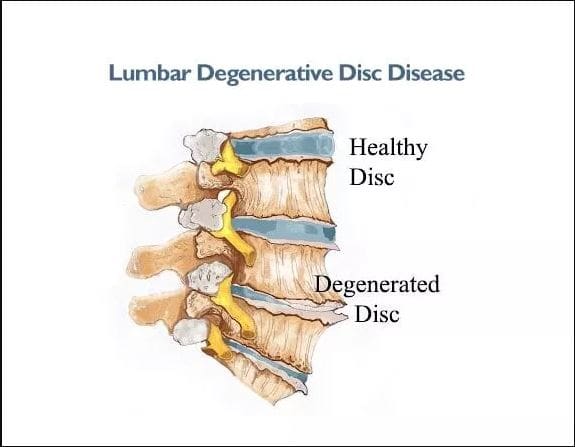
Do you feel tension or stiffness in your lower back after waking up in the morning? Do you feel sudden or gradual pain from bending down to lift a heavy object that is affecting your lower back? Or do you feel the pain in one location or another in your back that is causing you pain and discomfort in your lumbar spinal region? Many of these pain-like issues are often correlated with disc degeneration combined with low back pain. The spinal disc’s anatomy comprises three elements that work together in a specific pattern to resist forces placed in the lumbar spine. (Martin et al., 2002) Since the lumbar spine is the thickest portion of the back, the spinal disc supports the upper body’s weight while stabilizing the lower body. However, the spinal disc will shrink over time when the body ages. Since degeneration is a natural process, many individuals will begin to feel less mobile, which can cause many issues within the lumbar spine.
How Disc Degeneration Affects The Lumbar Spine
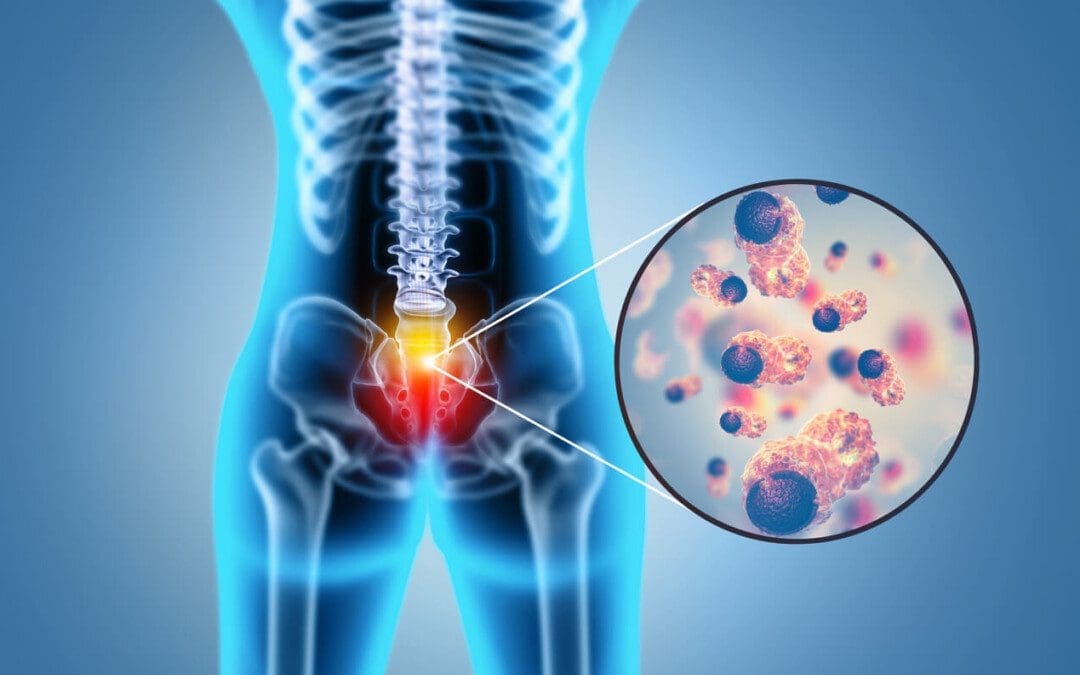
When disc degeneration occurs in the lumbar spine, the spinal disc begins to decrease in volume, and the nutrients that hydrate the disc start to deplete and become compressed. When disc degeneration affects the lumbar spine, the nerve roots from the central system are affected. They can be associated with any particular group of pathological conditions that may irritate the surrounding nerves and produce pain-like symptoms. (Bogduk, 1976) To that point, this causes referred pain in the lower limbs and radiating pain in the lower back. At the same time, glycosphingolipid antibodies are activated in the immune system, causing inflammatory effects. (Brisby et al., 2002) When people are dealing with low back pain associated with disc degeneration, many people will feel their lower back lock up, causing limited mobility and stiffness. At the same time, the surrounding muscle and soft tissues are overstretched and tightened. The spinal disc will also affect the nerve fibers surrounding the spine, leading to nociceptive lower back pain. (Coppes et al., 1997) However, many individuals can find available treatments to reduce low back pain associated with disc degeneration.
An Overview Of Spinal Decompression- Video
Spinal Decompression Can Reduce Lumbar Disc Degeneration
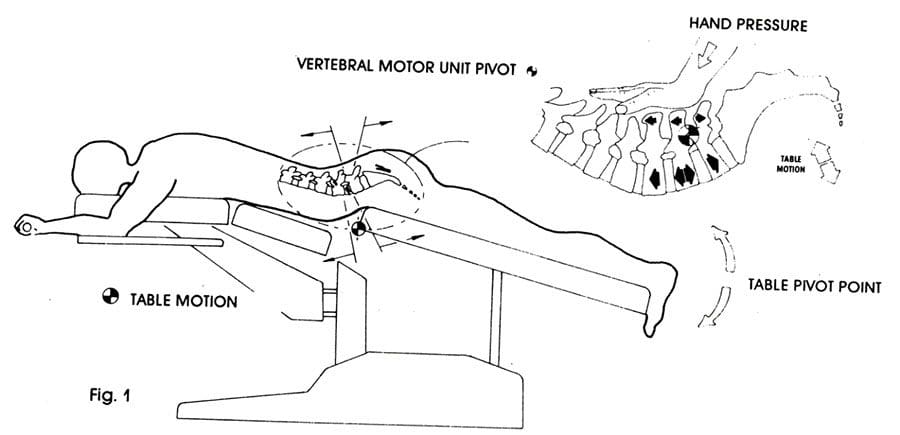
Many individuals can seek out non-surgical treatments to reduce low back pain associated with disc degeneration as it is cost-effective and, through consecutive treatments, can start feeling better. Some non-surgical treatments like spinal decompression can help rehydrate the spinal disc through gentle traction and promote natural healing. Spinal decompression can be manual or mechanical, using negative pressure to increase disc height. (Vanti et al., 2021) This allows many individuals to feel the relief they deserve and feel better over time. Spinal decompression can reduce disc degeneration, stabilize the lumbar spine, and help regain spinal mobility back to the lower portions. (Daniel, 2007) When many individuals begin to take care of their bodies and reduce the chances of low back pain from returning to cause more issues to the back.
Brisby, H., Balague, F., Schafer, D., Sheikhzadeh, A., Lekman, A., Nordin, M., Rydevik, B., & Fredman, P. (2002). Glycosphingolipid antibodies in serum in patients with sciatica. Spine (Phila Pa 1976), 27(4), 380-386. https://doi.org/10.1097/00007632-200202150-00011
Coppes, M. H., Marani, E., Thomeer, R. T., & Groen, G. J. (1997). Innervation of “painful” lumbar discs. Spine (Phila Pa 1976), 22(20), 2342-2349; discussion 2349-2350. https://doi.org/10.1097/00007632-199710150-00005
Daniel, D. M. (2007). Non-surgical spinal decompression therapy: does the scientific literature support efficacy claims made in the advertising media? Chiropr Osteopat, 15, 7. https://doi.org/10.1186/1746-1340-15-7
Martin, M. D., Boxell, C. M., & Malone, D. G. (2002). Pathophysiology of lumbar disc degeneration: a review of the literature. Neurosurg Focus, 13(2), E1. https://doi.org/10.3171/foc.2002.13.2.2
Vanti, C., Turone, L., Panizzolo, A., Guccione, A. A., Bertozzi, L., & Pillastrini, P. (2021). Vertical traction for lumbar radiculopathy: a systematic review. Arch Physiother, 11(1), 7. https://doi.org/10.1186/s40945-021-00102-5
For individuals dealing with chronic pain conditions can having a better understanding of pain management specialists help in developing effective multidisciplinary treatment plans?
Pain Management Specialists
Pain management is a growing medical specialty that takes a multi-disciplinary approach to treating all types of pain. It is a branch of medicine that applies scientifically proven techniques and methods to relieve, reduce, and manage pain symptoms and sensations. Pain management specialists evaluate, rehabilitate, and treat a spectrum of conditions, including neuropathic pain, sciatica, postoperative pain, chronic pain conditions, and more. Many primary healthcare providers refer their patients to pain management specialists if pain symptoms are ongoing or significant in their manifestation.
Specialists
Healthcare providers specializing in pain management recognize the complex nature of pain and approach the problem from all directions. Treatment at a pain clinic is patient-centric but depends on the clinic’s available resources. Currently, there are no set standards for the types of disciplines needed, another reason treatment options vary from clinic to clinic. Experts say that a facility should offer patients:
A coordinating practitioner specializing in pain management and consulting specialists on the patient’s behalf.
Other specialties represented in pain management are anesthesiology, neurosurgery, and internal medicine. A coordinating healthcare provider may refer an individual for services from:
A healthcare provider should have completed additional training and credentialing in pain medicine and be an MD with board certification in at least one of the following (American Board of Medical Specialties. 2023)
Anesthesiology
Physical rehabilitation
Psychiatry
Neurology
A pain management physician should also have their practice limited to the specialty they hold the certification.
Management Goals
The field of pain management treats all types of pain as a disease. Chronic, such as headaches; acute, from surgery, and more. This allows for applying science and the latest medical advances to pain relief. There are now many modalities, including:
Medication
Interventional pain management techniques – nerve blocks, spinal cord stimulators, and similar treatments.
Physical therapy
Alternative medicine
The objective is to minimize and make symptoms manageable.
Individuals determined that surgery does not benefit their condition.
A better understanding of pain syndromes by communities and insurance companies and increased pain studies will help increase insurance coverage for treatments and technology to improve interventional outcomes.
Nalamachu S. (2013). An overview of pain management: the clinical efficacy and value of treatment. The American journal of managed care, 19(14 Suppl), s261–s266.
American Society of Interventional Pain Physicians. (2023). Pain Physician.
For individuals with back pain, how can health practitioners incorporate non-surgical solutions to reduce spinal pain?
Introduction
The spine is one of the most important structures in the human body, providing host mobility and stability when vertical pressure is pressing on the spinal structure. The spine is surrounded by various muscles, ligaments, and tissues that help support the upper and lower body portions and extremities. When normal factors like heaving lifting, improper stances, obesity, or pre-existing conditions start to affect the body, it can cause the spinal structure to potentially cause unwanted issues that lead to back, neck, and shoulder pain. When experiencing these three common body pains often correlate with other associated symptoms that can affect the other extremities. When this happens, many individuals begin to miss out on work or daily activities that can cause them to be miserable, and they even try to look for various solutions to reduce the pain they are experiencing. Today’s article looks at one of the common body pains like back pain and how it can cause numerous issues that affect a person’s ability to function, and how non-surgical solutions can not only reduce the pain-like effects but also provide the necessary relief that many people deserve in their health and wellness journey. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to ease the pain-like symptoms associated with spinal issues causing back pain. We also inform our patients that there are non-surgical options to reduce these pain-like issues and restore spinal mobility to the body. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the lower back. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
Back Pain Affecting The Spine
Do you often experience radiating pain in your lower back that causes symptoms of numbness or tingling sensations down to your legs and feet? Do you feel muscle stiffness in the morning while getting up, only to slowly disappear throughout the day? Or do you feel symptoms of muscle aches and pain when carrying a heavy object from one location to another? Many individuals, more often than not, have dealt with back pain associated with various factors. With back pain being in the top three common problems in the workforce, many individuals have dealt with the common problem in multiple ways. From improper heavy lifting to excessive sitting at a desk, back pain can cause musculoskeletal issues that many are trying to find relief. Low back pain can either be acute or chronic, depending on the severity. It can lead to mobility impairment within the thoracic, lumbar, and sacroiliac spinal regions, causing referred pain to the lower extremities. It can lead to a life of impairment without any symptoms or signs of serious medical or psychological conditions associated with environmental factors. (Delitto et al., 2012) Back pain is also associated with spinal conditions like inflammation, asymmetric loading, and muscle strain, which can cause the spinal structures to be compressed, thus causing disc herniations. (Zemková & Zapletalová, 2021)
Additionally, back pain is a multifactorial musculoskeletal condition that causes many individuals to be in a socio-economic situation that can decrease their quality of life. Many examples of back pain are correlated with altered motor control within the spinal erector muscles that causes impaired proprioception in the spine. (Fagundes Loss et al., 2020) When this happens to many individuals, they often experience a hindrance of lumbar stability, body balance, posture, and postural control. At the same time, when many working individuals are having severe back pain associated with everyday factors, the amount of pain they are in can change the threshold of the mechanoreceptors that are transmitting the pain signals through the spinal cord. To this point, back pain can affect the neuromuscular response and affect normal musculoskeletal functionality. Fortunately, numerous treatments can help reduce back pain and provide relief to spinal pain that is affecting many individuals.
The Role Of Chiropractic Care- Video
How many times a day do you experience back pain associated with stiffness, general aches, or pains that are affecting your ability to work? Do you notice you hunching more when moving from one location to another? Or do you feel aches and pain in your back after stretching in the morning? Many individuals dealing with these common environmental factors are closely associated with back pain. Back pain is in the top three most common problems many individuals have experienced at some point in their lives. More often than not, many people have dealt with back pain by using home remedies to reduce the pain-like effects. However, research studies reveal that when many individuals start to ignore the pain, it can lead them to a life of disability and cause numerous amounts of distress if not treated right away. (Parker et al., 2015) Hence, non-surgical treatments can not only reduce the pain associated with back pain but also help restore spinal mobility. Non-surgical treatments like chiropractic care incorporate spinal manipulation, which can positively affect the spine. (Koes et al., 1996) What chiropractic care does is that it includes mechanical and manual manipulation techniques to stretch out tight muscles and reduce trigger points from reforming. The video above shows how chiropractic care can positively affect the individual while being part of a health and wellness journey to reducing back pain.
Non-Surgical Spinal Decompression For Back Pain
Just like chiropractic care, spinal decompression is another non-surgical treatment that uses traction to gently pull and stretch the spine to alleviate compressed spinal discs associated with back pain and help stretch out tight muscles. When many people start to incorporate spinal decompression as part of their routine, they will notice that spinal decompression can reduce intradiscal pressure within the negative range. (Ramos, 2004) What this does is that when the spinal discs are being pulled by gentle traction, all the fluids and nutrients that were not hydrating the disc flow back and help kickstart the body’s natural healing process. When many people begin to utilize spinal decompression for their back pain, they will notice a huge reduction in their pain after a few consecutive sessions. (Crisp et al., 1955) When many people start to combine other various non-surgical therapies with spinal decompression, they will be able to regain their spinal mobility while being more mindful of what environmental factors are affecting their spine and not repeat the issue to allow back pain to return.
References
Crisp, E. J., Cyriax, J. H., & Christie, B. G. (1955). Discussion on the treatment of backache by traction. Proc R Soc Med, 48(10), 805-814. https://www.ncbi.nlm.nih.gov/pubmed/13266831
Delitto, A., George, S. Z., Van Dillen, L., Whitman, J. M., Sowa, G., Shekelle, P., Denninger, T. R., & Godges, J. J. (2012). Low Back Pain. Journal of Orthopaedic & Sports Physical Therapy, 42(4), A1-A57. https://doi.org/10.2519/jospt.2012.42.4.a1
Fagundes Loss, J., de Souza da Silva, L., Ferreira Miranda, I., Groisman, S., Santiago Wagner Neto, E., Souza, C., & Tarrago Candotti, C. (2020). Immediate effects of a lumbar spine manipulation on pain sensitivity and postural control in individuals with nonspecific low back pain: a randomized controlled trial. Chiropr Man Therap, 28(1), 25. https://doi.org/10.1186/s12998-020-00316-7
Koes, B. W., Assendelft, W. J., van der Heijden, G. J., & Bouter, L. M. (1996). Spinal manipulation for low back pain. An updated systematic review of randomized clinical trials. Spine (Phila Pa 1976), 21(24), 2860-2871; discussion 2872-2863. https://doi.org/10.1097/00007632-199612150-00013
Parker, S. L., Mendenhall, S. K., Godil, S. S., Sivasubramanian, P., Cahill, K., Ziewacz, J., & McGirt, M. J. (2015). Incidence of Low Back Pain After Lumbar Discectomy for Herniated Disc and Its Effect on Patient-reported Outcomes. Clin Orthop Relat Res, 473(6), 1988-1999. https://doi.org/10.1007/s11999-015-4193-1
Ramos, G. (2004). Efficacy of vertebral axial decompression on chronic low back pain: study of dosage regimen. Neurol Res, 26(3), 320-324. https://doi.org/10.1179/016164104225014030
Zemková, E., & Zapletalová, L. (2021). Back Problems: Pros and Cons of Core Strengthening Exercises as a Part of Athlete Training. International Journal of Environmental Research and Public Health, 18(10), 5400. https://doi.org/10.3390/ijerph18105400
Can various therapeutic options provide relief for individuals with upper crossed syndrome to restore muscle strength?
Introduction
Many individuals often suffer neck and shoulder pain from poor posture, improper heavy lifting, musculoskeletal conditions, auto accidents, whiplash, etc. The surrounding muscles that connect the neck and shoulders help protect the cervical and thoracic region of the spine and can succumb to injuries that can cause pain-like symptoms causing discomfort to the individual. Neck, shoulder, and back pain are the three most common issues many individuals have experienced. These musculoskeletal disorders can also correlate with pre-existing conditions; many people will feel pain and discomfort while trying to find the relief they seek. One of the most common issues people often experience is upper crossed syndrome, which can be associated with neck and shoulder pain. Today’s article explains what upper cross syndrome is and how it affects the neck and shoulders while also diving into how different therapeutic options like spinal decompression and chiropractic care can reduce the effects of upper cross syndrome. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to mitigate upper-crossed syndrome in the neck and shoulders. We also inform our patients that there are many therapeutic options, like chiropractic care and spinal decompression, to minimize muscle pain in the neck and shoulders. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with upper-crossed syndrome. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer
What Is Upper Crossed Syndrome?
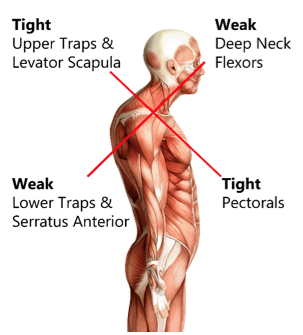
Have you been dealing with muscle pain in your shoulders or neck after being on the computer for a while? Do you feel stiffness in your shoulders that rotating them causes temporary relief? Or does it hurt when you turn your head from side to side? Many of these pain-like scenarios are often associated with upper-cross syndrome. Many people don’t often realize that upper crossed syndrome is a musculoskeletal condition that affects the neck, shoulder, and chest muscles and causes them to be weak and tight due to poor posture. The upper crossed syndrome can cause referred pain to the upper extremities, leading to cervicogenic headaches, limited range of motion, trigger points in the muscles, and muscle imbalance. (Moore, 2004) When many people are dealing with upper crossed syndrome due to poor posture, it can lead to many issues in the neck and shoulders.
How Does It Affect The Neck & Shoulders?
Now, why does upper crossed syndrome affect the neck and shoulders? Many people unintentionally hunched over when looking at their phones, being on the computer, or relaxing at home. This causes specific muscles in the neck and shoulder region, like the serratus and lower trapezius muscles, to become weak while the pectoral and neck muscles are tight. (Chu & Butler, 2021) This, in turn, causes the shoulders to be more rounded and hunched, causing the neck and head to crane forward. When people are dealing with upper crossed syndrome, many would often complain about pain-like symptoms like:
Headaches
Neck Strain
Muscle tightness
Upper back pain
Restricted range of motion
Numbness/Tingling sensations in the arms
The upper crossed syndrome can also occur gradually over time and cause nerve compression to the upper extremities. When the upper neck and shoulder muscles start to affect the surrounding nerve roots, which then leads to nerve dysfunction in the sensory and motor skills when a person picks up an object. (Lee & Lim, 2019) However, many individuals dealing with upper-crossed syndrome can seek treatment to relieve muscle pain in their neck and shoulders.
An Overview Of Upper Crossed Syndrome- Video
Since upper cross syndrome is a musculoskeletal condition that affects the neck and shoulders, it can result in muscle imbalance and pain in the individual. Many people, especially in the working field, develop this syndrome by being hunched over for an extended period. (Mujawar & Sagar, 2019) This causes the head to be more forward, the neck posture to be curved and hunched, and the shoulders to be rounded. The video above explains upper-crossing syndrome, its causes, and how it is treated.
Numerous treatments can help restore muscle strength and reduce muscle pain in the neck and shoulders. Treatments like spinal decompression can help reduce upper crossed syndrome by slowly using gentle traction to the cervical spine region and gently stretching the neck muscles to provide relief. Spinal decompression is one of the non-surgical treatments that many individuals with headaches associated with upper crossed syndrome can find the comfort they seek through pain reduction and improve their quality of life. (Eskilsson et al., 2021) At the same time, spinal decompression can be part of a personalized treatment plan that many individuals can add to their daily routine to prevent the pain from returning. (Saunders, 1983)
Chiropractic Care Restoring Muscle Strength
Just like spinal decompression, chiropractic care is a non-surgical treatment that can be combined with various stretching techniques to restore the neck’s range of motion and reduce pain associated with upper-crossed syndrome. (Mahmood et al., 2021) Chiropractic care incorporates manual and mechanical techniques like MET (muscle energy techniques) and spinal manipulation to realign the spine out of subluxation. When chiropractors integrate MET to manage upper crossed syndrome, many individuals find that their pain has decreased, their cervical range of motion is improved, and their neck disability is reduced. (Gillani et al., 2020) When many individuals start thinking about their health and wellness, they can make small changes to improve their posture and be more mindful of their bodies to reduce the chances of upper-cross syndrome returning.
References
Chu, E. C., & Butler, K. R. (2021). Resolution of Gastroesophageal Reflux Disease Following Correction for Upper Cross Syndrome-A Case Study and Brief Review. Clin Pract, 11(2), 322-326. https://doi.org/10.3390/clinpract11020045
Eskilsson, A., Ageberg, E., Ericson, H., Marklund, N., & Anderberg, L. (2021). Decompression of the greater occipital nerve improves outcome in patients with chronic headache and neck pain – a retrospective cohort study. Acta Neurochir (Wien), 163(9), 2425-2433. https://doi.org/10.1007/s00701-021-04913-0
Gillani, S. N., Ain, Q., Rehman, S. U., & Masood, T. (2020). Effects of eccentric muscle energy technique versus static stretching exercises in the management of cervical dysfunction in upper cross syndrome: a randomized control trial. J Pak Med Assoc, 70(3), 394-398. https://doi.org/10.5455/JPMA.300417
Mahmood, T., Afzal, W., Ahmad, U., Arif, M. A., & Ahmad, A. (2021). Comparative effectiveness of routine physical therapy with and without instrument assisted soft tissue mobilization in patients with neck pain due to upper crossed syndrome. J Pak Med Assoc, 71(10), 2304-2308. https://doi.org/10.47391/JPMA.03-415
Moore, M. K. (2004). Upper crossed syndrome and its relationship to cervicogenic headache. J Manipulative Physiol Ther, 27(6), 414-420. https://doi.org/10.1016/j.jmpt.2004.05.007
Mujawar, J. C., & Sagar, J. H. (2019). Prevalence of Upper Cross Syndrome in Laundry Workers. Indian J Occup Environ Med, 23(1), 54-56. https://doi.org/10.4103/ijoem.IJOEM_169_18
Can individuals with low back pain find relief with spinal decompression combined with chiropractic care to reduce muscle pain?
Introduction
Everyone worldwide has dealt with low back pain, a multifactorial common problem that can mask other musculoskeletal disorders. Low back pain can develop naturally through spinal degeneration, normal environmental factors people put their bodies through, or traumatic factors that can gradually affect the lumbar region over time. The lower back is part of the lumbar spine region as it takes most of the upper body’s weight and stabilizes the lower body when in motion. The lumbar region is thick to support the upper body’s weight and is protected by the surrounding ligaments, muscles, and tissues; however, it is the most susceptible to injury. Many people don’t realize they are experiencing low back pain until an accident or repetitive motions begin to affect the surrounding ligaments or the lumbar intervertebral discs are severely compressed. To that point, many individual are experiencing radiating pain in their lower extremities. However, all is not lost, as there are numerous ways to alleviate low back pain and provide relief to many individuals. Today’s article focuses on the factors that lead to the development of low back pain and how treatments like chiropractic care and spinal decompression can help reduce low back pain and its symptoms. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to ease low back pain and its associated symptoms. We also inform our patients that there are non-surgical options like chiropractic care and spinal decompression to minimize the radiating pain associated with low back pain. We encourage our patients to ask intricated and educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the lower back. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer
Factors That Lead To The Development Of Low Back Pain
Do you feel muscle aches and pains in your lower back when stretching? Does the pain cause issues in your mobility when going to run errands? Or do you feel sudden or gradual pain after a long workday of carrying heavy objects or excessively sitting at your desk? When many individuals are experiencing pain in these various scenarios, it can lead to the development of a lower back that correlates with these environmental factors. Low back pain is a common nuisance that many working and non-working individuals experience occasionally. When various risk factors are associated with low back pain, it can cause many individuals to deal with the physical and psychological demands that cause them to do multiple things like heavy lifting, awkward positions, and excessive bending, which can develop pain-like symptoms in the lumbar region. (To et al., 2021) At the same time, compared with other health conditions, low back pain is the highest global burden, causing many individuals to miss out on important events like work and daily activities. (Petrozzi et al., 2020) This causes them to live a life of disability and causes them to feel miserable. Low back pain can affect a person’s socioeconomic demographic and the functionality that they seek the treatment they deserve.
Many individuals who experience low back pain will often lead a life of disability and socioeconomic burden correlated with these factors. (Wong et al., 2022) Many people often think that low back pain only happens to older adults, but low back pain can happen to anybody at any age. Many factors that correlate to the development of low back pain include:
Improper heavy lifting
Walking incorrectly
Being in a slouched or hunched position
An auto accident
Obesity
Gastrointestinal issues
Referred musculoskeletal disorders
Physical inactivity
Many of these environmental factors are associated with low back pain that many people are unaware of when doing their routine. This is due to the surrounding tissues, ligaments, and muscles being overused and affected and the intervertebral disc being constantly compressed from repetitive motions. When this happens, many individuals will often seek treatment to reduce the painful effects of low back pain.
How Chiropractic Care Can Transform Pain Into Relief- Video
When it comes to reducing low back pain, many individuals will try home remedies to mitigate muscle pain and reduce inflammation associated with low back pain. This provides temporary relief to acute low back pain, but many will seek non-surgical treatment when it comes to chronic low back pain. Non-surgical treatments can help reduce low back pain and its associated symptoms through mechanical and manual techniques. Non-surgical treatments, which include chiropractic care and spinal decompression, could help alleviate low back pain. Since low back pain is associated with altered motor control within the lumbar region, it can hinder lumbar stability, cause impaired detection of passive motion, and affect postural stability. (Fagundes Loss et al., 2020) With non-surgical treatments, many pain specialists can incorporate vertebral mobilizations and manipulation procedures to improve spinal mobility and reduce pain in the lumbar region. The video above explains how chiropractic care and spinal decompression can alleviate lower back pain and help restore functionality in the body.
Chiropractic Care & Low Back Pain
When it comes to reducing low back pain associated with environmental factors, many pain specialists can look at the physical distress cognitive, and functional patterns that are correlated with faulty lumbar movement. (Khodadad et al., 2020) This allows the pain specialist to create a personalized treatment plan for low back pain. Non-surgical treatments like chiropractic care are excellent for reducing low back pain. Chiropractic care incorporates spinal manipulation techniques to realign the spine and help stretch the affected surrounding muscles. Many individuals who include chiropractic care in their routine find significant pain reduction and reduced disability after a few consecutive treatments. (Gevers-Montoro et al., 2021) Chiropractic care can be combined with physical and massage therapy to stretch and strengthen the affected muscles. This, in turn, helps the individual regain spinal mobility and reduce pain.
Spinal Decompression & Low Back Pain
Spinal decompression is another non-surgical treatment that can help alleviate low back pain, like chiropractic care. Spinal decompression utilizes gentle traction on the lumbar spine to be gently pulled to relieve the affected muscles causing lower back pain. Spinal decompression can also ease leg pain associated with low back pain and reduce referred pain affecting the lower extremities. (Wang et al., 2022) Spinal decompression can also improve spinal disc height and help improve muscle strength and trunk endurance. (Kang et al., 2016) The combination of spinal decompression and chiropractic care to reduce lower back pain is effective as these two forms of non-surgical treatments can effectively reduce many people’s musculoskeletal pain and make them aware of the environmental factors that are the root causes of their lower back pain and prevent it from returning.
References
Fagundes Loss, J., de Souza da Silva, L., Ferreira Miranda, I., Groisman, S., Santiago Wagner Neto, E., Souza, C., & Tarrago Candotti, C. (2020). Immediate effects of a lumbar spine manipulation on pain sensitivity and postural control in individuals with nonspecific low back pain: a randomized controlled trial. Chiropr Man Therap, 28(1), 25. https://doi.org/10.1186/s12998-020-00316-7
Gevers-Montoro, C., Provencher, B., Descarreaux, M., Ortega de Mues, A., & Piche, M. (2021). Clinical Effectiveness and Efficacy of Chiropractic Spinal Manipulation for Spine Pain. Front Pain Res (Lausanne), 2, 765921. https://doi.org/10.3389/fpain.2021.765921
Kang, J.-I., Jeong, D.-K., & Choi, H. (2016). Effect of spinal decompression on the lumbar muscle activity and disk height in patients with herniated intervertebral disk. Journal of Physical Therapy Science, 28(11), 3125-3130. https://doi.org/10.1589/jpts.28.3125
Khodadad, B., Letafatkar, A., Hadadnezhad, M., & Shojaedin, S. (2020). Comparing the Effectiveness of Cognitive Functional Treatment and Lumbar Stabilization Treatment on Pain and Movement Control in Patients With Low Back Pain. Sports Health, 12(3), 289-295. https://doi.org/10.1177/1941738119886854
Petrozzi, M. J., Rubinstein, S. M., Ferreira, P. H., Leaver, A., & Mackey, M. G. (2020). Predictors of low back disability in chiropractic and physical therapy settings. Chiropr Man Therap, 28(1), 41. https://doi.org/10.1186/s12998-020-00328-3
To, D., Rezai, M., Murnaghan, K., & Cancelliere, C. (2021). Risk factors for low back pain in active military personnel: a systematic review. Chiropr Man Therap, 29(1), 52. https://doi.org/10.1186/s12998-021-00409-x
Wang, W., Long, F., Wu, X., Li, S., & Lin, J. (2022). Clinical Efficacy of Mechanical Traction as Physical Therapy for Lumbar Disc Herniation: A Meta-Analysis. Comput Math Methods Med, 2022, 5670303. https://doi.org/10.1155/2022/5670303
Wong, C. K., Mak, R. Y., Kwok, T. S., Tsang, J. S., Leung, M. Y., Funabashi, M., Macedo, L. G., Dennett, L., & Wong, A. Y. (2022). Prevalence, Incidence, and Factors Associated With Non-Specific Chronic Low Back Pain in Community-Dwelling Older Adults Aged 60 Years and Older: A Systematic Review and Meta-Analysis. J Pain, 23(4), 509-534. https://doi.org/10.1016/j.jpain.2021.07.012
In individuals with lumbar back pain, can pain specialists utilize distraction techniques to reduce muscle spasms?
Introduction
Many individuals dealing with specific or nonspecific back pain can agree that it can dampen their moods as they try to find the relief they seek to get back to their routine. More often than not, back pain is a common multifactorial musculoskeletal disorder that can affect the entire body, and it all starts with how people do simple movements incorrectly, causing compression to the spine. Since the spine is the main backbone of the body, it is responsible for training, stability, and flexibility. The surrounding muscles that encompass the spine act like a barrier to protect the skeletal joints and the spinal cord from injuries that are either traumatic or normal wear and tear. Lumbar back pain is also an economic burden that can cause unnecessary stress to the body, which leads to muscle spasms and causes even more stress to the individual. With lumbar back pain being a common nuisance to everyone worldwide, many will opt for treatment to reduce the pain and continue their daily activities. In today’s article, we will explore the issues of lumbar back pain and how treatments with distraction techniques alleviate the effects of lumbar back pain and reduce muscle spasms. We speak with certified medical providers who incorporate our patients’ information to provide numerous treatment plans to mitigate lumbar back pain associated with environmental factors. We also inform our patients that there are non-surgical options to reduce the pain-like symptoms related to lumbar back pain and reduce the effects of muscle spasms. We encourage our patients to ask astounding educational questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with the lumbar spine. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer
The Issues Of Lumbar Back Pain
Do you often feel pain radiating from your lower back to your legs after work? Did you lift something heavy that caused your back muscles to strain and be in pain? Or do you and your loved ones feel muscle spasms in your lower back after stretching in the morning? When many individuals are dealing with these musculoskeletal issues, it often correlates with lumbar back pain. As stated earlier, the spine is the body’s backbone, and its main job is to support the body’s weight, provide stability to the upper and lower quadrants, and allow the host to move without pain or discomfort. When normal or traumatic factors start to affect many individuals over time, it can lead to the development of lumbar back pain, and it can become an issue for many young and older adults. Since lumbar back pain can be mechanical or nonspecific, it can arise intrinsically from the spine and the spinal components through repetitive muscle trauma that can be overused while being one of the common causes many people experience pain in their lumbar spine. (Will et al., 2018) When many individuals are dealing with lumbar back pain, it can become a reoccurring issue, and many go to medical clinics to get treatment for their lumbar back pain.
Another issue that lumbar back pain causes is affecting the spinal structure and the surrounding muscles, tissues, and ligaments that protect the spine. Since the body is remarkable for sensing when pain affects the spine, the vital structures are affected and start to respond by adopting other measures to maintain the spine’s stability. (Hauser et al., 2022) This means that when the body starts to develop muscle spasms in the spine, the stretched ligaments react rapidly to prevent the spine from destabilizing. This leads to individuals feeling aches and pain in their lower back, which then causes them to miss out on their activities.
The Road To Recovery: Chiropractic Care- Video
When it comes to lumbar back pain, many everyday factors can contribute to its development and cause issues for many individuals. Many individuals with lumbar back pain often experience referred pain in their lower extremity regions as the lumbar portions of the spine have compressed spinal discs, which can also correlate with nerve entrapment. To this point, many will seek out various treatments to reduce low back pain and its associated symptoms. When patients have prolonged symptoms correlating with lumbar pain, conservative management that is either non-surgical or surgical can help treat the pain-like symptoms related to lumbar back pain. (Mohd Isa et al., 2022) Lumbar back pain treatments can be customizable and cost-effective to the person’s pain severity. Non-surgical treatments can help lumbar back pain issues and reduce referred pain symptoms from different body locations in the upper or lower body quadrants. When people go to get their lumbar back pain treated, pain specialists like chiropractors, massage therapists, and physical therapists utilize various techniques and treatments to reduce pain affecting the surrounding ligaments, tissues, and muscles through stretches and traction. The video above explains how these treatments can help reduce pain caused by environmental factors and also help speed up recovery.
Distraction Techniques To Reduce Lumbar Back Pain
When many individuals get treated for lumbar back pain, many opt for non-surgical treatments due to being more affordable than surgical treatments. Pain specialists like chiropractors or massage therapists use distraction techniques to reduce the pain. These pain specialists also incorporate manual and mechanical therapy to be body-oriented to mobilize, manipulate, and stretch out the soft tissues and strengthen them. (Kuligowski et al., 2021) This, in turn, can help reduce lumbar back pain while allowing the individual to be more mindful about their actions to reduce the chances of back pain from returning. At the same time, the effectiveness of treating lumbar back pain through traction can effectively reduce nerve root compression and unresponsive movement symptoms. (Vanti et al., 2021) Traction therapy is a non-surgical treatment that gently stretches the spine to alleviate pain and help kick-start the natural healing process.
Distraction Techniques Reducing Muscle Spasms
Pain specialists incorporate distraction techniques to reduce lumbar back pain and muscle spasms in the lumbar region. As stated earlier, distraction techniques associated with non-surgical treatments can be an excellent way to minimize lumbar back pain. Distraction manipulation can help elevate the affected intervertebral disc by reducing the pressure off the disc and increasing its height in the spine. (Choi et al., 2015) Many individuals feel better when they incorporate distraction therapy to reduce lumbar pain. At the same time, distraction therapy can also be incorporated into a personalized plan to reduce muscle spasms and strengthen weak muscles that surround the lumbar region. The effects of lumbar traction combined with distraction therapy can improve pain and reduce functional disability within the lumbar spine. (Masood et al., 2022) When many people start to think more about their health and wellness, they can make small changes in their routine to prevent low back pain from progressing into something chronic and strengthen their weak muscles to control the pain-like symptoms from returning.
References
Choi, J., Lee, S., & Jeon, C. (2015). Effects of flexion-distraction manipulation therapy on pain and disability in patients with lumbar spinal stenosis. Journal of Physical Therapy Science, 27(6), 1937-1939. https://doi.org/10.1589/jpts.27.1937
Hauser, R. A., Matias, D., Woznica, D., Rawlings, B., & Woldin, B. A. (2022). Lumbar instability as an etiology of low back pain and its treatment by prolotherapy: A review. J Back Musculoskelet Rehabil, 35(4), 701-712. https://doi.org/10.3233/BMR-210097
Kuligowski, T., Skrzek, A., & Cieslik, B. (2021). Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int J Environ Res Public Health, 18(11). https://doi.org/10.3390/ijerph18116176
Masood, Z., Khan, A. A., Ayyub, A., & Shakeel, R. (2022). Effect of lumbar traction on discogenic low back pain using variable forces. J Pak Med Assoc, 72(3), 483-486. https://doi.org/10.47391/JPMA.453
Mohd Isa, I. L., Teoh, S. L., Mohd Nor, N. H., & Mokhtar, S. A. (2022). Discogenic Low Back Pain: Anatomy, Pathophysiology and Treatments of Intervertebral Disc Degeneration. Int J Mol Sci, 24(1). https://doi.org/10.3390/ijms24010208
Vanti, C., Turone, L., Panizzolo, A., Guccione, A. A., Bertozzi, L., & Pillastrini, P. (2021). Vertical traction for lumbar radiculopathy: a systematic review. Arch Physiother, 11(1), 7. https://doi.org/10.1186/s40945-021-00102-5
How can spinal decompression reduce pain while restoring spinal flexibility in many individuals with lumbar degenerative disorders?
Introduction
As we naturally age, so do our spines and spinal discs, as the natural fluids and nutrients stop hydrating the discs and cause them to degenerate. When disc degeneration starts to affect the spine, it can cause pain-like symptoms in the lumbar regions, which then develop into lower back pain or other musculoskeletal disorders that affect the lower extremities. When disc degeneration starts to affect the lumbar region, many individuals will notice that they are not as flexible as when they were younger. The physical signs of straining their muscles from improper lifting, falling, or carrying heavy objects can cause muscle strain and pain. When this happens, many individuals will treat the pain with home remedies, which can provide temporary relief but can aggravate it more when people make repetitive motions to their lumbar spine, which can result in injuries. Fortunately, non-surgical treatments that can help slow down the process of disc degeneration while rehydrating the spinal disc. Today’s article looks at why disc degeneration affects lumbar flexibility and how treatments like spinal decompression reduce disc degeneration while restoring lumbar flexibility. Coincidentally, we communicate with certified medical providers who incorporate our patients’ information to provide various treatment plans to reduce the disc degeneration process and provide pain relief. We also inform them that there are non-surgical options to reduce the pain-like symptoms associated with disc degeneration and help restore lumbar flexibility. We encourage our patients to ask amazing educational questions to our associated medical providers about their symptoms correlating with body pain in a safe and positive environment. Dr. Alex Jimenez, D.C., incorporates this information as an academic service. Disclaimer
How Does DDD Affect Lumbar Flexibility?
Have you been experiencing stiffness in your back when you wake up in the morning? Do you feel muscle aches and pains when bending down and picking up heavy objects? Or do you feel radiating pain in your legs and back? When many individuals are in excruciating pain, many don’t often realize that their lower back pain could also be associated with their spinal disc degenerating. Since the spinal disc and the body can degenerate naturally, it can lead to the development of musculoskeletal disorders. DDD, or degenerative disc disease, is a common disabling condition that can greatly impact the musculoskeletal system and is the main cause of individuals missing out on their daily activities. (Cao et al., 2022) When normal or traumatic factors begin to cause repetitive motions to the spine, it can cause the spinal disc to be compressed and, over time, degenerate. This, in turn, causes the spine to be less flexible and becomes a socio-economic challenge.
When disc degeneration starts to cause spinal inflexibility, it can lead to the development of low back pain. Since low back pain is a common health concern, it can affect many individuals worldwide, as disc degeneration is a common factor. (Samanta et al., 2023) Since disc degeneration is a multi-factorial disorder, the musculoskeletal and organ systems are also affected as it can cause referred pain to different body locations. Luckily, many individuals can find the treatment they are looking for, as many seek relief from the many pain issues that disc degeneration has caused.
Lumbar Spine Injuries In Athletes- Video
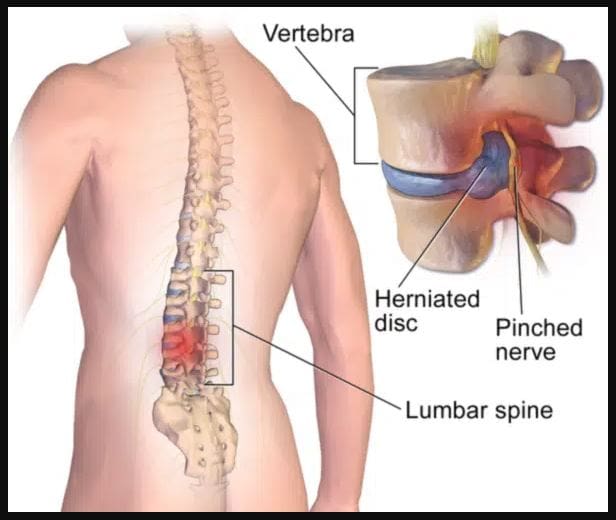
Since disc degeneration is a multi-factorial cause of disability, it can become a primary source of back pain. When normal factors contribute to back pain, it likely correlates with disc degeneration and can cause cellular, structural, compositional, and mechanical changes throughout the spine. (Ashinsky et al., 2021) However, many individuals seeking treatment can look into non-surgical therapies as they are cost-effective and safe on the spine. Non-surgical treatments are safe and gentle on the spine as they can be customizable to the person’s pain and combined with other treatment forms. One of the non-surgical treatments is spinal decompression, which uses gentle traction on the spine to rehydrate the spinal disc from degeneration and help kick-start the body’s natural healing process. The video above shows how disc degeneration is correlated with disc herniation and how these treatments can reduce its pain-like effects on the spine.
Spinal Decompression Reducing DDD
When many individuals are going in for treatment for disc degeneration, many will often try spinal decompression as it is affordable. Many healthcare professionals will assess the individual by creating a personalized plan before entering the traction machine. Many individuals will get a CT scan to assess the changes caused by DDD. (Dullerud & Nakstad, 1994) This determines how severe the disc space is. The traction machine for spinal decompression determines the optimal treatment duration, frequency, and mode of administrating traction to the spine to reduce DDD. (Pellecchia, 1994) Additionally, the efficiency of traction from spinal decompression can help many people with low back and provide relief. (Beurskens et al., 1995)
References
Ashinsky, B., Smith, H. E., Mauck, R. L., & Gullbrand, S. E. (2021). Intervertebral disc degeneration and regeneration: a motion segment perspective. Eur Cell Mater, 41, 370-380. https://doi.org/10.22203/eCM.v041a24
Beurskens, A. J., de Vet, H. C., Koke, A. J., Lindeman, E., Regtop, W., van der Heijden, G. J., & Knipschild, P. G. (1995). Efficacy of traction for non-specific low back pain: a randomised clinical trial. Lancet, 346(8990), 1596-1600. https://doi.org/10.1016/s0140-6736(95)91930-9
Cao, G., Yang, S., Cao, J., Tan, Z., Wu, L., Dong, F., Ding, W., & Zhang, F. (2022). The Role of Oxidative Stress in Intervertebral Disc Degeneration. Oxid Med Cell Longev, 2022, 2166817. https://doi.org/10.1155/2022/2166817
Dullerud, R., & Nakstad, P. H. (1994). CT changes after conservative treatment for lumbar disk herniation. Acta Radiol, 35(5), 415-419. https://www.ncbi.nlm.nih.gov/pubmed/8086244
Samanta, A., Lufkin, T., & Kraus, P. (2023). Intervertebral disc degeneration-Current therapeutic options and challenges. Front Public Health, 11, 1156749. https://doi.org/10.3389/fpubh.2023.1156749
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine