Back Clinic Chronic Pain Chiropractic Physical Therapy Team. Everyone feels pain from time to time. Cutting your finger or pulling a muscle, pain is your body’s way of telling you something is wrong. The injury heals, you stop hurting.
Chronic pain works differently. The body keeps hurting weeks, months, or even years after the injury. Doctors define chronic pain as any pain that lasts for 3 to 6 months or more. Chronic pain can affect your day-to-day life and mental health. Pain comes from a series of messages that run through the nervous system. When hurt, the injury turns on pain sensors in that area. They send a message in the form of an electrical signal, which travels from nerve to nerve until it reaches the brain. The brain processes the signal and sends out the message that the body is hurt.
Under normal circumstances, the signal stops when the cause of pain is resolved, the body repairs the wound on the finger or a torn muscle. But with chronic pain, the nerve signals keep firing even after the injury is healed.
Conditions that cause chronic pain can begin without any obvious cause. But for many, it starts after an injury or because of a health condition. Some of the leading causes:
Arthritis
Back problems
Fibromyalgia, a condition in which people feel muscle pain throughout their bodies
Infections
Migraines and other headaches
Nerve damage
Past injuries or surgeries
Symptoms
The pain can range from mild to severe and can continue day after day or come and go. It can feel like:
A dull ache
Burning
Shooting
Soreness
Squeezing
Stiffness
Stinging
Throbbing
For answers to any questions you may have please call Dr. Jimenez at 915-850-0900
Understand the implications of an auto accident and how to navigate the aftermath effectively for recovering from WAD.
Understanding Whiplash-Associated Disorders from Motor Vehicle Accidents: Causes, Treatments, and Recovery
Whiplash-associated disorders (WAD) sound like something you’d get from a wild roller coaster ride, but unfortunately, they’re a lot less fun. These injuries often occur after a motor vehicle accident (MVA), leaving victims with neck pain, stiffness, and sometimes a whole laundry list of other symptoms. If you’ve ever been rear-ended at a stoplight and felt your head snap back like a bobblehead, you’ve probably experienced the forces that can lead to WAD. In this blog post, we’ll dive deep into why WAD and the cervical spine are so closely tied to MVAs, how these injuries develop, and what you can do to recover without feeling like you’re stuck in a neck brace forever. We’ll also spotlight Dr. Alexander Jimenez, a rockstar chiropractor in El Paso, Texas, who’s helping accident victims navigate the road to recovery with advanced diagnostics and a knack for bridging the medical and legal worlds. Buckle up (safely, of course) for a comprehensive, SEO-optimized guide that’s over 5,000 words, written for a high school reading level, with a sprinkle of humor to keep things light—because nobody likes reading about neck pain without a chuckle or two.
What Are Whiplash-Associated Disorders (WAD)?
Let’s start with the basics. Whiplash-associated disorders are a collection of symptoms that pop up after your neck goes through a rapid back-and-forth motion, like a whip cracking (hence the name). This usually happens in MVAs, especially rear-end collisions, where your car gets hit from behind, and your head decides to do its best impression of a ping-pong ball. The Quebec Task Force, a group of experts who’ve studied this stuff, classifies WAD into five grades, from “no pain at all” (Grade 0) to “ouch, there’s a fracture or dislocation” (Grade 4). Most people fall into Grades 1 or 2, which involve neck pain, stiffness, or tenderness, sometimes with reduced range of motion or point tenderness (Spitzer et al., 1995).
The cervical spine—those seven vertebrae in your neck (labeled C1 to C7)—is the star of this unfortunate show. It’s a flexible, hardworking structure that supports your head, protects your spinal cord, and lets you turn your head to check your blind spots (or avoid awkward eye contact). But when an MVA sends your neck into overdrive, the cervical spine can take a beating, leading to WAD symptoms like:
Neck pain and stiffness
Headaches, often starting at the base of the skull
Shoulder or upper back pain
Dizziness or vertigo
Tingling or numbness in the arms
Fatigue, irritability, or even trouble concentrating (because apparently, whiplash doesn’t think neck pain is enough)
These symptoms can show up right after the accident or sneak in days later, like an uninvited guest who overstays their welcome. So, why does the cervical spine get so cranky after an MVA? Let’s break it down.
References
Spitzer, W. O., Skovron, M. L., Salmi, L. R., Cassidy, J. D., Duranceau, J., Suissa, S., & Zeiss, E. (1995). Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: Redefining “whiplash” and its management. Spine, 20(8S), 1S–73S.
The Clinical Rationale: Why MVAs Cause WAD and Cervical Spine Injuries
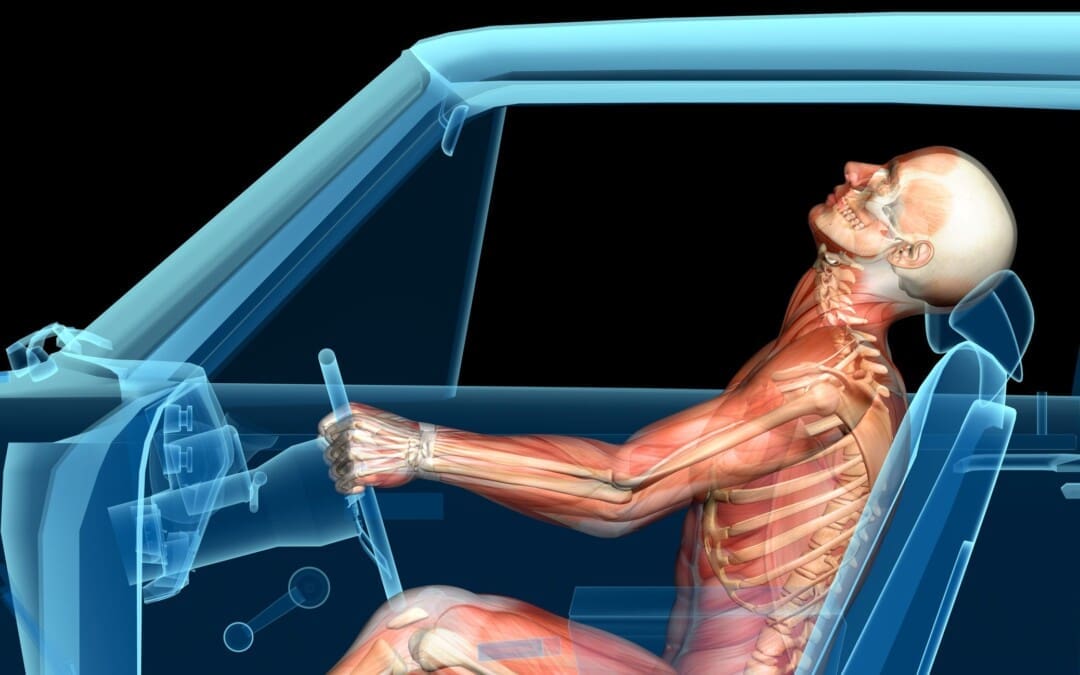
Picture this: You’re stopped at a red light, singing along to your favorite tune, when BAM! A distracted driver rear-ends you. Your car lurches forward, but your seatbelt keeps your body in place—except for your head, which snaps backward and then forward faster than you can say “whiplash.” This is what experts call a cervical acceleration-deceleration (CAD) injury, and it’s the key to understanding why MVAs and WAD are such close cousins.
The Biomechanics of Whiplash
During a rear-end collision, your cervical spine goes through a wild ride. High-speed cameras and crash test dummies (who have a worse day than you) show that the lower cervical vertebrae (C5 and C6) hyperextend—meaning they bend backward too far—while the upper vertebrae (C1 and C2) hyperflex, bending forward. This creates an S-shaped curve in your neck, which is not how your spine likes to hang out (Kaneoka et al., 1999). This abnormal motion stretches or tears soft tissues like:
Ligaments: The anterior longitudinal ligament (ALL) and facet joint capsules can get overstretched or sprained.
Muscles: The sternocleidomastoid and trapezius muscles might strain or develop trigger points.
Joints: The zygapophyseal (facet) joints can get compressed or irritated.
Discs: Intervertebral discs might bulge or herniate under pressure.
These injuries cause inflammation, edema (swelling), and sometimes tiny hemorrhages, which is why your neck feels like it’s auditioning for a role as a rusty hinge. In severe cases, the rapid motion can even affect nerves, leading to symptoms like arm tingling or weakness (Grade 3 WAD). And if you’re unlucky, you might end up with a fracture or dislocation (Grade 4), but that’s rare.
Why the Cervical Spine Is Vulnerable
The cervical spine is like the acrobatic gymnast of your body—flexible but prone to injury if pushed too far. Here’s why it’s so susceptible in MVAs:
Flexibility: The cervical spine’s range of motion makes it great for turning your head but terrible at handling sudden, forceful movements.
Weight of the Head: Your head weighs about 10–12 pounds (like a bowling ball). When it’s whipped around, it puts massive stress on the neck’s delicate structures.
Lack of Support: Unlike your torso, which is strapped in by a seatbelt, your head is free to flop around, amplifying the forces on the cervical spine.
S-Curve Formation: That S-shaped curve during whiplash creates high shearing forces, especially at the C5–C6 level, where injuries are most common (Bogduk & Yoganandan, 2001).
Dr. Alexander Jimenez, a chiropractor and family nurse practitioner in El Paso, explains that these biomechanical forces are why even low-speed collisions (think 10–15 mph) can cause significant damage. “The cervical spine isn’t designed for rapid, unnatural movements,” he says. “When you add the element of surprise in an MVA, the muscles don’t have time to brace, leaving ligaments and joints to bear the brunt” (Jimenez, n.d.).
The Role of MVAs in WAD Development
MVAs, especially rear-end collisions, are the poster child for WAD because they perfectly set up the CAD mechanism. Studies show that 62% of people in MVAs report neck pain, with 93% feeling it within 24 hours (Schofferman et al., 2015). But it’s not just rear-end crashes—side impacts, frontal collisions, or even amusement park rides can trigger WAD. The key is the sudden acceleration-deceleration that throws your neck out of whack.
Chronic WAD, where symptoms last more than six months, affects up to 50% of victims with Grades 1 or 2 injuries. This is partly because the initial injury can lead to:
Sensory Hypersensitivity: Your nervous system gets cranky, making you more sensitive to pain or pressure (Sterling et al., 2006).
Motor Deficits: Reduced neck mobility and muscle weakness can persist, making it hard to turn your head without wincing.
Psychological Factors: Stress, anxiety, or post-traumatic stress disorder (PTSD) from the accident can amplify pain perception (Gaab et al., 2004).
Dr. Jimenez emphasizes that untreated or poorly managed WAD can spiral into chronic pain, which is why early intervention is critical. “The sooner we address the injury, the better we can prevent long-term complications,” he notes (Jimenez, n.d.).
References
Bogduk, N., & Yoganandan, N. (2001). Biomechanical basis of whiplash injury. Journal of Whiplash & Related Disorders, 1(1), 85–97.
Gaab, J., Baumann, S., Budnoik, A., Gmünder, H., Hottinger, N., & Ehlert, U. (2004). Reduced reactivity of the hypothalamic–pituitary–adrenal axis in chronic whiplash-associated disorder. Pain, 111(3), 289–297.
Jimenez, A. (n.d.). About Dr. Alex Jimenez. El Paso Back Clinic. https://elpasobackclinic.com/
Kaneoka, K., Ono, K., Inami, S., & Hayashi, K. (1999). Motion analysis of cervical vertebrae during whiplash loading. Spine, 24(8), 763–770.
Schofferman, J., Bogduk, N., & Slosar, P. (2015). Chronic whiplash and whiplash-associated disorders: An evidence-based approach. Journal of the American Academy of Orthopaedic Surgeons, 23(10), 596–606.
Sterling, M., Jull, G., Vicenzino, B., & Kenardy, J. (2006). Physical and psychological factors maintain long-term predictive capacity post-whiplash injury. Pain, 122(1–2), 102–108.
How WAD Affects Individuals from Auto Injuries
If you’ve ever had whiplash, you know it’s not just a pain in the neck (pun intended). WAD can turn everyday tasks—like driving, working, or even sleeping—into a challenge. Let’s explore how these injuries impact your life and why they’re such a big deal in personal injury cases.
Physical Impacts
The most obvious effect of WAD is physical discomfort. Neck pain and stiffness can make it hard to turn your head, which is a problem when you’re trying to check your mirrors or dodge a rogue shopping cart in the grocery store. Headaches, often caused by irritation of the upper cervical spine or occipital nerves, can feel like a marching band in your skull. For some, symptoms like dizziness or arm tingling add to the misery, making it tough to focus or stay active.
Chronic WAD is particularly sneaky. Studies show that 20–88% of chronic WAD patients report headaches, often linked to upper cervical spine injuries (Panjabi et al., 2004). Muscle strains in the neck and upper back, like the splenius capitis or trapezius, can lead to trigger points—those tender spots that feel like someone’s poking you with a hot needle (Elliott et al., 2016). In rare cases, WAD can even cause visual problems, like blurred vision or accommodative spasm, where your eyes refuse to focus properly (Endo et al., 2006).
Psychological and Social Impacts
WAD doesn’t just mess with your body—it can mess with your mind, too. The stress of an MVA, combined with ongoing pain, can lead to anxiety, depression, or PTSD. One study found that a significant number of WAD patients develop PTSD symptoms, which can make pain feel worse and recovery harder (Gaab et al., 2004). Socially, WAD can isolate you—nobody wants to go bowling when their neck feels like it’s made of concrete. Work can also take a hit, with some patients needing time off or struggling with tasks that require neck movement.
Economic and Legal Impacts
In places like El Paso, where MVAs are all too common, WAD is a major player in personal injury cases. In the U.S., whiplash-related claims account for over 65% of bodily injury claims, costing around $8 billion annually (Freeman, 1999). These cases often involve proving that the injury was caused by the accident, which is where medical expertise and legal documentation come in. Victims may face medical bills, lost wages, and the hassle of dealing with insurance companies, all while trying to heal.
Dr. Jimenez sees this firsthand in his El Paso practice. “Many of my patients are dealing with not just physical pain but the stress of navigating insurance claims or legal battles,” he says. “That’s why comprehensive care and clear documentation are so important” (Jimenez, n.d.).
References
Elliott, J. M., Hoggarth, M. A., Sparks, C. L., & Weber, K. A. (2016). Advancements in imaging technology: Do they (or will they) equate to advancements in our knowledge of recovery in whiplash? Journal of Orthopaedic & Sports Physical Therapy, 46(10), 862–872.
Endo, K., Ichimaru, K., Komagata, M., & Yamamoto, K. (2006). Cervical vertigo and dizziness after whiplash injury. European Spine Journal, 15(6), 886–890.
Freeman, M. D. (1999). A review and methodologic critique of the literature refuting whiplash syndrome. Spine, 24(1), 86–98.
Gaab, J., Baumann, S., Budnoik, A., Gmünder, H., Hottinger, N., & Ehlert, U. (2004). Reduced reactivity of the hypothalamic–pituitary–adrenal axis in chronic whiplash-associated disorder. Pain, 111(3), 289–297.
Jimenez, A. (n.d.). About Dr. Alex Jimenez. El Paso Back Clinic. https://elpasobackclinic.com/
Panjabi, M. M., Ito, S., Pearson, A. M., & Ivancic, P. C. (2004). Injury mechanisms of the cervical intervertebral disc during simulated whiplash. Spine, 29(11), 1217–1225.
The Science of Motion- Video
Treatments for WAD and Cervical Spine Injuries
Good news: You don’t have to live with WAD forever. With the right treatments, most people recover within weeks or months, though chronic cases may need extra TLC. Let’s explore the evidence-based options, with insights from Dr. Jimenez, who’s been helping El Pasoans get back on their feet (or at least turn their heads) for years.
Conservative Treatments
Conservative treatments—those that don’t involve surgery—are the first line of defense for WAD Grades 1–3. These include:
Active Mobilization: Forget the soft collar (unless your doctor insists). Studies show that early movement, like gentle neck exercises, speeds up recovery compared to immobilization (Schnabel et al., 2004). Dr. Jimenez often prescribes range-of-motion exercises to restore flexibility without aggravating the injury.
Physical Therapy: A physical therapist can guide you through exercises to strengthen deep neck flexors (like the longus colli) and scapula stabilizers (like the rhomboids). This helps take pressure off the cervical spine and improves posture (Kay et al., 2005).
Manual Therapy: Chiropractic adjustments or mobilization can reduce pain and improve joint mobility. Dr. Jimenez uses spinal manipulation to realign the cervical spine, which can relieve pressure on irritated nerves and joints (Bryans et al., 2014).
Pain Management: Over-the-counter meds like ibuprofen or acetaminophen can help with pain and inflammation. For severe cases, doctors might prescribe muscle relaxants or short-term steroids (Peloso et al., 2007).
Dr. Jimenez emphasizes a multimodal approach, combining these treatments for the best results. “No single treatment works for everyone,” he says. “We tailor the plan to the patient’s symptoms, whether it’s muscle spasms, joint dysfunction, or nerve irritation” (Jimenez, n.d.).
Advanced Interventions
For chronic WAD or cases that don’t respond to conservative care, more advanced options may be considered:
Trigger Point Injections: Injecting a local anesthetic or botulinum toxin (Botox) into trigger points can reduce pain and improve range of motion. One study found that Botox injections into muscles like the trapezius helped chronic WAD patients after just four weeks (Freund & Schwartz, 2000).
Radiofrequency Neurotomy: For persistent facet joint pain, this procedure uses heat to disrupt pain signals from the nerves. It’s effective for some chronic WAD cases but requires careful diagnosis (Lord et al., 1996).
Psychological Support: If PTSD or anxiety is making pain worse, cognitive-behavioral therapy (CBT) can help. Dr. Jimenez often refers patients to counselors to address the emotional side of recovery (Teasell et al., 2010).
Dr. Jimenez’s Approach to Treatment
At El Paso Back Clinic, Dr. Jimenez combines chiropractic care, physical therapy, and advanced diagnostics to create personalized treatment plans. His dual training as a chiropractor and family nurse practitioner gives him a unique perspective, allowing him to address both the physical and systemic aspects of WAD. He often uses:
Chiropractic Adjustments: To restore proper alignment and reduce joint irritation.
Therapeutic Exercises: To strengthen neck muscles and improve stability.
Lifestyle Advice: To help patients avoid activities that strain the cervical spine, like hunching over a phone (we’re all guilty of that).
Dr. Jimenez also stresses the importance of patient education. “When patients understand their injury and what they can do about it, they’re more likely to stick with the plan and recover faster,” he says (Jimenez, n.d.).
References
Bryans, R., Decina, P., Descarreaux, M., Duranleau, M., Marcoux, H., Potter, B., … & White, E. (2014). Evidence-based guidelines for the chiropractic treatment of adults with neck pain. Journal of Manipulative and Physiological Therapeutics, 37(1), 42–63.
Freund, B. J., & Schwartz, M. (2000). Treatment of whiplash-associated disorders with botulinum toxin-A: A pilot study. Journal of Rheumatology, 27(9), 2222–2226.
Jimenez, A. (n.d.). About Dr. Alex Jimenez. El Paso Back Clinic. https://elpasobackclinic.com/
Kay, T. M., Gross, A., Goldsmith, C., Santaguida, P. L., Hoving, J., & Bronfort, G. (2005). Exercises for mechanical neck disorders. Cochrane Database of Systematic Reviews, (3), CD004250.
Lord, S. M., Barnsley, L., Wallis, B. J., McDonald, G. J., & Bogduk, N. (1996). Percutaneous radio-frequency neurotomy for chronic cervical zygapophyseal-joint pain. New England Journal of Medicine, 335(23), 1721–1726.
Peloso, P., Gross, A., Haines, T., Trinh, K., Goldsmith, C. H., & Burnie, S. (2007). Medicinal and injection therapies for mechanical neck disorders. Cochrane Database of Systematic Reviews, (3), CD000319.
Schnabel, M., Ferrari, R., Vassiliou, T., & Kaluza, G. (2004). Randomised, controlled outcome study of active mobilisation compared with collar therapy for whiplash injury. Emergency Medicine Journal, 21(3), 306–310.
Teasell, R. W., McClure, J. A., Walton, D., Pretty, J., Salter, K., Meyer, M., … & Death, B. (2010). A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): Part 3 – interventions for subacute WAD. Pain Research & Management, 15(5), 305–312.
Recovery from WAD: Preventing Further Damage
Recovering from WAD is like trying to get your car back in shape after a fender-bender—it takes time, effort, and a good mechanic (or, in this case, a chiropractor). The goal is to heal the cervical spine, reduce symptoms, and prevent chronic issues. Here’s how to do it, with tips from Dr. Jimenez and the latest research.
Early Intervention
The first 12 weeks after an MVA are critical. Research shows that active mobilization—starting gentle exercises within days of the injury—leads to faster recovery and less pain than wearing a soft collar (Rosenfeld et al., 2005). Dr. Jimenez recommends starting with simple range-of-motion exercises, like slowly turning your head side to side, to keep the cervical spine mobile without overdoing it.
Physical Therapy and Exercise
Physical therapy is your best friend during recovery. A therapist can teach you exercises to strengthen neck muscles and improve stability, which helps protect the cervical spine from further strain. For example:
Isometric Exercises: Pressing your hand against your forehead without moving your head strengthens neck flexors.
Scapular Retractions: Pulling your shoulder blades back improves posture and reduces stress on the neck.
Stretching: Gentle stretches for the trapezius and levator scapulae muscles can relieve tightness.
Dr. Jimenez often incorporates thoracic spine exercises, too, since poor upper back mobility can put extra pressure on the cervical spine (Pho & Godges, 2004).
Avoiding Reinjury
To prevent further damage, you’ll need to make some lifestyle tweaks:
Posture Check: Sit up straight and avoid slouching, especially when using your phone or computer. Dr. Jimenez calls this “text neck prevention 101.”
Ergonomics: Adjust your car seat so your headrest supports the back of your head, reducing whiplash risk in future accidents.
Activity Modification: Avoid heavy lifting or high-impact activities (sorry, no wrestling matches) until your neck is stronger.
Monitoring Progress
Recovery isn’t a straight line—some days you’ll feel great, others like you got hit by a truck (again). Regular check-ins with your healthcare provider are key to track progress and adjust your treatment plan. Dr. Jimenez uses tools like the Neck Disability Index (NDI) to measure how WAD affects your daily life and ensure you’re on the right path (Vernon & Mior, 1991).
Long-Term Recovery
For most people, WAD symptoms improve within 3–6 months, but chronic cases can linger. To avoid this, stick with your treatment plan, even when you start feeling better. Dr. Jimenez warns, “Stopping therapy too soon is like pulling a cake out of the oven before it’s done—it might look okay, but it’s not fully set” (Jimenez, n.d.). Long-term strategies include:
Maintenance Exercises: Keep up with neck and upper back strengthening to maintain stability.
Stress Management: Techniques like meditation or yoga can reduce tension that exacerbates neck pain.
Regular Chiropractic Care: Periodic adjustments can prevent minor issues from becoming major problems.
References
Jimenez, A. (n.d.). About Dr. Alex Jimenez. El Paso Back Clinic. https://elpasobackclinic.com/
Pho, C., & Godges, J. (2004). Management of whiplash-associated disorder addressing thoracic and cervical spine impairments: A case report. Journal of Orthopaedic & Sports Physical Therapy, 34(9), 511–523.
Rosenfeld, M., Seferiadis, A., & Gunnarsson, R. (2005). Active involvement and intervention in patients exposed to whiplash trauma in automobile crashes reduces costs: A randomized, controlled clinical trial and health economic evaluation. Spine, 30(16), 1799–1804.
Vernon, H., & Mior, S. (1991). The Neck Disability Index: A study of reliability and validity. Journal of Manipulative and Physiological Therapeutics, 14(7), 409–415.
Dr. Alexander Jimenez: El Paso’s Personal Injury Expert
In El Paso, where I-10 traffic can feel like a demolition derby, personal injury cases from MVAs are a fact of life. Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a standout practitioner helping victims of WAD and other auto injuries get back on track. With over 30 years of experience, he’s not just a chiropractor—he’s a medical-legal liaison who bridges the gap between healing and justice.
Advanced Diagnostics and Imaging
Dr. Jimenez doesn’t mess around when it comes to diagnosing WAD. He uses advanced imaging like:
X-Rays: To rule out fractures or dislocations (Grade 4 WAD). Dynamic X-rays, where you move your head during the scan, can spot instability not visible in standard views (Ronnen et al., 1996).
MRI: To check for soft tissue damage, like ligament tears or disc herniations, which are common in WAD but often missed on X-rays (Krakenes & Kaale, 2006).
CT Scans: For detailed views of bones or suspected fractures, especially in complex cases.
These tools help him pinpoint the exact cause of your symptoms, whether it’s a sprained ligament, an irritated facet joint, or a cranky nerve. “Accurate diagnosis is the foundation of effective treatment,” Dr. Jimenez says. “Without it, you’re just guessing” (Jimenez, n.d.).
Dual-Scope Procedures
Dr. Jimenez’s dual training as a chiropractor and nurse practitioner gives him a “dual-scope” approach, blending hands-on therapies with medical expertise. For example, he might combine chiropractic adjustments with trigger point injections or refer patients for advanced procedures like radiofrequency neurotomy if needed. This holistic approach ensures that both the structural and systemic aspects of WAD are addressed.
Medical-Legal Liaison Role
Personal injury cases require airtight documentation to prove that the MVA caused your injuries, and Dr. Jimenez excels at this. He provides detailed reports that link your symptoms to the accident, using data from imaging, physical exams, and diagnostic evaluations. These reports are gold for attorneys, helping them build strong cases for compensation. He also works closely with legal teams to ensure patients get the medical care they need while their claims are processed.
In El Paso, where personal injury claims are common, Dr. Jimenez’s reputation is unmatched. His LinkedIn profile highlights his commitment to “functional medicine and injury care,” with a focus on helping patients recover physically and financially (Jimenez, n.d.). Whether you’re dealing with insurance adjusters or preparing for court, Dr. Jimenez is the guy you want in your corner.
References
Jimenez, A. (n.d.). About Dr. Alex Jimenez. El Paso Back Clinic. https://elpasobackclinic.com/
Jimenez, A. (n.d.). Dr. Alex Jimenez’s LinkedIn profile. LinkedIn. https://www.linkedin.com/in/dralexjimenez/
Krakenes, J., & Kaale, B. R. (2006). Magnetic resonance imaging assessment of craniovertebral ligaments and membranes after whiplash trauma. Spine, 31(25), 2820–2826.
Ronnen, H. R., de Korte, P. J., Brink, P. R., van der Bijl, H. J., Tonino, A. J., & Franke, C. L. (1996). Acute whiplash injury: Is there a role for MR imaging? A prospective study of 100 patients. Radiology, 201(1), 93–96.
The Importance of Personal Injury Cases in El Paso
El Paso’s busy roads, from I-10 to Loop 375, see their fair share of MVAs, making personal injury cases a big deal. WAD is a leading injury in these cases because it’s so common and can have long-lasting effects. Victims often face medical bills, lost income, and pain that disrupts their lives, which is why fair compensation is crucial.
Personal injury cases hinge on proving causation—that the MVA caused your injuries—and documenting the extent of the damage. This is where medical experts like Dr. Jimenez shine. His detailed evaluations and imaging reports provide the evidence needed to show that your neck pain or headaches are directly tied to the accident. Without this, insurance companies might try to lowball you, claiming your symptoms are “preexisting” or “not that bad.”
Dr. Jimenez’s work goes beyond the clinic. By acting as a medical-legal liaison, he ensures that patients get the care they need while their legal cases move forward. His reports can make or break a claim, helping victims secure settlements for medical costs, lost wages, and pain and suffering. In a city like El Paso, where community matters, having a trusted practitioner like Dr. Jimenez is a game-changer.
Conclusion
Whiplash-associated disorders are a serious consequence of motor vehicle accidents, driven by the cervical spine’s vulnerability to rapid acceleration-deceleration forces. These injuries, ranging from mild neck pain to chronic disability, can disrupt lives physically, emotionally, and financially. Understanding the biomechanical causes—like the S-shaped curve that stresses ligaments, muscles, and joints—helps explain why WAD is so common in MVAs. Early intervention, through conservative treatments like physical therapy and chiropractic care, is critical to prevent chronic pain and restore function. In El Paso, Dr. Alexander Jimenez stands out as a leader in WAD care, using advanced diagnostics, dual-scope procedures, and medical-legal expertise to help victims recover and seek justice.
Disclaimer: This blog post is for informational purposes only and should not be taken as medical or legal advice. Always consult a qualified healthcare provider or attorney for personalized guidance. The information provided is based on current research and clinical insights, but individual cases vary, and professional evaluation is essential.
References
Spitzer, W. O., Skovron, M. L., Salmi, L. R., Cassidy, J. D., Duranceau, J., Suissa, S., & Zeiss, E. (1995). Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: Redefining “whiplash” and its management. Spine, 20(8S), 1S–73S.
Bogduk, N., & Yoganandan, N. (2001). Biomechanical basis of whiplash injury. Journal of Whiplash & Related Disorders, 1(1), 85–97.
Kaneoka, K., Ono, K., Inami, S., & Hayashi, K. (1999). Motion analysis of cervical vertebrae during whiplash loading. Spine, 24(8), 763–770.
Schofferman, J., Bogduk, N., & Slosar, P. (2015). Chronic whiplash and whiplash-associated disorders: An evidence-based approach. Journal of the American Academy of Orthopaedic Surgeons, 23(10), 596–606.
Sterling, M., Jull, G., Vicenzino, B., & Kenardy, J. (2006). Physical and psychological factors maintain long-term predictive capacity post-whiplash injury. Pain, 122(1–2), 102–108.
Gaab, J., Baumann, S., Budnoik, A., Gmünder, H., Hottinger, N., & Ehlert, U. (2004). Reduced reactivity of the hypothalamic–pituitary–adrenal axis in chronic whiplash-associated disorder. Pain, 111(3), 289–297.
Panjabi, M. M., Ito, S., Pearson, A. M., & Ivancic, P. C. (2004). Injury mechanisms of the cervical intervertebral disc during simulated whiplash. Spine, 29(11), 1217–1225.
Elliott, J. M., Hoggarth, M. A., Sparks, C. L., & Weber, K. A. (2016). Advancements in imaging technology: Do they (or will they) equate to advancements in our knowledge of recovery in whiplash? Journal of Orthopaedic & Sports Physical Therapy, 46(10), 862–872.
Endo, K., Ichimaru, K., Komagata, M., & Yamamoto, K. (2006). Cervical vertigo and dizziness after whiplash injury. European Spine Journal, 15(6), 886–890.
Freeman, M. D. (1999). A review and methodologic critique of the literature refuting whiplash syndrome. Spine, 24(1), 86–98.
Bryans, R., Decina, P., Descarreaux, M., Duranleau, M., Marcoux, H., Potter, B., … & White, E. (2014). Evidence-based guidelines for the chiropractic treatment of adults with neck pain. Journal of Manipulative and Physiological Therapeutics, 37(1), 42–63.
Freund, B. J., & Schwartz, M. (2000). Treatment of whiplash-associated disorders with botulinum toxin-A: A pilot study. Journal of Rheumatology, 27(9), 2222–2226.
Kay, T. M., Gross, A., Goldsmith, C., Santaguida, P. L., Hoving, J., & Bronfort, G. (2005). Exercises for mechanical neck disorders. Cochrane Database of Systematic Reviews, (3), CD004250.
Peloso, P., Gross, A., Haines, T., Trinh, K., Goldsmith, C. H., & Burnie, S. (2007). Medicinal and injection therapies for mechanical neck disorders. Cochrane Database of Systematic Reviews, (3), CD000319.
Schnabel, M., Ferrari, R., Vassiliou, T., & Kaluza, G. (2004). Randomised, controlled outcome study of active mobilisation compared with collar therapy for whiplash injury. Emergency Medicine Journal, 21(3), 306–310.
Teasell, R. W., McClure, J. A., Walton, D., Pretty, J., Salter, K., Meyer, M., … & Death, B. (2010). A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): Part 3 – interventions for subacute WAD. Pain Research & Management, 15(5), 305–312.
Pho, C., & Godges, J. (2004). Management of whiplash-associated disorder addressing thoracic and cervical spine impairments: A case report. Journal of Orthopaedic & Sports Physical Therapy, 34(9), 511–523.
Rosenfeld, M., Seferiadis, A., & Gunnarsson, R. (2005). Active involvement and intervention in patients exposed to whiplash trauma in automobile crashes reduces costs: A randomized, controlled clinical trial and health economic evaluation. Spine, 30(16), 1799–1804.
Vernon, H., & Mior, S. (1991). The Neck Disability Index: A study of reliability and validity. Journal of Manipulative and Physiological Therapeutics, 14(7), 409–415.
Krakenes, J., & Kaale, B. R. (2006). Magnetic resonance imaging assessment of craniovertebral ligaments and membranes after whiplash trauma. Spine, 31(25), 2820–2826.
Ronnen, H. R., de Korte, P. J., Brink, P. R., van der Bijl, H. J., Tonino, A. J., & Franke, C. L. (1996). Acute whiplash injury: Is there a role for MR imaging? A prospective study of 100 patients. Radiology, 201(1), 93–96.
Jimenez, A. (n.d.). Dr. Alex Jimenez’s LinkedIn profile. LinkedIn. https://www.linkedin.com/in/dralexjimenez/
Find out how cervical collars are used for MVAs, which provide crucial support during recovery from cervical injuries like whiplash.
Whiplash Injuries and the Cervical Spine: A Comprehensive Guide to Motor Vehicle Accident Recovery
Introduction: The Whiplash Wake-Up Call
Picture this: you’re cruising down the road, maybe humming along to your favorite tune, when—bam!—a car slams into your rear bumper. Your heart races, your car’s a mess, and soon, your neck starts to complain. Welcome to the world of whiplash, a neck injury that’s as common as it is misunderstood. Whiplash happens when your head is whipped back and forth, like a slinky toy caught in a windstorm, straining the delicate structures of your neck. It’s estimated that around one million whiplash injuries occur each year in the United States, making it a leading cause of neck pain from motor vehicle accidents (MVAs) (ScienceDirect, n.d.). While many people bounce back quickly, others face lingering pain, making proper understanding and treatment critical.
In this guide, we’ll dive into why whiplash is so closely tied to MVAs, how it affects the cervical spine, and what treatments work best. We’ll also spotlight Dr. Alexander Jimenez, a dual-licensed chiropractor and nurse practitioner in El Paso, who’s helping MVA victims recover and navigate personal injury cases with expertise. So, buckle up (safely, of course) as we explore this neck-twisting topic with a sprinkle of humor to keep things light!
Understanding the Cervical Spine: Your Neck’s Delicate Design
Your neck, or cervical spine, is like the unsung hero of your body—it holds up your head (all 10-12 pounds of it!) while letting you nod, shake, and tilt like a bobblehead. It’s composed of seven vertebrae, labeled C1 to C7, which form a gentle curve known as lordosis. These bones protect the spinal cord, support the skull, and allow a wide range of motion, from checking your blind spots to head-banging at a concert (Johns Hopkins Medicine, 2024).
But this flexibility is a double-edged sword. The cervical spine’s design makes it vulnerable during MVAs, especially rear-end collisions. When a car is hit, the sudden force can push the body forward while the head lags behind, stretching muscles, ligaments, and even nerves beyond their normal limits. Think of it like pulling a rubber band too far—it might not snap, but it’s not happy (Cleveland Clinic, 2022).
Table 1: Key Structures of the Cervical Spine Affected by Whiplash
The Mechanism of Whiplash: A Neck-Snapping Rollercoaster
So, how does a simple fender-bender turn your neck into a grumpy, achy mess? The biomechanics of whiplash, also known as cervical acceleration-deceleration (CAD) injury, are akin to a high-speed dance gone wrong. In a rear-end collision, the car is suddenly pushed forward, and your body follows, pressed against the seat. Your head, however, plays hard to get, staying put due to inertia before snapping backward and then forward. This rapid motion creates an S-shaped curve in the cervical spine, stressing the lower vertebrae into extension and the upper ones into flexion (Physiopedia, n.d.).
Research suggests that this movement can strain muscles, sprain ligaments such as the nuchal and anterior longitudinal ligaments, and even compress facet joints. In severe cases, it may lead to disc herniation or nerve irritation. One study found that the forces in low-speed collisions (8.7-14.2 km/h) are enough to cause these injuries, debunking the myth that only high-speed crashes cause whiplash (PubMed, 1998). It’s like your neck is trying to do a gymnastics routine it never practiced for!
Symptoms and Diagnosis: When Your Neck Says “Ouch”
Whiplash symptoms can be as sneaky as a cat burglar, sometimes not showing up until hours or days after the accident. Common complaints include:
Neck pain and stiffness
Headaches, often starting at the base of the skull
Dizziness or vertigo
Shoulder or upper arm pain
Tingling or numbness in the arms (Healthline, 2023).
In some cases, patients report cognitive issues like trouble concentrating or irritability, which may signal a concurrent concussion (Cognitive FX, 2023). Diagnosing whiplash can be challenging because soft tissue damage often doesn’t show up on X-rays or MRIs. Doctors rely on a patient’s history and physical exam, checking for tenderness, range of motion, and neurological signs. It’s a bit like being a detective, piecing together clues without a clear picture (Mayo Clinic, 2024).
Treatment Options: Getting Your Neck Back in the Game
Treating whiplash is all about relieving pain and restoring function without turning your neck into a permanent grumpy cat. In the past, cervical collars were the go-to, like a neck brace straight out of a sci-fi movie. But research now suggests they may do more harm than good for most whiplash cases. A 2008 study found that collars are primarily beneficial for spinal fractures, rather than soft tissue injuries, and prolonged use can lead to muscle degeneration and reduced function (El Paso Chiropractor Blog, 2016). 68% of whiplash patients in one study were prescribed collars, but those who wore them were more likely to miss work compared to those who didn’t.
Instead, active treatments shine. Chiropractic care, including neck adjustments and manual manipulation, can improve symptoms in up to 93% of patients (El Paso Chiropractor Blog, 2016). Physical therapy, gentle stretches, and exercises also help strengthen the neck and speed recovery. Pain relievers like ibuprofen may be used short-term, but the goal is to keep moving, not stay still like a statue.
Table 2: Comparison of Whiplash Treatment Approaches
In El Paso, Dr. Alexander Jimenez stands out as a beacon of hope for whiplash victims. As a dual-licensed Doctor of Chiropractic (DC) and Family Nurse Practitioner (FNP-BC), he brings a unique blend of expertise to the table. At his El Paso Chiropractic Rehabilitation Clinic and Integrated Medicine Center, Dr. Jimenez utilizes evidence-based protocols to treat complex injuries, such as whiplash. His approach includes chiropractic adjustments, functional medicine assessments, and sports medicine techniques, tailored to each patient’s needs (El Paso Back Clinic, n.d.).
Dr. Jimenez doesn’t just stop at treatment. He employs advanced imaging and diagnostic evaluations to pinpoint the extent of injuries, ensuring a comprehensive recovery plan. His dual-scope procedures—combining chiropractic and medical perspectives—make him a trusted partner for patients navigating the aftermath of MVAs. Plus, he’s got a knack for making patients feel at ease, like a friendly guide helping you through a neck-pain maze.
Getting rear-ended is bad enough, but dealing with insurance claims and legal battles can feel like adding insult to injury. Personal injury cases arise when someone’s negligence, like a distracted driver, causes harm. In these cases, victims may seek compensation for medical bills, lost wages, and pain and suffering. Accurate medical documentation is the backbone of these claims, and this is where Dr. Jimenez shines in El Paso.
With his expertise, Dr. Jimenez provides detailed medical reports that link injuries to the MVA, using advanced imaging and diagnostics. He acts as a liaison between medical care and legal proceedings, ensuring patients’ injuries are properly documented for court or insurance purposes. It’s like having a translator who speaks both “doctor” and “lawyer,” making sure nothing gets lost in translation (El Paso Back Clinic, n.d.).
Whiplash from MVAs can turn your life upside down, but with the right care, recovery is within reach. The cervical spine’s vulnerability makes it prone to injury, but active treatments like chiropractic care and physical therapy offer the best chance of returning to normal. In El Paso, Dr. Alexander Jimenez provides expert care, combining medical and chiropractic expertise to help patients heal and navigate personal injury cases. Disclaimer: This article is for informational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.
Texting and motor vehicle accidents are preventable. Explore the dangers and advocate for responsible driving practices.
The Perils of Distraction: Texting While Driving and Its Impact on Auto Injuries
Introduction
Picture this: you’re cruising down the highway, your favorite song blasting, when your phone pings with a new text. It’s tempting to glance at it—just for a second, right? But that quick peek could change everything. Texting while driving is a leading cause of motor vehicle accidents (MVAs), often resulting in serious injuries like whiplash, which can lead to chronic neck pain and long-term health challenges. In El Paso, Texas, experts like Dr. Alexander Jimenez, DC, APRN, FNP-BC, are helping victims recover from these injuries while supporting their personal injury cases with advanced diagnostics and medical expertise.
This comprehensive blog post explores the dangers of texting while driving, the clinical reasons it leads to MVAs and injuries like whiplash, and how these injuries contribute to chronic neck pain. We’ll also delve into Dr. Jimenez’s role as a distinguished practitioner in El Paso, highlighting his utilization of advanced imaging and diagnostic tools to bridge the gap between medical and legal needs. To keep things engaging, we’ll sprinkle in a bit of humor—because who doesn’t need a chuckle when discussing serious topics? However, don’t worry, we’ll conclude with a serious note and a disclaimer to ensure the gravity of this issue is clear.
The Dangers of Distracted Driving
Distracted driving is any activity that takes your focus away from driving, and texting is the most alarming culprit. According to the National Highway Traffic Safety Administration (NHTSA), distracted driving resulted in 3,275 fatalities in the U.S. in 2023 (NHTSA, 2023). Texting while driving is particularly dangerous because it involves three types of distractions:
Visual: Taking your eyes off the road to read or send a text.
Manual: Removing your hands from the steering wheel to type.
Cognitive: Diverting your mental focus from driving to the message.
A study by the Virginia Tech Transportation Institute found that texting increases the risk of a crash or near-crash by 23 times compared to driving without distractions (Virginia Tech Transportation Institute, 2009). When you text, your eyes are off the road for an average of 5 seconds. At 55 mph, that’s like driving the length of a football field blindfolded (NHTSA, 2023).
The statistics are sobering:
In 2019, over 3,100 people were killed and about 424,000 were injured in crashes involving distracted drivers (CDC, 2024).
About one in five people killed in distraction-related crashes were not in vehicles—they were pedestrians or cyclists (Gruel Mills Nims & Pylman PLLC, 2022).
Distracted driving accounts for over 58% of teen crashes, with texting being a major factor (Gruel Mills Nims & Pylman PLLC, 2022).
A Touch of Humor: If cars could talk, they might honk and say, “Put the phone down, pal—I’m not a texting booth!” Or maybe, “I’m built for driving, not for typing love notes!” These playful reminders serve as a reminder to stay focused behind the wheel.
Table 1: Distracted Driving Statistics (2023)
Metric
Data
Deaths in distraction-affected crashes
3,275 (NHTSA, 2023)
Injuries in distraction-affected crashes
~325,000 (NHTSA, 2023)
Teen crashes due to distraction
>58% (Gruel Mills Nims & Pylman PLLC, 2022)
Crash risk increase from texting
23 times higher (Virginia Tech Transportation Institute, 2009)
Virginia Tech Transportation Institute. (2009). Impact of Text Messaging on Driver Behavior in Naturalistic Driving.
Whiplash Injuries: The Clinical Connection to MVAs
Whiplash is a neck injury caused by a sudden, forceful back-and-forth movement of the head, most commonly in rear-end collisions. These accidents are often linked to distracted driving, as texting drivers may fail to stop in time when traffic slows. The clinical impact of whiplash is significant, with research indicating that it affects approximately one million people annually in the U.S., resulting in medical expenses of up to $29 billion and lost productivity (Pearson et al., 2006).
Clinical Rationale for Whiplash
A study in BMC Musculoskeletal Disorders provides key insights into why whiplash is so debilitating:
Whiplash significantly weakens neck ligaments, with a failure force of 149.4 N compared to 186.0 N in controls (P = 0.036) (Pearson et al., 2006).
Ligaments, such as the ligamentum flavum and interspinous ligaments, exhibit increased laxity, which can lead to chronic pain due to altered muscle responses and inflammation (Pearson et al., 2006).
Pain relief techniques, such as nerve blocks and radiofrequency ablation, confirm that damage to capsular ligament nerves contributes to symptoms (Pearson et al., 2006).
These findings support the ligament-injury hypothesis, suggesting that even minor collisions can cause microscopic tears in neck ligaments, which can lead to long-term issues.
Chronic Neck Pain: A Lasting Impact
Whiplash often leads to chronic neck pain, which can persist for months or years. Symptoms include stiffness, headaches, and reduced range of motion. In severe cases, it may cause cervical radiculopathy (nerve root compression) or myelopathy (spinal cord compression). A study in Pain found that patients with chronic whiplash-associated disorder (WAD) have altered sensorimotor control, which may explain persistent symptoms (Sterling et al., 2003).
A Touch of Humor: If your neck could complain after a whiplash injury, it might say, “Ouch! I wasn’t built for this rollercoaster ride!” Or, “Next time, tell that distracted driver to keep their eyes on the road, not their phone!” Humor aside, whiplash is no laughing matter, and proper treatment is essential.
Table 2: Whiplash Injury Statistics
Metric
Data
Annual U.S. incidence
~1 million (Pearson et al., 2006)
Societal cost
Up to $29 billion (Pearson et al., 2006)
Ligament failure force (whiplash vs. control)
149.4 N vs. 186.0 N (P = 0.036) (Pearson et al., 2006)
Chronic symptom prevalence
5-8% of patients (Pearson et al., 2006)
References:
Pearson, A. M., et al. (2006). Whiplash causes increased laxity of cervical capsular ligament. BMC Musculoskeletal Disorders, 7, 103. Retrieved from http://www.biomedcentral.com/1471-2474/7/103
Sterling, M., et al. (2003). Sensory hypersensitivity occurs soon after whiplash injury and is associated with poor recovery. Pain, 104(3), 509-517.
Pain Relief Through Chiropractic- Video
Dr. Alexander Jimenez: A Leader in Auto Injury Treatment
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a highly respected chiropractor and functional medicine practitioner in El Paso, Texas, with over 30 years of experience (Dr. Alexander Jimenez, n.d.). His clinic, El Paso Back Clinic, specializes in treating complex injuries from auto accidents, including whiplash and soft tissue damage (El Paso Back Clinic, n.d.).
Clinical Approach to Auto Injuries
Dr. Jimenez employs a patient-centered approach, utilizing advanced imaging techniques (e.g., MRI, CT scans) and comprehensive diagnostic evaluations to assess injuries accurately. He reportedly uses dual-scope procedures—though specific details are limited—to develop personalized treatment plans (Personal Injury Doctor Group, n.d.). His methods focus on non-invasive treatments, avoiding drugs or surgery when possible.
Dr. Jimenez emphasizes the biomechanics of whiplash, noting that rapid acceleration-deceleration forces can cause microscopic tears in neck ligaments and muscles, leading to inflammation and pain (Jimenez, n.d.). He states, “Whiplash is often underestimated because there are no broken bones or visible injuries. However, the damage to soft tissues can be significant and lead to chronic pain if not properly treated” (Jimenez, n.d.).
Role in Personal Injury Cases
In El Paso, personal injury cases from MVAs are common, and Dr. Jimenez is a key figure in supporting victims. His ability to provide detailed, evidence-based medical reports is crucial for insurance claims and legal proceedings. These reports link patient injuries to the accident’s circumstances, helping victims secure fair compensation (Personal Injury Doctor Group, n.d.). Dr. Jimenez acts as a liaison between medical and legal services, ensuring accurate documentation.
A Touch of Humor: If Dr. Jimenez’s clinic had a slogan, it might be, “We’ll fix your neck and help you get that check!” Or, “From whiplash to winning your case, we’ve got your back!” These lighthearted phrases reflect his dual role in healing and advocacy.
Table 3: Dr. Jimenez’s Expertise
Area
Details
Experience
Over 30 years in chiropractic care (Dr. Alexander Jimenez, n.d.)
Specialties
Auto injuries, whiplash, soft tissue injuries (El Paso Back Clinic, n.d.)
Diagnostic Tools
MRI, CT scans, dual-scope procedures (Personal Injury Doctor Group, n.d.)
Role in Legal Cases
Provides evidence-based reports for personal injury claims (Personal Injury Doctor Group, n.d.)
Texting while driving is a triple threat, as it distracts drivers visually, manually, and cognitively. The Centers for Disease Control and Prevention (CDC) reports that nine people are killed daily in the U.S. in crashes involving distracted drivers (CDC, 2024). In Texas, where distracted driving caused nearly one in five crashes in 2024, 373 people died and 2,587 were seriously injured (TxDOT, n.d.).
Dr. Jimenez notes that distracted drivers, particularly those texting, have delayed reaction times, increasing the likelihood of high-impact collisions (Jimenez, n.d.). These crashes often result in severe injuries like whiplash, which can have lasting effects if not treated promptly.
A Touch of Humor: Imagine a road sign that reads, “Texting Zone: Next Crash Ahead!” Or a car’s GPS chiming in, “Recalculating… because you’re too busy texting!” These playful nudges remind us to keep our phones down and our eyes on the road.
El Paso sees a high volume of personal injury cases due to MVAs, many linked to distracted driving. Dr. Jimenez’s clinic is a trusted resource for victims, offering acute injury treatment and rehabilitation for conditions like whiplash (El Paso Back Clinic, n.d.). His detailed medical reports, supported by advanced imaging and diagnostics, provide critical evidence for legal claims, helping victims navigate the complex process of seeking compensation (Personal Injury Doctor Group, n.d.).
Texting while driving is a dangerous habit that significantly increases the risk of motor vehicle accidents, leading to injuries like whiplash and chronic neck pain. The clinical evidence is clear: distraction delays reaction times, resulting in high-impact collisions that damage neck ligaments and cause lasting pain. Experts like Dr. Alexander Jimenez in El Paso play a vital role in treating these injuries and supporting personal injury cases with advanced diagnostics and detailed medical reports.
Drivers must prioritize safety by avoiding distractions, such as texting. For those injured in MVAs, seeking expert medical care and legal advice is essential to recovery and justice. Let’s all commit to keeping our eyes on the road and our hands on the wheel.
Disclaimer: This blog post is for informational purposes only and does not constitute medical or legal advice. If you’ve been in a motor vehicle accident, seek immediate medical attention from a qualified healthcare professional. For legal matters, consult an attorney specializing in personal injury law.
Auto injuries in rotator cuffs can lead to significant discomfort. Discover how to manage and recover from these injuries effectively.
Shoulder Pain and Injuries from Motor Vehicle Accidents: A Comprehensive Guide
Welcome to the grim reality of motor vehicle accidents (MVAs), where the road to recovery can be as bumpy as a poorly paved highway. If you’ve ever found yourself clutching your shoulder after a car crash, you’re not alone. Shoulder injuries are a common souvenir of MVAs, and they come with a side of pain that can make you feel like you’re auditioning for a role in a tragic play. But fear not, dear reader, for we’re about to dissect the clinical reasons behind this misery with a touch of Wednesday Addams’ dark humor—because nothing says “fun” like exploring the mechanics of bodily harm.
In this extensive guide, we’ll unravel why shoulder pain and injuries are so prevalent after MVAs, focusing on the rotator cuff’s starring role in this unfortunate drama. We’ll also spotlight Dr. Alexander Jimenez, a distinguished chiropractor in El Paso, Texas, whose expertise in treating MVA victims and navigating personal injury cases is nothing short of legendary. So, let’s buckle up (safely, of course) and dive into the twisted world of shoulder injuries.
Anatomy of the Shoulder: A Delicate Dance of Bones and Tendons
To understand why your shoulder throws a tantrum after an MVA, let’s first take a peek under the hood. The shoulder is like a gothic ballroom, where bones, muscles, and tendons perform a delicate dance—until a car crash turns it into a mosh pit.
The shoulder is a ball-and-socket joint, where the head of the humerus (upper arm bone) nestles into the glenoid cavity of the scapula (shoulder blade). This design allows for a wide range of motion, letting you wave dramatically or throw a punch in slow motion. However, this flexibility comes at a cost: stability. The shoulder relies heavily on soft tissues for support, particularly the rotator cuff.
The rotator cuff is a quartet of muscles—supraspinatus, infraspinatus, teres minor, and subscapularis—and their tendons, which wrap around the humeral head to keep it snug in the socket. These tendons pass through a tight space called the subacromial space, making them vulnerable to pinching or tearing when subjected to sudden forces. It’s like trying to thread a needle during an earthquake—not exactly a recipe for success.
When an MVA strikes, the rotator cuff can take a beating, leading to pain that feels like a personal vendetta from your own body. Understanding this anatomy sets the stage for why shoulder injuries are so common in car accidents.
References
Frank, C. B., Shrive, N. G., Lo, I. K. Y., & Hart, D. A. (2004). Form and function of tendon and ligament. In J. A. Buckwalter, T. A. Einhorn, & S. R. Simon (Eds.), Orthopaedic Basic Science: Biology and Biomechanics of the Musculoskeletal System (pp. 229-253). American Academy of Orthopaedic Surgeons.
Lo, I. K. Y., Thornton, G., Miniaci, A., Frank, C. B., Rattner, J. B., & Bray, R. C. (2003). Structure and function of diarthrodial joints. In J. B. McGinty (Ed.), Operative Arthroscopy (3rd ed., pp. 41-126). Lippincott Williams & Wilkins.
Mechanisms of Shoulder Injury in MVAs: A Crash Course in Chaos
Picture this: you’re cruising along, minding your own business, when another car decides to play bumper cars with your vehicle. The result? Your shoulder becomes the unwilling star of a physics experiment gone wrong. Let’s break down how MVAs wreak havoc on your shoulder, with a nod to the grim absurdity of it all.
Mechanism
Description
Impact on Shoulder
Impact and Force Transmission
Collisions transfer massive forces through the vehicle to your body, even with seatbelts and airbags.
Shoulders absorb shock, straining muscles and tendons.
Bracing for Impact
Instinctively gripping the steering wheel or dashboard positions shoulders awkwardly.
Rotator cuff tendons are stretched or torn under sudden force.
Whiplash Effect
Rapid back-and-forth head and neck movement is often associated with rear-end collisions.
Strains shoulder muscles and tendons, mimicking neck injury patterns.
Direct Trauma
Shoulder hitting the steering wheel, door, or dashboard during a crash.
Causes fractures, dislocations, or soft tissue damage.
Indirect Forces
Seatbelt pulling on the shoulder or body twisting during impact.
Leads to sprains, tears, or nerve injuries.
Imagine you’re in a rear-end collision. Your hands grip the steering wheel, shoulders tensed, as your body lurches forward and snaps back. The seatbelt digs into your shoulder, and the rotator cuff tendons scream in protest. It’s like your shoulder is caught in a medieval torture device, only with worse music playing in the background.
These mechanisms explain why shoulder injuries are so prevalent in MVAs. The sudden, forceful movements exploit the shoulder’s delicate balance of mobility and stability, often targeting the rotator cuff (Alexander Orthopaedics, 2023).
MVAs can leave your shoulder with a variety of injuries, each with its brand of discomfort. Here’s a rundown of the most common culprits, served with a side of dark humor to keep things grimly entertaining.
Injury Type
Description
Symptoms
Rotator Cuff Tears
Tears in the tendons stabilizing the shoulder, ranging from partial to full-thickness.
Severe pain, weakness, difficulty lifting arm, popping sounds.
Sprains and Strains
Damage to ligaments (sprains) or muscles/tendons (strains).
Damage to nerves supplying the arm, often from side-impact or rollover crashes.
Numbness, weakness, tingling, or paralysis in the arm.
Acromioclavicular (AC) Joint Injuries
Damage to the joint connecting the collarbone and shoulder blade.
Pain at the top of the shoulder, instability, swelling.
Rotator cuff tears are the grim celebrities of MVA injuries, often stealing the spotlight due to their frequency and impact. A 2008 study noted nearly 2 million Americans sought medical attention for rotator cuff issues, many linked to trauma like car accidents (El Paso Chiropractor Blog, 2016). Brachial plexus injuries, meanwhile, are the shadowy villains, causing nerve-related chaos that can leave your arm feeling like it’s auditioning for a zombie flick.
If your shoulder is staging a protest after an MVA, it’s likely sending you some clear signals. Recognizing these symptoms and getting a proper diagnosis is crucial unless you enjoy living in a world of perpetual discomfort.
Common symptoms include:
Pain: Sharp or aching, especially when moving the arm.
Weakness: Difficulty lifting objects or raising the arm.
Limited Range of Motion: Feeling like your shoulder is stuck in a straitjacket.
Swelling or Bruising: Visual cues that your shoulder is not happy.
Popping or Clicking: Sounds that make you wince with every movement.
Numbness or Tingling: Suggesting nerve involvement, like a brachial plexus injury.
Diagnosing these injuries requires a mix of clinical evaluation and advanced imaging. Healthcare providers may use:
X-rays: To detect fractures or dislocations.
MRI: For detailed views of soft tissues like rotator cuff tendons.
CT Scans: To assess complex bone injuries.
Ultrasound: Occasionally used for soft tissue evaluation.
Electromyography (EMG): To check nerve function in suspected brachial plexus injuries.
Dr. Alexander Jimenez, with his expertise in chiropractic care, utilizes advanced imaging and dual-scope procedures to assess the extent of shoulder injuries precisely. His approach ensures accurate diagnoses, which are critical for both treatment and legal documentation in personal injury cases (El Paso Back Clinic, n.d.).
Chiropractic Care After Accidents and Injuries- Video
Treatment Options: Mending the Broken Dance
Treating shoulder injuries from MVAs is like trying to fix a broken music box—delicate work that requires patience and precision. Treatment depends on the injury’s severity, but here are the main approaches:
Treatment
Description
Best For
Conservative Treatment
Rest, ice, compression, elevation (RICE), and over-the-counter pain relievers.
Mild sprains, strains, or minor tears.
Chiropractic Care
Adjustments and manipulations are made to realign the spine and shoulders, thereby reducing pain.
Exercises to restore strength, flexibility, and range of motion.
Most shoulder injuries, post-surgical recovery.
Medications
Prescription pain relievers or anti-inflammatories.
Moderate to severe pain and inflammation.
Injections
Corticosteroids to reduce inflammation.
Persistent pain not responding to conservative measures.
Surgery
Repairing large tears, stabilizing joints, or fixing fractures.
Severe rotator cuff tears, dislocations, fractures.
Dr. Jimenez’s multidisciplinary approach combines chiropractic care with functional medicine, addressing not just the injury but the whole person. His clinic offers tailored rehabilitation programs, including gentle therapies for post-surgical recovery, rooted in evidence-based practices (El Paso Back Clinic, n.d.). It’s like giving your shoulder a new script for a less tragic performance.
Importance of Early Treatment: Avoiding a Lifetime of Gloom
Ignoring shoulder pain after an MVA is like ignoring a creaking floorboard in a haunted house—it’s only going to get worse. Early treatment is critical for several reasons:
Preventing Chronic Pain: Untreated injuries can lead to persistent pain syndromes, turning your shoulder into a lifelong nemesis.
Avoiding Muscle Atrophy: Inactivity due to pain can weaken shoulder muscles, leading to increased instability.
Reducing Re-injury Risk: Proper rehabilitation strengthens the shoulder, making it less prone to future damage.
Supporting Legal Claims: Early documentation of injuries is vital for personal injury cases, ensuring fair compensation.
Dr. Jimenez emphasizes the importance of prompt evaluation, as delays can complicate recovery and impact legal outcomes. His clinic’s focus on early intervention helps patients avoid the grim fate of chronic pain (AICA Orthopedics College Park, 2022).
Personal Injury Cases in El Paso: Dr. Jimenez’s Expertise
El Paso, with its bustling border traffic, sees its fair share of MVAs, making personal injury cases a significant concern. Navigating these cases is like walking through a legal labyrinth, but Dr. Alexander Jimenez serves as a guiding light for victims.
With over 30 years of experience, Dr. Jimenez is a top-rated chiropractor in El Paso, recognized by Three Best Rated® from 2015 to 2024. His clinic specializes in treating complex injuries from MVAs, including shoulder pain, using a blend of chiropractic care, physical therapy, and functional medicine. What sets him apart is his ability to bridge the worlds of medicine and law.
Dr. Jimenez uses advanced imaging (like MRI and CT scans) and dual-scope procedures to provide detailed diagnoses, which are crucial for personal injury claims. His comprehensive medical reports serve as vital evidence, helping victims secure compensation for medical costs, lost wages, and pain and suffering. In El Paso’s unique legal landscape, his expertise is invaluable (El Paso Back Clinic, n.d.; LinkedIn, n.d.).
Shoulder pain and injuries from motor vehicle accidents are a serious matter, driven by the complex interplay of forces on the shoulder’s delicate structure. Rotator cuff tears, sprains, fractures, and nerve injuries can significantly impact your quality of life, but early diagnosis and treatment can make a world of difference. In El Paso, Dr. Alexander Jimenez stands out as a beacon of hope, offering expert care and legal support to MVA victims. His holistic approach and meticulous documentation ensure that patients not only recover but also receive the justice they deserve.
Disclaimer: This blog post is for informational purposes only and should not be taken as medical advice. Always consult a qualified healthcare professional for diagnosis and treatment of shoulder injuries.
Understand how chiropractic treatment MVA aids in healing and pain management post motor vehicle accident.
Chiropractic Care After Motor Vehicle Accidents: A Comprehensive Guide to Recovery
Introduction: The Unexpected Twist of a Car Crash
Picture this: you’re driving along, maybe humming to your favorite tune, when—bam!—a collision turns your day into a scene straight out of a grim fairy tale. Motor vehicle accidents (MVAs) are no laughing matter. Still, if Wednesday Addams were to narrate your post-crash saga, she’d probably say, “Congratulations, you’ve just auditioned for the role of ‘human piñata.’ Now, let’s fix that spine before it starts creaking like a haunted house.” In all seriousness, MVAs can leave you with injuries that linger like a bad plot twist, and chiropractic care might be the hero your body needs.
Each year, over 2 million people in the United States are injured in MVAs, with musculoskeletal injuries like whiplash, back pain, and fractures topping the list (StatPearls, 2023). These injuries can disrupt your life, turning simple tasks into painful ordeals. Chiropractic care offers a non-invasive, drug-free approach to recovery, focusing on realigning the body and relieving pain. In El Paso, Texas, Dr. Alexander Jimenez, a renowned chiropractor, has established a reputation for helping MVA victims recover and get back on their feet. This blog post dives into why chiropractic care is a smart choice after an MVA, how it addresses musculoskeletal pain, and why Dr. Jimenez is a go-to expert for personal injury cases in El Paso—all with a touch of dark humor to keep things lively.
Understanding Motor Vehicle Accidents and Their Impact
The Mechanics of Mayhem
When a car crash happens, your body becomes an unwilling participant in a physics experiment. The sudden acceleration or deceleration transfers energy through your muscles, bones, and joints, often in ways they weren’t designed to handle. This can lead to a range of musculoskeletal injuries, which affect the body’s movement system—think muscles, tendons, ligaments, nerves, and bones.
According to research, MVAs are a leading cause of spinal cord injuries, accounting for 38% of such cases between 2010 and 2013 (StatPearls, 2023). The mechanism of injury (MOI) varies depending on factors like crash direction, seatbelt use, and vehicle speed. For instance, a rear-end collision might whip your head back and forth, while a side-impact crash could twist your spine like a plot twist in a gothic novel.
Common Musculoskeletal Injuries
Here’s a rundown of the most frequent injuries from MVAs, each with its brand of misery:
Whiplash: The poster child of car crash injuries, whiplash occurs when your neck is jerked rapidly, straining muscles and ligaments. Symptoms include neck pain, stiffness, headaches, and sometimes dizziness or blurred vision.
Back Injuries: Sprains, strains, herniated discs, or even vertebral fractures can result from the force of impact, leading to chronic lower back pain or sciatica.
Shoulder Injuries: The shoulder can take a hit, especially if you brace yourself against the steering wheel, causing dislocations, rotator cuff tears, or fractures.
Extremity Injuries: Arms and legs can suffer sprains, fractures, or dislocations from being thrown against the car’s interior.
Soft Tissue Injuries: Muscles, tendons, and ligaments can stretch or tear, resulting in pain and reduced mobility.
These injuries can have long-term consequences, like reduced work capacity or diminished quality of life, especially if not treated promptly (PMC, 2021). It’s like your body’s saying, “I’d rather stay in bed than deal with this pain.” Chiropractic care steps in to rewrite that narrative, aiming to restore function and banish discomfort.
Injury Type
Description
Common Symptoms
Whiplash
Rapid neck movement causes muscle and ligament strain
Neck pain, stiffness, headaches, dizziness
Back Injuries
Sprains, strains, herniated discs, or fractures in the spine
Lower back pain, sciatica, limited mobility
Shoulder Injuries
Dislocations, rotator cuff tears, or fractures from impact
Shoulder pain, weakness, reduced range of motion
Extremity Injuries
Fractures, sprains, or dislocations in the arms or legs
Pain, swelling, difficulty moving
Soft Tissue Injuries
Tears or strains in muscles, tendons, or ligaments
Pain, swelling, bruising, stiffness
Chiropractic Care After Accidents and Injuries- Video
The Role of Chiropractic Care in Recovery
What Chiropractic Care Does
Chiropractic care is like a reset button for your musculoskeletal system. Chiropractors use hands-on techniques, primarily spinal adjustments, to correct misalignments, reduce inflammation, and promote healing and overall well-being. Unlike popping a painkiller, which might mask the problem, chiropractic care targets the root cause—whether it’s a misaligned vertebra or a strained muscle.
After an MVA, chiropractic care can offer several benefits, as outlined by Dr. Alexander Jimenez’s practice (Dr. Alex Jimenez, n.d.):
Restores Alignment: Adjustments realign the spine, reducing pressure on nerves and improving function.
Reduces Inflammation: Manual therapies decrease swelling around injured tissues, speeding up recovery.
Improves Mobility: Targeted exercises and stretches enhance flexibility and range of motion.
Manages Pain: Non-invasive techniques offer relief without the risks associated with long-term medication use.
Addresses Whiplash: Specialized adjustments target cervical spine issues, a common MVA injury.
Treats Associated Symptoms: Helps alleviate headaches, dizziness, numbness, and anxiety following an accident.
Imagine your spine as a creaky old staircase in a haunted mansion. Chiropractic care is like the handyman who tightens the loose boards, making it safe to climb again, without the ghostly groans.
Additional Therapies
Chiropractors often go beyond adjustments, incorporating therapies like:
Massage Therapy: Relaxes tight muscles and improves blood flow.
Cranial Sacral Therapy: A gentle technique to release tension in the head and spine, particularly effective for whiplash.
Heat or Cold Therapy: Reduces swelling or soothes muscle spasms at home.
Rehabilitation Exercises: Strengthens muscles and prevents re-injury.
These methods work together to create a comprehensive recovery plan, ensuring you’re not just patched up but fully restored.
Clinical Rationale for Chiropractic Care
Evidence-Based Guidelines
The clinical rationale for chiropractic care following a motor vehicle accident (MVA) is grounded in structured treatment protocols, such as the Croft Whiplash Treatment Guidelines. These guidelines categorize whiplash injuries by stage and severity, tailoring treatment to the patient’s needs. Based on an analysis of approximately 2,000 cases, they outline:
Injury Stages:
Stage I (Acute Inflammatory, 0-72 hours): Focus on rest, ice, and gentle mobilization to reduce swelling.
Stage II (Repair, 72 hours–14 weeks): Introduce spinal adjustments, physical therapy, and exercises.
Stage III (Remodeling, 14 weeks–12 months): Continue rehabilitation to ensure proper healing.
Stage IV (Chronic): Long-term management for persistent symptoms.
Severity Grades:
Grade I: Minimal symptoms, no ligament damage.
Grade II: Slight limitation of motion, no ligament injury.
Grade III: Moderate limitation, some ligament damage, neurological symptoms.
Grade IV: Severe limitation, ligament instability, possible fractures.
Grade V: Requires surgical intervention, with chiropractic care post-surgery.
Grade
Description
Treatment Frequency
Duration
Grade I
Minimal, no ligament injury
3x/week for 1 week, then 1x/month
Up to 10 weeks
Grade II
Slight limitation, no ligament injury
3x/week for 1 week, then 1x/month
Up to 4 months
Grade III
Moderate limitation, neurological symptoms
3x/week for 1-2 weeks, then 1x/month
Up to 6 months
Grade IV
Severe limitation, ligament instability
3x/week for 2-3 weeks, possible permanent care
Varies, often long-term
Grade V
Requires surgical stabilization
Post-surgical chiropractic care
Varies
These guidelines ensure treatments are evidence-based and progressive, minimizing the risk of chronic pain (Croft Guidelines, n.d.).
Why It Works
Chiropractic care aligns with the body’s natural healing processes. By correcting spinal misalignments, it reduces nerve irritation, which can cause pain and dysfunction. Studies suggest that early intervention can prevent acute injuries from becoming chronic, improving outcomes for MVA victims (PMC, 2018). It’s like catching a small crack in a window before it shatters completely.
Dr. Alexander Jimenez: El Paso’s Injury Specialist
A Multidisciplinary Approach
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a cornerstone of MVA recovery in El Paso. With over 30 years of experience, he’s earned the title of El Paso’s top injury specialist, recognized by Three Best Rated® from 2015 to 2024 (LinkedIn, n.d.). His clinic, Injury Medical Clinic, specializes in complex injuries like herniated discs, sciatica, and whiplash, using a blend of:
Chiropractic Adjustments: To realign the spine and relieve nerve pressure.
Functional Medicine: Addressing underlying health issues that affect recovery.
Spinal Decompression: Non-surgical treatment for disc injuries.
Acupuncture and Electro-Acupuncture: For pain relief and muscle relaxation.
Nutritional Counseling: To support overall healing.
Dr. Jimenez collaborates with orthopedic surgeons, neurologists, and physical therapists to ensure a holistic approach (El Paso Back Clinic, n.d.). His dual licensure as a chiropractor and nurse practitioner allows him to offer comprehensive care, from diagnostics to treatment.
Advanced Diagnostics
What sets Dr. Jimenez apart is his use of advanced imaging and diagnostic evaluations. He employs tools such as MRI and X-rays to pinpoint injuries, ensuring that treatments are precise. This is crucial for MVA patients, as accurate diagnosis can mean the difference between recovery and chronic pain. His clinic’s personalized care plans often include virtual or in-person health coaching, making recovery accessible and effective.
A Touch of Humor
If Dr. Jimenez were a character in the Addams Family, he’d be the one calmly stitching up Gomez’s latest sword-fighting mishap while offering sage advice on posture. His ability to navigate the chaos of injury recovery with precision and care is nothing short of magical, minus the cauldron, of course.
Personal Injury Cases in El Paso
The Importance of Documentation
In El Paso, personal injury cases from MVAs are common, and proper medical documentation is critical. Dr. Jimenez excels in this area, providing detailed reports that link injuries to the accident through advanced diagnostics. This documentation is invaluable in legal proceedings, helping victims secure compensation for medical costs, lost wages, and pain and suffering.
His role as a liaison between medical and legal services ensures that patients receive the care they need while their legal teams have the evidence required for a strong case. It’s like having a translator who speaks both “doctor” and “lawyer,” making sure nothing gets lost in translation.
Why El Paso Stands Out
El Paso’s busy roads and proximity to major highways make MVAs a significant concern. Dr. Jimenez’s expertise addresses this local need, offering specialized care for auto accident victims. His clinic’s focus on evidence-based, non-invasive treatments aligns with the needs of personal injury claimants, providing a path to recovery that’s both effective and legally sound.
Conclusion: A Serious Note on Recovery
Chiropractic care offers a beacon of hope for those navigating the aftermath of a motor vehicle accident. Addressing musculoskeletal injuries with precision and care can transform pain into progress, helping you reclaim your life. Dr. Alexander Jimenez’s expertise in El Paso exemplifies this, combining advanced diagnostics with compassionate care to guide patients through recovery and legal challenges.
However, recovery is a personal journey, and chiropractic care is just one piece of the puzzle. Always consult a qualified healthcare provider to create a personalized treatment plan tailored to your specific needs. Your body deserves the best care, not a one-size-fits-all fix.
Disclaimer: This blog post is for informational purposes only and does not constitute medical advice. Please consult with a qualified healthcare provider for diagnosis and treatment of any medical condition.
Learn how PTSD can arise from severe whiplash sustained in auto accidents. Discover healing approaches and recovery insights.
Understanding PTSD Associated with Severe Whiplash from Motor Vehicle Accidents
Introduction
Picture this: you’re driving along, maybe singing to your favorite tune, when bam!—a car rear-ends you. Your head snaps back and forth like it’s auditioning for a bobblehead commercial. That’s whiplash, and it’s no laughing matter. Whiplash is a neck injury caused by rapid head movement, often in motor vehicle accidents (MVAs), and it can lead to serious pain and long-term issues. But here’s the kicker: it’s not just your neck that might suffer. The trauma of the crash can also mess with your mind, potentially leading to Post-Traumatic Stress Disorder (PTSD).
PTSD is a mental health condition that can develop after a terrifying event, like a severe car accident. It brings symptoms like flashbacks, nightmares, and constant anxiety that make you feel like you’re reliving the crash. When whiplash is severe, the physical pain can team up with the emotional trauma, making recovery a tough road. This blog post dives into why severe whiplash and PTSD often go hand-in-hand, using research and insights from experts like Dr. Alexander Jimenez, a top chiropractor and nurse practitioner in El Paso, Texas. We’ll also explore why personal injury cases are important in El Paso and how Dr. Jimenez assists victims with advanced medical care and legal support. Buckle up (safely, of course) for a journey through the science, symptoms, and solutions for these conditions.
The Mechanism of Whiplash in Motor Vehicle Accidents
Whiplash is like your neck getting an unwanted rollercoaster ride. It happens when your head is suddenly forced forward and backward, or side to side, stretching the muscles, ligaments, and tendons in your neck beyond their normal range. In a typical rear-end collision, the car’s impact pushes your body forward, while your head lags, causing your neck to hyperextend. Then, as your body stops, your head whips forward, hyperflexing the neck. This rapid motion can damage the cervical spine (the upper part of the spine) and the surrounding soft tissues.
The forces involved are no joke. Even a low-speed crash at 7-8 mph can make your head move 18 inches at 7 G (that’s seven times the force of gravity) in less than a quarter of a second (Barnsley et al., 1994). These forces can cause capsular ligament laxity, where the ligaments that hold your neck bones together become stretched or torn, leading to cervical instability. This means your neck becomes wobbly, which can cause ongoing pain and other symptoms. The upper neck (C0-C2) might lead to dizziness or headaches, while the lower neck (C3-C7) can cause muscle spasms or numbness in your arms.
Muscle spasms, crepitation, paresthesia, and chronic neck pain
This physical damage sets the stage for both immediate and long-term problems, including the potential for psychological issues like PTSD.
Symptoms of Severe Whiplash
Severe whiplash can feel like your neck is staging a full-on rebellion. Symptoms often include:
Neck pain and stiffness: Your neck might feel like it’s made of concrete.
Headaches: Often starting at the base of your skull.
Dizziness or vertigo: Like the world’s spinning without you.
Blurred vision: Making it hard to focus.
Shoulder and back pain: Because your neck’s not suffering alone.
Numbness or tingling in arms: Like pins and needles that won’t quit.
Cognitive issues: Trouble concentrating or feeling foggy.
These symptoms might show up right after the crash or sneak up days later, which is why whiplash is sometimes called a “sneaky” injury (El Paso Back Clinic). In severe cases, symptoms can persist for months or years, rendering daily life a significant challenge. About 10% of whiplash victims end up with permanent disability, and the U.S. spends around $10 billion a year on whiplash-related costs, including medical bills and lost work (Brookdale Health).
Development of PTSD Following Motor Vehicle Accidents
PTSD is like your brain hitting the replay button on a scary movie you didn’t sign up for. It can develop after a traumatic event, and car accidents are a leading cause. Symptoms include:
Flashbacks or nightmares: Reliving the crash like it’s happening again.
Avoidance: Steering clear of driving or even talking about the accident.
Hypervigilance: Jumping at every honk or sudden noise.
Negative mood changes: Feeling hopeless or detached.
Sleep problems: Because your brain won’t let you rest.
MVAs are the top cause of PTSD in the general population, with studies showing up to 45% of survivors may develop it (Hickling & Blanchard, 2003). A study found that 27.5% of MVA patients had PTSD six months after a crash, and 24.3% still had it at 12 months (Mayou et al., 2002). Risk factors include severe injuries, a history of depression, or if the crash involved a fatality. The sudden, life-threatening nature of an accident can overwhelm your brain’s ability to cope, setting the stage for PTSD.
Correlation Between Severe Whiplash and PTSD
Here’s where things get tangled: severe whiplash and PTSD often team up to make recovery tougher. A study by Pedler and Sterling (2013) found that 25.7% of whiplash patients had PTSD, and it made their physical symptoms, like neck pain and disability, worse (Pedler & Sterling, 2013). Patients with both PTSD and sensory hypersensitivity (being extra sensitive to pain) had the worst outcomes. The study looked at 331 whiplash patients within three months of an MVA and found that PTSD alone was linked to more pain and disability, even without hypersensitivity.
Why does this happen? Chronic pain from whiplash can make you feel stressed or anxious, which feeds into PTSD. Meanwhile, PTSD can make you more aware of pain, creating a vicious cycle. The trauma of the crash itself—say, the screech of tires or the crunch of metal—can also trigger PTSD, especially if you’re already dealing with physical pain. Shared symptoms, like dizziness or cognitive issues, can blur the line between whiplash and PTSD, making diagnosis tricky.
Understanding Long-Lasting Injuries- Video
Clinical Insights from Dr. Alexander Jimenez
Dr. Alexander Jimenez is like the superhero of injury recovery in El Paso, Texas. With over 25 years as a chiropractor and nurse practitioner, he’s a go-to expert for whiplash and MVA injuries (El Paso Back Clinic). While specific studies on PTSD and whiplash from Dr. Jimenez aren’t widely published, his approach is all about treating the whole person, body, and mind.
Dr. Jimenez utilizes advanced tools, such as MRI and CT scans, to identify injuries that standard X-rays may miss, including soft tissue damage and cervical instability. He also employs functional imaging, such as digital motion X-ray (DMX), to see how your neck moves in real-time. His treatments include:
Chiropractic adjustments: To fix spinal misalignments and ease nerve pressure.
Spinal decompression: A non-surgical way to relieve disc pressure.
Functional medicine: Addressing diet and lifestyle to boost healing.
Dr. Jimenez’s holistic approach likely helps patients with both whiplash and PTSD by reducing physical pain, which can ease emotional stress. He also acts as a bridge between medical care and legal needs, providing detailed reports for personal injury cases.
Importance of Personal Injury Cases in El Paso
El Paso sees its fair share of car accidents, and personal injury cases are a big deal. With over 5.2 million MVAs in the U.S. each year, causing 2.2 million injuries, the need for expert care and legal support is huge (NHTSA, 2022). Dr. Jimenez excels in this area, providing medical evaluations that effectively link injuries to accidents, which is crucial for insurance claims or lawsuits.
His ability to use advanced imaging and diagnostics, like fMRI or DMX, helps prove the extent of injuries, especially when symptoms like pain or PTSD aren’t visible on standard tests. This makes him a key player in helping victims get fair compensation and the care they need. His dual role as a chiropractor and nurse practitioner enables him to provide both hands-on treatment and medical documentation, making the legal process smoother.
Role of Advanced Imaging and Diagnostic Evaluations
Diagnosing whiplash is like trying to find a needle in a haystack—standard X-rays often come back normal, even when you’re in pain. That’s where advanced imaging comes in. Tools like:
Functional MRI (fMRI): This technique enables the visualization of brain activity and soft tissue damage.
Digital Motion X-ray (DMX): Captures neck movement to spot instability.
Functional CT (fCT): Provides detailed images of bones and joints.
These can reveal issues, such as ligament tears or cervical instability, that regular X-rays may miss. For example, one study found that only 1 in 10 ligament disruptions showed up on standard X-rays (Barnsley et al., 1994). By pinpointing the injury, doctors like Dr. Jimenez can create targeted treatment plans, which might include chiropractic care, physical therapy, or even psychological support for PTSD.
Treatment Approaches for Whiplash and PTSD
Treating whiplash and PTSD is like tackling a two-headed monster—you need to hit both physical and mental symptoms. For whiplash, treatments include:
Chiropractic care: Adjustments to restore neck mobility (Jimenez, LinkedIn).
Pain management: Use heat, ice, or medications such as ibuprofen.
Electro-acupuncture: To reduce pain and inflammation.
For PTSD, options include:
Cognitive-Behavioral Therapy (CBT): Helps change negative thoughts about the trauma.
Eye Movement Desensitization and Reprocessing (EMDR): Reduces the intensity of traumatic memories.
Medications: Antidepressants or anti-anxiety drugs to manage symptoms.
Combining these is key. For example, easing whiplash pain with chiropractic care can make PTSD therapy more effective by reducing stress. Dr. Jimenez’s integrated approach, blending chiropractic and functional medicine, is a great example of this dual focus.
Statistics on Whiplash and PTSD from Motor Vehicle Accidents
The numbers tell a sobering story. Whiplash affects over 3 million Americans yearly, with about 1.2 million cases from MVAs alone (Brookdale Health). Around 10% of these lead to permanent disability, costing the U.S. $10 billion annually. Rear-end collisions are the primary cause, accounting for a significant portion of the 5.2 million U.S. crashes each year (NHTSA, 2022).
PTSD is just as common. Up to 45% of MVA survivors may develop PTSD, with 27.5% showing symptoms six months post-crash (Mayou et al., 2002). In severe crashes, the risk is higher, especially for women or those with prior mental health issues. These stats highlight why early treatment is critical.
Condition
Prevalence in MVA Survivors
Key Risk Factors
Whiplash
Over 3 million annually
Rear-end collisions, low-speed impacts
PTSD
Up to 45%
Severe injuries, prior depression, and crash fatalities
Conclusion
Severe whiplash from car accidents can do more than just hurt your neck—it can team up with PTSD to make life tough. The pain from whiplash can feed into anxiety and trauma, while PTSD can make physical symptoms feel worse. Understanding this link is crucial for helping people recover. In El Paso, Dr. Alexander Jimenez is a standout, using advanced imaging and a whole-person approach to treat whiplash and support personal injury cases. His work shows how combining physical and psychological care can make a big difference.
If you’ve been in a crash, don’t brush off your symptoms—whether it’s neck pain or nightmares, help is out there. Seek a healthcare provider to get the right diagnosis and treatment. Recovery might feel like climbing a mountain, but with the right support, you can get to the top.
Disclaimer: This blog post is for informational purposes only and is not medical advice. If you have whiplash or PTSD, consult a qualified healthcare professional for proper diagnosis and treatment.
Get informed about the effects of auto accidents, such as whiplash and Achilles tendinosis, and their implications for recovery.
Introduction
Imagine you’re driving along, singing to your favorite tune, when—bam!—another car rear-ends you. Your head snaps back and forth like a bobblehead on a bumpy road. That’s whiplash, folks, and it’s no laughing matter, despite the cartoonish image. Whiplash is a neck injury caused by sudden, forceful head movement, most often from motor vehicle accidents (MVAs). It affects the muscles, ligaments, and tendons in the neck, leading to pain that can range from a mild nuisance to a life-altering ordeal.
In this in-depth guide, we’ll explore whiplash from every angle: what it is, how it occurs, its symptoms, and the most effective ways to treat it. We’ll delve into why ligament injuries are a significant concern and how they contribute to chronic pain. Plus, we’ll spotlight Dr. Alexander Jimenez, a top chiropractor in El Paso, Texas, whose expertise helps accident victims recover and navigate personal injury claims. With a touch of humor to keep things light, we’ll also delve into the serious legal aspects, illustrating how the medical and legal worlds intersect to support victims. Buckle up—it’s going to be an informative ride!
Whiplash is like your neck’s version of a bad rollercoaster ride. It occurs when your head is jerked backward and then forward (or vice versa) with enough force to strain or tear the neck’s soft tissues. This rapid motion, often referred to as a cervical acceleration-deceleration injury, is most commonly triggered by rear-end car collisions. Picture this: your car gets hit from behind, your body lurches forward, but your head lags for a split second before snapping back. Ouch!
Mechanism of Injury
The physics of whiplash is brutal. In a rear-end crash, the sudden force pushes your torso forward, while your head remains momentarily still, causing hyperextension (overstretching backward). Then, as your body stops, your head whips forward into hyperflexion. This S-shaped motion of the cervical spine exceeds its normal limits, causing damage to tissues (Whiplash Associated Disorders). Other causes include sports injuries, falls, or even a particularly wild amusement park ride.
Anatomy of the Neck
Your neck, or cervical spine, is a marvel of engineering. It’s made of seven vertebrae (C1-C7) that support your head’s weight and allow you to nod, shake, and tilt like a pro. Between these vertebrae are intervertebral discs, acting like tiny shock absorbers. Ligaments, such as the anterior longitudinal ligament (ALL) and the posterior longitudinal ligament (PLL), maintain stability. Muscles and tendons provide movement and support. Whiplash disrupts this delicate balance, often targeting ligaments and muscles.
Types of Injuries
Whiplash can cause a variety of injuries, including:
Muscle Strains: Overstretched or torn muscle fibers, leading to soreness.
Ligament Sprains: Stretched or torn ligaments, especially the ALL, causing instability.
Tendon Injuries: Damage to tendons connecting muscles to bones.
Disc Herniation: Protruding discs that press on nerves.
Nerve Damage: Irritation or compression causing numbness or weakness.
Fractures: Rare, but possible in severe cases.
These injuries explain why whiplash can be so painful and persistent if not treated properly (Whiplash Injury).
Whiplash symptoms are like uninvited guests—they might not show up right away, but can linger for an extended period. Some people feel fine after a crash, only to wake up the next day with a neck that feels like it’s been through a wrestling match.
Common Symptoms
Here’s what you might experience:
Neck Pain and Stiffness: The hallmark of whiplash, often worse with movement.
Headaches: Starting at the skull’s base, sometimes spreading forward.
Shoulder and Upper Back Pain: From muscle tension or referred pain.
Dizziness: Feeling woozy or like the room is spinning.
Fatigue: A general sense of being wiped out.
Cognitive Issues: Trouble focusing, memory lapses, or irritability.
Sensory Disturbances: Numbness or tingling in arms or hands.
Visual Problems: Blurred vision or light sensitivity.
Sleep Issues: Pain is making it hard to get a good night’s sleep.
Symptoms can vary in intensity and may take hours or days to appear (Whiplash Symptoms).
Diagnosis
Diagnosing whiplash is like solving a puzzle. Doctors start with:
Patient History: They’ll ask about the accident, when symptoms began, and any past neck issues.
Physical Exam: Checking neck movement, tenderness, and neurological signs like reflexes and strength.
Imaging Tests:
X-rays: To spot fractures or dislocations.
MRI: For soft tissue damage like ligament tears.
CT Scans: Detailed bone images.
Soft tissue injuries often don’t show on X-rays, so normal results don’t rule out whiplash. Early diagnosis is key to preventing chronic pain (Whiplash Diagnosis).
Importance of Early Diagnosis
Think of whiplash like a leaky faucet—ignore it, and you’ll have a bigger mess later. Prompt diagnosis enables timely treatment, thereby reducing the risk of long-term complications.
Treating whiplash is similar to fixing a car after a fender bender—you need the right tools and a skilled mechanic. The goal is to reduce pain, restore function, and prevent chronic issues. Research suggests active treatments work best, and Dr. Alexander Jimenez in El Paso is a master at this.
Standard Treatment Approaches
Pain Management:
Medications: Over-the-counter options like ibuprofen or acetaminophen. Severe cases may require muscle relaxants or stronger pain medications.
Ice and Heat: Apply ice for the first 48 hours to reduce swelling, then use heat to relax muscles (Whiplash Treatments).
Physical Therapy:
Exercises: To boost the range of motion and strengthen neck muscles.
Manual Therapy: Massage or mobilization to ease pain.
Rest and Activity Modification:
Short-Term Rest: Avoid activities that may aggravate the condition initially.
Gradual Activity: Returning to normal tasks to prevent stiffness.
Education: Understanding the injury and recovery process empowers patients.
The Root Causes of Pain- Video
Dr. Jimenez’s Approach
Dr. Jimenez is like the Tony Stark of chiropractic care, utilizing cutting-edge techniques to help patients recover quickly. His clinic offers:
Chiropractic Adjustments: Realigning the spine to reduce pain.
Soft Tissue Therapies: Myofascial release or trigger point therapy for muscle tension.
Massage Therapy: To improve circulation and relaxation.
Exercise Rehabilitation: Tailored programs to strengthen and stabilize the neck (Chiropractic Care).
He’s also vocal about ditching cervical collars, which can weaken muscles and slow recovery. A study he cites found better outcomes with active treatments over collars (Cervical Collars).
Evidence-Based Insights
The Croft Whiplash Treatment Guidelines outline treatment duration based on injury severity:
Interestingly, whiplash shares similarities with Achilles tendonosis, such as abnormal blood vessel growth, suggesting that some treatments may overlap (Tendonosis Similarities).
Ligaments are the unsung heroes of your neck, keeping your spine stable like the ropes on a suspension bridge. When whiplash strikes, these ligaments, especially the anterior longitudinal ligament (ALL), can sustain significant damage, leading to serious consequences.
Why Ligament Injuries Are Critical
The ALL runs along the front of your spine, preventing excessive backward bending. Whiplash’s hyperextension phase can cause stretching or tearing, leading to instability. This can lead to:
Chronic Pain: From abnormal spine movement.
Increased Injury Risk: A wobbly spine is prone to further damage.
Degeneration: Over time, instability may cause arthritis or disc issues (Ligament Injuries).
Ligament injuries can be challenging because they often don’t show up on X-rays, requiring MRI or specialized imaging techniques like digital motion X-ray (DMX) (DMX Study).
Research Insights
Studies confirm ligament damage is common in whiplash. One found that ALL can stretch to 56% of its failure point at just eight mph collisions (ALL Study). The Croft Guidelines note that Grade III and IV whiplash involve ligamentous injury, requiring longer treatment (Croft Guidelines).
Dr. Jimenez’s Expertise
Dr. Jimenez utilizes advanced imaging techniques to detect ligament damage, ensuring an accurate diagnosis. His treatments focus on stabilizing the spine through chiropractic care and exercises, addressing the root cause of pain (El Paso Back Clinic).
Getting whiplash from a car accident is bad enough, but then comes the paperwork jungle of personal injury claims. In El Paso, where MVAs are all too common, experts like Dr. Jimenez bridge the gap between medical care and legal justice.
Understanding Personal Injury Law
Personal injury law helps victims harmed by someone else’s negligence—like a distracted driver—get compensation for medical bills, lost wages, and pain. Whiplash cases often involve claims against the at-fault driver’s insurance or lawsuits if settlements fail (Medical Experts).
The Role of Medical Documentation
Medical records are the backbone of a personal injury case. They prove:
The injury’s nature and extent.
The link to the accident.
The treatment and costs involved.
Without solid documentation, claims can falter (Doctors’ Role).
Dr. Jimenez’s Contribution
Dr. Jimenez is like a superhero with a stethoscope and a law library. He:
Provides Detailed Reports: Using MRI and diagnostic tools to document injuries.
Offers Expert Testimony: Explaining medical details to judges and juries.
Acts as a Liaison: Ensuring medical records reach lawyers and insurers accurately (El Paso Back Clinic).
His work strengthens cases by providing clear evidence of the impact of whiplash.
Importance in El Paso
El Paso’s busy roads see frequent accidents, making skilled practitioners like Dr. Jimenez vital. His reputation as a top chiropractor, recognized by awards from 2015 to 2024, makes him a trusted ally for victims (LinkedIn Profile).
While patient privacy prevents sharing specific cases, Dr. Jimenez has helped countless whiplash victims recover. Imagine a teacher rear-ended at a stoplight, suffering Grade II whiplash. After weeks of chiropractic adjustments, massage, and exercises at his clinic, she’s back in the classroom, pain-free. Such outcomes highlight the power of active treatment and expert care.
Conclusion
Whiplash is more than a sore neck—it’s a complex injury that can disrupt lives if ignored. Ligament injuries, such as those to the anterior longitudinal ligament, are a key reason why prompt, active treatment is crucial. Dr. Alexander Jimenez’s expertise in El Paso, combining advanced diagnostics with chiropractic care, offers hope for recovery and legal support for personal injury claims.
If you’ve been in an MVA, don’t wait for symptoms to worsen. Seek medical care immediately to protect your health and strengthen any potential legal case. The road to recovery starts with the right help.
Disclaimer: This guide is for informational purposes only and is not a substitute for professional medical advice. Always consult a qualified healthcare provider for diagnosis and treatment.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine