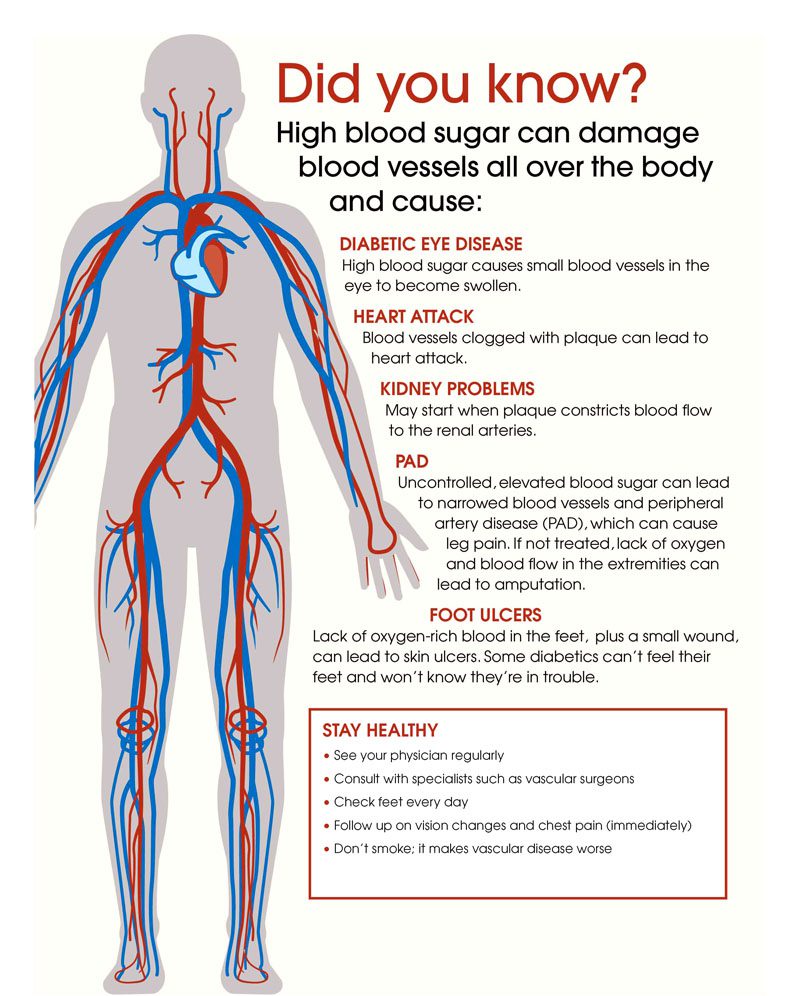
The diabetic disease processes can be a contributor to chronic back pain. Diabetes can damage the human body from the eyes to the feet if left untreated, and the spine/back is a prime target. Data from 11 studies consisted of individuals over 18 years of age diagnosed with type 1 or type 2 diabetes. The results showed individuals with diabetes had a 35% increased risk of experiencing lower back pain. According to the Centers for Disease Control and Prevention, around 34 million people were found to have diabetes in 2021. Diabetes primarily impacts blood sugar/glucose levels. However, the disease can affect several of the body’s systems. It is a state of chronic inflammation.
Diabetic Back Pain Connection
The connection between diabetes and back pain include:
Neuropathy
Diabetic neuropathy happens when constant high glucose levels damage/injure the nerves. The result is symptoms like pain, tingling, and numbness. It affects up to 50% of individuals with diabetes and can lead to severe chronic back pain. High sugar levels damage various organ systems including the nervous system that results in neuropathy that causes pain/discomfort.
Bone Health
A complication that diabetes can cause is compromised bone health.High glucose levels can damage the collagen that makes up bone. This creates an increased risk of vertebral and other types of fractures. The high-risk compounds fractures that do not heal properly or correctly. Diabetics have an increased risk of fracture because of the accumulation increase of advanced glycation products. This substance forms when proteins or lipids combine with sugar. With time these products can cause damage to various tissues that include bone.
Obesity
Obesity contributes to the development of type 2 diabetes and is also a complication that results from incorrect glucose level management. Regardless of which came first, the added weight is a major contributor to back pain because of the added pressure/load on the spine. Excess weight and physical inactivity can result in serious issues of the musculoskeletal system.
Additional Factors
Poorly controlled diabetes also reduces muscle blood flow and increases cartilage inflammation. Other types of tissue damage can occur like degeneration of intervertebral discs and spinal canal stenosis. Disc degeneration and spinal stenosis are common causes of back and neck pain. Diabetics are prone to infection/s. This can cause back pain if it is in the bone known as osteomyelitis.
Diabetic Back Pain Management
There are steps that can help ease pain and discomfort.
Getting Involved In Physical Activity
Exercising/physical activity is a must. The body needs to move to get all the systems flowing improving diabetes and back pain. A sedentary lifestyle can take back pain to new levels with time. Even though when pain presents the first instinct is to stop and rest. Simple ways to get moving include:
Walks
Stretches
Gentle laps in a pool
All can help with:
Improved blood flow
Aids in weight loss
Recommended for both conditions
Exercising releases endorphins, which are the pain relief chemicals that the body produces naturally.
Yoga can reduce physical pain and discomfort throughout the body
Quitting Bad Habits
Smokers have a significantly higher risk for low back pain compared to non-smokers. Nicotine can alleviate pain short term, but over time the nerves become more sensitive and can increase the pain. Alcohol use can help numb the pain short term, but it can cause muscle spasms and dehydration intensifying the pain. Complications can arise if taking pain medication. The most important thing is managing diabetes effectively.Injury Medical Chiropractic and Functional Medicine Clinic will help the individual feel better, move better, and keep back pain away.
Body Composition
Vitamin D and Healthy Blood Sugar Levels
Vitamin D benefits muscle health, muscle mass, and blood sugar. Insulin is the hormone that lets blood sugar into the muscles. Individuals with adequate blood vitamin D levels significantly lower the risk of hyperglycemia than those with below-recommended levels. Research shows daily vitamin D supplements used in combination with calcium decelerate the gradual rise in blood sugar in those with prediabetes. Adequate vitamin D levels can prevent the progression of hyperglycemia. Supplementation is beneficial for individuals going through a deficiency. Adults should aim for a dietary intake of 600 – 800 IU per day. However, supplements are never a substitute for a healthy and diverse diet.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Pozzobon, Daniel, et al. “Is There an Association between Diabetes and Neck and Back Pain? A Systematic Review with Meta-Analyses.” PLOS ONE, vol. 14, no. 2, 2019, doi:10.1371/journal.pone .0212030.
Murray, Cliodhna E, and Cynthia M Coleman. “Impact of Diabetes Mellitus on Bone Health.” International Journal of Molecular Sciences, MDPI, 30 Sept. 2019, www.ncbi.nlm.nih.gov/pmc/articles/PMC6801685/.
Groen BBL, Hamer HM, Snijders T, van Kranenburg J, Frijns D, Vink H, et al. Skeletal muscle capillary density and microvascular function are compromised with aging and type 2 diabetes. Journal of Applied Physiology. 2014;116(8):998–1005. pmid:24577061
Eivazi M, Abadi L. Low Back Pain in Diabetes Mellitus and Importance of Preventive Approach. Health Promotion Perspectives. 2012;2(1):80–8. pmid:24688921
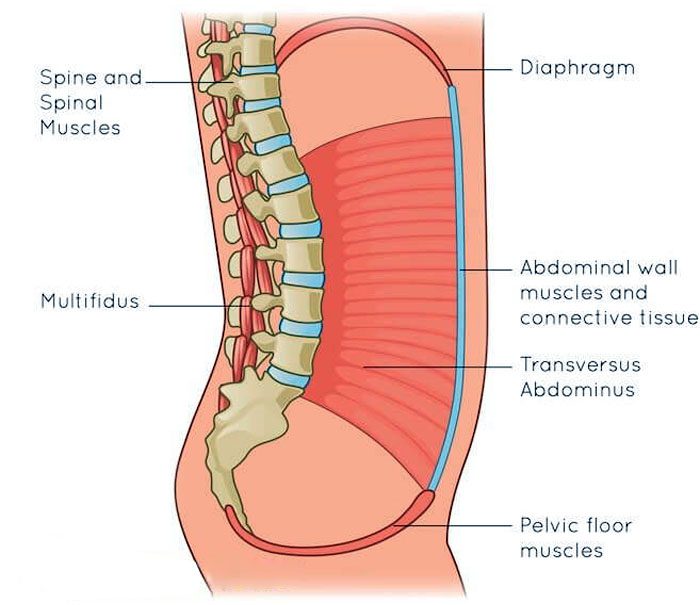
The pelvis is designed to bear and distribute the weight of the body along with regular everyday movement. It is built to properly distribute weight between the upper and lower body that utilizes the core muscles, ligaments, and joints creating a complex pelvic girdle that helps the body function properly. The bones of the pelvis house and protect organs like the:
Reproductive system
Bladder
Below the digestive tract
When pain in the pelvis presents, daily physical activities can become difficult to get through. Chiropractic treatment combined with lifestyle adjustments can bring pain relief and strengthen the pelvis muscles/bones to maintain optimal function.
Causes of Pelvic Pain
When pain presents there can be a variety of underlying causes contributing to it. Certain causes are more serious than others. This is why seeking professional medical guidance is highly recommended for the best outcomes. Possible causes include:
These are a few causes that can contribute to mechanical changes and imbalances within the pelvis anatomy. If the pain is thought to be caused by an internal organ issue with nausea, fever, vomiting, or severe pain contact a healthcare provider immediately.
Chiropractic Relief
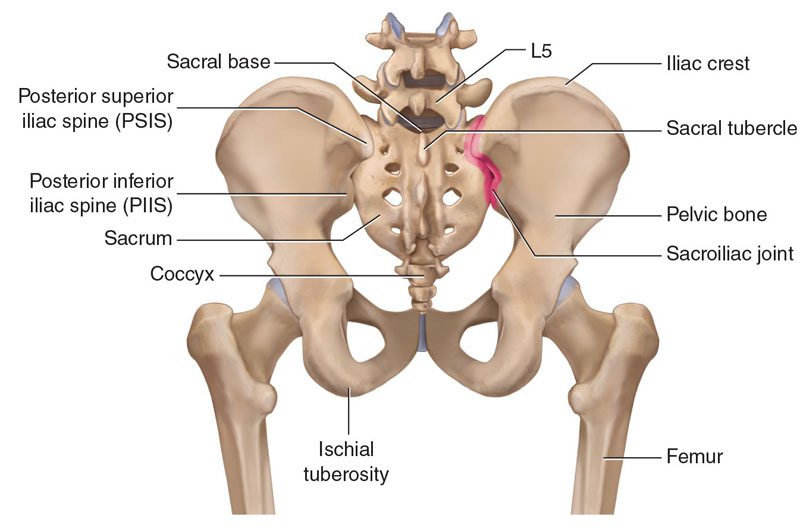
The pelvis can be thought of as a direct continuation of the spine. The lowest fused five vertebrae are known as the sacrum and are part of the pelvic girdle complex. Individuals dealing with pelvic pain typically experience the sensation within the joints themselves. These are the pubic symphysis and/or sacroiliac joints. These joints interact with the entire skeletal system. Learning how they operate can help bring relief and recovery. This is where a chiropractor can help.
Chiropractors are experts in total body alignment, restoring balance to the pelvis and spine. Plus through the treatment, they help increase the body’s natural ability to heal itself. When the lower back or pelvis is out of alignment the entire body along with its systems can be thrown off balance causing dysfunction. Chiropractic promotes and increases balance with pelvic adjustments and diverse therapies that include:
A professional chiropractor is one of the best options for the management and alleviation of pelvis pain. Pelvis misalignment can impede nerve energy and adequate blood flow. Chiropractic restoration strengthens and maintains optimal long-lasting results. Whether the pelvic pain comes from an injury, pregnancy, or pelvic shift/imbalance, a chiropractic provider can help address and alleviate the pain.
Body Composition
Lifestyle Adjustments for Optimal Kidney Health
The kidneys are small organs that work twenty-four-seven to filter blood and flush waste. In one day the kidneys pump more than 400 gallons of recycled blood throughout the body. When the kidneys do not function properly the body can be engulfed with waste. This is why it is vital to keep them healthy. Individuals usually don’t realize how an unhealthy lifestyle can harm/injure the kidneys. Chronic kidney disease slowly progresses over years, and it is not reversible. Incorporating some basic healthy lifestyle adjustments can lower the risk of developing kidney-related diseases. Here are a few lifestyle adjustments that can keep the kidneys healthy.
Drinking plenty of water
An adequate supply of water in the kidneys flushes out sodium, urea, and toxins helping avoid kidney stones. The goal is to drink eight 8-ounce glasses of water every day. Everyone’s water levels are different but body composition analysis can calculate what a normal level should be.
Healthy foods maintain a healthy body
Poor diet and visceral fat gain have been linked to chronic kidney disease. Reducing visceral fat can be achieved by eating a restricted caloric diet of vegetables, fruit, and lean protein, as well as cutting back on processed foods.
Be cautious consuming supplements, antibiotics, and over the counter medications
Regular use of common medications and supplements can cause kidney damage and disease. Consult with a doctor before taking medications and supplements if there is kidney function impairment.
Fitness and activity
Individuals need to participate in regular cardiovascular and weight-resistance physical activity/exercise. High blood sugar levels have been shown to stress the kidneys. Building adequate muscle mass helps control blood sugar.
Smoking and kidney health issues
Smoking narrows the blood vessels in the kidneys. This reduces proper blood flow and accelerates kidney malfunction.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
Kim DH, Cho D, Dickman CA, Kim I, et al. Surgical Anatomy & Techniques to the Spine. 2nd Ed. Saunders, Elsevier, Inc. Philadelphia, PA.
Lirette LS, Chaiban G, Tolba R, Eissa H. Coccydynia: An Overview of the Anatomy, Etiology, and Treatment of Coccyx Pain. Ochsner J. 2014 Spring;14(1): 84-87.
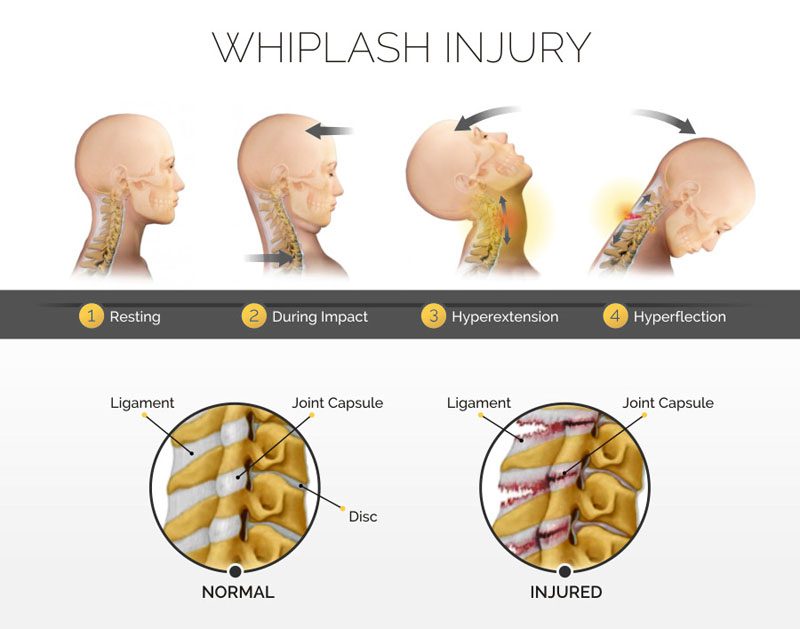
A whiplash injury can cause pain for months, even years after the accident/incident. It can cause persistent pain in the neck, shoulders, back, as well as, headaches, and sleep problems. Waiting to see if it will go away is not recommended. Chiropractic treatment can effectively and successfully expedite the healing process getting back to normal life as quickly as possible. Chiropractors treat whiplash successfully using a combination of techniques, approaches, and exercises for pain relief, recovery, and long-term spinal health. The extent and severity of the whiplash injury determine what type of chiropractic treatment will be implemented.
The Severity of a Whiplash Injury
Whiplash injuries are often the result of:
Automobile accidents
Work injuries
Sports
Amusement park rides
It is primarily an injury of the neck muscles and ligaments, but can also damage the vertebral discs. It is not considered a serious or life-threatening injury, but it can cause long-term complications and severe chronic pain. The biggest risk comes from the delayed presentation of symptoms. It can take days and sometimes weeks for the effects of the injury to present. Individuals that are older or those with arthritis are more likely to have severe and long-term issues.
Other Symptoms
Typical symptoms like neck pain, blurry vision, stiffness, and dizziness are well known. These can range from mild to severe, and last for a few days, weeks, or, in severe cases, years. However, there are some symptoms that most don’t know about and include:
Individuals should be alert for signs/symptoms that the injury requires immediate medical attention. If any of the following are experienced seek immediate care.
The arms, shoulders, or legs are numb, tingling, and/or weak
The neck pain and stiffness return after going away
Bowel or bladder problems could indicate nerve damage
Chiropractic
Chiropractic treatment depends on the individual case. A doctor of chiropractic will determine the right treatment plan by the:
The severity of the pain
Location of the injury
Accompanying symptoms
Medical history
X-rays will be taken of the affected area to rule out any other trauma or injury. The chiropractor will evaluate the entire spine. This is based on how one part of the body influences other areas with the objective being to get the whole body functioning successfully at optimal levels.
Treatment Options
Some of the more common treatments for whiplash include:
Initial
Visiting a chiropractor a short time after the injury means the neck will be inflamed. The doctor will utilize gentle, anti-inflammatory options like:
Cold therapy
Ultrasound
Stretching
Electrical therapy
Laser therapy
Spinal Manipulation
There are different types of spinal manipulation, these include:
Specific Manipulation
This type involves a gentle but firm thrusting, usually done with the hands to the soft tissue areas. It stimulates the nervous system to realign subluxations, and restore mobility/flexibility of the spinal joints and vertebrae.
Flexion Distraction Technique
This is also a hands-on technique that treats slipped and bulging discs. This type of treatment utilizes a pumping motion on the disc/s and not the spine itself.
Instrument Assistance
This treatment is used for patients with degenerative disc disease. Special instrument assistance is often used in combination with hands-on care.
Massage
Massage promotes healing, reduces pain, and improves blood circulation in and around the affected area. It helps relieve tension/stress in the shoulder and neck.
Stretching and Trigger Point Therapy
The muscles and tendons can become tight. A chiropractor will gently stretch the area to relieve pain, ease tension, and reduce tension headaches. Trigger point therapy uses persistent pressure by the chiropractor’s fingers. It relaxes and releases the tight areas.
McKenzie Exercises
McKenzie exercises help reduce disc tears common to these types of injuries. The chiropractor will show how to perform these simple movements at home as part of the recovery.
What to do outside of the clinic
A chiropractor will offer tips and guidance on how to successfully avoid worsening the injury or create new injury/s. Stretches and exercises will be recommended to strengthen and maintain flexibility. Depending on an individual’s:
Overall health
Posture
Work/Occupation
Lifestyle factors
They will offer recommendations to avoid long-term issues.
Body Composition
Successfully regaining fitness after an injury
It is difficult to predict how long it will take to regain a previous level of fitness after an injury. Retraining to peak condition depends on the injury and how much damage was done. A key factor is to not adopt a sedentary lifestyle.Muscle memory can help as the muscles have special cells in the fibers that can recollect previous movements. This means when back to working out after an extended layoff, the body is able to regain the lost muscle. Some tips to help get back into shape:
Ease back into working out to avoid/worsen the injury
Wait a month before starting a less-intense version of a regular workout
Patience and persistence are essential to regaining fitness successfully.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Dagenais, Simon, and Scott Haldeman. “Chiropractic.” Primary care vol. 29,2 (2002): 419-37. doi:10.1016/s0095-4543(01)00005-7
Ritchie, Carrie et al. “Medical and allied health service use during acute and chronic post-injury periods in whiplash injured individuals.” BMC health services research vol. 20,1 260. 30 Mar. 2020, doi:10.1186/s12913-020-05146-0
Ferrari, Robert, and Anthony Science Russell. “Survey of general practitioner, family physician, and chiropractor’s beliefs regarding the management of acute whiplash patients.” Spine vol. 29,19 (2004): 2173-7. doi:10.1097/01.brs.0000141184.86744.37
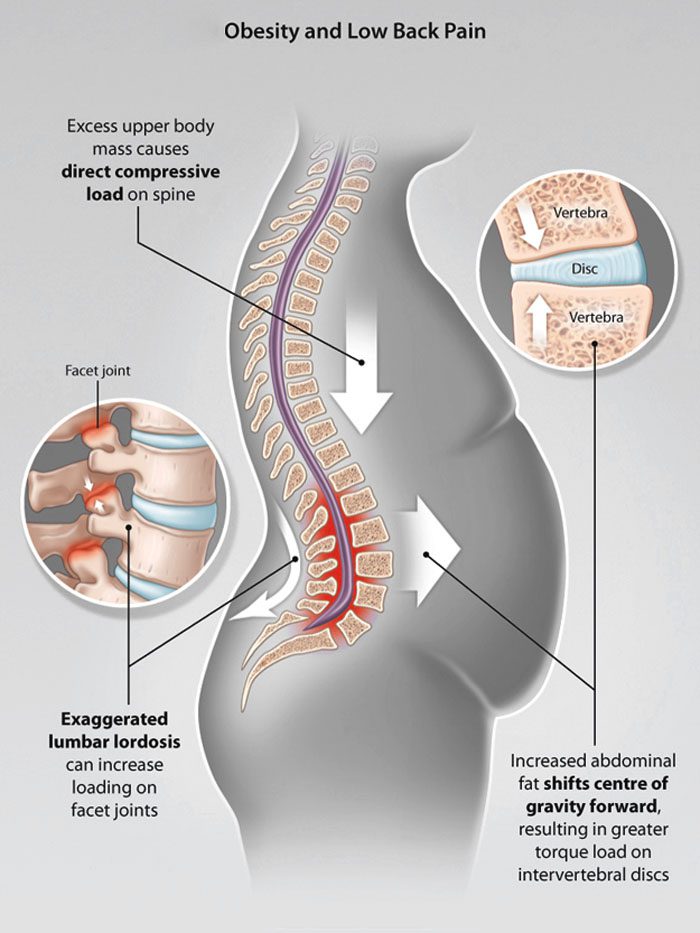
Belly fat is a gateway to back pain/spinal issues that can lead to various health problems. The bulging belly population has grown a bit since the beginning of the COVID-19 pandemic. 37% of individuals have gained weight since it began, according to a global Ipsos survey. If back pain is presenting and there is excess weight around the abdomen known as abdominal obesity, this could be a contributing factor.
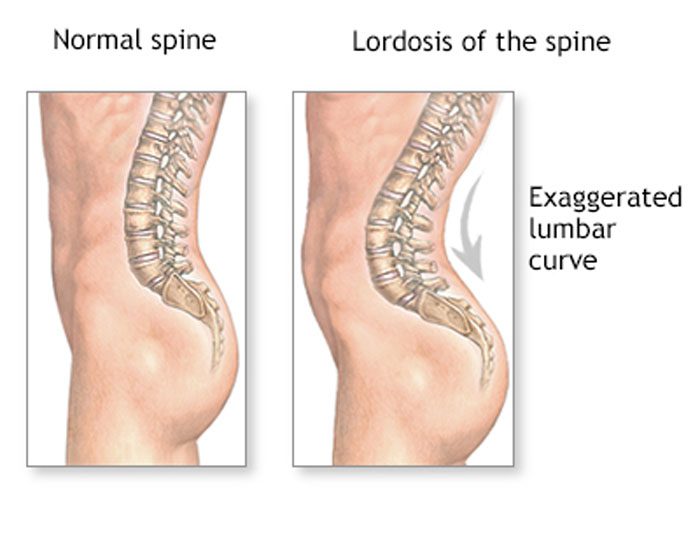
Belly fat and posture
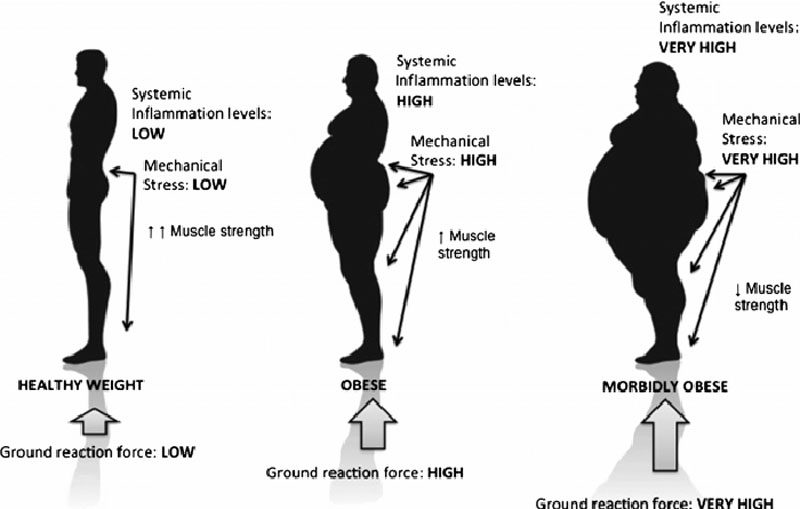
When the natural curves of the spine are normal, the core is stable and well-supported. Excessive weight, including a large abdomen, shifts these curves out of correct alignment. Excessive abdominal fat has been associated with lordosis, which is an excessive inward curve of the spine toward the lower back. One study found that severely obese individuals had pain and changes in posture. This was especially visible in the spine, knees, and feet.
Front-loading shift
The back pain felt from a bulging belly can be caused by a shift in posture and body mechanics. Studies show these can have a negative impact on back pain and body positioning. All or most of the weight is placed on the lower back.
Overloaded discs
Abdominal obesity can damage/injure the discs/shock absorbers of the spine. This leads to:
And a bulging belly can flatten the height of the intervertebral discs.
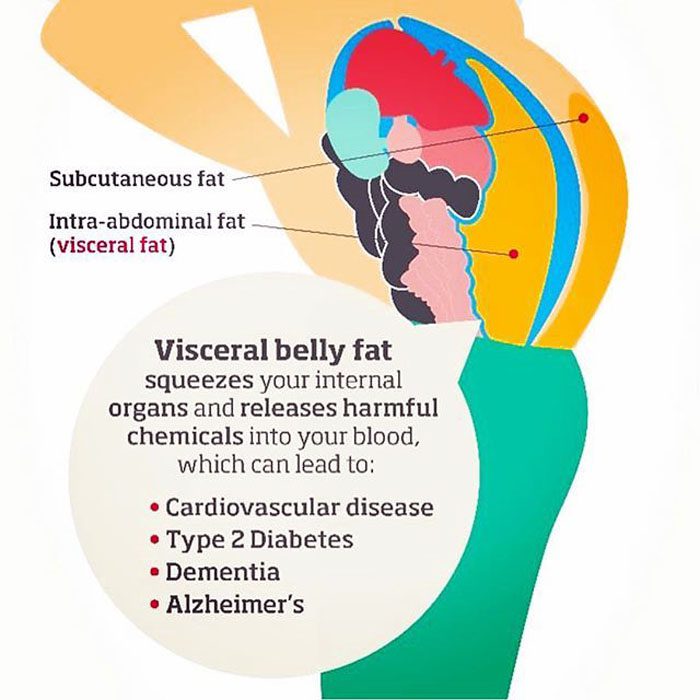
Fat pollutants in the blood
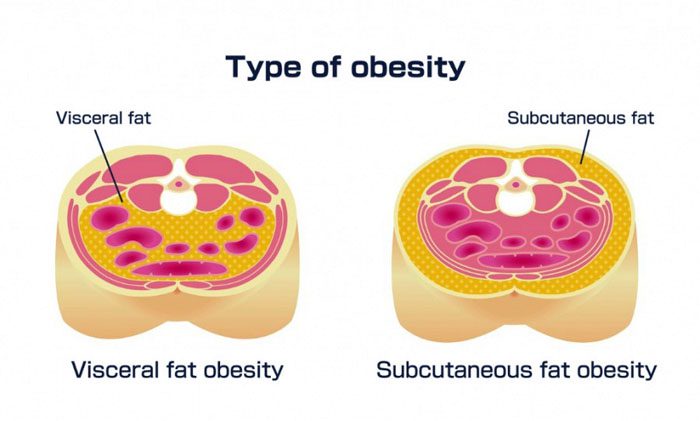
Fat can accumulate and secrete toxins that contribute to swelling and inflammation that can be painful. Over time, these toxins wear down components of the skeletal system.A study found potential links between obesity and degenerative disc disease. Scientists found a connection in obese men, but not obese women. This is believed to be because men tend to store fat in their bellies, and women tend to store fat in the buttocks and thighs.
Damage to the musculoskeletal system
The bones constantly renew themselves, but when there is excess body fat it can interfere with the process. This has the potential to turn into osteoporosis over time. Studies associate visceral fat with lower bone mineral density, and an increase in the risk of fractures.
Ankylosing spondylitis treatment and fat interference
Ankylosing spondylitis is an inflammatory disease that causes chronic back pain and can cause the vertebrae to fuse. The back can be extremely stiff, and the condition can lead to a permanently hunched posture. There are medications to improve symptoms and slow the disease. However, being overweight reduces the drugs’ effectiveness. This is because belly fat can cause medication absorption problems.
Rare spinal condition linked to obesity
Obesity along with a high Body Mass Index increases the risk of a rare condition called spinal epidural lipomatosis or SEL. This is an overgrowth of body fat in the spinal canal. Spinal epidural lipomatosis can cause various types of back pain. This is why it is recommended to have a doctor examine and evaluate any aches or pains.
Body Composition
Kombucha beneficial for gut bacteria
Kombucha contains a wide variety of bacteria and fungi that helps ferment the sugar in kombucha drinks. It is able to affect the existing microbes in the gut by inhibiting the growth of various gut-dwelling pathogens. These include:
It is a probiotic drink made from fermenting green or black tea
It is made up of healthy bacteria that produce acetic acid that is beneficial for blood sugar, insulin levels, and body composition
It helps the body process food by lowering insulin levels after a meal
It contains polyphenols that reduce oxidative stress, to help fight disease risks
It destroys unhealthy bacteria in the gut
It helps increase healthy bacteria
Kombucha can be thought of as a natural antibiotic. However, it does not come with the weight-gain side effect. Improving the health of the gut through fermented foods like kombucha help reduce the risk for weight gain/obesity, as well as restore gut health for those trying to lose weight by creating a healthy gut environment.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
Going through traumatic accidents that result in injuries can cause injury-related stress and anxiety for individuals. It is understandable that stress and anxiety are high as individuals figure out how to navigate through the situation. Therefore, it is very important to find ways to manage stress and anxiety because if they go unchecked it could become chronic leading to poor health and quality of life.
Stress/Anxiety Affects Health
Injury related stress and anxiety can be exacerbated through different factors. These can include:
Medical bills
Employment
Relationships
Independence
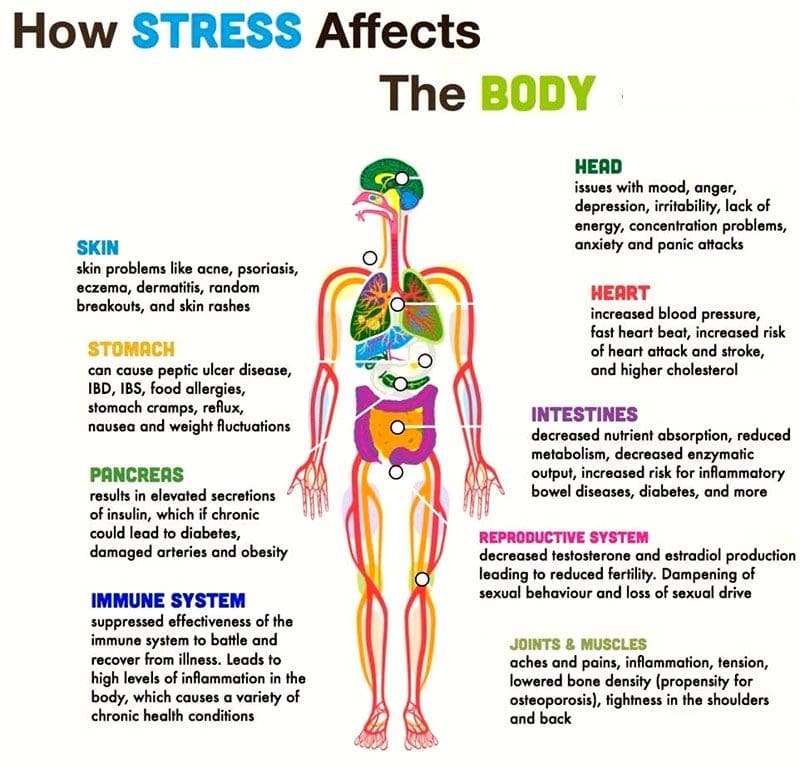
The causes/reasons can vary however, the physical response the body goes through is the same. A stress-inducing situation can leave an individual feeling threatened and generate a physical stress response. The body responds to stress by releasing hormones that shift the body into survival mode. This requires a lot of energy placing massive strain on the body. This is an important mechanism for healthy living. However, if it begins to present on a regular basis it can lead to negative health issues that include:
The body needs time every day to recover and rejuvenate. This is not possible when the body is constantly entering a heightened state of stress. Traditional treatment can lead to the over-prescription of medications that come with their own side effects. Effective injury-related stress treatment addresses issues like:
Injury-related stress and anxiety affect mental health and can lead to physical symptoms and disease. These include:
Chronic pain
Sleep problems
Gastrointestinal issues
Obesity
Asthma and breathing problems
Alzheimer’s, dementia, and memory loss
Chiropractic Treatment and Care
A healthy brain and spinal cord are vital to the body’s optimal health. When nerve energy and blood flow get blocked it can worsen injury-related stress and anxiety. Chiropractic delivers results helping to better manage mental health by addressing underlying issues with spinal misalignment. When the spine is properly aligned neural health is optimized for everyday functions. This increases vitality and an overall sense of well-being. With brain function improved adjusting to the injury and its effects no longer cause intense stress. Individuals cannot remove all the stressors and anxiety-inducing events from their lives, but proper spinal alignment can help build resilience for whatever situations life throws.
Body Composition
Recovery and Swelling
Recovery is an essential part of maintaining optimal body health. This goes for regular work, working out, athlete’s training, and just participating in physical activity. A significant sign that the body has gone through intense physical exertion and needs recovery time is swelling. Swelling presents for different reasons. It is the body’s response to tiny, microscopic tears in the muscle that happens from constant and intense use. Running or lifting heavy objects are two examples that cause swelling. Swelling can be seen in body composition analysis results. An increase in Lean Body Mass reflects an increase in water. Recovery is about giving the body a chance to:
Relax
Recuperate
Recover from the swelling with the end goal of resuming physical activities
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
References
Pickar, Joel G. “Neurophysiological effects of spinal manipulation.” The spine journal : official journal of the North American Spine Society vol. 2,5 (2002): 357-71. doi:10.1016/s1529-9430(02)00400-x
Coleman, Brian C et al. “Factors Associated With Posttraumatic Stress Disorder Among Veterans of Recent Wars Receiving Veterans Affairs Chiropractic Care.” Journal of manipulative and physiological therapeutics vol. 43,8 (2020): 753-759. doi:10.1016/j.jmpt.2019.10.016
Jamison, J R. “Stress management: an exploratory study of chiropractic patients.” Journal of manipulative and physiological therapeutics vol. 23,1 (2000): 32-6. doi:10.1016/s0161-4754(00)90111-8
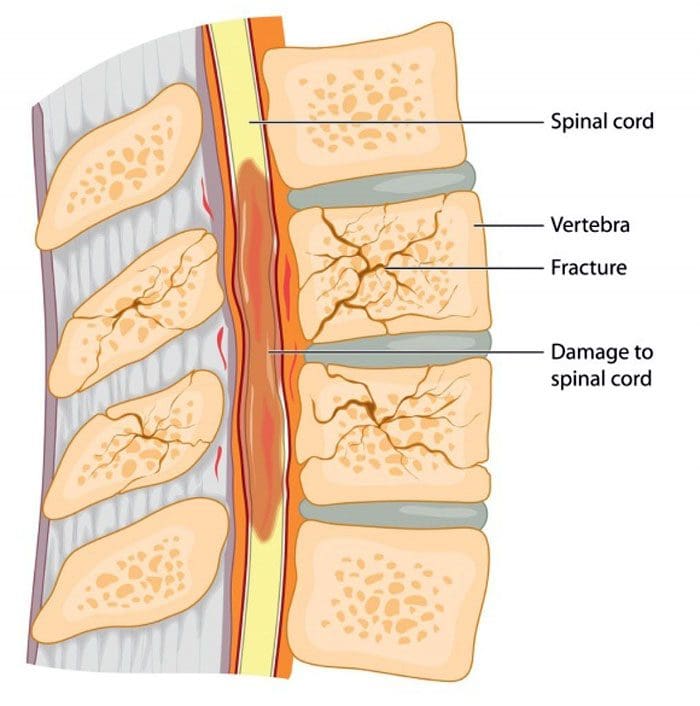
Spinal vertebral compression fractures are a common injury in older individuals brought on from a lowered bone density. Hip and wrist fractures get most of the attention when it comes to osteoporosis. However, spinal fractures happen almost twice as often and affect around 700,000 individuals yearly. This is according to the American Academy of Orthopaedic Surgeons or the AAOS. These types of fractures are also known as:
Fragility fractures
Vertebral compression fractures
Osteoporotic compression fractures. These usually happen as a result of thinning and weakening bones caused by osteoporosis.
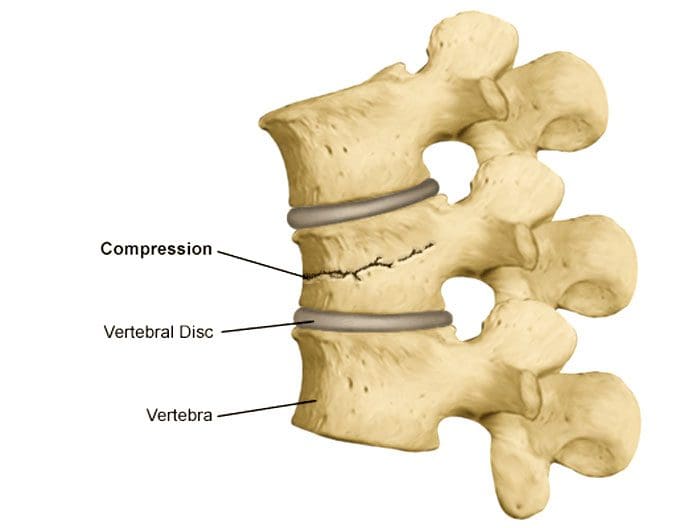
The Academy of Orthopedic Surgeons notes that changes in the body’s musculoskeletal bone structure can go unnoticed for years. This leads to the vertebrae narrowing and flattening, rounding the spine as a result, creating compression. Because of the weakened bone, the pressure, even from everyday low-impact movements like reaching, bending or twisting. There are strategies that can help prevent osteoporosis and osteoporotic compression fractures.
More Movement and Physical Activity
One prevention strategy that is highly recommended is more movement and physical activity. This does not include occasional gentle movements like taking a break from sitting. Improving the spine’s health means using the full range of motion and loading the bones so they can get build strength. This could be walking more, which creates spinal resistance. Also using light weights with high repetitions with five to ten pounds of a load is enough to challenge the spine without generating muscle stress.
Individuals think they need to rest more as they get older, but to build and maintain bone density to prevent osteoporotic compression fractures more physical activity is needed. Moving around for 10 to 15 minutes every hour is a good way to start. Incorporating more activity, and focusing on healthy diet changes will help shed excess weight. This will decrease pressure on the spine, reducing the risk of fractures. For individuals with osteoporosis of the spine, it is important to review any exercise plans with a physician or doctor of chiropractic to ensure that they are safe. The wrong types of movement or too much stress on a fragile spine can definitely cause a fracture.
Medications and Other Conditions
There are medications that can help build bone density, but there are also medications for conditions that can actually cause faster bone density loss. Individuals could be taking a medication that’s good for one issue/condition, but not realize it may be associated with a reduction in bone density. This is why it is important to review prescriptions with a doctor with bone density loss side effects in mind. Medications that can cause bone loss include:
Anti-seizure drugs like carbamazepine and phenytoin
Diuretics like furosemide
Also, review any underlying conditions that could affect osteoporosis. As an example, the National Institutes of Health or NIH note that individuals with diabetes, specifically type 1, can have poor bone quality increasing their risk of fractures.
Adding Calcium To The Diet
An adequate intake of calcium is essential for osteoporosis prevention and helps lower the risk of fragility fractures. A low calcium intake contributes significantly to lower bone density and faster bone loss with age. Vitamin D also helps in bone injury prevention.
Treatment
Compression fracture/s diagnosis are confirmed through imaging tests like:
X-rays
Magnetic resonance imaging MRI scan
Bone scan
Computed tomography CT scan
Bone density testing with dual-energy x-ray absorptiometry DEXA will determine bone mineral density. If a scan reveals there is a vertebral compression fracture, the most common approach is no treatment. According to the Academy of Orthopedic Surgeons, most individuals with this type of injury improve within three months with a combined rest period and limited pain medication use.
Some individuals are recommended to wear braces to restrict movement so the fracture can heal without any added compression or stress. For those that do not respond to non-surgical treatment, minimally invasive surgery could become an option. In both cases, a doctor will suggest similar aforementioned strategies to help strengthen the bones and prevent worsening or creating new issues.
More flab on the middle that gets harder to burn off
Performance at work, the gym, or on the road slows down or begins to reverse
Workouts, sporting events, physical activity that the body was able to bounce back from quite easily now take twice as long to recover from
Things start to change when the body enters its 30’s. Whether light exercise, playing weekend games, local sports, etc, the key is to just stay active. By paying close attention to nutrition and making minor adjustments, individuals can maintain and improve body composition, stay strong and healthy in their 30s and be ready for the future.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
Self-cracking and popping the spine can feel good but should it be done without professional/chiropractic assistance? We’ve all done it getting up from bed or the couch, lean back, and wait for the sound of the spine cracking/popping. Some even have a friend help pop the spine to get that satisfying feeling. There are proper stretching techniques to follow, but cracking the spine without professional help is not recommended as it could lead to problems or worsen any underlying spinal issues.
Sounds
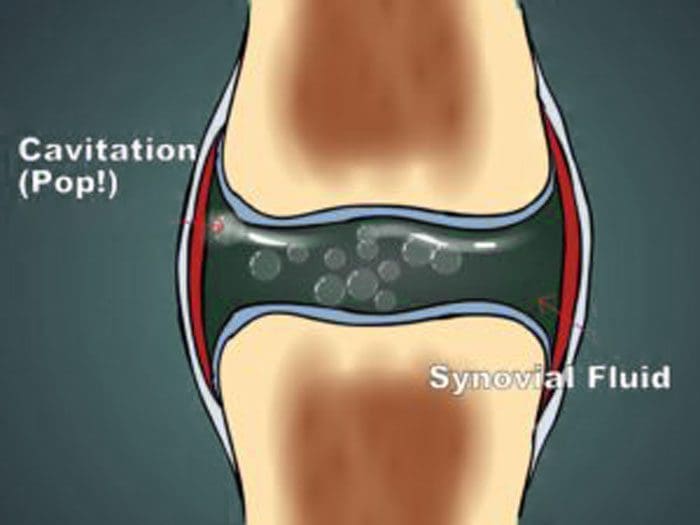
Self cracking, popping the spine refers to the sounds the neck or back make with certain movements. The joints in the spine contain fluid and gas. When the body moves, stretches can create cracking popping sounds as different pressures are exerted. The sound is known as joint cavitation, is the normal exchange of gases like oxygen, nitrogen, and carbon dioxide around the joints.
Spaces form in the synovial fluid that surrounds the joints. These spaces make an audible sound when the pressure changes/cavitation causing the gases to be released. The gases are naturally present in the body. A doctor of chiropractic mobilizes the joints very carefully through adjustments using their hands or specific instruments to increase the spine’s range of motion and stability. When adjustments and manipulations are not performed by a professional, problems can happen, that can include:
Loss of strength
Soft tissue swelling
Muscle spasms
When it’s done properly and safely injuries are prevented and any issues like swelling and tightness around the neck and spine are also avoided.
Self-cracking performed incorrectlycan lead to excessive force bringing the joints to excessive ranges of motion that can potentially cause injury. Individuals need to be careful even when self-cracking as the spine can make sounds for other reasons.
Age-related arthritis can generate a crunching type of sound when moving known as crepitus
A ligament or tendon can rub over a bone or bone spur, creating different sounds
These sounds are usually not problematic, but when they are consistent with certain movements they could cause inflammation and/or pain.
Chiropractic Professional Adjustments
The primary reasons most individuals seek chiropractic help are for problems, like pain, tightness, and weakness. Individuals can voluntarily see a chiropractor or they could be referred to one by a different doctor. Doctors routinely work with chiropractors to help patients recover from musculoskeletal injuries and conditions. A chiropractor performs manipulations in a safe, controlled manner. They are familiar with the sounds that the joints make and know they are safe. They usually have a multidisciplinary team that is involved in the management of various musculoskeletal conditions.
Why chiropractic care is so helpful?
All doctors of chiropractic are trained to diagnose and treat neuro-musculoskeletal conditions. During the diagnosis, the chiropractor will go through the individual’s medical history and conduct a physical exam to determine what treatment plan is best for the individual and their injury or condition. Many are now flocking to chiropractic care to avoid taking pain medications. Scientific evidence supports the health benefits of adjustments for various types of musculoskeletal pain, as well as to improve function and mobility
It is also recommended to work with a chiropractor in addition to other health professionals, like orthopedic specialists and physical therapists. They can help decrease pain, provide increased mobility and stability. If there is a constant need to self crack the back, or are having other issues with pain and tightness, talk with a doctor to see if chiropractic adjustments and manipulation will help. This will ensure that the right diagnosis is made and will help to create the optimal treatment plan to develop a stronger healthier body.
Body Composition
Increasing muscle mass is a recommended way to improve body composition and increase immune system function. Research shows senior adults with a higher skeletal muscle mass have an increased number of immune cellsin the blood. This indicates that the muscles and the immune system are connected. When working out myokines or hormone-type proteins are released that strengthen the immune system to help protect and fight diseases. Regular exercise with moderate intensity increases the release of T lymphocytes/T cells improving the body’s immunity. Regular exercise also helps reduce the risk of developing chronic diseases like:
Type 2 diabetes
Obesity
Different types of cancer
Cardiovascular diseases
Improved body composition with regular exercise and a well-balanced diet helps maintain a healthy proportion of muscle and fat mass. The more developed the body’s muscle mass becomes strengthens the immune system and lowers the risk of diseases and various health conditions.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP, CIFM, CTG* email: [email protected] phone: 915-850-0900 Licensed in Texas & New Mexico
“The Prevalence, Patterns, and Predictors of Chiropractic Use Among US Adults: Results From the 2012 National Health Interview Survey.” Spine. Dec 2017. https://pubmed.ncbi.nlm.nih.gov/28459779/
“Chiropractic Use in the Medicare Population: Prevalence, Patterns, and Associations With 1-Year Changes in Health and Satisfaction With Care.” Journal of Manipulative and Physiological Therapeutics. Oct 2014. https://www.sciencedirect.com/science/article/pii/S0161475414001444
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine