In many working individuals with back pain, how does non-surgical decompression achieve pain reduction to the intervertebral disc in pain management?
Introduction
Low back pain is a common complaint in the workforce. It can cause individuals to miss work, become disabled, and frequently visit their primary doctors. Many factors contribute to the development of low back pain. You may have experienced constant back muscle aches from sitting down and hunched over a computer. Or maybe you have felt your back muscles strain from carrying heavy objects from one location to another. Carrying equipment around your hips, like a utility belt in construction or a law enforcement job, can also contribute to back pain. These scenarios can all be related to the development of low back pain. When the lower extremity muscles are over or under-active, it can cause muscle and tissue fibers to shorten or become overstretched. This can lead to tiny nodules known as trigger points forming. Additionally, repetitive motions caused by overload axial pressure can compress the lumbar spinal structure and cause the spinal disc to care constantly. However, there are ways to manage low back pain. By focusing on common issues associated with each back pain syndrome, non-surgical treatments like spinal decompression can achieve pain management for the intervertebral disc. As we work with certified medical providers who use our patients’ information to treat working individuals suffering from low back pain combining non-surgical decompression as part of their routine can alleviate the pain-like symptoms. We inform them about non-surgical treatments to ease low back pain issues while achieving pain management. We encourage our patients to ask essential questions while seeking education from our associated medical providers about their situation. Dr. Alex Jimenez, D.C., provides this information as an educational service. Disclaimer
Each Low Back Pain Syndrome Is Common
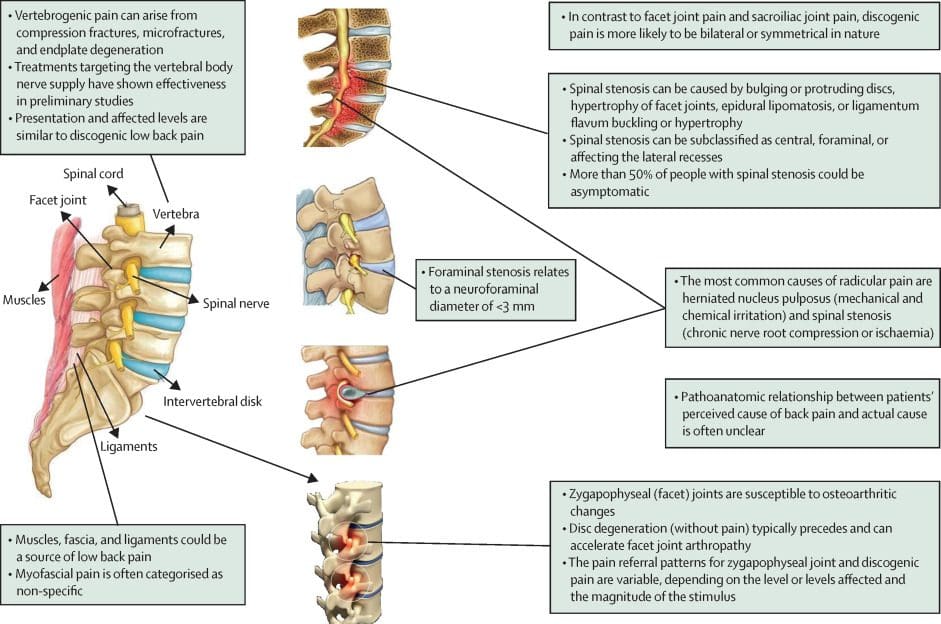
When it comes to low back pain, many individuals will come to their primary doctor and inform them that they are in constant pain in their lower back. As stated earlier, repetitive motions from normal factors can cause the back muscles to be over or under-stretched, causing muscle aches. At the same time, the spinal discs are constantly being compressed with unnecessary pressure. When the spinal discs are under constant pressure, they can begin to bulge or herniate, depending on the severity of the issue. To that point, the compressed spinal discs can aggravate the spinal nerve roots to cause referred localized pain down to the legs or arms, causing symptoms of numbness or tingling sensations in the hands and feet. Low back pain has four categories that can affect many individuals and has different treatment pathways. (Bogduk & Twomey, 1991) These four categories can vary with intense symptoms that pertain to the pain and how they were developed. These include:
Acute muscularity (can involve sciatic radiation)
With or without neurological dysfunction
Chronic muscularity (can have recurring symptoms)
Neoplastic low back pain (can have frequent symptoms and become progressive)
These four categories of low back pain all have common features, as well as regional pain, muscle impairment, mechanical dysfunction exacerbated by daily activities, and mood/behavioral changes. Additional low back pain can be specific or non-specific, associated with many working individuals. Many individuals dealing with low back pain will often work through the pain rather than find the proper relief because of that fear of missing out on work. (Becker & Childress, 2019) Luckily, many ways exist to reduce low back pain and alleviate compressed spinal discs.
Revolutionizing Healthcare-Video
Have you or your loved ones felt aches and pains in your lower back after regular activities? Do your legs and lower back feel stiffer than usual when walking with heavy equipment? Or do you hunch or slouch constantly while relaxing on a chair or sofa? Many of these factors are the root cause of low back pain, and it can affect a person’s routine without treatment right away. When many individuals deal with low back pain in the workforce, they often try home remedies to alleviate the pain temporarily to get back to work, only to cause more issues in the future. To that point, this causes the working individual to be under constant pain and miss out on work, which then causes more unnecessary stress and pressure on the lower back. Luckily there are available treatments that can reduce the effects of low back pain and ease the minds of many individuals looking for cost-effective and safe options. Non-surgical treatments for low back pain are safe for the spine and can be cost-effective to help manage the pain associated with compressed spinal discs and allow people to be more mindful of their back and spine. Non-surgical treatments can range from chiropractic care to spinal decompression, depending on the severity of the pain that the person is experiencing. The video above goes more in-depth with how non-surgical treatments can revolutionize healthcare.
The Biomechanic Principal Of Decompression
When it comes to individuals trying to find relief for their low back pain, many will opt for traditional surgical treatments if the home treatments are not working. While conventional surgical treatments can provide more rapid relief, they can be pricey and cause a financial burden to the working individual. Hence why many will often seek out non-surgical therapies. (Schoenfeld & Weiner, 2010) Non-surgical treatments are affordable to the active individual and can be customizable depending on the issue. One of the non-surgical treatments is decompression. Decompression incorporates mechanical traction to gently stretch the spine as a distracting force to realign the spine back to normal, increase the body’s fluids and nutrients to promote healing factors, and relieve abnormal pressure on the nociceptive receptors system. (Judovich, 1954) The effects of spinal decompression allow the spine to regain mobility, stability, and reduction of low back pain, allowing the compressed spinal disc to return to its original position.
The Decompression Benefits For Common Occurring Back Pain Syndrome
During the mechanical traction process of spinal decompression, the spinal disc space is slightly increased, which reduces the lumbar disc protrusion and causes the disc herniation to disappear over time after a few sessions. (Andersson, Schultz, & Nachemson, 1983) These are a few benefits of spinal decompression, as traction therapy can also alleviate additional musculoskeletal disorders associated with low back pain. (Bettmann, 1957) Musculoskeletal disorders associated with low back pain can be treated with spinal manipulation combined with decompression, as it is used to improve spinal and hip mobility in the lower extremities, thus reducing pain and incapacity in people with low back pain. (Fagundes Loss et al., 2020) Additionally, mechanical traction from decompression can help inhibit positive results for many individuals looking for relief from mechanical stress from their backs. (Wegner et al., 2013) Spinal decompression can help reduce low back pain and its associated symptoms for many working individuals who want the relief they deserve.
References
Andersson, G. B., Schultz, A. B., & Nachemson, A. L. (1983). Intervertebral disc pressures during traction. Scand J Rehabil Med Suppl, 9, 88-91. https://www.ncbi.nlm.nih.gov/pubmed/6585945
Becker, B. A., & Childress, M. A. (2019). Nonspecific Low Back Pain and Return To Work. American Family Physician, 100(11), 697-703. https://www.ncbi.nlm.nih.gov/pubmed/31790184
Fagundes Loss, J., de Souza da Silva, L., Ferreira Miranda, I., Groisman, S., Santiago Wagner Neto, E., Souza, C., & Tarrago Candotti, C. (2020). Immediate effects of a lumbar spine manipulation on pain sensitivity and postural control in individuals with nonspecific low back pain: a randomized controlled trial. Chiropr Man Therap, 28(1), 25. https://doi.org/10.1186/s12998-020-00316-7
Schoenfeld, A. J., & Weiner, B. K. (2010). Treatment of lumbar disc herniation: Evidence-based practice. International Journal of General Medicine, 3, 209-214. https://doi.org/10.2147/ijgm.s12270
Wegner, I., Widyahening, I. S., van Tulder, M. W., Blomberg, S. E., de Vet, H. C., Bronfort, G., Bouter, L. M., & van der Heijden, G. J. (2013). Traction for low-back pain with or without sciatica. Cochrane Database Syst Rev, 2013(8), CD003010. https://doi.org/10.1002/14651858.CD003010.pub5
In many inviduals with low back pain, how does spinal decompression and inversion therapy reduce nerve entrapment?
Introduction
Low back pain is a common problem worldwide that can cause individuals to miss out on important aspects of their lives, including work. The severity of the pain can be specific or non-specific, and it can be localized in one area or spread throughout the body, causing referred pain. Many normal and traumatic factors can contribute to low back pain, such as improper lifting, excessive weight gain, stress, excessive sitting, or repetitive motions. These factors can compress the spinal discs and cause the surrounding muscles to become over-stretched and tight, leading to nerve entrapment. However, various treatments are available to reduce low back pain and restore functionality to the body. This article focuses on two therapies, inversion therapy, and spinal decompression, and how they can be used together to reduce the likelihood of low back pain returning. By working with certified medical providers who use our patients’ information to treat individuals suffering from low back pain while combining inversion therapy and spinal decompression as part of their routine. We inform them about non-surgical treatments to regain spinal mobility and restore muscle strength to the back muscles while preventing the effects of low back pain from reoccurring. We encourage our patients to ask essential questions while seeking education from our associated medical providers about their situation. Dr. Alex Jimenez, D.C., provides this information as an educational service. Disclaimer
How Does Inversion Therapy Reduce Back Pain
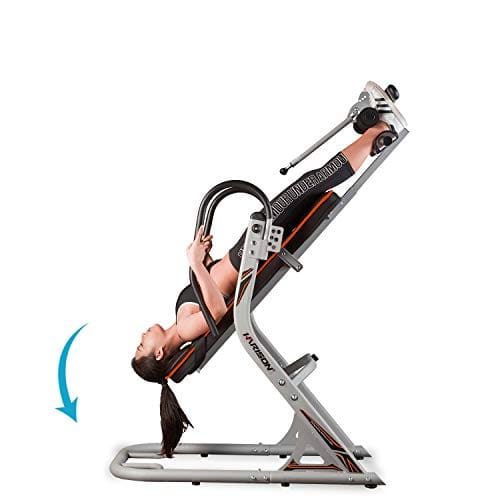
Do you suffer from muscle aches and strains in your lower back due to sitting for extended periods? Do you experience pain after carrying heavy objects or from being physically inactive? If these symptoms are associated with low back pain, seeking treatment is common. Many take over-the-counter medicines, hot/cold packs, or home remedies for temporary relief. Inversion therapy is another treatment option. In “The Ultimate Spinal Decompression” by Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., inversion therapy is mentioned as a method where the individual is suspended upside down in an inversion table for a few minutes to relieve pain-like symptoms. Inversion therapy can reverse the effects of gravity on the back, which can compress the spine and spinal disc over time, leading to back pain. Inversion therapy can relieve acute back pain by decompressing the back.
Using inversion therapy can help alleviate the symptoms of low back pain and reduce the need for surgery among many individuals. This practice, which has been used for thousands of years, involves utilizing gravity to provide traction for those experiencing lumbar disc herniation related to low back pain. By opting for non-surgical treatments, such as inversion therapy, individuals suffering from low back pain caused by various factors, including nerve entrapment, can experience relief. (Mendelow et al., 2021)
Back Pain & Nerve Entrapment Reduced
It is possible to experience low back pain with or without additional symptoms caused by factors affecting the back. This type of pain can result in mobility issues in the spinal region, pain that radiates into the lower extremities, and general discomfort associated with musculoskeletal conditions. (Delitto et al., 2012) Nerve entrapment can be a factor related to low back pain, and it can impact the peripheral pathway because signals from the peripheral system can cause irregular transmissions to the brain. This can lead to inflammatory cytokines releasing in the affected muscle and radiating shooting pain to the legs. As a result, the body can mimic leg pain correlated with low back pain, leading to a misdiagnosis of the issue. (Saal et al., 1988) Fortunately, various non-surgical treatments, such as inversion therapy and spinal decompression, can help reduce low back pain and its associated symptoms.
Enhance Your Lifestyle-Video
If you’re suffering from low back pain, non-surgical treatments can be a cost-effective, gentle, and safe solution. Innovative techniques are used to target the root cause of the pain and alleviate it from the musculoskeletal system. Inversion therapy, spinal decompression, and chiropractic care are some non-surgical treatments that can help relieve low back pain and prevent it from recurring. These therapies involve physical and mechanical manipulation of the spine to correct any subluxations. Misalignment of the body can cause low back pain and negatively impact one’s quality of life. Incorporating non-surgical treatments into your routine can help your body heal naturally and promote a healthy lifestyle. For more information on the benefits of these treatments, check out the video above.
How Spinal Decompression & Inversion Therapy Reduce Back Pain
As one of the forms of non-surgical treatment, spinal decompression is safer and more cost effective than traditional surgical treatments. Non-surgical treatments can be combined with other therapies to help improve and control the movement in the lumbar spine. (Zaina et al., 2016) So when spinal decompression is combined with inversion therapy, it can help decompress the spine, allowing the spinal discs to slip back into their original position and reduce the pressure off the aggravated and irritated nerve root from causing low back pain to occur again. Since inversion therapy is used for acute low back pain, spinal decompression therapy is used for individuals with chronic issues. After a few sessions of these treatments, the body will function normally and allow the back to be mobile again. When people start to think about their health and wellness for back pain issues, they can incorporate non-surgical treatments as part of their routine.
References
Delitto, A., George, S. Z., Van Dillen, L., Whitman, J. M., Sowa, G., Shekelle, P., Denninger, T. R., Godges, J. J., & Orthopaedic Section of the American Physical Therapy, A. (2012). Low back pain. J Orthop Sports Phys Ther, 42(4), A1-57. https://doi.org/10.2519/jospt.2012.42.4.A1
Kaplan, E., & Bard, P. (2023). The Ultimate Spinal Decompression. JETLAUNCH.
Mendelow, A. D., Gregson, B. A., Mitchell, P., Schofield, I., Prasad, M., Wynne-Jones, G., Kamat, A., Patterson, M., Rowell, L., & Hargreaves, G. (2021). Lumbar disc disease: the effect of inversion on clinical symptoms and a comparison of the rate of surgery after inversion therapy with the rate of surgery in neurosurgery controls. Journal of Physical Therapy Science, 33(11), 801-808. https://doi.org/10.1589/jpts.33.801
Saal, J. A., Dillingham, M. F., Gamburd, R. S., & Fanton, G. S. (1988). The pseudoradicular syndrome. Lower extremity peripheral nerve entrapment masquerading as lumbar radiculopathy. Spine (Phila Pa 1976), 13(8), 926-930. https://www.ncbi.nlm.nih.gov/pubmed/2847334
Zaina, F., Tomkins-Lane, C., Carragee, E., & Negrini, S. (2016). Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst Rev, 2016(1), CD010264. https://doi.org/10.1002/14651858.CD010264.pub2
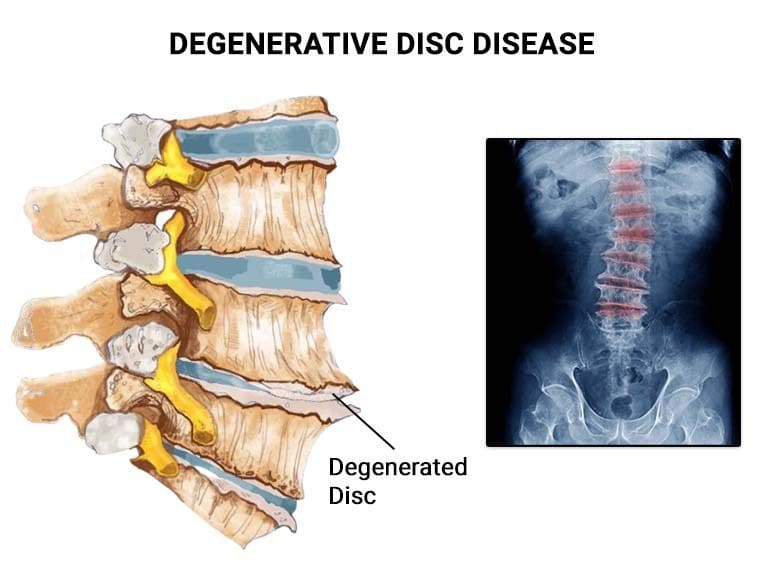
Many individuals are unaware of their pain until they perform specific movements that cause discomfort. This is due to the heavy weight that causes the body to carry an axial overload, compressing the spinal disc, which can lead to herniation or degeneration over time if not treated promptly. Compressed spinal discs can cause chronic conditions such as low back pain, spinal stenosis, or intervertebral disc disease (IDD). Several factors contribute to the development of IDD, including chronic conditions that can lead to compressed spinal discs. This condition can be relieved over time through therapy treatments that can reduce the pain effects of IDD and help individuals be more mindful of their spine. This article will discuss IDD therapy’s role in relieving spine pain, treatment protocols, and how it is combined with spinal decompression, a non-surgical therapy. We work with certified medical providers who use our patients’ valuable information to treat individuals suffering from back and spinal disc degeneration while informing them about non-surgical treatments like IDD(intervertebral disc degeneration) therapy and spinal decompression that can help relieve their pain and help rehydrate their spinal disc. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
What Is IDD Therapy?
The spine comprises muscles, tendons, ligaments, discs, and bones extending from the skull’s base to the bottom of the sacrum. Its primary function is to keep the body upright and protect the spinal cord from injuries. According to research studies, the spinal discs act as shock absorbers during movement and can become damaged over time, causing pain-like symptoms and chronic conditions. IDD therapy is a common treatment for reducing pain caused by degenerative discs.
Research suggests that intervertebral disc degeneration can cause symptoms related to musculoskeletal disorders such as low back pain, disc herniation, and spinal stenosis. Conservative and non-invasive treatments can reduce the pain-like symptoms and effects caused by IDD. IDD therapy allows the spine to be re-toned, restructured and re-educated. Like spinal decompression, IDD therapy uses gentle traction pulling to rehydrate the discs and reduce the pressure on the nerve roots, as stated by research studies. IDD therapy helps restore muscle strength, increase the spine’s range of motion, and promote the body’s natural healing process to reduce spinal pain associated with environmental factors.
Home Exercise For Pain Relief- Video
Do you experience difficulty doing activities due to back pain? Do you feel stiffness or instability in your lower back? These may be symptoms of intervertebral degenerative disease caused by repetitive motions. IDD can cause chronic musculoskeletal disorders and disability. However, available non-surgical treatments like IDD therapy, which uses negative pressure to rehydrate the spinal disc, can reduce pain. Other non-surgical therapies like chiropractic care and physical therapy can help restore mobility and strengthen back muscles. Check out the video above for home exercise routines that relieve pain.
IDD Treatment Protocols
Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., wrote “The Ultimate Spinal Decompression,” explaining how chiropractors and massage therapists use personalized IDD therapy plans to treat musculoskeletal pain associated with intervertebral degenerative disease. IDD therapy involves strapping the individual to a traction machine and utilizing specific protocols for treatment.
The Treatment Schedule
The first step in IDD therapy is examining the individual’s range of motion, muscle strength, nerve conduction, and SSEP tests. This allows the doctor to document the pain’s location and develop a personalized treatment plan, including the indicated problem, treatment frequency, duration, etc. Afterward, the individual will receive other treatments before the IDD traction therapy machine.
Therapeutic Ultrasound
Electro-stimulation
Interferential Stimulation
Hydrocolator
This machine gently pulls the spine to create negative space between the spinal column, allowing nutrients to rehydrate the disc and begin healing. The process lasts 20-30 minutes and may cause mild soreness, but progress is seen after a few sessions.
Pre-& Post-Session Physical Therapy
The benefit of combining IDD therapy with physical therapy is that stretching techniques can loosen the surrounding muscles before spinal mobilization, allowing the soft tissues to accept the treatment. After treatment, cryo-therapeutic therapy or an ice pack can alleviate soreness and inflammation. Drinking plenty of water is important to replenish intra-cellular cells, and physical activities can be slowly incorporated to strengthen muscles.
Conclusion
Taking care of the spine is important by not constantly allowing axial overload to compress the spinal disc through repetitive motion. This causes the disc to degenerate and lead to back pain. However, non-surgical treatments like IDD therapy can help reduce the pain and help strengthen the surrounding muscles protecting the spine. IDD therapy is similar to spinal decompression, which allows the individual to be harnessed to a machine and uses gentle traction on the spine to create negative space in the spinal column and promote the body’s healing factors. Many individuals can see the beneficial results over time and continue their daily routine pain-free.
Many people experience neck and back pain due to various factors that affect their daily routine. These pain conditions are common and can be caused by repetitive motions that impact the surrounding muscles, tissues, ligaments, and spinal discs. Chronic pain can develop depending on the severity and duration of the condition. People with demanding jobs, pre-existing conditions, or older adults may seek medical attention to reduce the pain-like symptoms of neck and back pain. However, treatment costs can be high. There are safe, cost-effective, and non-invasive treatments to relieve neck and back pain. This article will explore why neck and back pain is expensive and why non-surgical treatments are cost-effective. It will also discuss how non-surgical therapies like spinal decompression can alleviate back and neck pain. We work with certified medical providers who use our patients’ valuable information to treat individuals suffering from back and neck pain while informing them about non-surgical treatments like spinal decompression that can help relieve their neck and back pain. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
Why Does Back & Neck Pain Cost More?
Many people report to their primary doctors that they are experiencing radiating pain from the neck or lower back, which affects their upper or lower extremities. For neck pain, they may experience headaches or shoulder pain that causes pain-like symptoms like numbness or tingling sensations down to their arms and fingers. For back pain, they may experience muscle soreness in their lumbar region, which can result in numbness in the glute muscles or cause sciatic nerve pain, affecting their walking ability. Research studies reveal that cognitive, affective, and lifestyle factors all affect the neck and back. High-demanding jobs, stress, or trauma from an accident can develop neck and back pain. As a result, the body takes more overbearing loads, tightening the surrounding muscles in the neck and back. If not treated right away, it can lead to problematic issues that disrupt their routine.
Based on the book “The Ultimate Spinal Decompression” by Dr. Eric Kaplan D.C., FIAMA, and Dr. Perry Bard, D.C., humans’ evolution to walk upright has strained their stability, leading to axial overload and potential neck and back pain. The book also highlights that the human body was not meant to remain sedentary, which can also contribute to the development of such pain. Research studies revealed that neck and back pain can be nociceptive with neuropathic components, making treatment costly and time-consuming. This economic burden can discourage individuals from seeking treatment despite the pain and expense involved.
Fighting Inflammation Naturally- Video
Are you experiencing persistent neck and back pain? Do your upper or lower extremities feel stiff or tingly? Or is your mobility limited, interfering with your daily activities? These issues are often associated with neck and back pain, disrupting a person’s routine and preventing them from enjoying life. Neck and back pain are common ailments that can be expensive to treat. Research studies revealed that they can also influence individuals’ ability to return to work, increasing treatment costs.
Additionally, pain-like symptoms often accompany neck and back pain, leading some individuals to spend nearly a billion dollars on treatment. However, cost-effective treatments are available that can help alleviate these symptoms. The video above explains how non-surgical treatments can reduce neck and back pain and relieve pain-like symptoms.
Why Non-Surgical Treatments Are Cost Effective?
Research studies have shown that non-surgical treatments are a cost-effective and effective solution for neck and back pain. Many individuals can utilize these treatments combined with various therapies to improve their quality of life and reduce pain symptoms. Non-surgical treatments offer personalized plans as healthcare providers work together to find solutions. They provide individuals with a positive approach to regaining their health and wellness by informing them about their bodies and how to be more mindful of how pain affects their daily routines. Some non-surgical treatments that can relieve neck and back pain include:
Chiropractic care
Physical therapy
Spinal Decompression
Acupuncture
Massage therapy
How Spinal Decompression Can Alleviate Back & Neck Pain
You might be interested in non-surgical treatments like spinal decompression if you suffer back or neck pain. This technique uses gentle traction on the spinal column to alleviate pain while helping your body heal naturally. Research studies have found that cervical spinal decompression can increase disc height and reduce pain caused by compressed cervical discs. This treatment can also alleviate residual pain symptoms like headaches or muscle stiffness and restore mobility to the neck. For back pain, research suggests that spinal decompression can reduce the effects of compressed spinal discs, which can aggravate nerve roots like the sciatic nerve in the lumbar region. Many people who try spinal decompression feel relief after just a few sessions and become more mindful of what triggers their pain. This can help them make small lifestyle changes to continue their journey toward health and wellness.
Conclusion
Many people struggle with neck and back pain, which can be caused by multiple normal and traumatic factors and can be costly. Individuals often prefer to endure the pain rather than subject themselves to invasive treatments. However, non-surgical therapies that are cost-effective and gentle on the body are available. Spinal decompression therapy is one such treatment that can help alleviate pain and promote the body’s natural healing processes. By reducing pain symptoms, many individuals who undergo spinal decompression therapy can return to their daily routines pain-free.
Back pain is widespread and can negatively impact an individual’s work productivity. The severity and location of where the pain can vary from acute to chronic, making it a complex problem that can be expensive to treat. Several factors can contribute to back pain, affecting the surrounding muscles, ligaments, and spinal discs in the spinal region. The most commonly affected area where back pain is causing issues is the lumbar region, which supports the upper body’s weight and stabilizes the lower body. Lower back pain can also cause radiating referred pain down to the legs, further affecting an individual’s quality of life. In this article, we will explore the economic cost and burden of chronic back pain and how spinal decompression can help alleviate the pain, allowing many individuals to return to work pain-free. We work with certified medical providers who use our patients’ valuable information to treat individuals with back pain and inform them about non-surgical treatments like spinal decompression that can help relieve them from back pain and get them back to their daily activities. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
The Burden Of Chronic Back Pain
Back pain can range from acute to chronic, depending on the extent of the injury. It can affect the non-specific or specific area of the spine. Non-specific back pain doesn’t have an underlying cause, while specific back pain is due to environmental factors that increase the risk of compressing the spinal discs. Research studies revealed that back pain can be a burden because it is difficult to treat and costly, affecting millions of individuals in the workplace. It is a widespread musculoskeletal disorder that can be disheartening without relief.
The Economic Cost Of Back Pain
Back pain is a significant cause of work loss and limitations for many individuals, as reported by “The Ultimate Spinal Decompression” by Dr. Perry Bard, D.C., and Dr. Eric Kaplan, D.C., FIAMA. Working adults with back pain are more likely to utilize healthcare services, leading to costs of over $12 billion per year, making it one of the most expensive conditions in the U.S. Additional research studies revealed that back pain has a greater economic impact than most other health conditions due to its effect on work absenteeism, reduced productivity, and increased risk of leaving the labor market. This can leave working adults feeling disheartened, angry, depressed, and stressed. However, many cost-effective and safe treatments can help relieve individuals suffering from back pain, eliminating the need for expensive surgeries.
Reducing Soft Tissue Injuries With Chiropractic-Video
Are you suffering from pain that radiates from your back down to your legs? Do you experience stiffness in certain areas of your back or constant stress affecting your work productivity? If so, you may be dealing with back pain, a common complaint among many individuals in the workforce. Depending on its severity, back pain can be either specific or non-specific and is a complex condition that can be expensive to treat. Unfortunately, many working adults continue to work with back pain, which can cause them to take a leave of absence from work due to the pain. This can lead to more harm and disability since the pain can be unbearable. However, there are ways to reduce the effects of back pain and provide relief to many working individuals. Non-surgical treatments such as MET, chiropractic manipulation, traction therapy, and spinal decompression can help reduce the impact of back pain by relieving pain from the surrounding muscles, soft tissues, and ligaments affected by back pain. Additionally, individuals can combine non-surgical treatments with other therapies to prevent back pain from reoccurring and promote overall health and wellness. A video demonstrating these non-surgical treatments is available for your convenience.
The Effects Of Spinal Decompression On Back Pain
Many individuals choose non-surgical treatments to alleviate back pain for their cost-effectiveness, safety, and non-invasiveness. One such treatment is spinal decompression, which research studies have shown to improve lumbar spine conditions in individuals with associated back pain. Spinal decompression uses gentle traction to pull the spine and allow compressed spinal discs to return to their original position, restoring nutrients and oxygenated blood and reducing back pain’s effects. It also relieves nerve root compression, which can affect surrounding muscles. Through regular spinal decompression sessions, individuals can begin to feel relief from back pain while becoming more mindful of the environmental factors that cause it.
Conclusion
Many people in the workforce suffer from back pain, causing them to miss work frequently. This problem is common and expensive to treat due to its complexity. Back pain is often accompanied by other symptoms associated with various conditions that can cause chronic pain. Fortunately, cost-effective and safe treatments can help alleviate back pain and allow individuals to return to work. One effective treatment is spinal decompression, which involves gentle traction that pulls the spine and relieves associated symptoms. This non-surgical treatment is safe, affordable and helps the body heal naturally. After a few sessions, many individuals experience significant relief from back pain and reduced chances of recurrence.
References
Kaplan, E., & Bard, P. (2023). The Ultimate Spinal Decompression. JETLAUNCH.
The human body has various muscle groups, tendons, ligaments, and spinal structures that allow mobility, standing upright, and performing daily activities without discomfort. The spinal column is divided into three regions: cervical, thoracic, and lumbar, each with specific functions. Unfortunately, low back pain affects many working individuals worldwide and can significantly impact their daily lives and productivity. This pain can be caused by various injuries, conditions, and diseases affecting the muscles, tendons, and spinal discs. Enduring the pain and continuing daily activities can worsen the situation, causing more damage to the back and spine. This article explores the causes of low back pain and how non-surgical therapies like spinal decompression can prevent it from returning. We work with certified medical providers who use our patients’ valuable information to treat individuals with low back pain and inform them about spinal decompression’s benefits in alleviating it from reoccurring. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
What Causes Low Back Pain To Return?
Are you experiencing pain in your lower body? Is it impacting your ability to work? Do you feel muscle stiffness when stretching your sides? In the U.S., 25-60% of people who experience low back pain report recurring pain within a year. Research studies revealed that most low back pain is non-specific, meaning no specific causes or structures can be identified as the pain source affecting the low back. Low back pain can be caused by many factors, such as improper lifting of heavy objects, physical inactivity, and excess body weight, which can strain the back muscles. Studies have also revealed that psychological factors like stress, anxiety, or depression can cause tension in the lumbar region, leading to repetitive motions that correlate with low back pain.
People who experience low back pain often take over-the-counter medications for temporary relief before returning to normal activities. However, this only provides short-term relief, and the pain often returns due to various factors like muscle, nerve, and bone issues and referred pain to the abdominal organs, as research studies revealed. To address this, individuals may seek treatment from their primary care doctor. However, as additional studies mentioned, treating low back pain can be difficult due to the specific or non-specific factors involved. Thankfully, non-surgical treatments are available to alleviate symptoms and reduce the likelihood of the pain returning.
The Benefits Of Stretching- Video
Are you someone who spends most of their day sitting down and experiencing muscle stiffness? Do you feel pain in your legs due to radiating pain? Or do you often feel discomfort after lifting or carrying heavy objects? These symptoms are often associated with low back pain, a common problem many people in the workforce experience at some point. The severity of low back pain can range from acute to chronic, depending on how badly the individual has hurt their low back. If left untreated, low back pain can harshly affect a person. However, there are many ways to prevent low back pain from occurring. Multiple treatments can help reduce the associated symptoms of low back pain and can help re-strengthen the muscles. The video above explains the benefits of stretching, how it can help relieve sore muscles affected by low back pain, and how stretching can be combined with other therapies to promote health and wellness.
How Spinal Decompression Can Relieve Low Back Pain
Many people experience low back pain at some point in their lives. If the pain is left untreated, it can develop into chronic back pain. According to “The Ultimate Spinal Decompression,” written by Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., reoccurring low back pain can lead to further degeneration of the lumbar spinal column or be the result of stress and trauma in adjacent muscles. Spinal decompression can provide relief for individuals experiencing this pain. Studies show that spinal decompression creates negative pressure in the spine, which can decrease pressure on the nerve root and hydrate the spinal disc, promoting the body’s natural healing process. Spinal decompression is a safe, gentle, and cost-effective solution for many individuals seeking relief from low back pain.
Conclusion
Low back pain is a common issue that affects many people. Depending on its severity, various factors can cause it, ranging from acute to chronic. Unfortunately, this pain can interfere with daily activities, including work. Thankfully, non-surgical treatments like spinal decompression may help relieve the symptoms associated with low back pain. This treatment involves gentle traction on the lumbar region of the spine, providing much-needed relief to the body. Spinal decompression is an excellent option for those who want to start their journey toward better health and wellness.
Back pain is a common problem that affects people worldwide, but many individuals are unaware of it until they experience constant back muscle aches. Back pain can impact the cervical, thoracic, and lumbar spine and can even lead to referred pain in the arms and legs. Repetitive movements, poor posture, prolonged sitting, and physical inactivity are common causes of back pain. In some cases, traumatic incidents or accidents can also contribute to the development of back pain. To manage back pain, individuals often seek treatments to alleviate it and improve their quality of life. In this article, we’ll explore two treatments to help alleviate back pain and provide tips on managing the pain effectively. We work with certified medical providers who use our patients’ valuable information to treat individuals with back pain and find the right treatment to alleviate their pain. We encourage patients to ask essential questions and seek education from our associated medical providers about their condition. Dr. Jimenez, D.C., provides this information as an educational service. Disclaimer
Spine Surgery For Low Back Pain
Are you experiencing pain in your upper, middle, or lower back? Do you feel a radiating pain running down your arms or legs, or have you noticed that you are hunching over more than usual? These symptoms are often associated with back pain, which can be debilitating. Many people who suffer from back pain seek relief and may opt for surgery to alleviate their symptoms. Research studies revealed that spinal surgery could effectively reduce neurogenic pain and deficits that exacerbate spinal nerve root compression and may help individuals regain their functionality and mobility. However, as research studies stated, surgery is typically recommended only after conservative treatments have been tried for at least six months without success. Several surgical options are available, including injection therapy, non-fusion stabilization, facet and disc replacement, and spinal fusion surgery, which may relieve back pain.
Managing Back Pain After Surgery
Individuals who undergo surgery for back pain must follow a recovery plan to prevent the pain from recurring. Research studies suggest that the effects of spinal surgery for back pain should last for three days, after which adequate rest is essential. Following this, individuals should become pain-free and able to move again. To prevent back pain from returning, doctors often recommend changing daily habits and activities and creating a personalized treatment plan to strengthen back muscles. While surgery for back pain can be expensive, non-surgical treatments are available to alleviate the pain.
The Science Of Motion & Chiropractic Care- Video
Are you experiencing pain in your upper, middle, or lower back? Do you feel discomfort, stiffness, or aches when stretching? Have you engaged in activities that can strain your back muscles? These symptoms often indicate back pain, a common problem many people face at some point. Several factors contribute to back pain, including repetitive movements, spinal disc compression, and spinal nerve root irritation. Physical inactivity, prolonged sitting, heavy lifting, and poor posture are common causes of back pain that can lead to disability. However, various treatments can alleviate the effects of back pain and prevent it from recurring. The video above demonstrates how chiropractic care can help relieve back pain by using spinal manipulation to align the spine. Chiropractic care is a safe, gentle, and affordable non-surgical treatment that can be combined with other therapies to prevent future back pain.
Spinal Decompression For Back Pain
When relieving back pain, some people avoid surgery because it can be expensive. Fortunately, alternative treatments are safe, affordable, and gentle on the spine. Non-surgical options can relieve many individuals suffering from back pain without surgery. Research shows that spinal decompression is an effective treatment that uses gentle traction to create negative pressure in the spinal disc. This can increase hydration and reduce pressure on the nerve root, which can alleviate back pain. Spinal decompression can also help relax and stretch the back muscles by gently pulling the spine. This treatment is cost-effective and can be combined with other therapies to prevent the return of back pain.
The Effects Of Spinal Decompression On Back Pain
Dr. Eric Kaplan, D.C., FIAMA, and Dr. Perry Bard, D.C., wrote “The Ultimate Spinal Decompression,” which states that spinal decompression is safe and effective in reducing back pain. Through spinal decompression, the herniated disc causing back pain is pulled back to its original position, allowing the surrounding nerve roots to relax. Research studies have shown that spinal decompression can help increase spinal disc height and restore mobility to the back and spine, enabling individuals to return to their daily activities without pain.
Conclusion
Across the world back pain is a widespread problem that affects many people worldwide. It can be a significant problem if left untreated. Fortunately, numerous treatment options can alleviate the symptoms and allow individuals to resume their daily activities. The two main types of treatment are surgical and non-surgical therapies. While surgical treatment can be effective, it is also expensive. Non-surgical therapy, on the other hand, is cost-effective. Combining these treatments with other therapies is possible to decrease the likelihood of back pain returning. By listening to their bodies and taking preventive measures, individuals can avoid a reoccurrence of pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine