Andres “Andy” Martinez first came to see Dr. Alex Jimenez in Push Fitness after experiencing low back pain and knee problems. Following a period of physical therapy and rehabilitation, Andy became involved in crossfit, where he learned everything he needed to know about health and wellness from the trainers at Push. Andres Martinez expresses how grateful he is to receive the amount of care he does from the staff and he describes how much his perspective of fitness has changed from the first time he walked in to Push Fitness. Andy has found a family at Push who led him to a healthy, clean life and both the trainers and staff mean everything to Andres Martinez.
Chiropractic Low Back Pain Therapy
CrossFit is a strength and conditioning system consisting chiefly of a mixture of aerobic exercise, calisthenics (body weight exercises), and Olympic weightlifting. CrossFit, Inc. clarifies its strength and conditioning system as “continuously diverse functional movements executed at high intensity across wide time and modal domain names,” with the stated goal of enhancing fitness, which it defines as “work capacity across wide time and modal domains.” CrossFit gyms use gear from multiple disciplines, such as barbells, dumbbells, hands rings, pull-up bars, jump ropes, kettlebells, medicine balls, plyo boxes, resistance bands, rowing machines, and various mats. CrossFit is focused on”constantly diverse, high-intensity, operational motion,” drawing on categories and exercises.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Biochemistry of Pain:�All pain syndromes have an inflammation profile. An inflammatory profile can vary from person to person and can also vary in one person at different times. The treatment of pain syndromes is to understand this inflammation profile. Pain syndromes are treated medically, surgically or both. The goal is to inhibit/suppress the production of inflammatory mediators. And a successful outcome is one that results in less inflammation and of course less pain.
Biochemistry Of Pain
Objectives:
Who are the key players
What are the biochemical mechanisms?
What are the consequences?
Inflammation Review:
Key Players
Why Does My Shoulder Hurt? A Review Of The Neuroanatomical & Biochemical Basis Of Shoulder Pain
ABSTRACT
If a patient asks �why does my shoulder hurt?� the conversation will quickly turn to scientific theory and sometimes unsubstantiated conjecture. Frequently, the clinician becomes aware of the limits of the scientific basis of their explanation, demonstrating the incompleteness of our understanding of the nature of shoulder pain. This review takes a systematic approach to help answer fundamental questions relating to shoulder pain, with a view to providing insights into future research and novel methods for treating shoulder pain. We shall explore the roles of (1) the peripheral receptors, (2) peripheral pain processing or �nociception�, (3) the spinal cord, (4) the brain, (5) the location of receptors in the shoulder and (6) the neural anatomy of the shoulder. We also consider how these factors might contribute to the variability in the clinical presentation, the diagnosis and the treatment of shoulder pain. In this way we aim to provide an overview of the component parts of the peripheral pain detection system and central pain processing mechanisms in shoulder pain that interact to produce clinical pain.
INTRODUCTION: A VERY BRIEF HISTORY OF PAIN SCIENCE ESSENTIAL FOR CLINICIANS
The nature of pain, in general, has been a subject of much controversy over the past century. In the 17th century Descartes� theory1 proposed that the intensity of pain was directly related to the amount of associated tissue injury and that pain was processed in one distinct pathway. Many earlier theories relied upon this so-called �dualist� Descartian philosophy, seeing pain as the consequence of the stimulation of a �specific� peripheral pain receptor in the brain. In the 20th century a scientific battle between two opposing theories ensued, namely specificity theory and pattern theory. The Descartian �specificity theory� saw pain as a specific separate modality of sensory input with its own apparatus, while �pattern theory� felt that pain resulted from the intense stimulation of non-specific receptors.2 In 1965, Wall and Melzack�s 3 gate theory of pain provided evidence for a model in which pain perception was modulated by both sensory feedback and the central nervous system. Another huge advance in pain theory at around the same time saw the discovery of the specific mode of actions of the opioids.4 Subsequently, recent advances in neuroimaging and molecular medicine have vastly expanded our overall understanding of pain.
So how does this relate to shoulder pain?�Shoulder pain is a common clinical problem, and a robust understanding of the way in which pain is processed by the body is essential to best diagnose and treat a patient�s pain. Advances in our knowledge of pain processing promise to explain the mismatch between pathology and the perception of pain, they may also help us explain why certain patients fail to respond to certain treatments.
BASIC BUILDING BLOCKS OF PAIN
Peripheral sensory receptors: the mechanoreceptor and the �nociceptor�
There are numerous types of peripheral sensory receptors present in the human musculoskeletal system. 5 They may be classified based on their func�tion (as mechanoreceptors, thermoreceptors or nociceptors) or morphology (free nerve endings or different types of encapsulated receptors).5 The dif�ferent types of receptor can then be further subclas�sified based on the presence of certain chemical markers. There are significant overlaps between dif�ferent functional classes of receptor, for example
Peripheral Pain Processing: �Nociception�
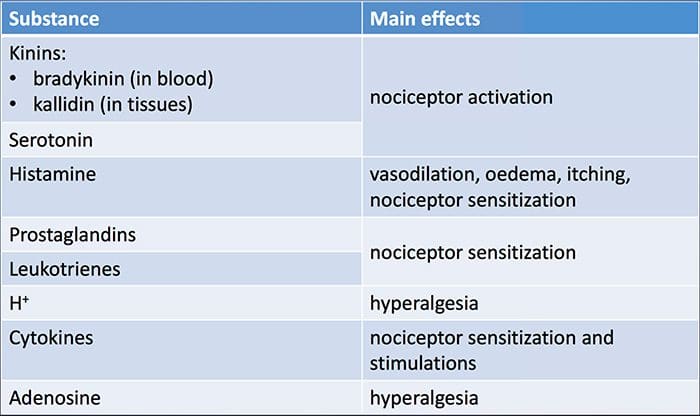
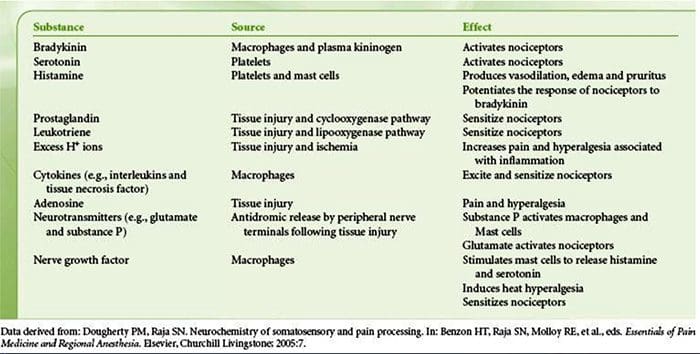
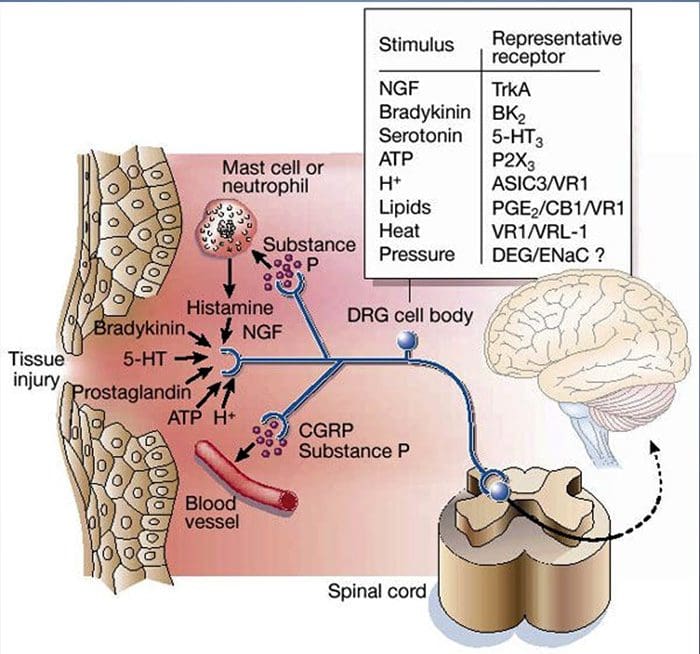
Tissue injury involves a variety of inflammatory mediators being released by damaged cells including bradykinin, histamine, 5-hydroxytryptamine, ATP, nitric oxide and certain ions (K+ and H+). The activation of the arachidonic acid pathway leads to the production of prostaglandins, thromboxanes and leuko- trienes. Cytokines, including the interleukins and tumor necrosis factor ?, and neurotrophins, such as nerve growth factor (NGF), are also released and are intimately involved in the facilitation of inflammation.15 Other substances such as excitatory amino acids (glutamate) and opioids (endothelin-1) have also been implicated in the acute inflammatory response.16 17 Some of these agents may directly activate nociceptors, while others bring about the recruitment of other cells which then release further facilitatory agents.18 This local process resulting in the increased responsiveness of nociceptive neurons to their normal input and/or the recruitment of a response to normally subthreshold inputs is termed �peripheral sensitization�.�Figure 1 summarizes some of the key mechanisms involved.
NGF and the transient receptor potential cation channel subfamily V member 1 (TRPV1) receptor have a symbiotic relationship when it comes to inflammation and nociceptor sensitization. The cytokines produced in inflamed tissue result in an increase in NGF production.19 NGF stimulates the release of histamine and serotonin (5-HT3) by mast cells, and also sensitizes nociceptors, possibly altering the properties of A? fibers such that a greater proportion become nociceptive. The TRPV1 receptor is present in a subpopulation of primary afferent fibers and is activated by capsaicin, heat and protons. The TRPV1 receptor is synthesized in the cell body of the afferent fibre, and is transported to both the peripheral and central terminals, where it contributes to the sensitivity of nociceptive afferents. Inflammation results in NGF production peripherally which then binds to the tyrosine kinase receptor type 1 receptor on the nociceptor terminals, NGF is then transported to the cell body where it leads to an up regulation of TRPV1 transcription and consequently increased nociceptor sensitivity.19 20 NGF and other inflammatory mediators also sensitize TRPV1 through a diverse array of secondary messenger pathways. Many other receptors including cholinergic receptors, ?-aminobutyric acid (GABA) receptors and somatostatin receptors are also thought to be involved in peripheral nociceptor sensitivity.
A large number of inflammatory mediators have been specifically implicated in shoulder pain and rotator cuff disease.21�25 While some chemical mediators directly activate nociceptors, most lead to changes in the sensory neuron itself rather than directly activating it. These changes may be early post- translational or delayed transcription dependent. Examples of the former are changes in the TRPV1 receptor or in voltage- gated ion channels resulting from the phosphorylation of membrane-bound proteins. Examples of the latter include the NGF-induced increase in TRV1 channel production and the calcium-induced activation of intracellular transcription factors.
Molecular Mechanisms Of Nociception
The sensation of pain alerts us to real or impending injury and triggers appropriate protective responses. Unfortunately, pain often outlives its usefulness as a warning system and instead becomes chronic and debilitating. This transition to a chronic phase involves changes within the spinal cord and brain, but there is also remarkable modulation where pain messages are initiated � at the level of the primary sensory neuron. Efforts to determine how these neurons detect pain-producing stimuli of a thermal, mechanical or chemical nature have revealed new signaling mechanisms and brought us closer to understanding the molecular events that facilitate transitions from acute to persistent pain.
The Neurochemistry Of Nociceptors
Glutamate is the predominant excitatory neurotransmitter in all nociceptors. Histochemical studies of adult DRG, however, reveal two broad classes of unmyelinated C fiber.
Chemical Transducers To Make The Pain Worse
As described above, injury heightens our pain experience by increasing the sensitivity of nociceptors to both thermal and mechanical stimuli. This phenomenon results, in part, from the production and release of chemical mediators from the primary sensory terminal and from non-neural cells (for example, fibroblasts, mast cells, neutrophils and platelets) in the environment36 (Fig. 3). Some components of the inflammatory soup (for example, protons, ATP, serotonin or lipids) can alter neuronal excitability directly by inter- acting with ion channels on the nociceptor surface, whereas others (for example, bradykinin and NGF) bind to metabotropic receptors and mediate their effects through second-messenger signaling cascades11. Considerable progress has been made in understanding the biochemistry basis of such modulatory mechanisms.
Extracellular Protons & Tissue Acidosis
Local tissue acidosis is a hallmark physiological response to injury, and the degree of associated pain or discomfort is well correlated with the magnitude of acidification37. Application of acid (pH 5) to the skin produces sustained discharges in a third or more of polymodal nociceptors that innervate the receptive field 20.
Cellular & Molecular Mechanisms Of Pain
Abstract
The nervous system detects and interprets a wide range of thermal and mechanical stimuli as well as environmental and endogenous chemical irritants. When intense, these stimuli generate acute pain, and in the setting of persistent injury, both peripheral and central nervous system components of the pain transmission pathway exhibit tremendous plasticity, enhancing pain signals and producing hypersensitivity. When plasticity facilitates protective reflexes, it can be beneficial, but when the changes persist, a chronic pain condition may result. Genetic, electrophysiological, and pharmacological studies are elucidating the molecular mechanisms that underlie detection, coding, and modulation of noxious stimuli that generate pain.
Introduction: Acute Versus Persistent Pain
Figure 5. Spinal Cord (Central) Sensitization
Glutamate/NMDA receptor-mediated sensitization.�Following intense stimulation or persistent injury, activated C and A? nociceptors release a variety of neurotransmitters including dlutamate, substance P, calcitonin-gene related peptide (CGRP), and ATP, onto output neurons in lamina I of the superficial dorsal horn (red). As a consequence, normally silent NMDA glutamate receptors located in the postsynaptic neuron can now signal, increase intracellular calcium, and activate a host of calcium dependent signaling pathways and second messengers including mitogen-activated protein kinase (MAPK), protein kinase C (PKC), protein kinase A (PKA) and Src. This cascade of events will increase the excitability of the output neuron and facilitate the transmission of pain messages to the brain.
Disinhibition.�Under normal circumstances, inhibitory interneurons (blue) continuously release GABA and/or glycine (Gly) to decrease the excitability of lamina I output neurons and modulate pain transmission (inhibitory tone). However, in the setting of injury, this inhibition can be lost, resulting in hyperalgesia. Additionally, disinhibition can enable non-nociceptive myelinated A? primary afferents to engage the pain transmission circuitry such that normally innocuous stimuli are now perceived as painful. This occurs, in part, through the disinhibition of excitatory PKC? expressing interneurons in inner lamina II.
Microglial activation.�Peripheral nerve injury promotes release of ATP and the chemokine fractalkine that will stimulate microglial cells. In particular, activation of purinergic, CX3CR1, and Toll-like receptors on microglia (purple) results in the release of brain-derived neurotrophic factor (BDNF), which through activation of TrkB receptors expressed by lamina I output neurons, promotes increased excitability and enhanced pain in response to both noxious and innocuous stimulation (that is, hyperalgesia and allodynia). Activated microglia also release a host of cytokines, such as tumor necrosis factor ? (TNF?), interleukin-1? and 6 (IL-1?, IL-6), and other factors that contribute to central sensitization.
The Chemical Milieu Of Inflammation
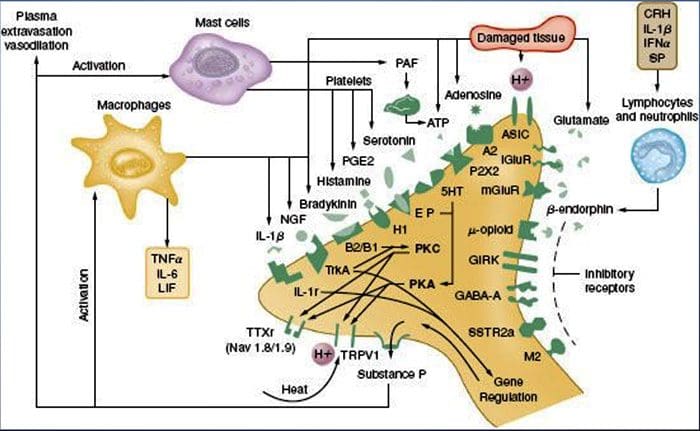
Peripheral sensitization more commonly results from inflammation-associated changes in the chemical environment of the nerve fiber (McMahon et al., 2008). Thus, tissue damage is often accompanied by the accumulation of endogenous factors released from activated nociceptors or non-neural cells that reside within or infiltrate into the injured area (including mast cells, basophils, platelets, macrophages, neutrophils, endothelial cells, keratinocytes, and fibroblasts). Collectively. these factors, referred to as the �inflammatory soup�, represent a wide array of signaling molecules, including neurotransmitters, peptides (substance P, CGRP, bradykinin), eicosinoids and related lipids (prostaglandins, thromboxanes, leukotrienes, endocannabinoids), neurotrophins, cytokines, and chemokines, as well as extracellular proteases and protons. Remarkably, nociceptors express one or more cell surface receptors capable of recognizing and responding to each of these pro-inflammatory or pro-algesic agents (Figure 4). Such interactions enhance excitability of the nerve fiber, thereby heightening its sensitivity to temperature or touch.
Unquestionably the most common approach to reducing inflammatory pain involves inhibiting the synthesis or accumulation of components of the inflammatory soup. This is best exemplified by non-steroidal anti-inflammatory drugs, such as aspirin or ibuprofen, which reduce inflammatory pain and hyperalgesia by inhibiting cyclooxygenases (Cox-1 and Cox-2) involved in prostaglandin synthesis. A second approach is to block the actions of inflammatory agents at the nociceptor. Here, we highlight examples that provide new insight into cellular mechanisms of peripheral sensitization, or which form the basis of new therapeutic strategies for treating inflammatory pain.
NGF is perhaps best known for its role as a neurotrophic factor required for survival and development of sensory neurons during embryogenesis, but in the adult, NGF is also produced in the setting of tissue injury and constitutes an important component of the inflammatory soup (Ritner et al., 2009). Among its many cellular targets, NGF acts directly on peptidergic C fiber nociceptors, which express the high affinity NGF receptor tyrosine kinase, TrkA, as well as the low affinity neurotrophin receptor, p75 (Chao, 2003; Snider and McMahon, 1998). NGF produces profound hypersensitivity to heat and mechanical stimuli through two temporally distinct mechanisms. At first, a NGF-TrkA interaction activates downstream signaling pathways, including phospholipase C (PLC), mitogen-activated protein kinase (MAPK), and phosphoinositide 3-kinase (PI3K). This results in functional potentiation of target proteins at the peripheral nociceptor terminal, most notably TRPV1, leading to a rapid change in cellular and behavioral heat sensitivity (Chuang et al., 2001).
Irrespective of their pro-nociceptive mechanisms, interfering with neurotrophin or cytokine signaling has become a major strategy for controlling inflammatory disease or resulting pain. The main approach involves blocking NGF or TNF-? action with a neutralizing antibody. In the case of TNF-?, this has been remarkably effective in the treatment of numerous autoimmune diseases, including rheumatoid arthritis, leading to dramatic reduction in both tissue destruction and accompanying hyperalgesia (Atzeni et al., 2005). Because the main actions of NGF on the adult nociceptor occur in the setting of inflammation, the advantage of this approach is that hyperalgesia will decrease without affecting normal pain perception. Indeed, anti-NGF antibodies are currently in clinical trials for treatment of inflammatory pain syndromes (Hefti et al., 2006).
Glutamate/NMDA Receptor-Mediated Sensitization
Acute pain is signaled by the release of glutamate from the central terminals of nociceptors, generating excitatory post-synaptic currents (EPSCs) in second order dorsal horn neurons. This occurs primarily through activation of postsynaptic AMPA and kainate subtypes of ionotropic glutamate receptors. Summation of sub-threshold EPSCs in the postsynaptic neuron will eventually result in action potential firing and transmission of the pain message to higher order neurons.
Other studies indicate that changes in the projection neuron, itself, contribute to the dis- inhibitory process. For example, peripheral nerve injury profoundly down-regulates the K+- Cl- co-transporter KCC2, which is essential for maintaining normal K+ and Cl- gradients across the plasma membrane (Coull et al., 2003). Downregulating KCC2, which is expressed in lamina I projection neurons, results in a shift in the Cl- gradient, such that activation of GABA-A receptors depolarize, rather than hyperpolarize the lamina I projection neurons. This would, in turn, enhance excitability and increase pain transmission. Indeed, pharmacological blockade or siRNA-mediated downregulation of KCC2 in the rat induces mechanical allodynia.
Share Ebook
Sources:
Why does my shoulder hurt? A review of the neuroanatomical and biochemical basis of shoulder pain
Benjamin John Floyd Dean, Stephen Edward Gwilym, Andrew Jonathan Carr
Cellular and Molecular Mechanisms of Pain
Allan I. Basbaum1, Diana M. Bautista2, Gre?gory Scherrer1, and David Julius3
1Department of Anatomy, University of California, San Francisco 94158
2Department of Molecular and Cell Biology, University of California, Berkeley CA 94720 3Department of Physiology, University of California, San Francisco 94158
Molecular mechanisms of nociception
David Julius* & Allan I. Basbaum�
*Department of Cellular and Molecular Pharmacology, and �Departments of Anatomy and Physiology and W. M. Keck Foundation Center for Integrative Neuroscience, University of California San Francisco, San Francisco, California 94143, USA (e-mail: [email protected])
Doctor 0f Chiropractic: Charlie Quiroga found the extra “push” she needed at PUSH Fitness so as to regain her fitness and get back in shape, as well as to improve her overall health and wellbeing. Charlie Quiroga is grateful to the coaches which helped keep her motivated to continue following a healthier lifestyle. Charlie Quiroga has heard the significance of “pushing” herself towards her goals and remaining positive. Charlie Quiroga urges PUSH as the fitness choice that is very best.
Weight Loss Doctor Of Chiropractic
Weight management techniques encircle long-term lifestyle plans that promote healthy eating and daily physical activity. Effective weight management programs consider not just weight reduction but also the maintenance of a healthy body weight with time. Moreover, weight control entails understanding of meaningful procedures to track weight over time and set perfect body weights for different individuals. Weight control doesn’t include things like fad diets that promote quick weight loss. It targets the results that are achieved through weight loss.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Bernadette Banda informs her compelling weight loss story while she clarifies how much her life has changed since she discovered the right fitness regimen with Dr. Alex Jimenez and Daniel “Danny” Alvarado in PUSH Fitness. PUSH became Bernadette Banda’s life philosophy, where she took it on herself never to give up and to always “push” herself towards any fitness goal she wished to attain. With tremendous gratitude, Bernadette Banda praises Danny’s and all the other coach’s efforts and support to help her become healthy.
Chiropractic Weight Loss Treatment
Intentional weight loss is the decrease in total body mass because of attempts to improve fitness and wellness. Weight loss in people who are overweight or obese can decrease health risks, increase health, and may delay the onset of diabetes. It may decrease pain and increase movement in people with osteoarthritis of the knee. Weight reduction may result in a drop in hypertension. Weight loss occurs when the body is expending more energy in metabolism than it’s swallowing from meals or additional nutrients. It is going to then use stored reserves from fat or muscle, slowly resulting in weight loss.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Neurogenic inflammation, or NI, is the physiological process where mediators are discharged directly from the cutaneous nerves to commence an inflammatory response. This results in the creation of local inflammatory reactions including, erythema, swelling, temperature increase, tenderness, and pain. Fine unmyelinated afferent somatic C-fibers, which respond to low intensity mechanical and chemical stimulations, are largely responsible for the release of these inflammatory mediators.
When stimulated, these nerve pathways in the cutaneous nerves release energetic neuropeptides, or substance P and calcitonin gene related peptide (CGRP), rapidly into the microenvironment, triggering a series of inflammatory responses. There is a significant distinction in immunogenic inflammation, that’s the very first protective and reparative response made by the immune system when a pathogen enters the body, whereas neurogenic inflammation involves a direct connection between the nervous system and the inflammatory responses. Even though neurogenic inflammation and immunologic inflammation can exist concurrently, the two are not clinically indistinguishable. The purpose of the article below is to discuss the mechanism of neurogenic inflammation and the peripheral nervous system’s role in host defense and immunopathology.
Neurogenic Inflammation � The Peripheral Nervous System�s Role in Host Defense and Immunopathology
Abstract
The peripheral nervous and immune systems are traditionally thought of as serving separate functions. This line is, however, becoming increasingly blurred by new insights into neurogenic inflammation. Nociceptor neurons possess many of the same molecular recognition pathways for danger as immune cells and in response to danger, the peripheral nervous system directly communicates with the immune system, forming an integrated protective mechanism. The dense innervation network of sensory and autonomic fibers in peripheral tissues and high speed of neural transduction allows for rapid local and systemic neurogenic modulation of immunity. Peripheral neurons also appear to play a significant role in immune dysfunction in autoimmune and allergic diseases. Therefore, understanding the coordinated interaction of peripheral neurons with immune cells may advance therapeutic approaches to increase host defense and suppress immunopathology.
Introduction
Two thousand years ago, Celsus defined inflammation as involving four cardinal signs � Dolor (pain), Calor (heat), Rubor (redness), and Tumor (swelling), an observation indicating that activation of the nervous system was recognized as being integral to inflammation. However, pain has been mainly thought of since then, only as a symptom, and not a participant in the generation of inflammation. In this perspective, we show that the peripheral nervous system plays a direct and active role in modulating innate and adaptive immunity, such that the immune and nervous systems may have a common integrated protective function in host defense and the response to tissue injury, an intricate interaction that also can lead to pathology in allergic and autoimmune diseases.
Survival of organisms is critically dependent on the capacity to mount a defense against potential harm from tissue damage and infection. Host defense involves both avoidance behavior to remove contact with a dangerous (noxious) environment (a neural function), and active neutralization of pathogens (an immune function). Traditionally, the role of the immune system in combating infective agents and repairing tissue injury has been considered quite distinct from that of the nervous system, which transduces damaging environmental and internal signals into electrical activity to produce sensations and reflexes (Fig. 1). We propose that these two systems are actually components of a unified defense mechanism. The somatosensory nervous system is ideally placed to detect danger. Firstly, all tissues that are highly exposed to the external environment, such as epithelial surfaces of the skin, lungs, urinary and digestive tract, are densely innervated by nociceptors, high threshold pain-producing sensory fibers. Secondly, transduction of noxious external stimuli is almost instantaneous, orders of magnitude quicker than the mobilization of the innate immune system, and therefore may be the �first responder� in host defense.
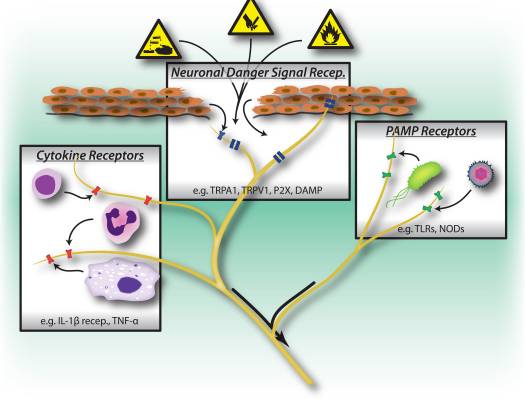
Figure 1: Noxious stimuli, microbial and inflammatory recognition pathways trigger activation of the peripheral nervous system. Sensory neurons possess several means of detecting the presence of noxious/harmful stimuli. 1) Danger signal receptors, including TRP channels, P2X channels, and danger associated molecular pattern (DAMP) receptors recognize exogenous signals from the environment (e.g. heat, acidity, chemicals) or endogenous danger signals released during trauma/tissue injury (e.g. ATP, uric acid, hydroxynonenals). 2) Pattern recognition receptors (PRRs) such as Toll-like receptors (TLRs) and Nod-like receptors (NLRs) recognize Pathogen associated molecular patterns (PAMPs) shed by invading bacteria or viruses during infection. 3) Cytokine receptors recognize factors secreted by immune cells (e.g. IL-1beta, TNF-alpha, NGF), which activate map kinases and other signaling mechanisms to increase membrane excitability.
In addition to orthodromic inputs to the spinal cord and brain from the periphery, action potentials in nociceptor neurons can also be transmitted antidromically at branch points back down to the periphery, the axon reflex. These together with sustained local depolarizations lead to a rapid and local release of neural mediators from both peripheral axons and terminals (Fig. 2) 1. Classic experiments by Goltz (in 1874) and by Bayliss (in 1901) showed that electrically stimulating dorsal roots induces skin vasodilation, which led to the concept of a �neurogenic inflammation�, independent of that produced by the immune system (Fig. 3).
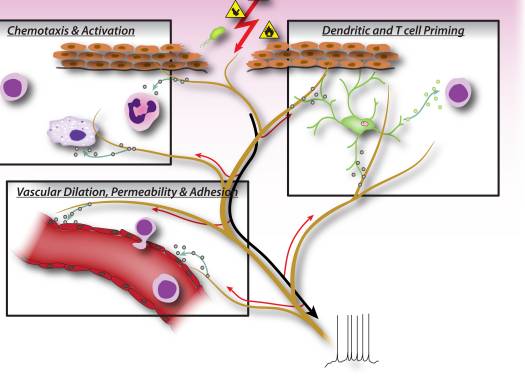
Figure 2: Neuronal factors released from nociceptor sensory neurons directly drive leukocyte chemotaxis, vascular hemodynamics and the immune response. When noxious stimuli activate afferent signals in sensory nerves, antidromic axon reflexes are generated that induce the release of neuropeptides at the peripheral terminals of the neurons. These molecular mediators have several inflammatory actions: 1) Chemotaxis and activation of neutrophils, macrophages and lymphocytes to the site of injury, and degranulation of mast cells. 2) Signaling to vascular endothelial cells to increase blood flow, vascular leakage and edema. This also allows easier recruitment of inflammatory leukocytes. 3) Priming of dendritic cells to drive subsequent T helper cell differentiation into Th2 or Th17 subtypes.
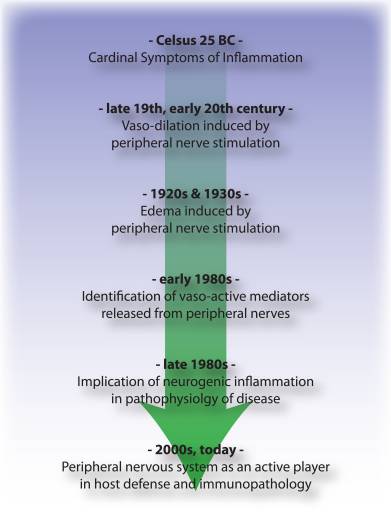
Figure 3: Timeline of advances in understanding of the neurogenic aspects of inflammation from Celsus to the present day.
Neurogenic inflammation is mediated by the release of the neuropeptides calcitonin gene related peptide (CGRP) and substance P (SP) from nociceptors, which act directly on vascular endothelial and smooth muscle cells 2�5. CGRP produces vasodilation effects 2, 3, whereas SP increases capillary permeability leading to plasma extravasation and edema 4, 5, contributing to the rubor, calor and tumor of Celsus. However, nociceptors release many additional neuropeptides (online database: http://www.neuropeptides.nl/), including Adrenomedullin, Neurokinins A and B, Vasoactive intestinal peptide (VIP), neuropeptide (NPY), and gastrin releasing peptide (GRP), as well as other molecular mediators such as glutamate, nitric oxide (NO) and cytokines such as eotaxin 6.
We now appreciate that the mediators released from sensory neurons in the periphery not only act on the vasculature, but also directly attract and activate innate immune cells (mast cells, dendritic cells), and adaptive immune cells (T lymphocytes) 7�12. In the acute setting of tissue damage, we conjecture that neurogenic inflammation is protective, facilitating physiological wound healing and immune defense against pathogens by activating and recruiting immune cells. However, such neuro-immune communications also likely play major roles in the pathophysiology of allergic and autoimmune diseases by amplifying pathological or maladaptive immune responses. In animal models of rheumatoid arthritis for example, Levine and colleagues have shown that denervation of the joint leads to a striking attenuation in inflammation, that is dependent on neural expression of substance P 13, 14. In recent studies of allergic airway inflammation, colitis and psoriasis, primary sensory neurons play a central role in initiating and augmenting the activation of innate and adaptive immunity 15�17.
We propose therefore, that the peripheral nervous system not only plays a passive role in host defense (detection of noxious stimuli and initiation of avoidance behavior), but also an active role in concert with the immune system in modulating the responses to and combat of harmful stimuli, a role that can be subverted to contribute to disease.
Shared Danger Recognition Pathways in the Peripheral Nervous and Innate Immune Systems
Peripheral sensory neurons are adapted to recognize danger to the organism by virtue of their sensitivity to intense mechanical, thermal and irritant chemical stimuli (Fig. 1). Transient receptor potential (TRP) ion channels are the most widely studied molecular mediators of nociception, conducting non-selective entry of cations upon activation by various noxious stimuli. TRPV1 is activated by high temperatures, low pH and capsaicin, the vallinoid irritant component of chili peppers 18. TRPA1 mediates the detection of reactive chemicals including environmental irritants such as tear gas and industrial isothiocyanates 19, but more importantly, it is also activated during tissue injury by endogenous molecular signals including 4-hydroxynonenal and prostaglandins 20, 21.
Interestingly, sensory neurons share many of the same pathogen and danger molecular recognition receptor pathways as innate immune cells, which enable them also to detect pathogens (Fig. 1). In the immune system, microbial pathogens are detected by germline encoded pattern recognition receptors (PRRs), which recognize broadly conserved exogenous pathogen-associated molecular patterns (PAMPs). The first PRRs to be identified were members of toll-like receptor (TLR) family, which bind to yeast, bacterial derived cell-wall components and viral RNA 22. Following PRR activation, downstream signaling pathways are turned on that induce cytokine production and activation of adaptive immunity. In addition to TLRs, innate immune cells are activated during tissue injury by endogenous derived danger signals, also known as damage-associated molecular patterns (DAMPs) or alarmins 23, 24. These danger signals include HMGB1, uric acid, and heat shock proteins released by dying cells during necrosis, activating immune cells during non-infectious inflammatory responses.
PRRs including TLRs 3, 4, 7, and 9 are expressed by nociceptor neurons, and stimulation by TLR ligands leads to induction of inward currents and sensitization of nociceptors to other pain stimuli 25�27. Furthermore, activation of sensory neurons by the TLR7 ligand imiquimod leads to activation of an itch specific sensory pathway 25. These results indicate that infection-associated pain and itch may be partly due to direct activation of neurons by pathogen-derived factors, which in turn activate immune cells through peripheral release of neuronal signaling molecules.
A major DAMP/alarmin released during cellular injury is ATP, which is recognized by purinergic receptors on both nociceptor neurons and immune cells 28�30. Purinergic receptors are made up of two families: P2X receptors, ligand-gated cation channels, and P2Y receptors, G-protein coupled receptors. In nociceptor neurons, recognition of ATP occurs through P2X3, leading to rapidly densensitizing cation currents and pain 28, 30 (Fig. 1), while P2Y receptors contribute to nociceptor activation by sensitization of TRP and voltage-gated sodium channels. In macrophages, ATP binding to P2X7 receptors leads to hyperpolarization, and downstream activation of the inflammasome, a molecular complex important in generation of IL-1beta and IL-18 29. Therefore, ATP is a potent danger signal that activates both peripheral neurons and innate immunity during injury, and some evidence even suggests that neurons express parts of the inflammasome molecular machinery 31.
The flip side of danger signals in nociceptors is the role of TRP channels in immune cell activation. TRPV2, a homologue of TRPV1 activated by noxious heat, is expressed at high levels in innate immune cells 32. Genetic ablation of TRPV2 led to defects in macrophage phagocytosis and clearance of bacterial infections 32. Mast cells also express TRPV channels, which may directly mediate their degranulation 33. It remains to be determined whether endogenous danger signals activate immune cells in a similar manner as nociceptors.
A key means of communication between immune cells and nociceptor neurons are through cytokines. Upon activation of cytokine receptors, signal transduction pathways are activated in sensory neurons leading to downstream phosphorylation of membrane proteins including TRP and voltage-gated channels (Fig. 1). The resulting sensitization of nociceptors means that normally innocuous mechanical and heat stimuli can now activate nociceptors. Interleukin 1 beta and TNF-alpha are two important cytokines released by innate immune cells during inflammation. IL-1beta and TNF-alpha are directly sensed by nociceptors which express the cognate receptors, induce activation of p38 map kinases leading to increased membrane excitability 34�36. Nerve growth factor (NGF) and prostaglandin E(2) are also major inflammatory mediators released from immune cells that act directly on peripheral sensory neurons to cause sensitization. An important effect of nociceptor sensitization by immune factors is an increased release of neuropeptides at peripheral terminals that further activate immune cells, thereby inducing a positive feedback loop that drives and facilitates inflammation.
Sensory Nervous System Control of Innate and Adaptive Immunity
In early phases of inflammation, sensory neurons signal to tissue resident mast cells and dendritic cells, which are innate immune cells important in initiating the immune response (Fig. 2). Anatomical studies have shown a direct apposition of terminals with mast cells, as well as with dendritic cells, and the neuropeptides released from nociceptors can induce degranulation or cytokine production in these cells 7, 9, 37. This interaction plays an important role in allergic airway inflammation and dermatitis 10�12.
During the effector phase of inflammation, immune cells need to find their way to the specific site of injury. Many mediators released from sensory neurons, neuropeptides, chemokines, and glutamate, are chemotactic for neutrophils, eosinophils, macrophages, and T-cells, and enhance endothelial adhesion which facilitates immune cell homing 6, 38�41 (Fig. 2). Furthermore, some evidence implies that neurons may directly participate in the effector phase, as neuropeptides themselves may have direct antimicrobial functions 42.
Neuronally derived signaling molecules can also direct the type of inflammation, by contributing to the differentiation or specification of different types of adaptive immune T cells. An antigen is phagocytosed and processed by innate immune cells, which then migrate to the nearest lymph node and present the antigenic peptide to na�ve T cells. Depending on the type of antigen, costimulatory molecules on the innate immune cell, and the combinations of specific cytokines, na�ve T cells mature into specific subtypes that best serve the inflammatory effort to clear the pathogenic stimulus. CD4 T cells, or T helper (Th) cells, can be divided into four principle groups, Th1, Th2, Th17, and T regulatory cells (Treg). Th1 cells are mainly involved in regulating immune responses to intracellular microorganisms and organ-specific autoimmune diseases; Th2 are critical for immunity against extracellular pathogens, such as helminths, and are responsible for allergic inflammatory diseases; Th17 cells play a central role in protection against microbial challenges, such as extracellular bacteria and fungi; Treg cells are involved in maintaining self tolerance and regulating immune responses. This T cell maturation process appears to be heavily influenced by sensory neuronal mediators. Neuropeptides, such as CGRP and VIP, can bias dendritic cells towards a Th2-type immunity and reduce Th1-type immunity by promoting the production of certain cytokines and inhibiting others, as well as by reducing or enhancing dendritic cell migration to local lymph nodes 8, 10, 43. Sensory neurons also contribute considerably to allergic (mainly Th2 driven) inflammation 17. In addition to regulating Th1 and Th2 cells, other neuropeptides, such as SP and Hemokinin-1, can drive the inflammatory response more toward Th17 or Treg 44, 45, which means that neurons may also be involved in regulating inflammatory resolution. In immunopathologies such as colitis and psoriasis, blockade of neuronal mediators like substance P may significantly dampen T cell and immune mediated damage 15�17, although antagonizing one mediator may by itself only have a limited effect on neurogenic inflammation.
Considering that signaling molecules released from peripheral sensory nerve fibers regulate not only small blood vessels, but also the chemotaxis, homing, maturation, and activation of immune cells, it is becoming clear that neuro-immune interactions are much more intricate than previously thought (Fig. 2). Furthermore, it is quite conceivable that it is not individual neural mediators but rather specific combinations of signaling molecules released from nociceptors that influence different stages and types of immune responses.
Autonomic Reflex Control of Immunity
A role for a cholinergic autonomic nervous system �reflex� circuit in the regulation of peripheral immune responses also appears prominent 46. The vagus is the chief parasympathetic nerve connecting the brainstem with visceral organs. Work by Kevin Tracey and others point to potent generalized anti-inflammatory responses in septic shock and endotoxemia, triggered by an efferent vagal nerve activity leading to a suppression of peripheral macrophages 47�49. The vagus activates peripheral adrenergic celiac ganglion neurons innervating the spleen, leading to the downstream release of acetylcholine, which binds to alpha-7 nicotinic receptors on macrophages in the spleen and gastrointestinal tract. This induces activation of the JAK2/STAT3 SOCS3 signaling pathway, which powerfully suppresses TNF-alpha transcription 47. The adrenergic celiac ganglion also directly communicates with a subset of acetylcholine producing memory T cells, which suppress inflammatory macrophages 48.
Invariant natural Killer T cells (iNKT) are a specialized subset of T cells that recognize microbial lipids in the context of CD1d instead of peptide antigens. NKT cells are a key lymphocyte population involved in the combat of infectious pathogens and regulation of systemic immunity. NKT cells reside and traffic mainly through the vasculature and sinusoids of the spleen and liver. Sympathetic beta-adrenergic nerves in the liver directly signal to modulate NKT cell activity 50. During a mouse model of stroke (MCAO), for example, liver NKT cell mobility was visibly suppressed, which was reversed by sympathetic denervation or beta-adrenergic antagonists. Furthermore, this immunosuppressive activity of noradrenergic neurons on NKT cells led to increases in systemic infection and lung injury. Therefore, efferent signals from autonomic neurons can mediate a potent immuno-suppression.
Dr. Alex Jimenez’s Insight
Neurogenic inflammation is a local inflammatory response generated by the nervous system. It is believed to play a fundamental role in the pathogenesis of a variety of health issues, including, migraine, psoriasis, asthma, fibromyalgia, eczema, rosacea, dystonia and multiple chemical sensitivity. Although neurogenic inflammation associated with the peripheral nervous system has been extensively researched, the concept of neurogenic inflammation within the central nervous system still needs further research. According to several research studies, however, magnesium deficiencies are believed to be the main cause for neurogenic inflammation. The following article demonstrates an overview of the mechanisms of neurogenic inflammation in the nervous system, which may help healthcare professionals determine the best treatment approach to care for a variety of health issues associated with the nervous system.
Conclusions
What are the respective specific roles of the somatosensory and autonomic nervous systems in regulating inflammation and the immune system (Fig. 4)? Activation of nociceptors leads to local axon reflexes, which locally recruit and activate immune cells and is therefore, mainly pro-inflammatory and spatially confined. In contrast, autonomic stimulation leads to a systemic immunosuppression by affecting pools of immune cells in liver and spleen. The afferent signaling mechanisms in the periphery leading to the triggering of the immunosuppressive vagal cholinergic reflex circuit are poorly understood. However, 80�90% of vagal fibers are primary afferent sensory fibers, and therefore signals from the viscera, many potentially driven by immune cells, may lead to activation of interneurons in the brainstem and through them to an output in efferent vagal fibers 46.
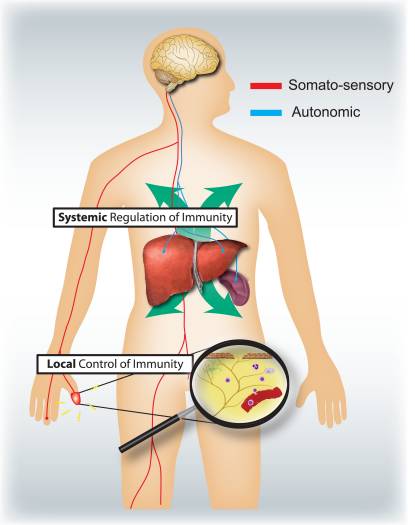
Figure 4: Sensory and autonomic nervous systems modulate local and systemic immune responses respectively. Nociceptors innervating epithelial surfaces (e.g. skin and lung) induce localized inflammatory responses, activating mast cells and dendritic cells. In allergic airway inflammation, dermatitis and rheumatoid arthritis, nociceptor neurons play a role in driving inflammation. By contrast, autonomic circuits innervating the visceral organs (e.g. spleen and liver) regulate systemic immune responses by blocking macrophage and NKT cell activation. In stroke and septic endotoxemia, these neurons play an immunosuppressive role.
Typically, the time course and nature of inflammation, whether during infection, allergic reactions, or auto-immune pathologies, is defined by the categories of immune cells involved. It will be important to know what different types of immune cells are regulated by sensory and autonomic signals. A systematic assessment of what mediators can be released from nociceptors and autonomic neurons and the expression of receptors for these by different innate and adaptive immune cells might help address this question.
During evolution, similar danger detection molecular pathways have developed for both innate immunity and nociception even though the cells have completely different developmental lineages. While PRRs and noxious ligand-gated ion channels are studied separately by immunologists and neurobiologists, the line between these two fields is increasingly blurred. During tissue damage and pathogenic infection, release of danger signals are likely to lead to a coordinated activation of both peripheral neurons and immune cells with complex bidirectional communication, and an integrated host defense. The anatomical positioning of nociceptors at the interface with the environment, the speed of neural transduction and their ability to release potent cocktails of immune-acting mediators allows the peripheral nervous system to actively modulate the innate immune response and coordinate downstream adaptive immunity. Conversely, nociceptors are highly sensitive to immune mediators, which activate and sensitize the neurons. Neurogenic and immune-mediated inflammation are not, therefore, independent entities but act together as early warning devices. However, the peripheral nervous system also plays an important role in the pathophysiology, and perhaps etiology, of many immune diseases like asthma, psoriasis, or colitis because its capacity to activate the immune system can amplify pathological inflammation 15�17. Treatment for immune disorders may need to include, therefore, the targeting of nociceptors as well as of immune cells.
Acknowledgements
We thank the NIH for support (2R37NS039518).
In conclusion,�understanding the role of neurogenic inflammation when it comes to host defense and immunopathology is essential towards determining the proper treatment approach for a variety of nervous system health issues. By looking at the interactions of the peripheral neurons with immune cells, healthcare professionals may advance therapeutic approaches to further help increase host defense as well as suppress immunopathology. The purpose of the article above is to help patients understand the clinical neurophysiology of neuropathy, among other nerve injury health issues. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
1.�Sauer SK, Reeh PW, Bove GM. Noxious heat-induced CGRP release from rat sciatic nerve axons in vitro.�Eur J Neurosci.�2001;14:1203�1208.�[PubMed]
2.�Edvinsson L, Ekman R, Jansen I, McCulloch J, Uddman R. Calcitonin gene-related peptide and cerebral blood vessels: distribution and vasomotor effects.�J Cereb Blood Flow Metab.�1987;7:720�728.�[PubMed]
3.�McCormack DG, Mak JC, Coupe MO, Barnes PJ. Calcitonin gene-related peptide vasodilation of human pulmonary vessels.�J Appl Physiol.�1989;67:1265�1270.�[PubMed]
4.�Saria A. Substance P in sensory nerve fibres contributes to the development of oedema in the rat hind paw after thermal injury.�Br J Pharmacol.�1984;82:217�222.�[PMC free article]�[PubMed]
5.�Brain SD, Williams TJ. Interactions between the tachykinins and calcitonin generelated peptide lead to the modulation of oedema formation and blood flow in rat skin.�Br J Pharmacol.�1989;97:77�82.[PMC free article]�[PubMed]
6.�Fryer AD, et al. Neuronal eotaxin and the effects of CCR3 antagonist on airway hyperreactivity and M2 receptor dysfunction.�J Clin Invest.�2006;116:228�236.�[PMC free article]�[PubMed]
7.�Ansel JC, Brown JR, Payan DG, Brown MA. Substance P selectively activates TNF-alpha gene expression in murine mast cells.�J Immunol.�1993;150:4478�4485.�[PubMed]
9.�Hosoi J, et al. Regulation of Langerhans cell function by nerves containing calcitonin gene-related peptide.�Nature.�1993;363:159�163.�[PubMed]
10.�Mikami N, et al. Calcitonin gene-related peptide is an important regulator of cutaneous immunity: effect on dendritic cell and T cell functions.�J Immunol.�2011;186:6886�6893.�[PubMed]
11.�Rochlitzer S, et al. The neuropeptide calcitonin gene-related peptide affects allergic airway inflammation by modulating dendritic cell function.�Clin Exp Allergy.�2011;41:1609�1621.�[PubMed]
12.�Cyphert JM, et al. Cooperation between mast cells and neurons is essential for antigen-mediated bronchoconstriction.�J Immunol.�2009;182:7430�7439.�[PMC free article]�[PubMed]
13.�Levine JD, et al. Intraneuronal substance P contributes to the severity of experimental arthritis.�Science.�1984;226:547�549.�[PubMed]
14.�Levine JD, Khasar SG, Green PG. Neurogenic inflammation and arthritis.�Ann N Y Acad Sci.�2006;1069:155�167.�[PubMed]
15.�Engel MA, et al. TRPA1 and substance P mediate colitis in mice.�Gastroenterology.�2011;141:1346�1358.�[PubMed]
16.�Ostrowski SM, Belkadi A, Loyd CM, Diaconu D, Ward NL. Cutaneous denervation of psoriasiform mouse skin improves acanthosis and inflammation in a sensory neuropeptide-dependent manner.�J Invest Dermatol.�2011;131:1530�1538.�[PMC free article]�[PubMed]
17.�Caceres AI, et al. A sensory neuronal ion channel essential for airway inflammation and hyperreactivity in asthma.�Proc Natl Acad Sci U S A.�2009;106:9099�9104.�[PMC free article]�[PubMed]
18.�Caterina MJ, et al. Impaired nociception and pain sensation in mice lacking the capsaicin receptor.�Science.�2000;288:306�313.�[PubMed]
19.�Bessac BF, et al. Transient receptor potential ankyrin 1 antagonists block the noxious effects of toxic industrial isocyanates and tear gases.�FASEB J.�2009;23:1102�1114.�[PMC free article]�[PubMed]
20.�Cruz-Orengo L, et al. Cutaneous nociception evoked by 15-delta PGJ2 via activation of ion channel TRPA1.�Mol Pain.�2008;4:30.�[PMC free article]�[PubMed]
21.�Trevisani M, et al. 4-Hydroxynonenal, an endogenous aldehyde, causes pain and neurogenic inflammation through activation of the irritant receptor TRPA1.�Proc Natl Acad Sci U S A.�2007;104:13519�13524.�[PMC free article]�[PubMed]
22.�Janeway CA, Jr, Medzhitov R. Introduction: the role of innate immunity in the adaptive immune response.�Semin Immunol.�1998;10:349�350.�[PubMed]
23.�Matzinger P. An innate sense of danger.�Ann N Y Acad Sci.�2002;961:341�342.�[PubMed]
24.�Bianchi ME. DAMPs, PAMPs and alarmins: all we need to know about danger.�J Leukoc Biol.�2007;81:1�5.�[PubMed]
25.�Liu T, Xu ZZ, Park CK, Berta T, Ji RR. Toll-like receptor 7 mediates pruritus.�Nat Neurosci.�2010;13:1460�1462.�[PMC free article]�[PubMed]
26.�Diogenes A, Ferraz CC, Akopian AN, Henry MA, Hargreaves KM. LPS sensitizes TRPV1 via activation of TLR4 in trigeminal sensory neurons.�J Dent Res.�2011;90:759�764.�[PubMed]
27.�Qi J, et al. Painful pathways induced by TLR stimulation of dorsal root ganglion neurons.�J Immunol.�2011;186:6417�6426.�[PMC free article]�[PubMed]
28.�Cockayne DA, et al. Urinary bladder hyporeflexia and reduced pain-related behaviour in P2X3-deficient mice.�Nature.�2000;407:1011�1015.�[PubMed]
29.�Mariathasan S, et al. Cryopyrin activates the inflammasome in response to toxins and ATP.�Nature.�2006;440:228�232.�[PubMed]
30.�Souslova V, et al. Warm-coding deficits and aberrant inflammatory pain in mice lacking P2X3 receptors.�Nature.�2000;407:1015�1017.�[PubMed]
31.�de Rivero Vaccari JP, Lotocki G, Marcillo AE, Dietrich WD, Keane RW. A molecular platform in neurons regulates inflammation after spinal cord injury.�J Neurosci.�2008;28:3404�3414.�[PubMed]
32.�Link TM, et al. TRPV2 has a pivotal role in macrophage particle binding and phagocytosis.�Nat Immunol.�2010;11:232�239.�[PMC free article]�[PubMed]
33.�Turner H, del Carmen KA, Stokes A. Link between TRPV channels and mast cell function.�Handb Exp Pharmacol.�2007:457�471.�[PubMed]
34.�Binshtok AM, et al. Nociceptors are interleukin-1beta sensors.�J Neurosci.�2008;28:14062�14073.[PMC free article]�[PubMed]
35.�Zhang XC, Kainz V, Burstein R, Levy D. Tumor necrosis factor-alpha induces sensitization of meningeal nociceptors mediated via local COX and p38 MAP kinase actions.�Pain.�2011;152:140�149.[PMC free article]�[PubMed]
36.�Samad TA, et al. Interleukin-1beta-mediated induction of Cox-2 in the CNS contributes to inflammatory pain hypersensitivity.�Nature.�2001;410:471�475.�[PubMed]
37.�Veres TZ, et al. Spatial interactions between dendritic cells and sensory nerves in allergic airway inflammation.�Am J Respir Cell Mol Biol.�2007;37:553�561.�[PubMed]
38.�Smith CH, Barker JN, Morris RW, MacDonald DM, Lee TH. Neuropeptides induce rapid expression of endothelial cell adhesion molecules and elicit granulocytic infiltration in human skin.�J Immunol.�1993;151:3274�3282.�[PubMed]
39.�Dunzendorfer S, Meierhofer C, Wiedermann CJ. Signaling in neuropeptide-induced migration of human eosinophils.�J Leukoc Biol.�1998;64:828�834.�[PubMed]
40.�Ganor Y, Besser M, Ben-Zakay N, Unger T, Levite M. Human T cells express a functional ionotropic glutamate receptor GluR3, and glutamate by itself triggers integrin-mediated adhesion to laminin and fibronectin and chemotactic migration.�J Immunol.�2003;170:4362�4372.�[PubMed]
41.�Czepielewski RS, et al. Gastrin-releasing peptide receptor (GRPR) mediates chemotaxis in neutrophils.�Proc Natl Acad Sci U S A.�2011;109:547�552.�[PMC free article]�[PubMed]
42.�Brogden KA, Guthmiller JM, Salzet M, Zasloff M. The nervous system and innate immunity: the neuropeptide connection.�Nat Immunol.�2005;6:558�564.�[PubMed]
43.�Jimeno R, et al. Effect of VIP on the balance between cytokines and master regulators of activated helper T cells.�Immunol Cell Biol.�2011;90:178�186.�[PubMed]
44.�Razavi R, et al. TRPV1+ sensory neurons control beta cell stress and islet inflammation in autoimmune diabetes.�Cell.�2006;127:1123�1135.�[PubMed]
45.�Cunin P, et al. The tachykinins substance P and hemokinin-1 favor the generation of human memory Th17 cells by inducing IL-1beta, IL-23, and TNF-like 1A expression by monocytes.�J Immunol.�2011;186:4175�4182.�[PubMed]
46.�Andersson U, Tracey KJ. Reflex Principles of Immunological Homeostasis.�Annu Rev Immunol.�2011[PMC free article]�[PubMed]
47.�de Jonge WJ, et al. Stimulation of the vagus nerve attenuates macrophage activation by activating the Jak2-STAT3 signaling pathway.�Nat Immunol.�2005;6:844�851.�[PubMed]
48.�Rosas-Ballina M, et al. Acetylcholine-synthesizing T cells relay neural signals in a vagus nerve circuit.�Science.�2011;334:98�101.�[PMC free article]�[PubMed]
49.�Wang H, et al. Nicotinic acetylcholine receptor alpha7 subunit is an essential regulator of inflammation.�Nature.�2003;421:384�388.�[PubMed]
50.�Wong CH, Jenne CN, Lee WY, Leger C, Kubes P. Functional innervation of hepatic iNKT cells is immunosuppressive following stroke.�Science.�2011;334:101�105.�[PubMed]
Chiropractic Care: Tracy Ludech, club director and coach of the El Paso Diggers, expresses how much of a difference the fitness program at PUSH has done for her athletes. Working cohesively and diligently together with the staff and trainers at PUSH, Tracy Ludech has witnessed tremendous improvements in her athlete’s strength, mobility and flexibility. Tracy Ludech encourages others to experience the benefits that a fitness program can have on young athletes.
Chiropractic Care Power & Rehabilitation
Physical wellness is a condition of health and well-being and, more especially, the ability to do aspects of sport, jobs and daily activities. Physical fitness is generally accomplished through proper nourishment, moderate-vigorous physical exercise, and sufficient rest. An extensive fitness program tailored to someone normally concentrates on one or more specific skills, and on medical needs like bone health. Many sources also cite psychological, social and emotional wellbeing as an significant part overall wellbeing. Physical fitness may also prevent or treat several chronic health conditions brought on by unhealthy lifestyle or aging.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
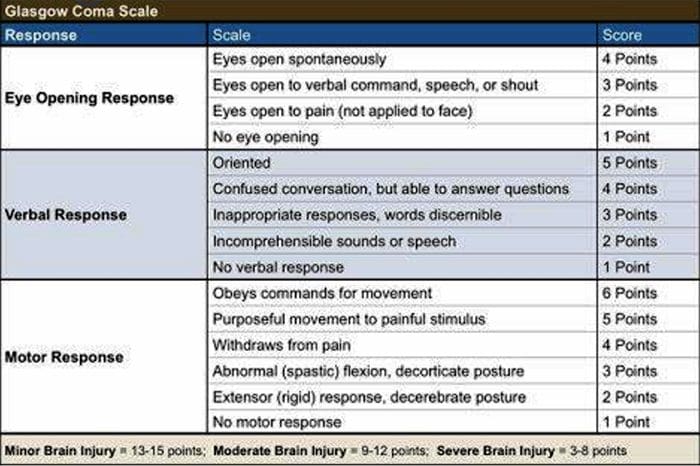
Concussions are traumatic brain injuries that affect brain function. Effects from these injuries are often temporary but can include headaches, problems with concentration, memory, balance and coordination. Concussions are usually caused by a blow to the head or violent shaking of the head and upper body. Some concussions cause loss of consciousness, but most do not. And it is possible to have a concussion and not realize it. Concussions are common in contact sports, such as football. However, most people gain a full recovery after a concussion.
Can also happen due to excessive shaking of the head or acceleration/deceleration
Mild injuries (mTBI/concussions) are the most common type of brain injury
Glasgow Coma Scale
Common Causes Of Concussion
Motor vehicle collisions
Falls
Sports injuries
Assault
Accidental or intentional discharge of weapons
Impact with objects
Prevention
Prevention of concussive injuries can be paramount
Encourage Patients To Wear Helmets
Competitive sports, especially boxing, hokey, football and baseball
Horseback riding
Riding bicycles, motorcycles, ATVs, etc.
High elevation activates such as rock climbing, zip lining
Skiing, snowboarding
Encourage Patients To Wear Seatbelts
Discuss the importance of wearing seatbelts at all times in vehicles with all of your patients
Also encourage use of appropriate booster or car seats for children to ensure adequate fit and function of seat belts.
Driving Safely
Patients should never drive while under the influence of drugs, including certain medications or alcohol
Never text and drive
Make Spaces Safer For Children
Install baby gates and window latches in the home
May in areas with shock-absorbing material, such as hardwood mulch or sand
Supervise children carefully, especially when they�re near water
Prevent Falls
Clearing tripping hazards such as loose rugs, uneven flooring or walkway clutter
Using nonslip mats in the bathtub and on shower floors, and installing grab bars next to the toilet, tub and shower
Ensure appropriate footwear
Installing handrails on both sides of stairways
Improving lighting throughout the home
Balance training exercises
Balance Training
Single leg balance
Bosu ball training
Core strengthening
Brain balancing exercises
Concussion Verbiage
Concussion vs. mTBI (mild traumatic brain injury)
mTBI is the term being used more commonly in medical settings, but concussion is a more largely recognized term in the community by sports coaches, etc.
The two terms describe the same basic thing, mTBI is a better term to use in your charting
Evaluating Concussion
Remember that there does not always have to be loss of consciousness for there to be a concussion
Post-Concussion Syndrome can occur without LOC as well
Symptoms of concussion may not be immediate and could take days to develop
Monitor for 48 post head injury watching for red flags
Blurred eyesight or other vision problems, such as dilated or uneven pupils
Confusion
Dizziness
Ringing in the ears
Nausea or vomiting
Slurred speech
Delayed response to questions
Memory loss
Fatigue
Trouble concentrating
Continued or persistent memory loss
Irritability and other personality changes
Sensitivity to light and noise
Sleep problems
Mood swings, stress, anxiety or depression
Disorders of taste and smell
Mental/Behavioral Changes
Verbal outbursts
Physical outbursts
Poor judgment
Impulsive behavior
Negativity
Intolerance
Apathy
Egocentricity
Rigidity and inflexibility
Risky behavior
Lack of empathy
Lack of motivation or initiative
Depression or anxiety
Symptoms In Children
Concussions can present differently in children
Excessive crying
Loss of appetite
Loss of interest in favorite toys or activities
Sleep issues
Vomiting
Irritability
Unsteadiness while standing
Amnesia
Memory loss and failure to form new memories
Retrograde Amnesia
Inability to remember things that happened before the injury
Due to failure in recall
Anterograde Amnesia
Inability to remember things that happened after the injury
Due to failure to formulate new memories
Even short memory losses can be predictive of outcome
Amnesia may be up to 4-10 times more predictive of symptoms and cognitive deficits following concussion than is LOC (less than 1 minute)
Return To Play Progression
Baseline: No Symptoms
As the baseline step of the Return to Play Progression, the athlete needs to have completed physical and cognitive rest and not be experiencing concussion symptoms for a minimum of 48 hours. Keep in mind, the younger the athlete, the more conservative the treatment.
Step 1: Light Aerobic Activity
The Goal: Only to increase an athlete�s heart rate.
The Time: 5 to 10 minutes.
The Activities: Exercise bike, walking, or light jogging.
Absolutely no weight lifting, jumping or hard running.
Step 2: Moderate activity
The Goal: Limited body and head movement.
The Time: Reduced from typical routine.
The Activities: Moderate jogging, brief running, moderate-intensity stationary biking, and moderate-intensity weightlifting
Step 3: Heavy, non-contact activity
The Goal: More intense but non-contact
The Time: Close to typical routine
The Activities: Running, high-intensity stationary biking, the player�s regular weightlifting routine, and non- contact sport-specific drills. This stage may add some cognitive component to practice in addition to the aerobic and movement components introduced in Steps 1 and 2.
Step 4: Practice & full contact
The Goal: Reintegrate in full contact practice.
Step 5: Competition
The Goal: Return to competition.
Microglial Priming
After head trauma microglial cells are primed and can become over active
To combat this, you must mediate the inflammation cascade
Prevent repeated head trauma
Due to priming of the foam cells, response to follow-up trauma may be far more severe and damaging
What Is Post-Concussion Syndrome (PCS)?
Symptoms following head trauma or mild traumatic brain injury, that can last weeks, months or years after injury
Symptoms persist longer than expected after initial concussion
More common in women and persons of advanced age who suffer head trauma
Severity of PCS often does not correlate to severity of head injury
PCS Symptoms
Headaches
Dizziness
Fatigue
Irritability
Anxiety
Insomnia
Loss of concentration and memory
Ringing in the ears
Blurry vision
Noise and light sensitivity
Rarely, decreases in taste and smell
Concussion Associated Risk Factors
Early symptoms of headache after injury
Mental changes such as amnesia or fogginess
Fatigue
Prior history of headaches
Evaluation Of PCS
PCS is a diagnosis of exclusion
If patient presents with symptoms after head injury, and other possible causes have been ruled out => PCS
Use appropriate testing and imaging studies to rule out other causes of symptoms
Headaches In PCS
Often �tension� type headache
Treat as you would for tension headache
Reduce stress
Improve stress coping skills
MSK treatment of the cervical and thoracic regions
Constitutional hydrotherapy
Adrenal supportive/adaptogenic herbs
Can be migraine, especially in people who had pre-existing migraine conditions prior to injury
Reduce inflammatory load
Consider management with supplements and or medications
Reduce light and sound exposure if there is sensitivity
Dizziness In PCS
After head trauma, always assess for BPPV, as this is the most common type of vertigo after trauma
Dix-Hallpike maneuver to diagnose
Epley�s maneuver for treatment
Light & Sound Sensitivity
Hypersensitivity to light and sound is common in PCS and typically exacerbates other symptoms such as headache and anxiety
Management of excess mesencephalon stimulation is crucial in such cases
Sunglasses
Other light blocking glasses
Earplugs
Cotton in ears
Treatment Of PCS
Manage each symptom individually as you otherwise would
Manage CNS inflammation
Curcumin
Boswelia
Fish oil/Omega-3s � (***after r/o bleed)
Cognitive behavioral therapy
Mindfulness & relaxation training
Acupuncture
Brain balancing physical therapy exercises
Refer for psychological evaluation/treatment
Refer to mTBI specialist
mTBI Specialists
mTBI is difficult to treat and is an entire specialty both in the allopathic and complementary medicine
Primary objective is to recognize and refer for appropriate care
Pursue training in mTBI or plan to refer to TBI specialists
Sources
�A Head for the Future.� DVBIC, 4 Apr. 2017, dvbic.dcoe.mil/aheadforthefuture.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
�Heads Up to Health Care Providers.� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 16 Feb. 2015, www.cdc.gov/headsup/providers/.
�Post-Concussion Syndrome.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 28 July 2017, www.mayoclinic.org/diseases-conditions/post- concussion-syndrome/symptoms-causes/syc-20353352.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 Why Does My Shoulder Hurt? A Review Of The Neuroanatomical & Biochemical Basis Of Shoulder Pain
Why Does My Shoulder Hurt? A Review Of The Neuroanatomical & Biochemical Basis Of Shoulder Pain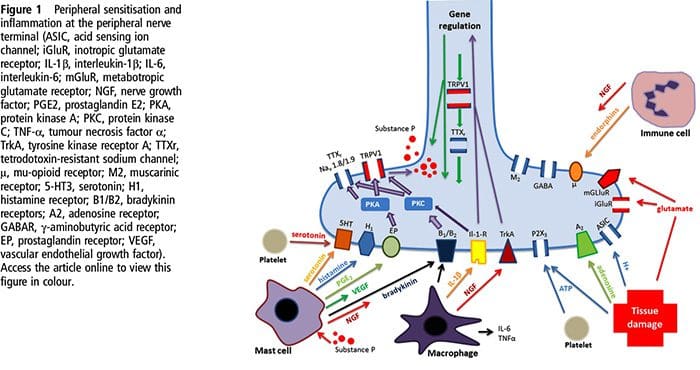 NGF and the transient receptor potential cation channel subfamily V member 1 (TRPV1) receptor have a symbiotic relationship when it comes to inflammation and nociceptor sensitization. The cytokines produced in inflamed tissue result in an increase in NGF production.19 NGF stimulates the release of histamine and serotonin (5-HT3) by mast cells, and also sensitizes nociceptors, possibly altering the properties of A? fibers such that a greater proportion become nociceptive. The TRPV1 receptor is present in a subpopulation of primary afferent fibers and is activated by capsaicin, heat and protons. The TRPV1 receptor is synthesized in the cell body of the afferent fibre, and is transported to both the peripheral and central terminals, where it contributes to the sensitivity of nociceptive afferents. Inflammation results in NGF production peripherally which then binds to the tyrosine kinase receptor type 1 receptor on the nociceptor terminals, NGF is then transported to the cell body where it leads to an up regulation of TRPV1 transcription and consequently increased nociceptor sensitivity.19 20 NGF and other inflammatory mediators also sensitize TRPV1 through a diverse array of secondary messenger pathways. Many other receptors including cholinergic receptors, ?-aminobutyric acid (GABA) receptors and somatostatin receptors are also thought to be involved in peripheral nociceptor sensitivity.
NGF and the transient receptor potential cation channel subfamily V member 1 (TRPV1) receptor have a symbiotic relationship when it comes to inflammation and nociceptor sensitization. The cytokines produced in inflamed tissue result in an increase in NGF production.19 NGF stimulates the release of histamine and serotonin (5-HT3) by mast cells, and also sensitizes nociceptors, possibly altering the properties of A? fibers such that a greater proportion become nociceptive. The TRPV1 receptor is present in a subpopulation of primary afferent fibers and is activated by capsaicin, heat and protons. The TRPV1 receptor is synthesized in the cell body of the afferent fibre, and is transported to both the peripheral and central terminals, where it contributes to the sensitivity of nociceptive afferents. Inflammation results in NGF production peripherally which then binds to the tyrosine kinase receptor type 1 receptor on the nociceptor terminals, NGF is then transported to the cell body where it leads to an up regulation of TRPV1 transcription and consequently increased nociceptor sensitivity.19 20 NGF and other inflammatory mediators also sensitize TRPV1 through a diverse array of secondary messenger pathways. Many other receptors including cholinergic receptors, ?-aminobutyric acid (GABA) receptors and somatostatin receptors are also thought to be involved in peripheral nociceptor sensitivity.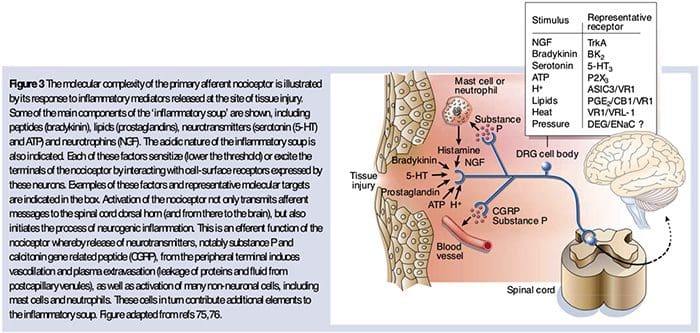 The Neurochemistry Of Nociceptors
The Neurochemistry Of Nociceptors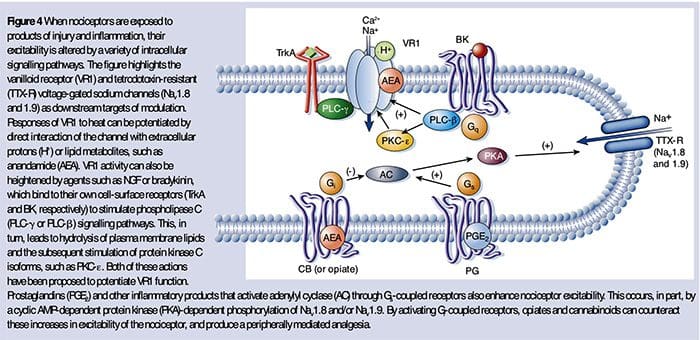 Cellular & Molecular Mechanisms Of Pain
Cellular & Molecular Mechanisms Of Pain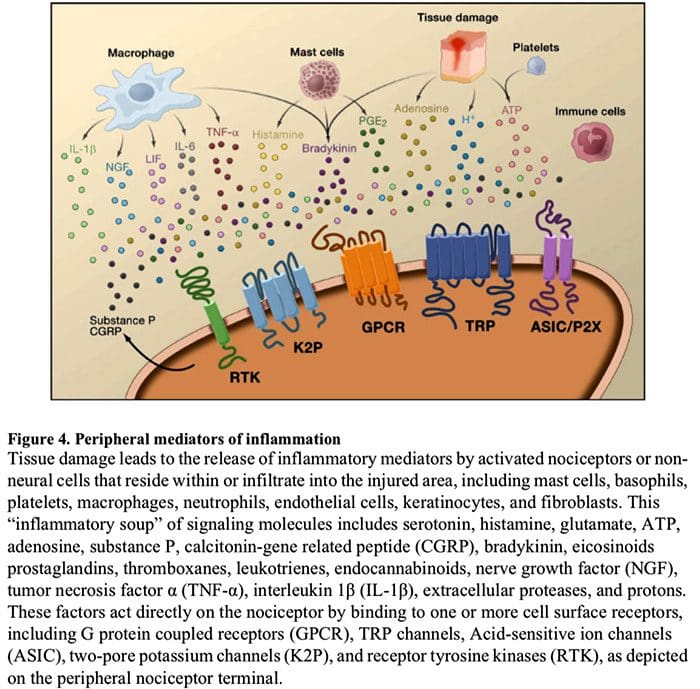
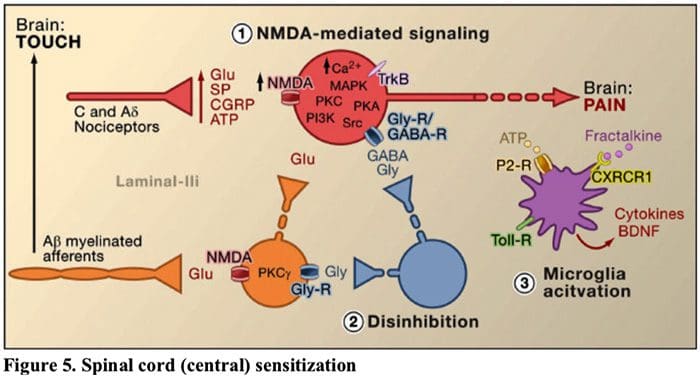 Figure 5. Spinal Cord (Central) Sensitization
Figure 5. Spinal Cord (Central) Sensitization