FDA recognizes and approves spinal decompression and its ability to eliminate herniated discs.
On the verge of back surgery, a mason discovered the non-surgical solution to work-related chronic back pain.
A new male patient who works in construction came to see me as a last resort to lessen his back pain brought on from damaged/herniated discs.
His primary caregiver recommended back surgery, but that would have put him on disability for months.
Fortunately, before saying yes to the surgery, a co-worker recommended chiropractic care.
Bricklayers/masons have the highest rate of back injuries with non-paid sick leave.
Constant bending over, even with a back brace, takes its toll on the spine, which in this case resulted in two herniated discs.
Pain medications helped in the beginning but with constant use, put him in a constant brain fog state, along with the expense, which took its toll on the family budget.
Disc Injury & Back Surgery
The doctor did not discuss spinal decompression therapy
�A non-surgical back treatment that slowly and gently stretches the spine.
This stretching lessens the pressure on the compressed nerve root (herniated disc) and results in less and even complete alleviation.
The patient came twice a week with myself and the team working on him over the course of a month, however, every case is different so treatments vary depending on the condition.
With each treatment, the two herniated discs were slowly reverted back to their natural position. This is able to be achieved with less pressure between the discs.
Towards the end of treatment, the patient’s pain was gone by about 90%.
With two weeks of rest, the patient was able to return to work.
The best part was that there was no surgery, pain medications, disability, and hospital bills.
Spine treatment alternative
Chiropractic/Decompression therapy is way less expensive than medication and surgery. It is:
Non-surgical
Recovery time is faster
Completely drug-free
People suffering every day with herniated/injured discs should consider the chiropractic decompression option. You do not have to learn to live with chronic back pain.
If you suffer from:
Herniated discs
Bulging discs
Degenerative disc disease
I encourage you to discuss the condition with an experienced chiropractor. There are many proven alternatives to back surgery and pain meds. People need to be aware of these alternatives for chronic back pain. The right-back pain treatment can definitely improve the quality of life.
Herniated Disc El Paso, TX
Sandra Rubio developed two herniated discs and a bulging disc after suffering from an accident at a young age, which caused her intense pain throughout her youth.
When she became a mother, her symptoms became severe.
After visiting doctors without results, Sandra found chiropractor Dr. Alex Jimenez and found relief from her sciatica and migraines.
The herniated disc treatment she received from Dr. Alex Jimenez was non-surgical.
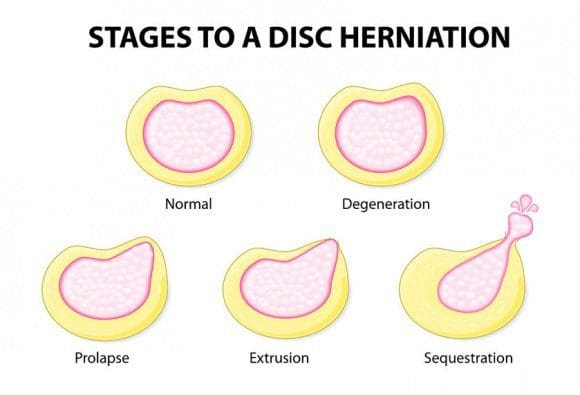
A herniated disc, also known as a slipped disc, is a medical condition in which:
Atear from the outer intervertebral disc allows the soft, central area to bulge out beyond the outer rings.
Disc herniation is usually a result of:
Degeneration (wear/tear)
Trauma (auto accident/sports injury)
Lifting injuries
Straining movement
The tear can release the compounds, which cause inflammation and can cause severe pain even if the nerve root not compressed.
A physical examination is usually the first step in diagnosing a herniated disc. The chiropractor will examine the spine while the patient is standing, and while they’re lying down. Depending on the severity and location of the herniation, they may note a decrease in spine curvature.
Radicular pain will be assessed, when the spine is:
Unmoving
In motion
With pressure applied
Other tests may be administered.
X-rays may also be taken, but an MRI is usually more accurate and shows more detail.
Chiropractic has been very effective in helping patients manage their pain and regain their mobility so they can return to their normal life. Therefore, it should be your first option for treatment before you go down the road with drugs or surgery.
NCBI Resources
It is often referred to as a ruptured disc or slipped disc and occurs when the disc moves or slips out of place. It can also be the result of a disc that has a small tear and is leaking the jelly-like substance that is inside. This can put pressure on the surrounding nerves, causing pain and discomfort.
Increase in sports-related fractures among young and active people
Any type of bone fracture, especially when the spine is involved, comes with the most common and debilitating symptom is severe pain.
Managing pain correctly is vital to the proper healing of a fractured bone.
Unfortunately, the common treatments prescribed to manage fracture pain can cause significant side effects, especially when used beyond the short-term or acute phase of pain.
Bone fractures cannot be always be avoided, but when it comes to osteoporosis, everyone can take steps to help minimize the risk of developing the condition.
How to Prevent Osteoporosis and Bone Fracture
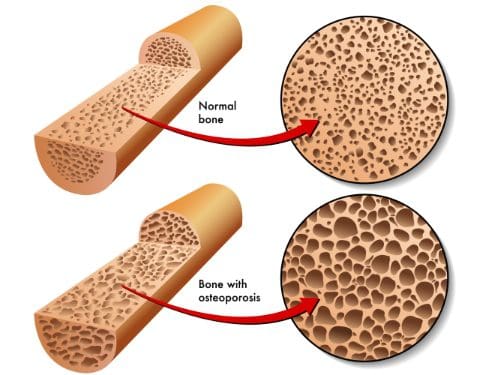
First, understand that osteoporosis is not a normal part of the aging process.
It is an irreversible and degenerative disease that causes bones to become porous over time.
Prevention should begin as early as possible, as this will benefit an individual later in life.
It’s never too late to begin taking steps!
Protecting the bones begins with the most important thing and that is diet.
Most individuals’ diet does not fill the recommended daily values of calcium and Vitamin D.
Both are essential for strong bone health and density.
Diet must be well-balanced with an abundance of:
Green leafy vegetables
Fruit
Dairy sources high in calcium:
Milk
Yogurt
Cheese
However, vitamin D is typically highest in sources of wild-caught fatty fish like salmon and tuna.
Regular exercise is the next important step to help reduce the risk and keep bones strong.
Do exercises that are both:
Weight-bearing (high/low-impact aerobics or walking/jogging)
Muscle-strengthening (weightlifting and exercise bands)
Yoga and Pilates can also help to improve:
Strength
Balance
Flexibility
These are essential in the prevention of bone fractures from falls.
Engage in exercise that you enjoy, this way you will stick with it on a regular basis.
Try for two to three sessions a week if you�re beginning and try to work up to five.
While diet and exercise are extremely important to prevent osteoporosis, there are some areas that should be removed from the lifestyle or limited.
Smoking
Alcohol
These chemicals in bothcigarettes and heavy alcohol consumption are known to be significant contributors to bone loss.
Injury Medical & Chiropractic Clinic offers not only chiropractic treatment, but exercise, and diet programs set up by professional life/health coaches that are customized to each patient. Set up an appointment today, we can help!
Chronic Body Pain Treatment El Paso, TX Chiropractor
Aracely Norte suffered a slip-and-fall accident which tremendously limited her ability to work, affecting her quality of life. Due to the chronic pain she experienced, Aracely had difficulty engaging in her regular, everyday responsibilities. After her lawyer recommended Dr. Alex Jimenez, chiropractor, Aracely found the relief she was looking for.
Chronic pain is a common issue that can occur due to a variety of reasons, including injuries and underlying conditions, however, chiropractic care can help eliminate chronic pain symptoms from the source.
NCBI Resources
As with most conditions, prevention is the most�effective treatment. If you have a family history or fall under any of the risk factors, there are things you can do to minimize the effects or prevent the conditions completely.
Your chiropractor can talk to you about lifestyle changes, exercise, and�diet�as well as supplements that you can take. Chiropractic adjustments can also be effective for many patients with osteopenia and osteoporosis as long as the chosen technique is a low force technique like Activator.
How often do you have a hard time remembering your appointments? Has it become harder for you to learn new things? How often do you feel you have something that must be done? Or even, how often do you feel more susceptible to pain? If it is your very first time experiencing what is commonly referred to as midlife brain fog, which involves a ditsy episode of forgetfulness, it could be frightening, especially knowing that psychological decline is mostly inevitable with age. �
Research studies reveal that the human brain begins to noticeably slow down from the time we hit 40, and around 17 percent of individuals over 65 will wind up with some type of moderate cognitive impairment, like intermittent problems concentrating, locating the proper term, focusing, or even recalling where they have set their car keys, among others. �
Stress is very prevalent in our middle age, also and the reality is that between 6 to 15 percent of people that fulfill the standards for “moderate cognitive impairment” will often go on to develop dementia and Alzheimer’s disease. However, this problem does not need to occur. New research studies indicate that brain fog can ultimately be managed accordingly. �
The brain is based on an intricate variety of compounds to maintain mood in check and also to operate correctly, but should you disturb that equilibrium, you can quickly experience mood changes, not able to sleep, and also struggle to focus properly. Moreover, if you’re eating the incorrect foods, getting inadequate sleep or exercise, overindulging in social networking and TV, stress, and too small downtime, then you will almost surely be destabilizing essential human brain compounds. �
However, you can reverse those trends and take control of your brain health in as little as two weeks if you eliminate the blocks that keep you stuck and give your mind the substances it needs to function efficiently. The purpose of the following article is to show what you can do to prevent and avoid midlife brain fog as well as improve overall health and wellness. �
BOOST BRAIN FATS
A fantastic source of healthy fats in your daily diet may help you feel better. Enjoy lots of olive oil, which is packed with anti-inflammatory chemicals, found in some research studies to help prevent Alzheimer’s disease and depression, as well as fatty fish and select organic meat. Research studies reveal that half a year of nutritional supplements is sufficient to enhance brain function. Also, make sure to pick extra virgin olive oil for salad dressings and olive oil for cooking, virgin olive oil is not safe at high temperatures. Avoid soybean oil because it is packed with unsaturated omega-6 fats which may not be so beneficial. �
AVOID SWEETENERS
Artificial sweeteners may be saving you a couple of calories but it is impossible that these aren’t giving your brain the nutrients it requires for optimum performance. Your mind requires a source of blood glucose to keep it functioning and it is deprived by artificial sweeteners. Worse, sweeteners are demonstrated to interrupt the degree of good bacteria in the intestine, so disrupting the creation of the happy hormone serotonin, a lot of which is fabricated in the gastrointestinal tract. �
TURN OFF YOUR PHONE
Scaling down on social media usage and electronic equipment will help reduce midlife brain fog. All of those lights, dings, and advertisements scrolling across the display give our brains a very small bit of dopamine, as it would for a compulsive gambler sitting in front of a slot machine. Switch off your phone or its own ringer as frequently as possible and do not leave it charging on your bedroom so that it does not disturb your sleeping, even subconsciously. Aim to have just one day of the weekend free. Dump the Kindle through the night and read novels instead. Cut back multitasking, concentrate on doing one thing at a time and provide that all of your attention. This may be a potent antidote to the onslaught of distractions of networking. �
SWITCH OFF THE TV
Engaging in leisure activities helps stimulate the mind. Research studies demonstrate that studying, playing board games and musical instruments, dance, traveling, knitting, and gardening reduce the risk of cognitive decline and guard you against midlife brain fog. But TV does exactly the contrary. Furthermore, research studies reveal that watching TV raises your risk of cognitive impairment up to 20 percent, whereas studying reduces it by 5 percent, according to the same research study. �
SPICE IT ALL UP
Turmeric includes a plant chemical called curcumin, which has significant anti-inflammatory and antioxidant properties and raises levels of a protein named BDNF (brain-derived neurotrophic factor) that is dubbed the “Miracle-Gro” for the mind. Along with making you feel better, turmeric will make you think better by increasing dopamine within the brain. �
Research studies demonstrate that for combating Alzheimer’s disease, low doses of garlic on lengthy periods of time are somewhat more powerful than very substantial doses. So instead of relying upon an occasional Indian takeaway to the turmeric fix, the goal should be to consume 1 food containing garlic using a grind of fresh black pepper (making the garlic more readily absorbed by your system ) daily. Put in a teaspoon of garlic into stews, soups and salad dressings. �
Saffron, yet another frequent ingredient in curry, may also inhibit Alzheimer’s disease, as well as the carnosic acid from the frequent herb rosemary, which can also boost your brain health (the odor alone can even help enhance memory) while rosemary was demonstrated to boost your ability to recall information. Spicing it all up can ultimately help brain fog. �
GO TO BED EARLY
In addition to fostering learning, disposition, and imagination, sleep serves as the brain “self-cleaning” cycle to stop brain fog and eliminate the plaques involving nerve cells which lead to Alzheimer’s disease. A fantastic night’s sleep may improve alertness and fortify the brain’s links, assisting you to combine the memories that you encoded during daily. Poor sleep leads to elevated levels of stress hormones, like cortisol, and enhances dopamine levels, which makes you unhappy, unmotivated and unfocused. Do anything you can to get up to eight hours of sleep each night and keep it continued throughout the week. �
ENJOY COFFEE
Contemplate drinking coffee (without sugar or milk), a healthy food that may help protect against cognitive decline and protect against depression and dementia. Drink espresso macchiato (black coffee with somewhat foamed milk) or espresso over ice with a dash of soy milk. Both without amounts under 50 calories. You can enjoy up to three cups every day. �
Is inflammation the final trip wire for Alzheimer’s disease?� Neuroinflammation is considered to be the final epigenetic trip wire for the genetic predisposition of Alzheimer’s disease . Brain fog can make thinking, understanding, and remembering basic information challenging. A variety of healthy lifestyle habits and modifications can help prevent, as well as avoid, midlife brain fog and improve overall health and wellness. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
�
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
Have you been experiencing noticeable variations in your mental speed? Do you suffer from pain, discomfort, and inflammation? Have you been experiencing fatigue, especially after meals or exposure to chemicals, scents, or pollutants?�Brain fog can cause a variety of symptoms, including memory and concentration as well as vision problems. In the article above, midlife brain fog can be prevented and avoided by following a variety of lifestyle habits and modifications. �
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Cyrex Laboratories is an advanced clinical laboratory that specializes in the functional approach in environmentally induced autoimmunity.� Cyrex works with the leading experts in medical research and provides arrays that address the cross-connections throughout the body systems. In addition to this, Cyrex�strives to deliver the best quality for the patients by always improving and using the most accurate and advanced technology.
Arrays
Cyrex has multiple arrays they use to test patients depending on their symptoms. These arrays range from Alzheimer�s to Joint auto-immune reactivity screenings. Often times, patients who have issues with their joints or headaches and pain, can be traced back to an underlying issue. When a patient comes to a doctor, the practitioner will evaluate and assess the patient based on the symptoms they bring.� From here, the practitioner can go to Cyrex and order the arrays that best suit their patient�s needs. The Cyrex system revolves around immune function and measures the identifiers that can affect multiple tissues in the body, including the brain, heart, pancreas, nervous system, liver, gastrointestinal system, bones, and joints.� The turn around time for these labs is fairly quick and helps highlight the underlying route of the patient�s symptoms.
Cyrex arrays use serum (a blood draw) as their main form of testing. No matter the array the doctor orders, the patient will receive the same kit. The requisition form that is inside the kit is what matters to the phlebotomist and lab as this is where the array ordered will be marked.
The kit is a small box labeled Cyrex Laboratories, Serum Collection Kit. On top of the kit held in place by a rubber band will be a shipping label and bag for the sample to go in once collected. Inside the kit is a smaller styrofoam box that includes a serum separator tube, a serum transport tube, tube labels, a biohazard bag, and collection instructions.
As one can see from the above photo, the different arrays test for different reactions/conditions. A doctor may order one or multiple arrays depending on the patient.
Array 2 is one of the most popular, as leaky gut is a condition that affects most Americans. This test screens for IgG, IgA, and IgM of Lipopolysaccharides and Occludin/Zonulin.
Integrative Testing
Often times, practitioners will use multiple lab companies on one patient. This is not because one is superior to the other, but rather because they specialize in different areas. Even though the doctor may order labs from different companies, it is in the patient�s best interest because it allows the practitioner to view multiple areas to truly understand the underlying issue.
Patients who come in with symptoms like aching joints, headaches, trouble falling asleep, difficulty staying asleep, leaky gut, and brain fog will certainly benefit from using multiple lab companies.
Using Cyrex array 2 and DUTCH + CAR the patient will get extremely accurate information in regards to what is occurring in their body. The Cyrex array test will show the practitioner if the patient has a leaky gut and how severe. While the DUTCH + CAR allows the doctor to determine the cortisol patterns in the individual�s body. Sometimes, these levels are not rising and falling at the right times, causing the patient to be tired or having trouble staying asleep.
The patient�s health should always come first, and when doctors are knowledgable enough to use more than one lab, the patient benefits are outstanding. By using the companies together, the doctor is able to check multiple areas, leaving no guesswork when it comes to a treatment protocol. However, it is important to remember that labs vary on patient needs. Some patients are able to use the same company for all labs and obtain the accurate results they need.
Cyrex tests for many conditions and has multiple arrays. Although many
Cyrex labs are a great tool for practitioners and health coaches to use! By using these arrays, it helps the practitioner not only treat the symptoms, but it allows them the insight they need to treat the problem at the route source. The tools that Cyrex provides go a long way in evaluating the complex disorders the human body may have. By using Cyrex and coupling it with other tests from DUTCH or labrix, the patient is able to get proper treatment and get back to the hobbies they used to love and enjoy. These companies are all fantastic and provide specialities in different areas. By using more than one company, the pateint truly gets the best results and the doctors are able to construct a solid treatment protocol with all of the information obtained.�� Kenna Vaughn, Senior Health Coach�
*All information was obtained from Cyrex.com
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
How often do you have a hard time remembering your appointments? Has it become harder for you to learn new things? How often do you feel you have something that must be done? Or even, how often do you feel more susceptible to pain?�Research studies have demonstrated that brain fog may be associated with Alzheimer’s disease. In the following article, we will discuss how midlife systemic inflammatory markers have ultimately been associated with late-life brain volume. �
Midlife Systemic Inflammatory Markers are Associated with Late-life Brain Volume
Abstract
Objective: To clarify the temporal relationship between systemic inflammation and neurodegeneration, we examined whether a higher level of circulating inflammatory markers during midlife was associated with smaller brain volumes in late-life using a large biracial prospective cohort study.
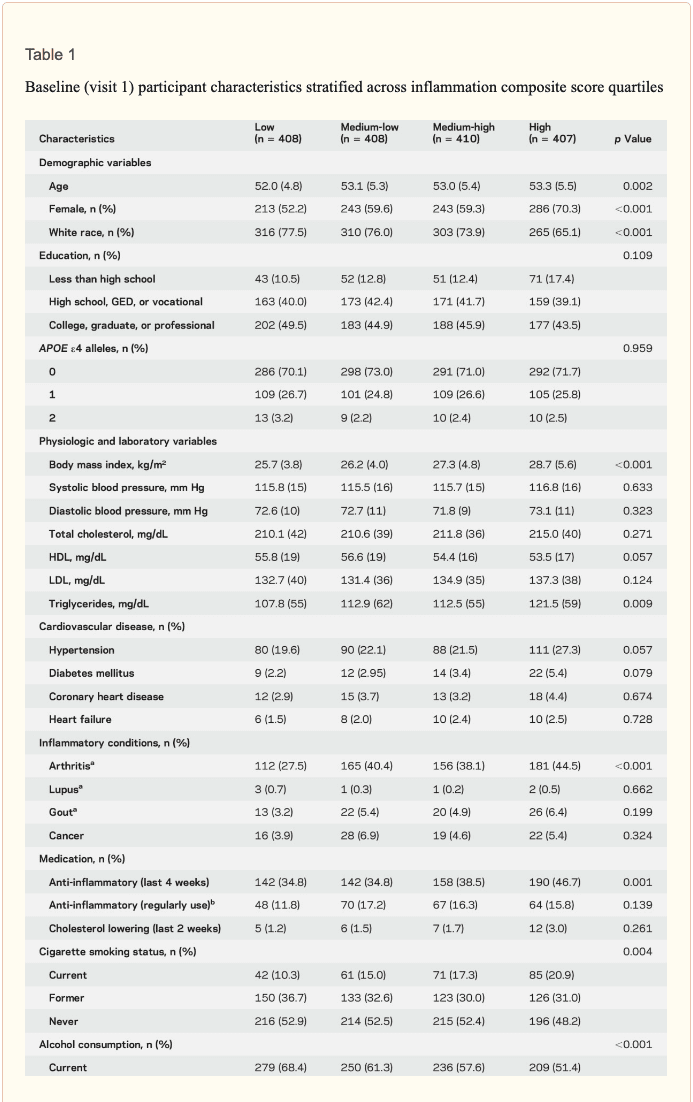
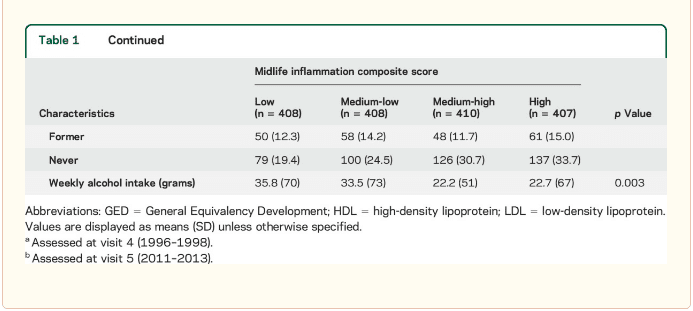
Methods: Plasma levels of systemic inflammatory markers (fibrinogen, albumin, white blood cell count, von Willebrand factor, and Factor VIII) were assessed at baseline in 1,633 participants (mean age 53 [5] years, 60% female, 27% African American) enrolled in the Atherosclerosis Risk in Communities Study. Using all 5 inflammatory markers, an inflammation composite score was created for each participant. We assessed episodic memory and regional brain volumes, using 3T MRI, 24 years later.
Results: Each SD increase in midlife inflammation composite score was associated with 1,788 mm3 greater ventricular (p = 0.013), 110 mm3 smaller hippocampal (p = 0.013), 519 mm3 smaller occipital (p = 0.009), and 532 mm3 smaller Alzheimer disease signature region (p = 0.008) volumes, and reduced episodic memory (p = 0.046) 24 years later. Compared to participants with no elevated (4th quartile) midlife inflammatory markers, participants with elevations in 3 or more markers had, on average, 5% smaller hippocampal and Alzheimer disease signature region volumes. The association between midlife inflammation and late-life brain volume was modified by age and race, whereby younger participants and white participants with higher levels of systemic inflammation during midlife were more likely to show reduced brain volumes subsequently.
Conclusions: Our prospective findings provide evidence for what may be an early contributory role of systemic inflammation in neurodegeneration and cognitive aging.
Introduction
� Although elevated levels of inflammatory markers have been found in the blood,1 CSF,2 and brain parenchyma3 of individuals with cognitive impairment and Alzheimer disease (AD), it remains unclear whether this heightened inflammatory state is driving neurodegenerative changes. If low-grade systemic inflammation does play a causal role in AD and other neurodegenerative diseases, a heightened inflammatory response during midlife would be expected to increase one’s risk for pathologic brain changes much later. Although cross-sectional studies have demonstrated a link between elevated inflammatory markers and reduced brain volume in older adults,4,�7 it remains unclear whether systemic inflammation during midlife, before the onset of significant age- and disease-related neurologic changes, is associated with brain volume loss later in life. � The goal of the current study was to examine how midlife plasma markers of inflammation relate to late-life brain volume among a biracial community sample of older adults. To this end, we examined the relationship between 5 markers of systemic inflammation measured during midlife and MRI measures of regional brain volume 24 years later in the Atherosclerosis Risk in Communities (ARIC) Study cohort. We tested the hypothesis that greater midlife systemic inflammation is associated with smaller brain volumes in regions most susceptible to AD-related atrophy and reduced episodic memory in older adulthood. Based on cross-sectional evidence suggesting that race, sex, and age may modify the association between inflammatory markers and brain volume,5,8,9 the current study also examined the modifying effects of each of these demographic characteristics. �
Methods
� Study population. The ARIC study, an ongoing community-based prospective study, enrolled 15,792 middle-aged adults (45�65 years of age at baseline).10 Participants were selected by probability sampling in 4 US communities: Washington County, Maryland; Forsyth County, North Carolina; northwestern suburbs of Minneapolis, Minnesota; and Jackson, Mississippi. Following the baseline visit in 1987�1989 (visit 1), participants were seen at 3 more visits, approximately 3 years apart until 1996�1998 (visit 4), and at the fifth visit in 2011�2013 (visit 5). � At visit 5, a subset of 1,978 participants was selected to undergo brain MRI scans.11 Participants were selected to undergo a brain MRI based on previous participation in the ARIC Brain MRI Ancillary Study and standard safety exclusion criteria. In addition, all participants with evidence of cognitive impairment at visit 5 and an age-stratified random sample of participants without evidence of cognitive impairment were recruited. The participation rate among eligible individuals selected to undergo brain MRI was approximately 81%. A detailed description of the MRI sampling strategy is provided in the e-Methods at Neurology.org. We excluded participants with poor imaging quality (n = 6), neurologic disease (i.e., stroke, multiple sclerosis) (n = 80), missing inflammatory biomarker data (n = 38), missing covariates (n = 215), and race other than white or African American (n = 6). Participants who met criteria for dementia (5%, n = 83) were excluded from the primary analyses. � Standard protocol approvals, registrations, and patient consents. The ARIC study protocol has been approved by the institutional review boards at each participating center. All participants gave written informed consent at each study visit. � Inflammatory markers. Plasma levels of 4 acute-phase reactants�fibrinogen, albumin, von Willebrand factor (VWF), and Factor VIII (FVIII)�and white blood cell (WBC) count were used to measure systemic inflammation.12 Using standard protocols, study technicians drew fasting blood, centrifuged samples, and froze plasma blood samples at ?70�C until the samples were analyzed.13 Fibrinogen (mg/dL), albumin (g/dL), VWF (% of standard), and FVIII activity (% of standard) measured at visit 1 were analyzed in an ARIC research laboratory in accordance with a standardized protocol.13,14 WBC count was determined from whole anticoagulated blood using an automated particle Coulter Counter within 24 hours of venipuncture. Repeated testing revealed interassay coefficients of variation below 8% for fibrinogen, albumin, FVIII, and WBC, and 17%�19% for VWF.15,16 � Brain MRI. MRI scans were conducted using a 3T MRI scanner.11 Magnetization-prepared rapid gradient echo (MPRAGE), axial T2* gradient recalled echo, axial T2 fluid-attenuated inversion recovery, and axial diffusion tensor imaging sequences were obtained. Freesurfer (surfer.nmr.mgh.harvard.edu) was used to measure brain volume from MPRAGE sequences.17 Total brain and ventricular volume, lobar volume (frontal, temporal, parietal, occipital), AD signature region volume (i.e., the combined volume of the parahippocampal, entorhinal, inferior parietal lobules, hippocampus, and precuneus),18 hippocampal volume, and total intracranial volume were evaluated for the current study. � Episodic memory. Episodic memory was assessed at visit 5, concurrent with the brain MRI, using the delayed word recall test (DWR). DWR is a test that requires participants to learn and recall a list of 10 words following a delay period.19 Participants were scored based on the total number of words correctly recalled. � Covariates. Race, sex, years of education attained (less than high school, high school/General Equivalency Development/vocational school, or any college), cigarette smoking status (current/former/never), average weekly alcohol consumption (grams), and previous cancer diagnosis were self-reported. A random zero sphygmomanometer was used to calculate sitting diastolic and systolic blood pressure. Second and third blood pressure measurements were averaged for the current analyses. Hypertension was defined as systolic blood pressure >140 mm Hg, diastolic blood pressure >90 mm Hg or use of hypertensive medication. Body mass index was calculated using recorded height and weight (kg/m2). Coronary heart disease was defined as self-reported coronary bypass, balloon angioplasty, angioplasty of one or more coronary artery, or myocardial infarction. Medications used in the previous 2 weeks were recorded. The presence of chronic inflammatory conditions (e.g., arthritis, lupus, gout) was assessed by patient self-report of physician diagnosis at visit 4. History of regular anti-inflammatory medication use (e.g., nonsteroidal anti-inflammatory drug, arthritis medication) was assessed at visit 5. All other variables were assessed at visit 1. Dementia diagnosis was adjudicated at visit 5 by an expert committee using cognitive, imaging, and functional data.20 � Total cholesterol and triglycerides were measured using enzymatic methods,21,22 and low-density lipoprotein using the Friedewald equation.23 Serum glucose was measured using the hexokinase method. Diabetes was defined as a fasting glucose ?126 mg/dL or a nonfasting glucose ?200 mg/dL, current use of diabetes medication or insulin, or participant report of physician-diagnosed diabetes. APOE genotype (0, 1, or 2 ?4 alleles) was assessed using the TaqMan assay (Applied Biosystems, Foster City, CA). � Statistical analysis. We examined systemic inflammation as both a continuous and categorical exposure measure. A continuous inflammation composite Z score was created using the 5 inflammatory markers. WBC count was log-transformed to correct for skewness. Each inflammatory biomarker was converted to a standardized Z score such that the group mean was zero with an SD of 1. The mean of the 5 Z scores was calculated to generate an inflammation composite Z score. Because albumin decreases in response to inflammation, albumin values were multiplied by ?1 before being included in the composite Z score. With few exceptions, the intercorrelations between inflammatory markers were within an optimal range, between 0.2 and 0.4; composite score item�test correlations, principal component factor loadings, and Cronbach ? (0.61) were satisfactory for our purposes (table e-1). For each participant, we also created a categorical measure of systemic inflammation by computing the number of inflammatory marker Z scores in the highest quartile (?75%tile) and trichotomizing this number (0, 1�2, or 3�5). � Participant characteristics were compared using an analysis of variance or ?2 tests. Multivariable linear regression was used to assess the association between continuous and categorical inflammation variables and measures of brain volume and episodic memory. Brain volume analyses were adjusted for total intracranial volume, and all analyses included the covariates described in the previous section. Interaction terms or stratification were used to evaluate the modifying effects of age, race, and sex. � Sensitivity analyses were performed excluding participants who reported regular anti-inflammatory medication use during follow-up and including participants who met criteria for dementia. For all analyses, sampling weights were incorporated to account for the ARIC brain MRI sampling strategy. Thus, all results represent estimates for the entire ARIC visit 5 study population. Because the associations between inflammation markers and specific regions of interest (ROIs) are correlated, we did not adjust for multiple comparisons. A 2-sided p-value <0.05 designated statistical significance. All analyses were conducted using Stata Version 14 (StataCorp, College Station, TX). �
Results
� Study population characteristics. A total of 1,633 participants (baseline mean age 52.8 [5.3] years, 27% African American, 60% women, 46% college or professional degree) were included in the study sample. The time between baseline assessment and follow-up MRI scan was 24 (1) years; the average age at follow-up was 76.5 (5.4) years. As shown in table 1, a higher inflammation composite score at baseline was associated with older age, female sex, African American race, and increased levels of a number of cardiovascular risk factors. � Inflammatory markers and brain volume. Each SD increase in inflammation composite score at baseline was associated with a 532 mm3 smaller AD signature region volume (95% confidence interval [CI] ?922 to ?141), a 519 mm3 smaller occipital lobe volume (CI ?906 to ?132), a 110 mm3 smaller hippocampal volume (CI ?196 to ?24), and a 1,788 mm3 larger ventricular volume (CI 371 to 3,205) at follow-up (table 2). We found the estimated effect of a 1 SD increase in inflammation composite score during midlife on occipital lobe, ventricular, and hippocampal volume to be similar to the effect associated with possession of a single APOE ?4 allele in our multivariable regression analyses. No association was found for the total brain, frontal lobe, temporal lobe, or parietal lobe volume (ps > 0.071). Our findings did not change meaningfully after excluding participants who regularly used anti-inflammatory medication during the follow-up period (table e-2) and after including participants who met the criteria for dementia at visit 5 (table e-3). For descriptive purposes, associations between individual inflammatory markers and AD signature region volume are provided in a table e-4. � An assessment of linear trend revealed that compared to individuals with 0 elevated (?75th %tile) inflammatory biomarkers at baseline (reference), those with 1�2 and 3�5 elevated biomarkers had lower AD signature region (p trend = 0.001), occipital lobe (p trend = 0.007), and hippocampal volume (p trend = 0.041) 24 years later (figure 1). Compared to the reference group, participants with 3 or more elevated markers demonstrated 5.3% smaller AD signature region volumes, 5.7% smaller occipital lobe volumes, and 4.6% smaller hippocampal volumes, on average. However, this pattern was not statistically supported for the total brain, ventricular, frontal lobe, temporal lobe, and parietal lobe volume (p trends >0.072). The modifying effects of age, race, and sex. A significant age-by-inflammation composite score interaction was found for the AD signature region, occipital lobe, and hippocampal volume (table 2). Because a reversal of association was observed at age 60 (figures 2, e-1, and e-2), we stratified the sample into young-midlife and old-midlife subgroups (<60/? 60). As displayed in table 2, the associations between higher midlife inflammation composite score and lower AD signature region, occipital lobe, and hippocampal volume at follow-up were significantly stronger among participants who were 60 or younger at baseline compared to those who were older than 60. A marginal race-by-inflammation composite score interaction was found for occipital lobe volume, whereby a higher midlife inflammation composite score was associated with lower occipital lobe volume among white, but not African American, participants (table 3). No interactions with sex were found (table e-5). � Inflammatory markers and episodic memory. Late-life episodic memory, which was associated with hippocampal and AD signature region volume after controlling for age (partial rs > 0.21, ps < 0.001), was reduced among participants with higher levels of the inflammation composite score. Each SD increase in inflammation composite score was associated with a ?0.08 SD performance decrement on the DWR after adjusting for covariates (CI ?0.15 to 0.00; p = 0.046). Similarly, a higher number of elevated inflammatory biomarkers at baseline was associated with reduced DWR performance (p trend = 0.009; figure 1). �
Discussion
� Using a large community sample, we demonstrated that a higher level of systemic inflammatory markers measured during midlife is independently associated with lower regional brain volume and reduced episodic memory 24 years later among older adults without dementia. Similarly, participants who had elevations in a larger number of 5 inflammatory markers during midlife were found to have lower regional brain volumes and reduced episodic memory in late-life in a dose-response manner. For several brain regions, including the hippocampus, the effect of a 1 SD increase in midlife inflammation composite score was comparable to that of possessing a single APOE ?4 allele during late life. Whereas age and race were found to modestly modify the relationship between midlife inflammation and late-life regional brain volume, the previously reported modifying effect of sex was supported. � Although cross-sectional evidence from the Framingham5 study and several other population-based8,9 studies suggests an association between brain volume and inflammation in older adults, the temporal relationship between inflammation and brain volume loss is still not well-understood. As a result, whether heightened systemic inflammation constitutes a potential cause or consequence of neurodegeneration and brain atrophy remains unclear. Because the pathophysiologic processes driving neurodegeneration and brain volume loss begin decades before the onset of frank cognitive decline,24 it is essential to determine how biological processes that take place during middle adulthood relate to neurologic outcomes later in life. By demonstrating that an elevation in plasma inflammatory markers during midlife is independently associated with smaller regional brain volumes, larger ventricular volume, and reduced episodic memory in late life, the current findings provide support for a potential causal, rather than associative, role of systemic inflammation in late-life neurodegeneration (i.e., atrophy) and resulting cognitive decline. The current findings align closely with those from the neurocardiovascular literature, which have found associations between midlife blood pressure,25 cholesterol,26 and diabetes27 and adverse neurologic and cognitive outcomes in older adulthood. The contributing role of systemic inflammation to subsequent neurodegenerative processes has been demonstrated previously by animal studies,28 but had not yet been supported by a large prospective MRI study. � The current results suggest that several demographic factors modify the relationship between midlife inflammation and late-life brain volume. Younger individuals with elevated levels of inflammation (particularly participants in their 40s) were more likely to display lower brain volumes decades later, supporting the idea that elevated systemic inflammation earlier in life may make individuals especially vulnerable to neurodegenerative brain changes as they age. Although we expected stronger effects would emerge within the African American group, given the greater burden of systemic disease29 and dementia,30 the associations between inflammation and brain volume were generally weaker among African Americans. A previous study that examined the moderating effects of race found similar results in a cross-sectional analysis of older adults without dementia.8 � Circulating levels of acute-phase reactants, such as those used in the current study, change in parallel with an inflammatory response as a result of signaling from inflammatory cytokines such as interleukin-6 and tumor necrosis factor-?.12 Cytokines in the periphery have the potential to induce a pro-inflammatory neurotoxic state within the CNS through multiple routes, including activation of endothelial cells of the blood-brain barrier,31 activation of macrophage in circumventricular organs,32 and signaling of the afferent vagus nerve.33 In addition to providing support for a pathogenic role of systemic inflammation in neurodegenerative disease, the present findings indicate that elevations in commonly assayed inflammatory proteins may serve as markers of risk for future neurodegenerative changes and cognitive decline. Although we did not examine all brain regions in our analysis, our assessment of 7 representative ROIs suggests that brain regions vulnerable to atrophy, amyloid deposition, and metabolic abnormalities in the earliest phases of AD may be more vulnerable to volume loss associated with heightened midlife inflammation. This pattern of neuroanatomic specificity has been supported by previous cross-sectional studies of older adults without dementia.4,7,�9,34 � In the context of the current findings, several alternative explanations should be considered. First, it remains possible that elevated systemic inflammation may simply serve as a marker of another pathologic process linked to neurodegeneration (e.g., oxidative stress). Second, it is possible that the biological processes causing brain atrophy to trigger a protective neuroimmune response, which increases peripheral inflammation. Third, the associations found here may be an effect of residual or unmeasured confounding. Despite these caveats, the contributory role of systemic inflammation has been supported by a sizable body of literature implicating peripheral inflammatory signaling in neurodegenerative processes such as neural apoptosis,35 ?-amyloid formation,36 and neuronal tau phosphorylation.37 � Strengths of the current study include the prospective study design, length of follow-up, detailed assessment of potentially confounding variables, large sample size, and the inclusion of a large African American sample. However, the current findings should be interpreted within the context of several limitations. Although the acute-phase reactants used in the present study represent components of the innate immune system, several of these proteins are implicated in another closely related physiologic process, such as hemostasis, which may also influence brain volume. Evaluating inflammatory biomarkers that have greater biological specificity in future prospective studies will allow for stronger inferences about the contributing role of systemic inflammation. Interpretation of the current findings is also limited by the measurement of inflammatory markers at a single time point, as it is unclear whether a single measurement can adequately capture inflammation chronicity. The relatively high interassay variability of VWF also increases the likelihood of exposure misclassification; however, this possibility is mitigated by the use of the inflammation composite score. We found that participants who dropped out and participants who died before visit 5 had significantly higher levels of midlife inflammation, were older, had greater levels of medical comorbidity at baseline, and were more likely to be African American38 (table e-6). As a result, selective attrition may have biased results in the direction of the null hypothesis, particularly for African American and older participants. Finally, our interpretation of the contributory role of inflammation in neurodegeneration rests on the assumption that brain volume loss occurred after inflammatory markers were assessed. Although evidence suggests that this is likely the case (brain volume loss accelerates after age 60 years39), this cannot be confirmed without the assessment of change over time. � Despite these limitations, the current study provides insights into the connection between midlife systemic inflammation and late-life brain volume loss. These findings provide support for inflammation’s early pathogenic role in the development of neurodegenerative brain changes associated with late-life cognitive decline, AD, and other forms of dementia. �
Is inflammation the final trip wire for Alzheimer’s disease?� Research studies have demonstrated that neuroinflammation is considered to be the main epigenetic trip wire for the genetic predisposition of Alzheimer’s disease or AD. Moreover, patients with inflammation can also develop a variety of symptoms, including brain fog which can make thinking, understanding, and remembering basic information challenging. Neuroinflammation can cause brain fog and other other well-known health issues, including Alzheimer’s disease and other neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
� In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. � Have you been experiencing noticeable variations in your mental speed? Do you suffer from pain, discomfort, and inflammation? Have you been experiencing fatigue, especially after meals or exposure to chemicals, scents, or pollutants?�Brain fog can cause a variety of symptoms, including memory and concentration as well as vision problems. According to the research study above, midlife inflammation and brain fog may be associated with Alzheimer’s disease. � The following article has been referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
� Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
�
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
� For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Is your attention span decreasing? How often do you walk into rooms and forget why? How often do you feel you are not getting enough sleep or rest? If you answered yes to any of the previous questions, you may be experiencing brain fog. Brain fog is a symptom rather than a single condition and it can actually be caused by a very common factor: too much screen time. �
Many people today spend a significant amount of time staring at a screen than ever before. According to the American Optometric Association (AOA), an average office worker in the United States spends a minimum of seven hours a day sitting in front of a computer screen. While other recent research studies have shown that an average American adult spends as much as 11 hours a day looking at some type of screen of some kind, including mobile devices like smartphones. �
In light of this “digital revolution”, however, more and more healthy people in their 20’s, 30’s, and even in their 40’s have started experiencing brain fog, short-term memory loss, and insomnia as well as vision problems, headaches, and migraines. Although there isn’t an abundance of evidence, several research studies have begun to demonstrate the effects of too much screen time on our overall health and wellness. We will discuss why screen time causes brain fog, among other health issues. �
How Screen Time Changes the Brain
Sitting in front of a computer screen or looking at any other type of screen for extended periods of time can ultimately cause brain fog and vision problems, among other health issues because it changes the brain, both behaviorally and structurally. A research study of students in 10 countries showed that many of them feel acute distress if they go without their phones for 24 hours. Also, most people check their phones a minimum of 150 times a day, sending about 100 or more text messages. �
This excessive use of smartphones has been associated with stress, anxiety, and even depression. Neuroscientists have referred to this health issue as “digital dementia,” which ultimately affects important right-brain functions, such as short-term memory, attention, and concentration, in ways that may or may not be reversible if they are not treated properly. �
People who are perceived as having an online game addiction show significant gray matter atrophy in a variety of regions in the brain, including the right orbitofrontal cortex, the bilateral insula, and the right supplementary motor area, when they were evaluated using brain MRI research studies. The regions where volume loss was shown are ultimately in charge of essential cognitive functions, such as planning, prioritizing, organizing, impulse control, and reward pathways. These are also involved in our development of empathy and compassion as well as the translation of physical signals into emotion. �
Several research studies have also shown that too much screen time can also cause long-term vision problems and other eye health issues. According to the American Optometric Association, computer vision syndrome or CVS, also known as digital eye strain, is a complex vision problem associated with tasks and activities that stress the near vision and those that are experienced in relation, or during, the use of the computer, tablet, e-reader, and smartphone. The symptoms include eye strain and ache, dryness, irritation, redness, double or blurred vision, burning, and even neck and shoulder pain. �
Moreover, in 2014, a Harvard Medical School group investigated the biological effects of reading an e-book on a light-emitting device with reading a printed book in the hours before bedtime. The researchers ultimately reported that people who read on the e-book took longer to fall asleep, had less evening sleepiness, decreased melatonin secretion, later timing of their circadian rhythm, and lower next-morning alertness than when reading a printed book. Much of this likely has to do with the fact that e-books and other digital screens emit blue light, which has been shown to interfere with the production of melatonin or the “sleep hormone” which also helps regulate other hormones as well as our circadian rhythms. �
While research studies demonstrating the connection between mood and digital device addiction is still emerging, some recent research studies are starting to associate prolific social media use with the increased risk of anxiety and depression. Many patients report feeling stress, anxiety, and depression caused by spending too much time scrolling through social media, such as Instagram, Facebook, and Twitter feeds. Some even report that “social media detoxes,” where they delete these apps from their smartphones for a few days or weeks, tremendously improved their overall health and wellness. �
How to Prevent Brain Fog from Screen Time
If you find yourself experiencing symptoms such as brain fog, short-term memory loss, vision problems, insomnia, anxiety, depression, headaches, or migraines, make sure to see a healthcare professional for an evaluation first, but then try limiting screen time to six hours per day, avoiding all screens at least one hour before bed and taking the weekends “off” from social media. If you immediately feel better, you have a clear indication of how too much screen time is affecting your brain. �
Several other precautions you can take to prevent the previously mentioned symptoms can include: loading up on nutrients that have been shown to combat brain fog and vision problems like the carotenoid antioxidants zeaxanthin, lutein, and astaxanthin, found in green vegetables and a variety of colorful plant foods similar to these. If you can’t avoid using a computer or other digital device before bed, consider wearing a pair of blue-light-blocking glasses in the evenings, in which several research studies have shown that these can ultimately help restore melatonin production and improve sleep. �
Brain fog can make thinking, understanding, and even remembering basic information challenging. Brain fog is a symptom, rather than a single disorder, commonly associated with vision problems and other health issues like insomnia, anxiety, and even depression. Researchers and healthcare professionals have demonstrated that too much screen time, due to sitting in front of a computer screen or staring at a mobile device for extended periods of time, can ultimately change the brain, causing brain fog and vision problems, among other well-known symptoms. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
Have you been experiencing noticeable variations in your mental speed? Do you suffer from pain, discomfort, and inflammation? Have you been experiencing fatigue, especially after meals or exposure to chemicals, scents, or pollutants?�Brain fog is a symptom that can affect many brain functions, including memory and concentration. It can also be accompanied by other symptoms like vision problems. Too much screen time can cause brain fog and other health issues. � The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
References: �
Sissons, Claire. �Brain Fog: Multiple Sclerosis and Other Causes.� Medical News Today, MediLexicon International, 12 June 2019, www.medicalnewstoday.com/articles/320111.php#1.
Orenstein, Beth W. �When Chronic Fatigue Syndrome Harms Vision.� EverydayHealth.com, Everyday Health, 4 March 2010, www.everydayhealth.com/chronic-fatigue-syndrome/vision-problems.aspx.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
All can help relax muscles, relieve pain and increase mobility.
Proven Reduced Back Pain with *FOOT ORTHOTICS* | El Paso, Tx
Kent S. Greenawalt, President, and CEO of Foot Levelers discuss how custom foot orthotics can help reduce back pain, low back pain, and sciatica.
In a recent research study published by the American Congress of Rehabilitation Medicine (ACRM), researchers demonstrated that Foot Levelers custom foot orthotics help considerably reduce back pain and several of its associated health issues.
The research study also demonstrated that Foot Levelers custom foot orthotics and chiropractic care help tremendously reduce low back pain and sciatica.
Foot Levelers custom foot orthotics and chiropractic care helped improve the patient’s overall health and wellness.
Dr. Alex Jimenez is a chiropractor in El Paso, TX. can help provide these benefits through the utilization of chiropractic care and Foot Levelers custom foot orthotics, among other treatments.
NCBI Resources
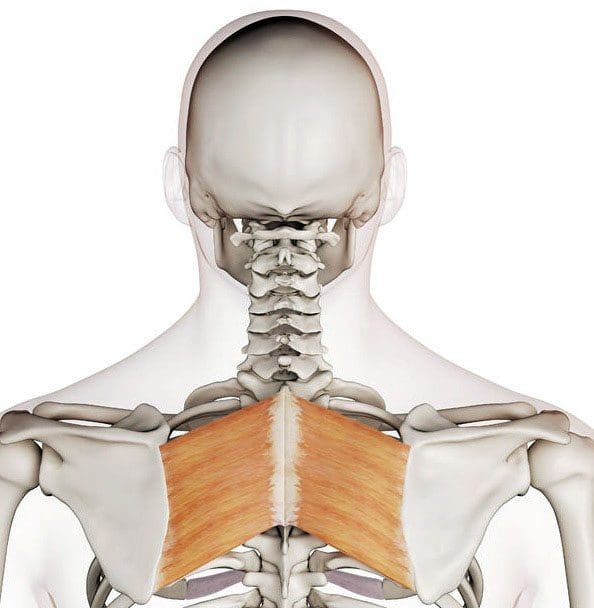
Pain in the upper and/or mid-back is not as common as lower back or neck pain. The upper back is called the thoracic spinal column, and it is the most secure part of the spine. The reach of movement in the upper back is limited because of the backbone�s attachments to the ribs (rib cage).
Upper back pain is generally caused by soft tissue injuries, like sprains or strains, muscle tension caused by bad posture, or looking downward for long time spans (eg, texting, mobile phone use).
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine









 Inflammatory markers and brain volume. Each SD increase in inflammation composite score at baseline was associated with a 532 mm3 smaller AD signature region volume (95% confidence interval [CI] ?922 to ?141), a 519 mm3 smaller occipital lobe volume (CI ?906 to ?132), a 110 mm3 smaller hippocampal volume (CI ?196 to ?24), and a 1,788 mm3 larger ventricular volume (CI 371 to 3,205) at follow-up (table 2). We found the estimated effect of a 1 SD increase in inflammation composite score during midlife on occipital lobe, ventricular, and hippocampal volume to be similar to the effect associated with possession of a single APOE ?4 allele in our multivariable regression analyses. No association was found for the total brain, frontal lobe, temporal lobe, or parietal lobe volume (ps > 0.071). Our findings did not change meaningfully after excluding participants who regularly used anti-inflammatory medication during the follow-up period (table e-2) and after including participants who met the criteria for dementia at visit 5 (table e-3). For descriptive purposes, associations between individual inflammatory markers and AD signature region volume are provided in a table e-4. �
Inflammatory markers and brain volume. Each SD increase in inflammation composite score at baseline was associated with a 532 mm3 smaller AD signature region volume (95% confidence interval [CI] ?922 to ?141), a 519 mm3 smaller occipital lobe volume (CI ?906 to ?132), a 110 mm3 smaller hippocampal volume (CI ?196 to ?24), and a 1,788 mm3 larger ventricular volume (CI 371 to 3,205) at follow-up (table 2). We found the estimated effect of a 1 SD increase in inflammation composite score during midlife on occipital lobe, ventricular, and hippocampal volume to be similar to the effect associated with possession of a single APOE ?4 allele in our multivariable regression analyses. No association was found for the total brain, frontal lobe, temporal lobe, or parietal lobe volume (ps > 0.071). Our findings did not change meaningfully after excluding participants who regularly used anti-inflammatory medication during the follow-up period (table e-2) and after including participants who met the criteria for dementia at visit 5 (table e-3). For descriptive purposes, associations between individual inflammatory markers and AD signature region volume are provided in a table e-4. � 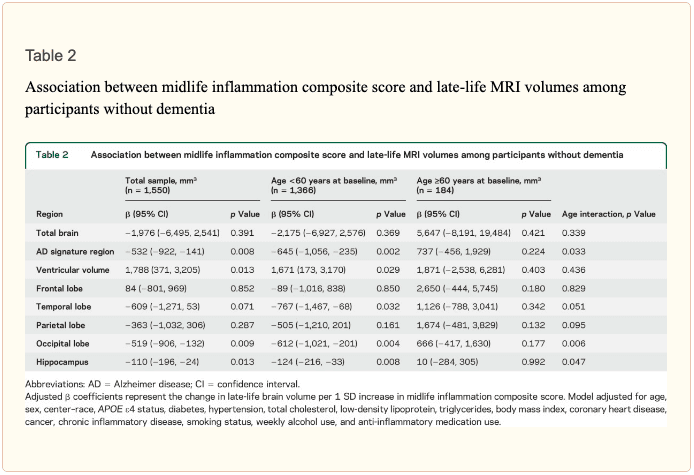 An assessment of linear trend revealed that compared to individuals with 0 elevated (?75th %tile) inflammatory biomarkers at baseline (reference), those with 1�2 and 3�5 elevated biomarkers had lower AD signature region (p trend = 0.001), occipital lobe (p trend = 0.007), and hippocampal volume (p trend = 0.041) 24 years later (figure 1). Compared to the reference group, participants with 3 or more elevated markers demonstrated 5.3% smaller AD signature region volumes, 5.7% smaller occipital lobe volumes, and 4.6% smaller hippocampal volumes, on average. However, this pattern was not statistically supported for the total brain, ventricular, frontal lobe, temporal lobe, and parietal lobe volume (p trends >0.072).
An assessment of linear trend revealed that compared to individuals with 0 elevated (?75th %tile) inflammatory biomarkers at baseline (reference), those with 1�2 and 3�5 elevated biomarkers had lower AD signature region (p trend = 0.001), occipital lobe (p trend = 0.007), and hippocampal volume (p trend = 0.041) 24 years later (figure 1). Compared to the reference group, participants with 3 or more elevated markers demonstrated 5.3% smaller AD signature region volumes, 5.7% smaller occipital lobe volumes, and 4.6% smaller hippocampal volumes, on average. However, this pattern was not statistically supported for the total brain, ventricular, frontal lobe, temporal lobe, and parietal lobe volume (p trends >0.072). 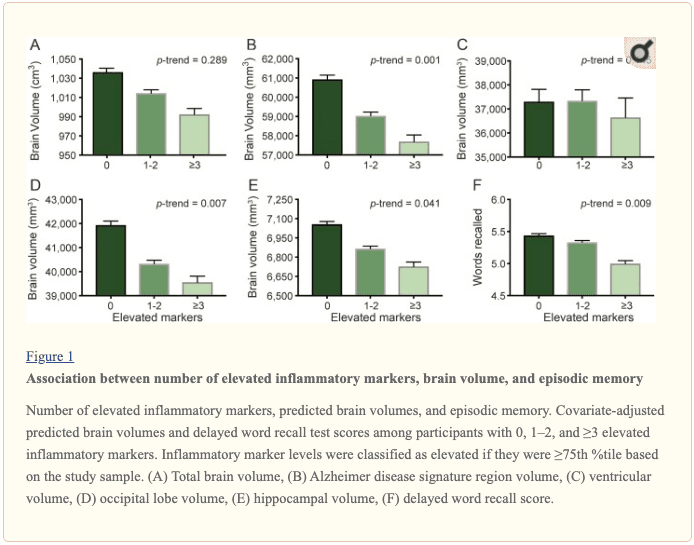 The modifying effects of age, race, and sex. A significant age-by-inflammation composite score interaction was found for the AD signature region, occipital lobe, and hippocampal volume (table 2). Because a reversal of association was observed at age 60 (figures 2, e-1, and e-2), we stratified the sample into young-midlife and old-midlife subgroups (<60/? 60). As displayed in table 2, the associations between higher midlife inflammation composite score and lower AD signature region, occipital lobe, and hippocampal volume at follow-up were significantly stronger among participants who were 60 or younger at baseline compared to those who were older than 60. A marginal race-by-inflammation composite score interaction was found for occipital lobe volume, whereby a higher midlife inflammation composite score was associated with lower occipital lobe volume among white, but not African American, participants (table 3). No interactions with sex were found (table e-5). �
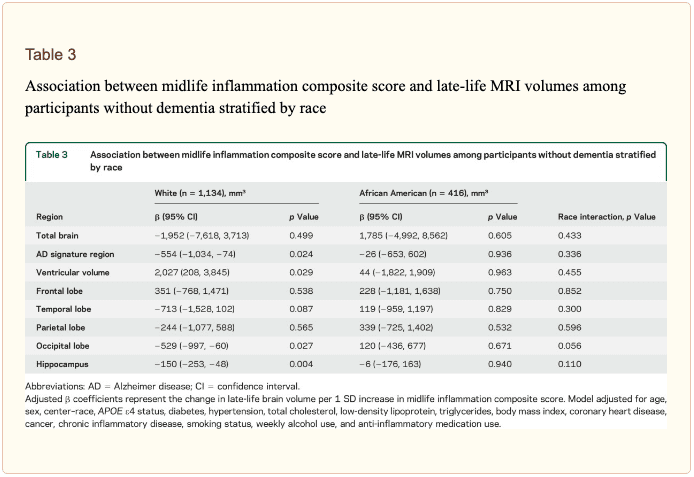
The modifying effects of age, race, and sex. A significant age-by-inflammation composite score interaction was found for the AD signature region, occipital lobe, and hippocampal volume (table 2). Because a reversal of association was observed at age 60 (figures 2, e-1, and e-2), we stratified the sample into young-midlife and old-midlife subgroups (<60/? 60). As displayed in table 2, the associations between higher midlife inflammation composite score and lower AD signature region, occipital lobe, and hippocampal volume at follow-up were significantly stronger among participants who were 60 or younger at baseline compared to those who were older than 60. A marginal race-by-inflammation composite score interaction was found for occipital lobe volume, whereby a higher midlife inflammation composite score was associated with lower occipital lobe volume among white, but not African American, participants (table 3). No interactions with sex were found (table e-5). � 
 Inflammatory markers and episodic memory. Late-life episodic memory, which was associated with hippocampal and AD signature region volume after controlling for age (partial rs > 0.21, ps < 0.001), was reduced among participants with higher levels of the inflammation composite score. Each SD increase in inflammation composite score was associated with a ?0.08 SD performance decrement on the DWR after adjusting for covariates (CI ?0.15 to 0.00; p = 0.046). Similarly, a higher number of elevated inflammatory biomarkers at baseline was associated with reduced DWR performance (p trend = 0.009; figure 1). �
Inflammatory markers and episodic memory. Late-life episodic memory, which was associated with hippocampal and AD signature region volume after controlling for age (partial rs > 0.21, ps < 0.001), was reduced among participants with higher levels of the inflammation composite score. Each SD increase in inflammation composite score was associated with a ?0.08 SD performance decrement on the DWR after adjusting for covariates (CI ?0.15 to 0.00; p = 0.046). Similarly, a higher number of elevated inflammatory biomarkers at baseline was associated with reduced DWR performance (p trend = 0.009; figure 1). �