Shoulder and arm pain can be debilitating, especially when there is no obvious cause or injury that needs to be treated. A rare condition known as brachial neuritiscan cause spasms along with pain down the arm, followed by numbness, tingling, and weakness. If not diagnosed and treated early, the symptoms can worsen with time. The pain experienced can be described as sharp, searing, and shooting. Brachial neuritis can be intense and disabling when it presents for hours and even days.
Utilizing a chiropractic approach, shoulder and spinal adjustments can provide relief and a faster healing/recovery from the inflammatory condition. Individuals experiencing shoulder, arm, and possible hand pain should consult with a chiropractor about a potential home and clinic treatment plan to improve their condition.
Medical History and Examination
The process of diagnosing brachial neuritis involves an individual’s medical history and physical exam. More complicated cases could require imaging studies and electrodiagnostic tests. The first steps in diagnosing the cause of shoulder and/or arm pain include:
Medical history
Information will be collected on an individual’s:
Medical history
Family history
Underlying conditions
Recent illnesses or injuries
Lifestyle habits
How and when symptoms began
Current symptoms
Physical examination
A chiropractor will palpate or inspect by feeling the neck, shoulder, and arm for irregularities. Then they will examine the range of motion, strength, and reflexes. If the individual’s history and physical exam suggest that the cause could be brachial neuritis or other condition involving the nerves, imaging studies, and diagnostic tests could be required to evaluate further.
Symptoms of Brachial Neuritis
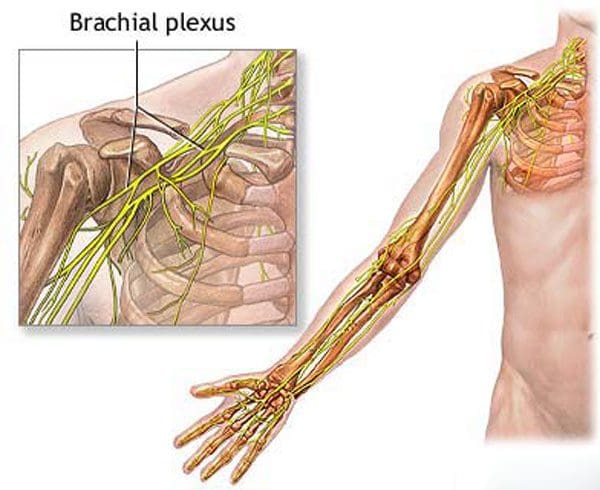
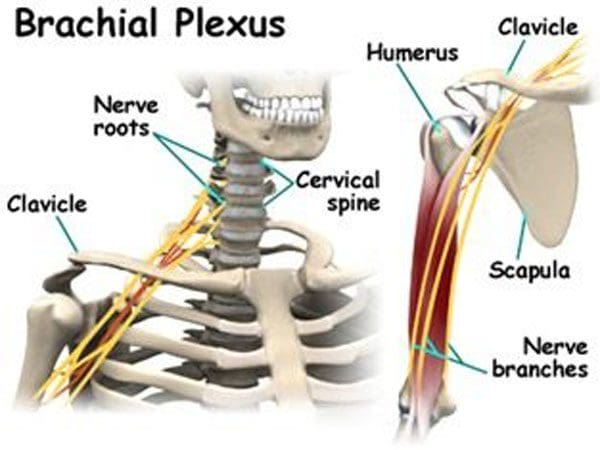
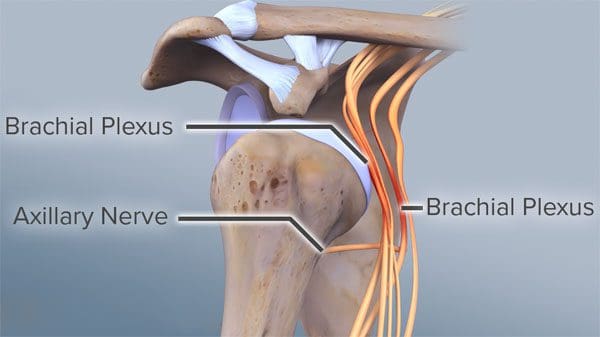
The condition is also known as Parsonage-Turner Syndrome. It affects the brachial plexus, a set of nerves that run from the neck and upper back to the shoulders. The condition usually affects only one side of the body and presents randomly.
What happens is the nerves become inflamed.
Inflammation can be triggered through an autoimmune response. This is often the result of an infection, surgical procedure, or other internal stressors. The inflammation can lead to severe debilitating shoulder pain over a few days.
This also leads to long-term numbness, weakness in the shoulder and arm.
The pain becomes worse with movement.
Typically, the pain goes away on its own within a few days.
Numbness, weakness, or tingling in the shoulder or arm continues.
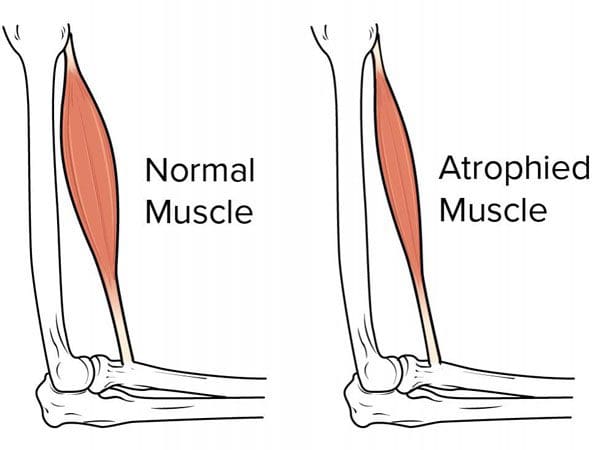
Over time the symptoms begin to worsen and, if left untreated, could lead to muscular atrophy of the arm.
The pain and weakness can make it difficult to move the arm, leading to decreased strength.
Symptoms can last up to a year or more.
This is why individuals have to find ways to strengthen their shoulder/arm despite the condition.
Chiropractic Relief
Treatment requires a pain management program until the pain subsides. Once the pain is manageable, chiropractic, physical therapy, exercises, and stretches could improve mobility and strength. Chiropractic can provide relief and tools necessary to prevent the worsening of symptoms. Chiropractic helps to:
Reduces pain
Improves mobility
Restores strength
Chiropractic manipulation will ensure that the nerves near the brachial plexus do not become compressed, but if they are, then chiropractic can be utilized to decompress/release them. In addition, trigger point release and massage can help alleviate the tension in the surrounding tissues of the arm and shoulder.
A chiropractor will educate the individuals on effective pain management techniques for home, including ice/heat therapy and stretching exercises. These techniques will help restore the proper alignment and flow of the spinal vertebrae, nerves, and muscle tissues, allowing the body to heal quickly, naturally, and more effectively.
Chiropractic Shoulder Pain Treatment
References
Feinberg, Joseph H, and Jeffrey Radecki. Parsonage-turner syndrome. HSS journal: the musculoskeletal journal of Hospital for Special Surgery vol. 6,2 (2010): 199-205. doi:10.1007/s11420-010-9176-x
Osteoporosis prevention can be accomplished, even with an osteoporosis diagnosis. There are steps along with your doctor’s treatment plan and recommendations to help control the disease from progressing. An osteoporosis prevention plan can be generated to improve general health and reduce the chances of a fracture in the spine or other bones. �
�
Doctor Discussion
Make an appointment with a specialist to talk about osteoporosis risk factors. If you are 40 years of age or older, take some time to review the list of potential risk factors to discuss. An individual’s response can help prepare for this healthcare discussion.
�
Risk Factors
The individual has had a bone fracture as an adult – wrist, hip, spine, etc.
History of osteoporosis in family – mother, sister, father.
Body Type – small, medium, large frame.
Body Shape – Thin, frail, overweight, obese.
No regular exercise.
Tobacco use – smoke, vaping, chewing, etc.
Alcohol consumption – Drinks 3 or more times a week, sometimes binge drinks.
Diet does not include calcium – milk, yogurt, or vitamin D – cheese, eggs.
Occasional crash diet.
Eating disorders – anorexia, purging, bulimia.
Corticosteroid/s use and/or anti-convulsant medication/s use.
Less stability on feet.
Experiences occasional falls.
Women – 45 or younger, beginning of menopause, 50 or older, post-menopause.
Men – Diagnosed with low testosterone levels.
�
Learn Your T-score
A bone mineral density test is the most dependable way to predict and detect osteoporosis. It is a painless test and can take around ten to thirty minutes to complete. The T-score is a number that lets an individual know where their bone density it and if it is good or not so good.
�
Build Bone Mass
Bone mass can be built up by including weight-bearing and resistance exercise into a regular workout. The difference between weight-bearing and resistance exercises is that weight-bearing uses the bone/s and muscle/s to work against gravity.
Walking, jogging, and dancing, are examples of weight-bearing exercises. Weight lifting or free weights are examples of resistance exercise. Here the body’s muscular strength is being utilized. This helps build bone mass and strengthen muscles.
�
Calcium/Vitamin D Rich Diet
Taking the time to nourish the body properly will help with osteoporosis prevention and achieve optimal health. Calcium and vitamin D won’t completely prevent or cure osteoporosis, but it is essential to include these minerals and vitamins in your diet daily. If an individual is lactose intolerant, there are fortified food products like orange juice and cereal/s to help meet daily mineral/vitamin requirements.
Check out the best and worst foods for bones. Supplements are another option to help boost calcium and vitamin D. Your doctor will know how much calcium and vitamin D you need. Taking too much is not being health-wise. Taking too much of a supplement can make an individual sick. Registered Dietitians and Health coaches can educate on making wise food and supplement choices. A doctor can aid in finding either in your area. �
�
Stop Smoking
Smoking increases the risk of osteoporosis. Smoking affects pretty much every organ in the body. Smoking interferes with the body’s ability to absorb calcium and lowers the hormones the body needs to build and keep the bone mass. Quitting will decrease the risk of cancer, heart, lung disease, and osteoporosis.
�
Reduce Alcohol
Too much alcohol consumption causes poor nutrition. Poor nutrition causes bone density to decline, which leads to osteoporosis. And alcohol increases the risk of falling. Falls are one of the leading causes of spinal/other bone fractures. So contact your doctor or chiropractor and discuss an osteoporosis prevention plan.
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Surgery for sciatica is sometimes necessary if medications, chiropractic, and physical therapy are not working to relieve sciatica symptoms, but don�t worry. Individuals sometimes have sciatica that just does not respond to conservative treatment can find relief through surgical procedures.
�
Questions begin to pop up, as to which procedure makes the most sense, what will the experience be like, and how long will it be until you can get back to a normal, pain-free life?
�
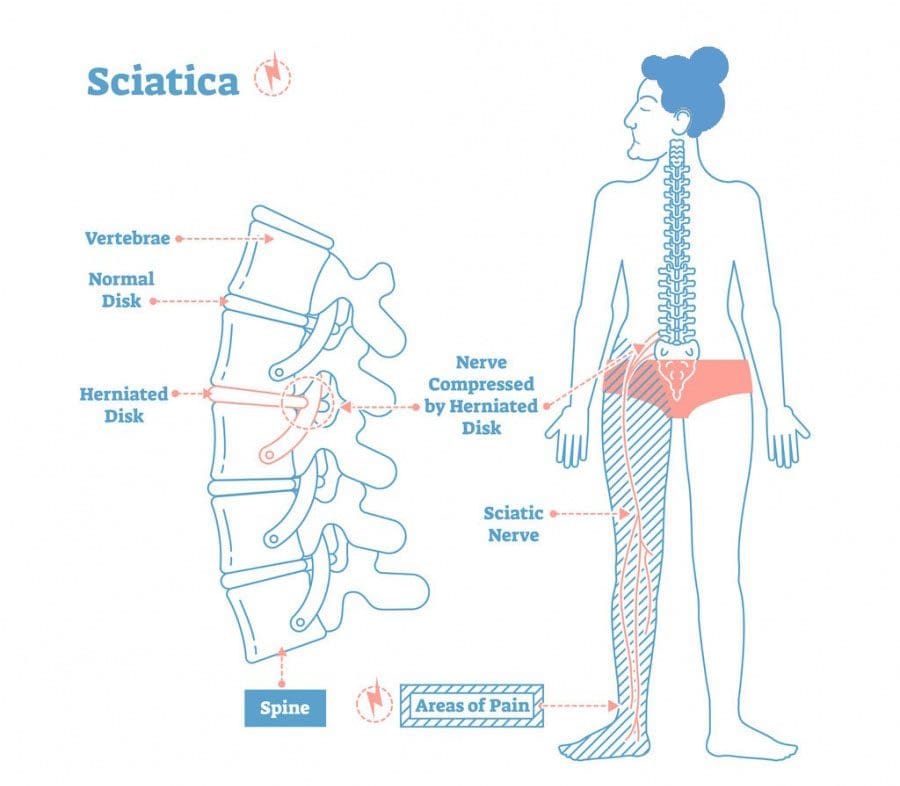
Sciatica
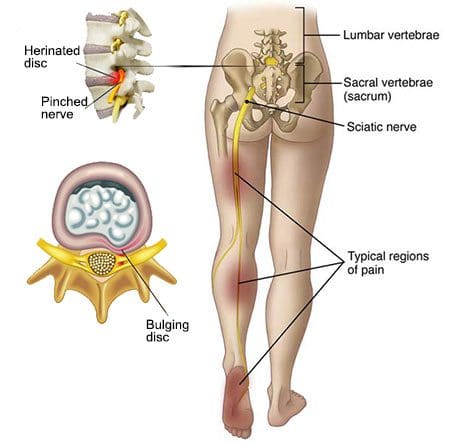
Sciatica is pain that runs down the longest nerve in the body, known as the sciatic nerve. Pain starts in the lower back and spreads down one leg, into the calf and possibly the foot. It is rare but sciatica can occur in both legs. The pain is mild to severe and feels worse when sneezing, coughing, bending, and standing/sitting in certain positions. The pain is often accompanied by numbness, tingling, or weakness in affected legs. �
�
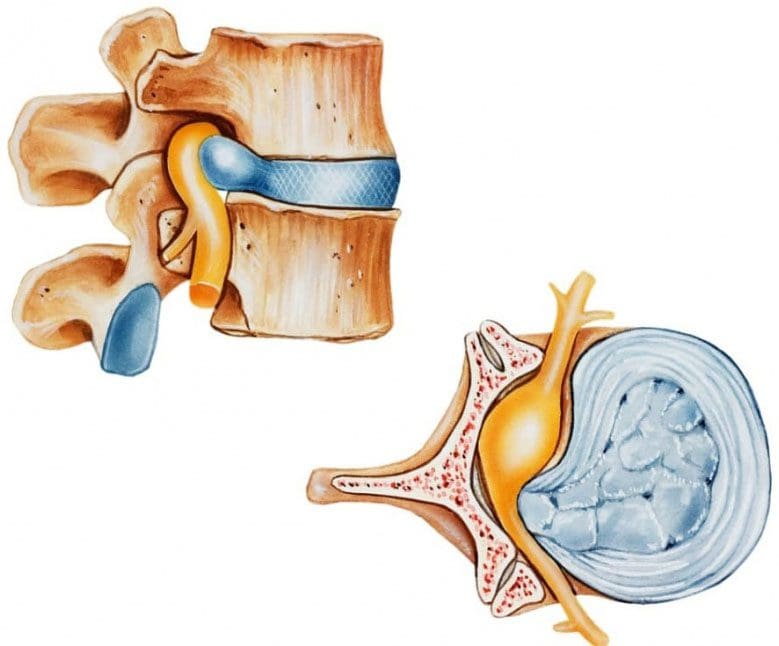
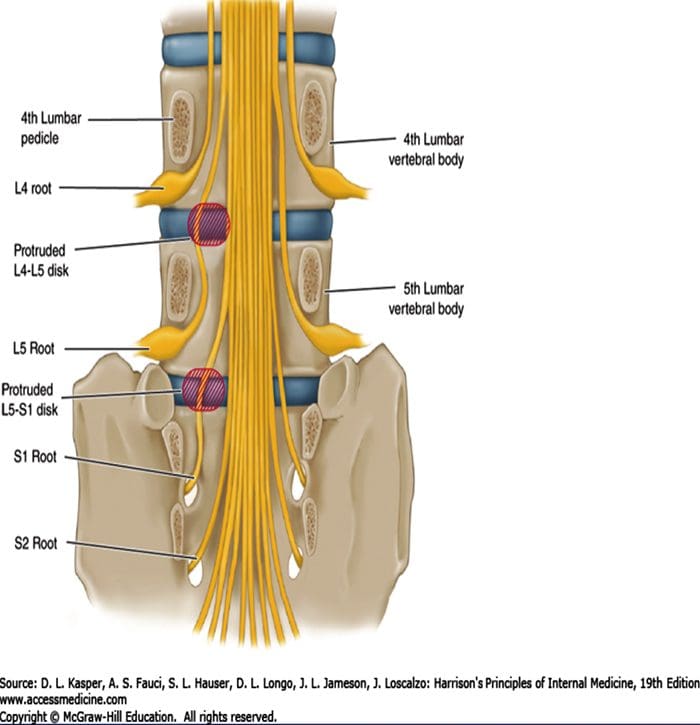
Sciatica a set of symptoms caused by other medical problems like an injury, tumor, or the most common cause around 90% of the time is a herniated disc in the lower back. The soft-gel center of the disc pushes through the tough exterior, where it can pinch or press on the sciatic nerve causing pain.
Research shows that sciatica affects 1% to 5% of the population, and around 40% will experience sciatica at some point in their life. Men between the ages of 30 and 50 have a higher risk along with smokers, individuals that sit for a long time, and those that perform physically strenuous work. Doctors and chiropractors can diagnose cases of sciatica with a medical history and physical exam. Diagnostic imaging can also be used in some cases.
�
When it’s Time to Consider Surgery for Sciatica
�
Most individuals with sciatica respond positively with non-surgical treatments like chiropractic, physical therapy, acupuncture, medication, spinal injection/s, etc. This makes spine surgery a rarely needed treatment for low back and leg pain caused by sciatic nerve compression. But there are situations when surgery for sciatica could be beneficial.
Symptoms become severe and non-surgical treatment is no longer effective
There are different types of surgical procedures for spine surgery. A spine surgeon will recommend the best approach for each patient’s sciatica. Which procedure they recommend will be based on the disorder causing sciatica with the entire procedure clearly explained so that you understand completely. Ask any questions to better understand the surgeon’s recommendation. Remember, the final decision is always up to you. A second opinion is recommended before deciding.
Sciatica usually goes away on its own with the majority of cases managed with conservative treatment. Depending on the cause, this could be heat or ice packs, chiropractic, therapeutic massage, pain medication, stretching exercises, physical therapy, or injections. �
Sciatica for Surgery Options
Surgery for sciatica is performed to relieve the added compression/pressure on the nerves and relieve the pain. Options include a microdiscectomy and laminectomy. Each has its similarities and differences when it comes to the preparation, process, and recovery for the operation. �
�
Microdiscectomy
During a microdiscectomy, part or all of the herniated disc is removed. Research has shown the effectiveness of relieving pain to be around 80 to 95 percent of patients. The operation is done in a hospital or surgery center and requires about one hour to complete. General anesthesia is administered during this procedure.
A surgeon will make an incision over the affected disc.
Skin and tissue covering the disc will be opened and moved for better access. Some of the bone could be taken out as part of the procedure called a laminotomy.
The surgeon will use various tools to remove all or part of the herniated disc.
Once the removal is done, the surgeon will close the incision and send you to a recovery room.
To quicken the healing process patients are encouraged to start walking within hours of the procedure.
Most go home the same day. Some patients will have to stay at the hospital for observation. This could be from other conditions present.
You will not be allowed to operate a vehicle the same day. Therefore a designated driver will be necessary.
�
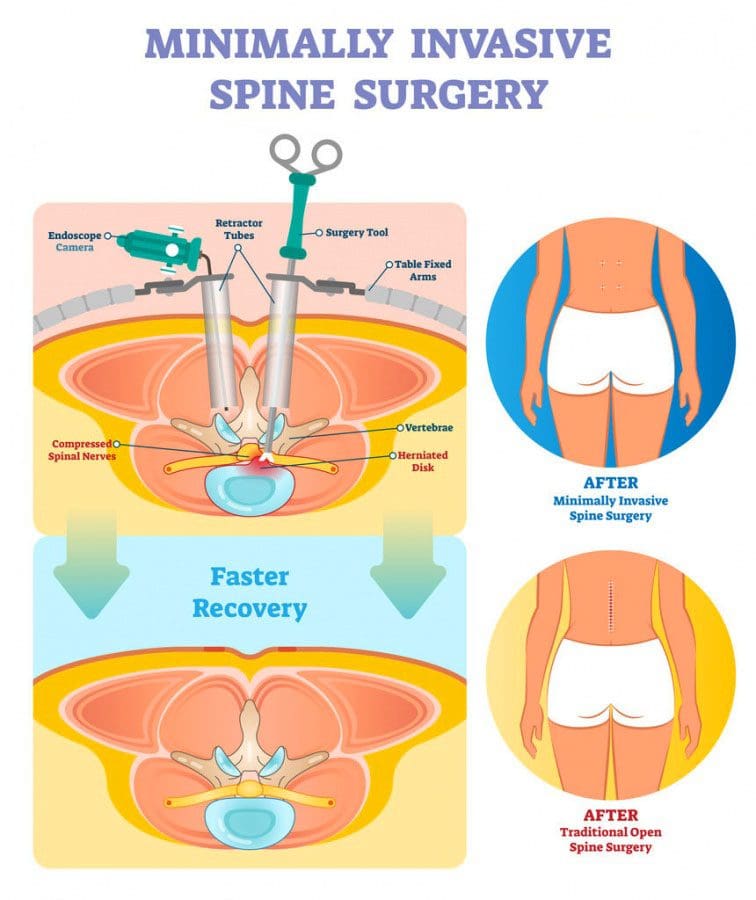
Laminectomy
�
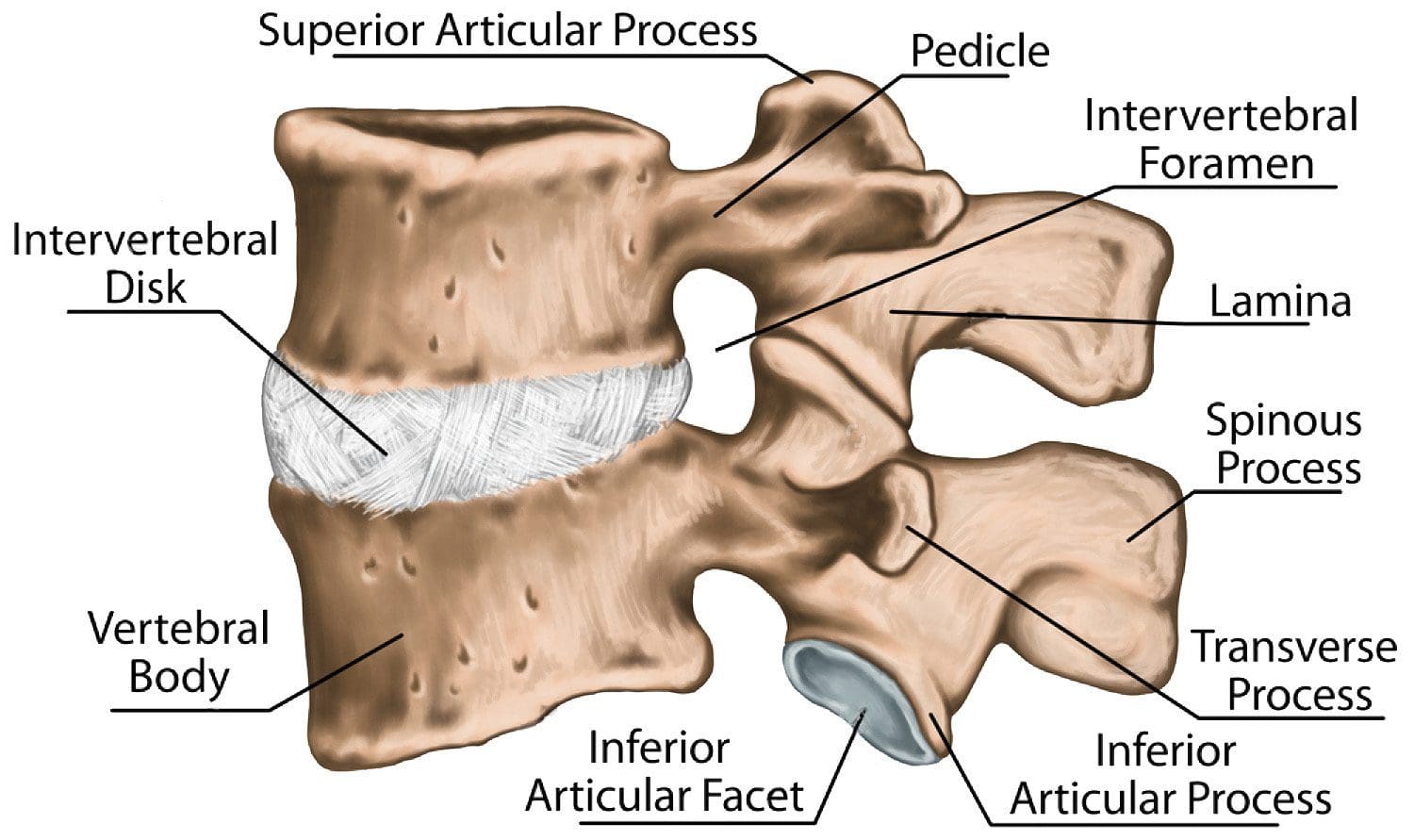
Preparation for a laminectomy is similar to a microdiscectomy. The lamina is the back part of the vertebrae, which protects the spinal canal. This procedure relieves pain by creating space for the nerves to move around.
The procedure takes about one to three hours from start to finish.
Both sides of the laminae are removed, along with the spinous process in the middle.
The patient lies face-down as the surgeon makes an incision near the affected vertebrae.
Skin and muscles are moved around and various tools/instruments are used to remove all or part of the lamina. Overgrowth of bone or spinal disc could also be removed.
The incision is stitched or stapled, bandaged, and sent to a recovery room.
Just like a microdiscectomy the individual will be encouraged to begin walking the same day.
Most individuals leave the hospital after surgery, however, a one to possible three-night could be required for others.
A driver does need to be designated for the ride home.
A microdiscectomy is recommended for stenosis caused by a herniated disc. However, if the stenosis is caused by another health issue/condition like bone spurs developed from arthritis, then a laminectomy could be the best approach. Laminectomies are usually performed on individuals in their 50s or 60s. While micro discectomies vary when it comes to age but are usually performed on younger individuals.
�
Recovery
�
At home, post-op rules need to be followed no matter what surgery for sciatica was performed. The incision area needs to stay clean and no lifting of heavy objects, bending and sitting for extended times. Surgery for sciatica is considered safe with complications being uncommon. All operations come with risks. These include nerve damage, blood clots, and infection.
The provider needs to know about unusual symptoms after the procedure. This could be fever, excess drainage, or pain around the incision area. Pain meds could be prescribed to ease the post-surgery pain, and chiropractic along with physical therapy could be implemented to speed recovery. Individuals are typically cleared to return to work two to four weeks after the procedure. It could be six to eight weeks if their job/occupation is physically demanding and strenuous.
Depending on how complex the spine surgery is an individual could be sitting upright the same day and walking within 24 hours. A course of pain meds could be prescribed to help manage postoperative pain. Instructions will be given on how to sit, rise, get out of bed, and stand in a careful manner. The body needs time to heal, so a doctor could recommend activity restriction. This could be anything that moves the spine too much. For sure contact sports, twisting, or heavy lifting during recovery are to be avoided. Report any problem/s like fever, increased pain, infection right away.
�
Spine Surgery Relief
Many individuals benefit from sciatica surgery, but it doesn�t work for everyone. A small percentage of individuals continue to feel discomfort in the weeks/months after. And sciatica can return in the future and in a different location. Your healthcare provider can help you decide if surgery for sciatica is the right choice for you.
�
Treating Severe & Complex Sciatica Syndromes
�
�
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Part 2 delayed braking reaction time caused by sciatica, we continue with the spinal cord, nerves, and how they communicate with the brain. A herniated disc can cause sciatica, which is a compressing of the nerve/s in and around the spinal cord. This compression causes a pinching of the nerve/s like bending a water hose cuts off the flow and damages the hose, is what happens to the spinal nerve/s cutting proper blood flow, and proper synapse/signal flow.
This occurs from the damage to the nerve/s and could delay braking signals for a split second. But that is all that is needed for an auto accident to happen. A delay in braking time has been found in individuals with herniated/bulging/ruptured/slipped discs. Fortunately, through chiropractic and physical therapy, the nerves can be re-stimulated and brought back to optimal function.
�
�
Communication
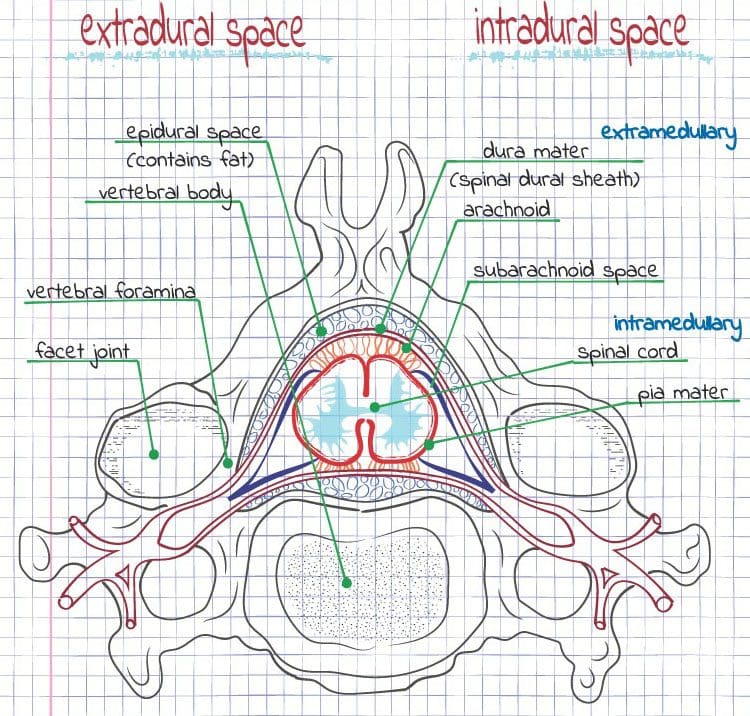
The spinal cord is about one inch across at its widest and around eighteen inches long. The spinal cord is a type of tube that is filled with nerves and cerebrospinal fluid. This protects and nourishes the cord. Spinal cord added protection includes:
There are three types of membranes surrounding the spinal cord referred to as meninges. The outer membrane is known as the dura mater, the middle membrane is the arachnoid mater and the innermost membrane is the pia mater. �
� These membranes can become inflamed and damaged by disease or trauma. Arachnoiditis is caused by inflammation of the arachnoid lining that results in intense stinging and burning pain. This can happen post-surgery and can cause the scarring of nerve/s.
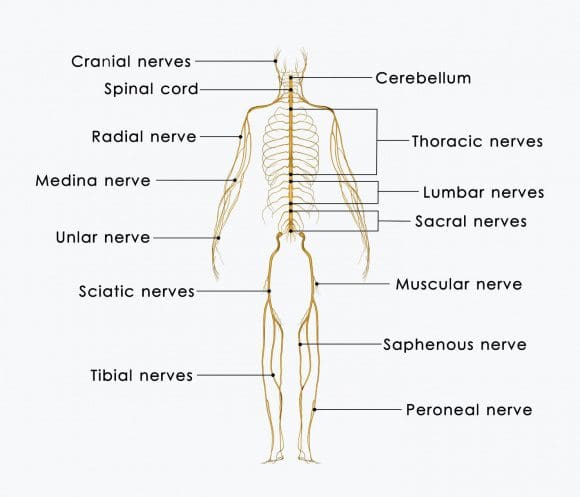
The nerves exit the spinal column and branch out to the rest of the body. All parts of the body are controlled by specific spinal nerves. The nerves are placed in and around the area they control. Like the nerves in the neck area branch out into the arms. This is why a neck ache/pain issue can lead to pain spreading into the arms and hands.
Thoracic spine controls the middle of the body,
The lumbar spine extends into the outer legs controlling that area
Sacral nerves control the middle of the legs and organ functions of the pelvis
�
The brain
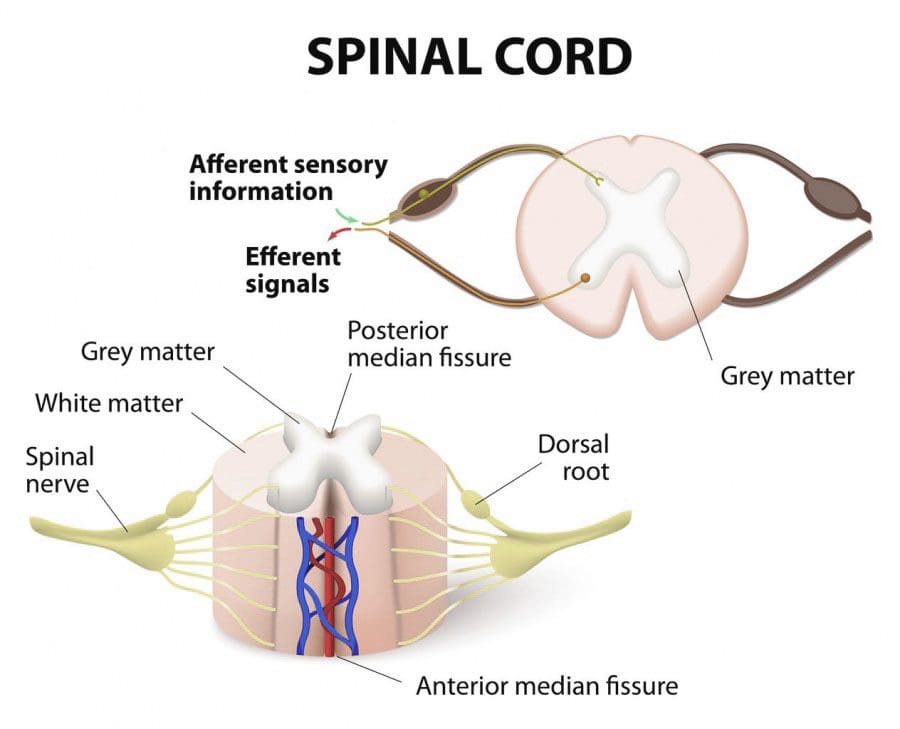
Two major types of nerves: sensory and motor. Sensory nerves send information like:
Touch
Temperature
Pain
These get sent to the brain via the spinal cord. Motor nerves relay signals from the brain back to the muscles making them contract voluntarily or reflexively. Peripheral nervous system – the PNS has nerves that extend down the spinal canal and branch out at openings in the vertebrae called foramina. �
�
�
Signals/messages get sent to and from the brain aka the central nervous system. It sends all types of signals including pain and initiates movement. For example, the nerves reflexively make the spine twist and turn when driving to keep balance when turning and braking. The peripheral nervous system is a collection of millions of nerves throughout the torso and limbs. This system conveys messages to the central nervous system.
�
Referred pain
When a health problem/issue/condition takes place in one part of the body with pain being felt in another or several areas, pain specialists call it referred pain.
�
Nerves
Nerves exiting the spinal cord is done in pairs with one being a sensory nerve, and the other a motor nerve. Motor nerves initiate movement and bodily function. Damage to a motor nerve could cause a weakness in a muscle or loss of function. For example, a prick in the foot that is not felt could mean there is some sensational loss, indicating a problem with the sensory nerves and or possible nerve damage. These are the nerves that control pain, temperature, etc. Sensory nerve issues can feel like shooting electrical pain Continuing with activities could exacerbate the nerve damage.
�
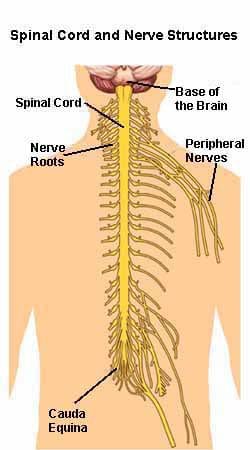
Cauda Equina
� The spinal cord ends at the lumbar low back, where the nerves extend in a bundle of strands called cauda equina, called this because it looks like a horsetail. These nerves provide motor and sensory function to the:
Legs
Intestines
Genitals
Bladder
Therefore, based on this knowledge there is adequate information displaying how sciatica could cause a delayed braking reaction time based on the nerves’ dysfunctional signal firing. Chiropractic treatment could be an option to help an individual realign their spine, work out tight muscles, nerves, ligaments preventing any further damage, and getting the individual back in top form.
�
Chiropractors & Sciatica Syndrome Expose
NCBI Resources
�
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Research has found that individuals with disc herniation/s can have a delayed braking time when driving. After undergoing surgery these individuals showed significant improvement in braking time.
Based on this information Dr. Jimenez looks at how individuals with functional sciatica, (often caused by a herniated disc) meaning they can move and operate a vehicle to a certain point without generating pain, however they often put themselves in extreme/awkward positions just to operate, could also have a delay in brake reaction time. �
�
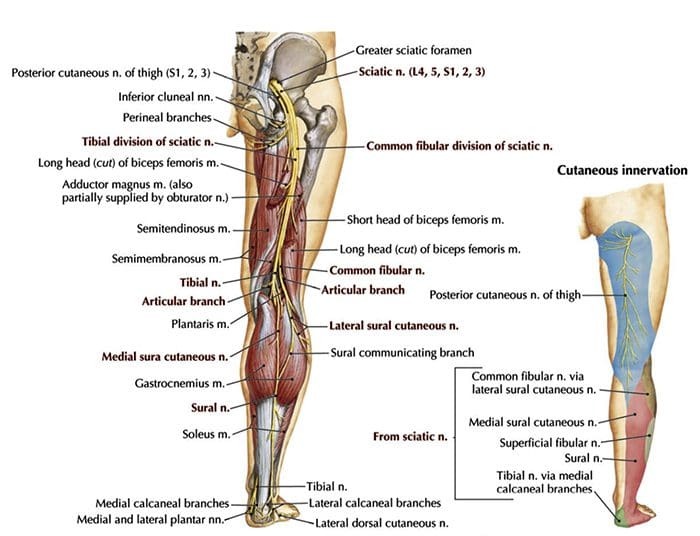
Sciatic Nerve
The sciatic nerve is a large nerve that travels from the lower back down both of the legs and into the feet.�Sciatica begins in the low back. The nerve roots in the lower spine come together and turn into the sciatic nerve. Sciatica happens when these nerves get pinched/compressed. This usually occurs from a herniated disc or when the spinal canal narrows called stenosis.
�
Symptoms
Typically, sciatica causes:
Pain in the leg/s
Shooting pain that goes down from the low back, through the leg, calf and sometimes into the foot
Electrical pain running/shooting down the leg
Burning pain
Pain from slight movement
Numbness
Weakness
�
A car accident can cause sciatica, but now it seems that sciatica can cause an automobile accident because of delayed braking reaction time. People with sciatica that is present without pain often say there is a constant non-painful tingling, numbness, or numbing sensation along the leg that lets them know the sciatica is still there.
This could be insufficient blood flow from wherever the impingement is happening. Keep in mind that there could be multiple areas of impingement. Just like the slow blood flow, they may find when they drive the impingement slows the motor-sensory signal and braking time to depress the brake pedal fast enough to avoid a collision.
�
Nerve Treatment
Sciatica can be treated non-surgically with:
Chiropractic
Physical therapy
24 to 48 hours of rest
Over the counter pain relievers like ibuprofen or acetaminophen
Muscle spasms can be treated with heat or ice
� Patients with sciatica feel better with time, usually a few weeks. However, if pain continues, other forms of treatment can be discussed.�A doctor or chiropractor may advise�light exercise and therapeutic stretching. As recovery progresses they may give you exercises to strengthen the back and core.
With new automobiles implementing automatic braking systems has helped significantly reduce accidents, however, there are still bugs to sort out. This is normal with these computerized systems. Reliance upon these systems, especially those with sciatica, herniated, or bulging disc/s, could be a dangerous combination, specifically when it comes to braking reaction time.
Sciatica Pain* Treatment Relief
�
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require added explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
The sciatic nerve can be compressed, pinched, twisted, moved out of position by a variety of things, including injury/s and spinal conditions, diseases, and the most common a herniated disc. This could be time to try the chiropractic solution that can treat sciatica symptoms and bring relief quickly. If you are experiencing a shooting, electrical, tingling, numb pain down one of your legs could be a presenting of sciatica symptoms.
Sciatica
Sciatica is really a symptom itself caused by lumbar radiculopathy. Lumbar radiculopathy is a medical term referring to a low back condition/injury/disorder that is affecting the nerves in this area. The sciatic nerve travels from the lower back down both of the legs and into the feet. Added pressure placed on the nerve from a herniated disc can lead to common symptoms.
Shooting pain that goes down from the low back, through the leg, calf and sometimes into the foot
A feeling of electricity down one leg
Burning pain
Pain from moving
Numbness
Weakness
Causes
Causes of sciatica include:
Vertebrae Out of Alignment
Misaligned vertebrae, referred to as subluxations can put pressure on nerves in the spine � including the sciatic nerve.
Disc Herniation
The discs that cushion the vertebrae are made up of a tough outer layer and a softer inner layer. When the outer layer is damaged and the inner layer comes out into the spine, it is referred to as disc herniation.
A herniated disc means that the inner layer of the disc is putting pressure on nerves in the spine. A herniated disc impacts the sciatic nerve and can lead to sciatica.
Car Accidents
A car accident can easily damage the spine and soft tissues. An accident can cause a misalignment of the spine, a herniated disc, or other injuries that cause symptoms of sciatica.
Sports Injury/s
Even the fittest athletes are susceptible to back injuries, which in turn can cause sciatica. The spine and discs can be damaged due to a large impact, repetitive motion injuries, or even twisting the wrong way.
Work Injuries
Many sufferers of sciatica do not realize that their workplace activities � including repetitive motions and sitting or standing in one position for long periods of time � can lead to sciatica.
How Chiropractic Solution Helps
Prevention found that sixty percent of individuals with sciatica failed to find relief from other treatments found their symptoms improved after chiropractic treatment.
The chiropractic solution works because it gets to the source of the problem and relieves pressure on the sciatic nerve. Chiropractic treatments include:
Realignment
Spinal misalignments are often the cause of sciatica can be corrected through careful chiropractic adjustments. The chiropractor analyzes the misalignment, then applies pressure to the area to correct the misalignment. The pressure is removed from the sciatic nerve, and this is done on and off to get the correct position and massaging the inflamed tissues until symptoms improve.
Spine Decompression
For those whose sciatica is caused by a herniated disc, spinal decompression can bring real relief. Using a specially designed table, the chiropractor can gently stretch the spine � creating space for the disc to heal and pull back from the sciatic nerve.
Find Relief
Please contact our chiropractic team today to schedule an appointment if you are experiencing symptoms of sciatica. We are ready to help you feel better and get back on your feet again. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.�We do this so that we may reach as many El Pasoans who need us, no matter the affordability issues.
Severe *Sciatica”* Pain Relief | El Paso, Tx (2020)
NCBI Resources
Patients with sciatica feel better with time, usually a few weeks. If pain continues, other treatment modalities can be discussed.�Muscle spasms can accompany sciatica symptoms and can be treated with heat or ice therapy. A doctor may advise�light exercise like short walks�and once recovery is established they may give you exercises to strengthen your back and core.
Sciatica is not only caused by a spinal injury, although this is the primary cause, sciatica can also surprisingly be caused by your clothes and shoes. Sciatica is defined as symptoms that include back, leg, and foot pain caused by the compression of the sciatic nerve. Other symptoms can include shootingelectrical rays of pain, weakness, and numbness from your low back all the way down your legs into your feet.
Because of the intensity, many assume it has to be something serious like a work/car accident, sports injury or severe trauma. All of this can lead to sciatica, but there are also everyday things that we do daily that can also cause it. Here are some lesser-known ways of developing sciatica.
Items in Your Back Pocket
Many of us put our phones or wallets into our back pockets. When we carry these items in our pocket and then sit down on them, this can become a gradual trigger to sciatica. When we sit with these items begin to irritate the piriformis muscle. The sciatic nerve is right underneath this muscle and can get compressed. This cause has not been defined by the medical community, but a few names floating around include (back-pocket sciatica and cell-phone sciatica).
Wearing High Heels
High heels push your weight forward and so your body wanting to remain upright responds by flexing the hips to keep you straight. The risk of sciatica happens when this flexing at the hips stretches the hamstrings that can irritate the sciatic nerve running alongside the hamstrings. And besides sciatica high heels can cause a bevy of other spinal problems.
Wearing Tight Jeans and Underwear
Overly tight-fitting pants and underwear might look and feel great, however, they can also contribute to sciatic nerve pain. Wearing tight clothing is not bad but realize that wearing this type of clothing every day will start to compress the muscles, ligaments, and nerves. Mix it up with clothing that allows you to move freely. If your clothing cuts off circulation absolutely do not wear it. And when it comes to tight pants, change postures and don’t stay in the same position for too long, especially sitting.
Excess Weight
Research has found an association between being overweight and having sciatica.�Excess body weight puts stress on your spine. This added pressure combined with sedentarism can cause spinal disorders that include sciatica. Being able to maintain a healthy weight will greatly reduce your risk of developing sciatica symptoms.
The Impact of Sciatica
Even if just gradual weakness develops down your leg or a sudden burst of pain comes and goes, do not ignore it and make an appointment with your doctor or chiropractor to understand the issue and underlying cause/s and set up a preventative treatment plan before it gets out of hand. There are many sciatica treatments/therapies to reduce or eliminate low back and leg pain. Your doctor/chiropractor will work with you to develop a custom sciatic preventive exercise treatment plan.
Severe *Sciatica”* Pain Relief | El Paso, Tx (2020)
NCBI Resources
A study cited by the health magazine�Prevention found that sixty percent of sciatica sufferers who failed to get relief from other treatments found their symptoms improved after chiropractic care. Please contact our chiropractic team today to schedule an appointment if you are experiencing symptoms of sciatica. We are ready to help you feel better and get back on your feet again.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine