Understanding your spine, the way it works and moves is critical to finding the right back pain treatment when back pain or injury creeps in.
People don’t really think about their spines until back pain rears its ugly head. The spine is not one continuous structure that extends from the neck to the tailbone. It is an intricate, complex group of several structures.
Some understanding of the spine can help individuals make informed decisions before getting involved in activities that can cause a spinal injury.
Anatomy
The spine is made up of 24 vertebrae, these are the bones stacked on top of each other and forms the spinal column.
The spinal cord passes through the vertebrae that acts as a protective frame.
The spinal column surrounds the spinal cord like an electrical cord. It protects the nerves that run from the brain, through the spinal column and out to the rest of the body.
The spinal cord is the highway of nerves that carry the brain’s signals to the rest of the body, allowing the ability to move the arms and legs, etc.
The soft, spongy shock absorbers in between the vertebrae are the intervertebral discs.
They keep the vertebrae separated so smooth function and movement is possible.
Because the spine is such a complicated network of bones, discs, muscles, nerves, and ligaments, getting to the bottom of exactly what�s wrong when back pain sets in can be a complicated process. This is where having some knowledge of your spine can help a doctor or chiropractor figure out what’s going on and then developing the best treatment plan possible.
Time
Dealing with time can be a tricky issue when suffering from back pain.
When only soreness, stiffness and muscle stress occur every so often then time can be the best medicine, as rest is all that is needed for the swelling to go down.
But when the pain does not go away with rest and is getting worse, waiting for evaluation is not an option.
Imagine all of those complex structures in the spine as dominos in a row.
If one domino/disc falls or slips pressure is placed on all the other dominos/discs to work harder to support the failing structure. But they can only do this for so long until the other discs or other areas of the body begin to fail.
Left untreated will eventually cause the failure of other structures of the body.
Strong Spine
It was designed to support the entire body combined with the additional weight that we carry.
It deserves care and respect.
Unfortunately, it is not made of titanium and is susceptible to injury.
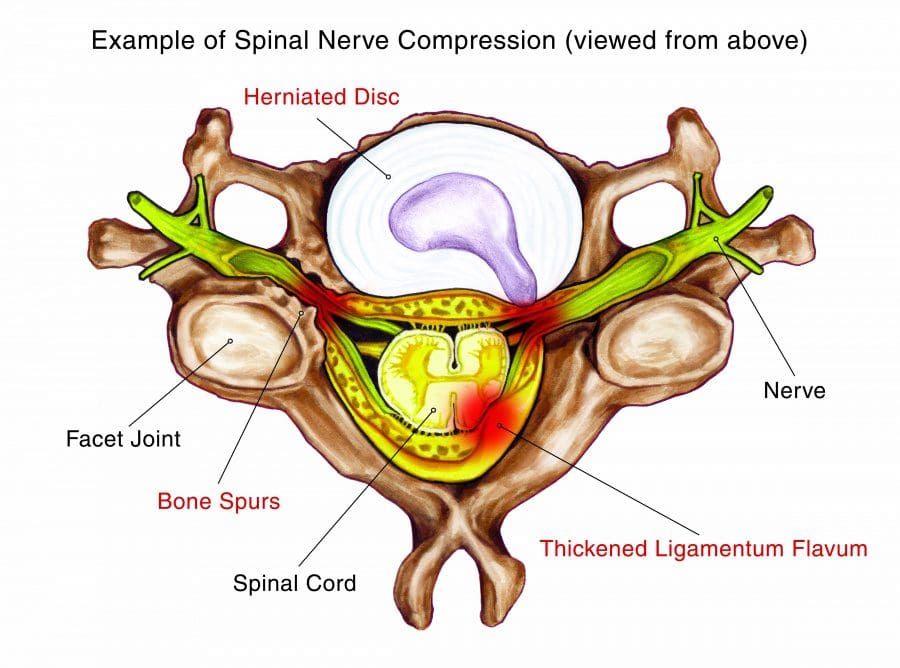
Spinal Nerve Compression
When a spinal nerve gets compressed, entrapped, or pinched it becomes inflamed and pain sets in. In the illustration of a neck spine segment, many different disorders are causing the�nerve�compression in this instance:
Herniated disc
Thickened ligament
Bone spurs called osteophytes
Making sure to pay close attention to your spine will safeguard it. So spend some time to understand how your spine operates.� Looking at some basic yoga for back poses can be a great start to understand how your spine functions.
What is Yoga?
In its purest form,�it is an ascetic and spiritual discipline that comes from Hindu culture. It involves simple meditation, breath control, and performing body postures.
While an ancient practice long used for spiritual and emotional healing as well as physical wellness, yoga has been adopted in western culture and widely accepted as a form of fitness as well as a therapeutic practice used for relaxation and overall good health. It focuses on inward healing with outward results.
Proven Reduced Back Pain with *FOOT ORTHOTICS* | El Paso, Tx
Kent S. Greenawalt, President, and CEO of Foot Levelers discuss how custom foot orthotics can help reduce back pain, low back pain, and sciatica. In a recent research study published by the American Congress of Rehabilitation Medicine (ACRM), researchers demonstrated that Foot Levelers custom foot orthotics help considerably reduce back pain and several of its associated health issues.
The research study also demonstrated that Foot Levelers custom foot orthotics and chiropractic care help tremendously reduce low back pain and sciatica. Foot Levelers custom foot orthotics and chiropractic care helped improve the patient’s overall health and wellness. Dr. Jimenez is a chiropractor in El Paso, TX who can help provide these benefits through the utilization of chiropractic care and Foot Levelers custom foot orthotics, among other treatments.
NCBI Resources
The spine is a complex structure. Understand that the spine is also surrounded by fibrous and muscular supporting structures, intervertebral discs, the spinal cord and nerve roots, and blood vessels. An injury such as a back sprain or strain caused by improperly lifting and twisting simultaneously can often be a cause for back pain. Chiropractic care is a well-known, alternative treatment option utilized to prevent, diagnose and treat a variety of injuries and conditions associated with the spine, primarily subluxations or spinal misalignments.
Do you often feel low brain endurance for focus and concentration? Do you often crave sugar and sweets in the afternoon? Or do you feel energized after meals? Glucose, or sugar, is the main source of energy in the human body. And, because the human brain has so many nerve cells or neurons, it is one of the most energy-demanding organs, which utilizes about one-half of all the energy from glucose in the human body. Sugar is important but too much of it can also have its downsides. �
Brain functions, such as memory, thinking, and learning, are relatively associated with glucose levels and how efficiently the brain utilizes this essential energy fuel source. If there isn�t enough glucose, or sugar, in the brain, by way of instance, neurotransmitters, or the human brain�s chemical messengers, don’t develop properly and the communications between neurons can ultimately break down. Additionally, dysglycemia, a common health issue caused by abnormal blood glucose levels, can cause loss of energy for brain function and has also been associated with poor attention and cognitive function. �
�The human brain is dependent on sugar or glucose as its main energy fuel source,� stated Vera Novak, MD, Ph.D., an HMS associate professor of medicine at Beth Israel Deaconess Medical Center. �It just simply cannot be without it.� �
What is Dysglycemia?
As previously mentioned, brain structure and function, such as cognition, can be affected by dysglycemia, or blood glucose abnormalities, in older adults. Researchers conducted a cross-sectional and longitudinal cohort research study, analyzing the association of dysglycemia with brain health. The researchers found that dysglycemia is associated with an increased number of brain infarcts, white matter hyperintensities volume, and decreased total white matter, gray matter, and hippocampus volume cross-sectionally. According to the research study, there was also a decrease in gray matter volume longitudinally. Dysglycemia was ultimately associated with reduced language performance, speed, and visuospatial function. �
�Our results suggest that dysglycemia affects brain health in elderly survivors, evidenced by higher cerebrovascular disease, lower white, and gray matter volume as well as language, visuospatial function, and cognitive speed,� stated the authors. �
Dysglycemia can cause changes in blood glucose levels which may cause a variety of health issues. Dysglycemia is also not necessarily defined by specific blood sugar levels. Instead, having an abnormally low, high, or unstable blood glucose levels suggests an underlying health issue that requires further investigation. Moreover, while type 1 and type 2 diabetes are the most common causes of dysglycemia, other examples of blood sugar level abnormalities can include gestational diabetes and pre-diabetic conditions as well as drug-related and genetically related abnormalities of the blood sugar levels. �
Furthermore, dysglycemia can be a result of hereditary or environmental factors, or it can even be a combination of both. Genes can predispose a person to ultimately develop dysglycemia over time, just as much as several lifestyle habits can, too. A poor diet high in unhealthy fats, sugars, and processed foods can commonly cause a person to develop dysglycemia. Lacking certain vitamins and minerals that enhance the human body�s sensitivity to insulin can also cause dysglycemia. �
Dysglycemia and Brain Health
Although the brain needs glucose or sugar, too much of this energy fuel source can also have several side-effects. A 2012 research study on animals conducted by researchers at the University of California at Los Angeles demonstrated a positive relationship between the consumption of fructose, another form of sugar, and the aging of cells. A 2009 research study, also utilizing animal models and conducted by a team of scientists at the University of Montreal and Boston College, connected excess glucose consumption to memory and cognitive deficiencies. Further research studies are still required. �
The effects of glucose and other forms of sugar on the human brain may be the most profound in diabetes, a group of health issues in which high blood glucose levels persist over a prolonged period of time. Type 1 diabetes is a health issue in which the immune system destroys the cells in the pancreas that produce insulin, a hormone utilized by the human body to maintain and regulate blood glucose levels. Type 2 diabetes, caused by dietary and other environmental factors, is a health issue in which cells become overwhelmed by insulin and fail to properly respond and they ultimately become insulin resistant. �
Long-term diabetes, either type 1 or type 2, can have many consequences for the brain cells, or neurons, as well as the brain. High blood glucose levels can affect the brain�s functional connectivity which connects brain regions that share functional properties and brain matter. It can also cause the brain to atrophy or shrink and it can lead to small-vessel disease, which restricts blood flow in the brain, causing cognitive difficulties and it can cause the development of vascular dementia. �
In her laboratory, Novak evaluated several ways to prevent these effects in people with type 2 diabetes. One of these ways involves a nasal spray known as intranasal insulin (INI). When used, INI enters the brain and binds to receptors in its memory networks, including the hippocampus, hypothalamus, and insular cortex. As signaling within these memory networks become more efficient, cognitive functions in these areas, such as learning and visual perceptions of spatial relationships, improve. �
�Type 2 diabetes accelerates brain aging,� says Novak, �which, in turn, accelerates the progression of functional decline. With intranasal insulin, we�re hoping to find a new avenue for treatment to slow down these effects or prevent them altogether.� �
In a pilot research study, Novak and her colleagues found that a single dose of INI had a positive effect on memory, verbal learning, and spatial orientation. She is now planning the first clinical trial of INI in older adults with type 2 diabetes. The results of the clinical trial are especially relevant because of the high prevalence of dementia and significant cognitive decline among older adults with diabetes. Sugar, or glucose, is fundamental, however, it must be controlled for overall brain health. �
Glucose, or sugar, is an important source of energy fuel for every cell in the human body, especially the brain. However, excess amounts of blood glucose, or sugar, levels can be more harmful than beneficial and it can ultimately cause a variety of brain health issues, including neurological diseases like dementia and Alzheimer’s disease. Dysglycemia, or abnormal blood glucose, or sugar, levels, is a common condition in diabetes. Managing and regulating glucose, or sugar, in patients with diabetes is essential to promote overall brain health and wellness, according to research studies. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Do you often feel low brain endurance for focus and concentration? Do you often crave sugar and sweets in the afternoon? Or do you feel energized after meals? Glucose, or sugar, is the main source of energy in the human body. And, because the human brain has so many nerve cells or neurons, it is one of the most energy-demanding organs, which utilizes about one-half of all the energy from glucose in the human body. Sugar is important but too much of it can also have its downsides. �
Brain functions, such as memory, thinking, and learning, are relatively associated with glucose levels and how efficiently the brain utilizes this essential energy fuel source. If there isn�t enough glucose, or sugar, in the brain, by way of instance, neurotransmitters, or the human brain�s chemical messengers, don’t develop properly and the communications between neurons can ultimately break down. Additionally, dysglycemia, a common health issue caused by abnormal blood glucose levels, can cause loss of energy for brain function and has also been associated with poor attention and cognitive function. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Marchione, Victor. �Cognition and Brain Structure Affected by Dysglycemia in Older Adults: Study.� Bel Marra Health – Breaking Health News and Health Information, Bel Marra Health, 10 Jan. 2017, www.belmarrahealth.com/cognition-brain-structure-affected-dysglycemia-older-adults-study/.
Edwards, Scott. �Sugar and the Brain.� Sugar and the Brain | Department of Neurobiology, neuro.hms.harvard.edu/harvard-mahoney-neuroscience-institute/brain-newsletter/and-brain-series/sugar-and-brain.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Health coaches are becoming more and more crucial as modern medicine continues to improve. Now more than ever, the health care field is progressing at high speeds and professionals do not always have the available time some patients desire. Here is where health coaches become involved. Basically, the position of a health coach was produced to fill the emptiness in several doctor offices. Many physicians contribute but do not have the time or resources to assist each individual and aid in constructing healthy habits on a day to day basis. However, health coaches are available to be a supportive mentor that assists and guides patients in making healthy lifestyle changes. Many patients who seek help to change their lifestyle are those suffering from some kind of chronic pain, headaches, or joint inflammation.
In the previous weeks, we have defined and explained what a health coach is and what they really do, as well as the first two steps a health coach might take with a patient. Throughout this article, the third and fourth steps will be broken down and analyzed.
Need a refresher? No problem!
Health Coaching in El Paso: Part 1 can be found by clicking here.�
Health Coaching in El Paso: Part 2 can be found by clicking here.�
Step 3: Building A Plan For Action
Once the health coach understands the values and goals of the patient, a plan for change can get mapped out. One thing that is unique about building a plan, is that the health coach encourages the patient to have a say in it and contribute to building the plan. The ways of medicine have changed, and this aspect is one of them. Before, many patients would sit silently as doctors instructed them on their new protocol. However, it has been shown that patients who build a plan of action with the practitioner, are more likely to comply and complete a program.
In addition to this, the perspective of the patient can help maintain expectations and keep the plan of action at a realistic timeline. The health coach will offer their suggestions during this process as well as their perspective. Often times, this will help the patient break down their overall goal, into smaller more specific goals or tasks.
As soon as the overall goals are broken down into specific tasks, the health coach will then map out the process to complete these tasks. It can be simple to overlook small steps when thinking of a bigger picture, so the health coach will provide tools to better help the patient understand.
An example of this would be for a patient who wants to lose weight. Mapping out these tasks will have an end result that looks similar to these:
� I will try a new fruit and vegetable every day this week and identify what I enjoy
� I will think of different, creative ways to work movement into my day, such as finding a walking trail in my neighborhood
� I will always keep a water bottle with me and refill it every two hours
� I will cook dinner two nights this week
� I will go for a walk after dinner every day this week
By providing the patients with these smaller tangible tasks, the patient now has “homework” in a sense to complete these throughout the week. The health coach will set a deadline with these tasks and check-in with the patient regularly to ensure they are on track.
Step 4: Tracking Progress And Results
Before progress can be tracked, the health coach will take into consideration the patient’s goal and determine how often the patient will need to come in for follow-ups. For many patients, a combination of follow up techniques are used. Health coaches understand that in-person is not always the most convenient and does not always fit into the patient’s schedule. If this is the scenario, health coaches work around that to create follow-ups by using some in-person visits, some phone conversations, or other virtual check-in meetings that are HIPAA compliant.
Often times, during a lifestyle change patients may become confused or discouraged. It is important to remember that this is normal and progress is not always a straight line up, but rather includes bumps along the way. In order to better help the patient, the health coach will provide them with a helpful “where to turn” guide.
As humans, at different times we require different types of support. The where to turn guide will be a supporting reminder of things to do to counteract these feelings when they arise. Items included in this guide will be ideas such as:
� Pursuing a hobby, like dancing or playing an instrument
� Getting out in nature
� Starting a mindfulness practice
� Making art, like drawing or writing
� Joining a community, religious, or spiritual group
In addition to these activities, the health coach will determine with the patient what kind of support (internal or external) is appropriate depending on the situation.
Lastly,� progress does not always look like a dip in the number on the scale. Progress can come in many different forms. In order to help the patient appreciate and realize all the progress they are making, a health coach will ask questions like:
1. How can you appreciate your progress?
2. How would you describe the benefits of your experience?
3. What�s been good about this experience?
4. How have you grown?
As mentioned earlier, a health coach is important to have as they help one realize all the steps it truly takes to be successful and reach their health goals. There are many critical steps that are easily overlooked when the big picture is on their minds. The final two steps that a health coach will work on with a patient is to help them visualize their best self and to create a plan for resiliency. These two topics will be discussed in the next article.
�Using a health coach to complete a lifestyle change is similar to the work of going to therapy. One must be willing to accept the tools and resources they are givien, and actually do the work provided or it will not produce results. If a patient is truly serious about completing a lifestyle change, using a health coach is an extremly beneifical resource! As one can see, they work with the patients to hammer down tasks and ideas that a patient might not have orignally thought of. By utilizing a health coach, the patient has a higher chance of reaching their goals. – Kenna Vaughn, Senior Health Coach
All information and resources for this post came from an Integrative Practioner article titled, “A Six-Step Approach To Health And Wellness Coaching: A Toolkit for Practice Implementation” and can be found by clicking here; as well as listed below in the proper bibliography.
*The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Bibliography:
American Psychological Association (2019). The Road to Resilience. Retrieved from: https://www.apa.org/helpcenter/road-resilience
Jonas, W. (2019). Empowering patients with chronic diseases to live healthier through health coaching: Integrative primary care case study. Samueli Integrative Health Programs.�Retrieved from: https://www.health.harvard.edu/staying-healthy/give-yourself-a-health-self-assessment
Miller, W. and Rose, G. (1991). Motivational Interviewing: Preparing People to Change Addictive Behavior. Guilford Publications.
Pecoraro, Wendy. �A Six-Step Approach to Health and Wellness Coaching: A Toolkit for Practice Implementation.� Official Media Integrative Practitioner, 17 Oct. 2019, www.integrativepractitioner.com/resources/e-books/a-six-step-approach-to-health-and-wellness-coaching-a-toolkit-for-practice-implementation.
Trzeciak, S. and Mazzarelli, A. (2019). Compassionomics. Studer Group. Virginia Polytechnic Institute and State University. The Stages of Change.Retrieved from: http://www.cpe.vt.edu/gttc/presentations/8eStagesofChange.pdf
Your Coach (2009). SMART goals.Retrieved from: https://www.yourcoach.be/en/coaching-tools/
Do you often feel energy level drops in the afternoon? Do you often crave sugar and sweets in the afternoon? Do you often have difficulty concentrating before eating? Various medical conditions can affect the overall health of our body and mind. However, research studies have found that anemia caused by iron deficiency can tremendously affect our brain health. �
Iron deficiency is considered to be one of the most prevalent nutritional health issues, affecting approximately 2.5 billion people worldwide. In developing countries, about 40 percent of children and 50 percent of pregnant women have an iron deficiency. Iron is an essential mineral found in approximately 5 percent of the earth�s crust, however, inefficiency in absorption, low iron levels in staple grain foods, and a variety of medical conditions can make iron deficiency a common problem among humans. In first world countries, iron deficiency is still one of the most common nutrient deficiencies. �
What Causes Iron Deficiency and Anemia?
Poor iron intake and increased iron loss, generally through bleeding or breastfeeding, are several of the main causes of iron deficiency. Pregnant women, breastfeeding women, women with heavy periods, children or picky eaters, vegetarians and vegans, as well as people with digestion health issues which cause decreased iron absorption like celiac disease or post gastric bypass, and people with increased bleeding, such as cancer, ulcers, gastritis, or parasites, are generally at higher risk for iron deficiency. High calcium intake, by way of instance, children who drink a lot of milk, can also affect iron absorption, together with drugs and/or medications, such as antacids and proton-pump inhibitors for gastroesophageal reflux disease. �
Although low iron levels are well-known for causing anemia because red blood cells need iron as a part of hemoglobin, iron is also needed for the brain and nerves. Severe iron deficiency in younger children can ultimately cause irreversible damage to cognition and result in lower IQ and developmental delays, especially during the most fundamental stages of human development and up to 16 months of age. Even in adults. the most common symptoms associated with iron deficiency are generally neurological symptoms, including fatigue, brain fog, and restless legs that cause insomnia, among other symptoms. �
Pica, the abnormal behavioral compulsion to eat non-nutritional foods like dirt or clay, is tremendously prevalent in regions of the world where iron deficiency is common. In the developed world, pica is a rare health issue, however, it still frequently occurs in children, pregnant women, and among other groups of people that are at higher risk for iron deficiency, including people who have had gastric bypass. Non-neurological symptoms associated with iron deficiency ultimately include pallor, generalized weakness, and higher than usual heart rate along with shortness of breath, especially with exertion. �
What are the Symptoms of Iron Deficiency?
As previously mentioned above, iron deficiency can cause problems associated with cognition and neurological health issues, such as restless legs and insomnia. The exact mechanisms of why this happens are unknown, however, without enough iron in the brain and nerves, there are problems with neurotransmitter signaling, the development of nerve insulation known as myelin, and brain energy metabolism. Reduced central neuron processing is considered to be one of the most critical problems associated with iron deficiency, which can be a cause of psychiatric symptoms and ongoing psychiatric problems. �
Occasionally, iron deficiency may also cause anxiety, depression, irritability, and even poor concentration and restlessness. By way of instance, iron deficiency has a much higher prevalence in children with ADHD but the symptoms can improve with iron supplements. People with iron deficiency have higher risks of developing psychiatric disorders, especially ADHD, and developmental disorders. Evidence has demonstrated that iron deficiency can cause a variety of other health issues. �
Iron enters the brain through the blood-brain barrier via transferrin receptors. Iron uptake into the brain is highly regulated but it also does highly depend on the iron status of the human body. Therefore, people with low iron levels will have much less iron going into the brain and people with high iron levels will have much more iron going into the brain. Several regions of the brain also appear to gather iron and have higher levels than others. Moreover, neurological symptoms can manifest before developing iron deficiency anemia. Thus, healthcare professionals can’t rule out iron deficiency anemia from the most commonly utilized basic screening test, a complete blood count. A better general screen involves ferritin levels, where less than 15 ng/ml presents the diagnosis for iron deficiency but less than 40 ng/ml presents with fatigue, brain fog, restless legs, and other neurological symptoms. Ferritin on its own can be misleading in populations of people with chronic inflammation, including people on dialysis, where ferritin can be high even if the person is diagnosed with iron deficiency. Furthermore, a full iron workup includes hemoglobin, MCV, ferritin, total iron-binding capacity, serum iron, and transferrin saturation. �
What is the Treatment for Iron Deficiency Anemia?
Treating iron deficiency is considerably simple through the utilization of iron supplements or in mild or moderate cases by encouraging the consumption of foods that are high in iron. Occasionally, people with severe absorption health issues will need iron transfusions intravenously. Meat and seafood are the best sources of easily absorbable heme iron, however, non-heme iron is naturally found in leafy greens, beans, and nuts. Make sure to talk to your doctor if you have iron deficiency. �
It is ultimately essential to make sure if you have iron deficiency before treating it with increased amounts of iron supplements. With the exception of blood loss, the only way to reduce excess iron is through the process of skin cells flaking off. Therefore, adult men who take a lot of iron supplements and people with a genetic tendency to absorb more iron from foods are at a higher risk of developing a medical condition, known as hemochromatosis or severe iron overload. �
Excess iron is stored in the liver and can lead to scarring of the liver, known as cirrhosis. Iron overload can also lead to joint and hormonal problems and it can also cause a bronze-ish skin color. Symptoms of hemochromatosis include joint pain, fatigue, and low sex drive as well as a higher risk of developing diabetes. High serum iron is associated with health issues like high blood pressure. People who aren�t iron deficient can consider regular blood donations to prevent accidental iron overload. Iron is one of those types of minerals that should neither be too high or too low but rather, just right. More research studies, especially clinical trials analyzing common medical conditions, such as restless legs, insomnia, and ADHD, are fundamental to help healthcare professionals understand the relationship between iron deficiency anemia and brain health. �
Recent research studies have demonstrated that iron deficiency anemia may be associated with brain health issues. Because the brain and nerves need iron for many functions, iron deficiency can cause a variety of symptoms and medical conditions, including brain fog, fatigue, restless legs with insomnia, anxiety, depression, and cognitive problems, besides anemia or lack of healthy red blood cells. Treatment for iron deficiency anemia may utilize iron supplements, however, it’s important to make sure to talk to a qualified healthcare professional in order to avoid risks and side effects through iron supplementation.� – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Do you often feel energy level drops in the afternoon? Do you often crave sugar and sweets in the afternoon? Do you often have difficulty concentrating before eating? Various medical conditions can affect the overall health of our body and mind. However, research studies have found that anemia caused by iron deficiency can tremendously affect our brain health. � Iron deficiency is considered to be one of the most prevalent nutritional health issues, affecting approximately 2.5 billion people worldwide. In developing countries, about 40 percent of children and 50 percent of pregnant women have an iron deficiency. Iron is an essential mineral found in approximately 5 percent of the earth�s crust, however, inefficiency in absorption, low iron levels in staple grain foods, and a variety of medical conditions can make iron deficiency a common problem among humans. In first world countries, iron is still considered to be the most common nutrient deficiency. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Deans, Emily. �Heavy Metal: Iron and the Brain.� Psychology Today, Sussex Publishers, 29 Nov. 2015, www.psychologytoday.com/us/blog/evolutionary-psychiatry/201511/heavy-metal-iron-and-the-brain.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Biomarkers are molecules that can help diagnose a health issue. These have become important for verifying investigations, choosing the best remedies, and monitoring disease progression. One exception, however, includes biomarkers for neurological diseases. Neurological biomarkers are found in the cerebral spinal fluid (CSF) or, in undetectable amounts, in the blood vessels. The human brain is closely guarded by the blood-brain barrier which protects it from damaging compounds circulating throughout the blood vessels. The blood-brain barrier has made it inaccessible to use these biomarkers. �
Biomarkers may be analyzed using the CSF but this also needs an invasive lumbar puncture process. Biomarker signatures, or recent improvements in discovery, in addition to the ability of clusters of biomarkers, are currently helping to make neurological disorders more treatable and more reachable. Treating and preventing neurological disorders, such as chronic traumatic encephalopathy (CTE), Alzheimer’s disease, Parkinson’s disease, autism, and major depressive disorder, is very likely to become less difficult to diagnose with the recent arrival of neurological biomarkers found in the blood. �
Biomarker for Brain Health Issues
Biomarker signatures, found with panels of high-quality antibodies, are yet another safe and effective tool for evaluating neurological disorders and diseases. Assistant professor of neurology and immunobiology at the University of Arizona College of Medicine at Tucson, Kristian Doyle, utilizes biomarkers to examine how the immune system deals with dead brain tissue. The system eliminates brain tissue with a procedure called liquefactive necrosis following a stroke but the pathophysiology of the procedure is unknown. This information is essential because liquefactive necrosis may be neurotoxic. �
“We utilize multiplex immunoassays to describe inflammation within chronic stroke infarcts in the point of liquefactive necrosis, and to describe changes by ordinary stroke comorbidities,” says Doyle. Because over 10 million individuals survive a stroke every year, Doyle expects that biomarkers may help them monitor the development of liquefactive necrosis and start to tailor remedies that mitigate the secondary harm due to this procedure,” he states. Another connection between inflammation and neurotoxicity is analyzed by Alysson Muotri, professor of molecular and cellular medicine and director of the Stem Cell Program at the University of California, San Diego School of Medicine. The Muotri laboratory uses induced pluripotent stem cells (iPSCs) from individuals with schizophrenia and autism to search for biomarkers of those ailments. �
Muotri’s laboratory started analyzing the cytokine interleukin-6 (IL-6) as a biomarker because evidence indicates that chronic exposure to elevated cytokines might be neurotoxic together with elevated levels associated with depression, autism, and schizophrenia. “The gap of one of the many brain disorders could function as cytokines act on particular types or subtypes of nerves, or within a particular brain area,” states Muotri. His laboratory differentiates iPSCs to cells, which they suspect might be releasing cytokines from patients. Also, because IL-6 can also be involved in immune-inflammatory pathways, Muotri supposes a connection between autism and in utero exposure to infection, such as the Zika virus. �
“Our forecast is that the inflammation caused by Zika vulnerability is sufficient to make a neurotoxic environment which could rewire how the human brain is shaped,” he states. “We see that in mice, therefore, we believe some Zika-exposed children are going to develop autism or have intellectual disabilities” Larger biomarker signatures are available with technologies from CDI Laboratories, which provides microarrays of practical human proteins, including over 20,000 to a single variety, to check the antibodies within human liquid biopsy samples, including blood, serum, plasma, CSF, or tissue lysates. The consequent “autoantibody profile” is a helpful tool for study and for diagnoses or prognoses of individuals. �
“We have worked in the area of biomarker discovery for various neurodegenerative diseases like multiple sclerosis, neuropsychiatric lupus, Alzheimer’s disease, and Parkinson’s disease,” states George Dorfman, director of business development in CDI Laboratories, a spin-off firm located in Baltimore, Maryland, and Mayaguez, Puerto Rico which was created from research in the High Throughput Biology Center at Johns Hopkins University. CDI’s stage is particularly beneficial in building panels for biomarker discovery because researchers can start by utilizing patient samples or banked trials to evaluate resistant profiles of cohorts that reveal specific symptoms or no indications in the event of control trials. �
“This provides us with an inherent candidate biomarker panel that offers advice on the following clinical outcome or curative efficacy, which is confirmed to yield the last panel, then interpreted into the state an ELISA-based kit or any other immunodiagnostic format at the clinical setting,” says Dorfman. “In the event of multiple sclerosis, as a patient grows through measures of this disease, their entire body creates novel antibodies or greater present antibody titers against specific proteins, such as myelination proteins. Our panels may discover these, to provide a notion about exactly what patients’ disease development might seem like, and supply a signature which may be interpreted into another evaluation or an FDA-approved diagnostic” CDI’s technologies have also been utilized to create an autoantibody profile for neuropsychiatric lupus, a beneficial diagnostic tool to ultimately help diagnose a neurological disorder that typically lacks obvious clinical signs. �
Understanding Biomarkers for Brain Health
The amount and types of biomarkers, as well as the quantity of information which researchers have to arrange, can help provide better remedies and prevention methods and techniques. “It ought to be no surprise that researchers spend around 80 percent of the time handling and not assessing statistics,” states Scott Marshall, managing director of translational informatics and diagnostic sciences in Precision for Medicine in Frederick, Maryland. The biomarker data management system, PATH, was made to incorporate any sort of biomarker information for further neurological disease diagnosis. �
“The true power of biomarkers comes if you connect this data to clinical information,” states Marshall. Their biomarker information management system supports translational research and biomarker-guided medicine development and puts no limitation on the number of biomarkers that may be tracked. “It can manage multiple biomarker technologies concurrently, such as complicated flow cytometry, next-generation sequencing, immuno-sequencing, epigenetic profiling, and other varieties of assays measuring biological variant too,” states Marshall. Their kind of “translational informatics” instrument is much more efficient than generating reams of information” with no strategy to acquire actionable insights out of these.” �
Research teams utilize Precision to Medicine’s platform for neuro-related programs that vary from illness pathogenesis to creating complicated signatures that are predictive of treatment response. By way of instance, the system was utilized in a research study including the evaluation of transcriptomic and genomic data in the treatment of major depressive disorder. The outcome is a genomically defined subset of individuals utilizing a probability of improvement. “This type of signature can now be evaluated by means of an assay, which may subsequently be developed to accompany diagnostic or free diagnostic to successfully target the correct individual group,” states Marshall. Biomarker data management systems become more fundamental as distinct kinds of biomarkers are examined collectively, ultimately including proteins and miRNAs. �
Combining kinds of biomarkers will very likely boost their usefulness. “Diagnostics is becoming increasingly more important as we know that the interplay between microRNAs, proteins, DNA, and messenger RNA is necessary,” states Pregibon. Clinical decision-making may profit particularly in which the human brain has been blocked by the blood-brain barrier until lately. “The chance to leverage biomarker-driven targeted treatments means that the sufferers that are more inclined to react to treatments are getting them quicker,” states Marshall. “For researchers, that’s the energy of biomarkers.” �
�
The recent ability to be able to detect neurological biomarkers in the blood, despite the blood-brain barries, is largely due in part to new technological advances in diagnosis and detection. Several of these technologies can ultimately increase sensitivity, however, increased sensitivity can help improve earlier detection or diagnosis of biomarkers for neurological diseases and disorders. Researchers and healthcare professionals currently believe that the presence of these biomarkers may be present earlier than we currently understand, which can help improve health issue diagnosis and treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
Biomarkers are molecules that can help diagnose a health issue. These have become important for verifying investigations, choosing the best remedies, and monitoring disease progression. One exception, however, includes biomarkers for neurological diseases. Neurological biomarkers are found in the cerebral spinal fluid (CSF) or, in undetectable amounts, in the blood vessels. The human brain is closely guarded by the blood-brain barrier which protects it from damaging compounds circulating throughout the blood vessels. The blood-brain barrier has made it inaccessible to use these biomarkers. �
Biomarkers may be analyzed using the CSF but this also needs an invasive lumbar puncture process. Biomarker signatures, or recent improvements in discovery, in addition to the ability of clusters of biomarkers, are currently helping to make neurological disorders more treatable and more reachable. Treating and preventing neurological disorders, such as chronic traumatic encephalopathy (CTE), Alzheimer’s disease, Parkinson’s disease, autism, and major depressive disorder, is very likely to become less difficult to diagnose with the recent arrival of neurological biomarkers found in the blood. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Smith, Caitlin. �Biomarkers on the Brain: Putting Biomarkers Together for a Better Understanding of the Nervous System.� Science, 15 Mar. 2018, www.sciencemag.org/features/2017/12/biomarkers-brain-putting-biomarkers-together-better-understanding-nervous-system.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Lower back pain is a condition that pretty much affects most of us at some point in our lives. Some find:
Sitting
Standing
Walking
can be painfully difficult or helpful, depending on the position or the activity they’re involved in.
Low back pain varies from person to person, yet there remains no consensus on the optimal way to diagnose and treat patients.
Lower back pain can be caused by a multitude of factors and can be difficult to diagnose the exact cause. However, there is an advanced method of diagnosing and treating individuals with musculoskeletal conditions/injuries.
TENS, Transcutaneous Electrical Nerve Stimulation in Physical Therapy. Therapist Positioning Electrodes onto Patient’s Lower Back
Successful treatment
Dividing patients with lower back pain into more similar groups based on the same factors that aggravate and alleviate the pain means that a more custom based treatment plan can be created.
The one size fits all method just doesn’t cut it. A more focused approach for every individual leads to better results.
Patients find that placing their bodies in certain positions and certain physical activities can:
Activate
Aggravate
Deactivate their back pain.
Patients also find the pain being either better or worse.
Understanding why sitting, standing, and walking can change the severity of low back pain can be helpful in diagnosis.
These are important cues that help to diagnose and treat low back pain.
People sit, stand, and walk all day. This is why so much research has been conducted on how these specific positions and activities contribute to low back pain.
Spine Anatomy
The alignment of the spinal column, from the skull to the pelvis, is S-shaped.
The cervical and lumbar spinal segments curve towards the front of the body, and so are lordotic,�while the thoracic spine curves towards the back of the body and is kyphotic.
The amount of curvature does not stay in one place and changes based on body position.
Compared to standing, sitting decreases lumbar lordosis by about 50%.
Changes in lumbar lordosis can relieve pain from certain forms of back pain but can aggravate others.
Picture The Spine Bending
Imagine you are holding a garden hose. Holding it vertically in front of you. The hollow part of the tube represents the spinal canal, the part of the hose facing you is the posterior spinal column, and the part of the hose facing away from you is the anterior spinal column.
Bend the hose in half. The hose on the outward-facing side of the curve will stretch out, while the hose on the inward-facing side of the tube will be compressed.
This exercise helps visualize that an object being bent will experience two forces, either:
Compression
Tension
Increasing lumbar curvature will compress the posterior column�and stretch out the anterior column vertebrae and discs.
Decreasing lumbar curvature will�stretch out�the posterior column and�compress�the anterior column. This is the basis of why certain body positions can relieve back pain symptoms for some people and make it worse for others.
Prolonged sitting, and especially if poor posture is involved, can cause overstretching of spinal muscles.
Arthritis can affect the joints.
The facet joints are posterior based structures and can become compressed with increased curvature. When the facet joints are the primary cause of back pain, patients usually find that sitting improves the pain, while standing and walking make it worse.
When the discs are the pain generator, sitting seems to aggravate the pain as there is more compression in the tissue.
With certain types of disc herniations, sitting can compress the disc to the point that the herniated tissue starts to press against a nerve root causing radicular pain or pain that radiates out to another area of the body like the legs. In this case, walking seems to alleviate the pain.
Spinal Conditions
Various spinal conditions definitely contribute to back pain and have the same presentations and alleviations.
Spinal Stenosis which means the narrowing of the spinal canal. Patients with this type of spine pain improve with leaning forward sitting. This is because the posture increases/opens the size of the canal�and decreases the nerve root compression.
Spondylolisthesis is when one vertebra slips forward over the vertebra right underneath. This is more commonly known as a slipped disc. There are various forms of this condition. But the pain occurs immediately when sitting, bending or walking and is usually relieved when standing still or in a neutral position for short periods.
Sacroiliac Joint Dysfunction comes from the sacroiliac joint becoming inflamed. Pain is usually aggravated when sitting or about to sit. especially when there is added weight on the affected side. This can be difficult to diagnose because of trying to figure out if it’s the hip or low back causing the pain.
Locating the Pain Generator
Sitting, standing, walking low back pain causes are different for everyone. But finding the root cause helps to prescribe the best treatment possible. A chiropractor uses many different techniques to relieve pain. These include:
Applied pressure
Massage
Hands-on manipulation (adjustments)
X-rays
MRI’s
Lab work
Health coaching
Chiropractors don�t prescribe medications, but they do recommend therapeutic, rehabilitative exercises and nutritional lifestyle counseling to help the body heal itself.
Low Back Pain Treatment El Paso, Texas
NCBI Resources
A chiropractor sets up treatment approaches based on the individual. This begins with the natural, non-invasive treatments before moving on to more aggressive techniques. And as an added bonus patient�s who have received chiropractic treatment have experienced improvements to their digestive health and have reported better and deeper sleep after a chiropractic visit.
Do you often feel that your energy levels drop in the afternoons? Do you often feel brain fog or have unclear thoughts and poor concentration? Do you often experience brain fatigue with chronic pain and inflammation? Diet and supplements are essential for overall well-being. However, fish oil omega-3s are a common supplement with a variety of health benefits. �
Fish oil is a well-known supplement that comes from fatty fish, such as sardines, anchovies, mackerel, and salmon. Fish oil has two types of omega-3 fatty acids, known as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), both of which are commonly used to support skin and heart health. Fish oil supplements can also promote brain health, especially when it comes to improving memory and mood problems like depression, as well as a variety of other health issues. The purpose of the following article is to discuss how the omega-3 fatty acids in fish oil may support and promote brain health. �
What Are Fish Oil Omega-3s?
Omega-3 fatty acids, best known as omega-3s, are polyunsaturated fats that offer most of the brain health benefits of fish oil. Fish oil has two main types of omega-3 fatty acids, EPA and DHA. These two omega-3s are found in cell membranes and these also have anti-inflammatory effects in the human body. They are also well-known for their fundamental roles in human development and heart health. EPA and DHA are found in fatty fish and fish oil. Because the majority of people do not eat the recommended amounts of fish, many people probably aren’t getting enough EPA and DHA in their regular diets. �
The human body can make EPA and DHA from another type of omega-3 fatty acid, known as alpha-linolenic acid (ALA). ALA is commonly found in a variety of foods, including walnuts, flaxseeds, chia seeds, canola oil, soybeans, and soybean oil. However, the human body can’t properly turn ALA into EPA and DHA, where healthcare professionals and researchers estimate that approximately less than 10 percent of the amount of ALA you eat is properly turned into EPA or DHA. Fish oil is a good option for people who don�t eat a lot of fish but are still looking to gain the health benefits of omega-3 fatty acids. �
How Do Omega-3s Improve Brain Health?
The omega-3 fatty acids EPA and DHA are essential for normal brain function during all stages of life. EPA and DHA play a fundamental role in the development of a baby�s brain. Several research studies have associated pregnant women�s fish intake or fish oil use with higher scores for their children on brain function and intelligence tests in early childhood. �
These omega-3s are also essential for the regulation of normal brain function throughout life. They are commonly found in the cell membranes of brain cells, preserving cell membrane health and facilitating communication between brain cells. �
When animals are fed diets without omega-3 fatty acids, the amount of DHA in their brains decreases, and they often demonstrate deficits in learning and memory. In older adults, decreased levels of DHA in the blood have ultimately been associated with smaller brain size, a prevalent symptom of accelerated brain aging. Clearly, it is essential to make sure that you get enough omega-3 fatty acids in order to avoid these detrimental effects on brain function and development. �
Fish Oil for Memory
The omega-3s found in fish oil play important roles in brain function and development. There are also claims that fish oil can improve brain function in people with memory problems, such as dementia and Alzheimer�s disease. Alzheimer�s disease affects brain function and quality of life in millions of elderly adults. That’s why finding a supplement or natural remedy that can help improve brain function in this population of individuals would be a major, if not a life-changing discovery. �
Unfortunately, a review of the research study found no compelling evidence that omega-3 supplements like fish oil can improve brain function in people with dementia and Alzheimer�s disease. However, several research studies suggest that fish oil supplements may improve brain function in people with more mild types of brain health issues, including mild cognitive impairment (MCI) or age-related cognitive decline. Although these types of brain conditions aren�t as severe as dementia and Alzheimer�s disease, they can still result in memory loss and sometimes other types of impaired brain function. �
One research study gave 485 older adults with age-related cognitive decline either 900 mg of DHA or a placebo every day. After 24 weeks, those taking DHA performed better on memory and learning tests. Similarly, another research study investigated the effects of taking 1.8 grams of omega-3 fatty acids from fish oil supplements daily for 24 weeks. The researchers found improvements in brain function in people with MCI but there were no benefits for those with dementia and Alzheimer�s disease. According to the research study, fish oil supplements may be most beneficial when people start taking them in the early stages of brain function decline. If you wait too long, fish oil may be of little benefit to brain health. �
Fish Oil for Depression
Finding treatments for depression and other mental health issues is still a public health priority. A recent review of several research studies concluded that taking fish oil supplements improved symptoms in people with depression. However, the greatest improvements in depressive symptoms seemed to occur in people who were also taking antidepressants. In addition, people seemed to experience greater effects when the fish oil supplement also had higher doses of EPA. �
It is still unclear how EPA and omega-3s help improve depressive symptoms. Researchers suggest that it may be associated with their effects on serotonin and serotonin receptors in the brain. Others have proposed that omega-3s from fish oil can improve depressive symptoms through their anti-inflammatory effects. Additional evidence suggests that fish oil may also help improve other mental health issues like borderline personality disorder and bipolar disorder. However, more high-quality research studies are required before the medical community can make definitive recommendations. �
Should You Take Fish Oil for Your Brain Health?
According to the evidence gathered from a variety of research studies, you may want to consider taking fish oil omega-3 fatty acids if you are experiencing mild memory loss, depression, or if you want to improve your overall brain health.�There are no official recommendations regarding how much omega-3s from fish oil you need to take to see benefits in brain function and mental health. The amounts of fish oil omega-3 fatty acids used in the research studies varied from each clinical trial. �
The US Food and Drug Administration has set a safe and effective limit for the intake of omega-3 fatty acid supplements to be at 3,000 mg per day. The European Food Safety Authority has set their recommendation a little higher, at no more than 5,000 mg per day. Taking 1,000 to 2,000 mg of omega-3 fatty acids from fish oil daily is likely a good starting point, which is under the recommended limit. People with depression should choose fish oil supplements with higher amounts of EPA. �
It is essential to read labels carefully when evaluating fish oil supplements. A 1,000-mg capsule of fish oil may have less than 500 mg of actual omega-3 fatty acids but this can vary for each brand. In general, fish oil supplements are considered to be safe and effective at dosages under those that were previously mentioned. Make sure you talk with a healthcare professional before taking fish oil omega-3 fatty acid supplements. Because research studies have reviewed their potential effects on blood clotting, this is especially important if you are taking blood-thinning medications or have an upcoming surgery. �
EPA and DHA are omega-3 fatty acids in fish oil that are fundamental for normal brain function and development. People with mild decline in memory or brain function and mood changes like depression may consider taking omega-3s from fish oil because these can improve symptoms and overall brain health. Although fish oil is typically praised for its benefits for heart health, it also has incredible effects on brain and mental health that are worth mentioning.�- Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Do you often feel that your energy levels drop in the afternoons? Do you often feel brain fog or have unclear thoughts and poor concentration? Do you often experience brain fatigue with chronic pain and inflammation? Diet and supplements are essential for overall well-being. However, fish oil omega-3s are a common supplement with a variety of health benefits. �
Fish oil is a well-known supplement that comes from fatty fish, such as sardines, anchovies, mackerel, and salmon. Fish oil has two types of omega-3 fatty acids, known as eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA), both of which are commonly used to support skin and heart health. Fish oil supplements can also promote brain health, especially when it comes to improving memory, mood problems like depression, as well as neurological diseases and other health issues. The purpose of the article above was to discuss how the omega-3 fatty acids in fish oil support and promote brain health. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine