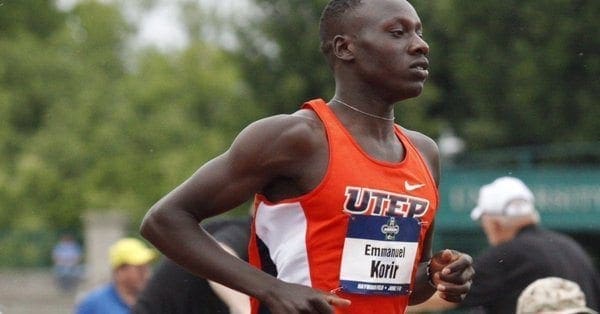
Eugene, Or. � UTEP�s Emmanuel Korir and Michael Saruni make history by being the first freshman duo from the same school to make the 800m final in meet history at the NCAA Championships on Wednesday night.
Running at their first ever NCAA Championships, All-American duo Korir and Saruni did not disappoint. Korir won the first of three heats in the men�s 800m semifinal with the fastest qualifying time of 1:46.38. Saruni�s time of 1:46.63 was enough to win the final heat of the 800m and the third-fastest qualifying time.
Korir and Saruni will run on Friday�s 800m final set to start at 7:45 p.m. MT.
In a valiant effort running the 4x400m relay, Saruni, Korir, Asa Guevara and James Bias clocked 3:18.65. Saruni and Korir had just 90 minutes to recuperate and compete in the mile relay.
Day two of the NCAA Championship will see Tobi Amusan in the 100m hurdles set to start at 6:25 p.m., Lilian Koech in the 800m set for a 7:10 p.m. start and Winny Koech to close out the night in the 10,000m final running at 8:05 p.m.
You can watch the 2017 NCAA Division I Outdoor Track and Field Championships live on the ESPN family of networks. Both the final day of the men�s championship and women�s championship will be aired in prime time on ESPN.
For live results and breaking news be sure to follow @UTEPTrack on Twitter and uteptrack on Instagram.
If anyone knows sneakers, it�s Health�s senior fitness editor Rozalynn Frazier. Whether she�s researching products for our monthly�gear awards�or reviewing�Nike�s new running shoe, Roz’s job requires her to constantly�test the latest sneakers (lucky!). She has so many sneakers and workout clothes, in fact, that she�s�had to devote an entire closet to her fitness gear�no easy feat in a New York City apartment.
With so many cool shoes at her disposable, how does the serious sneakerhead decide which pairs she’ll keep? We asked the six-time marathon runner to give us a tour of her fitness closet and show us her favorite sneakers for every kind of workout, from crushing a class at notoriously-challenging�Tone House (one of her favorite New York City workout studios) to climbing Chamonix-Mont-Blanc in the French Alps. Watch the video above for a full rundown of the sneakers that are “in heavy rotation” for Roz at the moment, then�read on for a few pairs we can’t stop�obsessing over.
This pair boasts “boost technology” in the midsole, which helps you spring forward with every step. “You want to think of it as�a spring, like a trampoline,” says Roz. “It’s very bouncy.” She also loves that the knit upper hugs the arch of the foot for a more customized fit. As an added�bonus, part of the fabric is made from waste that�s been recycled from the ocean. Sold.
Roz is big a fan of the Brooks Ghost model�so much so�that she�s worn the shoe during a handful of her (20 total!)�half marathons. In July, the�newest edition, Ghost 10, will hit stores. “It’s a little more plush,” Roz says of the upcoming model. “A little softer, a little lighter.” Until then, you can shop the Ghost 9.
Nike Air Zoom Strong
To buy: $110;�nike.com
If she�s doing HIIT�(such as Tone House), a boot camp workout, or weight lifting, these cross-trainers are one of Roz�s top picks. “It has the Zoom Air technology, so it�s going to be really quick and responsive,” she says. “I have this in three different colorways.” A thick strap�secures the foot and keeps laces tied during even the most intense sweat sessions.
This durable sneaker was basically made for CrossFit. According to Roz, the sturdy texture won’t wear and tear when you’re doing box jumps or climbing ropes, and the close-fitting heel locks you down as you squat low.�”This is going to be really durable, so you can feel like you can conquer your workout without messing up your shoes, messing up your feet,” she says. “And I just think it’s kind of cool-looking. Look at the colors!”
“I love these because of the gold toe,” says Roz. The metallic detail makes the stylish pair pop. Roz rocks these on the street or at the office, where they add dressy (but still comfortable) edge to any outfit.
Should you have occasional headaches which can be mild in nature, you probably have tension headaches. On the other extreme, in the event that you’ve intense headaches with pounding pain you are incapacitated by that, it is probably a migraine diagnosis.
It’s hard to be sure what kind of headache it’s if your headache is moderate, as well as your headache diagnosis may be more complex. You as well as your doctor may need some time to know in case your headache that is moderate is a symptom of another health condition, a strong tension headache, or a mild migraine.
Symptoms of Head Pain
Headaches are caused by another illness, plus they disappear when that illness goes away. They often accompany colds, the flu, and injuries. By producing a headache, in case you start or stop a medication, your body may complain.
In certain situations, your headache is a sign of a serious illness. In case your headache is accompanied by you should call your doctor, or visit an emergency room or urgent care clinic:
Any combination of nausea, sluggishness, confusion, or a head injury
A fever with pain when you bend your head
blurry vision
severe pain in one eye
Pain and sensitivity around your cheeks and eyes
Diagnosis: Types of Head Pain
You and your doctor can distinguish between a light migraine along with a strong tension headache. Your visit will start using a physical exam that includes capturing or updating your health history.
Together, your doctor and you will explore the symptoms that separate migraines from other headaches with questions such as:
Can you experience a pre-headache period where you are abnormally fatigued or feel strange?
What would you experience when you feel the headache coming on?
What makes your headaches worse?
Would you vomit or get nauseated with your headaches?
How often have you been experiencing headaches?
How long do your headaches typically last?
How do your headaches affect your vision? What do you really see?
Do your headaches make you sweat or give you the chills?
What would you experience or feel throughout your headache, especially in the rest of your body?
If these questions lead you to describe migraine symptoms, your doctor will probably treat you for migraines with self-help strategies and a triptan medication. If the treatments reduce your migraine pain and discomfort, you’re able to be confident of a migraine diagnosis. If your answers don’t fit the migraine headache profile, your doctor may conclude that you suffer from strong tension headaches.
She or he might refer you to a neurologist for additional exams and tests, to be sure your headaches aren’t related to a different health condition.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Cervicogenic Headache and Chiropractic
Neck pain associated with whiplash-associated disorders resulting from an automobile accident are reportedly the most prevalent cause for discomfort along the cervical spine. The sheer force of an impact from a rear-end car crash or other traffic incident can cause injuries or aggravate a previously existing condition. While neck pain is commonly the result of damage to the complex structures of the neck, cervicogenic headaches may also result due to neck issues. Chiropractic care can help carefully restore the alignment of the cervical spine to relieve headaches and neck pain.
Chiropractic care is a non-conservative, alternative treatment option, preferred by many individuals who seek a more natural approach to treat their spinal complications. A chiropractor is a health care professional who focuses on the diagnosis, treatment and prevention of injuries and conditions associated with the musculoskeletal and nervous systems, with a greater emphasis on the spine.
The goal of chiropractic treatment is to reduce painful symptoms and improve the function of the structures of the body as well as educating patients to maintain their overall health and wellness via the proper practice of ergonomics, stretches and exercises.
Chiropractic care is generally categorized as complementary medicine, stimulating the individual’s body to heal itself naturally, without the need of drugs, medications and/or surgery. This practice focuses to improve the relationship between the spine and the nervous system.
A structural misalignment of the spine and/or a bio-mechanical derangement of the vertebral bones can affect the complex network of nerves found throughout the body. In these cases, the goal of chiropractic is to reduce the pressure on the neurological tissue in order to restore the structural integrity of the spine and improve the function of the nervous system, ultimately restoring the well-being of the patient. The primary treatment of a chiropractor is to re-establish the original mobility of the spine, alleviating irritation and inflammation on the structures surrounding the spine.
While a chiropractor, or doctor of chiropractic (DC), is qualified and experienced in the treatment of a variety of spinal conditions, other healthcare professionals within the field of chiropractic have special training in specific areas of the spine, utilizing different forms of treatment than the general chiropractor.
Atlas Orthogonal for the Cervical Spine
Atlas orthogonal is a specialized chiropractic technique which utilizes a precise adjusting instrument to treat complications along the cervical spine, or neck. This type of adjustment has been recognized for its precision and gentleness, in comparison with traditional chiropractic adjustments and manipulations, using only three ounces of pressure per procedure.
As a matter of fact, many patients find it hard to believe how such a light technique can provide them relief, at least until they begin to experience decreased pain and discomfort as well as improved function.
There are many different techniques to adjust the spine. The Atlas Orthogonal procedure is a system which helps balance the anatomical structure of the spine and its surrounding tissues, reducing neurological symptoms caused by spinal misalignment, or subluxation, without using manual manipulation. Atlas Orthogonal incorporates the use of a state of the art floor-based percussion adjusting instrument along with precision X-ray analysis, to properly diagnose, treat and prevent further complications within the cervical spine, particularly the atlas, the topmost vertebra of the spine in which the axis forms the joint that connects the skull and spine.
Most chiropractors, or doctors of chiropractic (DCs) use methods of adjusting where they feel the spine, followed by a manual manipulation or spinal adjustment performed by applying force along the affected structure until a “popping sound” is heard. With the Atlas Orthogonal chiropractic technique, the chiropractor uses specific X-rays to view the cervical spine and determine exactly where and how the vertebrae are misaligned or subluxated. The Atlas Orthogonal Percussion Instrument, utilized for the procedure, is then set with those specific vectors to accomplish the precise and gentle adjustment. The patient feels no force and hears no pops or cracks. Patients adjusted this way stay in adjustment longer than patients who receive treatment with other chiropractors. This means fewer adjustments and more cost-effective health care.
The Atlas Difference Summary
Gentle, effective approach ideal for children, elderly and osteoporotic patients
Modern equipment along with the latest techniques
Specific care that is specialized means fewer adjustments needed
About the Atlas Orthogonal Procedure
In conclusion, chiropractic care is a safe and effective treatment for both neck and back pain, as well as other spinal complications. According to the patient’s needs, some chiropractic adjustment techniques may be most beneficial to them than others. The Atlas Orthogonal chiropractic technique is a gentle and precise form of adjustment which can benefit many patients with cervical spine issues. Despite the variety of treatment and care options available in the chiropractic field, it’s ultimately important for people to treat their spinal complications to achieve overall health and wellness.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Cervicogenic Headache and Chiropractic
Neck pain associated with whiplash-associated disorders resulting from an automobile accident are reportedly the most prevalent cause for discomfort along the cervical spine. The sheer force of an impact from a rear-end car crash or other traffic incident can cause injuries or aggravate a previously existing condition. While neck pain is commonly the result of damage to the complex structures of the neck, cervicogenic headaches may also result due to neck issues. Chiropractic care can help carefully restore the alignment of the cervical spine to relieve headaches and neck pain.
Women who drink diet drinks while pregnant almost double the risk that their child will be overweight or obese at 7 years of age, says a study lead by researchers at the National Institutes of Health. Childhood obesity is known to increase the risk for health problems later in life, such as diabetes, heart disease, stroke, and some cancers.
Researchers found that as the volume of amniotic fluid increases, pregnant women tend to increase their consumption of fluids. To avoid extra calories, many women replace sugar-sweetened soft drinks and juices with beverages containing artificial sweeteners.
Previous studies of adults have found that artificially sweetened beverages encouraged weight gain, and the study authors sought to discover if drinking diet beverages during pregnancy had an effect on the weight of children.
“Our findings suggest that artificially sweetened beverages during pregnancy are not likely to be any better at reducing the risk for later childhood obesity than sugar-sweetened beverages,” said the study’s senior author, Cuilin Zhang, Ph.D.
“Not surprisingly, we also observed that children born to women who drank water instead of sweetened beverages were less likely to be obese by age 7.”
The researchers limited their analysis to data from more than 900 pregnancies that were complicated by gestational diabetes, a type of diabetes that occurs only during pregnancy.
Approximately 9 percent of these women reported consuming at least one artificially sweetened beverage each day. Their children were 60 percent more likely to have a high birth weight, compared to children born to women who never drank sweetened beverages.
At age 7, children born to mothers who drank an artificially sweetened beverage daily were nearly twice as likely to be overweight or obese.
Drinking a daily artificially sweetened beverage appeared to offer no advantages over consuming one sweetened by sugar. At age 7, children born to both groups were equally likely to be overweight or obese.
Women who substituted water for sweetened beverages, however, reduced their children’s obesity risk at age 7 by 17 percent.
Scientists aren’t sure why drinking artificially sweetened beverages compared to drinking water may increase obesity risk. The authors cited an animal study that associated weight gain with changes in the types of bacteria and other microbes in the digestive tract.
Another animal study suggested that artificial sweeteners may increase the ability of the intestines to absorb the blood sugar glucose. Other researchers found evidence in rodents that, by stimulating taste receptors, artificial sweeteners desensitized the animals’ digestive tracts, so that they felt less full after they ate and were more likely to overeat.
According to the Centers for Disease Control and Prevention, the percentage of obese children has more than tripled since the 1970s. Today, 1 in 5 children between the ages of 6 and 19 are obese.
In addition to increased health risks as adults, obese children also have an increased risk of chronic health problems, such as asthma and Type 2 diabetes. They are also more likely to be bullied, and to suffer from depression and lower self-esteem.
It�s not always possible to keep up with your workout routine while traveling. So one hotel chain is making it easier�to cycle, do yoga, or sweat along to a cardio routine video�without ever�leaving your room.
Last month, Hilton Hotels debuted�their Five Feet to Fitness in-room mini gyms, which offer�11 different fitness equipment options�just steps�away from the bed and nightstand. Eight rooms are currently available�three�at Hilton’s�Parc 55 San Francisco and five�at Hilton McLean Tysons Corner in Virginia.
The chain plans to add�more than 100 rooms with mini-gyms around the country by the end of the year, says Ryan Crabbe, senior director of global wellness at Hilton. They’ll be available in Hilton hotels in�Atlanta, Austin, Chicago, Dallas, Las Vegas, New York, and San Diego.
What kind of workout options will guests have?�Features include a�stationary Wattbike, medicine balls, sandbags, a Bosu ball, TRX, a yoga mat, and a foam roller, among other gear and accessories. Each room also comes with a�a touch-screen “fitness kiosk” that shows guests the right way to use�each piece of equipment. The kiosks are also loaded with more than 200 workout�videos covering cardio, cycling, endurance, strength-training, HIIT, yoga, and stretching and recovery.
If guests aren’t up for a cycling session after a long day on a business trip or sight-seeing, Hilton still has them covered�by outfitting each room with other�wellness-related features�such as a�meditation chair, protein drinks in a hydration station, and mini Biofreeze packets for sore muscles.
Hilton�s focus on fitness and wellness was driven by feedback from hotel guests and research into how travelers use hotels. A recent study conducted by Cornell showed that while 46 percent of travelers intend to use the hotel gym, only 22 percent end up doing a workout.
�We know that creating a wellness stage right in the hotel room might just be the solution for those guests who need the convenience of being able to get a quick workout in before breakfast or after a long day of business meetings, or those that prefer to workout in the privacy of their own room,� says Crabbe. �We also know that movement and mindfulness make for a better travel experience.�
No one can pinpoint exactly what causes migraines and headaches or why some people are more prone to experiencing them than others, but what we do know is that there are many factors which could potentially trigger them.
Causes of Cluster Headaches
Abnormalities in the region of the brain, known as the hypothalamus, are the cause of cluster headaches. What makes these headaches different than other types of headache is that they manifest like clockwork. Episodes generally occur in the same time of day and they typically follow the seasons of the year, making these very predictable. These headaches are mostly attributed to changes in the brain rather than changes in the environment or from how people handle stress.
Causes of Tension Headaches
Tension headaches are some of the most common types of headaches and they can affect anyone. �These types of headaches frequently occur when the neck and scalp muscles become tense or tight. Additionally, people who have migraines are more likely to experience moderate or severe tension headaches. The�increased sensitivity to pain resulting from the tension headaches, which might be caused by miscommunication between nerve pathways to the brain. A tension headache is usually triggered by something.
Tension Headache Triggers
A head injury
An illness, such as for example a sinus infection
Drinking alcohol
Eating foods with withdrawal symptoms or too much caffeine from a lack of caffeine
Excessive smoking
Clenching your jaw
Grinding your teeth
Overexertion (caused by intense physical activity, etc.)
Poor posture
Sitting or standing within an uncomfortable position for too long (eg, working at a desk, sewing)
Sleeping with your neck in a abnormal position
Straining your eyes (working at a computer, reading something with very small text, etc.)
Tiredness
Causes of Migraines
Both genetics along with the environment may be the most common cause of migraines. For example, if your mother experiences cases of chronic migraines, you may experience them as well. But in the case you don’t have a family history of migraines, then they may be caused by means of a variety of factors from changes in the weather to too much stress and not handling stress effectively. It’s possible that migraines may also be caused by imbalances in chemicals in the brain. The hormone serotonin helps nerves communicate with each other as well as helps regulate pain in the body. A lack of serotonin may causes a migraine, according to research studies.
Migraine Triggers
Alcohol
Certain foods, for example aged cheese and foods with aspartame (an artificial sweetener)
Changes in your sleeping habits
Dehydration
Depression
Eating foods that have caffeine (eg, coffee, chocolate)
Extreme fatigue
Grinding your teeth
Hormonal changes and menstruation (in women)
Hunger
Poor sleeping habits, lack of sleep, or too much sleep
Skipping meals
Some medications, including oral contraceptives
In spite of the fact that the exact cause of migraines and headaches is unknown, avoiding the triggers mentioned above is certainly one of the best ways to try to prevent headaches and migraines. By avoiding the above mentioned triggers and understanding the causes, you are in a position to help reduce the amount of headaches or migraines you experience in the future.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Cervicogenic Headache and Chiropractic
Neck pain associated with whiplash-associated disorders resulting from an automobile accident are reportedly the most prevalent cause for discomfort along the cervical spine. The sheer force of an impact from a rear-end car crash or other traffic incident can cause injuries or aggravate a previously existing condition. While neck pain is commonly the result of damage to the complex structures of the neck, cervicogenic headaches may also result due to neck issues. Chiropractic care can help carefully restore the alignment of the cervical spine to relieve headaches and neck pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine