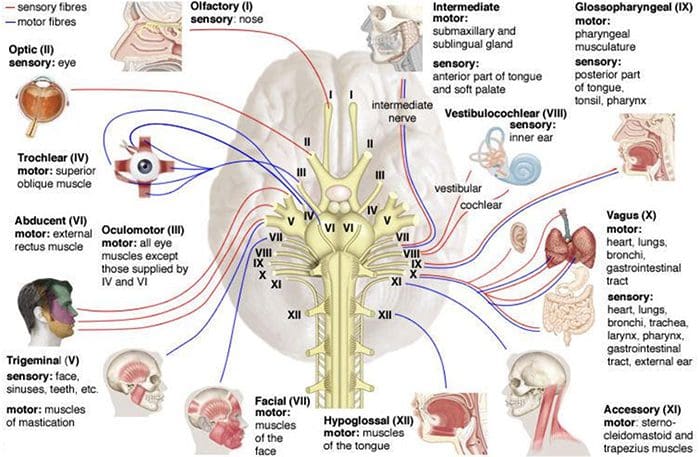
The spinal cord and brain make up the central nervous system while the spinal nerves that branch to the spinal cord and cranial nerves that branch to the brain makes up the peripheral nervous system.
There are thirty-one sets of nerves that extend out of the spinal cord and are connected to it by the nerve root. Each nerve branches out about a half inch from the spinal cord before dividing into smaller branches. The dorsal rami are on the posterior side of the branch while the larger ventral rami are on the anterior side.
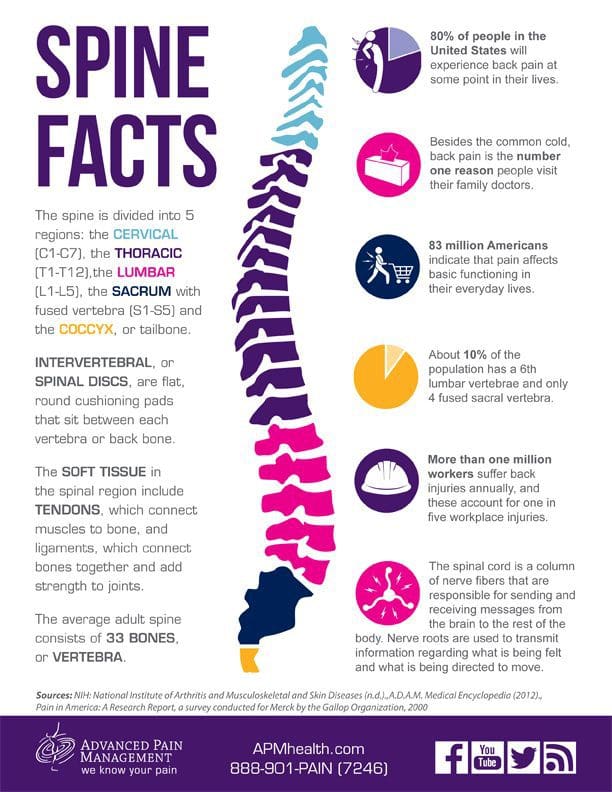
The dorsal rami provide nerve function for the skin of the trunk and posterior muscles. The ventral rami from T1 to T12 provide nerve function to the skin of the trunk as well as the lateral and anterior muscles. The anterior divisions that remain for plexuses, networks that provide nerve function to the body. Each plexus has specific areas on the body for skin sensitivity as well as certain muscles. Their point where they exit the spine determines how they are numbered. The four primary plexuses are:
Cervical plexus, C1 � C4, innervates the diaphragm, shoulder, and neck
Brachial plexus, C5 � T1, innervates the upper limbs
Lumbar plexus, T12/L1 � L4, innervates the thigh
Sacral plexus, L4 � S4, innervates the leg and foot.
These spinal nerves have two sets of fibers: motor and sensory. Motor fibers facilitate movement and provide nerve function to the muscles. Sensory fibers facilitate sensitivities to touch, temperature and other stimuli. They provide nerve function to the skin.
What are Myotomes and Dermatomes?
A group of muscles that are innervated by the motor fibers that stem from a specific nerve root is called a myotome. An area of the skin that is innervated by the sensory fibers that stem from a specific nerve root is called a dermatome. These patterns of myotome and dermatome are almost always identical from person to person. There are occasionally variances, but that is rare.
This consistency allows doctors to treat nerve pain in patients. If a specific area is hurting, they know that it is attributed to a certain myotome or dermatome, whichever the case may be, and its corresponding nerve root. Problems with nerve damage are often the result of stretching the nerve or compressing it.
When the nerves are injured in specific areas like the lumbosacral or brachial plexus, it presents as sensory and motor deficits in the limbs that correspond to them. Myotomes and dermatomes are used to assess the extent of the damage.
How are Myotomes and Dermatomes used to Assess Nerve Damage?
When a doctor tests for nerve root damage in a patient, he or she will often test the myotomes or dermatomes for the nerves assigned to that location. A dermatome is examined for abnormal sensation, such as hypersensitivity or lack of sensitivity.
This is done by using stimulus inducing tools such as a pen, paper clip, pinwheel, fingernails, cotton ball, or pads of the fingers. The patient is instructed to provide feedback regarding their response. Some of the abnormal sensation responses include:
A myotome is tested for nerve damage in the muscles which presents as muscle weakness. This grading scale, which assigns a rating to the degree of muscle weakness, is often used:
5 � Normal � Complete range of motion against gravity with full resistance
4 � Good � Complete range of motion against gravity with some resistance
3 � Fair � Complete range of motion against gravity with no resistance, active ROM
2 � Poor � Complete range of motion with some assistance and gravity eliminated
1 � Trace � Evidence of slight muscular contraction, no joint motion evident
0 � Zero � No evidence of muscle contraction
During a typical chiropractic exam, your chiropractor will assess both dermatomes and myotomes for potential neurological problems. This gives them additional insight on how to treat your condition, whether it’s related to a subluxation of vertebral bodies or other, other disease processes.
Pinched nerves are a common complaint that can cause a wide variety of symptoms. In many cases the condition can be resolved quickly through chiropractic care; sometimes with just one session. However, chiropractic should be treated as an ongoing practice for better health and wellness.
Not only can chiropractic care help you better manage pain and resolve many health problems it can also help prevent injuries and certain conditions from developing. This often means that seeking chiropractic for a pinched nerve is a wise decision and can bring a quick resolution.
In the spine, a herniated disc can put pressure on the nerve root, causing pain and discomfort. In the wrist, it can cause a condition known as carpal tunnel syndrome.
Why is a Pinched Nerve such a Challenge?
The issue with a pinched nerve is finding the source. When a nerve is pinched, the pain and other symptoms may not be at the actual site. Instead, the pain and other sensations can travel to other parts of the body, including down the leg or through the arm. This can make it difficult to treat, but an experienced, knowledgeable chiropractor can assess the situation and treat the condition, bringing relief to the patient.
Symptoms of a Pinched Nerve?
A pinched nerve can manifest with many different symptoms, often depending on its location in the body. They may worsen while the patient is sleeping. Some of the most common symptoms include:
Pain that is aching or sharp
Lower or mid back pain
Neck pain
Shoulder pain
General spinal pain
Pain that radiates down the leg or arm
Numbness or tingling in the legs, arms, fingers, or toes
Burning sensation in the legs, arms, fingers, or toes
Muscle weakness in the legs or back
Headaches
Frequently feeling like a hand or food is �asleep�
When the nerve is not pinched for very long, it typically does not leave the patient with any permanent damage. When the pressure is relieved, normal function returns rather quickly. On the other hand, if the pressure is not relieved, it can cause permanent damage to the nerve, leading to chronic pain.
Causes of a Pinched Nerve?
A pinched nerve can have a number of causes. Wrist or rheumatoid arthritis is a common cause, but others may include:
Injury
Repetitive motion that places stress on parts of the body
Obesity
Sports activities
Certain hobbies that require repetitive motion
Treatments for a Pinched Nerve?
The first line of treatment for a pinched nerve is rest. Medications may be recommended or prescribed, such as NSAIDs and muscle relaxers, but remember every drug has side effects so make sure you talk to your medical doctor before moving forward.
Physical therapy is another common treatment. The patient is taught certain exercises that stretch and strengthen muscles around the pinched nerve so that it relieves pressure. They are also given self-management techniques that they can do at home to get relief. However, if the pinched nerve is do to a misalignment in the spine, it doesn�t matter how many exercises you do; they won�t fix the problem. In severe cases, surgery may be recommended. This is usually a last resort.
Does Chiropractic for a Pinched Nerve Really Work?
Chiropractic care is a very effective treatment for pinched nerve because it addresses the root cause and works toward fixing the problem through spinal manipulation and very specific chiropractic adjustments. By bringing the body into alignment, pressure on the nerves is relieved. This helps relieve the pain but also facilitates healing allowing the patient to return to their normal daily activities and experience less downtime.
El Paso, TX Piriformis Syndrome Chiropractic Treatment
Truck driving can put serious stress on the body. Just spending hours behind the wheel can take its toll no matter what type of vehicle you are driving. When you factor in the shifting, steering, clutching, and constant monitoring that is required in a big truck, you have increased risk of neck, back, arm, hip, and leg pain.
If they drive a type of truck that requires loading, unloading, or tying down a load, the probability increases even more. Many drivers experience pain, difficulty in mobility, and decreased flexibility. This can impact how well they perform their job as well as how much they enjoy their downtime.
How Truck Driving Takes a Toll on the Body
Drivers spend a lot of time doing just that � driving. That is hard on the body in and of itself. With professional drivers, they do it every day for hours on end. Even local drivers who are home every night put in a lot of miles.
Often, drivers must also perform certain functions regarding what they are hauling. Some have to secure their load with straps and tie-downs, or have to handle heavy hoses and equipment to load and unload tankers.
Some drivers have to load and unload (known as �lumping�) their freight themselves. It can involve heavy lifting and repetitive movements. Loaded tanker trucks can be challenging to drive because of the slosh. Most big rigs require a lot of shifting. They may have to shift through 10, 15, or even 18 forward gears.
Team drivers have the added stress of being in a vehicle that is constantly in motion. Even while sleeping in the bunk, they can be subject to the constant vibrations and bouncing as the truck travels over the road. This can lead to impact trauma, often to the shoulder as the driver in the sleeper lays on his or her side. Roads that are poorly maintained can cause impact trauma to both the driver and the person in the bunk.
For all the physical exertion and exposure to a rough environment, though, drivers get very little exercise. They spend a lot of time sitting behind the wheel and making the same movements over and over.
This limited mobility can lead to structural problems like pain in the back, hip, knee, shoulder, arms, and legs. This is compounded by the fact that many prescription medications that are typically prescribed for these issues have side effects that can be dangerous for someone getting behind the wheel.
How Chiropractic can Help Truck Drivers
Chiropractic care provides truck drivers with a non-invasive, drug free way to treat injuries, manage conditions, and relieve pain. Regular chiropractic care can help correct postural habits that can expose the body to injury or move the body out of balance and the spine out of alignment. Often, it can identify emerging issues before they become a problem.
When a driver first visits a chiropractor�s office, he or she will go through a thorough check up and assessment to determine their needs and goals. The chiropractor may recommend certain lifestyle changes and show them some exercise they can do in the truck or while they are on the road as well as ways to minimize the effects of the activities their job requires.
Some of the larger truck stops are now offering drivers access to medical and chiropractic services which allows them to get treatment when they need it. Sometimes a driver is out for several weeks at a time and may not be able to get to their regular chiropractor for an adjustment. However, it is still a good idea to have a regular chiropractor at home and keep regular appointments so you can stay healthy and on the road.
18 Wheeler Accident Chiropractic Treatment El Paso, TX
April Hermosillo has achieved overall health and wellness by following proper nutrition and engaging in exercises/physical activities. As a regular fitness participant, April Hermosillo can experience low back pain which affects even her most basic tasks. April Hermosillo struggled with spine health issues and sciatica before receiving chiropractic care.
Dr. Alex Jimenez is a chiropractor in El Paso, TX who has helped April Hermosillo achieve pain relief so she can return to her everyday fitness routines. April Hermosillo describes how Dr. Jimenez has tremendously helped improve her overall symptoms. April Hermosillo highly recommends Dr. Alex Jimenez as the non-surgical choice for personalized spine and sciatica treatment and rehabilitation.
El Paso Back Clinic
We are blessed to present to you El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
We want you to live a life filled with more energy, positive attitude, better sleep, less pain, proper body weight and educated on how to maintain this way of life.
I assure you, I will only accept the best for you�
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend us.
Frozen shoulder syndrome is one common condition that affects the joint, limiting mobility and causing pain. When something goes wrong, it can dramatically impact a person�s quality of life. The shoulder bears the brunt of a lot of work even in day to day activity. The joint itself is quite complex with a wide range of motion, and that ability can become compromised due to overuse, injury, or age. The goal of the chiropractor is to keep the shoulder moving naturally and ensuring that it is a pain-free. Chiropractic is an effective treatment that helps patients regain range of motion and decrease or eliminate their pain.
What is frozen shoulder?
Frozen shoulder, or adhesive capsulitis, is characterized by pain, stiffness, and limited range of motion of the shoulder joint. It can occur as a result of overuse or after an injury, but can also be caused by diabetes or other diseases or even stroke.
It happens when the tissues that surround the joint become stiff, and scar tissue begins to form in the area. Shoulder movements become painful and difficult. It typically has a gradual onset, then goes away just as slowly. It can take a year or longer for the condition to subside.
What are the symptoms of frozen shoulder?
There are three stages of frozen shoulder and from onset to resolution. It develops gradually and subsides just as slowly with each stage lasting several months.
Stage 1 � Freezing Stage � The shoulder experiences pain during movement and the
Stage 2 � Frozen Stage � The shoulder is stiffer, but the pain may begin to decrease. However, using it becomes increasingly difficult.
Stage 3 � Thawing Stage � The shoulder begins to �loosen� and the range of motion starts to return.
Some patients may experience worsening pain at night which can lead to sleep problems.
What causes frozen shoulder?
Frozen shoulder often develops when the patient ceases regular use of the joint due to injury, pain, or a chronic health condition. There is no single cause of frozen shoulder; it can be caused by any problem involving the shoulder that prevents the patient from maintaining a full range of motion.
It can also happen when the capsule that encases the connective tissue of the shoulder becomes thick and tight. The movement of the shoulder joint is restricted, impacting its ability to move.
People who are 40 and older tend to be more at risk for frozen shoulder, and it occurs more often in women.
Patients who have had prolonged mobility of the shoulder or their shoulder has been completely immobilized are also at risk. These mobility issues may result from conditions including:
Broken Arm
Surgery recovery
Rotator cuff injury
Stroke
Certain diseases can also place patients in the high-risk category for frozen shoulder. Some disorders that may increase that risk includes:
Cardiovascular disease
Diabetes
Parkinson�s disease
Underactive thyroid
Tuberculosis
Overactive thyroid
How can chiropractic help frozen shoulder?
The primary treatment for frozen shoulder involves pain management and preserving the shoulder�s range of motion. Over the counter pain, relievers like NSAIDs and aspirin are often the first line of treatment. Physical therapy may also be used.
In situations where the symptoms persist, more aggressive treatment may be necessary. Doctors may recommend invasive remedies such as surgery and steroid injections.
However, chiropractic can treat the condition from onset through resolution. Even in instances where the symptoms persist, chiropractic can still be very effective. It can be as effective as more aggressive measures without drugs or invasive procedures. Regular chiropractic care can help return range of motion to the shoulder and return the patient�s quality of life.
More and more people are choosing chiropractic care for their pack pain and other issues. In fact, they are leaving their traditional medical practices with their pills and surgeries, and opting for the all-natural, non-invasive practice of chiropractic. So why this seemingly sudden exodus over to chiropractic care? It seems that there are several potential reasons.
The American College of Physicians recommends chiropractic for low back pain.
The American College of Physicians published its updated guidelines in 2017, recommending chiropractic and other non-drug treatments, as a first line treatment for chronic and acute lower back pain. Among the treatments listed was spinal manipulation which was �strongly recommended.� It is very effective when combined with exercises like Pilates, yoga, and tai chi.
Studies show chiropractic to be effective for low back pain.
A study published in the April 2017 issue of the Journal of the American Medical Association cited spinal manipulation therapy to be helpful in treating low back pain. The researchers reviewed and analyzed a number of randomized clinical trials that focused on spinal manipulation as a treatment for low back pain. The results were consistent with each, showing that chiropractic treatment, specifically spinal manipulation, was effective in helping low back pain patients with improving function while minimizing pain during treatment courses of up to six weeks.
95% of people who used chiropractic in the past would do it again.
In the 2016 Gallup-Palmer College of Chiropractic Annual Report, 95% of people who have used chiropractic in the past say that it is an effective treatment. What�s more, 97% of people who used a chiropractor in the previous year said that if they had back or neck pain they would seek chiropractic treatment again. More than half of adults who have never seen a chiropractor said they would seek chiropractic treatment if they developed neck or back pain.
In a consumer survey chiropractic was rated higher than all other treatments for back pain.
A Consumer Reports survey published in July 2011 ranked chiropractic higher than Pilates, yoga, and even medications for relieving back pain, osteoarthritis, and neck pain. Many chiropractic patients like the whole-body approach that includes lifestyle recommendations, dietary advice, and supplements for treating pain, immobility, and range of motion issues. Many of the respondents said they opted for the natural treatments like chiropractic in order to avoid the harmful and undesirable side effects of prescription medication.
People are concerned about the opioid epidemic.
With the Centers for Disease Control (CDC) declaring prescription drug (specifically opioid) abuse an epidemic, people are searching for safer, non-drug options. It is startlingly easy for a person to get addicted to pain medication, even while under a doctor�s care. Because of this, natural treatments are becoming more and more popular to people who want to avoid that potential for addiction or who are at a higher risk for becoming addicted.
With spinal fusion surgery on the rise, patients with back pain are seeking less invasive options.
Spinal fusion surgery has been on a steep rise, increasing by 500% in recent years. Many patients are choosing to seek out natural treatments like chiropractic in order to avoid a surgery this drastic. It also helps that chiropractic looks at the whole person and the patient may get advice on lifestyle habits they need to change, dietary adjustments, and exercises that they can do at home.
Although oral devices, such as splints and bite guards, are the most prevalent treatments for facial pain associated with temporomandibular disorders, or TMD, patients have found that these remedies are frequently less effective than self-care techniques, such as jaw exercises or warm compresses, according to a new research study published by researchers at the New York University (NYU) College of Dentistry in New York City.
The research study, published in the journal Clinical Oral Investigations, demonstrates that self-care techniques should primarily be utilized to help treat muscle-related temporomandibular disorders or TMD.
TMD, occasionally known as TMJ after the temporomandibular joint, is a collection of prevalent painful conditions which develop in the jaw joint and its surrounding muscles. Myofascial temporomandibular disorder, or mTMD, is a muscular condition which affects over 10 percent of women. Individuals with TMD often suffer from other chronic pain conditions. Research studies found that 7 to 18 percent of people with TMD also experience fibromyalgia, a condition characterized by widespread pain.
Treatments for TMD and Fibromyalgia
Dentists and patients utilize an assortment of treatments to help manage facial pain, such as oral devices like splints and bite guards, pain medicines, including nonsteroidal anti-inflammatory drugs, and self-care methods like jaw exercises and hot compresses.
Oral devices are a prevalent first-line treatment for TMD, regardless of research study outcome measures regarding their advantages, stated Vivian Santiago, Ph.D., MPH, research study scientist at the Department of Oral and Maxillofacial Pathology, Radiology, and Medicine at NYU College of Dentistry, and the research study’s leading author.
“While oral splints have been discovered to have some benefits, they have yet to be found to be as successful for patients who have widespread pain when treating mTMD,” she explained.
In this research study, the researchers evaluated what non-medication remedies women with mTMD utilized to handle their pain as well as how successful patients perceived these remedies. The researchers interviewed a total of 125 women including 26 women who had fibromyalgia and mTMD, so as to find out whether treatment differed for patients.
The most frequent treatments reported were oral devices (utilized by 59 percent of participants), physical therapy (utilized by 54 percent of participants), and at-home jaw exercises (utilized by 34 percent of participants). The least frequent treatments reported were acupuncture (utilized by 20 percent), chiropractic care (utilized by 18 percent), trigger point injections (utilized by 14 percent), yoga (utilized by 7 percent), and meditation (utilized by 6 percent). Participants frequently used more than one treatment.
Participants reported the most improvement in their pain from well-known self-care techniques, such as jaw exercises, yoga, meditation, massage, and warm compresses, with over 84 percent reporting that these techniques helped reduce painful symptoms. Only 64 percent of participants who used the oral devices reported that they helped improve their pain. About 11 percent of women who used oral devices stated that these made their pain worse, an area which warrants further research studies.
Oral devices failed to outperform self-care techniques in improving facial pain, according to Karen Raphael, Ph.D., professor at the Department of Oral and Maxillofacial Pathology, Radiology, and Medicine at NYU College of Dentistry, and the research study’s co-author.
“Our outcome measures encourage utilizing self-care techniques as the first line of treatment for mTMD before contemplating more costly interventions,” stated Raphael.
The researchers didn’t find substantial differences between the amount of remedies reported by women with and without fibromyalgia. While the use of alternative treatment options for mTMD was reported among women with fibromyalgia, further research studies are still required. Pain relief tended to be greater through the use of self-care techniques in women with and without fibromyalgia.
“While fibromyalgia is diagnosed by a healthcare professional, such as a rheumatologist, TMD is typically diagnosed and treated by a dentist,” said Santiago. “Our research study demonstrates that dentists must ask patients with facial pain if they also have widespread chronic pain because this might provide more information to help plan their treatment.”
Fibromyalgia is a health issue characterized by widespread chronic pain accompanied by fatigue, sleep, memory and mood problems. Fibromyalgia has been associated with a variety of other health issues, such as TMD and/or TMJ. Individuals with this painful disorder may often struggle to engage in their everyday physical activities. As a qualified and experienced chiropractor, I’ve helped treat numerous patients with fibromyalgia. It’s important for patients to know that they are not alone when it comes to treating their painful symptoms. Chiropractic care is an alternative treatment option which can help treat a variety of health issues, including fibromyalgia.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
The scope of our information is limited to chiropractic, spinal health issues, and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Acute Back Pain
Back pain is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. Your spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly, Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download
* All the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine