Biocentrism is the ethical perspective with the moral standing or holding that all life deserves equal, ethical consideration and value. Although components of biocentrism can be discovered in spiritual traditions, it was not until the late decades of the 20th century�that the topic was dealt with by philosophical ethics in the Western tradition in a systematic method.
As a normative theory, biocentrism has practical implications for human behaviour. The good of all living beings generates responsibilities on the part of human beings.
Biocentrism may best be viewed as a means with which to follow and not as a set of rules to approach life. Approaching any and every living being with awe and humility can help to make life more purposeful, and it is in this manner that with which humans interact with other beings. Biocentric ethics can help to develop a group of attitudes and habits.
Biocentrism and Chiropractic Perspective
Following a biocentric ideal, in order for humans to achieve overall health and wellness, healthcare professionals and specialists have discussed the importance of maintaining and caring for the well-being of all living organisms which can be found within the human body, including microorganisms like bacteria. One natural medicine option is available to help safely and effective treat the body, much like the biocentrism belief: chiropractic care.
Chiropractic care, involving manual manipulations and spinal adjustments, can naturally provide relief from bodily pain and symptoms of bigger problems at hand, however, it’s crucial to understand that chiropractic doesn’t aim to become a cure for any one illness, disease, or health condition. Rather, chiropractic helps ease these by bringing the body back into balance, alignment, and stability. Chiropractic allows the body to naturally heal itself.
Chiropractors believe that when your system is aligned from adjustment methods, it has a greater prospect of recovering and repairing itself from the inside out. This may indirectly treat issues impacting a patient, while also preventing potential health concerns from taking hold too. Studies have shown that a manipulation of the spinal column can help to reduce inflammation and stress as well as help boost a person’s disposition, regulate sleep cycles, and also stabilize blood pressure levels. These effects often add up to bring relief from more serious health conditions, such as diabetes. In this way, chiropractic does not treat the issue, but it helps the body combat it naturally.
In order to comprehend how the body is really helped by this kind of care, it’s important to understand the parts of the body it benefits, such as the brain and spine. When you think about it, the spine is the base of our bodies, as it’s in charge of carrying out many of the body’s important functions. Primarily, it keeps us vertical and gives us both equilibrium and stability. It is also a part of the nervous system, which is the human body’s communication center. The central nervous system as a whole, sends and receives messages all over the body, and its wellness determines body functions. Though you might immediately understand its importance, much like biocentrism, the ethical perspective that all life deserves equal moral consideration or has equal moral standing, the health and wellness of the spine is linked to the entire body, which is exactly what makes its general well-being so crucial to a lot of structures and functions.
Involving Biocentrism with Nutrition
Chiropractic is based on the premise that the body is able to achieve and maintain health through its own natural recuperative powers, provided it has a properly functioning nervous system which also receives the essential health care elements. These components include sufficient nourishment, water, rest, exercise and a clean atmosphere. Through a biocentric ideal, the human body can continue maintaining a healthy system by taking care of the microorganisms, such as the bacteria found in our gut, as well as the plants and animals which we consume. Biocentrism also involves taking care of the environment. A healthy environment can ensure humans are consuming healthy organisms as well.
The body consists of two synergistic elements that have to function at optimal for health. Issues in the biomechanical component, comprising joints, tendons, ligaments and bones controlled by the nervous system, can be handled by the chiropractic care, therapy and rehabilitation. Problems in the biochemical component, consisting of the organs with all of their functions and also controlled by the nervous system, are best addressed by nutrition, which includes food, water and supplements. As you can’t function without impacting the other, it is important to address both elements. With knowledge of nutrition and the ability to help individuals, individuals can begin to follow more biocentric ideals in order to make better decisions and to support the health of their own bodies.
Many chiropractors believe that their patients must accept responsibility for their wellness and well-being. Consequently, DCs, or doctors of chiropractic, provide exercise recommendations, dietary guidance, health-risk avoidance advice and wellness counseling. Chiropractors are often active in public health efforts to improve the well-being of individuals.
“All good health starts with the gut. A lack of gut health leads to more musculoskeletal issues. Sixty to 70 percent of our immune cells are in our gut,” stated Dr. Silverman, DC. His therapy revolves around changing patients’ lifestyles, making them more active and putting them on a suitable dietary plan. “It is important to indicate a healthy diet plan to keep a healthy nutrient supply to help the body with natural purpose and recovery procedures,” concluded Dr. Silverman.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most common symptoms reported among the general population. While back pain can occur due to a variety of injuries and/or underlying conditions, a work accident has often been associated as a frequent origin of back pain issues. Back pain can affect an individual at least once throughout their lifetime. Fortunately, federal employees who experience back pain, such as symptoms of sciatica, can benefit from programs like FECA.
Federal employees that are injured at work do not get benefits through workers’ comp insurance or their nation’s workers’ comp program.
Instead, federal employees receive workers’ compensation benefits through the Federal Employees Compensation Act, abbreviated as FECA, except for railroad workers, longshoremen, black lung coal miners, and refuge workers (that are insured under their own national laws for workers’ compensation). Members of the USA armed forces are also not considered federal employees for purposes of FECA.
FECA provides benefits and injury compensation for workers injured on the job, or even if their injury happened during the course and scope of their employment offsite. FECA covers both injuries and occupational diseases that arise over time work conditions. The United States Department of Labor, through the Office of Worker Compensation Programs, administers the workers’ comp benefits provided by the Federal Employees Compensation Act.
Qualifications
Coverage under FECA, or the Federal Employees Compensation Act, is supplied to all national government employees regardless of the number of years of service, nature of the position, or kind of job they perform. In order to be covered by FECA, you must be employed by the federal government, not a private government contractor. If you are currently working for a private business, the workers’ compensation laws in the state will cover you.
For the injury or illness to qualify under FECA, then you must have become injured while performing duties of your job or you developed a disease because of the conditions and hazards inherent in your job. This may consist of accidents occurring while working or traveling offsite as well.
FECA does not cover injuries and diseases that arise because of activities beyond the “course and scope of your employment.” Activities beyond the course and scope of employment include commuting to and from work, recreational excursions, and activities for private reasons. Injuries sustained while intoxicated or under the influence of non-prescription drugs will not be covered by the Federal Employees Compensation Act. FECA also provides benefits to surviving family members for employees that die on the job while performing work-related pursuits.
Back Pain in Federal Employees
As with anyone experiencing symptoms of back pain after being involved in a work accident, due to aggravated conditions or illness, or simply from wear-and-tear injuries, it’s essential for federal employees to seek the proper care and benefits for their symptoms to receive immediate medical attention. Spine issues resulting in sciatica can be debilitating and may affect an employee’s capability to work. Programs for federal employees like FECA may help substantially improve an individual’s overall health and wellness, allowing them to return to work as soon as possible.
FECA Workers’ Compensation Benefits
If your FECA workers’ compensation claim is permitted, you will start to receive workers’ compensation benefits to compensate you for your injury or illness and help you with the recovery. First, FECA will cover all necessary and appropriate claim-related medical therapy. This includes prescriptions, surgery and rehabilitation.
The Federal Employees Compensation Act provides compensation if a worker is disabled and unable to work as a result of industrial injury or occupational disease. You will be compensated by your service directly for your lost wages and more. Should your inability to work exceed 45 days, FECA will cover your wages that are lost.
If your workers’ compensation claim is based on an occupational disease, you’re entitled to compensation for lost salary from FECA after an initial three-day waiting period.
If your injury or illness results in permanent partial disability or permanent total disability, FECA will provide advantages and additional benefits. The total amount of the compensation is based on the severity of your permanent disability and the effect it has on your earning capacity. And if you have dependents, you will probably receive increased permanent disability compensation to account for your own requirement to supply for those dependents.
In the event that you need job retraining to return to the workforce after your injury or illness FECA provides compensation. Dependents are eligible to receive survivor’s benefits. For further details regarding the benefits of the Federal Employees Compansation Act, visit the�Division of Federal Employees’ Compensation (DFEC).
Speak to an Attorney
If your FECA employees’ compensation claim is refused, your claim may be more complicated, or your injury may have been considered more severe. You should carefully consider speaking to a lawyer in your area experienced in FECA employees’ compensation law. Although an attorney isn’t necessary to obtain workers’ compensation benefits, an attorney can help in ensuring you get all of the benefits you’re entitled to get, guiding you through the procedure.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Back pain is one of the most common symptoms reported among the general population. While back pain can occur due to a variety of injuries and/or underlying conditions, a work accident has often been associated as a frequent origin of back pain issues. Back pain can affect an individual at least once throughout their lifetime. Fortunately, federal employees who experience back pain, such as symptoms of sciatica, can benefit from programs like FECA.
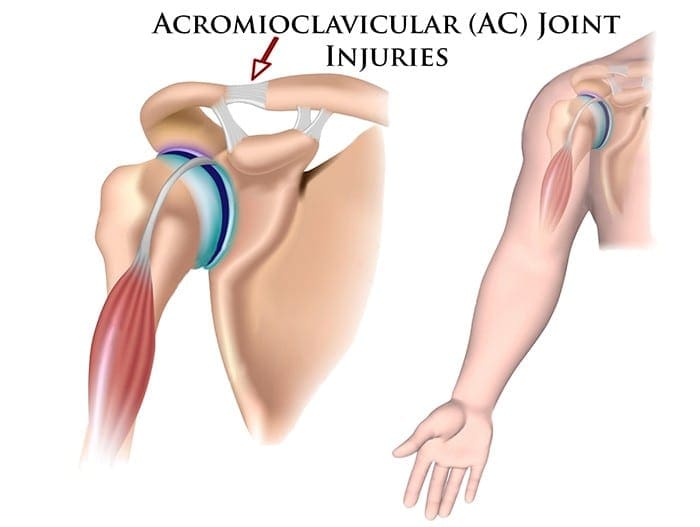
Two surgeons discuss the diagnosis and treatment of acromioclavicular injuries in athletes. El Paso, TX. Chiropractor, Dr. Alexander Jimenez follows the discussion.
Acromioclavicular (AC) joint injuries most often occur in athletic young adults involved in collision sports, throwing sports, along with overhead activities like upper-extremity strength training. They account for 3% of all shoulder injuries and 40% of shoulder sports injuries. Athletes in their second and third decade of life are more often affected(1), and men are injured more commonly than women (5:1 to 10:1)(1,2).
Acromioclavicular dislocation was known as early as 400 BC by Hippocrates(3). He cautioned against mistaking it for glenohumeral (shoulder joint) dislocation and advocated treating with a compressive bandage in an attempt to hold the distal (outer) end of the clavicle in a diminished position. Almost 600 decades later Galen (129 AD) recognized his own acromioclavicular dislocation, which he sustained while wrestling(3). He left the tight bandage holding the clavicle down as it was too uneasy. In today’s era this injury is better known, but its treatment remains a source of fantastic controversy.
Anatomy
The acromioclavicular joint combines the collarbone to the shoulder blade and therefore links the arm to the axial skeleton. The articular surfaces are originally hyaline cartilage, which affects to fibrocartilage toward the end of adolescence. The average joint size is 9mm by 19mm(4). The acromioclavicular joint contains an intra-articular, fibrocartilaginous disc which may be complete or partial (meniscoid). This helps absorb forces in compression. There is marked variability in the plane of the joint.
Stabilizers
There is little inherent bony stability in the AC joint. Stability is provided by the dynamic stabilizers — namely, the anterior deltoid muscle arising from the clavicle and the trapezius muscle arising from the acromion.
Additionally, there are ligamentous stabilizers. The AC ligaments are divided into four — superior, inferior, anterior and posterior. The superior is most powerful and blends with muscles. The acromioclavicular ligaments contribute around two- thirds of the constraining force to superior and posterior displacement; however, with greater displacement the coracoclavicular ligaments contribute the major share of the resistance. The coracoclavicular ligament consists of the conoid and trapezoid. The conoid ligament is fan-shaped and resists forwards motion of the scapula, while the more powerful trapezoid ligament is level and resists backward movement. The coracoclavicular ligament helps bunch scapular and glenohumeral (shoulder joint) motion and the interspace averages 1.3 cm.
Mechanism Of Injury
The athlete who sustains an acromioclavicular injury commonly reports either one of two mechanisms of harm: direct or indirect.
Direct force: This is when the athlete falls onto the point of the shoulder, with the arm usually at the side and adducted. The force drives the acromion downwards and medially. Nielsen(5) found that 70 percent of acromioclavicular joint injuries are caused by an direct injury.
Indirect force: This is when the athlete falls onto an outstretched arm. The pressure is transmitted via the humeral head into the acromion, therefore the acromioclavicular ligament is disrupted and the coracoclavicular ligament is stretched.
On Examination
The athlete presents soon after the severe injury with his arm splinted to his side. The patient may state that the arm feels better using superiorly directed support on the arm. Most motions are limited secondary to pain near the top of the shoulder; the degree varies with the grade of sprain. The hallmark finding is localized swelling and tenderness over the acromioclavicular joint.
In dislocations, the outer part of the collarbone will appear superiorly displaced using a noticeable step deformity (in fact, it is the shoulder which sags beneath the clavicle). Occasionally, the deformity may only be apparent later, if first muscle spasm reduces acromioclavicular separation. Forced cross-body adduction (yanking the affected arm across the opposite shoulder) provokes discomfort. The clavicle can frequently be moved relative to the acromion.
Acromioclavicular Visualisation
The typical joint width measures 1-3mm. It’s regarded as abnormal if it is more than 7mm in men, and 6mm in women. Routine anteroposterior views of the shoulder reveal the glenohumeral jointnonetheless, that the acromioclavicular joint is over penetrated and so dark to interpret. Reduced exposure enhances visualization. The individual stands with both arms hanging unsupported, both acromioclavicular joints on one film. Weighted viewpoints (stress X-rays) are obtained with 10-15 lb weights not held but suspended from the individual’s wrists. They help differentiate type II-III injuries, but are of little clinical significance and therefore are no longer recommended in our practice.
Classification Of AC Separation
The importance of identifying the injury kind can’t be over emphasized because the treatment and prognosis hinge on an accurate diagnosis. The injuries are graded on the basis of that ligaments are injured and how badly they’re torn.
Allman (6) classified acromioclavicular sprains as grades I, II and III, representing respectively, no involvement, partial tearing, and total disruption of the coracoclavicular ligaments. More recently, Rockwood (1) has further classified the more severe injuries as standard III-VI.
The injuries are classified into six categories:
Type I This is the most common injury encountered. Only a mild force is needed to sustain such an injury. The acromioclavicular ligament is sprained with an intact coracoclavicular ligament. The acromioclavicular joint remains stable and symptoms resolve in seven to 10 days. This injury has an excellent prognosis.
Type II The coracoclavicular ligaments are sprained; however, the acromioclavicular ligaments are ruptured. Most players can return to their sport within three weeks. There is anecdotal evidence to suggest that steroid injections into the acromioclavicular joint speed up the resolution of symptoms, but this practice is not universal.
Type III The acromioclavicular joint capsule and coracoclavicular ligaments are completely disrupted. The coracoclavicular interspace is 25-100% greater than the normal shoulder.
Type IV This is a type III injury with avulsion of the coracoclavicular ligament from the clavicle, with the distal clavicle displaced posteriorly into or through the trapezius.
Type V This is type III but with exaggeration of the vertical displacement of the clavicle from the scapula-coracoclavicular interspace 100-300% greater than the normal side, with the clavicle in a subcutaneous position.
Type VI This is a rare injury. This is type III with inferior dislocation of the lateral end of the clavicle below the coracoid
Treatment
The treatment of acromioclavicular joint injuries varies based on the seriousness or grade of the injury.
Initial treatment: These can be quite painful injuries. Ice packs, anti-inflammatories plus a sling are utilized to immobilize the shoulder and then take the weight of the arm. As pain starts to subside, it is important to start moving the fingers, wrist and elbow to prevent shoulder stiffness. Next, it’s important to begin shoulder motion in order to stop shoulder stiffness.
Un-displaced injuries only require rest, ice, and then a slow return to activity over two to six weeks. Major dislocations require surgical stabilization in athletes if their dominant arm is involved, and if they participate in upper-limb sports
Type I & II: Ice pack, anti-inflammatory agents and a sling are used. Early motion based on symptoms is introduced. Pain usually subsides in about 10 days. Range-of-motion exercises and strength training to restore normal motion and strength are instituted as the patient�s symptoms permit. Some symptoms may be relieved by taping (taking stress off acromioclavicular joint). The length of time needed to regain full motion and function depends upon the severity or grade of the injury. The sport and the position played determine when a player can return to a sporting activity. A football player, who does not have to elevate his arm, can return sooner than a tennis or rugby player. When a patient returns to practice and competition in collision sports, protection of the acromioclavicular joint with special padding is important. A simple �doughnut� cut from foam or felt padding can provide effective protection. Special shoulder- injury pads, or off-the-shelf shoulder orthoses, can be used to protect the acromioclavicular joint after injury.
Some Type II injuries may develop late degenerative joint changes and will need a resection of the distal end of the clavicle for pain relief. It is important to note that after a resection of the distal end of the clavicle, particularly in a throwing athlete, there may be formation of heterotopic bone on the under surface of the clavicle which can cause a painful syndrome which presents like shoulder impingement.
Type III: The treatment of type III injury is less controversial than in past years. In the 1970s, most orthopaedic surgeons recommended surgery for type III acromioclavicular sprains(7). By 1991, most type III injuries were treated conservatively(8). This change in treatment philosophy was prompted by a series of retrospective studies(9). These showed no outcome differences between operative and nonoperative groups.
What’s more, the patients treated non-operatively returned to full activity (work or athletics) earlier than surgically treated groups(10, 11). The exceptions to this recommendation include people who perform repetitive, heavy lifting, people who operate with their arms above 90 degrees, and thin patients who have prominent lateral ends of the clavicles. These patients may benefit from surgical repair(12).
Any discussion about the management of acute injuries to the AC joint must deal with which of the many methods of surgical therapy described is the best for their situation, but whether surgery should be considered at all. Surgery is generally avoided in athletes participating in contact sports since they will often re-injure the shoulder later on.
Type IV-VI: Account for more than 10-15% of total acromioclavicular dislocations and should be managed surgically. Failure to reduce and fix these will lead to chronic pain and dysfunction.
Surgery
Surgical repair can be divided into anatomical or non- anatomical, or historically into four types:
? Coracoclavicular repairs (Bosworth screws(13), cerclage, Copeland and Kessel repair).
? Distal clavicular excision.
? Dynamic muscle transfers.
? Disadvantages of surgery are that there are risks of infection, a longer time to return to full function and continued pain in some cases.
For the individual with a chronic AC joint dislocation or subluxation that remains painful after three to six months of closed treatment and rehabilitation, surgery is indicated to improve functioning and comfort.
For sequelae of untreated type IV-VI, or painful type II and III injuries, the Weaver Dunn technique is advocated. This�entails removing the lateral 2cm of the clavicle and reattaching the acromial end of the coracoacromial ligament to the cut end of the clavicle, thus reducing the clavicle to a more anatomical position.
Postoperatively, the arm is supported in a sling for up to six weeks. Following the first two weeks, the patient is permitted to use the arm for daily activities at waist level. After six weeks, the sling or orthosis is discontinued, overhead actions are allowed, formal passive stretching is instituted, and light stretching using elastic straps is initiated. Stretching and strengthening are begun slowly and gradually. The athlete shouldn’t return to their sport without restriction until full strength and range of motion has been recovered. This usually occurs four to six months following operation.
Conclusion
AC joint injuries are an important source of pain at the shoulder area and have to be assessed carefully. The management of these injuries is nonoperative in the majority of cases. Type I and II injuries are treated symptomatically. The present trend in uncomplicated type III injuries are a non operative strategy. In the event the athlete develops following problems, a delayed reconstruction might be undertaken. In athletes involved in heavy lifting or prolonged overhead activities, surgery may be considered acutely. Type IV-VI injuries are generally treated operatively.
No matter what kind of treatment is chosen, the ultimate purpose is to restore painless function to the wounded AC joint so as to reunite the athlete safely and as quickly as possible back to their sport. It is possible in the vast majority of acromioclavicular joint injuries.
References
Reza Jenabzadeh and Fares Haddad
1. Rockwood CA Jr, Williams GR, Young CD. Injuries of the Acromioclavicular Joint. In CA Rockwood Jr, et al (eds), Fractures in Adults. Philadelphia: Lippincott-Raven, 1996; 1341-1431.
2. Dias JJ, Greg PJ. Acromioclavicular Joint Injuries in Sport: Recommendations for Treatment. Sports Medicine 1991; 11: 125-32.
3. Adams FL. The Genuine Works of Hippocrates (Vols 1,2). New York, William Wood 1886.
4. Bosworth BM. Complete Acromioclavicular Dislocation. N Eng J Med 2 41: 221-225,1949.
5. Nielsen WB. Injury to the Acromioclavicular Joint. J Bone Joint Surg 1963; 45B:434-9.
6. Allman FL Jr. Fractures and Ligamentous Injuries of the Clavicle and its Articulation. J Bone Joint Surg Am 1967;
49:774- 784.
7. Powers JA, Bach PJ: Acromioclavicular Separations: Closed or Open Treatment? Clin Orthop 1974; 104 (Oct): 213-223
8. Cox JS: Current Methods of Treatment of Acromioclavicular Joint Dislocations. Orthopaedics 1992; 15(9): 1041-1044
9. Clarke HD, Mc Cann PD: Acromioclavicular Joint Injuries. Orthop Clin North Am 2000; 31(2): 177-187
10. Press J, Zuckerman JD, Gallagher M, et al: Treatment of Grade III Acromioclavicular Separations: Operative versus
Nonoperative Management. Bull Hosp Jt Dis 1997;56(2):77-83
11. Galpin RD, Hawkins RJ, Grainger RW: A Comparative Analysis of Operative versus Nonoperative Treatment of Grade III Acromioclavicular Separations. Clin Orthop 1985; 193 (Mar): 150-155
12. Larsen E, Bjerg-Nielsen A, Christensen P: Conservative or Surgical Treatment of AC Dislocation: A Prospective, Controlled, Randomized Study. J Bone Joint Surg Am 1986;68(4):552-555
13. Bosworth BM. Complete Acromioclavicular Dislocation. N Engl. J. Med. 241: 221-225,1949.
Return to play describes the stage in recovery from a sports injury when an athlete is able to go back to playing sports or participate in their specific physical activity at a pre-injury level.
Nobody likes to be sidelined with an undesired injury. Among the goals of sports medicine professionals and specialists is to try to restore an athlete back to action. Returning too soon, however before restoration or healing has taken place, can put an athlete at an increased risk for re-injury and down time.
With the ideal treatment and care plan for sport accidents and injury, from early identification and proper treatment to full functional rehabilitation, you can often safely accelerate your return to perform.
Lessons from Professional Athletes
Why does it seem that professional athletes come back to play so much quicker than the normal person or athlete? Professional athletes are often, at the time of injury, in tremendously good physical conditioning. This fitness level helps them in various ways. Various studies have demonstrated that conditioning the body properly can not only prevent injuries, it may also lessen the severity of an injury and speed up recovery.
Professional athletes also get prompt treatment once an injury happens, and this lessens the acute phase of the injury. Treatment and care is required as soon as an injury followed by symptoms such as, stiffness, swelling, and loss of muscle tone manifest. In addition, professional athletes work hard with a physical therapist or certified athletic trainer.
Many professional athletes contribute their healing to exactly what they bring to their game,a positive attitude. You are able to harness the power of a positive mindset to your own benefit, even though you may not have access to the tools that professional athletes possess.
Advice from the Pros to Boost Your Recovery
Maintain balanced physical conditioning
Make Sure injuries are recognized early and treated promptly
Participate in a complete functional rehabilitation program
Stay healthy while injured
Keep a positive, upbeat mental attitude
Proper Athletic Treatment Recovery Plan
Phases of Care
Recovery from an injury involves a set of logical steps from the time of the injury until you are able to return on the field or court. Every step should be summarized and monitored by your physician and therapist.
During the acute phase of injury, the focus should be on minimizing swelling. This entails the RICE formula (Rest, Ice, Compression, and Elevation), Together with a limitation of actions. Based on the type and severity of your injury, treatment may involve casting, or bracing and surgery in more serious cases.
During the acute period, it’s extremely important to keep overall conditioning while the injury heals. Creative techniques may be used to safely work around the injury. As an example, a runner with a leg injury may often run in plain water or use a bicycle to keep conditioning. By doing exercises if one leg is in a cast, the remainder of the human body can be exercised. Don’t wait till your injury is treated to get back into shape.
In another phase of recovery, you should focus on regaining full motion and strength of the injured limb or joint. Your doctor, physical therapist or certified athletic trainer will help outline an exact treatment plan. For injuries, gentle protective exercises can be started almost immediately. Muscle tone may be preserved by means of strengthening exercises or electric stimulation.
When strength returns to normal, functional drills could be started. For lower extremity injuries, this may include brisk walking, jumping rope, hopping, or light jogging. For upper extremity injuries, effortless ground strokes or light throwing could be carried out. The coordination that might have been lost in the injury can be brought back by specific exercises for agility and balance.
Once you have progressed with mobility, endurance, strength, and agility, and are tolerating functional exercises, you can try higher levels of sport-specific movement routines. Your physical therapist or certified athletic trainer monitors this. You could find that tape, braces, or supports help in this transition time.
Only when you are practicing hard without significant problem, and the healing has progressed to the point at which the probability of injury or harm is reduced, are you ready to return to play. During these phases of recovery, you ought to be carefully monitored. Special attention ought to be given to sufficient warm up following the activity prior to the activity and icing after engaging in the specific sport or physical activity.
Note Of Caution
The rational progression of recovery not only reduces the chance of re-injury but also assures that you will be able to perform at your best when you return to play. Frequently, athletes believe they are all set to return as soon as the limp or even the swelling subsides. They might feel good, but they are probably just 70 to 75% recovered. This invites re-injury.
Sports medicine experts are working on approaches to assist athletes to achieve near 100% healing as fast as the proper cautionary measures allows. The athlete’s health and safety has to be put over all other concerns, although there is enormous pressure to get the athlete back whenever possible.
A systematic recovery program has been successfully utilized every day, at all levels of play, from the recreational athlete to the elite professional or Olympic athlete, by a variety of specialized healthcare professionals. As with any type of sports injury, seek immediate medical attention from a qualified specialist to begin the rehabilitation process.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
BFR or blood flow restriction therapy has been around for a long time, but recently, the evidence for its use in the world that is rehabilitation has begun to emerge. The principle is very simple: that the circulation of blood flow is confined to the area of the human body that’s being trained or undergoing rehabilitation in a certain manner to boost the impacts of the training via lower load (less stress).
Is Blood Flow Restriction Effective?
According to the American College of Sports Medicine, to achieve an increase in muscle size and strength, you want to do 8 to 10 repetitions of an exercise. A moderate to high intensity is deemed to be 65 to 80 percent of their patient’s one rep maximum (the maximum amount of weight a person can lift 1 time). However, the majority of patients that are injured can’t deal with this kind of load, consequently restricting their capacity.
So again we’re faced with the question: Just how can we achieve hypertrophy and gain muscle strength without using heavy loads? The solution involves using a tourniquet to restrict blood flow into a muscle. This technique is known as blood flow restriction training (BFR).
According to the most recent research in the event the appropriate blood flow restriction therapy protocols are utilized, the benefits of the training are equal to those found when using 70 percent of an individual’s maximal load, while using as little as 20 to 30 percent of somebody’s maximum load. The secret is that restricted blood flow training allows healthcare professionals, such as physical therapists, to make a localized region of exercise that is anaerobic.
BFR is a tool that uses a doppler and tourniquet system placed on either thigh or the upper arm to limit blood circulation. After this, it begins to create lactate and hydrogen ions and denies the muscle oxygen. This is what causes the “burning” feeling when we lift heavy weights. The burn is simply the response to being in an active environment of the body. During heavy lifting (65-85%), we create small microtraumas in the muscle that the body then repairs by building more muscle. Together with BFR, we are not generating microtraumas at the muscle, so our body does not have to devote the energy to repair the muscle; rather our bodies just focus on creating the muscle.
Second, soreness is not experienced by us as we would when we were lifting weights. This means we can now lift at low loads (15-30%) and basically gain more muscle strength and size, at a quicker manner, as if we were lifting a more heavier load.
As soon as we create lactate, we activate growth hormone release. The release of IGF-1 subsequently stimulates once growth hormone is released. Such enables your muscles ability to activate; this in turn increases muscle protein synthesis, or our stem cells to the muscle. As previously mentioned, if we were to have muscle breakdown, these stem cells could have to concentrate on repairing muscles building. With blood flow restriction therapy or training, we skip the muscle repair and focus on muscle building. This result is not concentrated throughout the exercise, but impacts the tissues and muscles to create the greater benefit of BFR. BFR has shown to have the ability to help in endurance training and coaching, tendon healing and bone recovery.
All of our muscles are produced from other kinds of fibers, including type 1 which are slow to twitch and rely on oxygen and type 2, which are those we’re currently attempting to build with BFR training and fast-twitch fibers. By limiting the blood flow, we create an environment at the muscle group that compels the increase of more fibers that are type 2. Higher strength gains are the outcome because these type 2 fibers normally can produce more force. Another effect of blood flow restriction is that is allows for a synthesis of proteins needed to build and repair muscles and tissues.
In a treatment setting, this helps us achieve the outcomes for patients faster, and in sports it enables the gains to be attained with less strength and less damage to the muscle. That is why pro and college teams are currently turning to BFR as a training principle. In sports, athletes are attempting to come back to the field quicker after suffering trauma or injury from an accident. Some athletes re-injure themselves by lifting. That is really where BFR can come by lifting loads that are lower and receiving the same, or even much better profits. Healthcare specialists will tend to eliminate strength immediately following a sports injury, but they can not exercise at elevated levels. In this manner, they can not only keep the power but build strength in the process although together with blood flow restriction training.
Is Blood Flow Restriction Safe?
You might be thinking that its effects sounds fantastic, but is it safe? The brief answer is yes, but as with any rehab technique, there are precautions which should be taken and it’s recommended to first seek medical attention from a healthcare professional to discuss the option of BFR therapy for you. We certainly don’t recommend that individuals do this by themselves and tie bands around their limbs. In the practice, specialists can track it as you train and use special devices to know exactly how much you need to train to experience its benefits.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
In order to comprehend how BFR, or blood flow restriction, functions, it is important to perform a quick debriefing on how your circulatory system, also called vascular or cardiovascular system, works. Your arteries are blood vessels that carry oxygenated blood away from your heart to your body. Your veins are blood vessels that carry blood from the body back to the heart.
The objective of blood flow restriction training would be to restrict venous return while still allowing arterial flow by strategically wrapping the lightest portion of your own limbs. Blood can keep pooling to a muscle by restricting the veins rather than the arteries and it remains trapped there. It is like filling a water balloon to max capacity (with no popping up, of course).
By gathering all of the blood to the working muscles without letting it leave, a couple key things happen:�One, you receive a crazy pump and your muscles become supersized. The concept is that this contributes to cellular swelling that shocks the muscles into growth. Second, it’s gonna burn tremendously. Your muscles become deprived of oxygen and can not eliminate accumulating waste materials and this creates a great deal of acidosis or strain. Metabolic stress is just one of the three major mechanisms of muscle development and shouldn’t be dismissed.
The Science of BFR
Dr. Brad Schoenfeld is a regular contributor on hypertrophy (the scientific term for muscle growth). In his book Science and maturation of Muscle Hypertrophy, ” he states: “The prevailing body of literature shows that BFR training stimulates anabolic signaling and muscle protein synthesis and markedly increases muscle development despite using loads frequently considered too low to encourage substantial hypertrophy.” Brad goes on further, saying that “it has been speculated that metabolic stress would be the driving force behind BFR-induced muscle hypertrophy.”
Another interesting matter that occurs with blood flow restriction training is since your oxygen-dependent slow-twitch fibers fatigue way quicker than normal, you have to quickly begin tapping into the fast-twitch muscle fibers, which have the biggest potential for growth.
Interestingly enough, your fast-twitch fibers typically don’t get hit unless you’re using heavy loads or pretty hefty loads performed explosively. But BFR lets you really go fast-twitch with loads less than 50 percent of your own one-rep max. Actually, one study from the Journal of Applied Physiology revealed increased muscle cross-sectional area with BFR training using loads as light as 20 percent of one-rep maximum.
What this means for you is that with BFR training you can utilize lighter loads to construct muscle while sparing your muscles from heavy loading and without fatiguing your central nervous system. Additionally, it is important to note that research has proven the gains are not just for legs and the arms but also for muscle groups over the wraps.
How to Wrap For BFR Training
There are some high-end pressure cuffs which may be used to wrap your limbs for BFR, however any wraps will get the job done. Some people utilize knee/elbow or ace bandages wraps. Others use hospital tourniquets that are run-of-the-mill.
For your upper body, wrap it only beneath the shoulder at the top of upper arm so that the wrapping is nestling into your armpit.
For the lower body, wrap only below the gluteal fold from the back and just below the hip flexor in the front.
For both the upper and lower body, you want to wrap at about a 7 out of 10 on the tightness scale (10 being as tight as you can).
You shouldn’t feel any numbness or tingling sensations. That usually means you wrapped it tight, if you do. Wrapping it too tight will limit flow and prevent blood from pooling in the gut, so it defeats the purpose. When in doubt, wrap at first, particularly around the back side of the spectrum.
How can you know whether you wrapped it right? In the event you get your life’s muscular pump. Recall, if it feels sketchy just take off the wraps and re-wrap a tiny bit looser. There is a bit of a learning curve and thus don’t place too much stress to nail it on the first try.
How BFR Training Builds Muscle
The secret to effective BFR training is using light loads (40 to 50 percent of your one-rep maxor less), high repetitions (10 to 15 repetitions or longer), and short rest periods (30 minutes or less). In addition, it is important to note that BFR does not replace your regular training–it just enhances it. Here are my three favorite ways to execute BFR training:
BFR Finishers
After performing your main work out, hit a BFR finisher. If you completed an upper-body workout, hit an upper-body BFR finisher. If you finished a lower-body workout, hit on a BFR finisher. Hit on one for the upper and lower body if you do total-body sessions.
Extra Training Volume and Frequency
BFR is a excellent way to increase training volume (how much work you do) and coaching frequency (how often you train) without impairing your recovery. As an example, to bump up your training volume, if you did 3 routine sets of an exercise with heavier loads, try adding in an additional couple sets of BFR training to the same movement pattern or muscle group using a lighter load for higher reps and shorter rest periods between sets.
Active Recovery and Deloading
Since BFR training requires having lighter loads, it is considerably easier to recover from deeper training. This makes it a process to employ but still want to train. It’s also great to use if you integrate regular deloads–or intervals of decreased loading or training volume–into your training schedule.
It is worth mentioning that BFR is being used with remarkable success in rehabilitation settings, especially with wounded athletes. Being able to operate and develop muscles after an injury or operation with loads is a joint-sparing feature unique to BFR training. As always, consult your physician or physical therapist to find out if BFR training is right for you in such circumstances.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
Athletes face extreme pressure to return to play when they are hurt however, the true challenge for physicians is to get them back in the game safely. Athletes should be tough and maintain a positive attitude whilst regularly going through pain. When they’re made to sit out due to an accident, they should be focused and motivated to return to play as quickly as possible. They rehabilitate and rest as they trust that their bodies will ready after a full treatment plan.
This is the idealistic perspective of injury associated with athletes in their specific sport or physical activity. However, the reality is that accidents are an unavoidable by product of being an athlete and the transition from “active athlete” to “injured athlete” and back to “active athlete” does not always happen without complications.
Injured athletes fight with anxiety, frustration, anger and sometimes depression during their time away from play, which might also keep them from following their rehabilitation program effectively. Additionally, the return to the sport itself yields a fresh pair of adversities as athletes should browse through personal fears and a desire to come back to their pre-injury condition with the support of their family and healthcare physician.
Importance of Support for Injured Athletes
Social support can come from various forms, ranging from emotional support to task challenge assistance. Some wounded athletes want a caring individual simply to listen to their anxieties while others might prefer a challenging drive to work harder during rehab. Studies looking at the supply of social support have found that athletes feel most satisfied with the support provided by professionals in comparison to support supplied by teammates or coaches.
It would appear obvious that athletes would need support to assist with the injury recovery process. Because teams have access to trainers in a school setting, this additional support is possible. However, injuries are not unique to the collegiate population, which makes it important to address that �and provide this service.
Researchers who immediately addressed athletes’ tastes from healthcare professionals found that the desire to learn more concerning the injury resulted in a clearer timeline for return to play along with an open environment where athletes felt comfortable asking questions. In respect to athletes not fully understanding their injuries, they noticed that they would have appreciated the use of models and more sophisticated explanations from their physicians. It’s essential for healthcare professionals to take the time to help these athletes that are injured throughout the rehabilitation and recovery process and return to play with expertise.
Even though a complete return to play could be potential in time, it won’t happen immediately and teammates, parents, the athletes and coaches need to understand this. Trainers who have missed those who have been inactive for any period of time or numerous practices will require a slow progression back to their previous degree. This is bothersome for coaches who may “need” that athlete and also for the athlete who wants to return so as not to let the team down, trainer or themselves. Additionally, while appeasing the team and coach, the athlete may want to listen to doctors to ensure a safe recovery.
Goal-Setting to Facilitate Confidence And Motivation
Throughout the rehabilitation process, athletes should set modest goals, adjust their mindset, surround themselves with supportive people and develop their patience. It is important for others such as doctors, parents and trainers to understand the process, and provide athletes with resources and support to help them construct in these areas. Like setting rehabilitation targets that are daily followed by exercise goals, simple strategies can help athletes experience modest successes and build their own confidence.
Every injured athlete would like to return to 100 percent but it is going to take some time to reach that degree. They’re very likely to eliminate the drive and motivation to continue, if they don’t see improvements over time. The athlete has to set goals based on their current status. The athlete will see little daily improvements leading them in the path of better performances in the future.
Building and/or maintaining confidence is vital, and it cannot be connected to results. Athletes need to realize that confidence keeps them trying even if scenarios aren’t going their way, and helps them push through failures. Confidence is a way of behaving and thinking that should be evident in everything one does regardless of the outcome.
In Conclusion
Given potential effects related to harm and the emotions, it’s clear that more education is essential to guarantee positive consequences for athletes who’ve experienced sports injuries. Injuries are unavoidable but they do not need to be devastating to well-being and one’s life if handled effectively. It’s apparent that athletes encounter adversity due to the injury and due to the change for their own lives and daily routines. The recovery is sometimes more easy than the yield to perform since the bone may heal and the tear could be mended, but the brain doesn’t change as easily.
It is necessary for everyone involved to understand that helping an athlete recovery in order to return to play as soon as possible demands attention to both the body and the brain. This can be accomplished by one with awareness, education and effort of coaches, doctors, athletes and parents alike.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine