It’s no secret that sitting for long stretches�isn’t great for your body. Research has linked it to heart disease, obesity, diabetes, even�cancer. But there’s another health risk from sitting all day that most people don’t know about: gluteal amnesia, or�dead butt syndrome.
It almost sounds like a joke, but it’s not uncommon, says Andrew Bang, a chiropractor at the Cleveland Clinic�s Wellness Institute: �I see the injury all the time in varying degrees.”
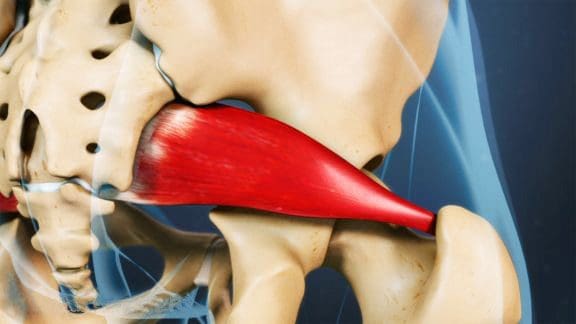
Dead butt syndrome develops when the gluteus medius�one of the three main muscles in the booty�stops firing correctly.�That can happen if you spend too much time parked in a chair, explains Kristen Schuyten, a physical therapist at Michigan Medicine. “But it can�also occur in very active individuals who just don�t engage the glute muscles enough,� she adds.
Since the gluteus medius�normally helps stabilize the pelvis, gluteal amnesia can lead to�lower back�pain and hip pain, as well as knee and ankle issues, as the body tries to compensate for the imbalance.
Dead butt syndrome has to do with reciprocal inhibition�the process that describes the give-and-take relationship between muscles on either side of a joint. “In general, when one muscle contracts, a nerve signal is sent to its opposing muscle to relax,� says Bang.
When you spend hours on end in a seated position, your hip flexors are contracting while your glutes�rest.��Over time, we�re basically training our glutes to be weak,� Bang says.
The same type of muscle imbalance�can happen in highly active people who have very strong�quads or hamstrings. Bang has�even seen marathon runners develop dead butt syndrome
One�way practitioners�diagnose the condition is with�the Trendelenburg test, a physical exam in which a person lifts�one leg in front of them while standing. �If the pelvis dips down on the side of the body where the leg is lifted, that indicates weakness in the gluteus medius on the opposite side,� says Bang.
The curve in a person’s�back can also suggest�gluteal amnesia. While the lumbar spine�(or lower back) should naturally form an S shape, more extreme curvature�may signal that the hip flexors are so tight they�re pulling the spine forward,�says Bang.
Try to take frequent breaks from your chair throughout the day. Get up and walk around, or do some stretches at your desk.�Schuyten recommends setting hourly reminders on your phone,�to prompt you to squeeze your butt muscles at regular intervals.
And when you work out, don’t forget to target that booty. Along with squats and�bridges,�lying-down leg lifts are a good move to add to your routine, says Bang.��Start on your left side with your right leg lifted and the big toe pointing toward the floor as you lift,� he�says. �This angle isolates the gluteus medius and minimus�muscles the most, so you�ll feel it within 10 to 15 lifts of the leg.� Add a band or ankle weight for extra resistance.
Above all, the best way to avoid gluteal amnesia is to mix up your daily routine, says Bang. Sit on an exercise ball for part of the day. Spend some time standing up, working at a high countertop. �Whatever you do, just don�t allow your body to get into a repetitive cycle,� he says.
SUGAR GROVE, Il.- UTEP men�s golfer Frederik Dreier earned PING All-Region Division I honors, the Golf Coaches Association of America (GCAA) announced on Saturday. Dreier, who wrapped up his collegiate career at the NCAA Washington Regional on May 17, earned a spot on the Central Regional list. He was the only UTEP honoree and one of the two Conference USA golfers to be recognized this year, with Middle Tennessee�s Joey Savoie making the Southeast Regional list.
Dreier helped lead the Miners to the Conference USA championship with his seventh place finish, the first conference title since 1985 and only the second championship in program history. The victory ticketed the team to the NCAA Regionals for the first time since 2004, where they finished in ninth place. Dreier shot 7-over 220 (76-68-76) to end his second appearance at the NCAA Regional with a share of 27th place.
A staple in the Miner�s lineup for four years, Dreier played in 46 tournaments while tallying 72.8 collegiate career stroke average. He was named the C-USA Golfer of the Year for the second consecutive year, the first Miner to accomplish the feat and only the third golfer in C-USA to repeat the honor. He also gained C-USA First Team recognition. Dreier has been ranked as high as no. 4 on the Arnold Palmer Cup European rankings and has been on the Danish national team since 2011.
A complete list of the all-region teams are below.
Division I PING All-Region Teams
Northeast
Cole Berman, Georgetown
Bennett Buch, Maryland
Tim Colanta, Maryland
Michael Davis, Princeton
Ryan Davis, Penn State
Robert Deng, Harvard
Eric Dietrich, Connecticut
Anton Frondelius, Wagner
Lloyd Jefferson Go, Seton Hall
Jimmy Hervol, Connecticut
Chris Houston, Rhode Island
JD Hughes, Penn State
Charles Huntzinger, Penn State
Dawson Jones, Rhode Island
Peter Kim, Army
David Kocher, Maryland
Jonathan Lai, Yale
Logan Lowe, George Washington
Sam Madsen, Georgetown
Cole Miller, Penn State
Gen Nagai, Seton Hall
Matthew Naumec, Boston College
Gregory Royston, Harvard
Kendrick Vinar, Harvard
Billy Walthouse, Rhode Island
East
Eric Bae, Wake Forest
Derek Bard, Virginia
James Clark, Georgia Tech
Ryan Cole, James Madison
Patrick Cover, UNCW
Chandler Eaton, Duke
Stephen Franken, NC State
Ben Grif n, North Carolina
Mark Lawrence Jr., Virginia Tech
Isaiah Logue, Liberty
Alexander Matlari, Duke
Jacob McBride, NC State
Paul McBride, Wake Forest
Bryson Nimmer, Clemson
Andrew Novak, Wofford
Matt Oshrine, Duke
William Rainey, College of Charleston
Doc Redman, Clemson
Luke Schniederjans, Georgia Tech
Benjamin Shipp, NC State
Alex Smalley, Duke
Jimmy Stanger, Virginia
Cameron Young, Wake Forest
Carson Young, Clemson
Will Zalatoris, Wake Forest
Southeast
Dawson Armstrong, Lipscomb
John Augenstein, Vanderbilt
Sam Burns, LSU
Trace Crowe, Auburn
Cristobal Del Solar, Florida State
Luis Gagne, LSU
Harry Ellis, Florida State
Broc Everett, Augusta
Lee Hodges, Alabama
Sam Hors eld, Florida
Theo Humphrey, Vanderbilt
Keenan Huskey, South Carolina
Phillip Knowles, North Florida
Patrick Martin, Vanderbilt
Cooper Musselman, Kentucky
Gordon Neale, Florida
Peng Pichaikool, Mississippi State
Brandon Pierce, LSU
Davis Riley, Alabama
Joey Savoie, Middle Tennessee
Matthias Schwab, Vanderbilt
Greyson Sigg, Georgia
Scott Stevens, South Carolina
Braden Thornberry, Ole Miss
Alejandro Tosti, Florida
David Wicks, Jacksonville
Ben Wolcott, Ole Miss
Central
Braden Bailey, Baylor
Zach Bauchou, Oklahoma State
Cameron Champ, Texas A&M
Brad Dalke, Oklahoma
Cooper Dossey, Baylor
Frederik Dreier, UTEP
Doug Ghim, Texas
Gavin Hall, Texas
Chase Hanna, Kansas
Grant Hirschman, Oklahoma
Viktor Hovland, Oklahoma State
Garrett May, Baylor
Max McGreevy, Oklahoma
Fredrik Nilehn, Texas Tech
Zachary Olsen, Oklahoma State
Alvaro Ortiz, Arkansas
Matthew Perrine, Baylor
Chandler Phillips, Texas A&M
Ivan Ramirez, Texas Tech
Hannes Ronneblad, Texas Tech
Scottie Schefer, Texas
Hunter Shattuck Baylor
Sam Stevens, Oklahoma State
Kristoffer Ventura, Oklahoma State
Nick Voke, Iowa State
Hayden Wood, Oklahoma State
Midwest
Fernando Barco, Purdue
Nick Carlson, Michigan
Justin Doeden, Minnesota
Austin Eoff, Purdue
Michael Feagles, Illinois
Will Grimmer, Ohio State
Nick Hardy, Illinois
Timmy Hildebrand, Purdue
Ian Holt, Kent State
Chase Johnson, Kent State
Raymond Knoll, Iowa
Edoardo Lipparelli, Illinois
Ryan Lumsden, Northwestern
Dylan Meyer, Illinois
Kyle Mueller, Michigan
Charlie Netzel, Michigan State
Bjarki Petursson, Kent State
Austin Squires, Cincinnati
Gisli Sveinbergsson, Kent State
Matthew Walker, Iowa
Sam Weatherhead, Michigan State
Daniel Wetterich, Ohio State
Josh Whalen, Kent State
Peyton White, Ohio
Dylan Wu, Northwestern
West
Viraat Badhwar, Stanford
Shintaro Ban, UNLV
Aaron Beverly, Sacramento State
Andrej Bevins, New Mexico
Chun An Yu, Arizona State
Wyndham Clark, Oregon
Roy Cootes, Pepperdine
Sean Crocker, Southern California
Jared du Toit, Arizona State
Patrick Fishburn, BYU
Harry Hall, UNLV
Rico Hoey, Southern California
Franklin Huang, Stanford
Maverick McNealy, Stanford
Collin Morikawa, California
John Oda, UNLV
Corey Pereira, Washington
Rhett Rasmussen, BYU
PJ Samiere, San Diego State
Hayden Shieh, Santa Clara
Justin Suh, Southern California
Sahith Theegala, Pepperdine
Tim Widing, San Franciscio
Brandon Wu, Stanford
Norman Xiong, Oregon
Carl Yuan, Washington
Scoliosis is defined as the abnormal, lateral deviation of the spine with a minimal Cobb angle of 10� in the coronal plane. It may be characterized as either non structural or structural scoliosis.
Non-structural scoliosis is identified as a non-progressive curve resulting from a leg length discrepancy, herniated disc or improper bearing which can be corrected by removing the causing factor. Structural scoliosis is identified by not only its vertebral distorted shape, but by a vertebral rotation towards the convex side, where the spinal processes also rotate toward the concave side, additionally, including rib deformity along with the convex sided ribs shifting posterior and superior while the concave sided ribs changing anterior and inferior.
After diagnosis, a person with scoliosis may present a pelvis that is not leveled in the transverse plane with unequal shoulder height, a thoracic or lumbar hump, and an asymmetrical lumbar triangle, loss of lumbar lordosis or loss of balance in the sagittal and coronal planes.
Scoliosis in the Modern World
Scoliosis approximately affects up to 2 to 3 percent of the population and it may be classified as congenital, neuromuscular, degenerative or idiopathic. Furthermore, scoliosis diagnosed after skeletal maturity, between the ages of 20 to 50, known as adult scoliosis, amounts up to 6 to 10 percent of the population. Adult scoliosis is divided into four types: Primary degenerative scoliosis resulting from the asymmetrical erosion of the disc, endplates and/or facet joints; progressive idiopathic scoliosis not previously treated or post-surgical; secondary adult curvature due to a pelvic obliquity; and secondary adult curvature due to metabolic bone disease.
According to research studies, the clinical presentation associated with adult scoliosis requiring immediate medical attention from a healthcare professional includes: back pain which manifests as muscle soreness, muscular exhaustion or mechanical instability; symptoms of radicular pain present during standing or walking; neurological deficits; and curve progression resulting in from axial overload or vertebral bodies with osteoporosis.
Literature has described a variety of treatments for scoliosis predicated on surgical and non-surgical classification, dependent on the severity and the character of the curvature as well as the danger of progression. Surgical intervention is an alternative treatment option for individuals that have completed the growth cycle and whose curve is greater than 50� and or whose curve is above 45� and are still in the growth cycle. Bracing and projecting is utilized for people in the growth interval and whose curve is between 20� and 40�. An individual with a curve of less than 25� and has completed growing might be observed throughout their life for curvature progression of 5� in one year, which can be determined to need surgical intervention.
Many healthcare professionals recommend surgery for scoliosis rather than an alternative, non-surgical treatment for scoliosis. In a study by Brigham and Mooney, a progressive exercise plan focusing on exercises combined with torso turning exercises were utilized to raise the strength in patients with scoliosis measuring 15�to 41�. The results showed a 20% � 23% improvement in the curvature without any type of bracing or casting.
Prevalence of the Schroth Method for Scoliosis
In comparison to America, conservative measures are more vigorously executed worldwide. Along with plans, such as for example SEAS (Scientific Exercise Method Of Scoliosis), FITS (Functional Individual Therapy of Scoliosis), Dobosiewicz method, ASCO (Anti-Scoliosis Shaking-Decompression) procedure, Lyonaise method, and physiologic�, the Schroth method is a scoliosis treatment approach which attempts to conservatively treat the spinal condition by emphasizing patient specific postural analysis and corrections in a multidimensional plane. In line with the method first created by Katharina Schroth, the torso is divided into three and sometimes four vertically stacked anatomical blocks. As an outcome of scoliosis, these blocks deviate in the vertical line and laterally shift and rotate against each other creating areas of convexities and concavities.
Depending on sensorimotor and kinesthetic principles, patients utilize proprioceptive and exteroceptive stimulus (visual, tactile, verbal) to achieve the proper spinal alignment through corrective breathing patterns and postures. This is a big element of the Schroth method for scoliosis. Three dimensional postural corrections and remedial exercises are used to achieve spinal de-rotation, de-flexion and elongation in order to re-gain postural symmetry and muscular equilibrium as well as for the stabilization of the corrected bearing through isotonic and isometric tension and reflex holding of muscles. Simultaneous performance of rotational angular respiration (RAB) helps correct the placement of the ribs by directing air into the thoracic concavities. Through the specific exercises of the Schroth method for scoliosis, patients learn to lift themselves out of passive alignments and endure a position that is corrected throughout their day-to-day activities.
The Schroth Method for Scoliosis
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Lower Back Pain After Auto Injury
After being involved in an automobile accident, neck injuries and aggravated conditions, such as whiplash, are some of the most commonly reported types of injuries, due to the force of the impact. A study discovered, however, that the seat of a vehicle can often lead to injuries as well, causing lower back pain and other symptoms. Lower back pain is also among one of the most common types of automobile accident injuries in the U.S. alone.
Dr. Alex Jimenez takes a look at new concepts on posture and sitting. �Fact: Sitting is the new smoking. �It is highly destructive to the body on many levels. �Here are some good choices that may assist in reducing postural issues as a result of prolonged sitting.
15 Best Active Sitting Chairs For Better Posture, Productivity And | Source: hobbr.com
Best Office Chair For Posture Home Design Ideas | Source: drgulas.com
Before having her son 2-year-old son Isaiah, Carrie Underwood would work out six or seven days a week, but she doesn�t put pressure on�herself to maintain such an intense workout schedule anymore.
�It just happens if and when it happens,� Underwood, 34, told PEOPLE of her new approach to working out at the CALIA by Carrie Underwood Summer Kick-Off event in Malibu on Friday. �I�ve gotten a lot better at doing what I can when I can, but also cutting myself a little slack. You have to!�
That means squeezing in a workout when it�s doable.
�Now it�s like, �Okay, I have 20 minutes. What can I do in 20 minutes?’� she says. �I can go run for a little while, I can go do some tabata rounds, I can do something.�Sometimes I�m like, my workout today is going be running around after my kid. If we�re going to go to the park, why not run there and push him in the stroller?�Then I get a good cardio session to and from, and then he gets to play, so everybody wins.�
If she does have a little more free time, she�ll�do�a full tabata workout.
�I �play cards� a lot ��I assign different exercises to each suit, and I sit�down at breakfast and plan out what each suit�s going to be,� she says.
Her other go-to activities are running and group exercise classes, like Barry�s Bootcamp.
�I love just putting headphones in and going for a run,� says Underwood. �I feel so good when I get home, especially when it�s hot. I�m one of those weirdos that likes to run when it�s super hot outside! Or classes. I find myself competing with other people in the room. I�m like, �Oh she�s good, I want to be like her!� I try to �beat� someone in the class. They have no idea we�re competing!�
The singer says finding time for herself is�possible thanks to family support.
�It helps having a supportive husband and a great unit around me,� she says. �You have to sit down and talk to those around you because I feel like I�m a better mom, a better wife, a better friend when I feel good about myself. It�s endorphins and all that stuff that�s being released, too. No bad things can come out of taking care of yourself!�
And having her own fashion line of workout gear is extra motivation to hit the gym.
�I used to go to the gym in ratty old sweats, but if you already feel good going into your workout, it just kind of gives you that little extra lift,� she says.
Underwood says her drive to work out comes from herself, and not from external pressures to look a certain way.
�It�s all about realizing why you do it,� she says. �I want to be a great mom and I want to be around for him for as long as I possibly can. I want to feel good about myself, I want to set that example for my child and make that a priority, because he�s watching. He�s a busy guy, so I need to keep my energy levels up to be able to play with him and chase him around. So it�s for me and my family and for feeling good about myself. Sometimes you have to remind yourself, but it helps to just say, �It�s not for everybody else, it�s for me.� �
According to the harshness of your whiplash symptoms, your doctor may prescribe drugs and/or spinal shots to manage the pain. To stress this point: they won’t help heal the injury, although the medications will help relieve your pain. Instead, medicines and/or spinal injections lessen your pain so which you can work on curing the soft tissue injuries (through physical therapy, for example).
Again depending on the seriousness of your pain, you could begin with over-the-counter medicines. If those don’t work to relieve your pain, the physician may prescribe stronger drugs. The doctor may imply shots if prescription drugs don’t work. The progression of treatment depends upon your individual symptoms and pain level.
Over-the-Counter Medications for Neck Injuries
Acetaminophen: Tylenol is a good example of an acetaminophen, a form of medicine that has turned out to be a great pain reliever. Most people refer as painkillers to acetaminophen medicines, although your doctor may call this an analgesic. They don’t help reduce inflammation, though. Acetaminophen works by essentially blocking your brain’s awareness of pain, and it is good for those pain flare-ups that will come with DDD.
Over the counter NSAIDs (non-steroidal anti-inflammatory drugs): These will reduce swelling (or inflammation) while relieving your pain. In whiplash, you could have inflammation from your soft tissue injury. If an over the counter NSAID is a choice that’s best for you personally, you have lots to select from. You can use ibuprofen (Advil), aspirin, or Aleve.
By taking an NSAID, you are really building up an anti inflammatory effect in the body, so that it’s essential to choose it for awhile. Which is, NSAIDs won’t be as effective if you take them only when you have pain. Before you notice an important impact on your pain, because they work to limit inflammation and build up in your body, you might have to take NSAIDs for several weeks.
Prescription Drugs for Neck Injuries
If over-the-counter drugs don’t deal with your pain enough, the doctor may prescribe something more powerful. The precise sort of drugs depends upon your symptoms, but the doctor may have you attempt:
Muscle Relaxants: You will need a muscle relaxant, which ought to help stop the spasms if you have muscle spasms brought on by the whiplash injury. Muscle relaxants may also enable you to sleep. Valium is an example of a muscle relaxant.
Opioids (Narcotics): In the most extraordinary cases, and just under careful supervision, you physician might prescribe an opioid, such as for instance codeine or morphine. Vicodin and Percocet are instances of narcotics.
Prescription NSAIDs: NSAIDs that are stronger can be taken by you than the over-the-counter variety, in case your physician believes this is best for your pain. For instance, she or he may recommend a COX-2 Inhibitor (Celebrex is an example). That is a kind of NSAID, but it will not cause gastrointestinal side effects as other prescription NSAIDs can.
Injections and Shots for Whiplash Associated Disorders
Shots for whiplash are most powerful when coupled with exercise plan or a physical therapy which assists you to work on strengthening the neck muscles. The shot should give pain relief to you so that you could turn your focus on curing the specific injury. Several kinds of injections useful for whiplash are:
Epidural Steroid Injection: This is only one of the very common injections. An epidural steroid injection (ESI) targets the epidural space, which will be the space enclosing the membrane that covers the spine and nerve roots. Nerves go through the epidural space and after that branch out to different parts of your own body, for example your arms. If your nerve root has become compressed (pinched) in the epidural space because of a whiplash injury, you could have pain that goes down your neck and perhaps into your arms (a symptom called radiculopathy).
An epidural steroid injection sends steroids�which are very powerful anti-inflammatories� to the nerve root that’s inflamed. This really is a pain management therapy, so that it is far better have a well-trained pain management specialist do the injection. You will likely need 2-3 shots; generally, you should not have more than that because of the potential side effects of the steroids.
Facet Joint Injection: Also called facet blocks, facet joint injections are useful in case pain is being caused by your facet joints. Facet joints in your spine assist you to supply and move stability. You’ll have pain, should they get inflamed, though, because of how your cervical spine affected human body. The joint will be numbed by a facet joint injection and can diminish your pain.
Trigger Point Injection: In extreme cases of whiplash, trigger point shots are a wise decision. (Trigger points are knots of muscle underneath the skin that form when muscles usually do not relax.) The shot has a local painkiller that occasionally features a corticosteroid to decrease the inflammation.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Neck Pain and Auto Injury
After being involved in an automobile accident, the sheer force of the impact can often cause whiplash, a common type of neck injury resulting from the sudden, back-and-forth motion of the head against the body due to a car wreck, or other incident. Because of this, many of the complex structures found within the neck, including the spine, ligaments and muscles, can be stretched beyond their normal range, causing injury and painful symptoms.
Many people suffer from lower back pain that spreads downward to the limbs and feet. This can often be alleviated by doing a deep piriformis stretch � a stretch that releases tight piriformis muscles, and relaxes the sciatic nerve.
Constriction of the piriformis muscle can irritate the sciatic nerve because they lay in close proximity to each other. By irritating the sciatic nerve, the result is pain (either in the lower back or thigh), numbness and tingling along the back of the leg and into the foot.
What Is The Piriformis?
The piriformis muscle is a small muscle located deep in the buttock, behind the gluteus maximus. It connects the spine to the top of the femur and allows incredible flexibility in the hip region (it�s the main muscle that allows for outward movement of the hip, upper leg and foot from the body).
The sciatic nerve passes underneath this muscle on its route to the posterior thigh. However, in some individuals, the sciatic nerve can actually pass right through the muscle, leading to sciatica symptoms caused by a condition known as piriformis syndrome.
Unfortunately, for a lot of individuals, their sciatic nerve passes through the piriformis muscle, leaving them with pain that just won�t go away (as well as poor mobility and balance).
Causes Of Piriformis Syndrome
The exact causes of piriformis syndrome are unknown. The truth is, is that many medical professionals can�t determine a cause, so they cannot really diagnose it. Even with modern imaging techniques, the piriformis is difficult to identify.
Lower back pain caused by an impinged piriformis muscle accounts for 6-8% of those experiencing back pain (1).
Suspected causes of piriformis syndrome include (2):
� Tightening of the muscle, in response to injury or spasm � Swelling of the piriformis muscle, due to injury or spasm � Irritation in the piriformis muscle itself � Irritation of a nearby structure such as the sacroiliac joint or hip � Bleeding in the area of the piriformis muscle
Any one of the above can affect the piriformis muscle, as well as the adjacent sciatic nerve.
Also, a misaligned or inflamed piriformis can cause difficult and pain while sitting and when changing positions (from sitting to standing). I actually stretched too far in a yoga pose once, and irritated my piriformis muscle � this took about 1-2 years to fully heal. I had major pain while sitting, and when changing positions from sitting to standing. I remember it being a huge pain in the butt (pardon the bun), but I just stuck with stretching and trigger point release and eventually it went away.
It is important to note, too, that over-stretching can actually make the condition worse. Light, gentle stretching is best. �No pain, no gain� does NOT apply here. I over-stretched my piriformis and that�s what made it inflamed for 1-2 years (because I was still doing yoga daily, and over-doing it in stretches).
Make sure you warm up your muscles before you stretch, because you can create a different injury. To warm up, simply walk or march in place or climb up and down a flight of stairs slowly for a few minutes before stretching.
Exercising and stretching the piriformis is well worth it � try it now with these 10 stretches:
1. Supine Piriformis Stretch
1. Lie on your back with your legs flat.
2. Pull the affected leg toward the chest, holding the knee with the hand on the same side of the body and grabbing the ankle with the other hand.
3. Pull the knee towards the opposite shoulder�until stretch is felt.
4. Hold for 30 seconds, then slowly return to starting position.
There are many variations of this stretch, but here is a good video to demonstrate:
2. Standing Piriformis Stretch
1. If you have trouble balancing, stand with your back against a wall, and walk your feet forward 24 inches. Position your knees over your ankles, then lower your hips 45 degrees toward the floor.
2. Lift your right foot off the ground and place the outside of your right ankle on your left knee.
3. Lean forward and lower your chest toward your knees while keeping your back straight. 4. Stop when you feel the glute stretch. 5. Hold for 30-60 seconds, then switch legs and do the same.
3. Outer Hip Piriformis Stretch
1. Lie on your back and bend the right knee.
2. Use the left hand to pull the knee over to the left side. Keep your back on the ground, and as you do so, you should feel the stretch in the hip and buttocks.
3. Hold for 20-30 seconds, and repeat on the other side.
�4. Long Adductor (Groin) Stretch
1. Sitting on the floor, stretch your legs straight out, as far apart as you can.
2. Tilt your upper body slightly forward at the hips and place your hands next to each other on the floor.
3. Lean forward and drop your elbows to the floor if you can. You will feel the pelvis stretching.
4. Hold for 10-20 seconds, and release.
5. Short Adductor (Inner Thigh) Stretch
1. For this exercise, sit on the floor and put the soles of your feet together.
2. Use your elbows to apply downward pressure to your knees to increase the stretch.
3. You should feel the stretch on the inner thighs. For a deeper stretch, bend your upper torso forward with a straight back.
4. Hold for 30 seconds, release, and flutter your legs in the same position for 30 seconds.
6. Side Lying Clam Exercise
1. Lay on your side with the hip that needs help on top.
2. Bend your knees and position them forward so that your feet are in line with your spine. 3. Make sure your top hip is directly on top of the other and your back is straight.
4. Keeping your ankles together, raise the top knee away from the bottom one. Do not move your back or tilt your pelvis while doing so, otherwise the movement is not coming from your hip.
5. Slowly return the knee to the starting position. Repeat 15 times.
7. Hip Extension Exercise
1. Position yourself on all fours with your shoulders directly over your hands. Shift your weight a little off the leg to be worked.
2. Keeping the knee bent, raise the knee off the floor so that the sole of the foot moves towards the ceiling.
3. Slowly lower the leg, almost back to the starting position and repeat 15 times.
8. Supine Piriformis Side Stretch
1. Lie on the floor with the legs flat, and raise the affected leg by placing that foot on the floor outside the opposite knee.
2. Pull the knee of the bent leg directly across the midline of the body using the opposite hand or towel until a stretch is felt. Do not force anything and be gentle.
3. Hold the piriformis stretch for 30 seconds, then return to starting position and switch legs.
4. Aim for a total of 3 repetitions.
9. Buttocks Stretch for the Piriformis Muscle
1. Laying with your stomach on the ground, place the affected foot across and underneath the trunk of the body so that the affected knee is on the outside.
2. Extend the non-affected leg straight back behind the body and keep the pelvis straight. 3. Keeping the affected leg in place, move your hips back toward the floor and lean forward on the forearms until a deep stretch it felt.
4. Hold for 30 seconds, and then slowly return to starting position. Aim for a total of 3 stretches.
10. Seated Stretch
1. In seated position, cross your right leg over your left knee.
2. Bend slightly forward, making sure to keep your back straight.
3. Hold for 3-60 seconds and repeat on the other side.
According to Myofascial Pain and Dysfunction: The Trigger Point Manual, written by doctors Janet Travell and David Simons, myofascial trigger points (tiny knot contractions) in overworked gluteus minimus and piriformis muscles in the buttocks are the main cause of sciatica and all the symptoms that come with it.
Picking up a copy of the book, or even following instruction in the video below can help release these knot contractions.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine






 �? Gear Patrol")
 �? Gear Patrol")

")