As doctor Mark Hyman says, “Food is medicine. You can not find anything in a bottle that is more powerful than what you put on your fork”. The best diet for pain relief depends on the individual but ultimately comes down to reducing inflammation and restoring the healthy bacteria in the gut.
Methylation Diet
Methylation is a natural process in the body that controls the replication of DNA. In turn, methylation is responsible for the aging of each cell and has been thought to play a role in the onset of, or a lack of, chronic disease.� Methylation is also responsible to control the unhealthy compound that can damage blood vessels called homocysteine, recycles molecules for optimal detoxification and keeps inflammation under control. The methylation diet focuses around adding foods into the diet that enhance the role in DNA methylation. The process behind methylation is to remove the obstacles the body faces that drain the natural methylation process while providing the body with a wide variety of nutrients for optimal balanced activity. This results in a gut that is not as irritated, leading to less gut inflammation and ultimately will reduce inflammation in the overall body, leading to less pain.
An example of breakfast following the methylation diet provided by Lara Zakaria found in the book “Everyday MDL” is Cranberry-Apple- Cinnamon Oatmeal. This meal consists of steel-cut oats, coconut oil, fresh cranberries, a crisp apple, and honey for topping!
Avoiding Nightshades
What is a nightshade?� A nightshade is a vegetable that contains Alkaloids, which are substances containing nitrogen. These nightshades are thought to increase inflammation in the gut and lead to other autoimmune diseases. Many nightshades are a rich source of nutrients and do not cause people issues. However, to reduce overall pain in the body,� avoiding these foods reduces inflammation and offers health benefits.
Examples of common nightshades to avoid include Eggplant, Peppers, Potatoes, and Tomatoes.
Gluten-Free
Joint pain and inflammation are two common symptoms when it comes to celiac disease. Celiac disease is when an individual has an autoimmune response to gluten. Gluten is the protein commonly found in wheat. For those with celiac disease, gluten does not get properly digested, causing damage to the small intestine and the inability to absorb the nutrients.
This leads to painful stomach aches, diarrhea, and inflammation of the intestines and tissues. This causes problems inside the gut, and outside the gut. By reducing gluten in the diet, patients see a reduction of depression, joint pain, headaches, and skin rashes. With the reduction of these symptoms, comes the reduction of pain. The less inflammation being caused from the inside of the body, the less pain felt by the patient.
Phytonutrient Diet
Phytonutrients come from plants. The word “Phyto” refers to the plant, in Greek. Phytonutrients are not essential to live, but they have been shown to help prevent disease and reduce inflammation by providing the body with natural compounds that are produced by plants.
Phytonutrients offer the body antioxidants, carotenoids to support immune health, flavonoids to aid in healthy cell communication that lead to detoxification, and glucosinolates to help eliminate toxins.
On top of all these diets, one of the best things to aid in pain relief is to add all-natural simple supplements into your daily lifestyle. Fish oils will help the body’s cardiovascular system as well as support healthy mental function as well as glucose and insulin metabolism.
Pre/Probiotics will feed the healthy bacteria along with providing a natural immune response, bowel regularity, and lactose digestion.
Vitamin D is a vitamin that almost everyone is deficient in. By adding this supplement to your diet it will support bone health and cardiovascular health.
Curcumin is derived from Tumeric. This is an all-natural supplement that provides antioxidant and cell activity, supports the joints and helps to relieve minor pain, provides the health of organs and their systems while promoting healthy cell growth.
Eating healthy and providing your body with a diet to allow it to work optimally, does not have to be repetitive, plain or boring. These foods and diets allow individuals to enjoy their life and their foods while ultimately reducing inflammation and experiencing pain relief. -Kenna Vaughn, Senior Health Coach
*The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request.�
References:
Hodges, Romilly. �Breakfast.� Everyday MDL Recipes for the Methylation Diet & Lifestyle Program for Optimal Genetic Expression, edited by Kara Fitzgerald , p. 35.
Musculoskeletal health is one of the highest costs in healthcare today.
There are 1 in 2 Americans that have a musculoskeletal condition. And the need for support along with body alignment is at an all-time high.
In today’s world surveys found that Americans wear two to three pairs of shoes during the week.
However, these shoes are not made to support:
The body
Fit the feet
And can be dangerous to general musculoskeletal health
Health and freedom from pain are important factors in a healthy quality of life. But it starts with proper support for the body that begins from the ground up.
Many believe that to get proper support all you need is to buy top shoes that are optimized with athletic properties. While athletic shoes are definitely more comfortable they do not provide adequate support for the body and can affect posture and the body’s alignment.
The shoes out on the market today, whether athletic or dress are more about fashion than function. These shoes are designed based on sample sizes. Shoe companies use for men a size ten and for women a size eight for their sample. Then material is�added or subtracted to create the larger or smaller sizes.
The resultant shoes are designed to fit and provide optimum performance but are not customized to conform to each individual’s unique feet.�
Shoes are designed to protect feet from the elements and adapt to various activities.
They are not designed to handle the additional forces necessary to support the body.
Take a look at the extensive wear patterns on your shoes and see if there are imbalances in the feet. If there are areas that are really worn/flattened out then there can be severe pronation taking place. This is one serious reason to look into foot orthotics,
Not to worry, as excessive foot pronation affects everyone.
While at school, work or conducting daily chores is when individuals pronate and while wearing shoes with no arch/spine support.
Pronation in the feet combined with shoes that don’t fit with no support has a negative impact on posture and alignment.
With no sufficient support, the body reverts to the imbalanced state. With continued use and not addressed will cause pain in the:
Knees
Hips
Back
Neck
And unfortunately, most of us ignore and even power through the pain caused by the poor fit and lack of support from these shoes.
Reasons to Use Custom Orthotics
The feet make up the body�s foundation. Just like a house, problems with the foundation will create problems throughout the structure over time. Therefore if the foundation is remedied properly then the other issues remedy themselves or are easier to treat because the feet are already taken care of.
Feet problems/issues create back problems. Fixing foot problems will make a difference with the back pain treatment plan.
Individuals think their feet are just fine. However, they don’t know what problems are in the background waiting for the worst moment to present. Imbalance/dysfunction is a silent issue that can ripple into many problems along with pain in the spine.
Feet are as unique as fingerprints. Custom orthotics will make a vast difference between the right and left foot and accommodate the body to achieve its full potential.
Custom orthotics are built just for you. Based on a high-resolution 3D scan of your feet, that is sent to a Foot Levelers� team of technicians, who create your 100% unique, tailored foot orthotic/s.
Don�t be fooled by over-the-counter knock offs. These are mass-produced insoles that can worsen pain. And while most cases of back pain respond well with Chiropractic care, adding custom foot orthotics will enhance the effectiveness of the treatment with no need for surgery or side effects from medications.
Your feet and your body will thank you and will improve health by maintaining proper posture, combined with full-body support to achieve optimal quality of life.
How to eliminate Back Pain naturally | (2020) Foot Levelers |El Paso, Tx
NCBI Resources
When there are problems with the feet, it can cause problems through the legs and all the way to the spine. This can cause the ankle to pronate, meaning it rolls inward. This alters the way the�bones of the foot�line up which extends through the tibia, or shin bone.
This can cause a condition called knock knees and it can change the way the entire body is aligned. This puts the body out of balance, destabilizing the spine, and can even cause the pelvis to tilt to one side or the other. When you are walking or standing, the stress caused by the misalignment can create a domino effect, causing or contributing to low back pain.
A trigger point is a knot or bundle of stiff spine muscle tissue that you can’t move or relax, and when touched pain spreads to the neck, shoulders, and upper back.
Pretty much everyone can relate to this type of pain in the neck or what is known as myofascial pain syndrome when several of these trigger points are grouped.
How to ease the pain and prevent it
Trigger points can form in muscles all over the body. Myofascial pain syndrome in the neck happens when trigger points develop in the muscles of the shoulders, upper back, and neck.
A Trigger Point
Trigger points have a unique connection to America. They were first identified in the 1940s by Janet Travell, MD, who was John F. Kennedy’s doctor. JFK had severe chronic back pain and had trigger point injections to ease the pain.
A trigger point is a sensitive area within the muscles. They are typically described as knots and feel like a bundle of tense, contracted muscles that twitch and spread pain when touched. The spreading pain is known as referred pain. Example: Trigger points in the shoulder send pain into the neck.
Trigger points cause muscles to stress and to contract. This results in:
Muscle weakness
Numbness
Limited muscle movement
Formation of Points in The Neck
They are usually caused by mechanical factors (factors that strain or stress the muscles).� Spinal trauma, like whiplash from an automobile accident or sports-related injury, can create trigger points.
They also develop through repetitive actions and routine everyday chores that can hurt the spine over time.
Straining the neck muscles from poor posture for extended times like craning the neck while working on a computer, carrying a heavy bag that stresses the muscles of the neck, upper back, and shoulders.
Trigger Points vs Fibromyalgia Tender Points
Trigger points do get confused with tender points of fibromyalgia. Trigger points and tender points are both defined as local areas of pain but are not the same.
Tender points do not cause referred pain the way trigger points do.
Tender points are symmetrical meaning that they are on both sides of the body. Whereas trigger points do not follow a symmetrical pattern.
But it can become complicated because individuals with fibromyalgia can have both tender points and trigger points. People with fibromyalgia can also have myofascial pain syndrome.
Trigger Point Diagnosis
Trigger points are a regular cause of different types of spine pain, that can range from neck pain to low back pain. However, doctors are still trying to understand how trigger points produce referred pain. This is why diagnosing trigger points can be difficult for doctors.
They are complex because they are easy to pinpoint but difficult to diagnose. As they can directly cause muscle pain but they can mimic other pain making conditions exactly the way Myofascial pain and fibromyalgia get confused.
Jaw pain
Earaches
Toothaches
These types of pain that do not go away could be caused by trigger point/s in the neck.
Individuals with chronic neck pain that don’t seem to have a cause, could be trigger points. A doctor will refer you to a physical therapist, chiropractor or another spine specialist to conduct an examination for trigger points.
Treatment
Treatment can range from home remedies, chiropractic care, physical therapy and if severe muscle injections. There is no one treatment that works, as everyone and their injuries are different, meaning that various treatment options need to be looked into.
Home
Before starting any home therapy, discuss it with a trained professional like a doctor, chiropractor, massage therapist, or physical therapist to identify the location of the trigger point to effectively treat it.
Treated with massaging the area but can be tough with hard-to-reach places in the upper back. If unable to reach the point slowly and gently roll over a foam roller, golf or tennis ball for quick relief.
Massage
Massage therapists are trained in relieving muscle pain. Deep tissue massage can relieve an irritated area. Regular massage sessions can reduce pain and prevent the points from reemerging.
Physical therapy
Physical therapy treats trigger points in different ways, this includes:
Massage
Heat
Electrical stimulation
Ultrasound
A cooling spray is applied followed with stretches to relax and relieve the contracted muscle/s
Medications
Muscle relaxants can be used to reduce the symptoms and relieve pain. However, these meds can have all kinds of side effects, and become habit-forming, so use should be limited and in conjunction with a proper chiropractic/physical therapy treatment plan.
Injections
If the pain continues despite the non-surgical treatments or worsens, then your doctor could recommend trigger point injections. Injections are late-stage therapy. Doctors want to avoid patients becoming dependant on injections and will prescribe injections with an exercise, chiropractic/physical therapy program for maximum relief and effectiveness.
Overall Health
The majority of people have felt tight muscles around the neck. Utilizing proper posture and healthy spinal mechanics can prevent trigger points and myofascial pain syndrome.
Our services are specialized and focused on injuries and the complete recovery process.�Our areas of practice include�Wellness & Nutrition, Chronic Pain,�Personal Injury,�Auto Accident Care, Work Injuries, Back Injury, Low�Back Pain, Neck Pain, Migraine Headaches, Sports Injuries,�Severe Sciatica, Scoliosis, Complex Herniated Discs,�Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, and Functional Medicine Treatments.
�Neck Pain and Chiropractic Treatment El Paso, Texas
NCIB Resources
Many people who have trigger points or myofascial pain syndrome in their spine have knots and tightness throughout their back and neck. To prevent myofascial pain syndrome one needs to practice a healthy lifestyle that promotes good spine health. Stretching and exercising regularly can help keep stress under control and prevent tension from building up, which makes it harder for trigger points to activate and cause pain.
Q: Can back pain be hereditary and run in the family? I’m 24 and have chronic low back pain. But I found out that my mother, grandmother, and brother also have back pain. None of us were diagnosed with any type of spine condition. So I’m wondering if there is a hereditary/gene link or if it’s just a coincidence? El Paso, TX.
A: Back pain is a very common problem, and it is not uncommon that you and family members have back pain. Every year, 13 million people visit a chiropractor for chronic back pain. I can’t say without further study and research of your family whether the chronic low back pain is directly associated with your genes. But there are studies that support the connection between back pain and genetics.
Research in the past was difficult to rule out environmental factors like stress, smoking, and diet as the only cause of back pain. But today, there is evidence that shows genetics do have a role in back pain.
Doctors are finding that chronic back pain does show a significant genetic hereditary link. Specifically the development of low spine degenerative disc disease, which is a disc-related condition associated with normal wear and tear.
In fact, several twin sibling studies and genetic marker studies have researched this connection. Below are a couple of studies that stand out in the correlation between back pain and genetics.
Back Pain & Hereditary Genes Studies
A spinal study, which began in 1991, was a multidisciplinary, multinational research project on the cause of disc degeneration. The most significant findings were that there was a substantial influence of genetic/hereditary influence in lumbar disc degeneration.
It identified the specific genes that are associated with disc degeneration. However, environmental factors, work, sports, injuries, etc are also part of the condition, what the study found is that there is a connection of disc degeneration through genetic influences.
A study on genetics and lumbar disc disease found evidence that back pain could run in families. Specifically, lumbar disc disease could be inherited. The severity of the disease could not be determined or a patients’ response to various treatments. But it does suggest that genetics do play a role. Other findings include:
People that have lumbar disc disease were more likely to have family members with the disease.
The risk of inheriting the disease increased in both close and distant relatives.
Research is still ongoing to identify the exact genes that influence disc degeneration and back pain.
And as you said that you or your family have not been diagnosed with a spine condition,� this could be something to talk to your doctor or chiropractor about, along with creating a back pain treatment plan. For now, you can do physical therapy, chiropractic massage, CrossFit rehabilitation, etc to reduce and prevent back pain. Hopefully, it is a coincidence, but if it is genetics, not to worry as there is a treatment plan for that as well. But do not wait to make an appointment and let the pain get any worse.
Our team has taken great pride in bringing our families and injured patients only clinically proved treatment protocols. �By teaching complete holistic wellness as a lifestyle, we also change not only our patient�s lives but their families as well.� We do this so that we may reach as many El Pasoans who need us, no matter the affordability issues.
How to eliminate Back Pain naturally | (2020) Foot Levelers |El Paso, Tx
NCBI Resources
Lumbar spine disc herniation is a well-known type of injury that often causes impairing low back pain, however, it can also compress the nerve roots in the area and generate radicular pain and other symptoms along the lower extremities, such as altered sensations and muscle weakness.
Do you have difficulty digesting protein-rich foods? Do you have difficulty digesting starch-rich foods? Do you have difficulty digesting fatty or greasy foods? Do you experience abdominal distention after meals? Do you have abdominal pain and inflammation? If so, you may be having SIBO symptoms. �
Small intestinal bacterial overgrowth (SIBO) is a gastrointestinal (GI) tract health issue that can become a persistent problem if it’s not managed accordingly, especially if it’s ultimately left untreated. For many people suffering from chronic gas, bloating, constipation, and/or diarrhea, they may have also already had a diagnosis of irritable bowel syndrome (IBS). However, research studies have shown that one of the main causes of IBS may be SIBO. �
SIBO is a digestive health issue where there are too many bacteria in the small intestine. Bacterial overgrowth can also cause IBS. Although there are many treatment options for SIBO, one of the most important treatments for SIBO is doing everything we can to help keep SIBO from coming back. The purpose of the following article is to discuss how understanding the migrating motor complex (MMC) can help treat small intestinal bacterial overgrowth (SIBO). �
What is the Migrating Motor Complex?
The migrating motor complex (MMC) refers to the collection of electrical waves that occur in the gut. The MMC helps regulate several important functions of the gut, such as sweeping out the stuff we no longer need in there and moving it down to the colon where it can then be excreted by the human body. �
Phases of the Migrating Motor Complex
The MMC is how the digestive system eliminates waste from the human body. The MMC cycle includes four phases, including:� �
The first phase is a period of calmness that lasts 45 to 60 minutes where rare action potentials and contractions occur.
The second phase is a period of about 30 minutes where peristaltic contractions occur and gradually increase in frequency. Peristalsis starts in the stomach and continues throughout the small intestine.
The third phase lasts 5 to 15 minutes and it’s made-up of rapid, evenly spaced out peristaltic contractions. The pylorus stays open during these peristaltic contractions which allow many indigestible materials to pass into the small intestine.
The fourth and final phase is a period of transition between the contractions from the third phase and the inactivity from the first phase.
Gastric, biliary, and pancreatic secretion increases during the MMC to further with the digestion process as well as to help decrease bacteria in the gastrointestinal (GI) tract. Healthcare professionals believe that motilin, the enteric hormone, regulates the MMC. Because eating food can interrupt the MMC, fasting between meals is important to help complete the four phases. Moreover, the well-known �growling” sounds you generally hear when you are hungry may be the migrating motor complex performing its job functions accordingly, such as cleaning your bowels of waste and excessive bacteria. �
Migrating Motor Complex (MMC) Health Issues
If the migrating motor complex (MMC) isn’t working properly, the foods we consume may ultimately remain in the stomach and small intestine longer than what is generally considered to be healthy, which can make us feel a heaviness after eating or it can make us feel too-full, even if you’ve only had a small meal. Furthermore, a slow MMC can also cause bacteria to stay in the gastrointestinal (GI) tract for too long, which can also lead to SIBO. � Approximately 70 percent of people with SIBO also have MMC health issues. Research studies have shown that reduced MMC function may be associated with excess methane and/or hydrogen gasses produced by the excess bacteria in the gut. SIBO can also increase inflammation and intestinal permeability. �
Other research studies have shown that utilizing acid-reducing medications or an H. pylori infection can affect MMC function. Lack of exercise, grazing, and constipation can also affect MMC. Stress can also affect MMC function. Finally, thyroid problems and adrenal fatigue can also affect MMC function. �
Research studies have shown that people with IBS can frequently have decreased MMC function although researchers still don’t understand how these changes occur. Several researchers believe that food poisoning and other bacterial infections can affect the gut microbiome which then changes how the gut microbiome signals the MMC to start and stop. Eating inflammatory foods or foods that you�re sensitive and/or allergic to can also cause nerve damage in the gut. Subsequently, these damaged nerves then can�t properly signal the MMC to function accordingly, leading to SIBO and other health issues. �
Small intestinal bacterial overgrowth (SIBO) is a serious health issue which usually occurs because of an underlying chronic health issue. Several common symptoms may ultimately help determine the presence of SIBO. In addition, research studies have demonstrated that poor migrating motor complex (MMC) function, or the collection of electrical waves that help regulate several important functions of the gut, can ultimately cause SIBO and other digestive system health issues if left untreated. SIBO, or small intestinal bacterial overgrowth is treatable. Patients should contact a healthcare professional immediately if they suspect they have SIBO so that they can begin treatment right away. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
Do you have difficulty digesting protein-rich foods? Do you have difficulty digesting starch-rich foods? Do you have difficulty digesting fatty or greasy foods? Do you experience abdominal distention after meals? Do you have abdominal pain and inflammation? If so, you may be having SIBO symptoms. �
Small intestinal bacterial overgrowth (SIBO) is a gastrointestinal (GI) tract health issue that can become a persistent problem if it’s not managed accordingly, especially if it’s ultimately left untreated. For many people suffering from chronic gas, bloating, constipation, and/or diarrhea, they may have also already had a diagnosis of irritable bowel syndrome (IBS). However, research studies have shown that one of the main causes of IBS may be SIBO. �
SIBO is a digestive health issue where there are too many bacteria in the small intestine. Bacterial overgrowth can also cause IBS. Although there are many treatment options for SIBO, one of the most important treatments for SIBO is doing everything we can to help keep SIBO from coming back. The purpose of the article above was to discuss how understanding the migrating motor complex (MMC) can help treat small intestinal bacterial overgrowth (SIBO).
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Curated by Dr. Alex Jimenez �
References:
Albina, Victoria. �SIBO Begone: 5 Easy Ways to Keep Your SIBO From Coming Back.� Victoria Albina, Victoria Albina, 26 Mar. 2019, victoriaalbina.com/sibo/.
Brisson, John. �Migrating Motor Complex (MMC) and Digestive Health.� Fix Your Gut, Fix Your Gut, 13 Dec. 2014, www.fixyourgut.com/mmc-digestive-health/.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance. �
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with food sensitivities. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs. �
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders. �
Formulas for Methylation Support
� XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
For most individuals experiencing symptoms,� health care providers will run a few tests. For the most part, these tests come back normal or inconclusive. The patient is usually relieved, but not satisfied as they are still experiencing symptoms. The truth of the matter is, most tests practitioners run on patients are basic.
What Does That Mean?
It means that they are checking your levels and ruling out issues based on standard testing, but they are not diving deep into the cause of the symptom itself. Most individuals have a family history of one or more autoimmune diseases. An autoimmune disease is when the body misidentifies its own cells as a foreign body leading them to attack. These diseases can be triggered at any point in one’s life.
So What Do I Do Now?
Due to family history,� an ANA test can be run. Most of the time for patients still experiencing symptoms after the standard tests came back negative, the ANA comes back positive. However, a positive test does not always mean answers. This test can provide useful information but does not include a definitive answer as to what kind of autoimmunity a patient may have.
Using A Functional Approach
In modern/traditional medicine, most practitioners will suggest the patient is fine and that there is nothing to treat until they have been diagnosed. However, by using a more naturopathic and holistic approach, integrative practitioners can take these symptoms and use them to the patient’s advantage to help avoid a full-blown diagnosis.� The main reason this is effective is due to the fact that individuals do not just wake up one day with a new disease, but rather there are steps progressing in the background that eventually build up to a diagnosis if not treated.
Uncovering the underlying issue and using this stage in someone’s life as an opportunity to improve their quality of living is what functional medicine revolves around. By combining symptoms, previous lab results, and the patients declining quality of life, testing that relates to triggers of autoimmunity can be conducted. These tests will provide insightful information allowing the practitioner to not only treat the symptom but more importantly, to treat the cause.
Testing
There are multiple factors, including environmental that cause an autoimmune response to start to express. There are certain markers in the body that will shift before the onset of the autoimmune disease in which the environmental triggers will be shown.
Many labs are equipt to test for these markers and use top of the line technology. Some tests that evaluate these triggers that contribute to the progression of autoimmunity are:
The Gut Zoomerfrom Vibrant Wellness:The Gut Zoomer provides information and patient potential risks for intestinal permeability, IBS & IBD, SIBO, celiac, MS, obesity, diabetes, nutrition, viruses, fungal or yeast species, worm species, bile acids, SCFAs and more
The Food Sensitivity Panel from Vibrant Wellness:This test from Vibrant Wellness recognizes the specific antibody-to-antigen responses in commonly ingested foods. This panel tests for IgG and IgA sensitivity to the food antigens. This test is beneficial so patients do not have to an elimination diet, but rather have the test remove the guesswork and let results tell them what foods cause their body inflammation.
Dietary Antigen Test Plus from Dunwoody Labs:��This specific test from Dunwoody Labs allows the health care provider to see if there is an increased antibody response to food. Often times, the antibodies this screens for attack the body’s tissue leading to more autoimmune symptoms. This test looks at 4 separate antibody types IgE, IgG4, Total IgG, IgA, and complement.
Oxidative Stress Test from Dunwoody Labs:If the body is under large amounts of stress, this will cause an increase in the activity of T-Cells, thus keeping the body out of balance.
GI Microbial Assay Plus (GI-MAP� ) from Diagnostic Solutions: This is a stool test that not only analyzes but also evaluates the DNA of the actual organisms that are living in the gut. This allows the health care providers to see what is impacting health such as, mucus metabolism, methane production, T-Cells, and inflammatory LPS.�
Why Would I Want / Need This?
Preventative medicine provides the ability to keep up with, if not improve a patient’s quality of life while decreasing or avoiding the hard prescription medicine! By treating the underlying cause and not just masking the symptom, it allows individuals to truly feel better.
The number of individuals diagnosed with a disease that could have been prevented should earlier steps have been taken, is on the rise while their quality of life is declining. Feeling good should not be a delicacy, but rather a normal standard. With the use of integrative medicine, many grandparents will be able to play hide and seek and tag with their grandchildren, parents will be able to get through the day without as much fatigue and headaches, and children will be able to play, focus, and learn with fewer belly aches no matter the hour of the day. Integrative medicine not only utilizes tests to guide patients in the right direction but also gives patients tools and further educates them on exercise and nutrition components that will help prevent inflammation and stimulate good bacteria in their bodies to grow. – Kenna Vaughn, Senior Health Coach
*The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Resources:
�Basic Oxidative Stress.� Dunwoody Labs, 20 July 2018, www.dunwoodylabs.com/index.php/ox-stress/.
Burdette, Cheryl. �Is There Such Thing as Being Pre-Autoimmune.� 3 Dec. 2019.
�588 Dietary Antigen A, G, E, and C.� Dunwoody Labs, 17 Jan. 2019, www.dunwoodylabs.com/index.php/dietary-antigen-and-environmental-allergen-exposure-profiles/.
You might not think it, but weight lifting and spine strengthening exercises can help reduce back pain. Remember the point of this type of weight lifting is not to build up the muscles like a bodybuilder but is to develop:
Core strength
Spine strength
Body strength
The muscles in the back keep the spine moving and functioning properly. When the spine or abdominal muscles are weak this creates a higher probability of a back strain or injury. Having strong, healthy spine muscles are important because they function in maintaining correct posture, which in some cases, causes chronic back pain because of poor posture.
If�only one part of the body is strengthened like the back is not enough. Therefore strengthening the rest of the body is a must. These include the body’s core and leg muscles. Total body strength will reduce back pain and can help perform regular activities, like lifting heavy objects much easier, with more confidence and with a lesser probability of injury.
Spine strengthening exercises benefits
Most important reasons are they:
Prevents future back injuries
Stabilizes the spine
Helps the spine move properly
Help maintain correct posture
Increases muscle tone
Teaches correct body mechanics
Helps build bone this is especially beneficial for those with osteoporosis or at risk of developing it
A personal trainer or sports chiropractor can help start a spine strengthening regimen. They will teach:
Simple
Specific
Strengthening
Weight lifting exercises.
A physical therapist can also develop a custom weight lifting/strength�exercise�program for optimal spine health and for reducing pain.
Most workout regimens incorporate a combination of weight lifting with actual weights/exercise machines and strengthening exercises/calisthenics with the body’s weight as the resistance for maintaining a healthy strong spine.
Here are a few weight lifting and back strengthening exercises that can help decrease and prevent back pain.
Talk to a doctor or chiropractor before beginning any exercise program. Remember to listen to your body and stop right away if there is something off.
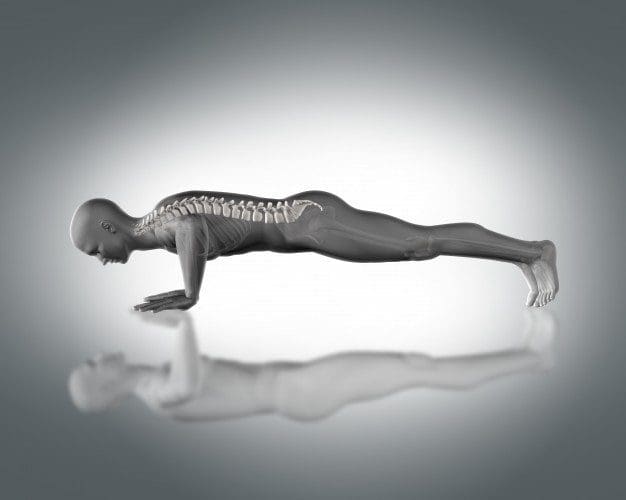
Push-ups
Push-ups help strengthen the:
Back
Chest
Arms
Core muscles
Your own body weight is the resistance.
To do this:
Position the body in a straight line from head to toe, the face looking down.
Hands should be wider than shoulder-distance apart. Walk the hands out so they are slightly higher than the shoulders
Keep the balance on toes and hands, with a straight back, lower the body to the floor by slowly bending the elbows until at a 90-degree angle.
Push up using arm upper back, and chest muscles.
Do 3 sets of 10 every day. As the strength increases do more reps.
Chest Flyes
Chest flies are excellent for building muscle in the:
Upper back
Chest
Dumbbells or a weight machine can be used for this exercise. To do this:
Lie on the floor with the knees bent and the feet flat on the ground.
Extend the arms out to either side of the body, and let them rest on the floor.
With a dumbbell in each hand, raise the dumbbells until they meet at the top at the same time, and keep a slight bend in the elbows.
Lower the hands to the ground, and repeat.
Do this exercise 15 times 3 times a week. With added strength add more reps.
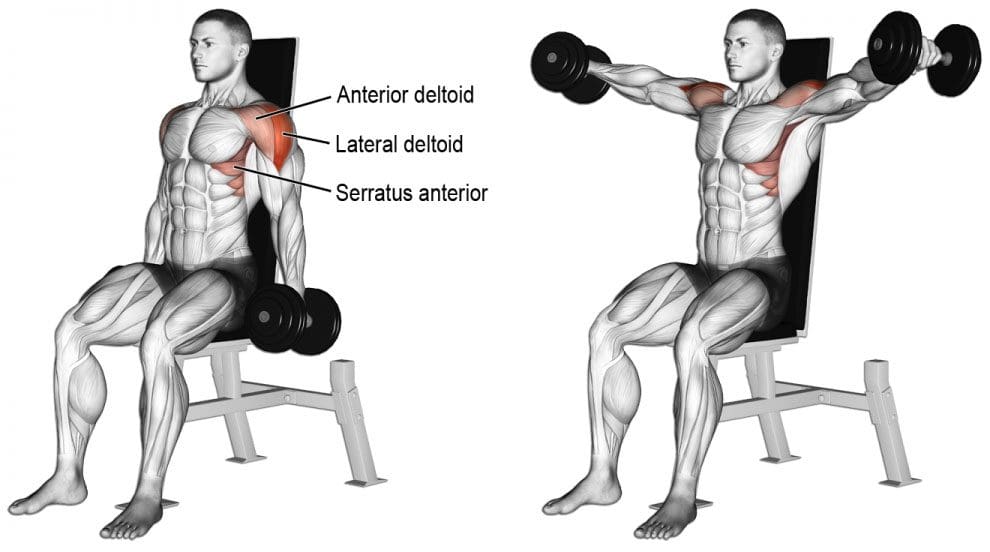
Lateral Raises
Lateral raises help strengthen the entire back. All that is needed is a set of dumbbells. To do this move:
Stand or sit with the feet equal hip-distance apart. Arms are at the side.
With a dumbbell in each hand and a slight bend in the elbows, raise the arms to the side until shoulder height. Keep the core engaged during the movement.
Once at shoulder height, slowly lower the dumbbells, and repeat.
Repeat this exercise 15 times 3 times a week. As strength increases add more reps.
These exercises should be performed slowly with a gradual build-up to more complex movements and adding more weight. Remember to breathe naturally. If you hold your breath during exercise, it can cause tension in the�muscles, which can worsen any pain or create new injuries.�Before adding weight or new spine strengthening exercises, talk to a doctor about exercising with back pain. They will let you know if there are certain movements or positions that should be avoided.
Weight lifting exercises done incorrectly can lead to more back pain and added injuries. If there is any pain while doing these exercises, stop and call a doctor, chiropractor or physical therapist right away.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
Back Pain Chiropractic Care | El Paso, Tx
NCBI Resources
It can be tempting to not exercise with a spinal condition. But remember that if there is no movement at all, you could make the pain worse. Knowing what your body can handle and sticking to a workable schedule, these healthy steps will relieve you and help with back pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine