How can healthcare professionals recognize and establish protocols for individuals who are being trafficked and provide a safe place?
Introduction
Today, we will look at part two of this series, which is about recognizing trafficking in a clinical setting. Today’s article in this two-part series of recognizing trafficking helps inform many healthcare professionals to understand the roles and protocols for identifying trafficking that is affecting their patients and help provide a safe, positive space for them. We discuss with certified associated medical providers who consolidate our patients’ information to assess and identify trafficking in the clinic while taking the proper protocols to ensure patient safety. We also inform and guide patients while asking their associated medical provider intricate questions to integrate and provide them with a safe and positive space. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
Health Care Professional’s Role in Identifying Trafficking
Even though they may come across victims of human trafficking and have the chance to step in, many healthcare professionals believe they lack the knowledge and self-assurance needed to recognize these victims and offer them the kind of aid they need. As an illustration:
Just 37% of social workers and medical professionals surveyed again had any training in recognizing and supporting victims of human trafficking (Beck et al., 2015).
It is extremely hard for processors to identify and aid victims because traffickers move their victims around a lot and employ various strategies to evade discovery. Frequently, it could be your final interaction with the victim (Macy & Graham, 2012).
There can be a companion who comes across as very domineering, who won’t let the patient spend time alone with you, or who insists on filling out paperwork or talking on the patient’s behalf.
It’s possible that neither the victim nor their friend will have identification or insurance paperwork and will just pay in cash.
The victim or their companion may refuse to answer questions.
The victim may decline additional testing and follow-up care.
The victim may have physical injuries, sexually transmitted diseases, and signs of psychosocial stress.
The victim may not know the city and state that they are in.
The victim may appear fearful when asked questions or in the presence of their companion.
The victim may exhibit feelings of shame, guilt, helplessness, or humiliation.
You may notice inconsistencies in basic information, such as age, name, address, work history, or information regarding living status and daily activities.
If the patient does not speak English, where are they from, and how did they arrive?
If the patient is a minor, who and where is the guardian?
The victim may have unusual tattoos to indicate that they are the “property” of their trafficker.
Recognizing the Signs of Trafficking
You can more easily spot possible victims and offer the right help if you are aware of the typical warning indicators of human trafficking. The following are typical signs that someone is being trafficked. Naturally, not all victims or forms of trafficking will exhibit all of the indicators. Work and Living Conditions (National Human Trafficking Hotline, n.d.):
The victim may not be able to come and go on their own or leave their current home or work situation.
Human trafficking victims are often minors who are forced to engage in commercial sex acts.
The individual may work in the commercial sex industry and be under the control of a pimp or manager.
The victim may be required to work unusual or excessively long hours.
The victim may receive little, if any, pay or may only receive tips.
The victim may be subjected to unusual or extreme restrictions at work or may not be allowed to take breaks.
The victim may owe a large debt to their “employer.”
The victim may have been lured to their current work or living situation through false promises about the nature of their work or living environment.
The victim’s home or work location may have unusually high security, such as opaque or boarded-up windows, bars on windows, high fences, and security cameras.
The victim may be required to live at their work location.
The victim may experience various signs of abuse at the hands of their employer.
The victim may not be paid directly. Instead, the money is directed to the supervisor or manager, who deducts a large percentage for living expenses and other debts.
The victim may be forced to meet unreasonable daily quotas.
The victim may be forced to work in unsafe work environments without the proper safety equipment.
Chiropractic Care for Healing After Trauma-Video
Best Practice Guidelines for Interviewing Trafficking Individuals
As a healthcare provider, you must continuously weigh the different courses of action at every interview process step. To establish trust and ensure safety, practitioners must, above all, put aside preconceived notions and assumptions about the victims and their behavior (Hodge, 2014; DeBoise, 2014; Hemmings, Jakobowitz, & Abas, 2016). Zimmerman and Watts (2003) suggest that the World Health Organization has produced rules for every phase of the interview process, which include the following recommendations:
It’s critical to keep in mind that every trafficking scenario and survivor is distinct, making it crucial to pay attention to and accept each person’s account.
It could take some time for victims to open up and be willing to talk about their experiences because it can be hard for them to build rapport and trust.
You should take precautions to protect both you and the victim because you should anticipate that the victim is at risk of psychological, bodily, social, and legal harm.
To prevent further upsetting the victim, you should consider the risks and advantages before beginning the interview process, as it can be a traumatic experience in itself.
While you should direct victims to available resources when necessary, you should avoid making unfulfilled promises or pledges.
The amount of time it takes for victims of human trafficking to be prepared to embrace change might vary greatly. Some victims can be eager to look for new possibilities and to improve their circumstances. Some people can be less likely to accept assistance because they haven’t developed enough trust issues or because they fear retaliation from their trafficker.
Depending on the situation, many service providers or interpreters must be present during the interview. Everyone taking part in the interview process ought to be reasonably knowledgeable about human trafficking, including how traffickers manipulate their victims and how to interact with them in a way that respects their cultural differences. To maintain anonymity and ensure the victim can communicate freely and honestly, you should refrain from using interpreters who are acquainted with the victim or who live in the same neighborhood.
Having an emergency safety plan in place is crucial to shielding the victim from harm—both from others and self-harm.
Consent must always be obtained voluntarily for all interventions, including interviews. For many victims who have never known autonomy or self-determination, this may be a foreign idea.
Avoid using legal or technical jargon.
Furthermore, it’s critical to remember that trauma survivors may suffer after treatment can have a lasting effect on all facets of their lives, making psychological, emotional, and physical safety a top priority. It is reasonable to presume that the person provides the most accurate account of their experience at that time. A person’s guarded, defensive, and belligerent behavior may be only their coping mechanism for their trauma. (V. Greenbaum, 2017)
How to Report Known or Suspected Trafficking
The best way to report suspected trafficking is by calling the National Human Trafficking Hotline or texting the number 711 if the patient responds affirmatively to the evaluation questions if your findings imply that they might be victims of human trafficking. Additionally, you can text 233733. Basic details about the case will be requested from you, such as (National Human Trafficking Hotline, n.d.):
the location of the suspected trafficking
the name of the alleged trafficker, if possible
your city and state
how you learned about the hotline
Health care providers who know or believe that a youngster is being abused, neglected, or abandoned should report their concerns to law enforcement or the relevant child welfare agency right away, as they are required reporters under child abuse and neglect statutes. You can report abuse online or by calling the Department of Children and Families Abuse Hotline in the state you are residing in.
Documenting Physical Findings
Physical findings should be meticulously and precisely recorded using written descriptions, freehand sketches that have been identified and annotated, and digital or film photos with the patient’s consent. Regarding photography, the picture should show the patient’s face and the lesion or injury measured using a coin, ruler, or other common object. The photo should include a piece of paper bearing the date the picture was taken. More photos can capture up close shots of every pertinent lesion or injury. Serial follow-up photos over seven to ten days can be used to record the healing or advancement of ecchymoses and other injury-related symptoms. A statement identifying the photographer and attesting to the accuracy and integrity of the images ought to be incorporated into the chart. Before any photos are taken, consent for the photographic documentation should be sought and recorded. Patients should be aware of their rights, which include the ability to decline all photographic documentation or limit it to a limited number of specified locations.
In addition to providing essential medical care, the healthcare professional should work to establish an environment where each patient feels respected, comfortable, cared for, validated, and empowered to reveal if they so choose. If the patient does not feel “ready” to demonstrate in the clinical environment, disclosure may happen later. As a result, for at-risk patients, every single clinical interaction should be seen as a step toward their eventual safety.
Laws & Policies for Human Trafficking
The United States has enacted a variety of laws and policies designed to prevent human trafficking, punish the perpetrators, and protect the survivors. One of these laws and policies is the Trafficking Victims Protection Act law or the TVPA (U.S. Congress).
This is the centerpiece of federal human trafficking legislation. The act focuses on three primary areas:
The TVPA seeks to prevent human trafficking through increased training and awareness.
The act seeks to protect trafficking victims by providing them access to services using federal funds similar to other refugees.
The act establishes trafficking and related crimes as federal offenses subject to stiff penalties.
One way that the legislation protects victims of human trafficking is that it absolves them of consequences for engaging in criminal activities that arise from their trafficking experience, such as entering the nation using fraudulent documents or working without the proper authorization. In addition, families of trafficking victims are qualified for T visas, which let them stay in the nation to support federal law enforcement in their pursuit of the offenders. After three years, victims can then apply to become permanent residents. Depending on the specific circumstances, many individuals may be entitled to assistance and benefits, such as access to the Witness Security Program and reparations. In addition, individuals between 16 and 24 could qualify for the Job Corp program and work permits.
Others criticize the TVPA. Usually, the onus is on the victim to prove their innocence or compulsion first. Second, the act emphasizes sex trafficking more than other types of human trafficking, which ignores how intricate human trafficking is. Only victims and survivors of “severe” types of trafficking who are prepared to cooperate with the investigation and prosecution of their offenders are eligible for the services provided under the act. This ignores the severity of the abuse the victims endured and the degree of mistrust and terror they might harbor toward both the abuser and others in positions of power.
Preventing Trafficking Through Awareness, Interventions, & Resources
In the shadows, human trafficking flourishes. We eradicate the shadows where human traffickers lurk by increasing public and health practitioner awareness of the problem (Hodge, 2008; Gozdziak & MacDonnell, 2007). For instance, putting up signs and pamphlets on human trafficking can not only help to enhance public awareness but also boost the chance that victims may come forward on their own. Brochures and posters are free from the Campaign to Rescue and Restore Victims of Trafficking.
When assisting victims of human trafficking, practitioners and service providers need to be able to engage with a variety of governmental, legal, medical, and social service organizations and institutions. Generally speaking, there are three main categories into which the care and services that a victim falls (Dell et al., 2019; Johnson, 2012; Oram & Domoney, 2018):
Immediate Services
Services Related to Recovery
Services About Reintegration
Resources for Providers
The National Human Trafficking Resource Center’s referral database can be consulted by providers looking to connect with local programs that assist victims of human trafficking or who need assistance for a victim or survivor. Many healthcare providers can check out the website to provide helpful resources in their local area.
Conclusion
Any human trafficking violates fundamental rights. Since human trafficking has many underlying roots, eradicating the issue would need different approaches on various fronts. When it comes to addressing racism, poverty, oppression, prejudice, and other factors that lead to human trafficking, healthcare professionals need to be dedicated to facing this issue both within their patient population and in partnership with colleagues from different disciplines. Physicians, social workers, counselors, and other health care professionals are required by their code of ethics to lead in addressing power abuses and advancing social justice. Practitioners can accomplish this, among other things, by teaching others and themselves about the intricate dynamics and international scope of human trafficking.
References
Beck, M. E., Lineer, M. M., Melzer-Lange, M., Simpson, P., Nugent, M., & Rabbitt, A. (2015). Medical providers’ understanding of sex trafficking and their experience with at-risk patients. Pediatrics, 135(4), e895-902. https://doi.org/10.1542/peds.2014-2814
DeBoise, C. (2014). Human Trafficking and Sex Work: Foundational Social-Work Principles. Meridians: Feminism, Race, Transnationalism, 12(1), 227–233. https://muse.jhu.edu/article/541879/pdf
Dell, N. A., Maynard, B. R., Born, K. R., Wagner, E., Atkins, B., & House, W. (2019). Helping Survivors of Human Trafficking: A Systematic Review of Exit and Postexit Interventions. Trauma Violence Abuse, 20(2), 183-196. https://doi.org/10.1177/1524838017692553
Gozdziak, E., & MacDonnell, M. (2013, March 4). Closing the Gaps: the Need to Improve Identification and Services to Child Victims of Trafficking by School of Foreign Service – Georgetown University – Issuu. Issuu.com. https://issuu.com/georgetownsfs/docs/gozdziak-closing-the-gaps
Greenbaum, V. J. (2017). Child sex trafficking in the United States: Challenges for the healthcare provider. PLoS Med, 14(11), e1002439. https://doi.org/10.1371/journal.pmed.1002439
Hemmings, S., Jakobowitz, S., Abas, M., Bick, D., Howard, L. M., Stanley, N., Zimmerman, C., & Oram, S. (2016). Responding to the health needs of survivors of human trafficking: a systematic review. BMC Health Serv Res, 16, 320. https://doi.org/10.1186/s12913-016-1538-8
Hodge, D. R. (2008). Sexual trafficking in the United States: a domestic problem with transnational dimensions. Soc Work, 53(2), 143-152. https://doi.org/10.1093/sw/53.2.143
Macy, R. J., & Graham, L. M. (2012). Identifying domestic and international sex-trafficking victims during human service provision. Trauma Violence Abuse, 13(2), 59-76. https://doi.org/10.1177/1524838012440340
How do healthcare professionals provide a clinical approach to recognizing HIV for individuals in pain and providing relief?
Introduction
The human body has dealt with various environmental factors, injuries, and pathogens that can cause issues to the body system. As many individuals are always on the go from one location to another, being healthy is extremely important. Making time to make an appointment for a person’s health and well-being is extremely important, as many people have experienced comorbidities and overlapping risk profiles that are causing them pain. When individuals experience onset issues of fatigue, muscle and joint pain, or immune disorders, many healthcare professionals must assess the situation and ask the individuals when they experienced these overlapping risk profiles and how they affect their daily activities. One of the overlapping risk profiles that seems to affect the body is a viral infection known as Human Immunodeficiency Virus or HIV. This can get many healthcare professionals to come up with a personalized treatment plan to reduce these overlapping risk profiles and educate the individual on what to do to manage HIV symptoms. Today’s article looks at how HIV can impact a person, their symptoms, and non-surgical treatments to manage HIV. We discuss with certified associated medical providers who consolidate our patients’ information to assess the effects of HIV and its associated symptoms. We also inform and guide patients on how to be aware of the impact of HIV and ask their associated medical providers intricate questions to integrate a customized treatment plan to incorporate multiple non-surgical therapies to manage the symptoms. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
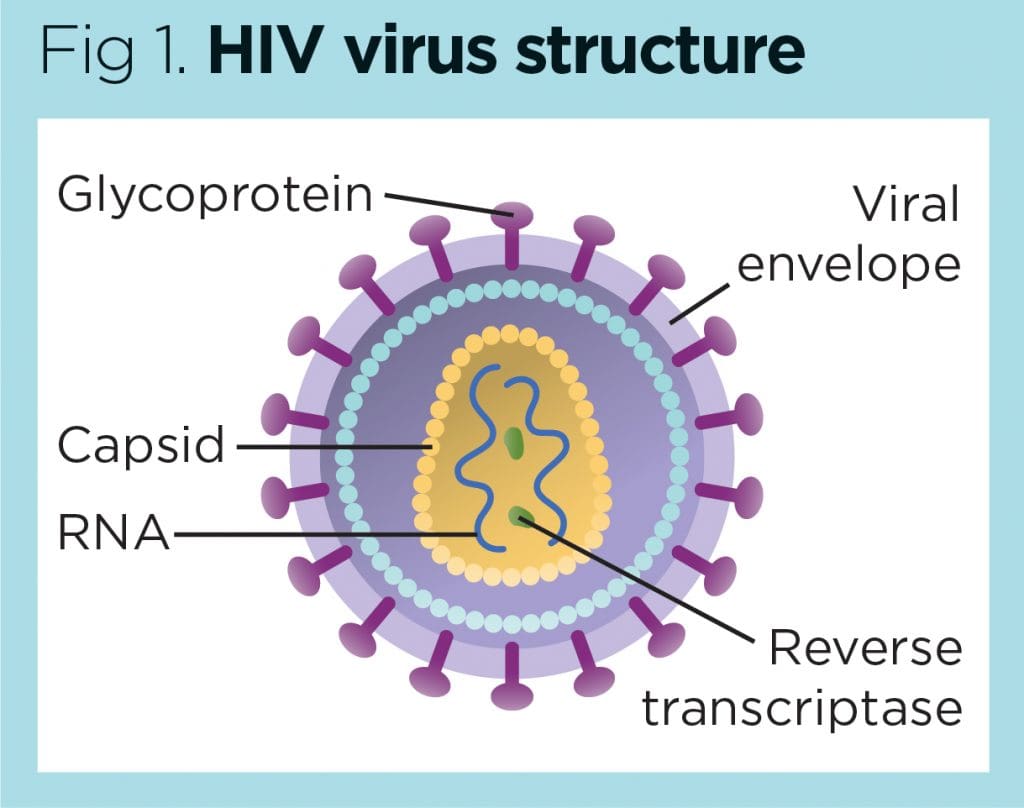
What Is HIV?
Do you constantly feel tired even after taking a good night’s rest? Do you feel your throat being sore without the flu symptoms? Or are you experiencing muscle and joint pain in different locations of your body? Worldwide, many individuals have often experienced these symptoms from a viral infection known as Human Immunodeficiency Virus or HIV. HIV belongs to the retroviridae family, which targets the body’s immune system, especially the CD4+ T cells. The CD4+T cells play an important role in the body’s immune response, but when HIV starts to deplete the receptors and terminate the host cells. (Masenga et al., 2023) This causes individuals to have acute stages of HIV and, if not treated immediately, can lead to the progression of severe stages. However, how do individuals contract HIV? Well, the most common mode is through unprotected sexual intercourse, sharing needles, or through maternal-infant exposure, which diminishes the T-helper cell population and, over time, can increasingly weaken the immune system. (van Heuvel et al., 2022) This causes many individuals to develop various symptoms from HIV that can vary, depending on the severity and the progression stages of the virus.
The Symptoms
Now, for the progression of HIV to infect the body’s immune system and cause various symptoms to affect the individual, many healthcare professionals have to look at the process of the host’s exosomes and their correlation role with HIV. The generational process of exosomes causes overlapping risk profiles with the viral assembly of HIV as exosomes can transport the virus from the infected cells to the uninfected cells of the body by helping it regulate the host’s immune response to the virus infection. (Chen et al., 2021) To that point, it can lead to the progression of several stages of HIV and its associated symptoms. When a person is dealing with an HIV infection in its acute stages, the symptoms can be mild and easily mistaken for a common viral infection. Some of the symptoms can include:
Muscle aches
Joint pain
Difficulty falling asleep
Fatigue
Neuropathy
Shortness of breath
Swollen glands
This is because the inflammatory cytokines from the immune system are heightened and influenced by HIV. When inflammatory cytokines become associated with HIV, symptoms have a huge impact on an individual’s life, causing them to be miserable. (Schnall et al., 2020) Additionally, when HIV is in a clinical latency stage, the virus is less active but can still replicate without exhibiting any symptoms in the body. However, when HIV progresses to its severe stage, it can lead to the development of AIDS. Luckily, treatment advancements to treat HIV from its acute stages can help manage the associated symptoms.
The Non-Surgical Approach To Wellness- Video
Non-Surgical Treatments For HIV
When it comes to treating HIV, non-surgical treatments can help manage its associated symptoms while dramatically improving the life expectancy and quality of life of the individual who is affected by the virus. For non-surgical treatments, the main goal is to diagnose HIV as early as possible and to assess the situation by coming up with new and innovative HIV testing initiatives to increase the frequency and prevention of HIV in both clinical and non-clinical settings. (Delaney & DiNenno, 2021) Below are some non-surgical treatments to manage HIV.
Antiretroviral Treatments
Now, some of the non-surgical treatments to manage HIV is by taking antiretroviral therapy. This allows the individual with HIV to be more mindful of taking antiretroviral medications daily, which then helps improve sustained viral suppression of HIV and provides effective strategies of therapeutic approaches to enhance antiretroviral activities. (Huerta, 2020) Additionally, the primary goal of antiretroviral therapy is to reduce the HIV load to an undetectable level, keep the immune system functioning, and prevent the progression development of AIDS.
Lifestyle Adjustments
While living with HIV today is vastly different from decades past, thanks to significant medical advancements. Many individuals can go to their healthcare providers for an early diagnosis and effective treatment to live long and healthy lives. Awareness, education, and staying proactive with health checks remain key in the fight against HIV and its progression. Additionally, proper nutrition, regular exercise, and mental health support are also crucial for people living with HIV, helping to boost the immune system and manage symptoms. At the same time, regular visits to a healthcare provider for blood tests are essential to monitor the effectiveness of ART and adjust the treatment regimen as needed to live a healthier life.
Delaney, K. P., & DiNenno, E. A. (2021). HIV Testing Strategies for Health Departments to End the Epidemic in the U.S. Am J Prev Med, 61(5 Suppl 1), S6-S15. https://doi.org/10.1016/j.amepre.2021.06.002
Masenga, S. K., Mweene, B. C., Luwaya, E., Muchaili, L., Chona, M., & Kirabo, A. (2023). HIV-Host Cell Interactions. Cells, 12(10). https://doi.org/10.3390/cells12101351
Schnall, R., Jia, H., & Reame, N. (2020). Association Between HIV Symptom Burden and Inflammatory Cytokines: An Analysis by Sex and Menopause Stage. J Womens Health (Larchmt), 29(1), 119-127. https://doi.org/10.1089/jwh.2019.7749
van Heuvel, Y., Schatz, S., Rosengarten, J. F., & Stitz, J. (2022). Infectious RNA: Human Immunodeficiency Virus (HIV) Biology, Therapeutic Intervention, and the Quest for a Vaccine. Toxins (Basel), 14(2). https://doi.org/10.3390/toxins14020138
Certain neurological disorders can cause acute episodes of peripheral neuropathy, and for individuals diagnosed with chronic peripheral neuropathy, can physical therapy help improve the ability to move around safely along with medications, procedures, and lifestyle adjustments to help control and manage symptoms?
Peripheral Neuropathy Treatments
Peripheral neuropathy treatment includes symptomatic therapies and medical management to help prevent worsening nerve damage.
For acute types of peripheral neuropathy, medical interventions and therapies can treat the underlying process, improving the condition.
For chronic types of peripheral neuropathy, medical interventions and lifestyle factors can help to prevent the condition’s progression.
Chronic peripheral neuropathy treatment focuses on controlling the pain symptoms and protecting areas of diminished sensation from damage or infection.
Self-Care and Lifestyle Adjustments
For individuals who have been diagnosed with peripheral neuropathy or are at risk of developing the condition, lifestyle factors play a significant role in managing symptoms and preventing nerve damage from worsening and can even prevent the condition from developing. (Jonathan Enders et al., 2023)
Pain Management
Individuals can try these self-care therapies and see if and which help reduce their discomfort and then develop a routine that they can work off of. Self-care for pain symptoms include:
Placing a warm heating pad on painful areas.
Placing a cooling pad (not ice) on painful areas.
Covering the area or leaving it uncovered, depending on comfort levels.
Wear loose-fitting clothes, socks, shoes, and/or gloves not made with material that can cause irritation.
Avoid using lotions or soaps that can cause irritation.
Use soothing creams or lotions.
Keeping the painful areas clean.
Injuries Prevention
Diminished sensation is one of the most common effects that can lead to problems like stumbling, difficulty getting around, and injuries. Preventing and regularly checking for injuries can help avoid complications like infected wounds. (Nadja Klafke et al., 2023) Lifestyle adjustments to manage and prevent injuries include:
Wear well-padded shoes and socks.
Inspect feet, toes, fingers, and hands regularly to look for cuts or bruises that may not have been felt.
Clean and cover cuts to avoid infections.
Use extra caution with sharp utensils like cooking and work or gardening tools.
Disease Management
Lifestyle factors can help prevent disease progression and are closely correlated with the risks and underlying causes. To help prevent peripheral neuropathy or its progression can be done by: (Jonathan Enders et al., 2023)
Maintain healthy glucose levels if you have diabetes.
Avoid alcohol for any peripheral neuropathy.
Maintain a well-balanced diet, which can include vitamin supplements, especially for vegetarians or vegans.
Over-the-Counter Therapies
A few over-the-counter therapies can help with painful symptoms and can be taken as needed. Over-the-counter pain therapies include: (Michael Überall et al., 2022)
Topical lidocaine spray, patch, or creams.
Capsaicin creams or patches.
Topical Icy Hot
Non-steroidal anti-inflammatory medications – Advil/ibuprofen or Aleve/naproxen
Tylenol/acetaminophen
These treatments can help relieve painful symptoms of peripheral neuropathy, but they do not help improve diminished sensation, weakness, or coordination problems. (Jonathan Enders et al., 2023)
Prescription Therapies
Prescription therapies for treating peripheral neuropathy include pain medications and anti-inflammatories. Chronic types of peripheral neuropathy include:
Alcoholic neuropathy
Diabetic neuropathy
Chemotherapy-induced neuropathy
The prescription treatments for chronic types differ from the treatments for acute types of peripheral neuropathy.
Pain Management
Prescription treatments can help manage the pain and discomfort. Medications include (Michael Überall et al., 2022)
Sometimes, a prescription strength supplement or vitamin B12 given through injection can help prevent progression when peripheral neuropathy is associated with a severe vitamin deficiency. Prescription treatment can help treat the underlying process in some types of acute peripheral neuropathy. Treatment for acute peripheral neuropathy, such as Miller-Fisher syndrome or Guillain-Barré syndrome, can include:
Corticosteroids
Immunoglobulins – immune system proteins
Plasmapheresis is a procedure that removes the liquid portion of blood, returning the blood cells, which modifies the overactivity of the immune system. (Sanja Horvat et al., 2022)
Researchers believe there is an association between these conditions and inflammatory nerve damage, and modifying the immune system is beneficial for treating symptoms and the underlying disease.
Surgery
In some cases, surgical procedures can benefit individuals who have certain types of peripheral neuropathy. When another condition is exacerbating the symptoms or process of peripheral neuropathy, surgery may help relieve symptoms and prevent disease progression. This has proved effective when nerve entrapment or vascular insufficiency are factors. (Wenqiang Yang et al., 2016)
Complementary and Alternative Medicine
Some complementary and alternative approaches can help individuals cope with the pain and discomfort. These treatments can serve as an ongoing option for those who have chronic peripheral neuropathy. Options can include: (Nadja Klafke et al., 2023)
Acupuncture involves the placement of needles in specific areas of the body to help reduce pain symptoms.
Acupressure involves applying pressure on specific areas of the body to help reduce pain symptoms.
Massage therapy can help relax muscle tension.
Meditation and relaxation therapies can help manage symptoms.
Physical therapy can also serve as an important component of living with chronic peripheral neuropathy and recovering from acute peripheral neuropathy.
Physical therapy can help strengthen weak muscles, improve coordination, and learn how to adapt to sensory and motor changes to get around safely.
Individuals considering complementary or alternative treatment are encouraged to speak with their primary healthcare provider to determine whether it is safe for their condition. Injury Medical Chiropractic and Functional Medicine Clinic will work with the individual’s healthcare provider and/or specialists to develop an optimal health and wellness treatment solution to provide pain relief and improve quality of life.
Peripheral Neuropathy: A Successful Recovery Story
References
Enders, J., Elliott, D., & Wright, D. E. (2023). Emerging Nonpharmacologic Interventions to Treat Diabetic Peripheral Neuropathy. Antioxidants & redox signaling, 38(13-15), 989–1000. https://doi.org/10.1089/ars.2022.0158
Klafke, N., Bossert, J., Kröger, B., Neuberger, P., Heyder, U., Layer, M., Winkler, M., Idler, C., Kaschdailewitsch, E., Heine, R., John, H., Zielke, T., Schmeling, B., Joy, S., Mertens, I., Babadag-Savas, B., Kohler, S., Mahler, C., Witt, C. M., Steinmann, D., … Stolz, R. (2023). Prevention and Treatment of Chemotherapy-Induced Peripheral Neuropathy (CIPN) with Non-Pharmacological Interventions: Clinical Recommendations from a Systematic Scoping Review and an Expert Consensus Process. Medical sciences (Basel, Switzerland), 11(1), 15. https://doi.org/10.3390/medsci11010015
Überall, M., Bösl, I., Hollanders, E., Sabatschus, I., & Eerdekens, M. (2022). Painful diabetic peripheral neuropathy: real-world comparison between topical treatment with lidocaine 700 mg medicated plaster and oral treatments. BMJ open diabetes research & care, 10(6), e003062. https://doi.org/10.1136/bmjdrc-2022-003062
Horvat, S., Staffhorst, B., & Cobben, J. M. G. (2022). Intravenous Lidocaine for Treatment of Chronic Pain: A Retrospective Cohort Study. Journal of pain research, 15, 3459–3467. https://doi.org/10.2147/JPR.S379208
Yang, W., Guo, Z., Yu, Y., Xu, J., & Zhang, L. (2016). Pain Relief and Health-Related Quality-of-Life Improvement After Microsurgical Decompression of Entrapped Peripheral Nerves in Patients With Painful Diabetic Peripheral Neuropathy. The Journal of foot and ankle surgery: official publication of the American College of Foot and Ankle Surgeons, 55(6), 1185–1189. https://doi.org/10.1053/j.jfas.2016.07.004
For individuals dealing with chronic fatigue syndrome, can incorporating acupuncture with other treatment protocols help regain functionality and improve quality of life?
Acupuncture For Chronic Fatigue Syndrome
Research is looking at how acupuncture can help manage symptoms of chronic fatigue. These studies focused on specific acupoints and techniques and how they affected certain symptoms or abnormalities linked to the condition. The researchers found that acupuncture may help manage and alleviate some symptoms (Qing Zhang et al., 2019). However, they were still unable to determine the mechanisms of how acupuncture exactly works.
Symptom Relief
Various studies showed that acupuncture could improve physical and mental fatigue symptoms, including:
One case study showed improvements in groups of athletes who were put through a series of exhaustive physical exercises and short-term rest. One group of athletes was treated with acupuncture on selected acupoints while the others were given an extended rest. Analysis was applied to the metabolic profiles of urine samples collected from the athletes at three points: before the exercises, before and after the acupuncture treatment, or taking extended rest. The results indicated that the recoveries of disturbed metabolites in the athletes treated with acupuncture were significantly faster than in those who only took extended rest. (Haifeng Ma et al., 2015)
Researchers said studies involving acupuncture alone or in combination with other treatments appear to show that it is effective at lessening fatigue. (Yu-Yi Wang et al., 2014) However, further studies are needed to confirm the benefits. This is a significant change from a review that found limited evidence for the effectiveness of alternative treatments for relieving chronic fatigue symptoms. (Terje Alraek et al., 2011)
Another review of alternative therapies found acupuncture and certain meditation techniques showed the most promise for future investigation. (Nicole S. Porter et al., 2010)
Another study compared prednisone, a steroid, with an acupuncture technique called coiling dragon and an additional treatment called cupping. It suggested that acupuncture and cupping treatments surpassed the steroid regarding fatigue. (Wei Xu et al., 2012)
Another study found that needling with heat application or moxibustion produced better results than standard acupuncture regarding physical and mental fatigue scores. (Chen Lu, Xiu-Juan Yang, Jie Hu 2014)
From Consultation to Transformation: Assessing Patients In A Chiropractic Setting
References
Zhang, Q., Gong, J., Dong, H., Xu, S., Wang, W., & Huang, G. (2019). Acupuncture for chronic fatigue syndrome: a systematic review and meta-analysis. Acupuncture in medicine : journal of the British Medical Acupuncture Society, 37(4), 211–222. https://doi.org/10.1136/acupmed-2017-011582
Frisk, J., Källström, A. C., Wall, N., Fredrikson, M., & Hammar, M. (2012). Acupuncture improves health-related quality-of-life (HRQoL) and sleep in women with breast cancer and hot flushes. Supportive care in cancer : official journal of the Multinational Association of Supportive Care in Cancer, 20(4), 715–724. https://doi.org/10.1007/s00520-011-1134-8
Gao, D. X., & Bai, X. H. (2019). Zhen ci yan jiu = Acupuncture research, 44(2), 140–143. https://doi.org/10.13702/j.1000-0607.170761
Mandıroğlu, S., & Ozdilekcan, C. (2017). Impact of Acupuncture on Chronic Insomnia: A Report of Two Cases with Polysomnographic Evaluation. Journal of acupuncture and meridian studies, 10(2), 135–138. https://doi.org/10.1016/j.jams.2016.09.018
Zhu, L., Ma, Y., Ye, S., & Shu, Z. (2018). Acupuncture for Diarrhoea-Predominant Irritable Bowel Syndrome: A Network Meta-Analysis. Evidence-based complementary and alternative medicine : eCAM, 2018, 2890465. https://doi.org/10.1155/2018/2890465
Ma, H., Liu, X., Wu, Y., & Zhang, N. (2015). The Intervention Effects of Acupuncture on Fatigue Induced by Exhaustive Physical Exercises: A Metabolomics Investigation. Evidence-based complementary and alternative medicine : eCAM, 2015, 508302. https://doi.org/10.1155/2015/508302
Wang, Y. Y., Li, X. X., Liu, J. P., Luo, H., Ma, L. X., & Alraek, T. (2014). Traditional Chinese medicine for chronic fatigue syndrome: a systematic review of randomized clinical trials. Complementary therapies in medicine, 22(4), 826–833. https://doi.org/10.1016/j.ctim.2014.06.004
Alraek, T., Lee, M. S., Choi, T. Y., Cao, H., & Liu, J. (2011). Complementary and alternative medicine for patients with chronic fatigue syndrome: a systematic review. BMC complementary and alternative medicine, 11, 87. https://doi.org/10.1186/1472-6882-11-87
Porter, N. S., Jason, L. A., Boulton, A., Bothne, N., & Coleman, B. (2010). Alternative medical interventions used in the treatment and management of myalgic encephalomyelitis/chronic fatigue syndrome and fibromyalgia. Journal of alternative and complementary medicine (New York, N.Y.), 16(3), 235–249. https://doi.org/10.1089/acm.2008.0376
Lu, C., Yang, X. J., & Hu, J. (2014). Zhen ci yan jiu = Acupuncture research, 39(4), 313–317.
For individuals experiencing eye problems, can acupuncture treatment help and benefit overall eye health?
Acupuncture For Eye Health
Acupuncture is an alternative medical practice that involves inserting thin needles at specific points on the body. The objective is to restore balance and health by restoring and balancing energy circulation through pathways throughout the body. These pathways, known as meridians, are separate from nerve and blood pathways.
Studies have shown that the insertion of needles manipulates accumulations of certain neurotransmitters by nearby nerves and may be what causes beneficial health effects. (Heming Zhu 2014)
Scientists are not sure exactly how acupuncture works, but it has been shown to provide pain relief and alleviation of cancer treatment nausea. (Weidong Lu, David S. Rosenthal 2013)
Studies have shown that acupuncture can help treat eye conditions like dry eye syndrome. (Tae-Hun Kim et al., 2012)
Eye Problems
For some individuals, a body imbalance can be caused by eye problems or disease. With acupuncture, imbalance-causing symptoms are addressed. Acupuncture promotes the circulation of energy and blood around the eyes.
Acupuncture has been used as an alternative treatment for chronic dry eye syndrome. (Tae-Hun Kim et al., 2012)
Studies have shown acupuncture helps reduce the eye surface’s temperature to reduce the evaporation of tears.
The procedure is also sometimes used to treat glaucoma.
Glaucoma is an optic nerve disease usually caused by above-normal eye pressure levels.
Another study showed successful reduced allergic and inflammatory eye disease symptoms. (Justine R. Smith et al., 2004)
Eye Acupoints
The following acupoints are for eye health.
Jingming
Jingming – UB-1 is located in the inner corner of the eye.
This point is thought to increase energy and blood and to help with problems such as blurry vision, cataracts, glaucoma, night blindness, and conjunctivitis. (Tilo Blechschmidt et al., 2017)
Zanzhu
The Zanzhu point – UB-2 is in the crease at the inner end of the eyebrow.
This acupoint is used when individuals complain of headaches, blurred vision, pain, tearing, redness, twitching, and glaucoma. (Gerhard Litscher 2012)
Yuyao
Yuyao is in the middle of the eyebrow, above the pupil.
This point is used for treating eye strain, eyelid twitching, ptosis, or when the upper eyelid droops over, cloudiness of the cornea, redness, and swelling. (Xiao-yan Tao et al., 2008)
Sizhukong
The Sizhukog – SJ 23 area is in the hollow area outside the eyebrow.
It is thought to be a point where acupuncture can help with eye and facial pain, including headaches, redness, pain, blurred vision, toothache, and facial paralysis. (Hongjie Ma et al., 2018)
Tongzilia
The Tongzilia – GB 1 is located on the outside corner of the eye.
The point helps brighten the eyes.
Acupuncture also helps treat headaches, redness, eye pain, light sensitivity, dry eyes, cataracts, and conjunctivitis. (GladGirl 2013)
Early studies with acupuncture have shown promise for improving eye health. Individuals considering acupuncture are recommended to consult their primary healthcare provider to see if it can be an option for those who have not found a resolution by traditional means.
Neck Injuries
References
Zhu H. (2014). Acupoints Initiate the Healing Process. Medical acupuncture, 26(5), 264–270. https://doi.org/10.1089/acu.2014.1057
Lu, W., & Rosenthal, D. S. (2013). Acupuncture for cancer pain and related symptoms. Current pain and headache reports, 17(3), 321. https://doi.org/10.1007/s11916-013-0321-3
Kim, T. H., Kang, J. W., Kim, K. H., Kang, K. W., Shin, M. S., Jung, S. Y., Kim, A. R., Jung, H. J., Choi, J. B., Hong, K. E., Lee, S. D., & Choi, S. M. (2012). Acupuncture for the treatment of dry eye: a multicenter randomised controlled trial with active comparison intervention (artificial teardrops). PloS one, 7(5), e36638. https://doi.org/10.1371/journal.pone.0036638
Law, S. K., & Li, T. (2013). Acupuncture for glaucoma. The Cochrane database of systematic reviews, 5(5), CD006030. https://doi.org/10.1002/14651858.CD006030.pub3
Smith, J. R., Spurrier, N. J., Martin, J. T., & Rosenbaum, J. T. (2004). Prevalent use of complementary and alternative medicine by patients with inflammatory eye disease. Ocular immunology and inflammation, 12(3), 203–214. https://doi.org/10.1080/092739490500200
Blechschmidt, T., Krumsiek, M., & Todorova, M. G. (2017). The Effect of Acupuncture on Visual Function in Patients with Congenital and Acquired Nystagmus. Medicines (Basel, Switzerland), 4(2), 33. https://doi.org/10.3390/medicines4020033
Litscher G. (2012). Integrative laser medicine and high-tech acupuncture at the medical university of graz, austria, europe. Evidence-based complementary and alternative medicine : eCAM, 2012, 103109. https://doi.org/10.1155/2012/103109
Tao, X. Y., Sun, C. X., Yang, J. L., Mao, M., Liao, C. C., Meng, J. G., Fan, W. B., Zhang, Y. F., Ren, X. R., & Yu, H. F. (2008). Zhongguo zhen jiu = Chinese acupuncture & moxibustion, 28(3), 191–193.
Can individuals with jaw pain find relief in acupuncture therapy to reduce pain and improve jaw mobility in the upper body portions?
Introduction
The head is part of the upper musculoskeletal body quadrant supported by the neck area, which consists of the skull, various muscles, and vital organs that provide stability, mobility, and functionality. Around the head, the different facial features include the mouth, nose, eyes, and jaw to allow the host to eat, speak, smell, and see. While the head provides sensory and motor function, the neck includes motor stability to ensure no injuries or trauma affect the head. Located below the eyes is the jaw, which allows motor function with various muscles and joints to hyperextend without pain or discomfort. However, multiple factors can affect the jaw muscles and joints to invoke pain and discomfort, which can cause radiating referred pain down to the neck muscles. Today’s article looks at how jaw pain can affect the upper body, how non-surgical treatments can help with jaw pain, and how treatments like acupuncture can help restore jaw mobility. We talk with certified medical providers who consolidate our patients’ information to provide treatments to reduce jaw pain affecting their jaw and neck area. We also inform and guide patients on how acupuncture and non-surgical treatments can benefit many individuals with pain correlating with the jaw. We encourage our patients to ask their associated medical providers intricate and important questions about how their pain affects their quality of life and reduces jaw pain. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
Jaw Pain Affecting The Upper Body
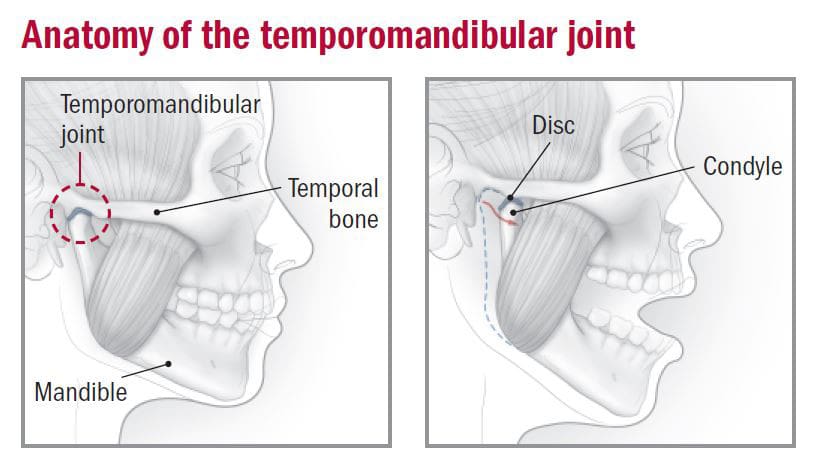
Do you feel muscle soreness in your jaw and neck muscles throughout the day? Have you constantly rubbed or massaged your jaw muscles to reduce tension? Or have you been dealing with headaches or neck pain continually that affects your daily routine? Many individuals experiencing these pain-like symptoms are dealing with jaw pain or TMJ (temporomandibular joint syndrome). The jaw consists of mastication muscles on each side that help provide various functions like chewing, swallowing, or talking. When multiple traumatic or ordinary factors start to affect the jaw, it can disrupt the sensory-motor function of the upper body. For individuals, jaw pain is common worldwide, and with TMJ, it can become an issue as the pain seems to affect the jaw’s motor control while being accompanied by restricted mouth opening and impaired max bite force. (Al Sayegh et al., 2019) Additionally, TMJ affects not only the mastication muscles but also the temporomandibular joint, the joint that connects the jaw to the skull, which becomes inflamed and causes more issues.
So, how would TMJ affect the upper body? Well, when TMJ affects the mastication muscles and the temporomandibular joint, many individuals will experience various symptoms like:
Difficulty moving mouth when chewing
Popping/cracking sensation when opening or closing the jaw
Headaches/Migraines
Ear pain
Tooth pain
Neck and shoulder pain
This causes myofascial and intraarticular disorders that affect the muscles and joints of the jaw, which are linked to the skull. (Maini & Dua, 2024) To that point, many individuals will be experiencing referred pain, thinking they are dealing with a toothache when it is due to trigger points in the mastication muscles. This is when TMJ is accompanied by muscle-joint pain in the neck or upper back or if teeth issues accompany TMJ, but it depends on the individual and situation they are under. However, numerous treatments can reduce jaw pain and its associated symptoms that affect the jaw and the neck.
The Non-Surgical Approach To Wellness- Video
Non-Surgical Treatments For Jaw Pain
When reducing jaw pain, many individuals seek treatment to minimize the pain-like effects and regain mobility back to their jaws. It can be challenging and complex when people are dealing with jaw pain. It is a multifactorial issue that can affect the neck and back areas. So, when people speak with their primary doctors about their jaw pain, they will get an evaluation of where their pain is located and if they have any complaints correlating with the jaw pain. Afterward, many doctors will refer to musculoskeletal specialists to relieve the jaws’ pain. Treatments and techniques used by chiropractors, massage therapists, and physiotherapists can help ease the inflamed and tense mastication muscles. Techniques like soft tissue mobilization can help relax the masticatory muscles by lengthening them to the extent of releasing the trigger points in the muscles. (Kuc et al., 2020) At the same time, physiotherapy can help the jaw muscle through various relaxing techniques to increase the range of motion while strengthening the jaw to reduce pain and stress. (Byra et al., 2020) Many of these treatments are non-surgical, which means they are non-invasive and effective for the person’s pain while affordable.
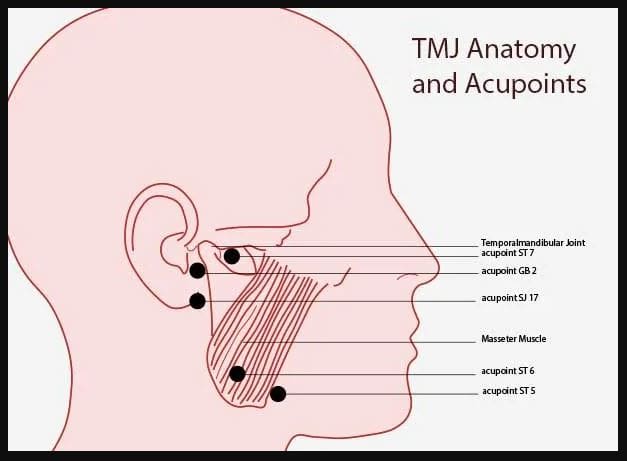
Acupuncture To Restore Jaw Mobility
When it comes to non-surgical treatments, one of the oldest forms is acupuncture, which can help reduce the pain-like effects of jaw pain and restore mobility. Acupuncture originates from China, and highly trained medical professionals use thin, solid needles to be placed in acupoints on the body to disrupt the pain signal and provide relief. For jaw pain, acupuncturists will put needles on the acupoints of the jaw or the surrounding muscles to reduce mechanical hypersensitivity of the nerve cells that are causing pain while improving the sensory-motor function with a positive response. (Teja & Nareswari, 2021) Additionally, when dealing with ear pain associated with TMJ affecting the neck muscles, acupuncture can help enhance the neck’s range of motion by placing the needles on the trigger points of the cervical muscles. (Sajadi et al., 2019) When acupuncture treatment helps many individuals with jaw pain affecting their necks and heads, they can provide beneficial, positive results through consecutive treatment and improve jaw mobility function.
References
Al Sayegh, S., Borgwardt, A., Svensson, K. G., Kumar, A., Grigoriadis, A., & Christidis, N. (2019). Effects of Chronic and Experimental Acute Masseter Pain on Precision Biting Behavior in Humans. Front Physiol, 10, 1369. https://doi.org/10.3389/fphys.2019.01369
Byra, J., Kulesa-Mrowiecka, M., & Pihut, M. (2020). Physiotherapy in hypomobility of temporomandibular joints. Folia Med Cracov, 60(2), 123-134. https://www.ncbi.nlm.nih.gov/pubmed/33252600
Kuc, J., Szarejko, K. D., & Golebiewska, M. (2020). Evaluation of Soft Tissue Mobilization in Patients with Temporomandibular Disorder-Myofascial Pain with Referral. Int J Environ Res Public Health, 17(24). https://doi.org/10.3390/ijerph17249576
Sajadi, S., Forogh, B., & ZoghAli, M. (2019). Cervical Trigger Point Acupuncture for Treatment of Somatic Tinnitus. J Acupunct Meridian Stud, 12(6), 197-200. https://doi.org/10.1016/j.jams.2019.07.004
Teja, Y., & Nareswari, I. (2021). Acupuncture Therapies for Addressing Post Odontectomy Neuropathy. Med Acupunct, 33(5), 358-363. https://doi.org/10.1089/acu.2020.1472
Individuals that engage in heavy exercise can develop heat cramps from overexertion. Can knowing the causes and symptoms help prevent future episodes from happening?
Heat Cramps
Heat cramps can develop during exercise from overexertion or prolonged exposure to high temperatures. The muscle cramps, spasms, and pain can range from mild to severe.
Electrolytes like sodium, calcium, and magnesium are important for properly functioning muscles, including the heart. The primary role of sweating is to regulate the body’s temperature. (MedlinePlus. 2015) Sweat is mostly water, electrolytes, and sodium. Excessive sweating from physical activity and exertion or a hot environment can cause electrolyte imbalances that lead to cramps, spasms, and other symptoms.
Causes and Activities
Heat cramps most commonly affect individuals who sweat excessively during strenuous activity or are exposed to hot temperatures for prolonged periods. The body and organs need to cool down, which causes sweat production. However, too much sweating can lead to dehydration and electrolyte depletion. (Centers for Disease Control and Prevention. 2022)
Age – Children and adults 65 years and older have the highest risk.
Excessive sweating.
Low sodium diet.
Preexisting Medical Conditions – heart disease, diabetes mellitus, and obesity are conditions that can increase the risk of muscle cramping.
Medications – blood pressure, diuretics, and antidepressants can affect electrolyte balance and hydration.
Alcohol consumption.
Self-Care
If heat cramps begin, immediately stop the activity and look for a cool environment. Rehydrate the body to replenish the fluid loss. Staying hydrated and drinking fluids regularly during intense activity or in a hot environment can help prevent the body from cramping. examples of beverages that increase electrolytes include:
Gently applying pressure and massaging affected muscles can help reduce pain and spasms. As symptoms resolve, it is recommended to not return to strenuous activity too soon because additional exertion can progressively lead to heatstroke or heat exhaustion. (Centers for Disease Control and Prevention. 2021) Heatstroke and heat exhaustion are two heat-related illnesses. (Centers for Disease Control and Prevention. 2022)
Heatstroke is when the body loses the ability to regulate temperature and can cause dangerously high temperatures.
Heat exhaustion is the body’s response to excessive fluid and electrolyte loss.
The majority of heat cramps develop during activities because of the exertion and sweating, causing more electrolytes to be lost and the body to become more dehydrated.
Symptoms can also develop minutes to hours after activity has ceased.
Duration
Most heat-related muscle cramps will resolve with rest and hydration within 30–60 minutes.
If muscle cramping or spasms do not subside within one hour, seek professional medical attention.
For individuals with heart conditions or on a low-sodium diet who develop heat cramps, regardless of duration, medical help is necessary to ensure there are no complications.
Drink plenty of fluids before and during physical activities.
Avoid alcohol and caffeinated beverages.
Avoid exercising or exposure to extreme heat during peak sunlight hours.
Avoid tight and dark-colored clothing.
Assessing Patients In A Chiropractic Setting
References
Gauer, R., & Meyers, B. K. (2019). Heat-Related Illnesses. American family physician, 99(8), 482–489.
Centers for Disease Control and Prevention. (2022). Heat stress — heat related illness. The National Institute for Occupational Safety and Health (NIOSH) Retrieved from https://www.cdc.gov/niosh/topics/heatstress/heatrelillness.html#cramps
MedlinePlus. (2015). Sweat. Retrieved from https://medlineplus.gov/sweat.html#cat_47
FoodData Central. (2019). Nuts, coconut water (liquid from coconuts). Retrieved from https://fdc.nal.usda.gov/fdc-app.html#/food-details/170174/nutrients
FoodData Central. (2019). Milk, nonfat, fluid, with added vitamin A and vitamin D (fat free or skim). Retrieved from https://fdc.nal.usda.gov/fdc-app.html#/food-details/746776/nutrients
Centers for Disease Control and Prevention. (2012). Frequently asked questions (FAQ) about extreme heat. Retrieved from https://www.cdc.gov/disasters/extremeheat/faq.html
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine