About 6 million people in the United States have Alzheimer�s disease (AD) and about 50 million people worldwide have dementia. There aren’t many treatments to treat these neurological diseases. Scientists in a 2018 research study on red light therapy and mice described that �treatment for Alzheimer�s disease and dementia has not been effective for more than 100 years.� Another research study described that there is currently “no treatment to prevent brain health issues. �
However, research studies on red light therapy as a treatment for Alzheimer�s disease and dementia have been positive over the last few years in laboratory settings with rodent models. Based on this lab data, researchers recommend red light therapy and near-infrared light therapy in human patients with AD and dementia. In this article, we will look at what the initial human research studies on red light therapy and Alzheimer�s disease/dementia have shown over the last few years. �
Red Light Therapy for Alzheimer�s and Dementia
The first few double-blinded, placebo-controlled human trials on red light therapy for AD, dementia, and other neurological diseases published in 2017 had very positive results. The data showed that red light therapy caused changes in executive function, clock drawing, immediate recall, memory, visual attention, and task switching, among other positive results. One research study showed that patients treated with transcranial light therapy experienced improvements, such as: �
Increased cognitive function
Better sleep
Fewer angry outbursts
Less anxiety
Less wandering
The research study noted that there were �no negative side-effects� on transcranial light therapy for neurological diseases. The research study concluded that transcranial light therapy shows potential for the treatment of brain health issues. �
More Human Trials with Red Light Therapy in Progress
The results of these initial human trials are encouraging for Alzheimer’s disease and dementia patients and families looking for better treatment options, especially natural and non-invasive treatments with no drugs/medications or side effects. �
In early 2019, three more human trials on red light therapy and AD/dementia have been in progress at the University of California and a hospital system in France. With the previous positive results, more and larger research studies and human trials are being organized. Scientists hope that in the following years, the base of positive evidence will be large enough to recommend red light therapy as a treatment for Alzheimer�s disease and dementia, among other neurological diseases. �
The results from human trials over the last few years have established a much bigger base of similarly positive results from research studies of rodent brains in Alzheimer�s disease and dementia models, both of which are outlined below. �
Red Light Therapy Reduces Oxidative Stress and Improves Memory
A 2018 research study of mice in an age-related AD/dementia model showed that red light therapy considerably reduced oxidative stress levels and restored memory function. The researchers also praised red light therapy for being a non-invasive treatment option as well as having a high rate of tissue penetration and low phototoxicity. The researchers additionally found that red light therapy not only prevented early-stage memory decline but also recovered late-stage memory deficits. �
Researchers in a similar 2015 research study with a mouse AD/dementia model utilized near-infrared (NIR) light instead of red light therapy. The NIR treatments also reduced oxidative stress in the cerebellar cortex. The researchers concluded that NIR treatments had the ability to prevent brain degeneration in every region of the mouse brain. The research studies concluded that light therapy opens a promising opportunity to translate LED-therapy into treatments for patients. �
Red Light Therapy Prevents Brain Degeneration
Several research studies have shown that red light therapy can suppress the buildup of Beta-amyloid (A?), a protein which causes senile plaques in people with Alzheimer�s disease and dementia. Synaptic dysfunction, due to the disruptive binding of (A?) in the brain, is one of the symptoms of AD and dementia responsible for causing initial cognitive decline. Preventing synaptic dysfunction can be an effective treatment for AD and dementia, helping to regulate and manage symptoms. �
Red Light Therapy Improves Memory, Motor Skills, and Recognition
Research studies in 2017 evaluated the hippocampus of rat brains in an Alzheimer�s model with light therapy. Both research studies considerably reduced A? plaques in the rats treated with light therapy. Both research studies also tested the subjects and found that treatments reduced hippocampal neurodegeneration and improved spatial memory, recognition, and basic motor skills in the light therapy groups. Another research study also showed considerable A? reduction and noted that NIR light can reduce synaptic dysfunction from A?, showing that NIR light therapy is a viable treatment for AD and dementia. �
Red Light Therapy Shows Promise for Neurological Diseases
The initial research studies on red light therapy for Alzheimer�s disease and dementia have ultimately been encouraging for researchers. Red light therapy is not FDA-approved for the treatment of Alzheimer�s Disease or dementia, however, there is hope that more positive results in human trials will show that light therapy is fundamental for AD and dementia treatment. �
Based on the available base of positive evidence, however, red light therapy shows promise as a natural, non-invasive, drug/medication-free treatment for brain degeneration where pharmacological solutions have long failed. �
By reducing oxidative stress and preventing the accumulation of the Beta-amyloid which causes brain plaques and synapse dysfunction, red light therapy offers hope towards delaying the onset of Alzheimer�s disease and dementia symptoms as well as hopefully even reversing or preventing brain degeneration and cognitive function decline. Researchers, patients, and families affected by AD and dementia will be watching closely in the following years as more positive results emerge. �
Research studies have demonstrated positive results on red light therapy for Alzheimer’s disease and dementia. Initial research studies on mice and rat models have shown the effects of light therapy on neurological diseases. Although, more human trials are still necessary to establish the effectiveness of red light therapy for AD and dementia, the base positive results are promising. Many healthcare professionals can help treat the symptoms associated with a variety of neurological diseases, among other health issues. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Research studies on red light therapy for AD and dementia have been positive over the last years. The initial human research studies on red light therapy and Alzheimer�s disease/dementia have been promising. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
The human brain comprises approximately billions of small cells that utilize electrical impulses and chemical signals to communicate with one another and other parts of the human body. These are known as neurons. When neurons stop functioning properly, it can cause various brain disorders, such as Alzheimer’s disease, epilepsy, and even depression.
Researchers developed several treatment methods and techniques of brain stimulation which allow them to control neural activity to understand better and regulate these type of health issues. In conventional treatment methods and techniques of deep brain stimulation, electrical neurostimulators, also known as brain pacemakers, are surgically implanted in the brain.
Researchers also developed non-invasive treatment approaches to stimulate cells found deep within the brain. While several researchers utilize magnetic pulses or sound waves to stimulate neurons, researchers in optogenetics utilize light therapy. Shuo Chen, Ph.D., winner of Science and PINS Prize for Neuromodulation, was recognized for his work in this area.
Dr. Chen demonstrated that near-infrared light, when utilized with certain nanoparticles, allowed the stimulation of neurons deep within the brain, stated Dr. Karl Deisseroth, professor of bioengineering, psychiatry, and behavioral sciences at Stanford University. More research studies are needed to make this a useful process, he said, but Dr. Chen took a key step.
Developing Light-Sensitive Neurons
Dr. Karl Deisseroth, one of the leading pioneers of optogenetics, developed a treatment method or technique in which the brain cells or neurons are genetically engineered to respond to light therapy. Through this method or technique of brain stimulation, researchers transmit fragments of genetic codes from algae and other microbes into the brain cells of mice and other animals. That genetic code ultimately causes neurons to produce light-responsive proteins known as opsins.
When opsin-producing neurons are exposed to specific wavelengths of visible-spectrum light, those brain cells turn on or off. By activating or suppressing the neurons, researchers can learn more about the fundamental role of neurons in brain function and brain disorders. Dr. Karl Deisseroth has also demonstrated the effects of developing light-sensitive neurons.
By developing light-sensitive brain cells, the causal role of cellular activity can be determined in the tissue and the behavior of interest of any species, ranging from memory to mood, stated Dr. Deisseroth. Furthermore, optogenetics brings the unmatched capability for speaking the brain’s natural language regarding cell-type specificity and speed, he added.
Developing Non-Invasive Treatment Approaches
Opsin-producing neurons, however, respond to visible-spectrum light which cant penetrate brain tissue. Therefore, optogenetic stimulation required the insertion of fiber-optic light sources inside the brain to stimulate neurons. Dr. Deisseroth and his colleague Polina Anikeeva, Ph.D., developed the utilization of near-infrared (NIR) light, a non-invasive type of light therapy.
NIR light can ultimately penetrate through the skull and brain tissue without inserting internal light sources inside the brain. However, NIR light also doesn’t trigger a response from opsin-producing neurons. To promote the tissue-penetrating abilities of NIR light therapy, Dr. Karl Deisseroth and Dr. Anikeeva developed a treatment approach known as NIR upconversion, which coats opsin-producing neurons in nanoparticles to convert NIR light into visible-spectrum light.
Dr. Shuo Chen utilized this treatment method and technique, demonstrating for the first time that NIR upconversion optogenetics can ultimately be utilized to control neurons deep in the brains of mice. In addition, Dr. Chen’s research studies utilized this method and technique to stimulate the release of dopamine in a region of the brain believed to play a role in depression.
Overcoming the challenge of optical penetration depth will be the fundamental key to realizing non-invasive remote optogenetics with high clinical translation potential, wrote Dr. Chen in his prizewinning essay on the topic. Our research study utilized a nanomaterial-assisted approach that shifts the existing optogenetic tools into the near-infrared region.
Brain Stimulation for the Human Brain
While researchers continue to research optogenetics in mice and other animals, it hasn’t been utilized to treat brain disorders in humans. Furthermore, more research studies are required to develop and evaluate non-invasive methods of light therapy and non-invasive methods and techniques for transmitting genetic code into brain cells or neurons.
It is too soon to predict which treatment approach will emerge at the forefront of next-generation non-invasive brain stimulation technology, Dr. Chen said in a press release issued by the American Association for the Advancement of Science. However, we believe that a variety of fundamental achievements, such as NIR upconversion optogenetics, are quickly unlocking development pathways and paving the way towards a bright therapeutic future for brain diseases, he continued.
In the meantime, other methods and techniques of non-invasive brain stimulation are also being developed, evaluated, and utilized in humans. For example, transcranial magnetic stimulation (TMS) is a non-invasive treatment approach that utilized magnetic fields to stimulate nerve cells in the brain. The Food & Drug Administration (FDA) has already allowed TMS marketing as a treatment approach for major depression as well as obsessive-compulsive disorder and migraine headaches.
There are also several non-invasive methods and techniques which don’t require the utilization of gene therapies, such as transcranial magnetic and electrical stimulation, which are commonly utilized with human subjects on an experimental, regular basis, stated Ed Boyden, Ph.D., a professor of neurotechnology at the Massachusetts Institute of Technology (MIT).
Members of Boyden”s research study group have also conducted research studies on transcranial electric stimulation (TES), a non-invasive treatment approach to brain stimulation in which electrodes are placed on the scalp. Researchers hope for this method and technique to reach neurons or cells deep within brain tissue with greater precision than TMS.
Although research studies have demonstrated that light therapy can stimulate brain cells or neurons of mice and other animals, urther research studies are required to determine how light therapy treatment methods and techniques can stimulate the human brain. According to these same research studies, light therapy can alter neurons or brain cells which can ultimately cause Alzheimers disease, epilepsy, and other brain diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The human brain consists of billions of small cells or neurons which communicate with one another and other parts of the human body. When neurons stop functioning properly, it can cause a variety of brain disorders. Researchers have developed a variety of light therapy treatment approaches to help stimulate the brain ultimately. The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals; however, chronic pain is different from the average pain type. The human body will continue sending pain signals to the brain with chronic pain, regardless of the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility, reducing flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual’s reactivity to 48 neurological antigens with connections to various neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
According to research studies, transcranial infrared laser stimulation, as well as other types of transcranial lasers, utilized on frontal cortex functions can improve sustained attention and working memory, among other brain functions. Transcranial laser stimulation with low-power density (mW/cm2) and high-energy density (J/cm2) monochromatic light in the near-infrared wavelengths regulates and maintains brain functions and may promote neurotherapeutic effects in a non-destructive and non-thermal manner. Researchers determined through the first controlled research study that transcranial laser stimulation improves human cognitive and emotional brain functions. �
In the field of low-level light/laser therapy or LLLT, developing a model to demonstrate how luminous energy from red-to-near-infrared wavelengths improves bioenergetics has been in development for the last 40 years. Previous LLLT research studies have demonstrated historical a variety of developments, principles and applications on the subject matter. The purpose of the following article is to demonstrate an update on LLLT’s neurochemical mechanisms supporting transcranial laser stimulation for cognitive-enhancing functions. We will describe the effect of LLLT on brain bioenergetics, briefly discussing its bioavailability and dose-response, and its effects on cognitive brain function. Although our focus is on prefrontal-related cognitive functions, LLLT should be able to improve other brain functions. By way of instance, stimulating different brain regions affect different functions associated with sensory and motor systems. �
Transcranial Lasers on Brain Bioenergetics
Near-infrared lasers and light-emitting diodes, or LEDs, affect brain function according to bioenergetics, a mechanism which is fundamentally different than other brain stimulation methods and techniques, such as electric and magnetic stimulation. LLLT has been demonstrated to regulate and maintain the function of neurons in cell cultures, and brain function in animals as well as cognitive and emotional functions in patients and health issues. Photoneuromodulation is associated with the absorption of photons by certain molecules in neurons which activate bioenergetic signaling pathways after being exposed to red-to-near-infrared light. The 600mm to 1150 nm wavelengths provide improved tissue penetration by photons because light is scattered at lower wavelengths and absorbed by water at higher wavelengths. Over 25 years ago, it was demonstrated that molecules which absorb LLLT wavelengths are part of the mitochondrial respiratory enzyme cytochrome oxidase in different oxidation states. Moreover, for red-to-near-infrared light, the main molecular photoacceptor of photon energy is cytochrome oxidase, also known as cytochrome c oxidase or cytochrome a-a3. �
Furthermore, photon energy absorption by cytochrome oxidase is the main neurochemical mechanism of action of LLLT in neurons. The more the enzymatic activity of cytochrome oxidase increases, the more metabolic energy which is developed through mitochondrial oxidative phosphorylation. LLLT provides the brain with metabolic energy in an analogous manner to the conversion of nutrients into metabolic energy with the utilization of light instead of nutrients developing the source for ATP-based metabolic energy. If an effective near-infrared light energy dose is provided, it stimulates brain ATP production and blood flow, ultimately fueling ATP-dependent membrane ion pumps, promoting greater membrane stability and resistance to depolarization, which has been demonstrated to transiently reduce neuronal excitability. Electromagnetic stimulation also directly affects the electrical excitability of neurons, as demonstrated in research studies. �
A long-lasting effect is provided by LLLT’s up-regulating the amount of cytochrome oxidase, which improved neuronal capacity for metabolic energy production which can be utilized to improve cognitive brain functions. In mice and rats, memory has been demonstrated to improve by LLLT and by methylene blue, a drug, which at low doses, provides electrons to cytochrome oxidase. Near-infrared light stimulates mitochondrial respiration by providing photons to cytochrome oxidase because cytochrome oxidase mainly accepts photons from red-to-near-infrared light in neurons. By stimulating cytochrome oxidase activity, transcranial LLLT promotes post-stimulation up-regulation of the amount of cytochrome oxidase in brain mitochondria. LLLT may also improve the conversion of luminous energy into metabolic energy during light exposure as well as the up-regulation of the mitochondrial enzymatic machinery to develop more energy after light exposure. �
Bioavailability and Hormetic Dose-Response by Transcranial Lasers
The most numerous metalloprotein found in nerve tissue is cytochrome oxidase and its absorption wavelengths are often associated with its enzymatic activity and ATP production. Increased LLLT bioavailability to the brain in vivo has been demonstrated in a variety of research studies by exposing brain cytochrome oxidase activity transcranially, resulting in improved extinction memory retention in healthy rats and improved visual discrimination in rats with impaired retinal mitochondrial function. Other LLLT research studies utilized a variety of wavelengths (633�1064 nm), daily doses (1�60 J/cm2), fractionation sessions (1�6), and power densities (2�250 mW/cm2) which ultimately characterized effective LLLT parameters for both rats and humans. �
By way of instance, researchers evaluated in rats the effects of different LLLT doses in vivo on brain cytochrome oxidase activity, at either 10.9, 21.6, 32.9 J/cm2, or no LLLT. Treatments were utilized for 20, 40, and 60 min through four 660-nm LED arrays with a power density of 9 mW/cm2. One day after the LLLT session, the brains of the rats were extracted, frozen, sectioned, and processed for cytochrome oxidase histochemistry. A 10.9 J/cm2 dose increased cytochrome oxidase activity by 13.6 percent. A 21.6 J/cm2 dose developed a 10.3 percent increase. A non-significant cytochrome oxidase increase of 3 percent was found after the highest 32.9 J/cm2 dose. Responses of brain cytochrome oxidase to LLLT in vivo were characterized by hormesis, with a low dose being stimulatory while higher doses were less effective. �
The first demonstration that LLLT increased oxygen consumption in the rat prefrontal cortex in vivo was demonstrated by another research study. Oxygen concentration in the cortex of rats was measured utilizing fluorescence-quenching during LLLT at 9 mW/cm2 and 660 nm. LLLT promoted a dose-dependent increase in oxygen consumption of 5 percent after 1 J/cm2 and 16 percent after 5 J/cm2. Because oxygen is utilized to develop water within mitochondria in a response developed by cytochrome oxidase, more cytochrome oxidase activity should promote more oxygen consumption. �
LLLT can also offer several benefits over other types of stimulation because LLLT non-invasively targets cytochrome oxidase, a fundamental enzyme utilized for energy production, with promoted expression associated with energy increase. LLLT is mechanistically specific and non-invasive while transcranial magnetic stimulation may be non-specific, prolonged forehead electrical stimulation may increase muscle spasms and deep brain or vagus nerve stimulations are invasive. �
Transcranial Lasers on Cognitive and Emotional Functions
LLLT through commercial low-power sources, such as FDA-cleared laser diodes and LEDs, is a highly promising, affordable, non-pharmacological alternative treatment option for improving cognitive brain function. LLLT offers safe doses of light energy which regulate and maintain neuronal functions, however, these are low enough to not damage the brain. In 2002, the FDA approved LLLT for pain relief in cases of head and neck pain, arthritis and carpal tunnel syndrome. LLLT has been utilized non-invasively in humans after ischemic stroke to improve neurological functions. It also improved recovery and ultimately reduced fatigue after exercise. One LLLT stimulation session to the forehead, as demonstrated in another research study, developed a considerable antidepressant effect in patients with depression. No adverse side effects were found either immediately nor at 2 or 4 weeks after LLLT. Therefore, LLLT treatments have been demonstrated to be safe and effective in humans. Although LLLT has been determined to be safe and it received FDA approval to be utilized for pain treatment, transcranial lasers for the augmentation of cognitive brain function should be limited for further research studies until further outcome measures support this application for clinical utilization. �
Transcranial laser stimulation to the forehead was utilized in a placebo-controlled, randomized research study, to demonstrate the effects of cognitive tasks associated with the prefrontal cortex, including a psychomotor vigilance task, or PVT, and a delayed match-to-sample, or DMS, memory task. The PVT evaluates sustained attention, with patients remaining vigilant during delay intervals, and pushing a button when visual stimulation appeared on a monitor. The laser stimulation targeted prefrontal regions which are believed to be utilized in the sustained attentional processes of the PVT. The DMS task supports the prefrontal cortex as part of a network of frontal and parietal brain regions. �
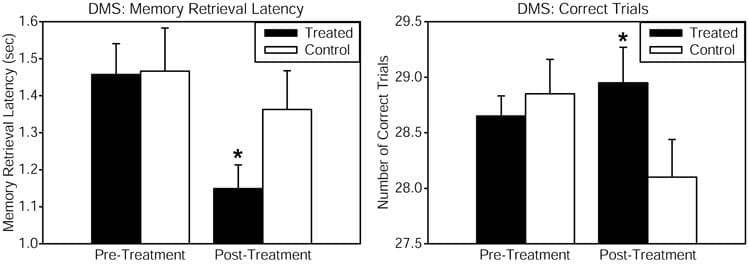
Healthy patients received consistent wave near-infrared light intersecting cytochrome oxidase’s absorption spectrum, targetted to the forehead utilizing a 1064 nm low-power laser diode, also known as �cold laser�, which increases tissue penetration due to its long wavelength and has been utilized in humans for other health issues. The power density or irradiance, 250 mW/cm2, and the cumulative energy density or fluence, 60 J/cm2, were identical which demonstrated the benefits of psychological effects in another research study. This laser exposure develops negligible heat and no physical damage at the low power level utilized. This laser apparatus is utilized safely in a clinical setting by the supplier of the laser. Reaction time in the PVT was improved by the laser treatment, as demonstrated by a considerable pre-post reaction time effect associated with the placebo group. The DMS memory task also demonstrated considerable improvements in measures of memory retrieval latency and number of correct trials, when comparing the LLLT-treated with the placebo group as demonstrated in Figure 1. Self-reported positive and negative affective or emotional states were also measured utilizing the PANAS-X questionnaire before and 2 weeks after laser treatment. As compared to the placebo, treated patients demonstrated considerably improved affective states. We suggest that this type of transcranial laser stimulation may serve as a non-invasive and efficacious method and technique to augment cognitive brain functions associated with attention, memory, and emotional functions. �
Figure 1. Cognitive performance in the delayed match-to-sample (DMS) memory task was improved after transcranial infrared stimulation to the right forehead. The DMS task involves presentation of a visual stimulus (grid pattern) on a screen. Then the stimulus disappears, and the participant must remember the stimulus through a delay. Then two choices appear, and the participant must decide which of these two is identical to the previous stimulus (the �match�). Treated subjects showed faster memory retrieval (left panel) and increased number of correct trials (right panel) out of 30 trials when attempting to choose the correct grid pattern. The function of frontal cortex regions, implicated in the attentional mode network utilized during this visuospatial memory task, was augmented by the laser treatment. Compared to baseline, this treatment also increased by 5% the oxyhemoglobin concentration of the prefrontal cortex as measured by near-infrared spectroscopy, both during the laser stimulation and during post-treatment DMS performance (in preparation). The data for the treated group consisted of n = 10 males and n = 10 females; the control group also consisted of n = 10 males and n = 10 females. *Significant treatment by pre-post score interaction, p < 0.05.
LLLT’s bioenergetics mechanisms associated with cognitive augmentation may also be associated in its neuroprotective effects. LLLT’s stimulation of mitochondrial respiration should improve cellular function due to increased metabolic energy and cellular survival after injury due to the antioxidant effects of increases in cytochrome oxidase and superoxide dismutase. �
Laser transmittance of the 1064-nm wavelength at the forehead LLLT site was estimated in a post-mortem human specimen, which demonstrated that approximately 2 percent of the light passed through the frontal bone. This yielded an absorption coefficient of a = 0.24, similar to the demonstrated a = 0.22 transmittance through cranial bone for this wavelength. Furthermore, it was estimated that about 1.2 J/cm2 of the 60 J/cm2 LLLT dose applied reached the surface of the prefrontal cortex. This value is similar to 1 J/cm2, the peak effective LLLT dose in neuron cultures for increasing cytochrome oxidase activity. �
Transcranial absorption of photon energy by cytochrome oxidase, the terminal enzyme in mitochondrial respiration, is associated as the bioenergetic mechanism of action of LLLT in the brain. Transcranial LLLT up-regulates cortical cytochrome oxidase and improves oxidative phosphorylation. LLLT improves prefrontal cortex-related cognitive functions, such as sustained attention, extinction memory, working memory, and affective state. Transcranial infrared stimulation may be utilized effectively to support neuronal mitochondrial respiration as a new non-invasive, cognition-improving intervention in animals and humans. This fascinating new treatment approach should also be able to affect other brain functions associated with the neuroanatomical site stimulated and the stimulation parameters utilized. �
Low-level laser therapy, or LLLT, and other types of transcranial lasers are non-invasive, low-powered lasers which are now being utilized in specific cortical regions of the brain to improve physiological responses and cognitive function. Many research studies have demonstrated that transcranial lasers can ultimately improve attention, memory, and reactions, where many other research studies have also demonstrated that these can also help improve depression and possibly even Alzheimer’s disease. Although further research studies are still required, the outcome measures are promising. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
According to research studies, transcranial infrared laser stimulation, as well as other types of transcranial lasers, utilized on frontal cortex functions can improve sustained attention and working memory, among other brain functions. Transcranial laser stimulation regulates and maintains brain functions and may promote neurotherapeutic effects in a non-destructive and non-thermal manner. Researchers determined through the first controlled research study that transcranial laser stimulation improves human cognitive and emotional brain functions. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
�
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
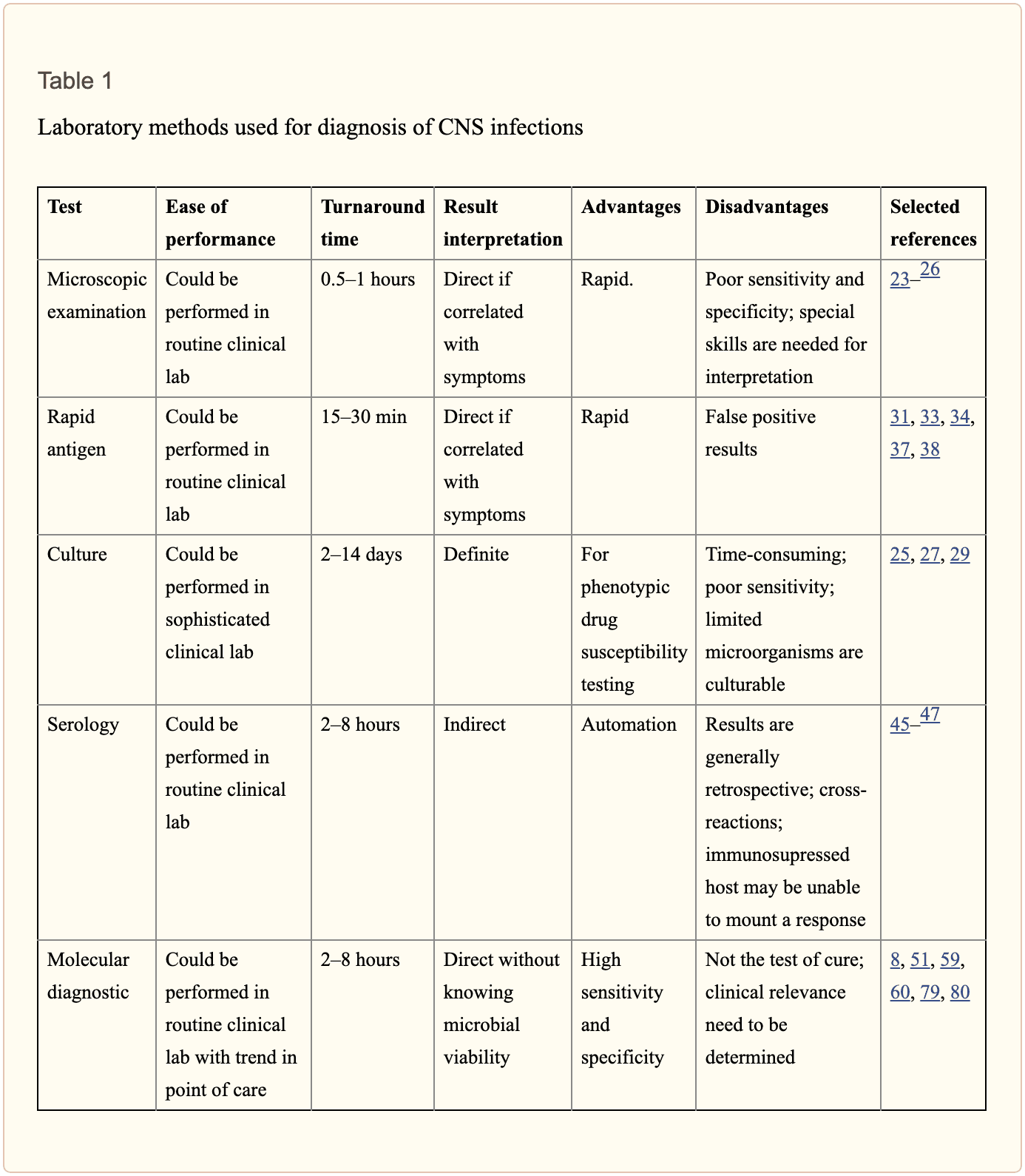
Central nervous system, or CNS, infections can be life-threatening if they are not diagnosed and treated early. Because CNS infections are non-specific, determining an accurate diagnosis can be challenging. The nucleic acid in vitro amplification-based molecular methods are starting to be utilized for routine microbial diagnosis. These molecular methods have improved beyond conventional diagnostic techniques with increased sensitivity and specificity. Moreover, molecular methods utilized on cerebrospinal fluid samples are considered the new standard for diagnosis of CNS infections caused by pathogens. �
Molecular methods for the diagnosis of CNS infections offers a variety of monoplex and multiplex PCR assays to diagnose several types of health issues. Pan-omic molecular platforms can also help diagnose CNS infections. Although molecular methods are utilized for the diagnosis of CNS infections, the outcome measures for these diagnostic techniques must be carefully identified by healthcare professionals. The following article discusses conventional diagnostic techniques and molecular methods utilized for the diagnosis of central nervous system infections, their application, and future approaches. �
Molecular Methods in the Diagnosis of CNS Infections
Because of increased sensitivity and specificity, nucleic acid in vitro amplification-based molecular methods has tremendously improved the ability to diagnose CNS infections in a reasonable and effective time frame. Several PCR-derived techniques have also ultimately increased the flexibility and rigor of currently available diagnostic techniques. �
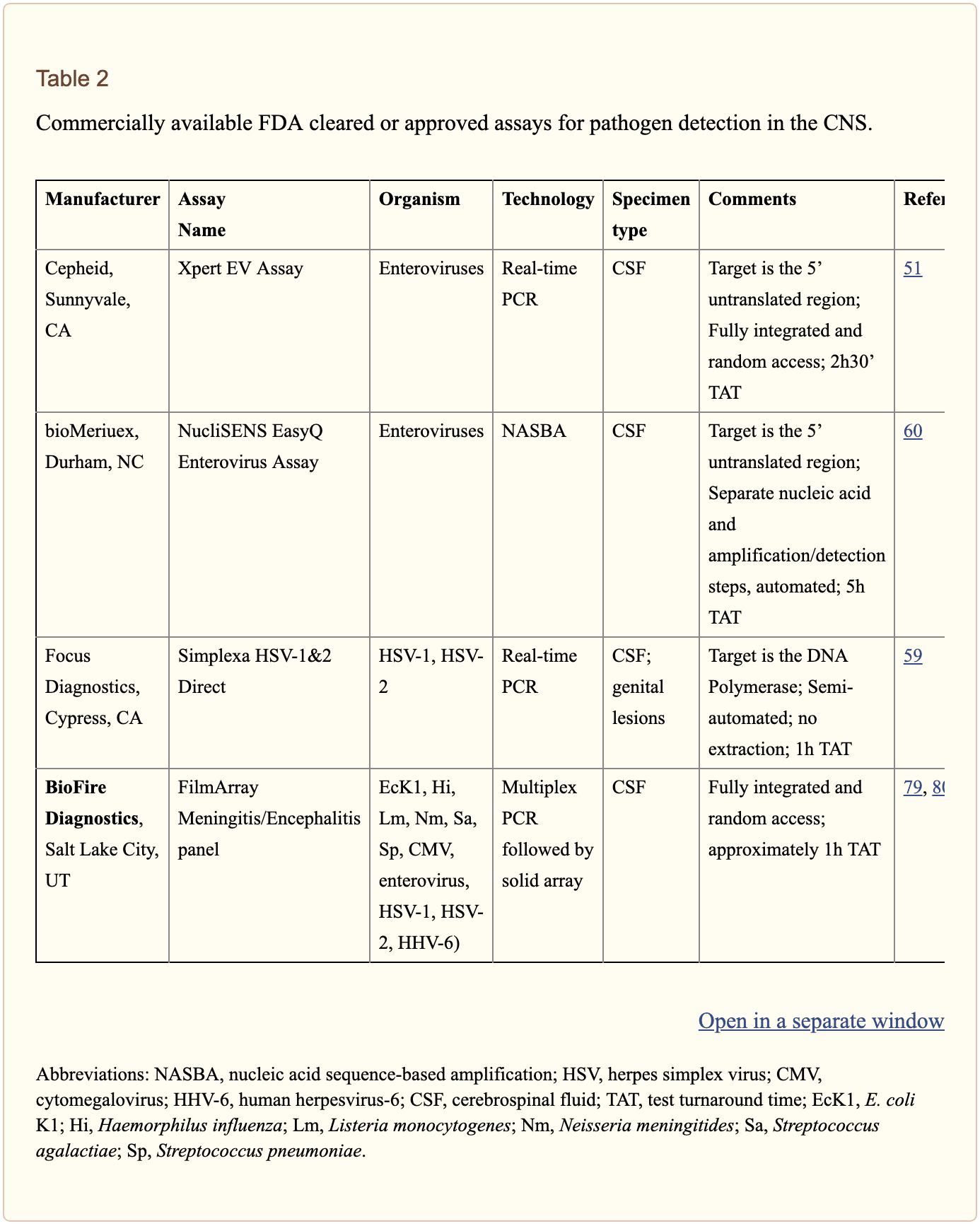
Reverse transcriptase, or RT,-PCR was developed to increase RNA targets. Its utilization plays a fundamental role in the diagnosis of RNA-virus infections as well as managing their reaction to treatment. Timely access to enterovirus RT-PCR outcome measures has demonstrated shorter hospital stays, reduced unnecessary antibiotic utilization, and decreased ancillary laboratory evaluations and tests. Broad-range rRNA PCR techniques, which utilize a single pair of primers targeting conserved regions of genes, have been utilized to diagnose bacterial pathogens and herpes viruses in the CSF. Isothermal amplification-based techniques. including loop-mediated isothermal amplification or LAMP, have been developed to offer a diagnosis within several minutes to hours. Table 2 demonstrates commercial molecular in vitro diagnostic devices, or IVD, which have been cleared by the US Food and Drug Administration, or FDA, for diagnosis of microbial pathogens in CSF. �
Monoplex Assays
A conventional molecular method involves three phases: sample extraction, target nucleic acid amplification, and amplicon detection. One of the first molecular assays successfully utilized for the diagnosis of CNS infections was utilized for the diagnosis of HSV in cerebrospinal fluid or CSF. PCR became the test of choice when research studies demonstrated that CSF PCR was similar to culture of brain tissue for diagnosis of HSV encephalitis and meningitis. Many PCR based methods for the diagnosis of herpes and enteroviruses have become available with increased sensitivity compared to viral culture. �
Real-time PCR with nucleic acid amplification and amplicon detection further improved the transition to molecular methods in clinical laboratories. Unlike conventional PCR, the real-time system is a �closed� system and it overcomes the fundamental problem of carryover contamination. At the time of manuscript preparation, three molecular assays utilized to help diagnose HSV and enteroviruses in CSF have ultimately been approved by the FDA as demonstrated in Table 2 of the previous article. � Real-time PCR-based methods are the main diagnostic technique utilized to help diagnose the Zika virus, which was first reported in Uganda in 1947, and is now a worldwide concern after the virus spread widely in Brazil and Central America. Research studies developed a one-step RT-PCR assay utilized to diagnose the Zika virus in human serum with a limited detection of 7.7pfu/reaction. Along with plasma, the Zika virus RNA can be diagnosed through urine and plasma within the first 2 weeks after symptoms have manifested. In March 2016, the FDA approved a trioplex-PCR assay under emergency use authorization for the simultaneous diagnosis of Zika, Chikungunya, and Dengue viruses in serum, urine, CSF and amniotic fluid. The RT-PCR assay utilizes dual labeled hydrolysis probes with a LOD of 1.54�10 4 GCE/ ml of Zika virus in serum. �
Introduction of real-time PCR based diagnostic assays have affected early and effective diagnosis of several bacterial infections. Isothermal amplification-based molecular assays have excellent performance characteristics and they don’t require any specialized equipment. These assays are fundamental for the utilization of on or near point-of-care testing. LAMP-based methods have been utilized to diagnose Neisseria meningitis, Streptococcus pneumoniae, Haemophilus influenzae type b, M. tuberculosis, and JEV in the CSF. The Xpert MTB/RIF assay has tremendously improved regulation of tuberculosis by offering an integrated and automated system which allows quick clinical decision making in a POC or near-care context. Several research studies have utilized the Xpert MTB/RIF to evaluate the diagnosis of M. tuberculosis in CSF from TB meningitis. In a meta-analysis of thirteen research studies, the pooled sensitivity of the Xpert assay was 80.5 percent, or 95 percent CI 59.0 percent to 92.2 percent, against culture and 62.8 percent, or 95 percent CI 47.7 percent to 75.8 percent, against composite standard. Utilizing a large volume of sample, of at least 8�10 ml, is necessary for testing CSF and centrifugation can cause considerable improvements in yield. Despite the lack of standardization for sample processing, WHO has allowed testing CSF with the automated Xpert MTB/RIF assay as the first-line test over conventional microscopy. �
Multiplex Assays
Simplicity makes multiplex molecular assays fundamental for the diagnosis of a panel of microbial targets. Several multiplex PCR assays have been developed to diagnose bacterial pathogens in CSF targeting the most common causes of meningitis: S. pneumoniae, N. meningitis, H. influenzae, L. monocytogenes, S. agalactiae, S. aureus, E. coli, and M. pneumoniae. A multiplex PCR followed by Luminex suspension array can simultaneously diagnose eight bacterial and viral pathogens in CSF, including N. meningitis, S. pueumoniae, E. coli, S. aureus, L. monocytogenes, S. agalactiae, HSV-1/2, and VZV, among others. �
Considering the variety of pathogens involved in CNS infection, application of comprehensive molecular panels with multiple bacterial and viral targets have improved the efficiency of diagnosis. The BioFire FilmArray Meningitis/Encephalitis panel is currently the only FDA cleared multiplex assay utilized for the diagnosis of six bacterial, such as Escherichia coli K1, Haemophilus influenzae, Listeria monocytogenes, Neisseria meningitides, Streptococcus agalactiae and Streptococcus pneumoniae, seven viral, such as cytomegalovirus, enterovirus, HSV-1, HSV-2, human herpesvirus 6 or HHV-6, human parechovirus and VZV, as well as a single fungal, such as Cryptococcus neoformans/gattii, target in CSF as demonstrated in Table 2. The integrated FilmArray system takes about an hour, with only 2 minutes of hands-on time. During the preparation of the manuscript, two research studies demonstrated the performance of this assay. Utilizing 48 samples from gram stain negative CSF samples from suspected cases of meningitis, research studies demonstrated that this system diagnosed more viral pathogens, such as EBV. Four cases of WNV and a single case of Histoplasma were not diagnosed by this assay. Among HIV infected patients in Uganda, the test performance demonstrated increased sensitivity and specificity for the diagnosis of Cryptococcus. Although the FilmArray Meningitis/Encephalitis panel offers a quick diagnosis of CNS infections, further research studies are needed to determine its performance for a variety of targets and other high-risk populations. �
Co-infections are frequently found among immunocompromised patients and can ultimately be challenging to diagnose for clinicians. The multiplex design allows simultaneous diagnosis of multiple targets on the same sample. One research study utilized a panel of monoplex and multiplex molecular assays to conduct a prospective cohort research study in Uganda to comprehensively evaluate the etiology of meningitis among HIV-infected adults. Among the 314 HIV-infected patients with meningitis, EBV co-infection was diagnosed with Cryptococcus, M. tuberculosis, or other viral pathogens. EBV in CSF in these settings is not completely understood although a single research study associated increased EBV viral load as a marker of poor outcome measures in patients with bacterial meningitis and EBV co-infection/ reactivation, among others. �
Pan-Omic Molecular Assays
Technological improvements in metagenomic deep sequencing have increased its utilization for clinical diagnosis of CNS infections. Several research studies have demonstrated its ability to solve diagnostic technique problems which challenge the limits of traditional laboratory testing. Due to sterile status and protection by BBB, CSF and brain biopsies are fundamental to further explore the utilization of this technology for pathogen diagnosis. Metagenomics was successfully utilized to establish a diagnosis of neuroleptospirosis in a 14-year-old boy with severe combined immunodeficiency who also suffered from recurrent bouts of fever, headache, and coma. Similarly, high-throughput RNA sequencing performed on brain biopsy from an 18-month-old boy with encephalopathy diagnosed a new Astrovirus as the cause. Despite the utilization of metagenomics for the diagnosis of infectious disease, there are many technological and practical concerns which need to be addressed before this form of diagnostic testing can become mainstream and part of the clinical standard of care. �
Other promising advances have occurred in transcriptomics, proteomics and metabolomics. Host and microbial microRNA or miRNA, profiles have been utilized for a variety of inflammatory and infectious diseases. Two miRNAs, miR-155 and miRNA-29b, were reported as potential biomarkers for JEV infection and treatment targets for anti-JEV therapy. Host neural epidermal growth factor, including 2 and apolipoprotein B in CSF, was able to diagnose tuberculous meningitis with 83.3 percent to 89.3 percent sensitivity and 75 percent to 92 percent specificity. CSF metabolite profiling has been reported to be useful in the classification, diagnosis, epidemiology, and treatment assessment of CNS infections in HIV patients. CSF metabolic profile analysis demonstrated bioenergetic adaptation in regulating shifts of HIV-infected patients. �
Outcome Measures Associated with Diseases
Diagnosis of an etiologic agent in patients with CNS infections needs consideration of the most common causative organisms, the available diagnostic techniques and molecular methods for these agents, and the highest-yield clinical specimens for evaluation and testing. Knowledge of the epidemiology and clinical presentation of specific agents is fundamental in selecting which diagnostic methods are appropriate for patients. Animal or vector exposures, geographic location, recent travel history, season of the year, exposure of ill contacts, and occupational exposures should be considered. �
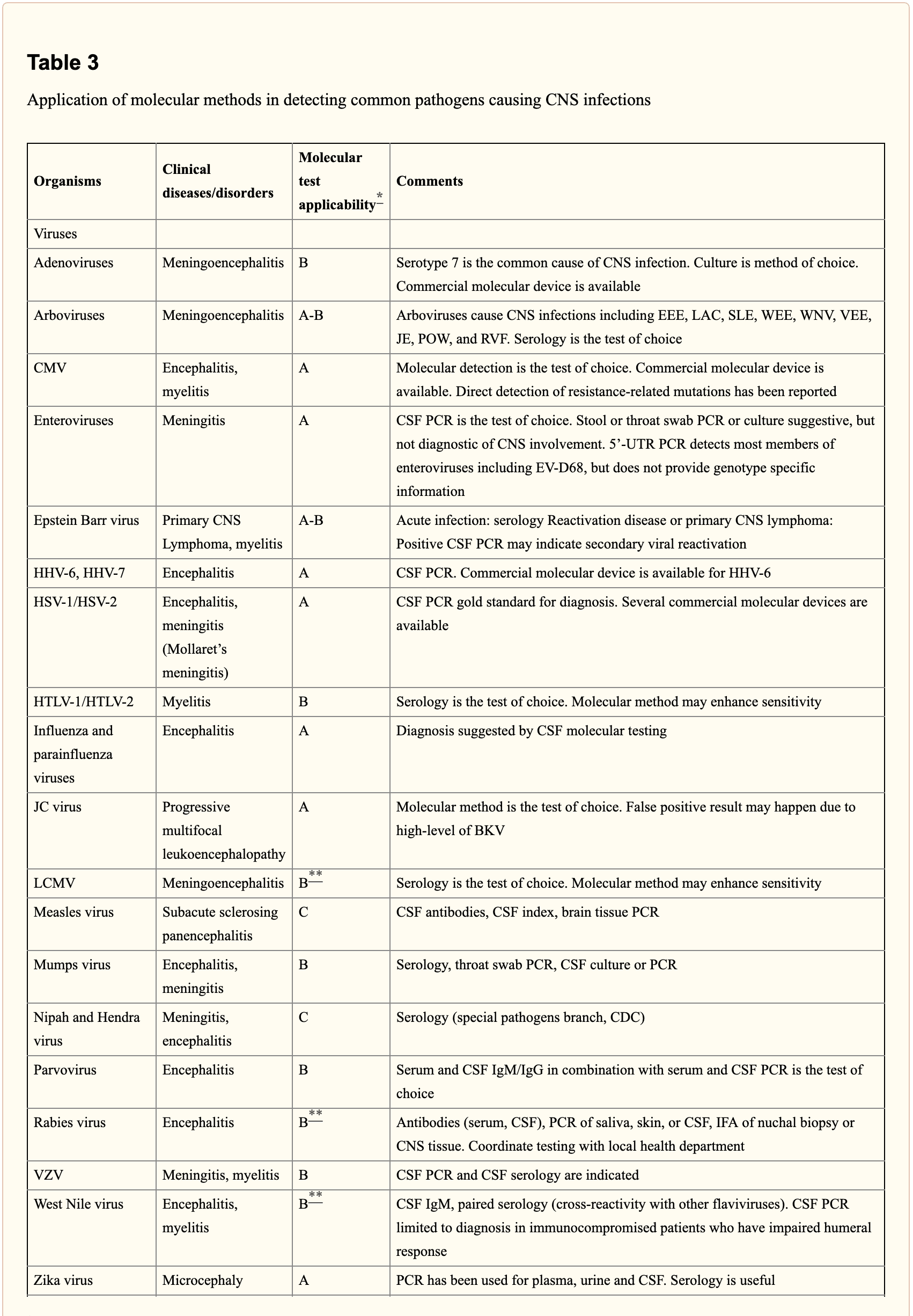
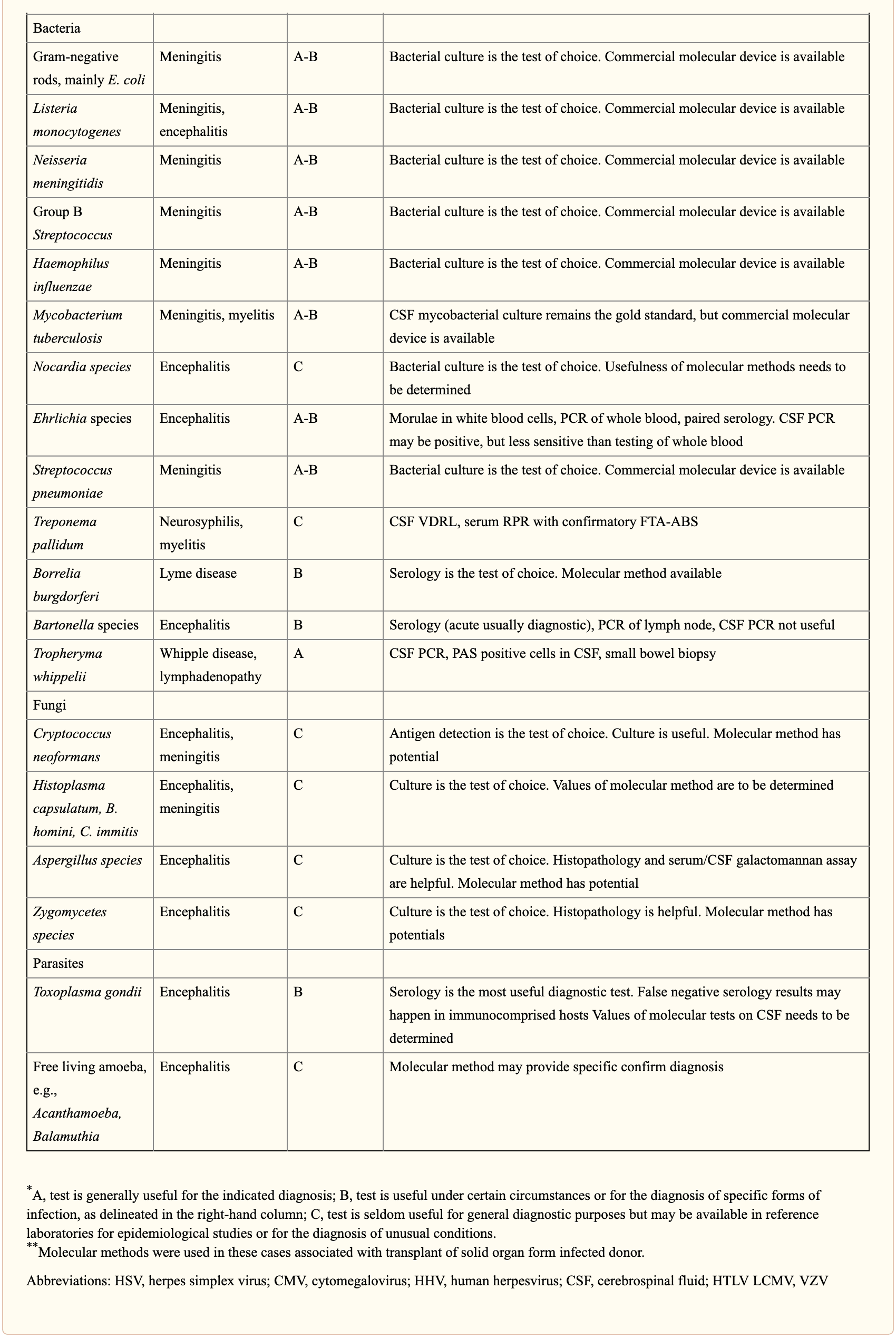
When selecting appropriate pathogen-specific molecular diagnostic methods, the following factors should be considered. CSF is the optimal specimen for PCR testing for patients with meningitis or meningoencephalitis. While indirect evidence can be determined by testing other specimen types, attempts should be made to obtain CSF samples early before treatment can compromise yield. Time of testing from the manifestation of symptoms is fundamental to understand and rule out false-negative results and recommend retesting within a certain time frame. By way of instance, HSV PCR can commonly render false-negative results if CSF sample is obtained very early or late in the process of HSE infection. Host health is also known to affect test performance characteristics. Immunocompromised patients are at risk for infection by a variety of opportunistic pathogens, by way of instance HHV-6, JC virus, Toxoplasma encephalitis in bone marrow transplant recipients and patients with HIV. Often, infection can be more severe, such as WNV, and challenging to diagnose in this population. Table 3 below demonstrates practical recommendations on application and pitfalls of molecular test for the diagnosis of CNS infections. �
Furthermore, a positive nucleic acid amplification testing results are considered to be complicated by the fact that some viruses survive latently in macrophages or neurologic tissues even if they’re incidentally diagnosed by sensitive molecular techniques without an actual pathogenic role which can potentially lead to overtreatment. Utilization of adjunctive biomarkers which help determine active replication is being explored to overcome this drawback in research studies. �
Historically, the diagnosis of microbiologic agents in patients with CNS infections has been hindered by the low yield of CSF culture for viral and fastidious bacterial organisms, delays in CNS production of organism-specific antibodies, and challenges in determining optimum samples for testing. The nucleic acid in vitro amplification-based molecular diagnostic methods and techniques have a wider and better application in clinical microbiology practice. The monoplex assay will likely be the main platform utilized for urgent, random-access, low throughput assays. Multiplex assays have the additional benefit of diagnosing multiple targets and mixed infections. As the volume of CSF sample retrieved is often small, multiplex assays enable comprehensive diagnostic analysis with a low amount of sample, obviating the need for repeated lumbar punctures. The clinical relevance and cost-effectiveness of simultaneous multi-pathogen diagnosis strategies need further research studies. Application of pan-omic techniques in challenging to diagnose CNS infections is the new exciting frontier, the technology is promising but routine implementation is expected to be slow due to various challenges, such as lack of applicable regulatory guidelines and adaptation in the clinical setting, although the outcome measures are promising. �
As previously mentioned, central nervous system, or CNS, infections can be life-threatening health issues if they are not accurately diagnosed and properly treated. However, determining a diagnosis of CNS infections can be challenging for many clinicians. Fortunately, a variety of diagnostic techniques and molecular methods can ultimately help determine the source of CNS infections and other health issues. These diagnostic techniques and molecular methods have tremendously improved over the years, as previously mentioned, and more of these evaluations are being utilized in clinical settings to accurately diagnose CNS infections for proper treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
In part 2 of our “Diagnosis of Central Nervous System Infections” article, we discussed the molecular methods and the pan-omic molecular assays which are utilized in the diagnosis of CNS infections as well as how specific testing outcome measures have ultimately been associated with clinical diseases and health issues. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
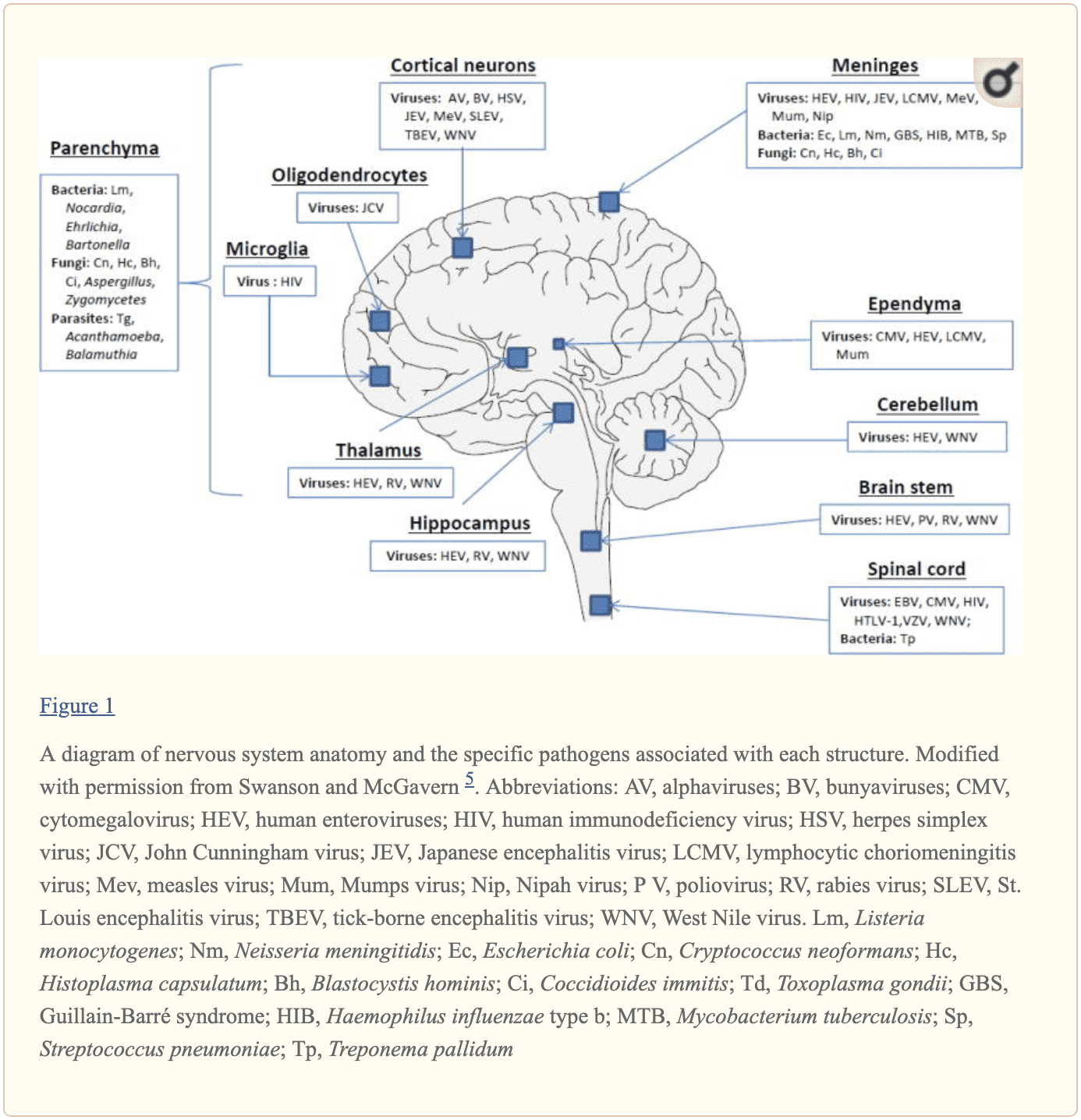
The central nervous system, or CNS, plays a fundamental role in the pathogenesis of infection. The CNS is regulated by the blood-brain barrier or BBB, however, it can still be exposed to a microbial invasion from a contiguous focus, hematogenous dissemination, or intraneural passage of organisms. A variety of environmental or commensal bacteria, viruses, fungi, protozoa, or parasites can enter the CNS and cause a variety of infections and health issues. Central nervous system infections can ultimately cause headache, stiff neck, vomiting, fever, photophobia, and focal neurological symptoms. �
What are Central Nervous System Infections?
CNS infections are characterized according to their affected region. Infection of the brain, spinal cord, and meninges results in meningitis, encephalitis, brain abscess, and myelitis. Infections can affect single or multiple regions of the brain, such as meningoencephalitis and encephalomyelitis. Moreover, CNS infections are characterized as acute, sub-acute, chronic, or recurrent based on their duration. Meningitis can cause headache, neck stiffness, fever, and photophobia over a period of hours to days. Encephalitis can cause brain parenchymal inflammation which can ultimately cause lethargy to coma. Last but not least, Myelitis can cause inflammation of the spinal cord including headache, fever, and paraparesis or paralysis. �
One of the most fatal CNS infections, acute bacterial meningitis, with three to five cases for every 100,000 people in the United States, has a mortality rate of 6 percent to 26 percent. Approximately 4,000 cases of acute bacterial meningitis occur in the U.S. every year with about 500 deaths. The frequent cause of acute bacterial meningitis includes Streptococcus pneumoniae, group B Streptococcus, Neisseria meningitides, Haemophilus influenzae, and Listeria monocytogenes. �
CNS infections caused by viruses are more common and are mostly mild and self-limited. However, these can manifest as meningitis and/or encephalitis. CNS infections caused by viruses can vary due to region and season. Non-polio enteroviruses are responsible for the majority of meningitis and/or encephalitis cases from late spring to fall. CNS infections due to herpes simplex viruses, or HSV, are associated with sporadic encephalitis and meningitis with severe sequelae if left untreated. �
Diagnosis of CNS Infections
Diagnosis of microbial pathogens is fundamental for treatment. Methods and techniques utilized in clinical microbiology laboratories include direct microscopic examination, and culture techniques as well as antigen and antibody detection assays. However, each method and technique has several essential limitations. By way of instance, direct microscopic examination of CSF restricted sensitivity and specificity. The sensitivity of culture for enteroviruses is between 65 percent to 75 percent with average retrieval time of 3.7 to 8.2 days. Moreover, several serotypes of enteroviruses, especially Coxsackievirus A strains, are well-known to be non-cultivable and frequently grow poorly. Because enteroviruses are missing a common antigen found throughout a variety of serotypes, universal antigen and/or antibody diagnosis is impossible. Diagnosis of CNS HSV infections through methods and techniques utilized to determine culture sensitivity from CSF is tremendously poor. The presence of HSV IgG antibodies in CSF can ultimately be utilized to determine a diagnosis, however, the production is delayed until day 10 or day 12 after infection and it is not considered ideal for early diagnosis.
Diagnostic techniques, especially PCR based amplification, have developed a variety of mainstay tools to help determine the diagnosis of microbial pathogens in CSF. Molecular methods have demonstrated greater diagnosis rates than other diagnostic techniques. One research study demonstrated that 16S rRNA PCR-based assays were able to diagnose the causative organism in 65 percent of banked CSF samples compared to 35 percent when utilizing culture and microscopy. In another research study, diagnosis based on diagnostic techniques like molecular methods were utilized to optimize antibiotic treatment of patients with infectious meningitis when conventional methods and techniques demonstrated a negative outcome measure. Molecular methods and diagnostic techniques utilized on CSF samples are a fundamental standard when compared to the culture standard in the diagnosis of CNS infections caused by viruses which are challenging to diagnose. �
The diagnosis of CNS infections has tremendously changed over the last several years. PCR-based molecular methods have become a fundamental element in the clinical microbiology laboratory, providing tools for an accurate diagnosis. As demonstrated in Table 2, a variety of commercial molecular assays have been cleared by the Food and Drug Administration, or FDA, for the diagnosis of microbial pathogens. The approved assays for pathogen detection in the CNS are shown below. �
However, there are still several challenges in molecular diagnostic techniques and methods. Utilizing a combination of conventional diagnostic techniques and molecular methods, research studies demonstrated that in approximately 62 percent of patients with encephalitis, an etiologic organism could not be identified. Researchers have started to focus on developing advanced techniques and methods. In the following series of articles, we will demonstrate an update on the current conventional and molecular platforms utilized for the diagnosis of CNS infections. We will also demonstrate a preview on the potential clinical application of future technologies, including pan-omic assays. The emphasis of the following series of articles is to demonstrate optimal test selection in the clinical scenario for the diagnosis of CNS infection. �
Conventional Microbiology Methods and Techniques
Microscopic Examination
A positive CSF Gram stain confirms the diagnosis of bacterial meningitis. The sensitivity of the Gram stain for the diagnosis of bacterial meningitis is approximately 60 percent to 80 percent in patients not on antimicrobial treatment and approximately 40 percent to 60 percent in patients on antibacterial treatment. In one research study, Gram stain diagnosed as much as 90 percent Streptococcus pneumoniae and 50 percent Listeria monocytogenes in CSF collected from patients with bacterial meningitis confirmed by PCR 26 techniques and methods. Two organisms which are frequently diagnosed by microscopy include Mycobacterium tuberculosis by acid-fast bacillus, or AFB, staining and Cryptococcus neoformans by India ink or Gram stain. However,� the sensitivities of these techniques and methods are poor and culture is generally utilized instead. �
Culture
Culture of brain tissue can demonstrate a positive diagnosis of CNS infections, however, getting biopsies are tremendously invasive and frequently avoided unless a clinician determines that they are absolutely necessary. CSF sampling is most commonly performed to diagnose CNS infection. CSF viral, bacterial, including mycobacterial, and fungal cultures are fundamental in the diagnosis of infectious meningitis. However, CSF cultures in these cases are extremely low. Another disadvantage of CSF bacterial culture is that it generally requires up to 72 hours to determine a final diagnosis. A recent research study demonstrated that CSF mycobacterial culture had a sensitivity of 22 percent and a specificity of 100 percent in the diagnosis of tuberculosis meningitis. For viruses, utilizing monoclonal antibodies through culture increased the speed and specificity. However, due to time and sensitivity, CSF viral culture is frequently unable to determine a diagnosis. �
Rapid Antigen Detection
Cryptococcal antigen is the most commonly utilized antigen assay for CNS infections. The test utilizes Cryptococcus capsular polysaccharide antigens in CSF through enzyme immunoassay to determine a diagnosis. In a single research study which evaluated patients less than 35 years of age with CNS cryptococcosis, overall sensitivity and specificity of 93 percent to 100 percent and 93 percent to 98 percent were shown. Cryptococcus is a neurotropic fungus. Polysaccharide serum antigen titers with host immune status are frequently utilized to determine the need for a lumbar puncture to evaluate the patient for CNS health issues. The baseline peak titer of polysaccharide antigen in serum or CSF has demonstrated fundamental prognostic significance with an increased titer, or peak titer less than 1:1024, associated with antifungal therapy failure. �
The diagnosis of galactomannan, or GM, antigen and 1,3 ?-D-glucan, or BDG, in CSF, can help in the diagnosis of CNS aspergillosis or other invasive fungal infection such as fusariosis. Increased BDG in serum and CSF is associated with fungal infections. Measuring the levels of BDG is a beneficial biomarker in the evaluation of fungal CNS infection. It was recently demonstrated that patients receiving effective antifungal therapy demonstrated a decrease in CSF BDG concentrations with less than 31pg/ml and for this reason, BDG titers in CSF are a beneficial biomarker when monitoring response to treatment. �
For acute bacterial meningitis, a rapid antigen assay can help diagnose for a pneumococcal capsular antigen. Several research studies have demonstrated the utilization of M. tuberculosis-specific antigens in CSF for the diagnosis of tuberculosis meningitis. M. tuberculosis Early Secreted Antigenic Target 6, or ESAT-6, has been utilized for tuberculosis meningitis. �
Serology
Serological diagnosis of CNS infections is determined by identifying IgM antibodies or by demonstrating an increase in neutralizing antibody titers between acute- and convalescent-phase CSF. Due to a delay in antibody response when symptoms have manifested, a negative antibody test cannot be utilized to rule out infections and retesting may be required. Moreover, in specific populations, such as immunocompromised patients, the tests may not offer optimum sensitivity. In most instances, nucleic acid amplification tests have surpassed antibody-based detection as the test of choice. For several CNS infections, these assays play a fundamental role. CSF IgM is the most commonly utilized test for West Nile virus, or WNV, infections. Antibodies may manifest in as soon as 3 days and may continue for up to 3 months. However, its accuracy is challenged by high cross-reactivity with other flaviviruses and associated vaccines. Antibodies in recombinant WNV E proteins can determine where cross-reacting viruses co-circulate or determine which patients have been immunized. �
Fundamental serological assays for CNS infections are utilized for the diagnosis of neurosyphilis. Neurosyphilis is determined by a positive CSF venereal disease research laboratory, or VDRL, test. Diagnosis of varicella-zoster virus, or VZV, IgG in CSF is the most common technique and/or method for the diagnosis of VZV associated with CNS infection. �
Central nervous system, or CNS, infections can ultimately be life-threatening health issues if they are not diagnosed and treated early. Determining an accurate diagnosis of CNS infections can be challenging. Fortunately, a variety of diagnostic techniques and molecular methods can help determine the source of CNS infections. These diagnostic techniques and molecular methods have tremendously improved over the years and more and more of these evaluations are being utilized in clinical settings to accurately diagnose CNS infections for early treatment. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
In part 2 of our “Diagnosis of Central Nervous System Infections” article, we will ultimately discuss the molecular methods and the pan-omic molecular assays which are utilized in the diagnosis of CNS infections as well as discuss how specific testing outcome measures are associated with clinical diseases and health issues. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
We often think of proteins are nutrients found in the food we eat and the main component of muscles, however, proteins are microscopic molecules located inside of cells which actually perform a variety of fundamental roles. The function of a protein depends on its shape, and when protein formation goes awry, the resulting misshapen proteins can cause numerous health issues, such as when proteins neglect their essential roles or when they form a sticky, clumpy clutter inside of cells. Protein formation is an error-prone procedure and mistakes along the way have been associated with neurological diseases. �
There are approximately 20,000 to over 100,000 unique types of proteins found inside a common human cell. Why so many? Proteins are the workhorses of the human cell. By way of instance, several of these proteins are structural, lending stiffness and rigidity to thin neurons or muscle tissues. Other proteins shuttle them to new places and bind to specific molecules and others catalyze responses. A property of proteins is possible through diversity and specificity in their role when they fold. �
Why Proteins Fold into a Functional Shape
A protein generally begins in the cell as a lengthy chain of about 300 building blocks known as amino acids. There are 22 different types of amino acids and their order decides what protein chain will fold onto itself. After folding, two types of structures will generally form. Several regions of the protein chain coil into slinky-like formations known as “alpha-helices,” while other regions fold into zigzag patterns known as “beta-sheets,” which resemble the folds of a paper fan. �
Both of these structures may interact to form complex structures. In one protein structure, many beta-sheets wrap themselves around to form a hollow tube. The tube is also generally short where the overall structure resembles snakes (alpha-helices) emerging out of a can (beta-sheet tubing ). Moreover, several other protein structures with descriptive names include the “beta-barrel,” that the”beta-propeller,” the”alpha/beta-horseshoe,” as well as the “jelly-roll fold”. �
These intricate structures allow proteins to perform their variety of roles in the cell. The “snakes in a can” protein, when embedded into a cell membrane, creates a tube which enables traffic in and out of cells. Other proteins form contours with pockets known as “active sites” which are perfectly shaped to bind to a certain molecule like a lock and key. By bending into different shapes, proteins can do different functions. To draw an analogy, all vehicles are made from steel, while a bus, dump truck, crane, or Zamboni are shaped to execute their very own tasks however races are won by the slick shape of a racecar. �
Why Protein Folding Sometimes Fails
Protein folding ultimately allows a protein to take a functional shape, however, it’s an intricate procedure which can sometimes fail. According to research studies, protein folding can go wrong due to three major reasons: �
A person may have a mutation which affects an amino acid in the protein chain, making it difficult for a specific protein to locate its favored fold or “native” state. This is how it is for mutations, such as those contributing to cystic fibrosis or sickle cell anemia. These mutations are found in the DNA sequence or “gene” which encodes one special protein. Therefore, these types of inherited mutations affect only that protein and its related function.
On the other hand, protein folding failure can be seen as an ongoing and much more general procedure which affects several proteins. When proteins are made, the structure which reads the instructions from DNA to produce the long chains of amino acids can make errors. Researchers estimate that the ribosome makes mistakes in as many as 1 in every 7 proteins. These mistakes can make the proteins which are resultantly inclined to continue to fold improperly.
Even though an amino acid chain does not have any mutations or mistakes, it may still not reach its own preferred folded shape because proteins don’t fold properly 100 percent of their time. Protein folding becomes much more difficult if the conditions in the cell change due to external factors such as temperature and acidity.
A collapse in protein folding can cause a variety of neurological diseases and researchers hypothesize that many health issues are associated with folding problems. There are two problems which exist in cells which don’t protein fold correctly. �
One type of problem, known as “loss of function,” results when not enough of a particular protein folds correctly, causing a lack of “specialized functions” necessary to perform a particularly important role. By way of instance, imagine a correctly folded protein is shaped to bind a toxin and split it into noxious compounds. Without enough of that protein accessible, the toxin will build-up to damaging levels. In another instance, a protein may be responsible for metabolizing sugar which can then be utilized by the cell for energy. The cell will grow due to lack of energy if not enough of this protein is accessible. The reason the cell becomes ill, in these cases, is because of a lack of one particular folded, functional protein. Cystic fibrosis, Tay-Sachs disease, Marfan syndrome, and some types of cancer are examples of health issues which result when one type of protein is unable to perform its role. Who knew that one type of protein out of thousands may be so significant? �
Proteins folding may also impact the overall health and wellness of the cell regardless of the utilization of the protein. When proteins fail to fold into their functional state, the consequent misfolded proteins could be contorted into shapes which are harmful to the crowded cell environment. Most proteins have sticky, “water-hating” amino acids which they bury deep inside their own core. Misfolded proteins utilize these parts on their exterior, such as a chocolate-covered candy which has been crushed to reveal a gooey center. These misfolded proteins commonly stick together to form clumps known as “aggregates.” Researchers discovered that the accumulation of misfolded proteins plays a fundamental role in several neurological diseases, including Alzheimer’s disease, Parkinson’s disease, Huntington’s disease, and Lou Gehrig’s (ALS) disease, however, researchers are still working to discover exactly how these misfolded molecules affect the well-being of the cells. �
One misfolded protein ultimately stands out from among the rest and it deserves particular attention. The “prion” protein in Creutzfeldt-Jakob disease, also known as mad cow disease, is an illustration of a misfolded protein gone rogue. This protein isn’t simply irreversibly misfolded, however, it also transforms other functional proteins into a similar twisted condition. �
How Cells Protect from Misfolded Proteins
Recent research studies have demonstrated that protein misfolding often occurs inside of cells. Fortunately, cells also have many systems in place and are accustomed to coping with this issue by refolding or destroying aberrant protein formations. � Appropriately known as chaperones, these structures accompany proteins throughout the folding procedure, enhancing a protein’s odds of folding properly and even allowing several misfolded proteins the opportunity to refold. Chaperones are proteins themselves. There are many distinct types of chaperones. A few chaperones supply safety to proteins, isolated from other molecules. Production of many chaperones is fostered when a cell encounters high temperatures or other states which can ultimately make protein folding more difficult, therefore, providing these chaperones the alias, “heat shock proteins.” �
The following line of cell defense against misfolded proteins is known as the proteasome. If misfolded proteins linger in the cell, they will be targeted for destruction by this structure, which chews proteins up and spits them out. The proteasome is similar to a center, permitting the cell to reuse amino acids to create proteins. The proteasome itself is not a single protein but many acting collectively. Proteins frequently interact to form larger structures. By way of instance, a human sperm’s tail is a structure made of various types of proteins which work together to produce a rotary engine which propels the sperm. �
Protein Folding and Misfolding Overview
Why is it that some misfolded proteins can evade systems such as chaperones and the proteasome? How can the neurological diseases previously mentioned above be caused by sticky misfolded proteins? Do some proteins misfold more often than others? These questions are at the forefront of research studies seeking to understand the health issues which ultimately result if protein fold goes awry as well as protein biology. The broad world of proteins, using its great assortment of shapes, bestows cells with capacities that allow for life to exist and allow for its diversity (e.g., the differences between eye, skin, lung or heart cells, and also the differences between species). But perhaps this is one of the many reasons why the word “protein” comes from the Greek word “protas,” meaning “of primary significance” and indeed they seem to be. �
Protein folding is a complex, physiochemical process by which a protein “folds” or assumes a functional shape to be able to perform their biological function. Proteins are nutrients we obtain from the food we eat and they are considered to be one of the main components of muscles, however, proteins play a wide variety of fundamental roles in the human body. According to research studies, protein misfolding can cause a variety of health issues, including neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to describe protein folding and how it’s associated with neurological diseases. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Mitochondria are the “energy factory” of the human body. Several thousand mitochondria can be found in nearly every cell. Mitochondria also play several fundamental roles in the body, such as converting chemicals from the foods we eat into energy as well as to process oxygen. Mitochondria produce 90 percent of the energy the human body requires to function accordingly. The purpose of the following article is to describe an overview of mitochondrial disease and well-being. �
What are Mitochondrial Diseases?
Mitochondrial diseases are characterized as chronic, genetic, and often inherited health issues which ultimately occur when mitochondria fail to produce enough energy for the human body to function properly. Mitochondrial diseases may develop from birth however they can frequently develop at any age. Mitochondrial disease can affect any region of the human body, including the cells of the brain, muscles, heart, liver, kidneys, pancreas, eyes, ears, and nerves, among other structures. �
When the mitochondria don’t function as well as they should because of another health issue, mitochondrial dysfunction occurs. Furthermore, many health issues can cause secondary dysfunction and result in other neurological diseases, such as Alzheimer’s disease, Lou Gehrig’s disease, and muscular dystrophy. People with secondary dysfunction don’t have genetic mitochondrial disease and do not need to be concerned about the ongoing development or worsening of symptoms. �
What are the Symptoms of Mitochondrial Disease?
Symptoms of mitochondrial disease depend on which cells of the human body are affected. Symptoms can develop at any age, involve one or more organs, and may range from mild to severe. Even patients within the same household, having the exact same mitochondrial disease can have gaps in symptoms, severity, and age of onset or beginning of symptoms. �
Symptoms of mitochondrial diseases can include: �
Poor growth
Muscle pain, muscle weakness, exercise intolerance, low muscle tone
Vision and/or hearing problems
Learning disabilities, delays in development, mental retardation
In many people, primary mitochondrial disease is a genetic health issue which can be inherited in several ways. To understand inheritance types, it is helpful to find out more about genes and DNA. Genes are substances which provide us our traits, like brown eyes or blue eyes. Genes contain DNA, which is the “blueprint” which gives each person their distinctive make-up. �
In normal circumstances, a child inherits one gene from the father and one gene from the mother. A child with a mitochondrial disease doesn’t receive the pair of genes from the parents. The gene has mutated or has become defective. Learning how the mitochondrial disease is inherited helps predict the prospect of passing the disease(s) to children. �
Inheritance types of mitochondrial disease are: �
Autosomal recessive inheritance: The child receives one mutated copy of a gene from each parent. There is a 25 percent chance that each child in the family will inherit a mitochondrial disease.
Autosomal dominant inheritance: The child receives one mutated copy of a gene from either parent. There is a 50 percent chance that each child in the family will inherit a mitochondrial disease.
Mitochondrial inheritance: In this unique type of inheritance, the mitochondria contain their own DNA. Only mitochondrial disorders caused by mutations in the mitochondrial DNA are exclusively inherited from mothers. There is a 100 percent chance that each child in the family will inherit a mitochondrial disease.
Random mutations: Occasionally, genes develop a mutation of their own which is not inherited from a parent.
How are Mitochondrial Diseases Diagnosed?
Mitochondrial diseases can be difficult to diagnose by a healthcare professional because mitochondrial diseases can ultimately affect a variety of organs and tissues in the human body and patients can also have a variety of symptoms. There is currently no single lab test or diagnostic test which can confirm the identification of mitochondrial disease. That is why a referral to a medical facility with healthcare professionals who focus on these diseases is essential to making the diagnosis. �
Diagnosis begins with a series of evaluations and tests which may include: �
A review of a patient�s family history
A complete physical evaluation
A neurological evaluation
A metabolic evaluation which includes blood and urine tests, and, if needed, a cerebral spinal fluid test
Other evaluations, determined by the regions of the human body and the patient’s symptoms which may include: �
Magnetic resonance imaging (MRI) or spectroscopy (MRS) for neurological symptoms
Retinal exam or electroretinogram (ERG) for vision symptoms
Electrocardiogram (EKG) or echocardiogram for symptoms of heart disease
Audiogram or auditory-brainstem evoked responses (ABER) for hearing symptoms
Blood test to detect thyroid dysfunction if the patient has thyroid problems
Blood test to perform genetic DNA testing
Testing may include biochemical testing. Biopsies of skin and muscle tissue may also be utilized for diagnosis. �
How are Mitochondrial Diseases Treated?
Unfortunately, there is no cure for mitochondrial disease, however, treatment can help reduce symptoms or slow the decline of overall well-being. Treatment varies from patient to patient and depends on the severity and the mitochondrial disease characterized. There is absolutely no way to predict a patient’s reaction or forecast how that person will be affected in the long-term. No two people respond the same way to the same treatment even if they have the same mitochondrial disease. �
Treatments for mitochondrial disease may include: �
Vitamins and supplements, including Coenzyme Q10; B complex vitamins, such as thiamine (B1) and riboflavin (B2), Alpha lipoic acid, L-carnitine (Carnitor), Creatine, and L-Arginine.
Exercise and physical activity, including endurance exercises and resistance/strength training to increase muscle strength. Endurance exercises include walking, running, swimming, dancing, cycling and others. Resistance/strength training includes exercises such as sit-ups, arm curls, knee extensions, weight lifting and others.
Conserving energy. Don�t try to do too much in a short period of time. Pace yourself.
Other treatments including speech therapy, respiratory therapy, physical therapy, and chiropractic care, among others.
Avoid situations which can make the health issue worse. This includes exposure to cold and/or warmth, starvation, lack of sleep, stressful situations, and usage of alcohol, smokes and monosodium glutamate or MSG, a flavor enhancer commonly added to Chinese foods, canned vegetables, soups, as well as processed meats, among other processed foods. �
Mitochondrial diseases are long-term, genetic, and frequently inherited health issues which occur when the mitochondria fail to produce enough energy for the human body to function accordingly. According to research studies, approximately one in 5,000 people has a genetic mitochondrial disease. Chiropractic care is an alternative treatment option which can help relieve symptoms associated with a variety of health issues, including mitochondrial diseases. Many chiropractors are qualified and experienced in the treatment of neurological diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to describe mitochondrial disease and its effect on overall health and wellness. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine