Each year in america there are between 6.5 million and 7 million MVA’s affecting many individuals. Of those accidents, about three million involve some kind of bodily injury. About two thirds of these injuries, while not debilitating, are permanent. This means that if you play the odds, you’ll be during the course of your lifetime in 4 or 5 car accidents. They are undoubtedly the major cause although MVA’s are certainly not the sole cause of injuries, such as whiplash.
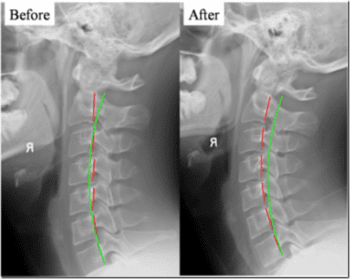
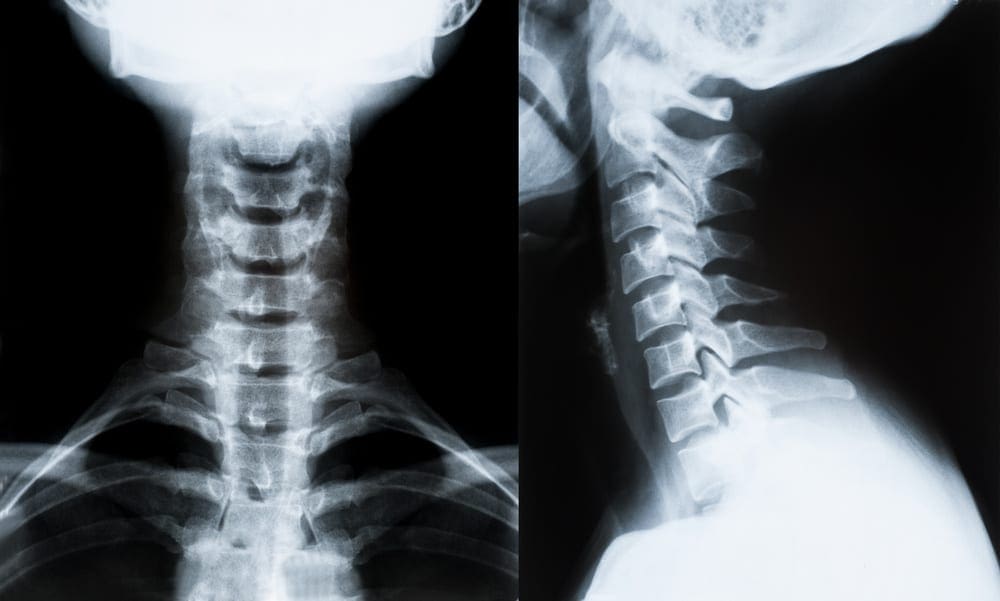
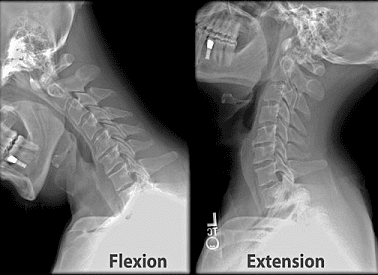
What is the significant whiplash sign we look for as far as imaging is concerned? A simple neutral lateral x-ray of the cervical spine is about as good as anything to demonstrate the extent of damage or injury.
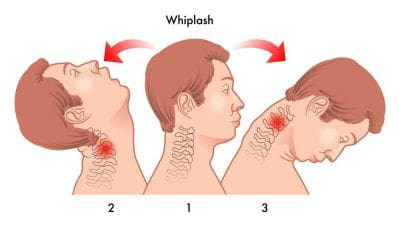
When an individual experiences whiplash, their fascia is often damaged or injured as their head slams backwards. Sooner or later the individual begins to get neck pain, headaches, and a loss of range of motion in their neck. The problem is that a Fascial Adhesion in the SCM may be pulling on their neck. A restriction (Fascial Adhesion) in the SCM is going to pull the head forward.
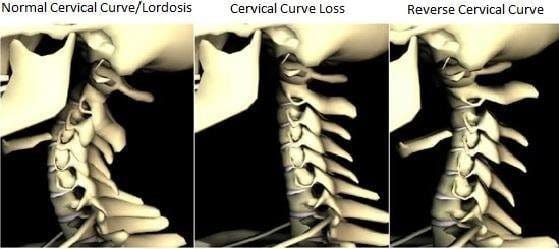
Normal Cervical Curves
Although you should not have spinal curves that run from 1 side of your body to the other (Scoliosis), it’s absolutely crucial to have the proper spinal curves that run from front to back. The normal front-to-back curve in your neck, should be the same as the front-to-back curve in your low back (lordosis) — the opposite of the curve in your mid back (kyphosis). Normal curves allow for normal motion, they act as shock absorbers. Think for a moment about it. A normal curve will dissipate much of the force, spreading it out like a spring when you walk down the sidewalk.
Abnormal Cervical Curves
Abnormal curves of the cervical spine (neck) come in two forms. You have the loss of cervical lordosis. This is the “Military Neck” you see in the first x-ray. Secondly, you get a complete reversal of the lordotic curve (second x-ray). These are some of the steps on the road to Degenerative Arthritis.
For those of you understanding the nature whiplash injury and the NEW MODEL of Repair and Tissue Healing, this picture of the PLATYSMA MUSCLE should help. The Platysma is a thin muscle that covers the entire front portion of the neck. It is likewise covered in Fascia. This is just one more piece of the puzzle so far as explaining the Chronic Pain people struggle with after a whiplash injury — by imaging which is always negative, pain that is not explained. And like SCM Muscles that are injured, it helps to explain the cervical curves. It pulls, as it restricts, and as it pulls, the head will come. Think that Forward Head Posture is no big deal? THINK AGAIN.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.
The cervical spine is C shaped, with its curve facing towards the rear of neck. The upper part of the spine in the neck is called the cervical spine and it’s composed of 7 cervical vertebra. A healthy cervical spine has a lordotic curve and it is anatomically important to bear the head’s weight.
Reduction of cervical lordosis can result in straightening of the cervical spine or in severe cases it may reverse the curve. The condition is also known as kyphosis. Loss of cervical lordosis may lead to stiffness and pain in the neck. It may also lead to referred pain in the hand, vertigo and many other symptoms.
Improper posture and muscular spasm are two important causes for reduction of cervical curvature. The problem is usually detected on X-rays of the cervical spine and it should be treated soon to prevent further deterioration and complications in the future.
Causes of Loss of Cervical Lordosis
Loss of cervical curvature usually occurs in adults. Children suffer from this issue as well although it is rare. Both women and men are equally affected. The condition is associated with long standing spasms of muscles in the neck.
Poor neck posture is often the only cause in young individuals. Working on a computer for long periods or doing desk work for long time without taking break can strain the muscles of the neck. The muscles cause a pull on the cervical vertebra. Prolonged pull will automatically disturb the normal alignment of the cervical spine. Injury to cervical spine may also lead to loss of cervical lordosis. A whiplash injury from automobile accident trauma on the neck can contribute to muscle strain and loss of curvature of the cervical spine.
Osteoporosis is another important factor that might cause abnormality in cervical spine curvature. It is mostly seen among elderly individuals. In osteoporosis the bone density of the vertebrae is lost. The weight of normal wear and tear may put pressure on the spine. Obesity and hereditary skeletal disorders, such as achondroplacia, can also change the curvature of the spine. Other less common causes of loss of cervical lordosis include tumor of cervical spine, systemic disease such as ankylosing spondylitis etc.. Radiotherapy for cancer between can also cause loss of spine curvature.
Loss Of Cervical Lordosis Symptoms
Loss of cervical lordosis involves an ongoing gradual procedure. It is a phenomenon. In its start phase the condition remains silent. This means there are no symptoms. And it’s detected accidentally on X-ray meant for some other purpose. After months or years, the individual may present complaints such as pain and stiffness in the neck.
A normal cervical lordosis has a 30 to 40 degree curve. Once the curve gets lesser than 20 degrees, the patient may complain about neck pain. It may lead to tingling in hands and fingers and may lead to cervical disc degeneration. These symptoms aren’t exactly those from compression of cervical vertebra, but because of pinched nerve because of loss of lordosis.
Loss of cervical lordosis also results in tension in the spinal cord and carotid blood vessels which supply blood to the head. Improper blood flow in the brain can result in dizziness, headaches, confusion, tinnitus etc..
Treatment for Loss of Cervical Lordosis
Loss of cervical lordosis may be detected on physical examination from diagnostic tests such as X-ray and MRI of the cervical spine. These evaluations are important to know the magnitude of loss of lordosis and nerve damage.
Medical treatment is only required when pain and stiffness are present. Muscle relaxants and pain killers will help to reduce spasms and pain of neck muscles. This increase the variety of motion of neck and will alleviate the distress.
Once first acute symptoms are relieved patient should start physiotherapy exercises aimed at strengthening the neck muscles and improvement of posture. A simple neck exercise is to bend the head forward and backward. Second exercise is to turn the neck and head sideways five to six times in a day. Severe case of loss of cervical lordosis may require the individual to wear a neck brace during day time and support pillows while sleeping. Both will help to restore the altered curvature of the spine.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.
The normal cervical lordosis is the natural curve of the neck when viewed from the side, the convexity is on the front and the concavity is on the back.
This curve starts to form as early as 10 months of development and is cemented during adolescence and infancy. Holding a child’s head in extension is quite important for infants as it encourages the normal curvature of the neck. Loss of lordosis can begin in early childhood, however, whiplash from automobile accidents, stress, injuries from falls and sports injuries can cause this issue in adulthood. Unfortunately, many of our “normal” daily tasks may also decrease the cervical lordosis, like viewing low lying computer screens (below eye level), sleeping with two pillows, as well as sitting in a recliner.
Many studies are demonstrating a clear causal connection between loss of lordosis and neck complaints, including neck stiffness and pain, headaches, premature degeneration, disc herniation, and numbness/tingling or weakness in the arms. A study from 1974 showed that a sharp reversal of the curve would lead to degenerative changes in 60 percent of patients. Literally, a reversed curve causes arthritis in the neck. A study from 2005 in the Journal of Manipulative and Physiologic Therapeutics found:
“The odds that a patient with cervical pain had a lordosis of 0 degrees or less was 18 times greater than for a patient having a non-cervical complaint. Patients with cervical pain had less lordosis and this was consistent over all age ranges” The authors of this study went so far as to recommend “Maintenance of a lordosis could be a clinical goal for chiropractic treatment”
Effects of Loss of Cervical Lordosis
But why neck pain? What does loss of the curve do to cause pain? Tingling? Numbness? Headaches? It’s actually very simple. Where they would not bear weight weight bearing stress is placed by A lack of lordosis onto joints at the neck. This causes muscle spasm, stiffness, and inflammation to stabilize the region. Muscles in the upper part of the neck then irritate nerves that travel up and over your head into the scalp. Supporting ligaments in the back of the neck stretch and those in front contract, working to further stabilize the neck in this unnatural posture, as time progresses. Weight is born mainly on the lower segments of the neck (C5-7), which then typically degenerate first. Arthritic spurring progresses in these dysfunctional segments, which could then impinge the exiting nerve roots and cause symptoms in the arms and hands like tingling, numbness, electrical shocks, and fatigue.
Tension After Auto Accident
As the curve becomes kyphotic, other neurologic complaints can attest. The spinal cord is tethered at the top by its attachment to the brain, and in the bottom by the lumbar nerve roots and meningeal attachment to your tailbone. The spinal cord is tractioned and forced against the back of the bodies of the vertebrae in the neck when the ordinary throat curve is reversed. This can cause sensory difficulties anywhere in the body as the pathways for sensation are located in the rear of the cord, and thus are affected by traction. The motor pathways are in the front of the cord and are compressed rather than stretched. Compression of a nerve is never a good thing, particularly when it’s the cord.
What many folks do not know is that most nerve fibers are insulated by a fatty layer called “myelin.” This layer works to allow the signal the nerve creates to travel at faster speeds than it could. Compression of a nerve may result in the death of those cells which maintain this layer; causing the signal the nerve carries to be permanently slower and thus not produce its intended effect. An animal study from 2005 hunted to replicate demyelination (a common diagnostic criteria for Multiple Sclerosis) via cervical kyphosis in Japanese small game fowls. That study’s results were startling. The authors concluded:
“Progressive kyphosis of the cervical spine resulted in demyelination of nerve fibers in the funiculi and neuronal loss in the anterior horn due to chronic compression of the spinal cord. These histologic changes seem to be associated with both continuous mechanical compression and vascular changes in the spinal cord.”
Treatment for Loss of Cervical Lordosis
In short, the reversed curve caused changes in the spinal cord indicative of progressive neurologic conditions. The cervical kyphosis was obtained using methods, but like any symptom of a cause, there are levels of dysfunction. The mechanical methods would hold true, although the methods used in this trial prevent duplication in humans as a result of obvious implications. It’s a fascinating area of research and one I hope continues to grow. To reiterate, the researchers showed that a cervical kyphosis (loss of cervical curve) causes changes in the spinal cord that lead to progressive neurologic degeneration. As Chiropractors, we’ve argued this for generations.
Chiropractic focuses on alignment of the spine so that the nervous system can function optimally. Research is showing a lack of adequate cervical lordosis is a element in a broad variety of conditions, some of which are severe.
If you are experiencing any of these symptoms–headache, stiff neck, neck pain, numbness, tingling, or weakness of your hands, or you’d like to get yourself or your family checked, make sure to seek help from a qualified and experienced healthcare professional to fix the cause.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.
Whiplash has been difficult to study because its pathoanatomy has remained poorly known, however, the facet joints have been recently isolated as a site of pain in many people that are whiplash-injured.
In a typical rear-end collision, the occupant’s pelvis, chest, and head are hastened forward in rapid succession. The massive inertia of the head leads to a horizontal translation (retraction) of the initially stationary head relative to the forward-accelerating torso, and this movement induces compression, shear, and ultimately tension in the cervical spine.
Recent studies have localized the chronic pain of several whiplash patients to the facet joints. Subsequent experiments involving both human subjects and cadaveric cells have demonstrated that harm to the capsular ligaments may play a part in the pathoanatomy of whiplash injury.
Kinematics of Whiplash Injuries
Biomechanical studies of whiplash injury have used human subjects, animals, cadavers, and mathematical models to investigate possible mechanisms of whiplash injury. Researcher ignorance of the tissues responsible for the pain has often limited the insights. Recent studies, however, has identified a candidate tissue for whiplash injury, and it has provided a focus for research into the mechanics of whiplash injury.
The comprehension of injury mechanics begins with an appreciation of how individuals respond to the kinds of perturbations that create whiplash injury. Rear-end collisions, where an occupant’s vehicle is struck from behind and hastened forward, have been associated with an increased risk of whiplash injury and a higher frequency of symptoms compared to other crash directions. As a result, perturbations that simulate a collision have been used by most biomechanical experiments conducted to investigate whiplash injury. Many research groups have studied subjects exposed to whiplash perturbations, and despite differences in subjects, vehicles, seats, and the crashes used with these groups, a stereotyped reaction has been observed in normally seated subjects.
The pelvis is hastened forward, due to a combination of occupant posture and seat compliance, acceleration of the torso lags behind acceleration of the pelvis. This difference in motion between the pelvis and upper torso produces a small rotation of the torso and leads to an initial flexion of the neck, despite the fact that the head is still effectively stationary at this stage in the induced kinematic response. As the torso accelerates forward relative to the head, a horizontal translation develops between the base of the head and the spine, causing the lower vertebrae of the spine to extend. The horizontal shear stiffness of the upright spine is inadequate to overcome the rotational and transitional inertia of the head, and because of this, the upper cervical segments bend. The changing configuration of the vertebrae results in the cervical spine being better able to encourage horizontal forces, and these forces both accelerate the bottom of the skull forward and establish a rearward rotation (expansion) of the head.
In the presence of a properly positioned head restraint, both the head extension angle and the horizontal translation between the torso and head (retraction) are arrested and reversed by the combination of an external force applied to the head from the head restraint and inner forces developed by both the ligamentous cervical spine and the reflex contraction of the cervical muscles.
Larger extension and retraction motions occur, and head motion could be arrested and reversed by inner ligamentous and muscle forces if no head restraint is present or if there exists a gap between the back of the head and the head restraint. The positions of the head and head restraint at effect can therefore have a substantial influence on the magnitude of the head and neck kinematics, and ultimately on the size of the loads applied to the tissues of the cervical spine.
After the interaction with the seat back and head restraint, the head and chest rebound forward. Forward torso motion could be limited by a seatbelt, whereas forward motion of the mind seems to be controlled by sustained activation of the posterior neck muscles.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, are frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. The sheer force of an impact can cause damage or injury to the cervical spine, as well as to the rest of the spine. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. Fortunately, a variety of treatments are available to treat automobile accident injuries.
Healthy, well-nourished women who breastfeed while pregnant don’t seem to increase their risk of delivering prematurely, miscarrying, or having a low-birth-weight baby, the authors of a new research review conclude.
But Gemma Lopez-Fernandez of Corporacio Sanitaria Parc Tauli in Barcelona, Spain, and colleagues write in the journal Women and Birth that more research is needed on the implications of nursing during pregnancy for mothers and children’s health.
While many women will decide to wean after getting pregnant, it is not uncommon for women to continue to nurse, Melissa Kotlen, an international board-certified lactation consultant based in New York, told Reuters Health in a telephone interview.
“If you’re healthy, you’re low risk, you’re not on bedrest, there’s really no problem with continuing to nurse while you’re pregnant,” Kotlen said. “Most of these moms end up tandem nursing once the baby’s born anyway.”
But even pediatricians and obstetricians can fall prey to unproven but common beliefs about nursing during pregnancy, Kotlen added, for example that nipple stimulation will trigger the release of oxytocin and bring on labor prematurely, or that nursing during pregnancy will deplete a mother’s nutritional stores.
To investigate these and other potential risks of breastfeeding in pregnancy, Lopez-Fernandez and her team reviewed 19 studies published between 1990 and 2015 and including a total of about 6,300 women.
They found some evidence that women who nursed during pregnancy gained less weight, had fewer fat reserves and lower levels of hemoglobin – the molecule in red blood cells that carries oxygen. But the reviewers note that most research on the issue was done in the developing world.
The investigators found no support for the idea that breastfeeding women were more likely to deliver prematurely or to miscarry. Evidence on the effects of nursing during pregnancy on fetal and infant growth, as well as on the growth of the nursing child, was mixed.
Mothers who become pregnant while nursing should not be overly concerned about their nutritional status, as long as they are eating and drinking well, Kotlen said. “Your body knows exactly what it needs to take in. If you’re pregnant and you’re nursing, your body is going to know very quickly you need to eat a little bit more and you need to drink a little more.”
Lopez-Fernandez was not available for an interview by press time.
Pregnant women who drink non-diet sodas during pregnancy are more likely to have kids who carry extra body fat by age 7, researchers say.
In the study of more than 1,000 mother-child pairs, each additional serving of sugary soda per day consumed in pregnancy was associated with higher increments of waist size and body mass in kids years later.
“Sugary beverages have been linked to obesity in children and adults,” said study author Sheryl Rifas-Shiman of Harvard Medical School in Boston.
Although past research has tied sodas and some fruit drinks to excess weight gain, obesity, metabolic syndrome and type 2 diabetes, few have looked at beverage intake during pregnancy, she and her colleagues write in Pediatrics.
“Childhood obesity is widespread and hard to treat,” Rifas-Shiman told Reuters Health by email. “So it’s important to identify modifiable factors that occur prenatally and during infancy so prevention can start early.”
The researchers recruited 1,078 women from among patients at eight obstetric offices affiliated with Atrius Harvard Vanguard Medical Associates in eastern Massachusetts.
The study team had in-person meetings with each woman at the end of her first and second trimesters, as well as during the first few months after her baby was born. In addition, kids were assessed in early childhood, around age 3, and in mid-childhood, around age 8. Mothers also completed mailed questionnaires every year for the child’s first six birthdays.
At all visits, researchers collected information about both parents and details of the household. During pregnancy, women answered questionnaires about what they typically ate and drank, including how much regular and sugar-free soda, fruit juice, fruit drinks and water they consumed each day.
At the mid-childhood visit, when kids were between ages 6 and 11 years, the research team measured each child’s height, weight, waist circumference and skinfold thickness. With these measurements, they calculated body fat percentage and body mass index (BMI), a measure of weight relative to height.
When researchers looked at data gathered during pregnancy, they found that more than half of mothers had consumed more than half a serving a day of non-diet soda during pregnancy, and nearly 10 percent had consumed two or more servings a day.
Mothers who drank more sugary drinks during pregnancy tended to be younger, had higher prepregnancy BMI, lower education, lower income, shorter breastfeeding times and were more likely to have smoked during pregnancy.
About one quarter of the children were overweight or obese by mid-childhood, and BMI, waist circumference and skinfold thickness were highest among kids whose mothers drank at least two servings of sugary drinks per day.
Only regular sodas were associated with this difference. Juice, diet soda and water consumed during pregnancy weren’t linked to a higher BMI score in kids. The research team also didn’t see differences based on the mother’s weight, race or ethnicity, the child’s gender or the amount of soda children themselves drank.
“I was surprised that maternal intake seemed to be more important than child intake,” Rifas-Shiman noted.
In the future, she and colleagues plan to study the long-term effects of efforts to reduce sugary beverage intake during pregnancy. They’re now using new methods to analyze when children’s intake of sugary beverages matters the most for their weight and health.
“I was struck that the differences in children’s body composition were seen in relation to intake levels that appear unremarkable, even less than one serving per day,” said Sian Robinson of the University of Southampton in the UK, who wasn’t involved in the study.
“We need to know more about the long-term effects of maternal nutrition on offspring health,” she told Reuters Health by email. “Few intervention studies in pregnancy have longer-term follow-up data to describe the effects on children’s body composition.”
Several of these intervention studies have been completed recently, Robinson added, and that follow-up data will be available soon.
“The links between sugar-sweetened beverages and obesity are well-established,” she said. “But this new data suggests mothers’ consumption is important and has public health relevance.”
After ruling out a herniated disc is not causing your sciatic nerve problems, you should look to the pelvis and many times the culprit is the piriformis muscle.
When the piriformis becomes tight or inflamed, it can put pressure on the sciatic nerve and you can get the sensations going down the leg. �Symptoms such as numbness, tingling, and sharp shooting pain.
A common mistake I�ve seen on YouTube videos and at different gyms and clinics, is people using a tennis ball, lacrosse ball, or foam rollers to apply pressure to the piriformis muscle in order to relax it.
If your sciatica is caused by piriformis syndrome, applying pressure to an area that�s already compressed will only add more pressure to the sciatic nerve and cause more pain.
What you should do instead, is stretch the muscle causing the problem so that it relaxes and takes pressure off the sciatic nerve. In this video you�ll learn an easy stretch you can do on the floor.
You simply lay on your back with both legs bent. Then cross the painful leg over the good one. And pull the affected leg towards the opposite shoulder and hold that stretch for 30 seconds.
Repeat the stretch as needed.
This will help to relieve the sciatic pain associated with piriformis syndrome.
As with any conditions, there is no quick fix. You have to consistently perform sciatica stretches and exercises to achieve the best results.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine