The forearms have a casual relationship with the hands and the wrist as they are below the elbow and have very important motor functions. The hands and wrists help many individuals hold onto items, while the forearms provide support by carrying items without pain. The various muscles surrounding the forearms, hands, and wrist joints help provide mobility and flexibility to the arms. Injuries like muscle sprain, strains, or stiffness in the forearms, hands, or wrist can be due to trigger points along the brachioradialis muscles affecting the hands and wrist. Today’s article looks at the brachioradialis muscle functions on the hands and wrist, how trigger points affect the hands and wrist, and how to manage trigger points associated with the hands and wrist. We refer patients to certified providers who specialize in arm pain treatments to aid individuals suffering from trigger points associated with the brachioradialis muscles along the wrist and hands of the body. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
The Brachioradialis Function On The Hands & Wrist
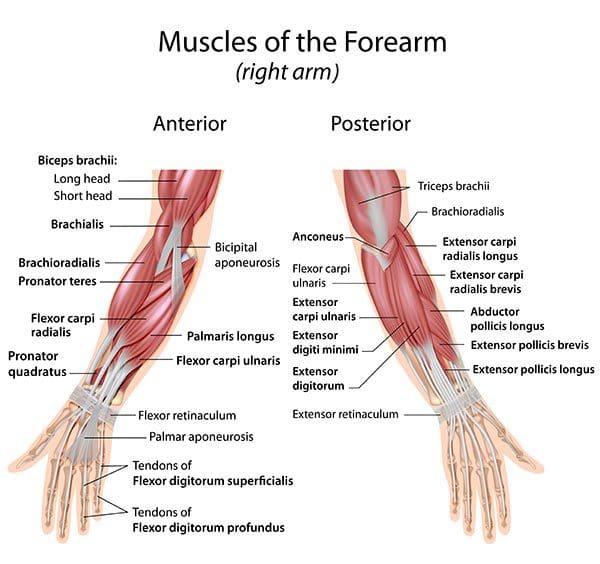
Have you been experiencing stiffness in your wrist or forearms? Do you have trouble gripping items in your hands? Or do you experience radiating pain from your forearms to your wrist? Many people experiencing these pain-like symptoms are associated with trigger points along the brachioradialis muscle that affect the forearms, hands, and wrist. The brachioradialis is a superficial muscle that is located in the lateral forearm. The brachioradialis muscle works with different muscles attached to the upper arms to provide flexion to the elbow joints while working with various muscle tendons along the wrist and hands. Research studies reveal that the brachioradialis muscle works with the central nervous system by sending signals to the forearm and provides reflexes to the wrist and fingers by lightly tapping the muscle tendon of the brachioradialis. This light tapping motion sends the signal back to the brain and shows which muscle is activated. However, injuries along the brachioradialis muscle can invoke referred pain to the wrist and hands.
Trigger Points Affecting The Hands & Wrist
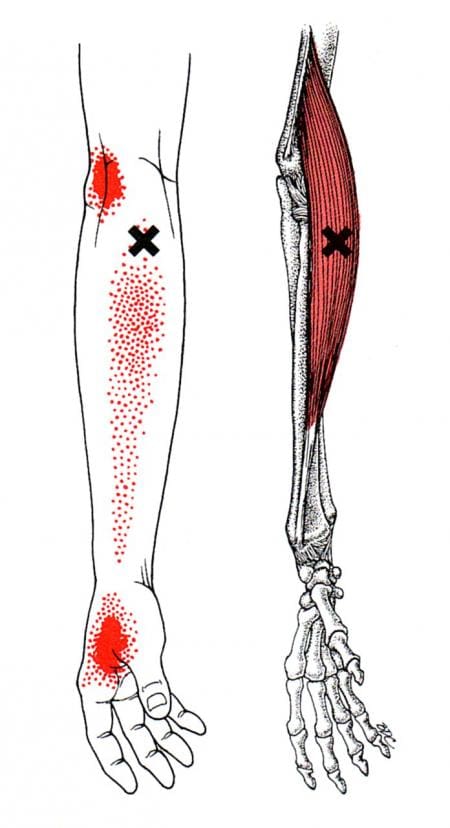
As stated in many research studies, trigger points or myofascial pain syndrome is a chronic musculoskeletal disorder that causes hard, discrete, tiny nodules along the taut muscle fiber bands of the affected muscle, causing pain. When the brachioradialis muscle has succumbed to pain-like symptoms from common factors or injuries, it can lead to the development of referred pain associated with trigger points affecting the hands and wrist of the body. So how would trigger points affect the hands and wrist? Well, trigger points can mimic other chronic conditions and cause pain to the affected muscles. So when trigger points affect the brachioradialis muscle, it also affects the hands and wrists.
Studies reveal that when trigger points affect the hands and the wrist, it can lead to symptoms of pain, stiffness, burning, or tingling sensations in the hands and wrist. To that point, a person can experience these pain symptoms even if they are not injured. Trigger points can form when the individual has made repetitive motions to the muscle that causes it to be overused and cause strain on the muscle, thus leading to trigger points associated with joint and muscle pain. Other studies reveal that non-specific shoulder pain associated with trigger points can increase pain intensity to the brachioradialis and affect hand grip strength. This can make many individuals unable to hold onto the items they carry.
Wrist & Hand Trigger Points- Video
Are you having trouble making a fist in your hands? Do you experience a burning sensation on your forearm down to your wrist? What about feeling pain radiating down from your elbows to your hands? Many people experiencing these pain symptoms might risk developing trigger points along the brachioradialis muscle affecting the hands and wrist. The video above explains what happens when trigger points affect the wrist and hand extensors muscles that work together with the brachioradialis muscles. Trigger points along the brachioradialis can cause referred pain to the forearms and lead to chronic symptoms that affect the functionality of the wrist and hands. This can lead to a decrease in grip strength and cause hand mobility issues for many people. At last, all is not lost, as various treatments are available to manage trigger points associated with the hands and wrist.
Managing Trigger Points Associated With The Hands and Wrist
Various treatments can help many individuals dealing with trigger points associated with the hands and wrist. Many people would go to pain specialists like chiropractors, massage therapists, or physiotherapists to manage trigger points affecting the brachioradialis muscles along the hands and wrist. These pain specialists will incorporate various techniques to reduce the pain and address the trigger points along the affected muscle. Studies reveal that acupuncture on the hands and wrist can reduce pain intensity caused by trigger points and bring back mobility function to the hands and wrist. This can regain the grip strength of the individual and improve hand and wrist functionality without pain. Other studies also reveal that trigger point therapy can also be utilized to reduce pain-like symptoms affecting the hands and wrist. Combined with gentle massages can prevent trigger points from forming in the future and reduce pain symptoms affecting grip mobility on the hands.
Conclusion
The forearms have a casual relationship with the hands and wrist as the brachioradialis muscles help provide mobility functions. The hands and wrist help grip items a person carries, while the forearms offer support. When injuries or ordinary factors are causing pain-like symptoms on the forearm, it can lead to the development of trigger points affecting the mobility function of the hands and wrist. To that point, it can lead to a burning sensation or decreased grip strength on the hands. This can affect a person as they won’t be able to hold onto items and are dealing with a numbing sensation along the wrist and hands. Luckily there are pain specialists available that can utilize various techniques to help manage trigger points along the affected muscle and help bring back grip function and mobility to the hands and wrist. People who incorporate these treatments as part of their daily life schedule can begin to get their sense of belonging back without pain in their wrists and hands.
References
Calvo Lobo, Cesar, et al. “Comparison of Hand Grip Strength and Upper Limb Pressure Pain Threshold between Older Adults with or without Non-Specific Shoulder Pain.” PeerJ, PeerJ Inc., 9 Feb. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5345821/.
Cao, Talia, and Prasanna Tadi. “Brachioradialis Reflex.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 26 Mar. 2022, https://www.ncbi.nlm.nih.gov/books/NBK554537/.
Hong, C Z. “Specific Sequential Myofascial Trigger Point Therapy in the Treatment of a Patient with Myofascial Pain Syndrome Associated with Reflex Sympathetic Dystrophy.” Australasian Chiropractic & Osteopathy : Journal of the Chiropractic & Osteopathic College of Australasia, BioMed Central, Mar. 2000, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2050812/.
Lung, Brandon E, et al. “Anatomy, Shoulder and Upper Limb, Forearm Brachioradialis Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 31 July 2021, https://www.ncbi.nlm.nih.gov/books/NBK526110/.
Oh, Sein, et al. “Causes of Hand Tingling in Visual Display Terminal Workers.” Annals of Rehabilitation Medicine, Korean Academy of Rehabilitation Medicine, Apr. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3660483/.
Trinh, Kien, et al. “The Effect of Acupuncture on Hand and Wrist Pain Intensity, Functional Status, and Quality of Life in Adults: A Systematic Review.” Medical Acupuncture, U.S. National Library of Medicine, 1 Feb. 2022, https://pubmed.ncbi.nlm.nih.gov/35251436/.
One of the many muscles that help stabilize the shoulders and provide movement when the arms are in motion. The tricep muscles are one of the most underrated muscles that many people don’t seem to take care of when working out. The other muscles in the upper arms and shoulders are more likely to be worked on when it comes to being physically active. The deltoids, biceps, and brachialis muscles are some of the muscles that get much more attention when working on shoulder mobility. Still, the triceps provide the functionality to the shoulders as well. When the shoulders or the upper arms are injured and develop pain-like symptoms in the muscle groups, it can develop trigger points along the affected muscle. Today’s article looks at the tricep muscles, how trigger points affect them, and ways to manage trigger points along the tricep muscles. We refer patients to certified providers who specialize in arm pain treatments to aid individuals suffering from trigger points associated with the tricep muscles along the upper arms and elbows. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
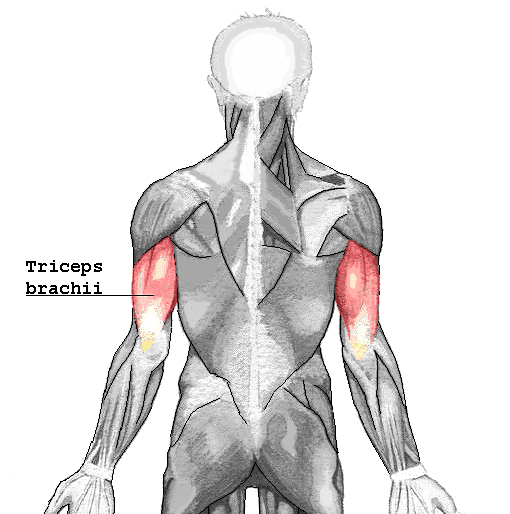
What Do The Tricep Muscles Do?
Do you experience pain underneath your forearm? How about feeling a dull ache on your elbows? Or do you feel a numbing sensation on your ring and pinky fingers? Individuals experiencing these symptoms in their arms could potentially develop trigger points along their tricep muscles. The tricep muscles are located under the upper arm and are a large, thick horseshoe-shaped muscle at the end of the arm. As stated earlier, the tricep muscles are one of the most underrated muscles in the arm that no one tends to work on during a workout, so they can be easily overlooked. However, the tricep muscles help in providing stability to the shoulders and help strengthen the arms. One of the main functions the triceps offer is that they allow the extension of the elbow joints. Studies reveal that the three head tendons that make up the triceps can influence elbow extension torque. The three heads of the triceps have different patterns of force when it comes to various activities during different shoulder evaluations. To that point, multiple combinations of the shoulder and elbows at different angles can affect the tricep’s shoulder extensions. Since many individuals don’t work on their triceps often, it can potentially develop issues that can make this underrated muscle weak.
How Trigger Points Affect The Tricep Muscles?
When the triceps don’t get worked on during a workout, it can lead to muscle weakness when doing pushups or when someone suffers from an injury with direct trauma in the elbows. When the tricep muscles become affected, it can lead to chronic conditions that are associated with myofascial pain or trigger points. Trigger points in the triceps can be formed when there are restrictions in extending the elbow joints. Studies reveal that when the triceps become overloaded from overusing the forearms from normal activities, it could potentially lead to tricep tendon rupture. To that point, which leads to the development of trigger points to invoke pain in the triceps and elbow joint. According to Dr. Janet Travell, M.D., trigger points associated with the tricep muscles could potentially involve referred pain in the vicinity of the elbow joints. What this refers to is that trigger points can mimic other chronic conditions so in this case, referred pain caused by trigger points associated with the tricep muscles can be mistakenly attributed to arthritis on the elbow joints. All is not lost, as there are ways to manage trigger points affecting the tricep muscles.
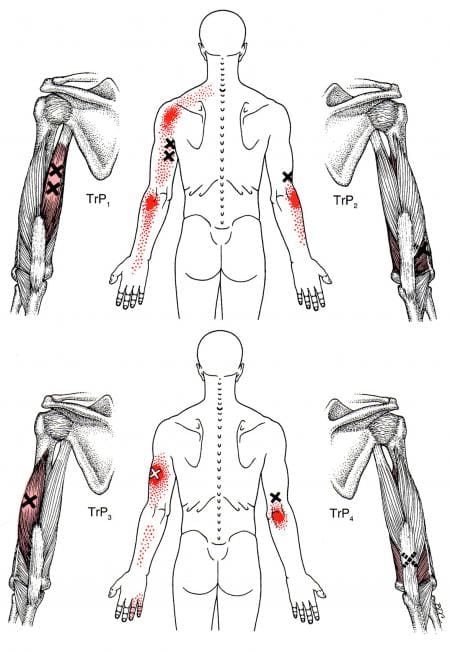
Treating Trigger Points On The Triceps- Video
Have you been experiencing pain in your shoulders, elbows, and hands? Do you have limited mobility when extending your elbows? Or do you notice that your triceps are weaker than normal? If you have been dealing with any of these symptoms, it could be due to trigger points associated with the tricep muscles that are causing referred pain to the upper arms and elbows. The triceps in the upper arms is one of the most underrated muscles people tend to overlook. When individuals begin to succumb to injuries that affect their triceps, it can lead to the development of trigger points along the muscle fibers in the tricep muscles. Trigger points can occur in the tricep muscles due to overusing the forearm muscles, causing stress in the elbow joint and the muscle itself. When the trigger points become active, it can lead to limited mobility to the elbow joint, causing the individual thinks they are developing arthritis when it is the trigger points causing the referred pain. There are ways that many people can manage trigger points associated with the elbows along the triceps to relieve the pain from the muscle. The video above shows where the active trigger points are located and how to release them through palpations and massage. Treating the trigger points along the tricep muscles allows many individuals to regain mobility in their elbows and upper arms.
Managing Trigger Points Along The Triceps
As stated earlier, the triceps are the underrated muscle that people tend to forget. When the tricep muscles succumb to trigger points, it can lead to referred pain along the elbow joints, causing pain-like symptoms affecting the elbow’s mobility function. When this happens to the upper arms, there are various ways to strengthen the tricep muscles and manage trigger points from developing in the future. Incorporating exercises targeting the tricep muscles can help improve mobility to the elbows and shoulders. If a person is playing sports like tennis, they can opt for a lighter racket and have a more lightweight grip on the handle. Suppose a person is in pain from their triceps. In that case, however, studies reveal that upper limb rehabilitation can help reduce the pain along the triceps and improve the mobility range caused by pain associated with trigger points. People can continue their daily activities without pain when they utilize these various ways to enhance their triceps’ functionality.
Conclusion
As the most underrated muscle that people tend to forget to work out, the tricep muscle can be overlooked. This large, thick horseshoe-shaped muscle has a job that provides stability to the shoulders and allows an extension to the elbow joints. When individuals don’t work on their tricep muscles, it can lead to muscle weakness and pain-like symptoms that lead to the development of trigger points. Trigger points associated with the tricep muscles can cause referred pain to the elbow joint, making many individuals believe they have arthritis. However, many individuals can regain mobility to their elbows by incorporating exercises targeting the triceps and utilizing treatments to manage trigger points along the muscle fibers. They can do daily activities that require the triceps without pain.
References
Landin, Dennis, et al. “Functions of the Triceps Brachii in Humans: A Review.” Journal of Clinical Medicine Research, Elmer Press, Apr. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5827912/.
Lennon, Olive, et al. “Effect of the Triceps Brachii Facilitation Technique on Scapulohumeral Muscle Activation during Reach and Point in a Healthy Population.” Physiotherapy Canada. Physiotherapie Canada, University of Toronto Press, 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6855346/.
Mangano, Tony, et al. “Chronic Tendonopathy as a Unique Cause of Non Traumatic Triceps Tendon Rupture in a (Risk Factors Free) Bodybuilder: A Case Report.” Journal of Orthopaedic Case Reports, Indian Orthopaedic Research Group, 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4719357/.
Tiwana, Manpreet S, et al. “Anatomy, Shoulder and Upper Limb, Triceps Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 6 Aug. 2021, https://www.ncbi.nlm.nih.gov/books/NBK536996/.
The upper extremities of the body, which include the head, neck, shoulders, chest, and arms, all have a specific job of keeping the body functioning and helping move from place to place. The head and neck work together to allow the host to have the mobility to turn, rotate from side to side, and lean from one side. The shoulders work with the arms to let the muscles have a full range of motion and even help stabilize the upper body. The shoulders have various muscles, tendons, and ligaments to protect the skeletal joints and even work to do everyday activities like carrying or lifting items. When injuries begin to affect the muscle groups of the upper body, it can lead to pain-like symptoms that can lead to chronic conditions developing over time if not treated right away. One of the muscles in the upper body is called the coracobrachialis muscle, which can be affected by injuries. Today’s article observes the coracobrachialis muscle, how trigger points affect the upper arm muscles, and how to manage trigger points associated with the coracobrachialis muscle. We refer patients to certified providers who specialize in shoulder pain treatments to aid individuals suffering from trigger points associated with the coracobrachialis muscles along the upper arms. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We established that education is a great solution to asking our providers profound questions the patient requests. Dr. Jimenez DC takes note of this information as an educational service only. Disclaimer
What Is The Coracobrachialis Muscle?
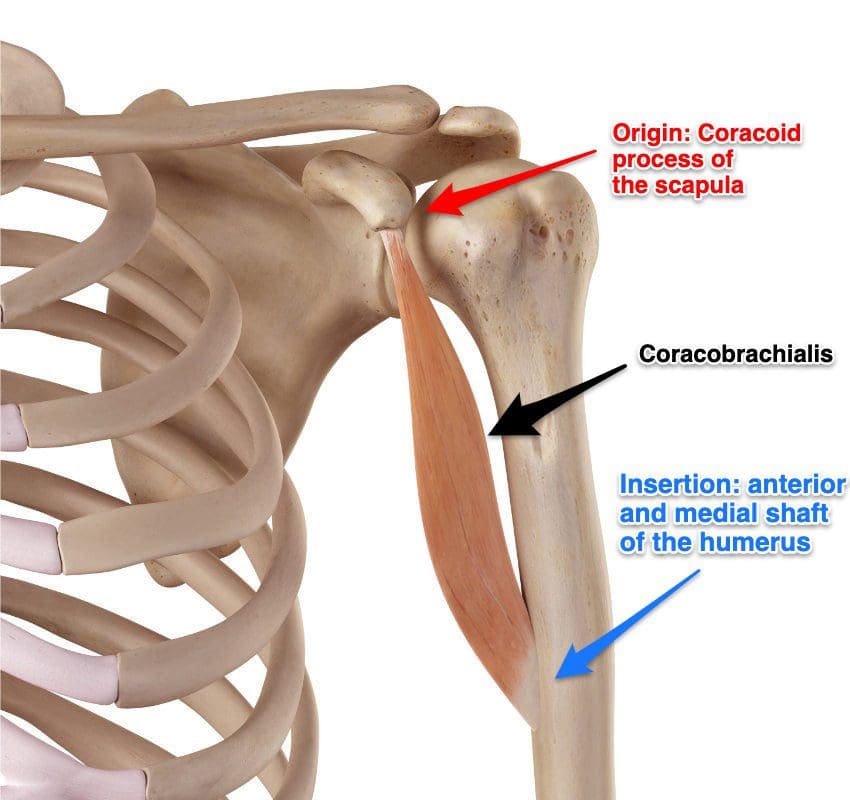
Have you been dealing with pain from the upper arms to the hands? Do simple arm and shoulder stretches seem to be difficult to do? Or have you been dealing with symptoms of pain, stiffness, or tenderness in your upper arms? Experiencing these pain-like symptoms could overlap other conditions affecting the upper arms and develop trigger points along the muscles, including the coracobrachialis. The coracobrachialis is the smallest muscle located in the front of the upper arm’s anterior that originated in the shoulder coracoid process. This small muscle is connected to the tendon located at the short head of the bicep brachii, and according to Dr. Janet Travell, M.D., the coracobrachialis muscle function helps flex and adduct the arms at the shoulders while working together with the surrounding muscles of the upper arm and shoulders. This allows the arms to move forward slightly and inward. This means that the coracobrachialis muscle will enable individuals to place their arms behind their back without pain. However, like any muscle in the body, injuries can occur in the upper arms and lead to the development of trigger points along the upper arm muscles affecting the coracobrachialis muscle.
How Trigger Points Affect The Upper Arm Muscles?
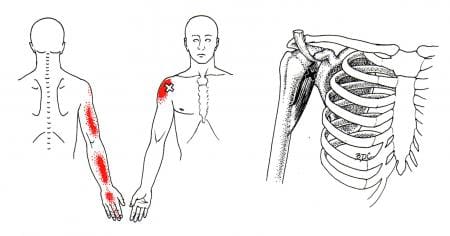
When the upper arm and the coracobrachialis muscle suffer from pain, tiny nodules along the muscle fiber bands known as trigger points can cause referred pain to the upper arms. Now trigger points are tricky to diagnose due to mimicking overlapping conditions affecting the upper arms. Studies reveal that non-specific arm pain could potentially be one of the causes that trigger points mimic due to strenuous physical activities or work-related activities that can overuse the upper arm muscles.
Studies reveal that individuals with idiopathic arm pain deal with high variable upper-extremity dysfunction, which could play a factor in pain-like symptoms along the surrounding muscles of the arms and shoulders. Many people often experience pain when reaching behind their back for the coracobrachialis affected by trigger points. Since the coracobrachialis works with the surrounding muscles in the shoulders and upper arms, trigger points associated with the coracobrachialis correspond to those muscles causing overlapping risk profiles. Trigger points affecting the coracobrachialis muscle can also mimic nerve entrapment since the coracobrachialis helps the bicep muscles when flexing. Pain associated with trigger points could potentially irritate the surrounding nerves in the muscle fibers, which causes radiating pain along the arms.
Treating The Coracobrachialis Muscle-Video
Does your arm feel stiff when trying to reach behind your back? Do your shoulders ache for no apparent reason? Or have you experienced sharp, shooting pain down your arm? Many people experience pain along their shoulders and arms, affecting their mobility to hold and carry items. They deal with overlapping symptoms associated with trigger points along the coracobrachialis muscle. Trigger points along the coracobrachialis muscle are developed when the upper arm muscles have been overused and irritate the surrounding nerves. This causes radiating referred pain down the arms and can affect a person’s ability to hold items. Thankfully there are ways to manage trigger points along the coracobrachialis and its surrounding muscles. The video above demonstrates a massage technique that works along the coracobrachialis muscle to release nerve entrapment and manage trigger points along the surrounding muscles.
Ways To Manage Trigger Points Affecting The Coracobrachialis
There are various techniques that many specialists, like chiropractors, massage therapists, and physiotherapists, can use to identify and manage trigger points in the body. Since trigger points are tricky to diagnose due to causing referred pain along the surrounding muscles, treatments like stretching, massages, acupuncture, and chiropractic adjustments can help alleviate the pain and reduce future trigger points from forming. Studies reveal that pain specialists could manage trigger points associated with shoulder pain along the coracobrachialis through treatments of manual compression and other various techniques. Once treatments have been incorporated to relieve trigger point pain along the affected muscle, many people can further prevent the symptoms from returning by not lifting or carrying heavy objects and not forcing their coracobrachialis to be a substitute for their bicep muscles.
Conclusion
The coracobrachialis is a short muscle that works with the bicep muscle and helps with mobility and motor functions for the arms and shoulders. This muscle allows the arms to move forward and can be placed in the back without pain. When muscle injuries affect the surrounding muscles that work with the coracobrachialis, it can develop trigger points associated with pain along the upper arms. When this happens, it can lead to symptoms of stiffness, pain, and tenderness in the upper arms, causing mobility issues. Pain specialists for trigger points can utilize various treatments to relieve the pain and reduce the effects that trigger points cause on the affected muscle. This allows the upper arms to gain mobility back and the host to do various activities without feeling pain.
References
Bron, Carel, et al. “Treatment of Myofascial Trigger Points in Patients with Chronic Shoulder Pain: A Randomized, Controlled Trial.” BMC Medicine, BioMed Central, 24 Jan. 2011, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3039607/.
Georgiev, Georgi P, et al. “Coracobrachialis Longus Muscle: Humeroepitrochlearis.” Cureus, Cureus, 13 May 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6044495/.
Moradi, Ali, et al. “Nonspecific Arm Pain.” The Archives of Bone and Joint Surgery, Archives of Bone and Joint Surgery Co., Dec. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4151410/.
Ring, David, et al. “Idiopathic Arm Pain.” The Journal of Bone and Joint Surgery. American Volume, U.S. National Library of Medicine, July 2004, https://pubmed.ncbi.nlm.nih.gov/15252084/.
The shoulders help stabilize the upper extremities of the body and provide a wide range of movements for the arms. The shoulders have many muscles, ligaments, and tendons that help support the joints from injuries and utilize the motor function to do everyday actions like throwing a ball or stretching for long distances. Even though the shoulders help stabilize the upper extremities, they are still prone to injuries since the shoulder muscles are constantly used throughout the day. One of the shoulder muscles that are continuously utilized is the deltoid muscle, which can lead to the development of trigger points when it becomes injured. Today’s article examines the deltoid muscles, how trigger points affect the deltoids and shoulders, and managing trigger points associated with the deltoid muscles. We refer patients to certified providers specializing in shoulder pain treatments to aid individuals suffering from trigger points associated with the deltoid muscles along the shoulders. We also guide and inform our patients by referring them to our associated medical providers based on their examination when appropriate. We ensure that education is a great solution to asking our providers insightful questions the patient requests. Dr. Jimenez DC observes this information as an educational service only. Disclaimer
What Is The Deltoid Muscle?
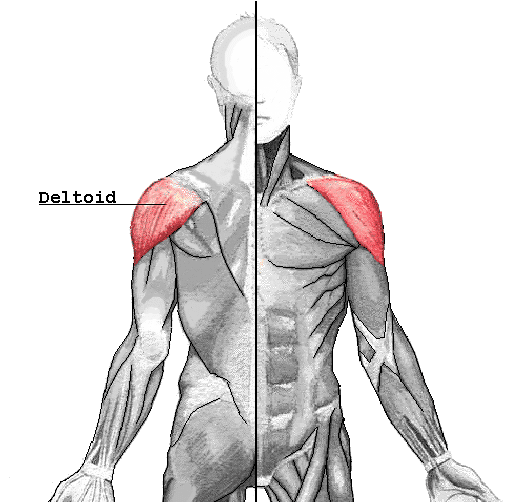
Have you been feeling pain on the top of your shoulders? Do your shoulders feel stiff when rotating them? Or do you feel radiating pain along your upper arms? Individuals with shoulder pain may be experiencing trigger points affecting their deltoid muscles. The deltoids are large triangular-shaped muscles that are associated with the shoulder girdle. The deltoids sit on top of the shoulder girdle and have anterior and posterior sections that work together with the rotator cuff muscles that provide a full range of motion to the arms. Studies reveal that the deltoid muscles have a more complex structure since the intramuscular tendons from the deltoids help provide different functions when it comes to the shoulders and arms’ motor function. According to Dr. Janet G. Travell, M.D., the anterior sections of the deltoid muscles are used in sports activities. In contrast, the posterior section works with the rotator cuff muscles for mobility. Injuring the deltoid muscles can lead to the development of trigger points associated with shoulder pain.
How Do Trigger Points Affect The Deltoids & Shoulders?
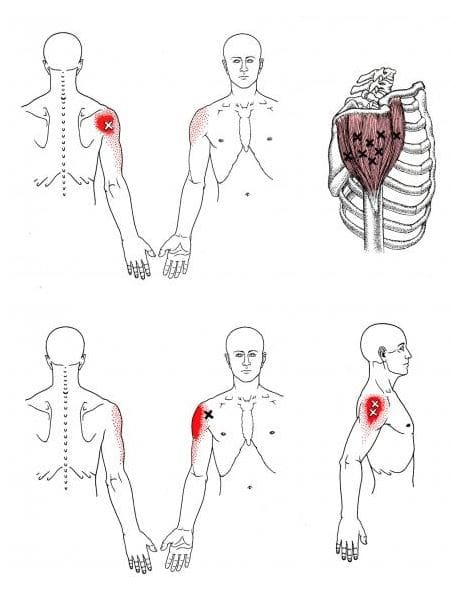
Regarding the shoulders, they can succumb to various injuries that can become an issue over time, lead to the development of trigger points in the shoulder muscles, and cause referred pain to the upper arms. Trigger points or myofascial pain syndrome along the deltoid muscles may invoke referred pain to the shoulders. Studies reveal that myofascial pain syndrome is often described as the sensory, motor, and autonomic symptoms caused by trigger points that cause tender spots on the hardened muscle to produce pain. Trigger points are a bit tricky to diagnose since they mimic other chronic conditions in the body. The deltoid muscles are superficial, and trigger points can cause referred pain to the muscles that mimic arthritis in the shoulder joints. Some of the other symptoms associated with trigger points along the shoulders and deltoids include:
Limited range of mobility
Tenderness in the shoulder muscles
Muscle spasms
Muscle pain
Stiffness in the deltoid muscles
Pain in the shoulders can cause the body to become unstable and cause many individuals to develop a hunched position over time to reduce the pain they are feeling; fortunately, there are various ways to manage the pain associated with trigger points along the shoulders and deltoid muscles.
Trigger Point Release On The Deltoid Muscle- Video
Have you been feeling stiffness along the shoulders or the deltoid muscles? Have you experienced muscle tenderness in your upper arms? Or do you feel like being hunched over reduces the pain in your shoulders? If you have been experiencing any of these symptoms, it could be the development of trigger points associated with shoulder pain along the deltoid muscles. Trigger points cause referred pain to the affected muscle area and are developed when the muscles are overused. For the deltoid muscles, when active trigger points affect the deltoids’ anterior or posterior sections, it can cause the muscles to twitch and later cause moderate tension. The video above explains where the trigger points are located on the deltoid muscles and how to release them through palpations and massages. This is one of the techniques that can help manage trigger points from affecting the shoulders and deltoid muscles.
Managing Trigger Points Associated With The Deltoid Muscles
When dealing with trigger points associated with the deltoid muscles can be managed through various techniques that many people can utilize to reduce the pain symptoms along the upper arms and shoulders. Studies reveal that dry needling is one of the techniques that can relieve trigger points to ease the pain intensity and irritability to the shoulders. Other techniques that many people can utilize are to correct how they carry heavy objects to reduce the load on their shoulders, stretch the arms and shoulders to minimize soreness and alleviate tight muscles, and even take a hot shower to relax the shoulder muscles, can reduce the chances of trigger points from forming in the future.
Conclusion
The deltoid is located on top of the shoulder girdle and is a large triangular-shaped muscle that works together with the rest of the shoulder and the rotator cuff muscles. The shoulders have many muscles, ligaments, and tendons that provide stability and perform everyday functionality to the body. When the shoulders become injured, the affected muscles could potentially develop trigger points to cause referred pain to the shoulders and upper arms. When trigger points affect the deltoid muscles, it can cause them to have symptoms of stiffness, tenderness, and pain that mimic other chronic conditions affecting the shoulders and arms. Thankfully, various techniques relieve referred pain from the arms and help manage trigger points along the deltoid muscle. This allows the deltoid muscle to relax and reduce trigger points from developing further on the shoulders.
References
Bron, Carel, and Jan D Dommerholt. “Etiology of Myofascial Trigger Points.” Current Pain and Headache Reports, Current Science Inc., Oct. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3440564/.
Calvo-Lobo, César, et al. “Dry Needling on the Infraspinatus Latent and Active Myofascial Trigger Points in Older Adults with Nonspecific Shoulder Pain: A Randomized Clinical Trial.” Journal of Geriatric Physical Therapy (2001), Wolters Kluwer Health, Inc., 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5728593/.
Elzanie, Adel, and Matthew Varacallo. “Anatomy, Shoulder and Upper Limb, Deltoid Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 15 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK537056/.
Many individuals do not realize they are in pain until they begin to feel symptoms of stiffness or tenderness in certain areas of their body. Many people have two most common complaints: back and shoulder pain. The shoulder and the back have a casual relationship that stabilizes the upper body and protects the spine’s thoracic region. When injuries or ordinary factors affect not only the shoulders but the back, it can lead to symptoms of pain and stiffness along the muscles, causing the development of trigger points along the upper back and shoulder muscles. One of the muscles affected by trigger points is the rhomboid muscles located in the upper back behind the scapula (shoulder blades). Today’s article looks at the rhomboid muscle, how superficial backaches and round shoulders can affect the rhomboid muscle, and managing trigger points associated with the rhomboid muscle. We refer patients to certified providers specializing in back pain treatments to aid individuals suffering from trigger points associated with the upper back along the rhomboid muscles. We also guide our patients by referring them to our associated medical providers based on their examination when appropriate. We ensure that education is a great solution to asking our providers insightful questions. Dr. Jimenez DC observes this information as an educational service only. Disclaimer
What Is The Rhomboid Muscle?
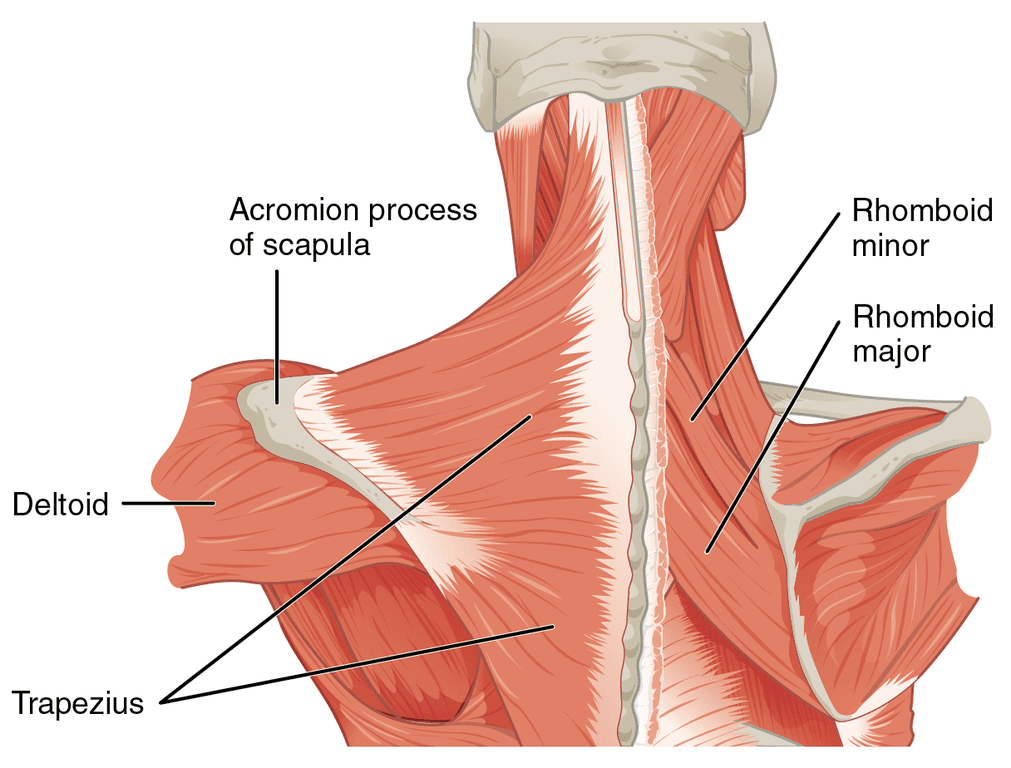
Do muscle stiffness in your shoulders seem to be causing you pain? Have you noticed that your shoulders seem more rounded than usual? What about the unexplainable upper backaches after being in a hunched position for a long period? Many individuals with these pain symptoms could be associated with the rhomboid muscles. The rhomboid muscles are a collective group of muscles important for upper limb movement and stability for the shoulder’s girdle and scapula. The rhomboid muscles consist of two separate muscles: the rhomboid minor and the rhomboid major, deep within the trapezius muscle and behind the scapula (shoulder blades). The functionality of the rhomboid is that they provide stability to the shoulder and when they are active, the upper arms move back and forth while walking.
How Superficial Backaches & Round Shoulders Affect The Rhomboid
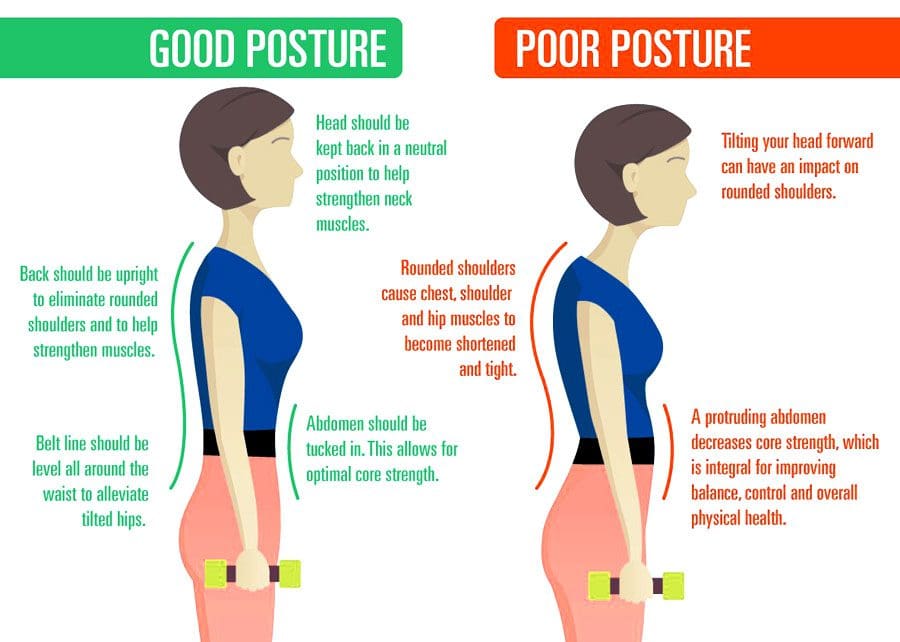
While the rhomboid muscles provide stability to the shoulders, they can succumb to pain like any muscles in different body sections. Ordinary factors like a bad sitting posture can cause the upper back and shoulder muscles to contract and strain. Studies reveal that the effects of bad sitting posture can lead to the development of a forwarding head posture with rounded shoulders, causing pain in the rhomboid muscles. When the shoulder muscles, like the rhomboid muscles, experience this sort of change over time, it can increase muscle tone and continuous stress in the neck and shoulders. To that point, it can lead to various symptoms like pain, numbness, loss of functionality in the upper limbs, and nerve root symptoms. Other issues like back pain can also be one of the symptoms that can lead to referred pain in the rhomboid muscles and can potentially lead to the development of trigger points along the shoulders and rhomboid muscles.
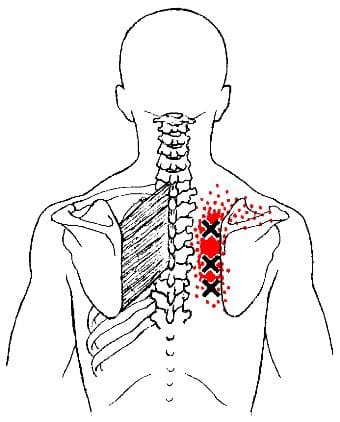
Other issues that can affect the rhomboid muscles are trigger points. Trigger points can be latent or active as they are tiny knots formed in the body’s muscle fibers. For the rhomboid muscles according to Dr. Janet G. Travell, M.D., when a person hears snapping and crunching noises during the movement of the shoulder blades, it may be due to the trigger points in the rhomboid muscles. Studies reveal that since trigger points can be either active or latent and elicit local referred pain, that can lead to muscle imbalance, weak and impaired motor function, and expose the joints to suboptimal loading. This means that trigger points in the rhomboid muscles can cause referred pain to the shoulder and mimic other chronic symptoms.
Stretching The Rhomboid Muscle & Managing Trigger Points-Video
Do you hear any snapping or crunching noises when rotating your shoulders? What about muscle stiffness along your shoulders or upper back? Or do you feel muscle aches from being hunched over for a long time? These symptoms could potentially involve trigger points associated with the rhomboid muscles. The rhomboid muscles help stabilize the shoulders and provide movement to the arms. When people overuse their shoulder muscles, it can cause the surrounding muscles to develop trigger points and inflict pain-like symptoms on the shoulders and upper back. Thankfully, all is not lost, as various treatments are available to relieve shoulder and upper back pain associated with trigger points along the rhomboid muscles. The video above explains where the trigger points are located on the rhomboid muscles and how to stretch that muscle to relieve trigger points from causing referred pain to the shoulders.
Managing Trigger Points Associated With The Rhomboid Muscle
Since the rhomboid muscles can become stiff due to overuse and could develop trigger points to inflict pain along the upper back and shoulders, this can cause many symptoms associated with pain and make the individual feel hopeless. Thankfully, various treatments can help manage trigger point pain associated with the rhomboid muscles. Studies reveal that thoracic spinal manipulation can relieve pain pressure sensitivity of the rhomboid muscles. Chiropractors are excellent when finding trigger points along the musculoskeletal system by utilizing spinal manipulation on the thoracic spine to loosen up the stiff muscles along the shoulders and upper back. Another way to manage trigger points associated with the rhomboid muscle is to stretch the shoulder muscles after a hot shower. This allows the muscles to relax and prevent future trigger points from forming along the rhomboid muscles.
Conclusion
The rhomboid muscles are a collective muscle group that has an important function in stabilizing the shoulder’s girdle and scapula (shoulder blades) while providing upper limb movement. The rhomboid muscles consist of two separate muscles: rhomboid minor and rhomboid major, which are behind the shoulder blades and deep within the trapezius muscles. When ordinary factors like poor posture or shoulder injuries affect the rhomboid muscles, it can develop trigger points that can cause stiffness in the rhomboid muscles. Various techniques can alleviate the referred pain along the shoulders, causing trigger points to develop along the rhomboid muscles. When these treatments are utilized on the rhomboid muscles, they can help prevent future shoulder issues.
References
Farrell, Connor, and John Kiel. “Anatomy, Back, Rhomboid Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 20 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK534856/.
Haleema, Bibi, and Huma Riaz. “Effects of Thoracic Spine Manipulation on Pressure Pain Sensitivity of Rhomboid Muscle Active Trigger Points: A Randomized Controlled Trial.” JPMA. The Journal of the Pakistan Medical Association, U.S. National Library of Medicine, July 2021, https://pubmed.ncbi.nlm.nih.gov/34410234/.
Ribeiro, Daniel Cury, et al. “The Prevalence of Myofascial Trigger Points in Neck and Shoulder-Related Disorders: A Systematic Review of the Literature.” BMC Musculoskeletal Disorders, BioMed Central, 25 July 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6060458/.
Yoo, Won-Gyu. “Effects of Pulling Direction on Upper Trapezius and Rhomboid Muscle Activity.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, June 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5468195/.
Look how young children position their backs. There is a natural S curve, and their movements are effortless. As the body ages, too much sitting, slouching, and inactivity can cause muscle fatigue and tension leading to posture issues. Rounded shoulders describe a resting position that has shifted the shoulders out of the body’s natural alignment, which can worsen if left untreated. Chiropractic care can realign the shoulders, as well as the spine, and restore musculoskeletal health to optimum levels.
Rounded Shoulders
Rounded shoulders are an excessive thoracic kyphosis referring to an uneven forward rounding or curvature of the middle and upper back. Rounded shoulders shift out of proper alignment with the spine, causing posture-related problems like shoulder/neck/back discomfort, tightness, stiffness, and pain. Overall unhealthy posture contributes to the following:
The head constantly being in a forward or backward position
Headaches
Body aches and pains
Muscle fatigue
Chronic back soreness
Bent knees when standing or walking
Body movement dysfunction
Joint problems
Potbelly
Rounded shoulders
Body responses to rounded shoulders include:
Chronic musculoskeletal aches and pains
Breathing problems
Limited body function
Impaired mobility performance
Increased mental and musculoskeletal stress
Causes
Rounded shoulders are typically caused by unhealthy posture, but can also be caused by muscle imbalances from, for example, overfocusing on building chest strength but neglecting the core and upper back. Other causes include:
Standing and sitting for long periods
Stress
Lack of physical activity
Environmental factors
Too much exercise, sports, and physical activities
Musculoskeletal Imbalance
Postural imbalances anywhere in the body can cause rounded shoulders.
For example, when an individual tilts their head forward to look at their phone, the upper back has to round forward to hold the head. Constantly tilting can begin to generate an unhealthy muscle memory causing the neck and shoulder muscles to remain in a semi-flexed position that starts to become the norm.
Another example is when the arms are held out and in front for prolonged periods, like driving, typing, and cooking, the chest muscles get shortened. As time goes on, this causes the shoulder blades to move forward on the ribcage, making the upper back and shoulder area hunch awkwardly and unhealthily.
Stress
When the brain perceives a threat, the body physically prepares to take action through the fight or flight response. Common reactions include:
Jaw tensing
Tightening the abdominal muscles
Holding one’s breath
Rounding the shoulders
Stressors can include:
Job worries
Money issues
Relationship problems
Family responsibilities
All can cause changes in the body that result in rounded shoulders.
Environmental Factors
Respiratory conditions like asthma, COPD, and allergies can affect the body’s breathing and the ability of the diaphragm to contract and relax correctly.
Ribcage restrictions caused by chronic breathing problems can result in the thoracic/middle back tightening up, causing excessive shoulder rounding.
Exercise and Physical Activities
Exercise and physical activities can contribute to rounded shoulders because of the long periods of spinal flexion. These can include:
Bike riding, martial arts, and swimming.
Knitting requires the arms to be out in front.
Gardening requires kneeling and being hunched over.
Chiropractic Treatment
Chiropractic adjustments, therapeutic massage, and decompression therapy can unlock tight shoulder and chest muscles. A chiropractor uses gentle targeted adjustments to relieve pain, restore function, and retrain the muscles.
The doctor will look at the individual’s resting position while standing.
An individual with slumped shoulders can slouch, even when standing up straight.
Their hands will likely face behind them, with their thumbs pointed at each other.
Once the adjustments are made, a correct standing posture will make the hands face the body with the thumbs facing ahead.
Exercises will be recommended to strengthen the core and stretches to maintain the adjustments.
Posture Chiropractic
References
Fathollahnejad, Kiana, et al. “The effect of manual therapy and stabilizing exercises on forward head and rounded shoulder postures: a six-week intervention with a one-month follow-up study.” BMC musculoskeletal disorders vol. 20,1 86. 18 Feb. 2019, doi:10.1186/s12891-019-2438-y
Go, Seong-Uk, and Byoung-Hee Lee. “Effects of scapular stability exercise on shoulder stability and rehabilitative ultrasound images in office workers.” Journal of physical therapy science vol. 28,11 (2016): 2999-3002. doi:10.1589/jpts.28.2999
Kwon, Jung Won, et al. “Changes in upper-extremity muscle activities due to head position in subjects with a forward head posture and rounded shoulders.” Journal of physical therapy science vol. 27,6 (2015): 1739-42. doi:10.1589/jpts.27.1739
Lee, Do Youn, et al. “Changes in rounded shoulder and forward head posture according to exercise methods.” Journal of physical therapy science vol. 29,10 (2017): 1824-1827. doi:10.1589/jpts.29.1824
Park, Sang-In, et al. “Effects of shoulder stabilization exercise on pain and functional recovery of shoulder impingement syndrome patients.” Journal of physical therapy science vol. 25,11 (2013): 1359-62. doi:10.1589/jpts.25.1359
The body is a functional machine that requires many muscles, organs, ligaments, joints, and tissues that provide everyday movements. In the upper extremities, the head, neck, and shoulders have many muscles, ligaments, and tissues that work together with the nerve roots from the nervous system that provides sensory-motor function to make the fingers move, the shoulders rotate, and the head turns from side to side. When injuries or common issues affect the muscles in the head, neck, or shoulders, it can cause small nodules to form along the muscle fibers of the affected muscle area and cause referred pain in different locations of the body. Today’s article looks at the scalene muscles, how trigger points affect the scalene muscles while mimicking shoulder pain, and how to manage chronic pain associated with trigger points. We refer patients to certified providers who specialize in musculoskeletal treatments to aid individuals suffering from trigger points related to the shoulders affecting the scalene muscles. We also guide our patients by referring them to our associated medical providers based on their examination when appropriate. We ensure to find that education is the solution to asking our providers insightful questions. Dr. Jimenez DC observes this information as an educational service only. Disclaimer
What Are The Scalene Muscles?
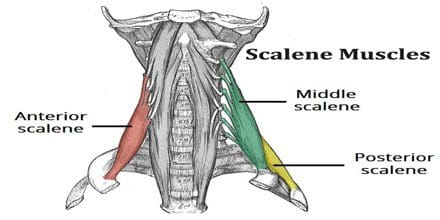
Have you been experiencing tingling sensations running down your fingertips? Do you feel stiffness when rotating your neck or shoulders? Or do you feel muscle soreness in your shoulders? Many individuals who are feeling any of these symptoms affecting their neck or shoulders could be dealing with trigger point pain along the scalene muscles. The scalene muscles play a crucial part in the head and neck as they are deep muscles positioned laterally on the cervical tract of the spine. These muscles have three different branches: the anterior, medius, and posterior, which play the role of being accessory breathing muscles while being an important contributor to head and neck movement. To that point, it allows stability to the cervical spine. The scalene muscles even help support and elevate the upper rib cage when a person is lifting, pulling, or carrying heavy objects. However, like most muscles in the body, the scalene muscles can be prone to injury and can develop issues that can affect the upper extremities of the body.
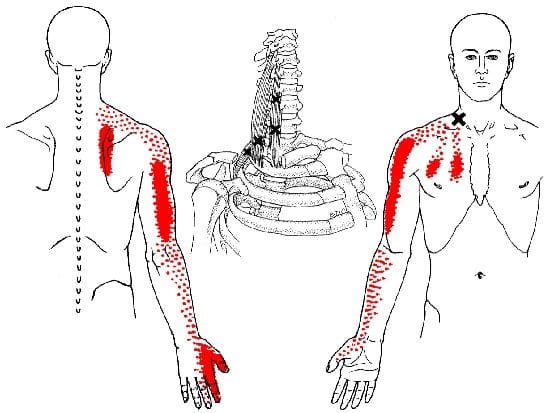
Trigger Points Affects The Scalene Muscles Mimicking Shoulder Pain
When common injuries like pulling a muscle when carrying a heavy object or even a traumatic injury like being involved in an auto accident can cause pain in the affected area, over time, if not treated, can cause various symptoms to overlap and affect the muscles. When the scalene muscles are affected by injuries, they can develop tiny nodules along the taut muscle fibers and become hyperirritable to the surrounding areas of the upper half of the body. This is known as trigger point pain and can mimic other chronic issues that affect different body areas. To that point, trigger points affecting the scalene muscles may mimic shoulder pain in the upper half of the body. Studies reveal that scalene myofascial pain is a regional pain syndrome that originates pain in the neck area and radiates pain down to the arm. Since trigger points mimic other chronic issues, it is often misdiagnosed as another neck pain associated with radiculopathy when the scalene muscles are affected. When this happens, the muscles become stiff and weak, causing a reduction in the range of movement.
Studies reveal that when individuals suffer from acute whiplash-associated disorders, the local and referred pain can be elicited from active trigger points to reproduce neck and shoulder pain. This causes a higher disability that exhibits widespread pressure causing the muscles to be hypersensitive and reducing the cervical range of motion. Many individuals often complain about shoulder pain while rubbing the upper parts of their arms. The scalene muscle is affected by active trigger points, thus mimicking shoulder pain.
Scalenes Trigger Points-Video
Have you been feeling muscle stiffness in your neck or shoulders? Have you been experiencing a numbing sensation along your arms? Have you felt tenderness along your shoulders when you touch them? Many of these pain symptoms are associated with trigger points along the scalene muscles. The video above explains where the trigger points are located along the scalene muscles and how they are causing referred pain in the neck and shoulder areas. Many factors can lead to the causation of trigger point pain and overlap with other chronic issues that can affect the upper extremities of the body, using sleep as an example. Studies reveal that poor sleeping posture can affect the neck and shoulders, leading to muscle stiffness along the scalene muscles and developing trigger points over time. Fortunately, various ways to manage referred shoulder pain are associated with trigger points.
Management Of Chronic Shoulder Pain Associated With Trigger Points
Many individuals are referred to pain specialists that can alleviate trigger points along the scalene muscle to reduce the effects of shoulder and neck pain. When referred pain along the scalene muscles causes chronic shoulder pain associated with trigger points, many people often do various movements to alleviate the pain. However, it can cause more pain in the affected area and prevent relief from the neck and shoulders. Studies reveal that various treatments like physiotherapy, trigger point injections, manipulation of the cervical spine, or acupuncture can help relax and lengthen the muscle fibers associated with the scalene muscle. To that point, this allows the neck to extend further without pain and reduces the overlapping symptoms that affect the upper extremities of the body.
Conclusion
The scalene muscles play a crucial part in the head and neck area as deep muscles are positioned laterally on the cervical tract of the spine. These muscles help elevate the upper chest and laterally bend the neck from side to side. When injuries affect the scalene muscles and form tiny nodules known as trigger points, it can cause referred pain to the shoulders and the neck. To that point, symptoms like numbing or tingling sensations can travel down the arms and fingers. Fortunately, available treatments can reduce the symptoms and manage myofascial trigger pain along the shoulders and neck associated with the scalene muscles. This allows a better range of motion to the neck and shoulder and prevents future trigger points from forming in the scalene muscles.
References
Abd Jalil, Nizar, et al. “Scalene Myofascial Pain Syndrome Mimicking Cervical Disc Prolapse: A Report of Two Cases.” The Malaysian Journal of Medical Sciences : MJMS, Penerbit Universiti Sains Malaysia, Jan. 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3216145/.
Bordoni, Bruno, and Matthew Varacallo. “Anatomy, Head and Neck, Scalenus Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 16 Apr. 2022, https://www.ncbi.nlm.nih.gov/books/NBK519058/.
Fernández-Pérez, Antonio Manuel, et al. “Muscle Trigger Points, Pressure Pain Threshold, and Cervical Range of Motion in Patients with High Level of Disability Related to Acute Whiplash Injury.” The Journal of Orthopaedic and Sports Physical Therapy, U.S. National Library of Medicine, July 2012, https://pubmed.ncbi.nlm.nih.gov/22677576/.
Lee, Won-Hwee, and Min-Seok Ko. “Effect of Sleep Posture on Neck Muscle Activity.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, June 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5468189/.
Thapa, Deepak, et al. “Management of Chronic Shoulder Pain with Restricted Mobility – a Case Series.” Indian Journal of Anaesthesia, Medknow Publications & Media Pvt Ltd, Nov. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5125193/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine