Do you frequently eat processed foods that are bagged or boxed? Do you frequently eat fried foods? Do you have difficulty digesting foods? Do you experience constipation or inconsistent bowel movements? Do you have increased bloating or gas? If so, you may be experiencing SIBO symptoms. �
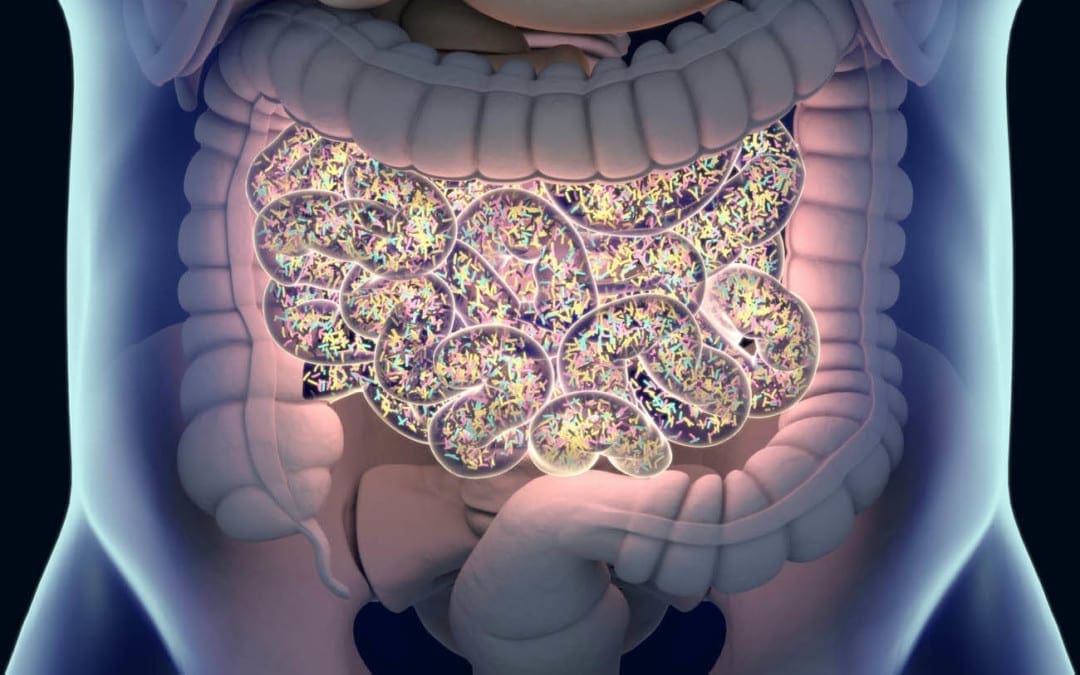
Small intestinal bacterial overgrowth (SIBO) is a serious health issue that happens when bacteria that generally grow in one region of the digestive system, such as the colon, grow in the small intestine, ultimately affecting the gastrointestinal (GI) tract. If left untreated, SIBO can commonly cause pain, discomfort, diarrhea, and malnutrition (because of the loss of nutrients), among other symptoms.�Proper nutrition can help decrease these harmful bacteria. �
Following the SIBO diet together with antibiotics can also help speed up recovery and ultimately help reduce uncomfortable symptoms. The purpose of the article below is to describe the benefits of following the SIBO diet as well as what foods you should and shouldn’t eat to help improve SIBO symptoms. �
Understanding the SIBO Diet
The SIBO diet involves gradually eliminating several types of foods in an attempt to help reduce inflammation in the gastrointestinal (GI) tract and help decrease bacterial overgrowth in the small intestine. In a variety of instances, the gradual elimination of sugars alone can help improve SIBO symptoms. �
Healthcare professionals recommend including a diet that is low in FODMAPs, or carbohydrates that can be difficult to digest and can become fermented by gut bacteria in the colon. When the digestive system is unable to break down carbs, these can sit in the gut and can cause SIBO symptoms, such as bloating and diarrhea. With SIBO, the bacterial overgrowth in the small intestine may ultimately start to ferment carbs too soon, causing a variety of symptoms. �
Foods You Should Eat for SIBO
As we will discuss further below, the list of foods you shouldn’t eat when you have small intestinal bacterial overgrowth (SIBO) can be considered restrictive, however, there are still several foods you can enjoy while following the SIBO diet. The SIBO diet includes foods that are high in fiber and low in sugar. �
Moreover, several foods can have low amounts of FODMAPs in smaller servings but these should still be limited or avoided because larger servings may increase the overall number of FODMAPs. Furthermore, several recommended types of foods for a SIBO, as well as a low FODMAP, diet include:� �
oatmeal
unsweetened cereal (with low FODMAP grains)
gluten-free crackers
rice or gluten-free noodles
quinoa
seeds
peanuts
several types of fruits, such as strawberries, blueberries, grapes, oranges
leafy greens
broccoli (heads only, less than 3/4 cup)
olives
potatoes
carrots
pumpkin
spaghetti squash and summer squashes
eggs
fish
meat
Foods You Shouldn’t Eat with SIBO
According to research studies, the low FODMAP diet has been demonstrated to safely and effectively help treat irritable bowel syndrome (IBS) and its associated symptoms. Patients with IBS also commonly have SIBO. Reducing or eliminating foods that are high in FODMAPs can improve digestive health. �
When reducing or eliminating FODMAPs as a part of the SIBO diet, healthcare professionals suggest focusing on the main categories, including: �
fructose, basic sugars frequently found in fruits and several types of vegetables as well as in honey and agave nectar,
fructans, a sugar substance or chemical found in many gluten products, fruits, several vegetables, and prebiotics,
polyols, sugar alcohol commonly utilized as a sweetener,
galactans, a substance or chemical found in several types of legumes, and
lactose, a sugar molecule frequently found in many dairy products.
Several types of foods which you may want to consider completely eliminating from your diet that has higher amounts of FODMAPs include: �
honey
agave nectar
high-fructose corn syrup
soda and other types of soft beverages
dried fruits
apples
asparagus
artichokes
peas
cauliflower
butternut squash
garlic
onions
beans
sweetened cereals
grains
barley
rye
flavored yogurt
ice cream
sausage
Evidence Findings of the SIBO Diet
Healthcare professionals utilize antibiotics as the main treatment approach for small intestinal bacterial overgrowth (SIBO) symptoms. However, research studies have demonstrated that dietary changes, such as limiting sugars and lactose, may also ultimately help reduce SIBO. The SIBO diet can be utilized together with probiotics and antibiotics. A 2010 research study also determined that probiotics can also help reduce SIBO symptoms. According to the research study, drinking more water while on the SIBO diet can also help reduce pain, discomfort, and inflammation. Make sure to talk to your doctor before making any dietary modifications or implementing a new treatment option. In addition, discuss all of the benefits and risks with your doctor or dietitian. �
The SIBO diet is a nutrition plan which temporarily eliminates high FODMAP foods while including a variety of low-FODMAP foods to help decrease bacterial overgrowth in the small intestine. The SIBO diet generally lasts anywhere between 2 to 6 weeks. Although it has been demonstrated to be a safe and effective treatment approach, the SIBO diet treats symptoms while it may not necessarily treat the underlying condition or disease. Conventional treatment options for SIBO shouldn�t be ignored. Talk to a healthcare professional before involving diet changes to any treatment plan. It�s also fundamental to mention that you should ultimately bring FODMAPs back into your normal diet when your SIBO symptoms improve. This can help prevent healthy gut bacteria loss. If your symptoms begin to worsen after implementing the SIBO or low-FODMAP diet, make sure to seek immediate medical attention. �
Small intestinal bacterial overgrowth (SIBO) is a serious health issue which usually occurs because of an underlying chronic health issue. Several common symptoms may ultimately help determine the presence of SIBO. Additionally, if the patient has a chronic condition or disease, such as celiac disease or Crohn’s disease, they should talk to a healthcare professional to develop a treatment plan, such as the SIBO diet. SIBO, or small intestinal bacterial overgrowth is treatable. If left untreated, this gastrointestinal (GI) tract problem can also cause dehydration and malnutrition. Patients should contact a healthcare professional immediately if they suspect they have SIBO so that they can begin treatment right away. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
�
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Do you frequently eat processed foods that are bagged or boxed? Do you frequently eat fried foods? Do you have difficulty digesting foods? Do you experience constipation or inconsistent bowel movements? Do you have increased bloating or gas? If so, you may be experiencing SIBO symptoms. �
Small intestinal bacterial overgrowth (SIBO) is a serious health issue that happens when bacteria that generally grow in one region of the digestive system, such as the colon, grow in the small intestine, ultimately affecting the gastrointestinal (GI) tract. If left untreated, SIBO can commonly cause pain, discomfort, diarrhea, and malnutrition (because of the loss of nutrients), among other symptoms. Proper nutrition can help decrease these harmful bacteria. �
Following the SIBO diet together with antibiotics can also help speed up recovery and ultimately help reduce uncomfortable symptoms. The purpose of the article above was to describe the benefits of following the SIBO diet as well as what foods you should and shouldn’t eat to help improve SIBO symptoms. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Anthony, Kiara. �SIBO Diet 101: What You Should and Shouldn’t Eat.� Edited by Natalie Butler, Healthline, Healthline, 16 Aug. 2018, www.healthline.com/health/sibo-diet.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
� XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
� Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
� Please call our office in order for us to assign a doctor consultation for immediate access.
� If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
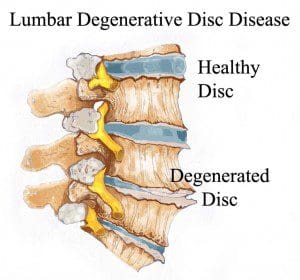
Q: Dr. Jimenez, I have a question about degenerative disc disease, and that is can it cause nerve pain in the feet? El Paso, TX.
A: Yes in certain cases, degenerative disc disease (DDD) can cause nerve problems with the feet.
Degenerative disc disease, specifically of the lower spine, can cause nerve pain to radiate and spread into the feet from the spine.
Degenerative disc disease
Is a spine condition that’s caused by everyday wear and tear of the spine can lead to significant loss of disc height.
A disc can also herniate and push on the nerves that flow into the feet, and cause:
Pain
Tingling
Numbness
The wear and tear of the spine combined with a herniated disc can pinch the nerves that go to the feet.
There is a condition known as foraminal spinal stenosis when the spinal foramen or the small opening between the bones of the spine begins to narrow and tighten so the nerves get compressed and do not allow signals and chemicals to flow properly.
This could explain the pain or other symptoms in the foot.
DDD can cause nerve problems in the feet, back and chronic back pain is the most common symptom of degenerative disc disease.
Common degenerative disc disease symptoms
The pain increases when:
Sit down for a long time
Bending
Lifting
Twisting
The pain decreases with:
Walking
Running
Lying down
Continually changing body positions
It’s important to remember that nerve issues with the feet are not always caused by spinal conditions, this could include
Depending on how severe the nerve problem is, there are a number of treatment options. These range from:
Chiropractic care
Physical therapy
Over-the-counter medication
Talk to a doctor or a chiropractor about the right treatment option for foot nerve pain. Whether it is caused by degenerative disc disease or some other condition.
These can help maintain a healthy weight, as being overweight puts extra pressure on the spine that leads to increased back pain. Consult with a registered dietitian or health coach to discuss the best foods for your diet.
Exercise
A training regimen that incorporates aerobic, strength and flexibility exercises that can help manage degenerative disc symptoms.
A personal trainer or sports chiropractor that has experience rehabilitating patients with spine conditions. They can teach exercises that can help relieve pain and other symptoms.
They can develop a custom physical therapy program
Regular chiropractic and physical therapy can help restore proper body mechanics, proper posture, as well as, avoiding positions that cause pain.
Surgery
Surgery is considered a last resort or if the condition is progressing and getting worse. If surgery is needed, your doctor will discuss the best treatment option for your condition.
Difference Foot Orthotics Make to *REDUCE FOOT PAIN* & Correct Posture | El Paso, TX.
NCBI Resources
Chiropractic focuses on restoring and maintaining overall health and wellness. Through the use of spinal adjustments and manual manipulations, a chiropractor can re-align the spine, and improve a patient�s strength, mobility, and flexibility.
Being pregnant is one of life’s many joys, however, with the added weight comes normal back pain that can lead to severe back pain that can lead to sciatica.
Expecting mothers have much to look forward to but when back pain and sciatica take hold, it can be exhausting, frustrating, and extremely painful. Women experiencing pregnancyback pain varies from woman to woman. To help prevent and alleviate back pain/sciatica, here are some answers as to how and why symptoms develop and what to do to make the pregnancy a joyful occasion.
Pregnancy Back Pain and Sciatica
Changes to the body throughout pregnancy affect more than its physical appearance.
The most common change is weight gain. Increased body weight, especially when bending puts pressure on the spinal discs. The most pressure is placed on the low back. Back, leg pain, and sciatica are common complaints.
Weight gain can cause piriformis syndrome and sciatica. The piriformis muscles help with thigh movement. Piriformis syndrome can develop if the muscle compresses the sciatic nerve, which causes a pinching or electrical shock feeling in the buttocks and back of the leg.
What some might not know is that as the uterus grows, the body’s center of gravity gets thrown off. What happens is the uterus expands inside the pelvis, and the spinal nerves in the low back that flow into the sciatic nerve gets compressed and irritated.
Hormones like relaxin, which is a hormone that relaxes the pelvic ligaments and helps prepare the mother’s body for birth. Relaxin loosens the ligaments in the other areas of the body, but primarily the joints in the pelvis, low back, and knees. When exercising or lifting objects it is easy to strain these relaxed areas. Therefore, move slowly, and avoid any sudden movements.
What Steps To Take
Work with a:
Doctor
Chiropractor
Midwife
Health care provider to keep body weight in check
Take note of posture:
Stand up straight
Shoulders back
Avoid leaning backward
Try a pillow:
A standard-sized pillow
Body pillow to help make sleeping comfortable
A pillow can be positioned between the knees and under the abdomen for support.
Prenatal yoga helps:
Stretch and tone muscles
Maintain flexibility
Improve balance and circulation
Relieves tension
Deep breathing plays a major role in yoga and is an added benefit as it can help expecting mothers relax during labor.
Simple cardiovascular exercises like walking or swimming can help keep weight under control and the body in shape. Ask a doctor or chiropractor if these types of exercises are right for you.
Prenatal massage is another option to help relieve pain and tension.
This type of massage eases:
Anxiety by stabilizing hormone levels
Back pain
Pelvic pain
Hip pain
Improves circulation and digestion
Helps reduce fatigue
A warm shower or bath can helps ease back pain.
Expectant mothers should avoid aromatic oils or aromatherapy candles like:
Basil
Juniper
Peppermint
Rosemary
Star anise
Some of these oils can cause contractions.
Acupuncture is another form of alternative therapy that can treat back pain and sciatica. Sterile, millimeter thin disposable needles are inserted into points on the body that are known as energy channels. The needles help to restore the balance of energy in the body. However, expectant mothers need to be past six months to receive this type of treatment as the energy flow can cause contractions.
Ergonomics At Work & Home
Expectant mothers should avoid:
Awkward postures
Over-exercising
Heavy lifting
Repetitive work
Especially during the third trimester.
The low back and leg muscles have to work harder to keep the body balanced. Just basic standing or walking can be a challenge. Swelling is common. Make sure to take constant breaks and full-body rest combined with elevating the feet can be very helpful.
Adding an ergonomic and adjustable chair with a lumbar support backrest and footrest is worth the investment. A chair like this can helps take the pressure off of the spine and working at a desk much more comfortable. It benefits to frequently stand and sit continually changing the body’s posture and working the various muscles, joints, and ligaments to keep the body loose. And it can be a form of exercise.
Light walking also helps to reduce any swelling through increased circulation.
Hopefully, you will not have to go through any kind of back pain or sciatica. But if pregnancy back pain and sciatica start to creep in, talk to your doctor, chiropractor, midwife, or health care professional first.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. We want to help you live a new and improved lifestyle. Over the last two decades, while researching and testing methods with thousands of patients, we have learned what works effectively at decreasing pain while increasing human vitality.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural and use the body’s own ability to achieve goals of improvement.
Back Pain During Pregnancy Treatment El Paso, TX Chiropractor
NCBI Resources
Keeping the body, including the spine, in proper alignment is vital to mobility, flexibility, and overall wellness of the body even when it is not pregnant. However, pregnancy puts specific stress on the body, creating certain needs that chiropractic care can meet. It is safe, it is effective, it is fast, and it works.
Do you feel irritable, nervous, shaky, or light-headed between meals? Do you have difficulty eating large meals in the morning? Do you feel fatigued after meals? Do you have sugar and sweet cravings after meals? Do you have an increased appetite?�If so, you may be experiencing early SIBO symptoms. �
SIBO, or small intestinal bacterial overgrowth, is a severe health issue that ultimately affects the small intestine in the digestive system. This gastrointestinal (GI) tract condition happens when the bacteria that generally grows in several different regions of the gut begin to grow in the small intestine. SIBO can commonly cause pain, discomfort, and diarrhea, among other symptoms. It can also cause malnutrition as bacteria utilize the human body�s nutrients.�
What are the Symptoms of SIBO?
Small intestinal bacterial overgrowth, or SIBO, is a serious condition that includes symptoms which can commonly affect the gut. These can include: �
pain or discomfort in the stomach
gas
bloating
constipation
diarrhea
cramps
indigestion
a general feeling of fullness
weight loss
What are the Causes of SIBO?
Small intestinal bacterial overgrowth (SIBO) is a severe health issue that is unfortunately not yet fully understood by researchers and healthcare professionals. According to research studies and clinical trials, however, this gastrointestinal, or GI, tract condition can ultimately happen when the small intestine is anatomically abnormal, due to pH changes in the small intestine, when the human body’s immune system isn’t functioning accordingly, or due to malfunctions in the muscular activity of the small intestine which can commonly cause food and bacteria to remain and not be removed from the organ. �
SIBO, or small intestinal bacterial overgrowth, is also commonly associated with a variety of health issues. These can involve the following, including: �
a stomach bug, known as viral gastroenteritis
celiac disease
Crohn�s disease
low stomach acid levels, known as hypochlorhydria
IBS or irritable bowel syndrome
gastroparesis
portal hypertension
nerve damage
cirrhosis
several gastric bypass procedures
surgical interventions which cause strictures or adhesions
What are the Risk Factors of SIBO?
Moreover, researchers and healthcare professionals have determined that an underlying chronic health issue and a previous surgery or surgical intervention that affects the gastrointestinal (GI) tract can be several risk factors of SIBO. Other wellness problems which can ultimately cause SIBO include: �
diabetes
scleroderma
hypothyroidism
Parkinson’s disease
HIV
narcotics or drugs/medications which slow down the digestive system
What is the Diagnosis for SIBO?
If you’ve experienced any of the SIBO symptoms mentioned above, see your doctor immediately. The doctor will ask the patient about their symptoms and medical history. The doctor will also perform a physical examination which may include palpating or gently feeling the patient’s abdomen. A qualified and experienced healthcare professional may also order additional blood, fecal, and/or any other tests to diagnose small intestinal bacterial overgrowth. �
A breath test is another common test utilized for the diagnosis of SIBO. Excess bacteria in the small intestine can cause the release of hydrogen and methane, two common gases which can be identified through a breath test. This test is non-invasive and can be performed in a doctor�s office. Before a breath test, the patient will need to fast overnight. During a breath test, the patient will first breathe into a tube. Then, the patient will take a specialized sweet drink provided by the doctor and they will breathe into several other tubes at regular intervals for 2 to 3 hours after taking the specialized sweet drink. �
If common tests for SIBO are inconclusive, the doctor may need to sample the fluid from the patient’s small intestine to see what bacteria is growing there. �
What is the Treatment for SIBO?
Common treatment approaches for SIBO, or small intestinal bacterial growth, can ultimately include a combination of antibiotics and diet modifications. �
Antibiotics
Treatment for SIBO first involves getting the bacteria in the digestive system under control. This is generally achieved by utilizing antibiotics, such as ciprofloxacin (Cipro), metronidazole (Flagyl), or rifaximin (Xifaxan). Further treatment for SIBO may also require intravenous (IV) therapy for nutrition and fluids if the serious gastrointestinal (GI) tract condition has ultimately caused malnutrition or dehydration, among a variety of other symptoms. �
Although antibiotics may help reduce the amount of bacteria in the small intestine, however, these will not always help address the underlying chronic health issues that caused the wellness problem in the first place. If the qualified and experienced healthcare professional determines that the patient’s SIBO is due to an underlying chronic health issue, the patient will also need to begin treatment for that wellness problem. Diet modifications may also help treat SIBO. �
Diet Modifications
Further research studies and clinical trials are still required to demonstrate if diet can cause small intestinal bacterial overgrowth (SIBO) but, many people with SIBO have reported feeling relief from their symptoms after diet modifications. Talk to your doctor before making any modifications to your diet. �
Furthermore, people with SIBO or other chronic health issues may only need to make small diet modifications to treat their symptoms. These can include: �
Eating a balanced and nutritious diet
Consuming minimal meals more often to prevent having too much food sit in the stomach
Avoid eating gluten products, if you have celiac disease or any other similar chronic health issues
The doctor may also recommend the patient to try an elemental diet to help treat SIBO. An elemental diet replaces food and drinks with several liquid formulas throughout an extended period of time. In one small-scale research study and clinical trial, approximately 80 percent of participants with SIBO had a normal breath test result following an elemental diet for 15 days. The researchers ultimately determined that an elemental diet may be a highly effective treatment approach for SIBO. However, further evidence is still needed. Talk to your doctor before starting an elemental diet and follow their instructions. �
Taking probiotics may also help restore the gut bacteria. A 2010 research study and clinical trial demonstrated that probiotic treatment can be more safe and effective for SIBO than taking antibiotics. However, a 2016 review determined that further evidence for the efficiency of probiotics in SIBO treatment was ultimately inconclusive. The best treatment approach for a patient with SIBO is to follow a qualified and experienced healthcare professional’s advice. �
SIBO, or small intestinal bacterial overgrowth, is a well-known and often severe health issue that generally occurs because of an underlying chronic condition or disease. Common symptoms may ultimately determine the presence of SIBO. In addition, if the patient has a chronic health issue, such as celiac disease or Crohn’s disease, they should talk to a doctor to develop a long-term treatment plan. SIBO, or small intestinal bacterial overgrowth is treatable. If left untreated, this gastrointestinal (GI) tract problem can also cause dehydration and malnutrition. Patients should contact a doctor immediately if they suspect they have SIBO so that they can begin treatment right away. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
�
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Madormo, Carrie. �Everything You Should Know About Small Intestinal Bacterial Overgrowth (SIBO).� Edited by Suzanne Falck, Healthline, Healthline, 14 June 2017, www.healthline.com/health/sibo#symptoms.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Chiropractic believes that optimal health comes from having a healthy nervous system, particularly a healthy spinal column.
Time, work, school, and everyday living means movement. And like anything that moves over and over again, at some point it’s going to get stuck or slip out of place. When the spine’s vertebrae become misaligned, pressure begins to press on the nerves that come out of the spinal cord. This is called a chiropractic subluxation and requires chiropractic realignment.
Chiropractors use a variety of techniques to mobilize the spinal discs so they can move freely along with returning them back�into place and in their proper positions.
These techniques are called spinal manipulations/adjustments.
During an adjustment, the vertebra is released or set free from the misaligned position and put back into the proper position in the spine’s column.
Adjustments allow the body to heal and maintain homeostasis.
Chiropractors are trained in a variety of adjustment techniques
Some are done by hand
Some use of specialized instruments
Ultrasound in physical therapy, treatment of shoulder muscles
Every patient is different, therefore a chiropractor will go through various treatment options with the patient, to choose the best technique and treatment plan for the patient’s condition.� Ask the chiropractor which technique they will be doing and how it works.
Adjustment Techniques
Chiropractors use�the following:
Toggle Drop
Using crossed hands a chiropractor presses down firmly on the areas that need adjusting and realignment. With a precise and quick thrust, the chiropractor adjusts the spine. This improves mobility in the vertebral joints.
Motion Palpation
This technique determines if the vertebrae are�freely�moving and with normal motion.
Lumbar Roll
The patient is on their side when the chiropractor performs a quick and precise thrust to the misaligned vertebra, that returns them to their proper position.
Treating Female Patient�s Spine
Release Work
Gentle pressure is applied with the fingertips which separate the vertebrae and opens them up.
Physiotherapist during an Achilles tendon treatment but the same technique applies to the spine
Table adjustment
Here a specialized table is used that drops incrementally with the adjustment. The chiropractor applies a quick thrust at the same time the table drops. This allows for lighter adjustments without twisting and turning that go with manual adjustments.
Instrument adjustments
This is considered the gentlest method of�spinal adjustment.
The patient lies on the table and the chiropractor uses an activator instrument to perform the adjustment/realignment/s.
TENS, Transcutaneous Electrical Nerve Stimulation in Physical Therapy. Therapist Positioning Electrodes onto Patient’s Lower Back
A chiropractic adjustment can be a great way to improve multiple areas of the body, along with improving overall health with non-invasive treatment. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers and premiere rehabilitation�providers to bring El Paso the top clinical treatments to our community.��Providing high non-invasive protocols is our priority.
Severe *Sciatica”* Pain Relief | El Paso, Tx (2020)
NCBI Resources
The nervous system, which consists of the�(spine/nerves/brain)�is the central headquarters of the body.�Subluxation removal helps the body function at its optimum level. Chiropractic adjustments�reduce pressure on the nerves and ease the flow of communication and signals going back and forth.
Q: Recently diagnosed with a bulging disc at C5-C6, is there anything I can do at home to relieve my pain?
� El Paso, TX.
A: Great question because anyone that has woken up with a stiff neck can relate. This is the most common area of herniation in the neck. It is highly susceptible to regular wear and tear but poor neck posture, like looking down at a phone for too long and improper motion mechanics can also be a cause.
Taking care of yourself without having to go to the doctor is very important and it is critical to learn proper healing methods, and techniques.
Healthcare professionals will say that most of the healing takes place at home.
There are various ways to reduce pain at home, but remember that there is a point when symptoms do warrant professional medical attention.
Good news
Bulging and herniated discs typically heal within six months � and less than 10% ever need surgery.
Non-surgical treatment for cervical bulging discs is usually enough to relieve pain and the best part is that you can do many of these treatments yourself.
Under chiropractic/therapist supervision, these treatments can be utilized at home or with the assistance
Cervical pillow
A proper pillow will help improve the quality of sleep and also give the neck proper support and position to heal.
Herbal remedies
The natural approach to medications is also welcome. There are plenty of herbal supplements to help relieve pain. There is capsaicin cream, that you can apply and helps reduces pain.
Ice and heat therapy
Ice should be applied in a bag or towel for 15-20 minute intervals, two or three times daily. Heat treatment comes in the later stages of the therapy but follows the same on-off interval technique.
Over-the-Door Traction
This therapy is very effective in helping relieve pain and muscle spasms. Your head and neck are attached to a harness. This is connected to a rope that is connected to a pulley system that goes over a door at your home. Then while sitting, leaning back, or lying down you go through the exercise.
Motion exercises
These exercises help the neck recover its full range of motion. This prevents stiffness from setting in and also helps strengthen the muscles in the neck. A therapist or a chiropractor can show a variety of exercises depending on the area of injury/stiffness.
However, if the pain does not go away a physical therapist/chiropractor can be your best option. Passive physical therapy includes:
Ultrasound
T.E.N.S electrical nerve stimulation
Mild neck traction
These treatment options are non-invasive and effectively help manage pain. It’s always important to remember that if your pain continues or starts to become worse tell your doctor and get medical attention.
Chiropractic Alignment
If the pain continues, then you may be referred to a chiropractor for spinal alignment.
Chiropractors are experts at treating neck conditions.� Aligning the cervical segments of the neck is a must as the injury can return if the cervical discs are not in proper alignment or even worsen. Chiropractic treatment can give relief and also stop cervical spine degeneration.
*Neck* Pain Chiropractic Care El Paso, Texas
NCBI Resources
People have a 70% likelihood of developing neck pain lives and neck pain is an important issue affecting economic productivity in modern society. Neck pain is a work-related musculoskeletal disorder that can occur when a person works for a long time or at a high intensity. An increase in the number of individuals visiting hospitals with pain in the neck, upper extremities, and the head as a result of excessive tension. Home therapies can help reduce pain.
Many research studies have arguably analyzed how gluten can affect the nervous system. However, people with celiac disease and non-celiac gluten sensitivity have demonstrated a variety of symptoms, ranging from headaches and brain fog to autoimmune disease. Moreover, brain health issues, such as anxiety, depression, and migraines, among others, are also common symptoms in people with gluten sensitivity or intolerance.
Gluten ataxia, a severe autoimmune disorder, affects a small percentage of the population. Evidence suggests that brain health issues, such as schizophrenia and bipolar disorder, may also be affected by gluten. In the following article, we discuss several common gluten-related brain health issues.
Brain Fog, Headaches, Migraines, Insomnia, and ADHD
Many people with brain health issues like celiac disease as well as gluten sensitivity or intolerance understand the risks of consuming gluten. But, if they do eat gluten, many people report feeling that their brains “cloud up” and they feel less efficient, even clumsy. This brain health issue, known as brain fog, requires further research studies, however, it’s another common symptom associated with celiac disease and gluten sensitivity or intolerance.
Attention deficit-hyperactivity disorder (ADHD) is yet another common brain health issue in both adults and children. Headaches and migraines are also commonly reported as celiac disease symptoms and gluten sensitivity or intolerance symptoms. These symptoms may ultimately cause insomnia.
Anxiety and Depression
Research studies demonstrate that people with celiac disease experience anxiety and depression. People that don’t have celiac disease but who do have gluten sensitivity or intolerance also report experiencing anxiety and depression although the connection between the brain health issues is unknown. Researchers believe that gluten-related intestinal permeability, or leaky gut, may cause nutritional deficiencies that cause anxiety and depression.
However, that doesn’t necessarily explain why people with non-celiac gluten sensitivity or intolerance also experience anxiety and depression. Several gluten sensitivity or intolerance experts like New Zealand pediatrician Dr. Rodney Ford have hypothesized that gluten directly affects the brain and leads to the development of these brain health issues. Regardless, you’re far from being alone if you experience gluten-related anxiety and depression symptoms.
Schizophrenia and Bipolar Disorder
Many research studies suggest that gluten may be associated with two very severe brain health issues: schizophrenia and bipolar disorder. In schizophrenia, decades of research studies have shown that eliminating gluten from the diet of schizophrenics can help with the brain health issue. Research studies have ultimately demonstrated that a gluten-free diet can be beneficial for people with schizophrenia, but further research studies are needed.
In bipolar disorder, research studies have shown that people with celiac disease and gluten sensitivity or intolerance may experience the brain health issue. A research study on the levels of antibodies to gluten in the blood of people with bipolar disorder found increased levels during a manic episode.
Autoimmune Disease
When gluten consumption causes your own body to attack its own cells and tissues, you suffer from a gluten-related autoimmune disease. There are three common gluten-related autoimmune diseases: celiac disease, dermatitis herpetiformis, and gluten ataxia. In gluten ataxia, the immune system attacks the cerebellum, the region of the brain responsible for coordination. In many circumstances, the brain damage is irreversible, however, a strict gluten-free diet can help stop the progression of the autoimmune disease. Many people with gluten sensitivity or intolerance may also experience similar symptoms.
Celiac disease and gluten sensitivity or intolerance can ultimately lead to a wide variety of brain health issues and neurological diseases. However, in many circumstances, people can tremendously reduce or even resolve their gluten-related brain health issue symptoms by following a strict gluten-free diet.
Gluten intolerance or sensitivity is described as the human body’s inability to digest or break down the gluten protein found in wheat and a variety of other grains. This health issue can ultimately range from a mild or moderate intolerance or sensitivity to full-blown celiac disease, a severe autoimmune disorder related to gluten intolerance or sensitivity. Additionally, research studies have demonstrated that people with gluten intolerances or sensitivities may also develop brain health issues or neurological diseases. Talking to a naturopathic doctor or functional medicine practitioner can help determine if you have a gluten intolerance or sensitivity. Avoiding gluten altogether can ultimately help improve your overall health and wellness. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
[wp-embedder-pack width=”100%” height=”1050px” download=”all” download-text=”” attachment_id=”52657″ /]
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez
References:
Anderson, Jane. �How Gluten Can Have a Damaging Effect on Your Brain and Nerves.� Verywell Health, Verywell Health, 20 Nov. 2019, www.verywellhealth.com/gluten-related-neurological-symptoms-and-conditions-562317.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900. For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download* All of the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine


 �
� �
�