Spinal decompression surgery could be a treatment option discussion with a doctor to relieve nerve pain brought on by a spinal condition or disorder. Everything to know about the procedures straight from the experts.
Spinal Decompression Surgery Types: Laminectomy or Laminotomy
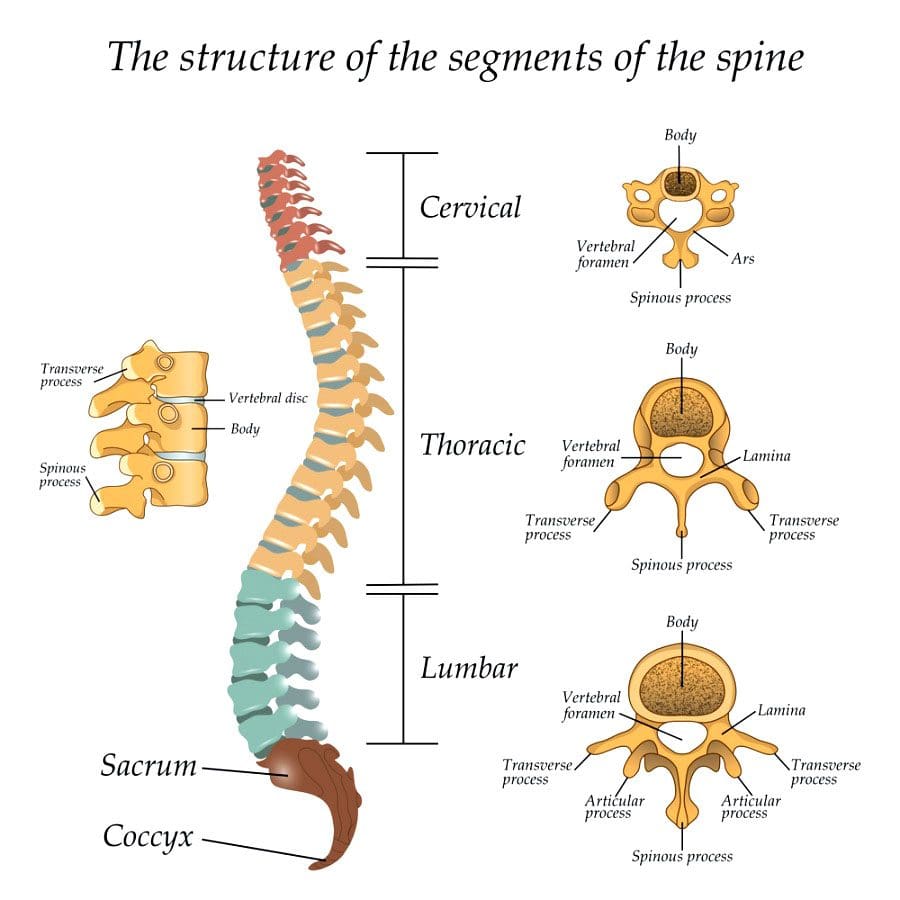
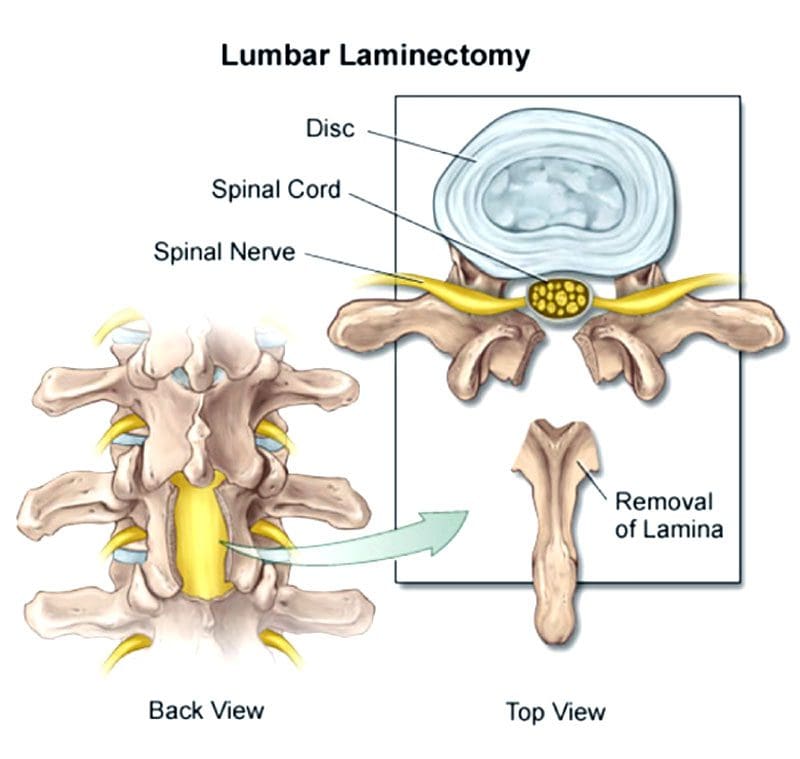
Both procedures involve the vertebrae�s lamina, which is an arch of bone that protects the spinal canal.
In a laminectomy, the lamina is removed almost entirely.
In a laminotomy, it is a partial removal.
Despite the removal, the large muscles of the back provide sustained protection for the nerves below. Therefore, the spinal nerves are still safe and secure following the procedures. Which one is right depends on the situation.
A laminectomy is usually performed to treat an arthritic condition of the spinal canal like spinal stenosis.
Laminotomy is used almost exclusively to remove a herniated disc.
A laminectomy removes more bone and sometimes the inner edge of the facet joint.
Ultimately, a surgeon will determine which of the two procedures is best for the individual’s needs and condition.
Decompression Surgery
Spinal stenosis or the narrowing of the spinal canal is usually caused by arthritis and overgrowth of the discs and joints. Similar compression issues respond well to non-surgical treatment. But sometimes surgery is necessary to treat uncommon but potentially severe cases. These include patients with:
Bowel or bladder problems caused by the pressure on the spinal nerves
Leg weakness that gets worse
Inability to walk or move for long periods and distance
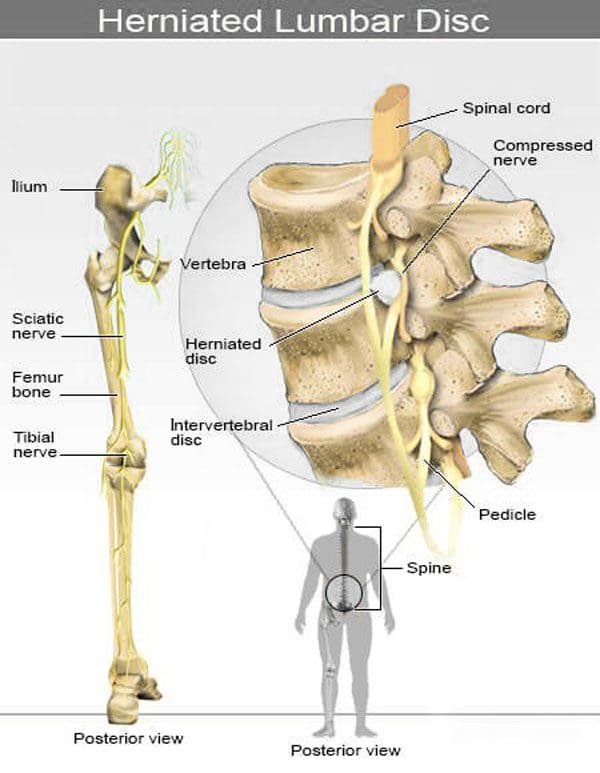
The objective of spinal decompression surgery is to create space around the spinal cord and surrounding nerves by removing the compressing structure/s. When the cord and/or nerve/s are compressed, physical and neurological symptoms are experienced down the nerve�s pathway. This includes:
Tingling
Numbness
Electric shock sensations
Radiating/spreading pain
Weakness
Once the compressed nerves have space to relax and move around symptoms subside.
Laminectomy process
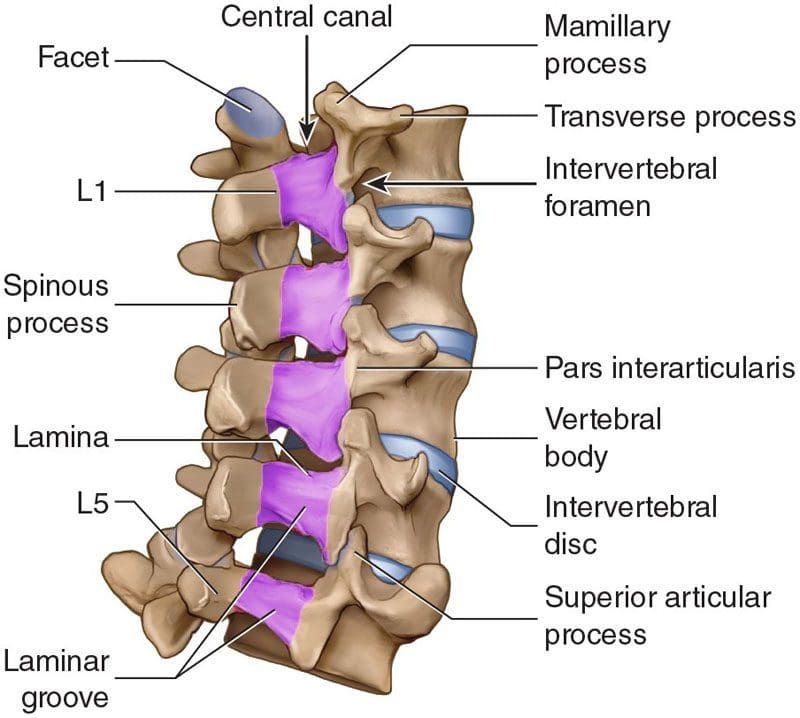
Lumbar laminectomy is the most common procedure to treat spinal stenosis in the low back.
It also helps treat herniated discs by allowing the surgeon to easily access the discs to repair any damage.
The surgeon removes the lamina and ligaments that have thickened and are causing problems to create more space in the canal.
The surgery enlarges the spinal canal so that pressure is relieved.
By removing the source of the pressure, the pain caused by the compressed nerves is alleviated.
An open laminectomy creates an incision of a couple of inches and exposes the spine.
The muscles of the spine and back are cut through to expose the bone.
Another technique that surgeons utilize is operating through a tube.
They’ve adapted these techniques to be able to decompress both the right and the left sides although they are only operating on one side.
Both procedures, minimal and traditional accomplish the same goals.
The difference is the minimally invasive approach involves one or more tiny incisions also known as skin punctures and small instruments designed to separate muscles and soft tissues instead of cutting through them.
The traditional approach requires a larger incision and instruments that retract, separate and cut tissues.
Laminectomy surgery
Laminectomies are performed under general anesthesia using a posterior approach/lying face down during the procedure.
It can be open or minimally invasive sometimes called a microlaminectomy.
In an open laminectomy, the surgeon makes an incision near the affected spinal area.
Once the incision is made, a retractor will move the skin, fat, and muscles to the side so the surgeon can access the spine.
Next, they remove or trim the lamina and thickened ligaments to enlarge the space surrounding the compressed nerves.
Once done, the retractor is removed and the incision is closed with sutures.
Minimally invasive surgery or MIS is performed using special instruments like endoscopes and tubular retractors.
These instruments allow for smaller incisions and less cutting.
They will also use special eyewear to have a detailed view of the surgical field.
Sometimes, the surgeon uses an endoscope or a microscope focused down the tube to perform the surgery.
The portion of the lamina is removed, along with any bone overgrowths/osteophytes and ligament tissue.
The tubular retractors are taken out so the soft tissue moves back into place, and the incision is closed with dissolving sutures.
Other spinal procedures performed alongside
Laminectomies and laminotomies are typically not performed together. However, a surgeon could perform both if the surgery affects multiple levels of the spine. They can also be combined with other spinal surgeries, that include:
Foraminotomy
A foraminotomy is also a decompression procedure. But instead of removing part or all the lamina, the surgeon accesses the nerves through the spine�s foramen or the passageway that nerves pass through on both sides.
Discectomy
This decompression surgery involves the removal of all or part of the damaged intervertebral disc and is utilized for herniated discs.
Spinal fusion
Fusion is often performed after spinal decompression surgery, as the space that was created by removing spinal structure/s can cause instability to the spine.
Candidates for spinal decompression surgery
Both are common procedures performed by neurosurgeons and orthopedic spine surgeons. Laminectomies are considered one of the most effective treatments for spinal stenosis and spinal canal issues like:
Tumors
Certain types of infections and abscesses
Spinal issues involving bowel/bladder dysfunction
The primary reason for laminectomy is spinal stenosis, most common in individuals over the age of 60.
Other considerations and conditions include:
Non-invasive treatments that don’t improve the condition that includes medication, massage, and physical therapy
Ask questions about the procedure to ensure you are comfortable with the operation. Here are some questions:
What are the risks associated?
Will the surgery relieve all symptoms?
Not having the surgery risks?
What is recovery like?
Recovery
Open or micro, recovery does take time. Following the doctor�s instructions carefully are essential to make a full, healthy recovery.
Individuals should be careful for about a month following the surgery. But does not mean laying down or being sedentary. Movement is crucial to recovery.
The patient should not stay in bed or lie on the sofa.
Wait a week or two before beginning physical therapy if necessary.
Most will have a weak core, poor posture, and poor body mechanics, the goal is to help develop and strengthen these areas.
Things to help with recovery include:
Ice/cold packs will help reduce swelling and pain.
Try not to sit for too long, as sitting is the least comfortable position after back surgery.
Body mechanic awareness means avoiding too much bending or lifting and using the right body mechanics when bending or lifting.
Especially before surgery. Quitting entirely or at least for at least six weeks before surgery will make recovery easier and healthier.
Losing weight
Speak with a doctor about weight. Just 5 pounds can make a significant difference during recovery.
Blood sugar
For individuals with diabetes, having an A1C under eight before surgery is ideal.
Every patient�s recovery is different. Recovery time depends on:
The complexity of the surgery
Personal medical history
Health issues
Recovery typically takes about two to four weeks after the surgery. However, it depends on the reason/s for the surgery.
Questions
Post-laminectomy syndrome
Post-laminectomy syndrome PLS also known as failed back surgery syndrome is a condition where an individual continues to have pain after surgery. Individuals still having symptoms after should speak with their doctor to determine the next phase of treatment.
How long before exercise?
Returning to the gym or getting into an exercise routine will take some time. It is important to follow the doctor�s recommendations and complete the full course of physical therapy before regular exercise activity can resume. Discuss workout plans with the doctor to determine the best timeline for the spine.
Full recovery?
Returning to some activity is possible around four weeks after surgery. Full recovery takes longer as each patient�s recovery is unique. Depending on the complexity of the surgery, most return to all activities within 6 to 9 months.
Body Composition Spotlight
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Pinched nerves occur when added pressure is applied to a nerve or set of nerves from surrounding tissues like bones, cartilage, muscles, or tendons. The pressure affects the nerve’s ability to function properly and usually causes pain, tingling, numbness, or weakness. A pinched nerve can occur at various sites in the body. Whether located in the neck, shoulder, arm, hand, back, or knees, they can lead to other debilitating conditions/injuries and permanent nerve damage if left untreated.
Pinched Nerves
The nerves are not actually being pinched but are being compressed. The added pressure on or around the nerve causes painful sensations that can also include:
Pinched nerves are nothing to dismiss. Individuals experiencing any of the above symptoms should get a proper diagnosis from a chiropractor.
Compression Goes Away By Itself
A compressed nerve can go away on its own if the pain has recently started or is not severe. In addition, home remedies like rest, heat, ice, and stretching can be utilized to help the compression subside on its own.
Length of Time It Takes for a Pinched Nerve to Heal
The length of time depends on the reason why the nerve is compressed and irritated. For example, some pinched nerves are brought on from poor posture and tight muscles. These can usually heal within 4 weeks. However, if the pain has been going on for some time, like more than 3 months, it will take longer, especially to identify the root cause/s and address them according to their severity.
Treatment Options
Chiropractic Adjustments and Massage
These two types of treatment/therapy highly complement each other. A chiropractor understands the importance of massage when it comes to healing and stress relief. Some cases of pinched nerves come from tight muscles and muscle spasms. Along with chiropractic adjustments, massage therapy is perfect for releasing and stretching the nerves back to their natural form.
Studies show that chiropractic massage therapy offers pain relief and also helps reduce any depression and anxiety that the pain symptoms can generate. In addition, comprehensive chiropractic treatment has been proven to be the best and fastest way to deal with pinched nerves.
Get More Sleep
Whenever the body is going through stress and needs repair, more sleep gives the body the time to heal itself. An extra hour of sleep also ensures that the injured area moves less. However, try to avoid sleeping on the stomach and make sure that the pillows being used provide plenty of support.
Warm/Hot Soothing Bath
Ice can really help lower swelling and inflammation, but if icing the area has not relieved the pain after 72 hours, it is time for a warm/hot bath. Warm water increases blood circulation, which delivers oxygen and nutrients to help heal and restore. In addition, heat relaxes the muscles of the body, which relieves pressure on the affected area.
Collagen Nerve Joint Repair
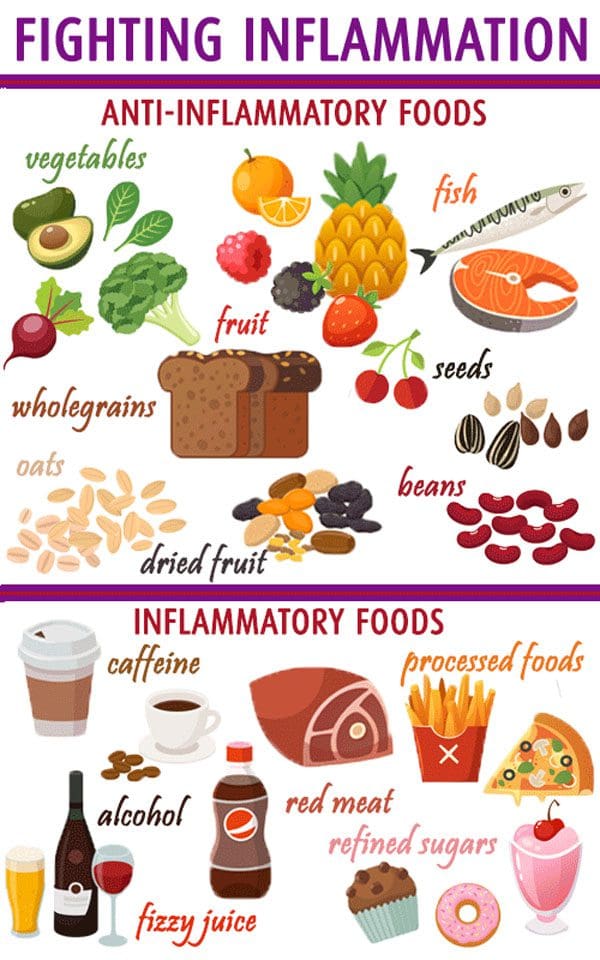
Collagen adds cushion to the spaces between the joints and bones while damaged tissues are being repaired. Collagen is the most plentiful natural protein in the human body. Supplements with glucosamine, chondroitin and hyaluronic acid can help and consume bone broth, a healthy collagen source. An anti-inflammatory diet can also help. Inflammation contributes to pain symptoms. Lowering inflammation lowers pain as well.
Proper Posture
Slouching and poor posture, whether sitting or standing, place added pressure/stress on the joints. When this goes on for long periods or when something traumatic occurs, a pinched nerve can result. A chiropractor will restore the body’s natural curvature. In addition, a chiropractor will discuss and show what proper posture should be and how to strengthen the core to maintain proper posture.
Other Treatment Options
Conventional treatments usually include:
Over the counter pain relievers
Prescription pain relievers for severe cases
Corticosteroids
Microdiscectomy spinal surgery
Regular surgery
Most individuals want to avoid any of the above treatment options. The body has a tremendous ability to heal itself. Chiropractic will reduce the amount of time that is required to heal a pinched nerve. It’s about treating the entire body, not just the symptoms. A customized treatment/recovery diet plan will be developed according to each individual’s needs. At Injury Medical Chiropractic and Functional Medicine Clinic, we encourage anyone experiencing any pain to call us right away.
Composition of the Body
What happens to the body when you stop eating
Not eating for a few hours causes glucose levels in the blood to drop, and insulin release stops. Alpha cells in the pancreas produce a hormone called glucagon that helps the liver break down the body’s stored glycogen, converting it back into glucose. The liver can also produce glucose by utilizing fats, amino acids, and waste.
If the body’s blood sugar levels drop, too low a condition called hypoglycemia happens. It occurs a few hours after eating when there is too much insulin in the blood or certain medications. This is why an individual might feel dizzy, shaky, anxious, or irritable when they have not eaten for several hours. Eating at least 15 to 20 grams of carbohydrates will reverse the symptoms.
Dr. Alex Jimenez’s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that directly or indirectly support our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Dubinsky RM, Miyasaki J.Assessment: Efficacy of transcutaneous electric nerve stimulation in treating pain in neurologic disorders (an evidence-based review). Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology.Neurology. 2010;74:173-176.
Shrier I. Does stretching help prevent injuries? Evidence-based Sports Medicine. Williston, VT: BMJ Books; 2002.
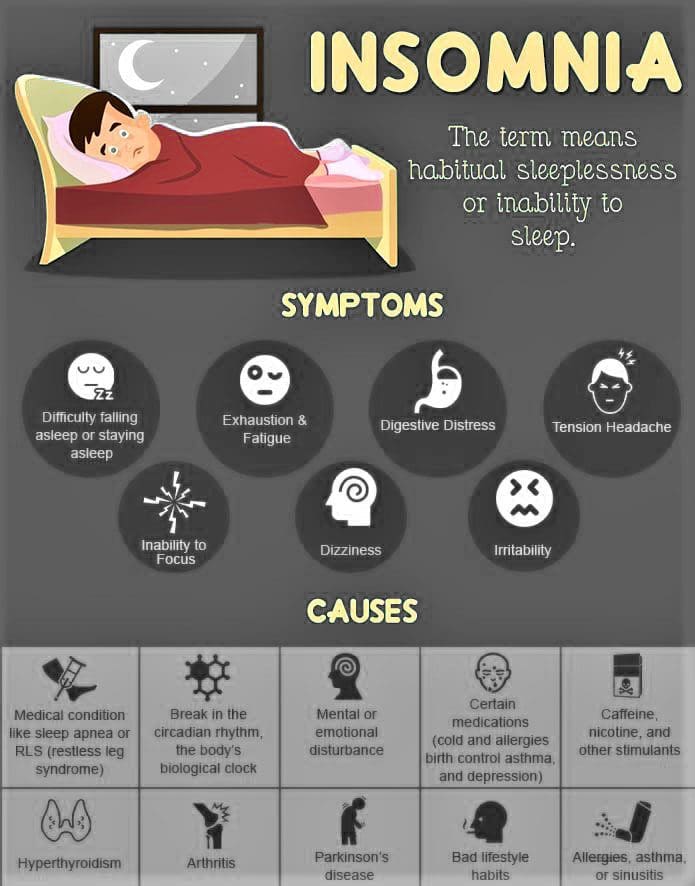
Combat insomnia with chiropractic care. Struggling to get a full night’s sleep, wide awake at three in the morning trying to fall back to sleep before the alarm goes off. Everyone suffers from occasional sleepless nights, but when insomnia occurs regularly it can lead to other issues like:
Daytime fatigue and/or sleepiness
Irritability
Depression
Anxiety
Gastrointestinal symptoms
Low motivation and energy
Poor concentration
Inability to stay focused
Lack of coordination can lead to errors and accidents
Research shows that around 50 percent of the population are experiencing some type of sleep problem. Adults require a little more than eight hours of sleep every night. However, very few individuals are able to manage that with busy/hectic lives. Job, children, and other obligations require many to be up and on the move and getting to bed much later than if following the body’s natural biological rhythm. A disruption to the body’s circadian rhythm, which governs hormone production, body temperature, and sleep, can lead to insomnia.
Combat Insomnia
The body needs adequate, restful healthy sleep to perform its best. Insomnia can cause mental fuzziness and interfere with how the body performs its regular activities. It also increases the risk of:
Depression
Headaches
Accidents
Stress, anxiety, regular caffeine, and alcohol use are some of the greatest contributors to insomnia. Learning how to combat stress effectively is highly recommended to increase the chances of getting a healthy night�s sleep, along with making small lifestyle adjustments could be the difference in getting back to normal sleep.
Sleep Suggestions
Some light regular exercise before dinner time can help put the body in a restful state by bedtime. But do not exercise close to bedtime, as this can amp up the body creating restlessness.
Get out into the sun as often as possible to stimulate melatonin release, which will help reset the circadian rhythm.
Reduce stress through yoga, meditation, and Tai Chi, whichever works and are great ways to help teach the mind and body to relax.
Caffeine and smoking keep the body stimulated. Try to avoid them from mid-afternoon onward.
Keep alcohol consumption to a minimum.
Have a small snack of protein with a complex carbohydrate just before bed, like some peanut butter on a whole-grain cracker. This will keep the blood sugar from dropping too low, causing the body to wake up.
Maintain a regular sleeping and waking schedule.
Turn off the television or any type of electronic device screen an hour before bed, as it stimulates the brain, causing sleep difficulties.
Keep the bedroom dark, quiet, and cool.
If lying awake for more than about 20 minutes, get up and sit in another dark/dimly lit room until sleepiness begins to come on.
Creating healthy sleep habits, along with discussing treatment options with a chiropractor, can help combat insomnia and bring sound sleep.
InBody Composition
Lack of Sleep Stops Muscle Growth
Lack of sleep has a significant effect on catabolic hormones, and specifically, a hormone called cortisol. Cortisol is a hormone that is released as a stress response. It helps break down tissue including muscle tissue, which gives the body energy that it needs to deal with whatever stressful situation the body is dealing with.
Research has shown that during restricted sleep and complete sleep deprivation, cortisol levels become elevated the following evening by up to 45%, potentially accelerating the development of metabolic and cognitive impairment. Cortisol has a muscle-reducing effect, and increased levels from a lack of sleep can threaten muscle development. The overall effect of not sleeping enough can seriously hamper efforts to gain muscle and increase Lean Body Mass.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Bolash R, Drerup M. How to Beat Insomnia When You Have Chronic Pain. Cleveland Clinic Web site. https://health.clevelandclinic.org/2015/12/managing-insomnia-for-those-with-chronic-pain/. Published December 18, 2015. Accessed April 18, 2017.
Improving Sleep: Special Health Report. Boston, MA: Harvard Medical School; 2015.
What is Sleep? American Sleep Association Web site. https://www.sleepassociation.org/patients-general-public/what-is-sleep/. Accessed April 18, 2017.
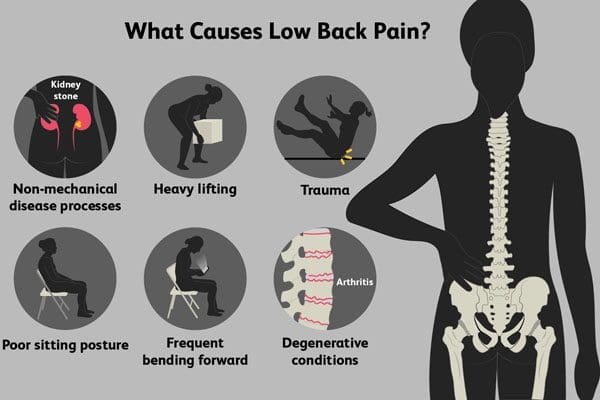
Back pain combined with sciatica is the number one cause of temporary disability all over the world. The spine is a complex interconnected system that supports the entire body. Being overweight does not help. Losing weight can help relieve sciatica and prevent future episodes. It can be done through chiropractic health coaching. According to research, overweight individuals have a higher risk of developing sciatica. The more weight the body carries the more stress is placed on the spine and joints, which can irritate/inflame the sciatic nerve.
Causes and Symptoms
To understand how sciatica is affected by the weight of the body one needs to understand how it works. A breakdown of the causes and symptoms.
The sciatic nerve runs from the lower spine, through the glutes, down the back of the thigh, and is attached under the foot.
The nerve becomes compressed or irritated where it exits the lower spine. This can be caused by a bulging or herniated disc, narrowing of the spinal canal, or bone spurs.
Symptoms include a sharp pain that spreads out from the low back and down the back of the leg. It also causes tingling, numbness, and weakness.
Indirect Cause Being Overweight
Being overweight can indirectly cause sciatica. When the body has to support added/extra weight it can cause problems. That extra weight also places tremendous stress on the joints, especially those in the spine. The lower back takes most of the force from this stress, which is how sciatica develops. The stress slowly pulls the spine out of alignment and compresses the discs between the vertebrae, which then compresses the sciatic nerve, causing pain and discomfort.
Sciatica and Weight Loss
Keep in mind that weight loss is not a cure for sciatica. Weight loss will surely help relieve sciatica pain but there are other issues at work that are combined with excess weight and are causing sciatica. Weight loss is only a step in the right direction. The most recommended and effective ways to lose weight and relieve sciatica pain is having a healthy diet, exercise, and chiropractic health coaching. Other things that can be done to relieve sciatic nerve pain include:
Regular exercise will help reduce the symptoms and strengthen the body’s core and leg muscles. There are a variety of things that make sciatica worse like:
Sitting too much
Sedentary lifestyle
Wearing shoes with no support
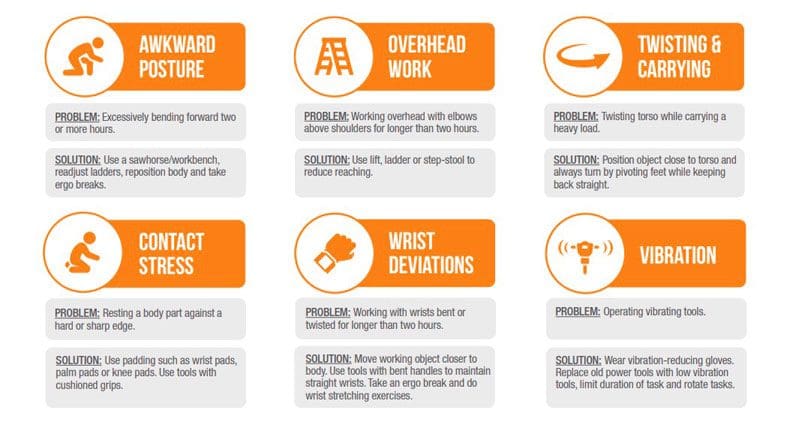
Lifting, bending, twisting, reaching, overuse
Exercise is the best antidote to sitting too much and living a sedentary. Exercising with sciatica does not mean a full gym routine but doing the right exercises that will not worsen the condition. The important thing is staying active. Avoiding exercise will only make sciatica worse. For example, yoga is great for sciatica and health in general. A 30-minute session of yoga 3 times a week combined with another form of exercise twice a week can produce optimal results.
Weight Training
Weight training will work with sciatica with certain adjustments and avoiding specific exercises that can cause pain and should be discussed with a doctor, chiropractor, physical therapist depending on the individual’s sciatic condition.
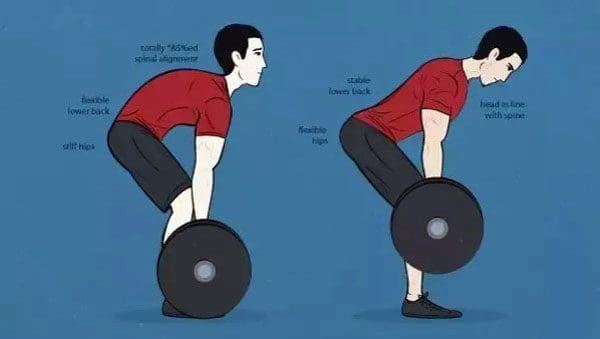
Form and Posture
Weight training form is essential. Practice slow repetitions with special attention to physical form. Proper posture, maintaining a neutral spine, and avoiding rounding the lower back will help avoid worsening sciatica, and prevent further injury/s.
Avoid Overhead and Straight Leg Exercises
Not until the sciatica pain reduces avoid overhead lifting exercises and straight leg exercises, as these can cause flare-ups. Also, avoid intensive abdominal exercises that require doing crunches.
Know The Limits
When sciatica is present, the body is in healing mode, the key is to not overdo it. This exercise is minimal, to help in the recovery process, and strengthen the muscles. Too much exercise can prolong the recovery.
Losing Belly Fat
Losing belly fat with sciatica is possible. But it will take a sustained effort that will be well worth it when sciatica. Losing the fat needs concentration on three things:
Nutrition
Eating whole nutritious foods with plenty of vegetables, and staying away from processed and sugary foods. This is where a health coach and nutritionist can offer the greatest recommendations and develop a customized diet/health plan.
Exercise
Weight training, yoga, cardio, or a combination of all is probably best. Whatever regimen is chosen the objective to stick with it.
Lifestyle adjustments
This includes improving posture, workstation set up, adjusting sitting routines, and limiting activities that cause back pain/sciatica.
Chiropractic Health Coaching
The full-body approach outlined is how chiropractic treats sciatica. Chiropractic can relieve the pain quickly with massage, spinal adjustments, and physical therapies. This is why chiropractic health coaching is ideal for those who have a hard time making nutrition, exercise, and lifestyle changes on their own. Numerous studies show that chiropractic promotes weight loss, reduced pain, improved posture, and increased well being. And it is done in a safe, non-invasive, medication-free way.
Body Composition
Eating Out A Significant Contributor For Weight Gain
When eating out, there is a tendency to consume excess empty calories and increase fat storage. This is why preparing food is so important. It gives the individual direct control over what is being consumed and allows trying out different dietary approaches to see which one works best for improving body composition and gut health. Even for those that don�t enjoy cooking, consult a chiropractic health coach to see what options are available.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
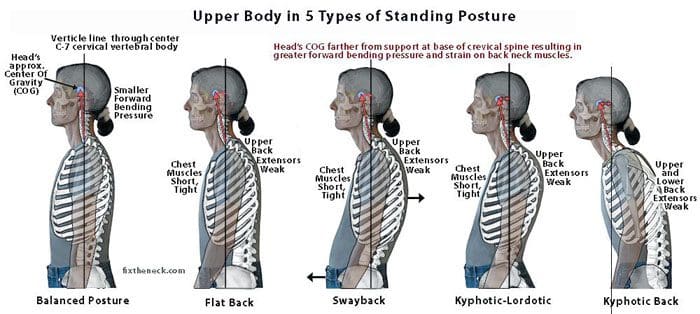
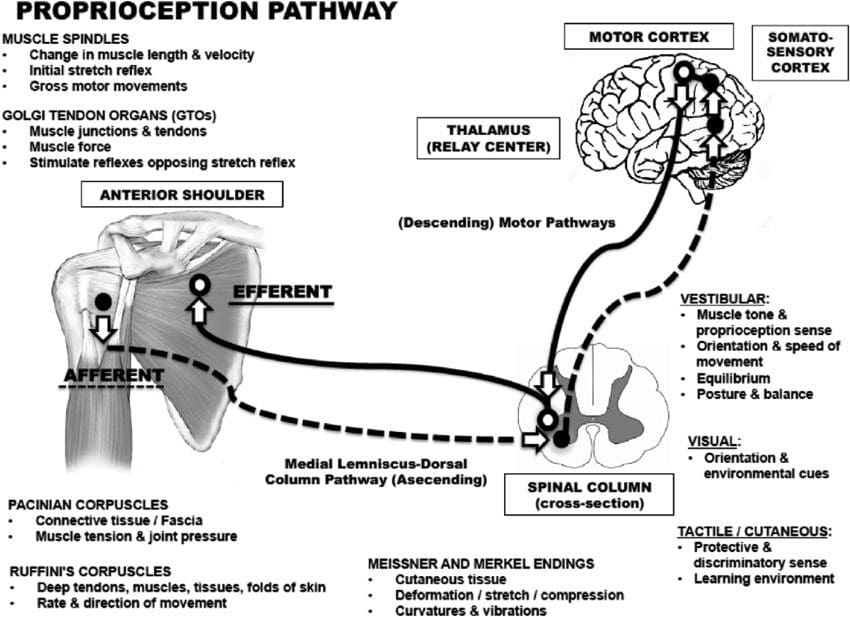
Individuals do not have a poor posture on purpose. It becomes a habit that just goes on until discomfort or pain present. Body awareness is known as proprioception. Proprioception is known as muscle sense or joint position sense. This is the subconscious nature of the body’s understanding of its position in space and the ability to position ourselves comfortably.
Achieving proper and healthy posture means there needs to be a constant mindset of staying aware of how the body is positioned. Then regular adjustments of body position are required to maintain healthy body awareness and from getting into bad habits. To illustrate this consider walking forward in complete darkness. The body knows its relative position even without seeing and understands its existence in space. This is a function of the brain.
It is part of the subconscious and so have little to no control over it. Because of this individuals begin to lapse into poor poster habits. An example tilting the head when looking forward or all the way down when checking the phone. Over time, these bad habits contribute to spinal misalignment. This is where chiropractic can help individuals realize their proprioception tendencies and actively relearn and strengthen positive body awareness and break away from negative postural habits.
Body Awareness Habits
Laying the groundwork for correction of body awareness involves understanding the body’s unconscious habits and the damage that is occurring. Chiropractic is highly effective for outlining what is happening with the help of radiological imaging and spinal curvature benchmarks. Once an individual begins to understand how their posture and spine health are being affected, they can make adjustments to combat this. This requires constant vigilance by the individual to actively realize and correct proprioception.
Optimal Body Exercises
For individuals that have engaged in dysfunctional habits for years, a chiropractor may recommend optimal loading exercises. This process involves teaching how to better balance the body for optimal posture development. For example, a chiropractor will have a patient strengthen a weak leg that is shifting the body’s weight to the other dominant leg that results in unbalanced weight distribution causing hip and back pain. Another example of optimal loading may include executing a series of motions/movements with the non-dominant side. The goal of optimal loading is to train the brain to balance the body in a healthier fashion, instead of reverting to a bad habit.
Ergonomics
Ergonomicscan also help correct dysfunctional proprioception. They can help to address specific defaults of the subconscious. For example, the positioning of a computer screen at the correct height and angle can improve the habit of turning or tilting the head. Another example is utilizing custom foot orthotics to balance the feet and prevent pronation. A chiropractor can determine exactly where the ergonomic intervention will have a significant effect in correcting dysfunctional proprioception.
Chiropractic Relief
Chiropractic postural adjustments, optimal loading exercises, and ergonomics are all recommended tools in rehabilitating and preventing bad posture habits. Injury Medical Chiropractic and Functional Medicine Clinicwill explore every possible approach to help patients understand and overcome the body�s bad habits, and help them achieve optimal spine health.
Body Composition
Muscles get weaker with too much sitting
When sitting the gluteal muscles, abdominal muscles, and legs become dormant. Sitting for extended periods day after day causes these muscles to begin to degenerate. Metabolism is linked with body composition. Having more muscle increases metabolism and helps the body burn more calories.
Any muscle loss, especially from the lower body which is the largest muscle group, can lead to progressive fat gain if the diet is not adjusted. With time gradual muscle loss from the lower body can hurt functional strength, and older age increases the risk of falls and affects the quality of life.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Corliss J. Too much sitting linked to heart disease, diabetes, premature death. Harvard Health Blog. http://www.health.harvard.edu/blog/much-sitting-linked-heart-disease-diabetes-premature-death-201501227618. Published January 22, 2015. Accessed January 7, 2017.
Ergonomics for Prolonged Sitting. UCLA Spine Center Web site. http://spinecenter.ucla.edu/ergonomics-prolonged-sitting. Accessed January 7, 2017.
Florido R, Michos E. Sitting Disease: Moving Your Way to a Healthier Heart.�U.S. News & World Report. http://health.usnews.com/health-news/patient-advice/articles/2015/09/14/sitting-disease-moving-your-way-to-a-healthier-heart. Published September 14, 2015. Accessed January 7, 2017.
For individuals getting up with pain and stiffness in the back, neck, shoulders practically every morning becomes frustrating and depressing. For most, the pain wears off throughout the day but having to deal with it at the start of the day. Dr. Jimenez of Injury Medical Chiropractic and Functional Medicine Clinic offers some suggestions for pain reduction and prevention.
The body spends around a third of each night sleeping because it is a vital part of life. Sleeping means it is time to relax and prepare for the next day. For many, sleeping can be uncomfortable and can be a cause of back and neck pain when getting up. There are steps an individual can take to ensure that correct sleep is achieved while preventing neck and back pain.
Sleep Position Is Important
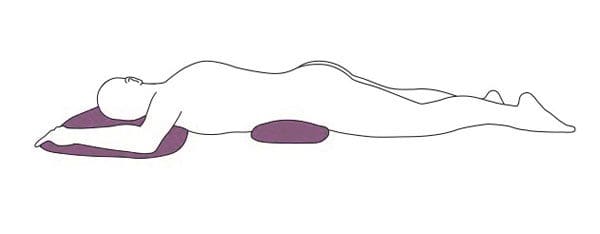
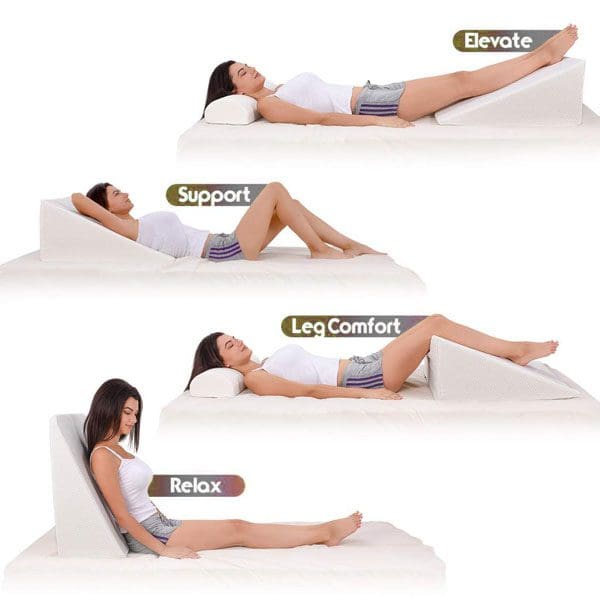
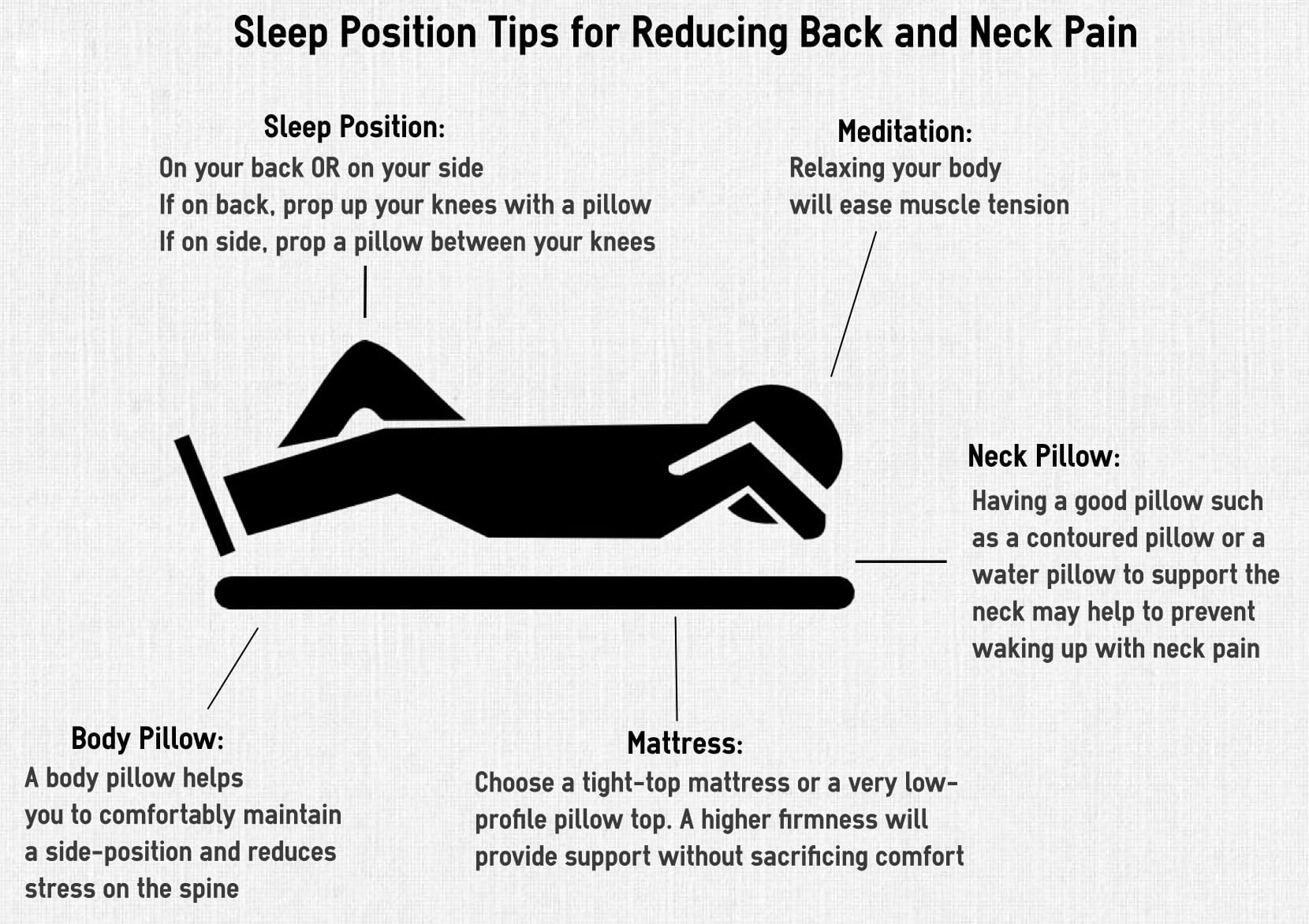
Sleeping in a position that maintains the natural curves of the spine is essential. It is recommended not to sleep on the stomach, as this places the spine in an unnatural position and allows the pelvis and lower back to sink into the mattress with no support. This position can also cause neck pain and headaches when getting up. If this is a position that can’t be changed from years of practice, place a pillow under the stomach and or pelvis to keep the lower back and pelvis straight.
Sleeping on the side or back is highly recommended.
Side sleepers should also place a pillow between the knees.
Back sleepers should place a pillow underneath the knees.
Placing a pillow between and underneath the knees gives the spine proper support to maintain the natural curves.
Check How The Bed Is Set Up
Make sure the bed/sleeping equipment is set up correctly. For example, most pillows do not provide the proper amount of neck support. This can cause neck soreness even if sleeping in the recommended side and back positions. If getting up with neck pain or headaches a cervical pillow can bring relief. A cervical pillow is designed to support the natural curves of the neck while sleeping and places the neck in the proper position. Cervical pillows are designed for side and back sleepers, but make it difficult to sleep on your stomach, which is an added perk to using them.
Using the proper mattress is equally important. The type of mattress being slept on can be a significant contributor to back and neck pain. Individuals that use a medium-firm mattress have less back pain compared to individuals that use too firm or too soft mattresses. Research has shown that mattresses should be replaced every 10 years. Mattresses that are 10 years old and beyond are shown to be a possible cause of back pain while you sleep.
Getting Up and Out of Bed In A Way That Doesn’t Cause Pain
Getting up and out of bed properly will help as well. Most individuals sit up, twist their back to get into a standing position and use the back to stand. This is like lifting with the back and not the legs, which will cause back pain and a possible spinal injury like a herniated disc.
The recommended way to get up and out of bed after waking is to roll onto the side and use the arm to push up and off from the side-lying position.
From this position, scoot to the very edge of the bed and get up using the legs, and not the back.
Implementing these suggestions into your routine can be a great way to decrease pain while sleeping and increase getting up without experiencing stiffness, soreness, and feeling refreshed.
The Body’s Composition
Muscle Mass and Workout Recovery
Looking at muscle mass and the intake of certain nutrients into the evening can be beneficial. Protein intake is essential in muscle formation and muscle recovery after working out or engaged in physical activity. Research has shown that a little protein before sleep helps stimulate muscle protein synthesis.
In a study, ingested proteins were shown to cause a rise in circulating amino acid levels, increased whole-body protein rates, and improved net protein balance. Following exercise, the muscles need to be able to recover properly and protein intake is essential. To achieve weight management goals, an individual must achieve a healthy amount of Lean Body Mass. Lean Body Mass is based on Skeletal Muscle Mass, and protein intake is essential.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Improving Sleep: Special Health Report. Boston, MA: Harvard Medical School; 2015.
Bolash R, Drerup M. How to Beat Insomnia When You Have Chronic Pain. Cleveland Clinic Web site. https://health.clevelandclinic.org/2015/12/managing-insomnia-for-those-with-chronic-pain/. Published December 18, 2015. Accessed April 18, 2017.
What is Sleep? American Sleep Association Web site. https://www.sleepassociation.org/patients-general-public/what-is-sleep/. Accessed April 18, 2017.
Inflammatory spinal arthritis can cause significant joint pain and severely damage sleep quality. Any of the following conditions can cause individuals to experience sleep problems:
Spondylosis (osteoarthritis)
Rheumatoid arthritis
Ankylosing spondylosis
Juvenile idiopathic arthritis
Dr. Jimenez from Injury Medical Chiropractic and Functional Medicine Clinic gives insight into how inflammatory spinal arthritis can disrupt healthy sleep, along with some tips to help individuals with joint pain restore healthy sleep.
Inflammatory Spinal Arthritis and Sleep
First, it is not just the joint pain of arthritis that is causing sleep problems. Research is discovering that more factors could be at play. A study in the journal SLEEP examined how individuals with chronic pain, including osteoarthritis slept. What was revealed was a strong connection between chronic pain and insomnia.
Insomnia can lead to added joint pain because poor sleep can trigger inflammatory pathways that worsen arthritis pain. Plus a poor night of sleep can heighten an individual’s perception of pain the next day. Arthritis pain does not just impact the sleep of adults, but young individuals with juvenile idiopathic arthritis can also struggle with getting healthy sleep. Sleep, pain levels, and mood are strongly related.
Sleep Tips
Achieving quality sleep and a well-rested body can be done. Things to consider to help secure a healthy sleep.
Medication interference/side effects
Corticosteroids could be part of the sleep problem, as corticosteroid treatment has been linked to insomnia. If struggling to fall asleep, talk with a doctor about altering any prescribed medication regimen before sleep like taking aspirin or a nonsteroidal anti-inflammatory NSAID medication in its place.
Adjust sleep position to joint pain
If the neck is sore/aching rest the head on a flat pillow so the cervical spine is in a neutral position. For low back joint pain, individuals might find relief by sleeping on their back or side with the knees and hips flexed at a 90-degree angle. For hip joint stiffness, sleeping on the side with a pillow between the legs is recommended.
A firm mattress and support pillow
A firm mattress will support the body and help reduce pain. The right pillow/s are also important for healthy sleep. A lumbar and cervical pillow can help cushion tender areas.
Readjust chores
Joint pain first thing in the morning needs time to adjust. For morning physical chores try to reschedule for later on in the day or if possible the night before. This could be fixing lunches, picking out clothes, preparing breakfast, or packing the work case, tools, etc. The extra time will reduce morning stress and allow the body to gently adjust.
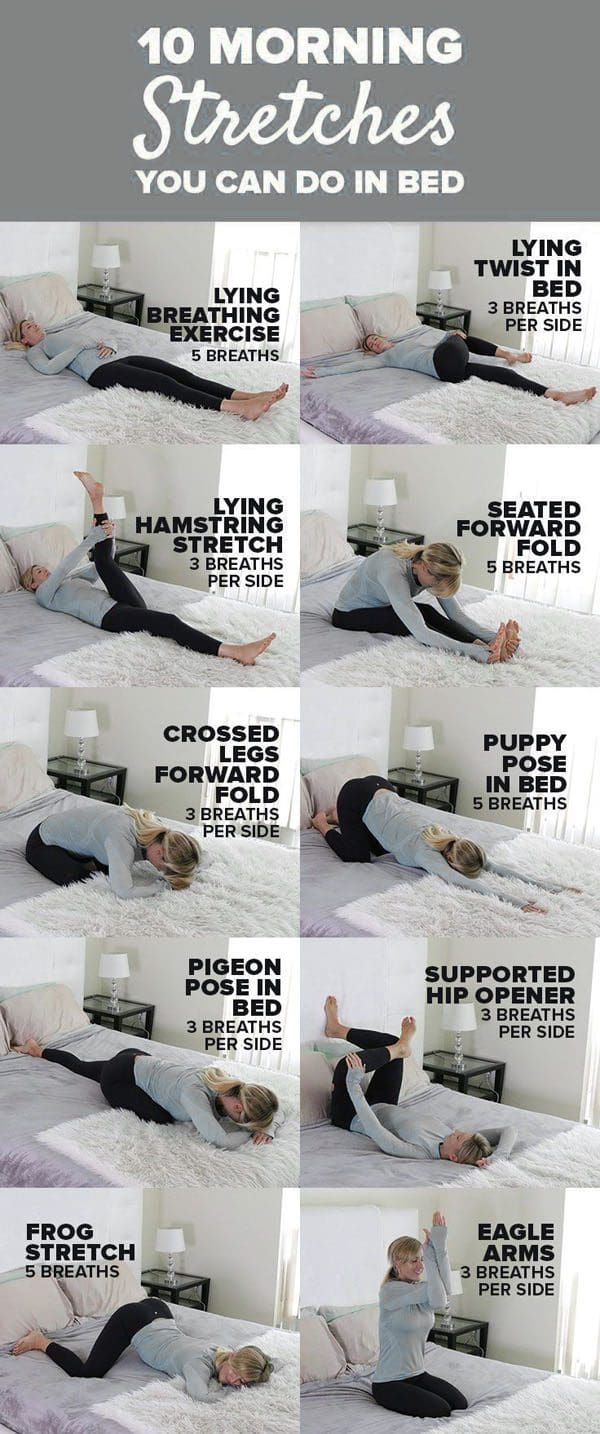
Wake up and stretch
With joint pain in the morning, some gentle stretching can help. Doing some stretches before even getting out of bed will help minimize pain and allow the body to gradually prepare for movement. Follow the stretch session up with a hot shower to loosen stiff joints.
Increase Sleep Quality
Sleep problems can affect anyone even those that don’t have inflammatory spinal arthritis/joint pain. There could be other issues causing sleep problems unrelated to joint pain. If still not getting quality sleep, talk to a rheumatologist about available options.
Body Composition
Osteoarthritis and Exercise
Obesity is a significant risk factor in the development of osteoarthritis. This is not only from the effects of extra weight on the body’s joints but also as a result of the pro-inflammatory effects of adipose tissue. The hips and knees are the weight-bearing joints. Excessive adipose tissue on the midsection and legs have been shown to negatively impact these weight-bearing joints.
Promoting Lean Body Mass and encouraging weight loss can potentially lower the risk of osteoarthritis and improve the quality of life. Gentle exercise is regarded as safe for individuals with osteoarthritis and is a key component to improve body composition, reduce body fat mass, improve lean body mass and maintain a healthy weight. Improving body composition and utilizing exercise in weight management can have a direct and positive effect on joint health.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Myers W. 9 Ways to Rise and Shine With Osteoarthritis. Everyday Health.�http://www.everydayhealth.com/osteoarthritis/ways-to-rise-and-shine-with-osteoarthritis.aspx. Last updated September 25, 2014. Accessed April 18, 2017.
Watson S. Why Osteoarthritis Could Disrupt Your Sleep�and Your Partner�s. Arthritis Foundation. http://www.arthritis.org/living-with-arthritis/comorbidities/sleep-insomnia/osteoarthritis-and-sleep.php. Accessed April 18, 2017.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine