Blanca suffered from heel spurs as a result of her occupation as a registered nurse. Her painful symptoms made it challenging for her to accomplish her daily tasks, both in the workplace and in her everyday life. Due to her unbearable heel spurs, Blanca considered finding a new job until she found Dr. Alex Jimenez, doctor of chiropractic. Blanca highly recommends Dr. Alex Jimenez as the non-surgical choice for heel spurs, among other sports injuries and health issues.
Heel Spurs Treatment
A heel spur is a health issue which occurs when a bony-like expansion, known as a calcium deposit, develops between the heel arch and bone of the foot. Heel spurs frequently start in front of the heels and finally affect different elements of the foot. Indicators of heel spurs can include pain, soreness, swelling, and inflammation in the front of the foot. The affected area may also feel hot to the touch. The indicators can also spread to the back of the foot. Finally, a tiny bony protrusion could be observable if left untreated.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Knee pain is a common health issue among athletes and the general population alike. Although symptoms of knee pain can be debilitating and frustrating, knee pain is often a very treatable health issue. The knee is a complex structure made up of three bones: the lower section of the thighbone, the upper region of the shinbone, and the kneecap.
Powerful soft tissues, such as the tendons and ligaments of the knee as well as the cartilage beneath the kneecap and between the bones, hold these structures together in order to stabilize and support the knee. However, a variety of injuries and/or conditions can ultimately lead to knee pain. The purpose of the article below is to evaluate patients with knee pain.
Abstract
Family physicians frequently encounter patients with knee pain. Accurate diagnosis requires a knowledge of knee anatomy, common pain patterns in knee injuries, and features of frequently encountered causes of knee pain, as well as specific physical examination skills. The history should include characteristics of the patient�s pain, mechanical symptoms (locking, popping, giving way), joint effusion (timing, amount, recurrence), and mechanism of injury. The physical examination should include careful inspection of the knee, palpation for point tenderness, assessment of joint effusion, range-of-motion testing, evaluation of ligaments for injury or laxity, and assessment of the menisci. Radiographs should be obtained in patients with isolated patellar tenderness or tenderness at the head of the fibula, inability to bear weight or flex the knee to 90 degrees, or age greater than 55 years. (Am Fam Physician 2003; 68:907-12. Copyright� 2003 American Academy of Family Physicians.)
Introduction
Knee pain accounts for approximately one-third of musculoskeletal problems seen in primary care settings. This complaint is most prevalent in�physically active patients, with as many as 54 percent of athletes having some degree of knee pain each year.1 Knee pain can be a source of significant disability, restricting the ability to work or perform activities of daily living.
The knee is a complex structure (Figure 1),2 and its evaluation can present a challenge to the family physician. The differential diagnosis of knee pain is extensive but can be narrowed with a detailed history, a focused physical examination and, when indicated, the selective use of appropriate imaging and laboratory studies. Part I of this two-part article provides a systematic approach to evaluating the knee, and part II3 discusses the differential diagnosis of knee pain.
History
Pain Characteristics
The patient�s description of knee pain is helpful in focusing the differential diagnosis.4 It is important to clarify the characteristics of the pain, including its onset (rapid or insidious), location (anterior, medial, lateral, or posterior knee), duration, severity, and quality (e.g., dull, sharp, achy). Aggravating and alleviating factors also need to be identified. If knee pain is caused by an acute injury, the physician needs to know whether the patient was able to continue activity or bear weight after the injury or was forced to cease activities immediately.
Mechanical Symptoms
The patient should be asked about mechan- ical symptoms, such as locking, popping, or giving way of the knee. A history of locking episodes suggests a meniscal tear. A sensation of popping at the time of injury suggests liga- mentous injury, probably complete rupture of a ligament (third-degree tear). Episodes of giving way are consistent with some degree of knee instability and may indicate patellar sub- luxation or ligamentous rupture.
Effusion
The timing and amount of joint effusion are important clues to the diagnosis. Rapid onset (within two hours) of a large, tense effusion suggests rupture of the anterior cru- ciate ligament or fracture of the tibial plateau with resultant hemarthrosis, whereas slower onset (24 to 36 hours) of a mild to moderate effusion is consistent with meniscal injury or ligamentous sprain. Recurrent knee effusion after activity is consistent with meniscal injury.
Mechanism of Injury
The patient should be questioned about specific details of the injury. It is important to know if the patient sustained a direct blow to the knee, if the foot was planted at the time of injury, if the patient was decelerating or stopping suddenly, if the patient was landing from a jump, if there was a twisting component to the injury, and if hyperextension occurred.
A direct blow to the knee can cause serious injury. The anterior force applied to the proximal tibia with the knee in flexion (e.g., when the knee hits the dashboard in an automobile accident) can cause injury to the posterior cruciate ligament. The medial collateral ligament is most commonly injured as a result of direct lateral force to the knee (e.g., clipping in football); this force creates a val- gus load on the knee joint and can result in rupture of the medial collateral ligament. Conversely, a medial blow that creates a varus load can injure the lateral collateral ligament.
Noncontact forces also are an important cause of knee injury. Quick stops and sharp cuts or turns create significant deceleration forces that can sprain or rupture the anterior cruciate ligament. Hyperextension can result in injury to the anterior cruciate ligament or posterior cruciate ligament. Sudden twisting or pivoting motions create shear forces that can injure the meniscus. A combination of forces can occur simultaneously, causing injury to multiple structures.
Medical History
A history of knee injury or surgery is important. The patient should be asked about previous attempts to treat knee pain, including the use of medications, supporting devices, and physical therapy. The physician also should ask if the patient has a history of�gout, pseudogout, rheumatoid arthritis, or other degenerative joint diseases.
Knee pain is a common health issue which can be caused by sports injuries, automobile accident injuries, or by an underlying health issue, such as arthritis. The most common symptoms of knee injury include pain and discomfort, swelling, inflammation and stiffness. Because treatment for knee pain varies according to the cause, it’s essential for the individual to receive proper diagnosis for their symptoms. Chiropractic care is a safe and effective, alternative treatment approach which can help treat knee pain, among other health issues.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Physical Examination
Inspection and Palpation
The physician begins by comparing the painful knee with the asymptomatic knee and inspecting the injured knee for erythema, swelling, bruising, and discoloration. The mus- culature should be symmetric bilaterally. In particular, the vastus medialis obliquus of the quadriceps should be evaluated to determine if it appears normal or shows signs of atrophy.
The knee is then palpated and checked for pain, warmth, and effusion. Point tenderness should be sought, particularly at the patella, tibial tubercle, patellar tendon, quadriceps tendon, anterolateral and anteromedial joint line, medial joint line, and lateral joint line. Moving the patient�s knee through a short arc of motion helps identify the joint lines. Range of motion should be assessed by extending and flexing the knee as far as possible (normal range of motion: extension, zero degrees; flex- ion, 135 degrees).5
Patellofemoral Assessment
An evaluation for effusion should be conducted with the patient supine and the injured knee in extension. The suprapatellar pouch should be milked to determine whether an effusion is present.
Patellofemoral tracking is assessed by observing the patella for smooth motion while the patient contracts the quadriceps muscle. The presence of crepitus should be noted during palpation of the patella.
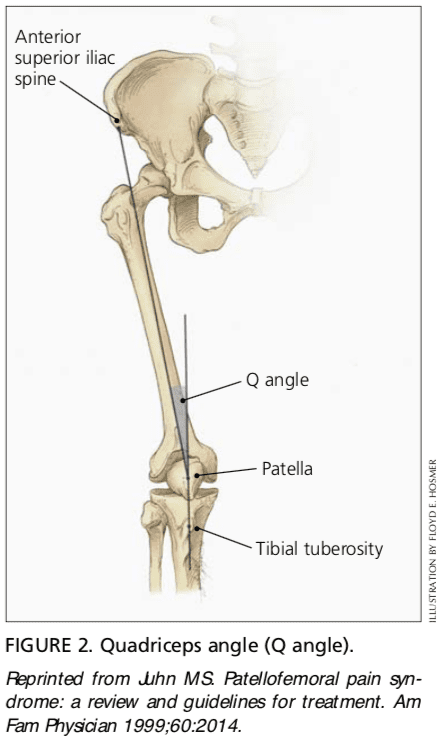
The quadriceps angle (Q angle) is determined by drawing one line from the anterior superior iliac spine through the center of the patella and a second line from the center of the patella through the tibial tuberosity (Figure 2).6 A Q angle greater than 15 degrees is a predisposing factor for patellar subluxation (i.e., if the Q angle is increased, forceful contraction of the quadriceps muscle can cause the patella to sublux laterally).
A patellar apprehension test is then performed. With fingers placed at the medial aspect of the patella, the physician attempts to sublux the patella laterally. If this maneuver reproduces the patient�s pain or a giving-way sensation, patellar subluxation is the likely cause of the patient�s symptoms.7 Both the superior and inferior patellar facets should be palpated, with the patella subluxed first medially and then laterally.
Cruciate Ligaments
Anterior Cruciate Ligament. For the anterior drawer test, the patient assumes a supine position with the injured knee flexed to 90 degrees. The physician fixes the patient�s foot in slight external rotation (by sitting on the foot) and then places thumbs at the tibial tubercle and fingers at the posterior calf. With the patient�s hamstring muscles relaxed, the physician pulls anteriorly and assesses anterior displacement of the tibia (anterior drawer sign).
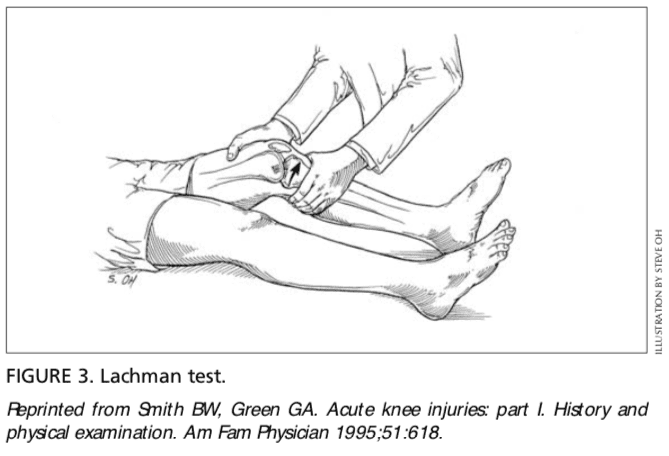
The Lachman test is another means of assessing the integrity of the anterior cruciate ligament (Figure 3).7 The test is performed with the patient in a supine position and the injured knee flexed to 30 degrees. The physician stabilizes the distal femur with one hand, grasps the proximal tibia in the other hand, and then attempts to sublux the tibia anteriorly. Lack of a clear end point indicates a positive Lachman test.
Posterior Cruciate Ligament. For the posterior drawer test, the patient assumes a supine position with knees flexed to 90 degrees. While standing at the side of the examination table, the physician looks for posterior displacement of the tibia (posterior sag sign).7,8 Next, the physician fixes the patient�s foot in neutral rotation (by sitting on the foot), positions thumbs at the tibial tubercle, and places fingers at the posterior calf. The physician then pushes posteriorly and assesses for posterior displacement of the tibia.
Collateral Ligaments
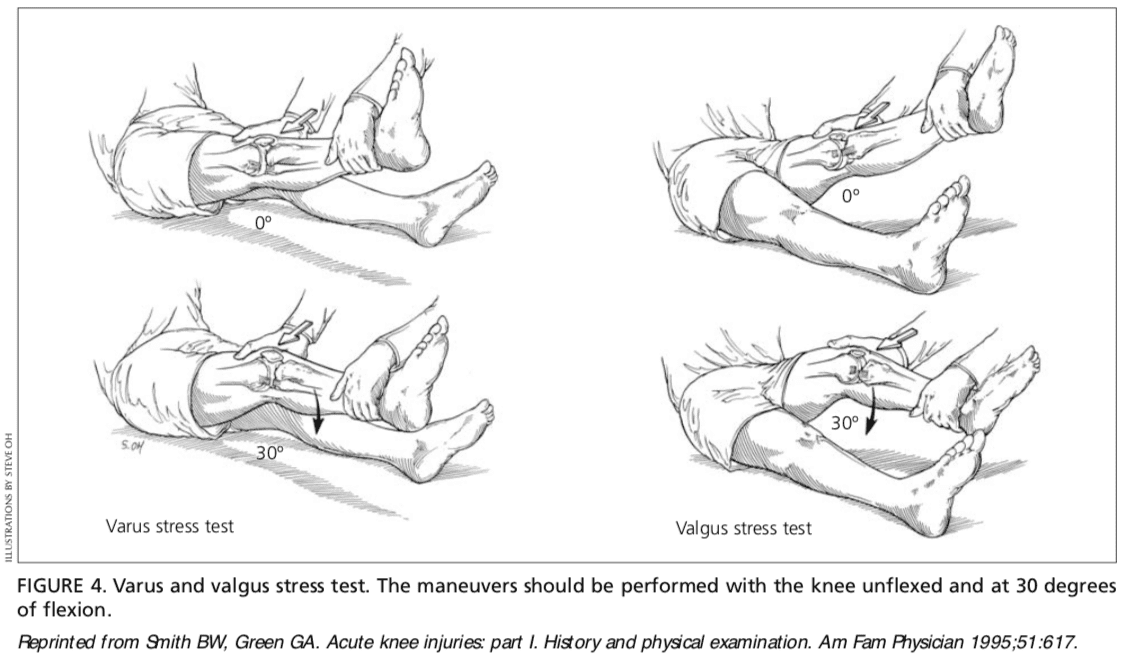
Medial Collateral Ligament. The valgus stress test is performed with the patient�s leg slightly abducted. The physician places one hand at the lateral aspect of the knee joint and the other hand at the medial aspect of the distal tibia. Next, valgus stress is applied to the knee at both zero degrees (full extension) and 30 degrees of flexion (Figure 4)7. With the knee at zero degrees (i.e., in full extension), the posterior cruciate ligament and the articulation of the femoral condyles with the tibial plateau should stabilize the knee; with the knee at 30 degrees of flexion, application of valgus stress assesses the laxity or integrity of the medial collateral ligament.
Lateral Collateral Ligament. To perform the varus stress test, the physician places one hand at the medial aspect of the patient�s knee and the other hand at the lateral aspect of the distal fibula. Next, varus stress is applied to the knee, first at full extension (i.e., zero degrees), then with the knee flexed to 30 degrees (Figure 4).7 A firm end point indicates that the collateral ligament is intact, whereas a soft or absent end point indicates complete rupture (third-degree tear) of the ligament.
Menisci
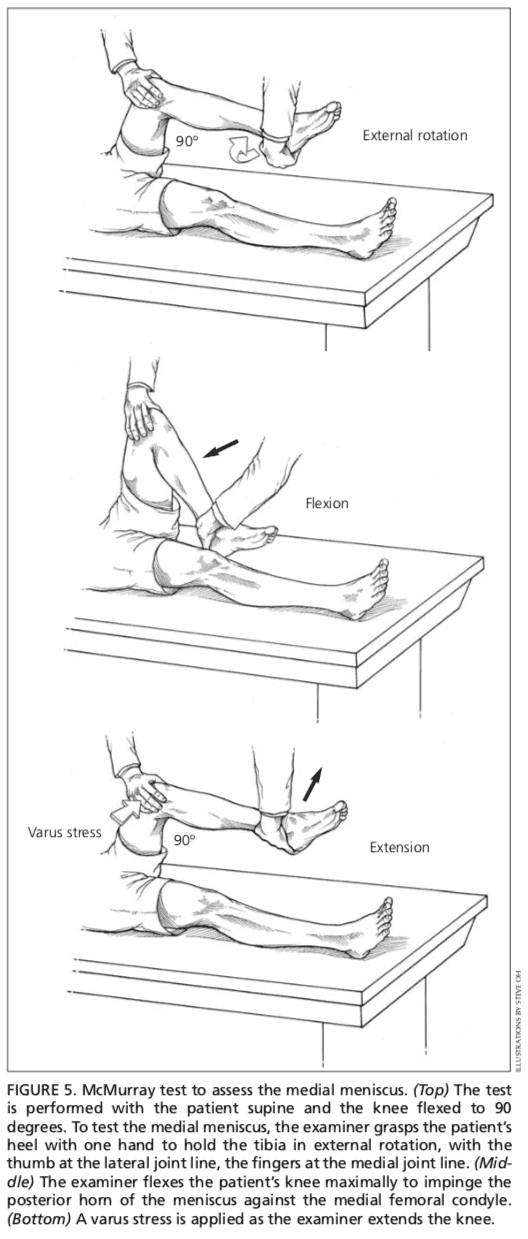
Patients with injury to the menisci usually demonstrate tenderness at the joint line. The McMurray test is performed with the patient lying supine9 (Figure 5). The test has been described variously in the literature, but the author suggests the following technique.
The physician grasps the patient�s heel with one hand and the knee with the other hand. The physician�s thumb is at the lateral joint line, and fingers are at the medial joint line. The physician then flexes the patient�s knee maximally. To test the lateral meniscus, the tibia is rotated internally, and the knee is extended from maximal flexion to about 90 degrees; added compression to the lateral meniscus can be produced by applying valgus stress across the knee joint while the knee is�being extended. To test the medial meniscus, the tibia is rotated externally, and the knee is extended from maximal flexion to about 90 degrees; added compression to the medial meniscus can be produced by placing varus stress across the knee joint while the knee is degrees of flexion. A positive test produces a thud or a click, or causes pain in a reproducible portion of the range of motion.
Because most patients with knee pain have soft tissue injuries, plain-film radiographs generally are not indicated. The Ottawa knee rules are a useful guide for ordering radiographs of the knee10,11.
If radiographs are required, three views are usually sufficient: anteroposterior view, lateral view, and Merchant�s view (for the patellofemoral joint).7,12 Teenage patients who report chronic knee pain and recurrent knee effusion require a notch or tunnel view (posteroanterior view with the knee flexed to 40 to 50 degrees). This view is necessary to detect radiolucencies of the femoral condyles (most�commonly the medial femoral condyle), which indicate the presence of osteochondritis dissecans.13
Radiographs should be closely inspected for signs of fracture, particularly involving the patella, tibial plateau, tibial spines, proximal fibula, and femoral condyles. If osteoarthritis is suspected, standing weight-bearing radiographs should be obtained.
Laboratory Studies
The presence of warmth, exquisite tenderness, painful effusion, and marked pain with even slight range of motion of the knee joint is consistent with septic arthritis or acute inflammatory arthropathy. In addition to obtaining a complete blood count with differential and an erythrocyte sedimentation rate (ESR), arthro- centesis should be performed. The joint fluid should be sent to a laboratory for a cell count with differential, glucose and protein measure- ments, bacterial culture and sensitivity, and polarized light microscopy for crystals.
Because a tense, painful, swollen knee may present an unclear clinical picture, arthrocentesis may be required to differentiate simple effusion from hemarthrosis or occult osteochondral fracture.4 A simple joint effusion produces clear, straw-colored transudative fluid, as in a knee sprain or chronic meniscal injury. Hemarthrosis is caused by a tear of the anterior cruciate ligament, a fracture or, less commonly, an acute tear of the outer portion of the meniscus. An osteochondral fracture causes hemarthrosis, with fat globules noted in the aspirate.
Rheumatoid arthritis may involve the knee joint. Hence, serum ESR and rheumatoid factor testing are indicated in selected patients.
The authors indicate that they do not have any conflicts of interest. Sources of funding: none reported.
In conclusion, knee pain is a common health issue which occurs due to a variety of injuries and/or conditions, such as sports injuries, automobile accidents, and arthritis, among other problems. Treatment of knee pain depends largely on the source of the symptoms. Therefore, it is essential for the individual to seek immediate medical attention to receive a diagnosis.
Chiropractic care is an alternative treatment option which focuses on the treatment of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
1. Rosenblatt RA, Cherkin DC, Schneeweiss R, Hart LG. The content of ambulatory medical care in the United States. An interspecialty comparison. N Engl J Med 1983;309:892-7.
2. Tandeter HB, Shvartzman P, Stevens MA. Acute knee injuries: use of decision rules for selective radiograph ordering. Am Fam Physician 1999;60: 2599-608.
3. Calmbach WL, Hutchens M. Evaluation of patients presenting with knee pain: part II. Differential diag- nosis. Am Fam Physician 2003;68:917-22
4. Bergfeld J, Ireland ML, Wojtys EM, Glaser V. Pin- pointing the cause of acute knee pain. Patient Care 1997;31(18):100-7.
6. Juhn MS. Patellofemoral pain syndrome: a review and guidelines for treatment. Am Fam Physician 1999;60:2012-22.
7. Smith BW, Green GA. Acute knee injuries: part I. History and physical examination. Am Fam Physi- cian 1995;51:615-21.
8. Walsh WM. Knee injuries. In: Mellion MB, Walsh WM, Shelton GL, eds. The team physician�s hand- book. 2d ed. St. Louis: Mosby, 1997:554-78.
9. McMurray TP. The semilunar cartilage. Br J Surg 1942;29:407-14.
10. Stiell IG, Wells GA, Hoag RH, Sivilotti ML, Cacciotti TF, Verbeek PR, et al. Implementation of the Ottawa knee rule for the use of radiography in acute knee injuries. JAMA 1997;278:2075-9.
11. Stiell IG, Greenberg GH, Wells GA, McKnight RD, Cwinn AA, Caciotti T, et al. Derivation of a decision rule for the use of radiography in acute knee injuries. Ann Emerg Med 1995;26:405-13.
12. Sartoris DJ, Resnick D. Plain film radiography: rou- tine and specialized techniques and projections. In: Resnick D, ed. Diagnosis of bone and joint disor- ders. 3d ed. Philadelphia: Saunders:1-40.
13. Schenck RC Jr, Goodnight JM. Osteochondritis dis- secans. J Bone Joint Surg [Am] 1996;78:439-56.
The tendons are powerful soft tissues which connect the muscles to the bones. One of these tendons, the quadriceps tendon, works together with the muscles found at the front of the thigh in order to straighten the leg. A quadriceps tendon rupture can affect an individual’s quality of life.
A quadriceps tendon rupture can be a debilitating injury and it usually requires rehabilitation and surgical interventions to restore knee function. These type of injuries are rare. Quadriceps tendon ruptures commonly occur among athletes who perform jumping or running sports.
Quadriceps Tendon Rupture Description
The four quadriceps muscles come together above the kneecap, or patella, to form the quadriceps tendon. The quadriceps tendon joins the quadriceps muscles into the patella. The patella is connected to the shinbone, or tibia, by the patellar tendon. Working collectively, the quadriceps muscles, the quadriceps tendon, and the patellar tendon, straighten the knee.
A quadriceps tendon rupture can be partial or complete. Many partial tears don’t completely disrupt the soft tissues. However, a full tear will divide the soft tissues�into two parts. If the quadriceps tendon ruptures entirely, the muscle is no longer attached to the kneecap or patella. As a result, the knee is unable to straighten�out when the quadriceps muscles contract.
Quadriceps Tendon Rupture Causes
A quadriceps tendon rupture frequently occurs due to an increased load on the leg where the foot is planted and the knee is somewhat flexed. By way of instance, when landing from an awkward jump, the power is too much for the soft tissues to bear, causing a partial or complete tear. Tears may also be due to falls, direct impacts to the knee, and lacerations or cuts.
A weakened quadriceps tendon is also more likely to rupture. Several factors may result in tendon weakness, including quadriceps tendinitis, the inflammation of the quadriceps tendon, called quadriceps tendinitis. Quadriceps tendinitis is one of the most common sports injuries in athletes who participate in sports or physicial�activities which involve jumping.
Weakened soft tissues may also be brought on by diseases that interrupt blood flow to the knee or patella. Utilizing corticosteroids and some antibiotics have also been connected to weakness associated with quadriceps tendon ruptures. Immobilization for an extended period of time can also decrease strength in the quadriceps tendons. Finally, quadriceps tendon ruptures can occur due to dislocations and/or surgery.
Quadriceps Tendon Rupture Symptoms
A popping or tearing feeling is one of the most common symptoms associated with a quadriceps tendon rupture. Pain followed by swelling and inflammation of the knee�might make the individual unable to straighten out their knee. Other symptoms of a quadriceps tendon rupture include:
An indentation at the top of the kneecap or patella of the affected site
Bruising
Tenderness
Cramping
Sagging or drooping of the kneecap or patella where the tendon tore
Difficulty walking because the knee is buckling or giving away
Quadriceps Tendon Rupture Evaluation
The healthcare professional will perform an evaluation to diagnose a quadriceps tendon rupture by first discussing the patient’s symptoms�and medical history.�After talking about the patient’s symptoms and medical history, the doctor will conduct a comprehensive evaluation of the knee.
To ascertain the precise cause of the patient’s symptoms, the healthcare professional will examine how well it is possible to stretch, or straighten,�the knee. Although this area of the evaluation can be debilitating, it’s essential to diagnose a quadriceps tendon rupture.
To verify a quadriceps tendon rupture diagnosis, the doctor may order some imaging tests, like an x-ray or magnetic resonance imaging, or MRI, scan. The kneecap moves from place once the quadriceps tendon ruptures. This can be quite evident on a sideways x-ray perspective of the knee.
Complete tears may frequently be identified with x-rays alone. The MRI can reveal the quantity of tendon torn along with the positioning of the tear. From time to time, an MRI will also rule out another injury with similar symptoms. Diagnostic imaging is helpful in the evaluation of sports injuries.
The quadriceps tendon is the large tendon found just above the kneecap, or patella, which allows us to straighten out our knee. While the quadriceps tendon is a strong, fibrous cord which can withstand tremendous amounts of force, sports injuries or other health issues may lead to a quadriceps tendon rupture. Quadriceps tendon ruptures are debilitating problems which can affect a patient’s quality of life.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Quadriceps Tendon Rupture Treatment
Non-Surgical Treatment
A majority of partial tears react well to non-surgical treatment approaches. The doctor may advise the patient to utilize a knee immobilizer or brace to allow the quadriceps tendon to heal. Crutches will help avoid placing weight onto the leg. A knee immobilizer or brace is used�for 3 to 6 months.
Once the initial pain, swelling, and inflammation have�decreased, alternative treatment options, such as chiropractic care and physical therapy, can be utilized. A doctor of chiropractic, or chiropractor, utilizes spinal adjustments and manual manipulations to carefully correct any spinal misalignments, or subluxations, which may be causing problems.
Furthermore, chiropractic care and physical therapy can provide lifestyle modifications, including physical activity and exercise programs to help speed up the recovery process. The patient may be recommended a variety of stretches and exercises to improve strength, flexibility and mobility. The healthcare professional will determine when it’s safe to return-to-play.
Surgical Treatment
Many individuals with complete tears require surgery to repair a quadriceps tendon rupture. Surgical interventions depend on the patient’s age, actions, and prior level of function. Surgery for quadriceps tendon ruptures involves re-attaching the tendon to the kneecap or patella. Surgery is carried out with regional spinal anesthetic or general anesthetic.
To reattach the tendon, sutures are put in the tendon and then threaded through drill holes at the kneecap. The stitches are attached in the base of the kneecap. The�physician will tie the sutures to find the ideal tension in the kneecap or patella. This will also make sure that the place of the kneecap closely matches that of the uninjured patella or kneecap.
A knee immobilizer, brace or a long leg cast may be utilized following the surgery. The patient may be allowed to set weight on their leg by means of crutches. Stretches and exercises are added into a rehabilitation program by a chiropractor or physical therapist after a surgical intervention.
The precise timeline for chiropractic care and physical therapy following a surgery for those patients that require it will be individualized personally. The patient’s rehabilitation program will be contingent upon the kind of tear, their surgery, medical condition, along with other requirements.
Conclusion
The majority of patients can return to their original routines after recovering from a quadriceps tendon rupture. The individual’s return will be addressed very carefully by the healthcare professional.�The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
When dealing with a sports injury or a similar type of injury, many people are familiar with the R.I.C.E. protocol for injury care. R.I.C.E. stands for Rest, Ice, Compression, and Elevation and has long been used when treating everything from sprained ankles to banged up knees. With acute injury patients, experts recommend adding �P� for protection because of the protection of the area is vital in the healing process. It is crucial that this is implemented as soon after the injury as possible and it should be maintained for anywhere from 24 hours to 72 hours afterward. Of course, this depends on the severity of the injury.
P is for Protection: Injuries hurt and pain can be a good thing because it prevents you from further injuring that area. It encourages you to protect it.
It is essential to listen to your body and protect the injured area through full or partial immobilization and restricted use. The way you do this depends on the body part.
An arm or shoulder injury can be protected with the use of a sling. An ankle injury may require a brace or splint, and you may have to avoid or limit weight bearing for a while. This means using crutches a walker, or a cane.
R is for Rest: The body needs rest to heal. This could mean complete rest, but in many cases, it means what is known as �relative rest.� This means that it allows for enough rest to heal but is not entirely restrictive which could slow or inhibit recovery.
This means avoiding activities that are stressful to the area to the point that they cause pain or that they might compromise healing. Many times, though, some movement is a good thing, even beneficial. Some gentle movements can speed recovery.
Isometric contractions of the muscles and joints that surround the injury and even some range of motion exercises can help. The key is to keep the movements gentle and to listen to your body for guidance on how much and how far to push.
I is for Ice:Cryotherapy or cold treatments can come in the form of actual ice, or there can be other types such as a cold soak. When treating acute injuries at home, the best known, and probably most straightforward way is to put some crushed ice in a freezer bag with a zip lock closure and wrap it in a small towel to keep the pack from directly touching the skin.
Frozen vegetables, like green beans, peas, or edamame work well too � remember to use the towel as a barrier between the skin and the pack. You should not use the pack more than 10 to 15 minutes as a time. The recommended cycle is 10 to 15 minutes on and 1 to 2 hours off.
In some cases, you may not be able to apply ice directly to the site. In those cases, you can use the pack at the joint above the affected area. For instance, a tightly wrapped ankle can still benefit from ice, you just apply the ice pack to the back on the knee on the same leg.
C is for Compression: A compression wrap can offer mild support and reduce swelling. Typically, an elastic bandage is used to compress or apply pressure to the injured tissue.
When applying a compression bandage, start it several inches below the area that is injured. It should be applied directly to your skin.
Use some tension as you wrap, but not to the point that it cuts off circulation (characterized by tingling or numbness and the soft tissue should not change color). Wrap the bandage in a figure eight configuration or spiral, depending on the area, stopping a few inches above the injury.
E is for Elevation: When an injured joint or extremity is not elevated, fluid can pool in the area and swelling can occur. This can lead to increased pain and limited range of motion. Elevation helps prevent these things from happening and can even help to speed up recovery.
The key to elevation is positioning the injured area at a level that is above the heart. The most effective way to accomplish this is to keep the area elevated as much as possible while awake and prop it up with pillows while sleeping for at least the first 24 to 48 hours. Some injuries may require more time though, so listen to your body.
Chondromalacia patellae, also referred to as runner’s knee, is a health issue in which the cartilage beneath the patella,�or kneecap, becomes soft�and ultimately degenerates. This problem is prevalent among young athletes,�however, it may also develop in older adults who suffer from arthritis of the knee.
Sports injuries like chondromalacia patellae are frequently regarded as an overuse injury. Taking some time off from participating in physical activities and exercise may produce superior outcomes. In the instance that the individual’s health issues are due to improper knee alignment, rest may not offer pain relief. Symptoms of runner’s knee include knee pain and grinding sensations.
What Causes Chondromalacia Patellae?
The kneecap,�or the patella, is generally found through the front of the knee joint. If you bend your knee, the rear end of your kneecap slips over the cartilage of your femur, or thigh bone, at the knee. Complex soft tissues, such as tendons and ligaments, connect the kneecap to the shinbone and thigh muscle. Chondromalacia patellae�can commonly occur when any of these structures fail to move accordingly, causing the kneecap to rub against the�thigh bone. Poor kneecap motion may result from:
Misalignment due to a congenital health issue
Weakened hamstrings and quadriceps, or the muscles of the thighs
Muscle imbalance between the adductors and abductors, the muscles on the inside and outside of the thighs
Continuous pressure to the knee joints from certain physical activities and exercise like running, skiing, or jumping
a direct blow or injury for a kneecap
Who is at Risk for Chondromalacia Patellae?
Below is an assortment of factors which may increase an individual’s chance for developing chondromalacia patellae.
Age
Adolescents and young adults have the highest risk for this health issue. During growth spurts, bones and muscles can often grow too rapidly, causing short-term muscle and bone imbalances in the human body.
Gender
Females are more likely than males to develop runner’s knee, because women generally possess less muscle mass than men. This may result in abnormal knee placement, and more lateral pressure on the kneecap.
Flat Feet
Individuals who have flat feet can add more strain to the knee joints as compared to individuals who have higher arches.
Past Injury
Previous injuries to the kneecap, including a dislocation, can raise the chance of developing chondromalacia patellae.
Increased Physical Activity
Increased levels of physical activities and exercise can place pressure on the knee joints, which may raise the risk for knee issues.
Arthritis
Runner’s knee may also be an indication of arthritis, a well-known problem causing pain and inflammation to the tissue and joint. Swelling can prevent the proper function of the knee and its complex structures.
What are the Symptoms of Chondromalacia Patellae?
Chondromalacia patellae will generally present as pain in the knee, called patellofemoral pain, accompanied by sensations of cracking or grinding when extending or bending the knee. Pain may worsen after sitting for an extended period of time or through physical activities and exercises that apply intense pressure for your knees, like standing. It’s essential for the individual to seek immediate medical attention if the symptoms of chondromalacia patellae, or runner’s knee, do not resolve on their own.
Diagnosis and Chondromalacia Patellae Grading
A healthcare professional will search for areas of pain and inflammation on the knee. They might also look at the way the kneecap aligns with the thigh bone. A misalignment may indicate the presence of chondromalacia patellae. The doctor may also perform a series of evaluations to ascertain the presence of this health issue.
The healthcare professional may also ask for any of the following tests to help diagnose chondromalacia patellae, including:�x-rays to show bone damage or misalignments or arthritis; magnetic resonance imaging, or MRI, to see cartilage wear and tear; and�arthroscopic examination, a minimally invasive procedure which involves inserting an endoscope and camera inside the knee joint.
Grading
There are four levels of chondromalacia patellae, ranging from grade 1 to 4, which characterize the level of the patient’s runner’s knee. Grade 1 is considered mild while grade�4 is considered severe.
Grade 1 indicates the softening of the cartilage in the knee region.
Grade 2 suggests a softening of the cartilage followed by abnormal surface features, the start of degeneration.
Grade 3 reveals the thinning of the cartilage together with active degeneration of the complex soft tissues of the knee.
Grade 4, or the most severe grade, demonstrates exposure of the bone through a substantial part of the cartilage Bone exposure means that bone-to-bone rubbing is most likely happening in the knee.
What is the Treatment for Chondromalacia Patellae?
The goal of treatment for chondromalacia patellae is to first decrease the strain being placed on the kneecap, or patella, and the femur, or thigh bone. Rest and the use of ice and heat agains the affected knee joint is generally the first line of treatment. The cartilage damage associated with runner’s knee may often repair itself with these remedies along.
Moreover, the healthcare professional may prescribe anti-inflammatory drugs and/or medications, such as ibuprofen, to decrease pain and inflammation around the knee joint. When tenderness, swelling, and pain persist, the following treatment options could be explored. As mentioned above, individuals should seek immediate medical attention if symptoms persist.�
Chiropractic Care
Chiropractic care is a safe and effective, alternative treatment option which focuses on the diagnosis, treatment, and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system, including chondromalacia patellae. Occasionally,�knee pain may originate due to spinal misalignments or subluxations. A doctor of chiropractic, or chiropractor, will use spinal adjustments and manual manipulations to carefully restore the natural integrity of the spine.�
Furthermore, a chiropractor may also recommend a series of lifestyle modifications, including nutritional advice and a physical activity or exercise guide to help ease symptoms associated with chondromalacia patellae. Rehabilitation may also focus on�strengthening the quadriceps, hamstrings, adductors, and abductors to improve muscular strength, flexibility, and mobility. The purpos of muscle balance is also to assist in preventing knee misalignment, among other complications.
Surgery
Arthroscopic surgery might be required to inspect the joint and ascertain whether there is a misalignment of the knee. This operation involves inserting a camera in the knee joint through a very small incision. A surgical procedure can repair the issue. One�common process is a lateral release. This surgery involves cutting a number of the ligaments to release tension and permit for more movement. Additional surgery may entail implanting the back of the kneecap, inserting a cartilage graft, or transferring the thigh muscle.
�
Chondromalacia patellae is characterized as the inflammation of the underside of the patella, or kneecap, caused by the softening of the cartilage surrounding the soft tissues of the knee joint. This well-known health issue is generally caused due to sports injuries in young athletes, although chondromalacia patellae may also occur in older adults with arthritis in the knee. Chiropractic care can help restore strength and balance to the knee joint and its surrounding soft tissues.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
How to Prevent Chondromalacia Patellae
A patient can ultimately lower their chance of developing runner’s knee, or chondromalacia patellae, by:�
Avoiding repeated stress on the knees. In case the individual needs to spend time on their knees, they could wear kneepads.
Produce muscle balance by strengthening the quadriceps, hamstrings, abductors, and adductors.
Wear shoe inserts that correct flat feet. This may reduce the amount of pressure being placed on the knees to realign the kneecap, or patella.
Keeping a healthy body weight can also help prevent chondromalacia patellae. Following the nutritional advice and guidance from a healthcare profesional can help promote a healthy body weight. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
You may have seen professional athletes, dancers, gymnasts, and others who engage in extremely physical activities using a type of tape on various points of their bodies. It is sometimes colored and does not seem to inhibit range of motion. While it looks like tape or maybe a very fancy bandage, it is a highly technical, specialized tape that is used to treat patients of all ages and activity levels. It is called Kinesio tape, and it is often used by chiropractors to help address specific injuries.
What is Kinesio Tape?
Also called Kinesio Tex Tape, Kinesio Tape is a special adhesive tape that has elastic properties. It was developed by Dr. Kenzo Kase, a chiropractor, and acupuncturist, in 1979. It is safe for all ages including pediatric and geriatric patients. The tape is comprised of a 100% cotton fiber strip with medical grade acrylic adhesive. It is soft and gentle, but it works.
The tape is hypoallergenic and latex free, so it is appropriate for a vast audience. It is also water resistant, making it wearable for many activities. When worn, the tape does not limit or inhibit range of motion, and the same tape can be worn for several days without losing its effectiveness.
How does Kinesio Tape Work?
The tape can stimulate or relax muscles, depending on the tension that it puts on the body when applied. When worn, it lifts the skin by microscopic increments which aids in lymphatic drainage.
It also helps to decrease inflammation and swelling which reduces pressure in the area. This allows the blood and lymphatic fluid to flow freer and more effectively in and out of the affected area.
When used correctly, Kinesio Tape can reduce inflammation, promote better circulation, prevent injury, facilitate healing, the re-educate the neuromuscular system. This helps the body return to homeostasis. It can be applied in many different configurations, but often the applications are a single �I,� �Y,� or �X.�
The Kinesio Taping Method
The Kinesio taping method is a systematic, therapeutic technique that offers a two-prong approach of supporting the patient and rehabilitating the condition or affected area. It can alleviate pain reduce swelling, providing relief to the patient. There are specific taping shapes that are specialized to address certain areas of the body as well as certain conditions. While it provides stability and support to the body�s joints and muscles, it does not restrict the range of motion. The technique is designed to address soft tissue injury by manipulating that area and facilitating healing.
What Conditions is Kinesio Taping used to Treat?
Many conditions throughout the body can benefit from Kinesio Taping. Chiropractors use it for:
Lower back strain
Plantar fasciitis
Back strain
Carpal tunnel syndrome
Rotator cuff injury
Ankle Sprains
Whiplash
Herniated disc
Post-surgery edema
Tennis elbow
Pre-surgery edema
Patella tracking
Athletes may also use it for additional support or to prevent injury. Because it relies on the body�s natural healing process, many people find it to be preferred treatment for many painful conditions. When combined with chiropractic care, Kinesio Tape is very effective.
When treating a condition with Kinesio Tape, the chiropractor may use a variety of techniques, depending on the illness or injury. They may use spinal manipulation, massage, and other treatments, combining them with recommendations for lifestyle changes and diet modifications.
The draw for this treatment is that it encourages the body to heal itself, eliminating the need for drugs with their undesired and unpleasant side effects, or more invasive procedures like surgery. Kinesio Taping is safe, natural, and a perfect complement to chiropractic care.
Stenosing tenosynovitis, also known as �trigger finger,� is a repetitive strain injury that is one of the most common injuries in the workplace. It is marked by one finger or thumb that is stuck in a bent position and pops or snaps when straightened. The�cause is an inflamed or irritated flexor tendon.
As it slides through the sheath tunnel, the back and forth motion creates irritation which can lead to thickening of the tendon and even the formation of nodules. This can impede its movement through the sheath which can also thicken so that the opening that the tendon slides through becomes smaller.
What are the symptoms of trigger finger?
A person that has�trigger finger may experience several symptoms in one or more fingers or thumb including:
Pain when straightening or bending the finger
Swelling
A lump in the palm that is tender
The finger or thumb joints have a popping or catching sensation
Stiffness
The impaired tendon may suddenly break free causing the finger to snap straight or feel like it is dislocating
Some symptoms, like the stiffness, popping, and catching, may be more pronounced after periods of inactivity. The patient may find that upon waking they have difficulty, but as they move their fingers they loosen, and the symptoms aren�t as cause. In severe cases, the patient is unable to straighten their finger, even with help.
What causes trigger finger?
Many times the cause of trigger finger is not known. They may notice a gradual decline or they may wake up one day and experience symptoms. There are certain health conditions and circumstances that put some patients at a higher risk of developing trigger finger:
Men tend to get trigger finger more than women do
The most common age group for trigger finger is between 40 and 60 years old
It is prevalent in patients with rheumatoid arthritis, diabetes, and other medical conditions
Repetitive hand motions such as typing, gripping power tools, or playing video games
Activities where the hands are in constant repetitive�action.
What are the treatments for trigger finger?
There are surgical and nonsurgical treatments for trigger finger, depending on the severity of the condition. When the symptoms are mild, the patient may be advised to, rest the finger and take over the counter pain relievers like acetaminophen or cause to help reduce inflammation and minimize pain. The patient may also wear a splint to facilitate the resting position of the finger better.
In some cases, the doctor may advise steroid injections administered directly into the tendon sheath to correct the problem. Sometimes this procedure only provides temporary relief and requires a�second injection. If the condition shows no improvement after the second injection, the patient may be advised to undergo surgery. If the patient has had trigger finger for a long time or if they have a medical condition such as diabetes, injections are not likely to be as, or a permanent solution.
Some patients undergo surgery to correct trigger finger. The is purely elective since the condition is not considered dangerous. The operation opens the tendon sheath, the tunnel that the tendon slides through, to move easier. It is usually done on an outpatient basis.
Chiropractic for trigger finger
Two chiropractic treatments for trigger finger:
Active Release Technique (ART)
Graston technique
Studies have found these chiropractic techniques to be very useful in treating trigger finger.
An instrument based soft tissue therapy may also be used to help reduce tension in the muscles around the area. Chiropractors typically use a whole-body approach to help the patient achieve relief and healing. They recognize that most conditions are not limited to only what appears to be the affected area so they will employ techniques that treat the associated regions of the body as well, which, provides the patient with more reliable relief without the use of invasive procedures. Chiropractic is a practical, natural way to treat trigger finger.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine