A doctor will rule out these causes to make a proper diagnosis.
Diagnosing
A doctor utilizes medical history and physical exam to diagnose coccydynia.
Imaging scans are usually not necessary, but a doctor may order:
Computed tomography (CT) scan
Magnetic resonance imaging (MRI) scan
If they believe a separate:
Bone
Nerve
Tissue
Problem to be the cause of tailbone pain.
Medical history is important, a doctor wants to know if a
Fall
Accident
Recent trauma
Might have caused the pain.
A physical exam is next in line along with symptoms.
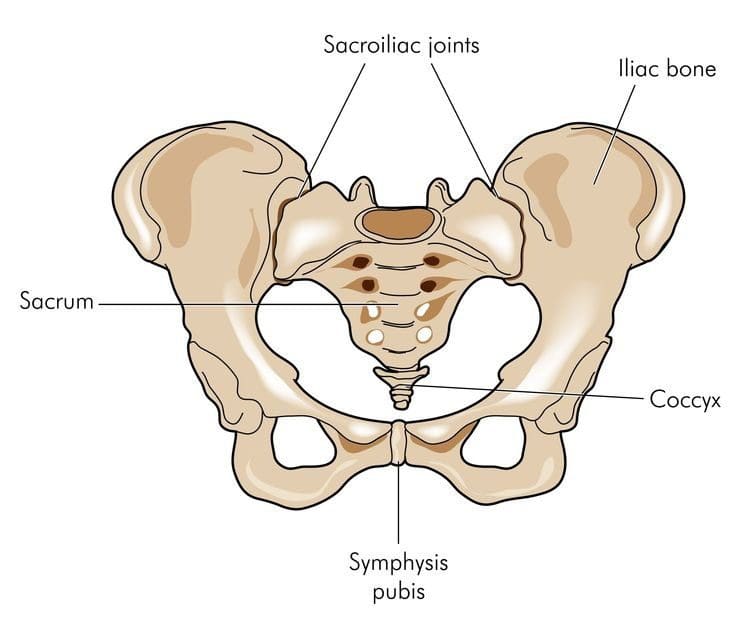
The pain is usually localized in the tailbone, making it straightforward to diagnose.
A doctor will want to know if the pain strikes when sitting or leaning back and which is worse.
A doctor might ask the patient to point to where they’re feeling the pain.
Pointing could be enough for the doctor to tell if the pain is coccydynia when compared to other low back pain conditions.
The doctor will want to palpate the tailbone area for signs of inflammation.
Non-surgical Treatment
Conservative treatment is extremely effective for coccydynia.
Ninety percent of people experience pain reduction using non-surgical means or any medical intervention.
It is first treated with noninvasive methods:
Ice or heating pad can help provide immediate, short-term relief.
Donut/Wedge cushion provides extra padding taking the pressure off the coccyx when sitting. These cushions are available at pharmacies.
Avoid sitting for long times, like a long flight will help prevent additional pain and injury.
Rest is very important to help avoid further injury during recovery.
If there is still pain after these therapies, a doctor may recommend over-the-counter or prescription-strength non-steroidal anti-inflammatory drugs (NSAIDs) or other pain medications.
If the medication doesn’t work then a doctor may try cortisone injection or local spine blocker to send strong medicine directly to the tailbone area.
Surgical Procedure
If none of the conservative treatments work then surgery could be the next step.
The procedure is called a coccygectomy, which means the removal of the tailbone.
A surgeon will discuss the procedure in great detail before it is performed.
These risks include:
Infection
Hematoma (abnormal collection of blood outside an artery or vein)
Perineal hernia (weakened pelvic muscles)
Chronic Coccydynia
A small portion of people can develop chronic coccydynia, which means the pain lasts for more than 2 months.
Chronic coccydynia can take a major toll on the quality of life. Talk to a doctor if symptoms are not resolving.
They may refer you to a doctor that specializes in coccydynia management.
Protecting the Tailbone
There is no exact way or method to prevent coccydynia,
However, reducing the risk of tailbone pain can be achieved by using caution when participating in sports like:
Skating – Ice, Inline, and Roller
Biking
Horseback riding
And take extra care when walking on icy/slippery/hazardous conditions so nobody falls.
El Paso, TX Severe Back Pain Chiropractic Treatment
Gale Grijalva suffered from acute back pain because of an automobile incident injury. Where it was once very tough to do her routine daily tasks, Gale Grijalva is now able to take part in physical activities she was not able to engage in earlier thanks to Dr. Alex Jimenez, a chiropractor in El Paso, TX. Gale Grijalva clarifies how patient Dr. Jimenez is and she discusses how completely he’s been able to help her, such as answering any concerns she might have.
Severe chronic back pain is a serious, recurring condition that affects an individual’s everyday life. Back pain lasting over three weeks is deemed chronic. The backbone is an essential component of the body. Severe chronic back pain might be the backbone’s way of telling the body that there’s a problem. The spine consists of bony vertebrae, soft spinal discs, facet joints, tendons, ligaments, and tendons. Within the bony vertebral artery lies that the spinal cord, the delicate but effective nerve pathway of the central nervous system.
NCBI Resources
Before you run screaming in horror to the medicine cabinet, one of the best reasons to participate in chiropractic treatment is that it helps reduce the chance of a recurrence. By working on the total body and getting it in the best shape possible, the patient is stronger and more balanced to handle their workload and other strenuous activities. Chiropractors also impart advice on how to minimize the chances of re-aggravating the lower back.
Millions of people suffer from back pain each year, and some never visit a chiropractor. Those who do choose�chiropractic treatment�are privy to treatment that reduces their pain, increases healing, shortens their downtime and lessens their chances of a recurrence. If over the counter medication and ice packs haven�t worked within a few days, it�s time to make an appointment for a consultation with a licensed chiropractor. You will be happy you did.
Sciatica doesn�t have to prevent you from being able to travel.
Sometimes a journey can create a series of challenges for people with sciatic nerve pain in the low back and leg.
A common issue among individuals is to prevent sciatica from flaring up when on the road or in the air.
A solution for this is to find ways to keep moving. However, easier said than done, but it can be done!
Flying and driving often mean long periods of sitting and sitting in a position typically not friendly with sciatic pain.
“When we drive or fly for an extended trip, it means long sitting times, and sitting in a position that can cause sciatica to flare up at any time,” says Dr. Alexander Jimenez, D.C. in El Paso, Texas, and member of the American Chiropractic Association (ACA).
Dr. Jimenez shares some basic tips for keeping mobility up, all the while pain-free, when flying and driving with sciatica.
He also offers additional advice to keep radiating pain from starting, upon arrival.
Flying with Sciatica
Sciatica pain radiates through the lower body meaning:
The low back
Hips
Buttocks
Legs
So when a flight anchors you to a seat, this can aggravate the area and cause pain.
The first thing to consider is the seat choice.
An aisle seat allows you the easiest access out of the seat, allowing you to move more during the flight.
Also when flying with sciatica, tell the flight crew about your condition.
When the seatbelt off light comes on, get up, stretch your legs and move around anywhere you can find room.
With a good portion of the population suffering from sciatica, most crews have seen people with this condition, and will usually let you do some stretching if they’re not busy.
A good sciatica stretch is to put your hands on something stable and do some deep knee bends.
This will use the upper body weight to stretch the lumbar spine comfortably.
Do a few and make sure you feel and return to your seat stretched and refreshed.
When taking a long flight, do this every hour to feel better when landing.
Sciatica Road Trip
Road trips, on the other hand, are easier to stop and move around. However, it can also create over-concentration on the drive and forgetting how much you are hurting until the pain is unbearable.
Dr. Jimenez advises frequentstops, if possible every hour is best to prevent pain.
On the stops walk two or three laps around the car/Suv/truck.
Rear bumper stretching prop
Place one foot on the bumper, and the other a few feet behind, lean into the bumper and square the hips with the lead foot.
This is like a hurdle stretch.
Stretch both legs on each break.
Regular stretching helps relieve the pressure on the low back so you can drive comfortably.
Arrival
Packing light is a healthy tip because hauling heavy luggage will aggravate sciatic nerve pain.
There are a few things that Dr. Jimenez recommends packing or getting upon arrival.
Gel ice pack you can keep in the refrigerator or freezer in a hotel.
Apply the cold pack to the low back for 20-minute increments will go a long way toward relieving pain.
Topical agent/cream/gel that has menthol or camphor, that you can apply to any area of tenderness or pain before the ice gel pack.
This increases the ice pack’s power by helping relax muscles and decreasing pain.
Supportive shoes or custom foot orthotics
People with sciatica should choose footwear or orthotics that support all three arches of the foot.
Leg length is usually not equal on each side, and proper arch supports can be custom made for you by your chiropractor to compensate for the difference.
Even a 5mm difference can cause chronic back pain.
And if possible, ask your chiropractor or primary physician if they can recommend a chiropractor, physical/massage therapist,� or acupuncturist that you can see in case you need emergency treatment.
This can give you some peace of mind.
Keep Your Exercise/Stretching Routine When Traveling
When we travel especially on vacations it can be easy to let healthy lifestyle habits you practice at home slide.
All are sciatica�s natural enemies make sure to bring these healthy practices with you to your destination.
Use the same good sense when you travel just like at home getting:
Get plenty of rest
Drink plenty of water
Don’t overeat
You will need more rest when you travel and don’t forget when you travel to:
Walk
Stretch
Stay mobile
Difference Foot Orthotics Make to *REDUCE FOOT PAIN* & Correct Posture | El Paso, TX (2019)
Custom made foot orthotics can help control foot motion and posture. Healthcare professionals prescribe custom foot orthotics to help patients focus on their foot posture and mobility control. Research studies have ascertained that using custom foot orthotics for posture and mobility control can help fix excessive foot pronation and supination to prevent a variety of foot health problems. The subsequent video describes how custom foot orthotics will help control foot posture and mobility to improve health and wellness.
NCBI Resources
Sciatica is generally caused by the compression of lumbar or sacral nerves or by compression of the sciatic nerve. When sciatica is caused by compression of a dorsal nerve root, it’s known as lumbar radiculopathy. This can occur because of a spinal disk bulge or spinal disk herniation (a herniated intervertebral disc), or by roughening, enlarging, or misalignment (spondylolisthesis) of the fascia, or as a consequence of degenerated discs which can reduce the diameter of the lateral foramen by which nerve roots exit the spine.
Myofascial syndrome, what is it? You’re probably thinking I don’t have that, but more than likely, you have.
Myo means muscle and fascia refer to the tissue bands that cover and connect the muscles/organs.
Tightness
Twitching areas
Painful knots
In the neck/back, then myofascial pain syndrome could be the cause.
Myofascial syndrome is a very common condition. It affects about 44 million people in the United States.
Trigger Points The Areas Where Pain Can Develop
Myofascial pain is associated with trigger points. These are areas that can become tender and stiff inside muscle tissue that reduce the range of motion.
Myofascial pain syndrome can happen when you have several active trigger points.
Trigger points are often referred to as knots because they feel tight and balled up compared to the softer relaxed surrounding muscle/s.
If the muscle becomes tight, it can cut off its blood supply, that can trigger:
Muscle tenderness
Pain
Spasm
Tightness
Trigger points can form all over the body which includes:
Neck
Mid-back
Low back
Common characteristics of trigger points are that they cause pain that travels or spreads to the surrounding area. For example, shoulder pain can radiate across the upper back.
The muscles can also twitch when touched.
Pretty much everyone has trigger points, but not all triggers cause symptoms.
Dormant or latent��trigger points can reduce the range of motion but only cause pain when directly palpated or compressed,
Active trigger points are painful any time, even when at rest.
Lifestyle factors like:
Stress
Poor posture
Can make a dormant trigger point become active.
Trigger Point Causes in the Spine
Spinal injury or trauma can result in myofascial pain syndrome, but lifestyle factors usually have a hand in the condition.
Poor posture over a long period, for example, sleeping in an awkward position can cause physical muscular stress on the spinal muscles.
Mental and emotional stress can present itself through muscle tension that helps the development of trigger points.
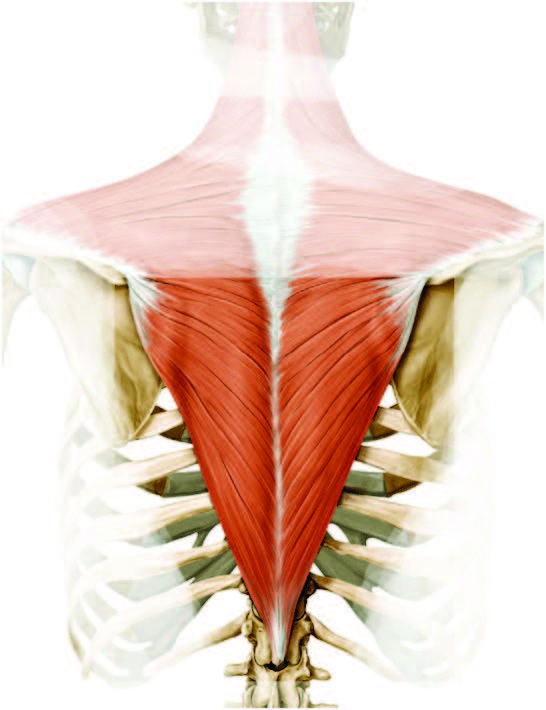
The trapezius muscle, that extends from the back of the neck down the shoulders and upper back, is the most common site of spinal trigger points and myofascial pain because of the significant amount of pressure that the muscle has to bear and its susceptibility to whiplash.
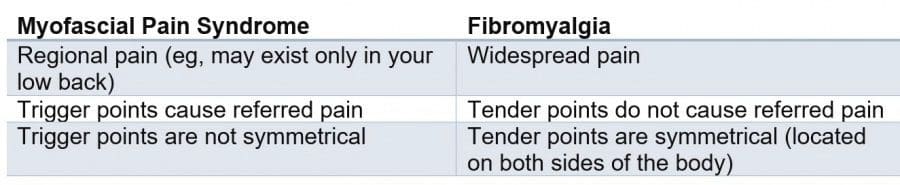
The Difference Myofascial Syndrome and Fibromyalgia
Because myofascial syndrome is linked to triggering points, fibromyalgia and its tender points bring out a comparison of the two.
Myofascial pain syndrome and fibromyalgia are two distinct conditions, and the table below outlines the primary differences.
Because they are unique conditions, there is a possibility to develop both conditions.
Doctor(s) can help craft a treatment approach that addresses the pain of both trigger points and tender points.
Diagnosis can be difficult
Myofascial pain syndrome is common but can be difficult to diagnose.
The challengingreasons behind diagnosing include:
Scientists are not sure how these trigger points cause pain.
The condition is often confused for other spinal disorders and conditions.
An example is having low back pain caused by myofascial syndrome in the lumbar spine. But low back pain brought on by arthritis can cause similar pain. That’s when the cause needs to be carefully and properly assessed.
There is no standard test for myofascial pain syndrome diagnosis yet.
There�s no standard diagnosing protocol but manual palpation or use of the hands to feel for:
Tenderness
Twitching
Tightness around the area
Is the most common way doctors diagnose the condition.
Some doctors might only utilize manual palpation but ultrasound is emerging as a diagnostic tool for myofascial pain syndrome.
Ultrasound produces clean images of the soft tissues and shows the active trigger points.
However, more research is needed to secure its place as a diagnostic method and tool.
A personal or primary care doctor can diagnose myofascial syndrome, but they may refer you to a pain specialist or a spine specialist like:
Doctors and researchers are still learning about myofascial syndrome, therefore, treatment options differ from doctor to doctor.
But most doctors do support a multidisciplinary treatment approach that is, using a variety of therapies and employing lifestyle changes to manage trigger point pain and prevent it from coming back.
Below are common treatments for myofascial pain syndrome.
Release Therapy
Myofascial release is a broad treatment option that consists of manual or instrument-guided therapydesigned to release the muscles and fascia by use of applying pressure.
Practitioners and clinicians are trained in myofascial release therapy, including:
Massage therapists
Physical therapists
Chiropractors
Physiatrists
The goal is the same:
Put pressure on the trigger point and release it.
Myofascial release technique might sound like a massage, but it is a distinct method compared to massage.
Massage moves muscles up and down,� myofascial release utilizes direct pressure into the stiff fascia and muscle.
Repeated pressure on the tight areas is not soothing, and patients tell of soreness during and after the treatment.
Once the trigger point loosens up, blood flow and nerve function begin to return to the area.
Then the pain is gone, hallelujah!
Additional Care Options
Myofascial release therapy is just one option for trigger point pain.
Other common treatments to manage spine-related pain include:
Home
If you know the location of the trigger points you can treat them at home with simple tools.
Rolling the trigger point over a:
Foam roller
Golf ball
Tennis ball
Can help loosen any of the tight areas.
Over-the-counter medication
If doctor-approved, then taking an over-the-counter pain reliever like acetaminophen (Tylenol) or ibuprofen (Motrin, Advil) can help with spine pain and allow daily activities.
Physical therapy
Physical therapy like:
Massage
Chiropractic
Heat
Electrical stimulation
Ultrasound
There are also stretches/exercises to keep muscles warm and flexible to help any future trigger points from forming.
Massage therapy
Licensed massage therapists practice myofascial release therapy, but also include other forms of massage
Deep tissue massage
Swedish massage
Can also help relieve trigger point pain.
Massage can also help to relax, and this is very important in preventing myofascial pain syndrome.
Also, learn how to keep stress and anxiety in check, and avoid tension that can turn into trigger points.
Dry needling/acupuncture
While both therapies use needles, dry needling and acupuncture are different treatments that can reduce the pain.
There is not a lot of research on dry needling like acupuncture, but it can help increase blood flow to the trigger point area.
Acupuncture means inserting needles into specific points on the body.
These needles help stimulate the body’s energy and help in sending signals to the nervous system to release chemicals into the body to help with the pain, which means less pain.
Trigger point injections
If any of these treatments don’t seem to be working, then you might want to talk to your doctor about trigger point injections.
Many people who have trigger points or myofascial pain syndrome in their spine have knots and tightness throughout their back and neck.
To prevent myofascial pain syndrome one needs to practice a healthy lifestyle that promotes good spine health.
Stretching and exercising regularly can help keep stress under control and prevent tension from building up, which makes it harder for trigger points to activate and cause pain.
El Paso Chiropractic Back Pain Therapy
Andres “Andy” Martinez first came to see Dr. Alex Jimenez in Push Fitness after undergoing back pain and knee issues. Following a period of physical therapy and rehabilitation, Andy became engaged in Crossfit, where he learned everything he needed to know about health and wellness from the coaches at Push. Andres Martinez expresses how grateful he is to receive the amount of care he does against the staff and he clarifies how much his perspective of fitness has shifted from the first time he walked into Push Fitness. Andy has seen a family at Push who led him to a healthy, clean life and both the trainers and staff mean everything to Andres Martinez.
NCBI Resources
The knots you have probably felt in your muscles or had others identify are also known as trigger points. These tight spots are often sensitive to the touch and can be found in any muscle in your body. As they develop, they may produce symptoms like numbness, burning, weakness, pain, and tingling. Trigger points are caused by trauma to the body, such as an accident in a car or during athletics. They can also be caused by more mild, long-term trauma, such as working at a desk without proper ergonomics or making a repetitive motion over a long period of time. Chiropractors are not only good at finding trigger points, but they are also good at treating them.
The human nervous system is made up of two parts: the central nervous system, which includes the brain and the spinal cord, and the peripheral nervous system, which includes the connection nerves running from the brain and the spinal cord to the rest of the human body, including the hands and the feet.
Many patients with neuropathy may experience a variety of painful symptoms due to nerve damage or injury. But, with the proper treatment approach, neuropathy can be effectively treated and even reversed. Diagnosis of neuropathy is fundamental towards proper treatment. Dr. Alex Jimenez, a chiropractor in El Paso, TX, can help patients with neuropathy.
Peripheral Neuropathy Causes & Symptoms | El Paso, TX (2019)
Neuropathy is a medical term used to describe a collection of general diseases or malfunctions which affect the nerves. The causes of neuropathy, or nerve damage, can vary greatly among each individual and these may be caused by a number of different diseases, injuries, infections, and even vitamin deficiency states. However, neuropathy can most commonly affect the nerves that control the motor and sensory nerves. Because the human body is composed of many different kinds of nerves which perform different functions, nerve damage is classified into several types.
Neuropathy can also be classified according to the location of the nerves being affected and according to the disease-causing it. For instance, neuropathy caused by diabetes is called diabetic neuropathy. Furthermore, depending on which nerves are affected will depend on the symptoms that will manifest as a result. Below we will discuss several specific types of neuropathies clinically treated by chiropractors, physical therapists and physical medicine doctors alike, as well as briefly describing their causes and their symptoms.
Peripheral neuropathy, which is often simply referred to as �neuropathy,� is a state that happens when your nerves become damaged or injured, oftentimes simply disrupted. It�s estimated that neuropathy affects roughly 2.4 percent of the general populace and approximately 8 percent of people older than age 55. However, this quote doesn�t include people affected by neuropathy caused by physical trauma to the nerves.
Types
Neuropathy can affect any of the three types of peripheral nerves:
Sensory nerves, which transmit messages from the sensory organs, eyes, nose to the brain
Motor nerves, which track the conscious movement of the muscles
Autonomic nerves, which regulate the involuntary functions of the body
Sometimes, neuropathy will only impact one nerve. This is medically referred to as mononeuropathy and instances of it include:
Ulnar neuropathy, which affects the elbow
Radial neuropathy, which affects the arms
Peroneal neuropathy, which affects the knees
Femoral neuropathy, which affects the thighs
Cervical neuropathy, which affects the neck
Sometimes, two or more isolated nerves in separate regions of the body can become damaged, injured or disrupted, resulting in mono neuritis multiplex neuropathy. Most often, however, multiple peripheral nerves malfunction at the same time, a condition called polyneuropathy. According to the National Institute for Neurological Disorders and Stroke, or the NINDS, there are over 100 kinds of peripheral neuropathies.
Causes
Neuropathies are often inherited from birth or they develop later in life. The most frequent inherited neuropathy is the neurological disease Charcot-Marie-Tooth disease, which affects 1 in 2,500 people in the USA. Although healthcare professionals are sometimes not able to pinpoint the exact reason for an acquired neuropathy, medically referred to as idiopathic neuropathy, there are many known causes for them, including systemic diseases, physical trauma, infectious diseases, and autoimmune disorders.
A systemic disease is one which affects the whole body. The most frequent systemic cause behind peripheral neuropathy is diabetes, which can lead to chronically high blood glucose levels that harm nerves.
Other systemic issues can cause neuropathy, including:
Kidney disorders, which permit high levels of nerve-damaging toxic chemicals to flow in the blood
Toxins from exposure to heavy metals, including arsenic, lead, mercury, and thallium
Certain drugs and/or medications, including anti-cancer medications, anticonvulsants, antivirals, and antibiotics
Chemical imbalances because of liver ailments
Hormonal diseases, including hyperthyroidism, which disturbs metabolic processes, potentially inducing cells and body parts to exert pressure on the nerves
Deficiencies in vitamins, such as E, B1 (thiamine), B6 (pyridoxine), B12, and niacin, that can be vital for healthy nerves
Alcohol abuse, which induces vitamin deficiencies and might also directly harm nerves
Cancers and tumors that exert damaging pressure on nerve fibers and pathways
Chronic inflammation, which can damage protective tissues around nerves, which makes them more vulnerable to compression or vulnerable to getting inflamed and swollen
Blood diseases and blood vessel damage, which may damage or injure nerve tissue by decreasing the available oxygen supply
Signs and Symptoms of Neuropathy
Depending on the reason and unique to each patient, signs, and symptoms of neuropathy can include:
Pain
Tingling
Burning/prickling sensations
Increased sensitivity to touch
Muscle weakness
Temporary or permanent numbness;
Paralysis
Dysfunction in glands or organs
Impairment in urination and
Sexual function
Such signs and symptoms are dependent on whether autonomic, sensory, or motor nerves, as well as a combination of them, are ultimately affected. Autonomic nerve damage can influence physiological functions like blood pressure or create gastrointestinal problems and issues. Damage or dysfunction in the sensory nerves may impact sensations and sense of equilibrium or balance, while harm to motor nerves may affect movement and reflexes. When both sensory and motor nerves are involved, the condition is known as sensorimotor polyneuropathy.
Complications
Peripheral�neuropathy�may result in several complications, as a result of disease or its symptoms. Numbness from the ailment can allow you to be less vulnerable to temperatures and pain, making you more likely to suffer from burns and serious wounds. The lack of sensations in the feet, for instance, can make you more prone to developing infections from minor traumatic accidents, particularly for diabetics, who heal more slowly than other people, including foot ulcers and gangrene.
Furthermore, muscle atrophy may cause you to develop particular physical disfigurements, such as pes cavus, a condition marked by an abnormally high foot arch, and claw-like deformities in the feet and palms.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
Neuropathy can be caused by a variety of injuries and/or aggravated conditions, often manifesting into a plethora of associated signs and symptoms. While every type of neuropathy, such as diabetic neuropathy or autoimmune disease-associated neuropathy, develops its own unique group of signs and symptoms, many patients will often report common complaints. Individuals with neuropathy generally describe their pain as stabbing, burning or tingling in character.
If you experience unusual or abnormal tingling or burning sensations, weakness and/or pain in your hands and feet, it�s essential to seek immediate medical attention in order to receive a proper diagnosis of the cause of your specific signs and symptoms. Early diagnosis may help prevent further nerve injury. Visit http://www.neuropathycure.org�for more details.
What exercise/stretches help reduce sciatic nerve pain?
Here are 4 exercise/stretches that your chiropractor/physical therapist may recommend to help you reduce sciatic nerve pain:
Pelvic tilt
Knee to chest
Lower trunk rotations
Arm and leg extensions
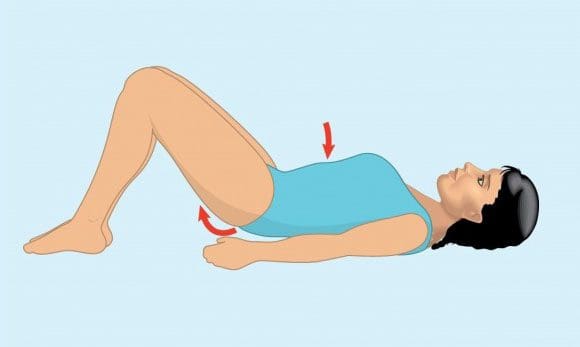
Pelvic Tilt
Its purpose is to strengthen the lower abdominal muscles and stretch the lower back.
How to do it:
Lie on back
Exhale and tighten abdominal muscles while pushing the belly button toward the floor and flatten the lower back
Hold the position for 5 seconds
Repeat 10 times holding the position for 5 seconds each
Am I doing it right?
Place the pinky finger on the hip bone and thumb on the lowest rib (same side).
When tightening the abdominal muscles, the amount of space between the pinky finger and thumb should get smaller.
Pelvic tilts help strengthen the lower abdominal muscles and stretch the low back.
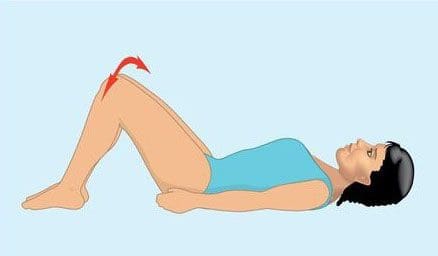
Knee to Chest
Its purpose is to help reduce nerve compression in the low back, that can help alleviate lower back pain.
Lie on back
Start with either� left or right knee and use hands to gently pull the bent knee toward chest
Hold for 10 seconds
Repeat movement on opposite knee
Perform 3 to 5 times holding position for 10 seconds each
Use hands to gently pull both knees toward chest
Hold for 10 seconds
Repeat movement with both knees 3 to 5 times holding position for 10 seconds each
Knee to chest exercise/stretches can help reduce nerve compression on the lumbar spine alleviating lower back pain.
Lower Trunk Rotation
Its purpose is to increase the spine�s mobility and flexibility.
Lie on back with both knees bent upright and both feet flat on the floor (aka the hook lying position).
Hold both knees together, rotate knees to one side
Hold for 3 to 5 seconds
There will be a gentle stretching sensation on the opposite side of lower back and hip area
Contract abdominal muscles and rotate both knees to opposite side
Hold for 3 to 5 seconds
Repeat 10 times on each side
Lower body rotations can help you strengthen your lower abdominal muscles and stretch your low back.�
All Fours Opposite Arm and Leg Extensions
Its purpose is to strengthen the abdominal muscles, low back and stabilize the areas.
Get in crawling position on all fours.
Contract abdominal muscles to keep back flat and straight
Raise one leg upward behind you and straighten outward
Hold for 3 to 5 seconds
Repeat the movement on the opposite side
Once this�exercise/stretch can be performed 10 times with functional pain, add arm movement with each leg extension:
Extend the arm (opposite side of leg) upward and outward in front of body
Hold for 3 to 5 seconds
Repeat on the opposite side
Perform 10 times
How do these exercise/stretches reduce sciatic pain
Abdominal and spinal muscles are essential components of the spine�s system.
These exercises/stretches can help:
Strengthen the spine
Increase flexibility
Increase range of motion
These exercises can help keep the spine�s structural components strong and healthy along with reducing pain and speeding up healing.
Regular exercise causes the body to release endorphins or hormones that interact with the pain receptors in the brain that reduce the perception of pain.
Will exercising with sciatica cause/exacerbate injury
Do not to perform any of these exercises without consulting your doctor,� spine specialist or chiropractor.
Whatever level of fitness, remember even trained professional athletes exercise with a doctor, physical therapist, or other healthcare expert’s approval and clearance.
Obtaining an accurate diagnosis for the exact cause of the sciatic pain
Is essential before considering any exercise program
Be gentle with your spine, don�t push too hard while doing exercises. This is to avoid exacerbating sciatic pain or creating a new injury.
If exercise increases pain or causes nerve-related symptoms like:
Weakness
Tingling sensation
Numbness
Stop and contact your doctor or chiropractor immediately!
El Paso, TX Best Sciatica Chiropractor Treatment
Sandra Rubio discusses Dr. Alex Jimenez and his team will help relieve your sciatica symptoms. Chiropractic care can improve pain and discomfort as well as reduce irritation and inflammation brought on by sciatica. Additionally, a chiropractor such as Dr. Jimenez can also offer nutritional and fitness tips for sciatic nerve pain. Other treatment procedures, such as deep-tissue massage, can help alleviate sciatica symptoms. Dr. Alex Jimenez is the homeopathic, noninvasive option for sciatic nerve disease and its related symptoms.
Sciatica is generally caused by the compression of lumbar or thoracic nerves or by compression of the sciatic nerve. When sciatica is caused by compression of a lower back nerve root, it’s called lumbar radiculopathy. This can happen due to a spinal disc bulge or spinal disk herniation (a herniated intervertebral disc), or by roughening, extending, or misalignment (spondylolisthesis) of the fascia, or as a result of degenerated discs that could reduce the diameter of the lateral foramen by which nerve roots exit the spine.
NCBI Resources
Sciatica is characterized by a shooting pain that originates in the lower back and travels down through the hip, buttock, and back of the leg. The pain can be so severe that it inhibits mobility and can prevent people from working, taking care of their home, or just enjoying their life. Doctors have treated the condition with medications and some invasive therapies, but chiropractic treatments have been found to be extremely effective in alleviating the pain and curing the condition.
Leg Length Discrepancy (LLD) has profound effects on the body’s biomechanics, which can result in back pain and a number of other debilitating conditions.
Overview
Also known as Leg length inequality leg length discrepancy affects as many as 60 to 90% of the population.
It is categorized as functional or structural, but both have profound effects on the body’s biomechanics and result in back pain.
Other conditions include:
Arthritis of the knee
Psoasitis
Arthritis of the hip
Patellar tendinitis
Patellofemoral pain syndrome
Plantar fasciitis
Medial tibial stress syndrome
Iliotibial band syndrome
Lateral knee pain
Trochanteric bursitis
Sacroiliac discomfort
Achilles tendinitis
Cuboid syndrome
Functional Short Leg: Alignment�difference of the supporting structures between the ground and the top of the femur or thigh bone.
This is caused by excessive pronation or the natural rolling in of the foot as someone walks.
Anatomical Short Leg: A difference in the size or length of the thigh bone (femur).
This is most often caused by growth asymmetry that can be inherited/genetic condition�but can sometimes come from a fracture or surgery.
Our body can work with leg inequality for short a period but over time, biomechanical problems throughout the body can begin to happen.
Our body’s ability to adapt to abnormal stress eventually takes its toll and the surrounding soft tissues can’t take it anymore.
Even the simplest movements begin to require much more muscular effort and energy, which reduces endurance.
Excessive stress gets transmitted to the ligaments, which then creates:
The first goal of treatment is to improve alignment and restore symmetry.
This can be accomplished with:
Spinal adjustments focus on providing better spinal column alignment
Exercises to help the affected muscles
Proper orthotics with a pronation wedge under the heel for long-term correction
Sometimes LLI causes a profound gait (walk) disfunction, which means physical therapy might be necessary.
Prevention
Keep your bones and tissues strong and healthy with exercise and diet can help.
Avoid tobacco and excessive alcohol use, which weaken bones and can cause problems with the blood supply in the legs.
Reduce your risk of injury by adhering to safety measures (like wearing a seatbelt).
Custom orthotics provide support, stability, and shock absorption.
Recovery
The body�s foundation can be made level with custom orthotics, but it does take some time to adjust to proper and healthier alignment/posture.
Talk to your doctor or chiropractor to learn more.
Symptoms:
Back pain
Leg pain
Pelvic obliquity
Scoliotic deviations of the lumbar spine
Increased risk of injury, especially in athletes
Chiropractic care does wonders for helping individuals regain their spinal alignment and loosen the joints and muscles affected by leg length inequality, and the orthotic heel lifts balance out the legs, which balances the hips and pelvis.
Reduce *PLANTAR FASCIITIS PAIN* with Custom Foot Orthotics | El Paso, TX (2019)
Foot problems can affect the overall well-being of the human body. Many health issues which affect the foot can result in poor posture, low back pain, and sciatica. These imbalances can ultimately result in a variety of other health issues. Custom-made foot orthotics can help promote and support overall well-being by relieving foot problems. The following video discusses how many health issues which affect the foot can cause a variety of foot problems, including poor posture, low back pain, and sciatica. Dr. Alex Jimenez is the non-surgical choice for foot problems and other health issues. Dr. Alex Jimenez can help promote and support overall well-being with the use of custom-made foot orthotics and other treatments approaches.
What’s Afoot
According to the�American Chiropractic Association, a study found 75% of subjects who suffered from lower back pain had legs that were slightly different lengths (5 millimeters or more). This condition is called�Short Leg Syndrome�and causes a variety of issues for its sufferers. The symptoms can be quite severe, depending on the degree of difference in the leg length.
NCBI Resources
The premise of this condition is that the leg length inequality disrupts the�body�s entire balance, possibly resulting in issues in the knees, hips, and back. The spinal system is designed to bear weight evenly, and, when one leg is shorter than the other, this places additional weight and stress on one side. According to�The Back Pain Authority, common causes of Short Leg Syndrome are a past history of fractures, hip or knee issues, or the individual was simply born that way.
Kyphosis is a condition that is most typically identified by a humped mid to upper back. It can be frustrating to find yourself diagnosed with kyphosis, both due to the unusual appearance it causes and the physical discomfort that can come with the condition. Fortunately, chiropractic offers a variety of treatment options for kyphosis that are non-invasive, drug-free and quite effective. With the right approach, it should be possible to get significant relief for your symptoms through chiropractic care.
Causes
Many times kyphosis is caused by poor posture. Years of hunching your back can cause the body to change the way the vertebrae sit atop one another�leading to stretching of soft tissues and a resting position that is hunched instead of upright.
Not all cases of kyphosis are the result of poor posture, however. There are some people who are born with kyphosis. There are also those that develop kyphosis following trauma or due to disease. One of the most common diseases that result in kyphosis is Scheuermann’s disease.
Chiropractic can often help resolve kyphosis that is caused by poor posture. If your kyphosis is due to trauma or other issues, chiropractic can still provide a much-needed relief from many of your symptoms�including pain and stiffness.
How Chiropractic Helps With Kyphosis
HEALTHCARE AND MEDICAL CONCEPT: KYPHOSIS
Diagnosing the Cause
Your first visit to the chiropractor will begin with a comprehensive examination to determine the cause of your condition. An accurate diagnosis is key to developing an effective treatment plan. The examination will most likely include imaging tests like an x-ray or MRI. It may also include a physical examination to figure out how your body currently moves, where you are tender and/or in pain, etc.
Treatment Plan
Your chiropractor will never move forward with treatment until he or she has explained your options and gotten your permission to begin. The treatment plan you are offered may include:
The joint in the human body, particularly the spinal joints, have an ideal alignment where everything fits together best. The more you can achieve and maintain this alignment, the less pain, stiffness and other disruptions you can expect to experience. Chiropractic adjustments aim to bring your body back into alignment.
Regular adjustments should help to improve your spinal alignment and straighten your back. In the case of poor posture, adjustments can aid you in learning how to improve your posture and keep those improvements over the long term.
Mobility Increased
The curving of the back typical of kyphosis can lead to a lot of stiffness in the spine and surrounding soft tissues. Lack of mobility makes everything you do more difficult, so it makes sense to try and increase your mobility when possible.
Chiropractic adjustments and complementary therapies are ideal for relaxing the soft tissues that may have become stiff as the kyphosis developed. One of the great things about improving the mobility of the spine is that it allows you to improve your posture. Over time, it should become easier to keep your back in a more healthy alignment.
Pain Lessened
Pain is common with kyphosis. The spine is not meant to hump as it does with kyphosis, which explains why pain is so typical with the condition. Chiropractic is very useful for decreasing pain related to spinal issues. Many patients get relief immediately following their first adjustment.
Schedule an Appointment With Us Today
If you are suffering from kyphosis, please contact us to schedule an appointment. Our chiropractic team is standing by to answer your questions and help you get treatment for your condition.
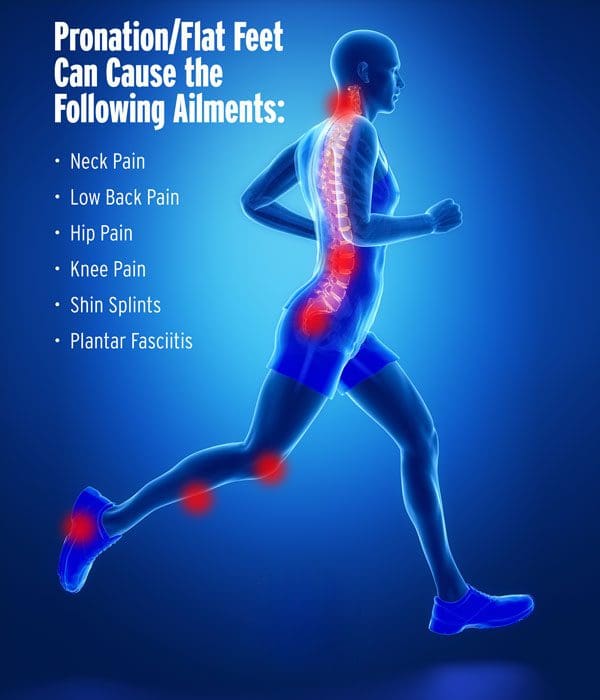
What is a Pronated Foot & What Can Custom Orthotics Do?
When a foot is pronated, it means its arches have fallen and the foot is flat. Flat feet do not absorb shock as well and make for a less stable base for�the bones, muscles, ligaments, and tendons. They can also:
Shift the body’s alignment out of order
Cause aches and pains in the feet, knees, hips, neck and/or spine
Lead to injury and problems like shin splints, Achilles tendinitis, and plantar fasciitis
Up to a third of people suffer from flat feet
Causes
The connective tissue, called the plantar fascia, on the underside of the foot is what maintains the foot�s healthy arch shape. Injury and health conditions can cause the fascia to stretch out and flatten. But so can everyday walking and standing. Once the fascia stretches out, it is unable to spring back. When the foot structure becomes flattened, the body�s foundation is prone to injury and health conditions.
Treatment
Chiropractic adjusting to ensure proper positioning of bones and joints
Custom orthotics in every pair of shoes for pronation control, support, and comfort
Get Rid of *Foot Pronation* with *FOOT ORTHOTICS* | El Paso, Tx (2019)
Pronation
Pronation describes the way that the foot rolls inward during its normal motion. The foot turns inward, flattening out, as the heel�s outer edge strikes the ground. For the foot to function correctly, there must be a significant degree of pronation. However, excessive pronation, or overpronation, can cause injury and damage to the foot and ankle. It creates the arch in the foot to flatten, and the ligaments, tendons, and muscles under the foot overstretch. For instance, overpronation of the foot causes a series of internal changes that extend up through the leg. The femur may rotate causing hip pain and inflammation of the sacroiliac joint which leads to back pain. Other misalignments in the body that are caused by foot problems can also lead to chronic lower back pain as well.
NCBI Resources
Sometimes there are abnormalities of the spine and it causes a misalignment of the natural curvatures or some curvatures may be exaggerated. These unnatural curvatures of the spine are characterized by three health conditions called�lordosis, kyphosis, and scoliosis. They gently curve, sloping slightly inward at the small of the back, and again slightly at the neck. The pull of gravity, combined with body movement, can put a great deal of stress on the spine and these slight curves help absorb some of the impact. Spinal manipulations for spinal curvature disorders�have been shown to be very effective. Chiropractic helps restore the spine�s natural balance even if the patient has one of these types of conditions.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine