Can individuals dealing with gut inflammation find relief from acupuncture therapy to reduce associated pain symptoms like back pain?
Introduction
When many start thinking about their health and well-being, they will notice the various factors negatively affecting their daily routine. Environmental factors or traumatic injuries can cause an impact on the person’s body, which then causes musculoskeletal issues as well as organ issues. One of the pain-like issues that many people seem to deal with is gut inflammation, and it can cause a cascading effect on the body and lead to referred pain in the upper and lower body portions. This can affect a person’s daily routine and cause overlapping risk profiles, leading to musculoskeletal conditions like back pain. At the same time, gut inflammation can be in acute or chronic stages and become an issue for people with pre-existing conditions. Luckily, numerous treatments reduce gut inflammation associated with back pain and provide a positive impact on individuals. Today’s article looks at the effect of gut inflammation on the body, how gut inflammation correlates with back pain, and how acupuncture therapy can help reduce gut inflammation. We talk with certified medical providers who consolidate our patients’ information to assess how gut inflammation is impacting their bodies and how it correlates with back pain. We also inform and guide patients on how acupuncture therapy can help reduce the inflammatory effects that are causing gut and back issues. We encourage our patients to ask their associated medical providers intricate and important questions about how their pain is causing issues to their bodies. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Effects Of Gut Inflammation On The Body
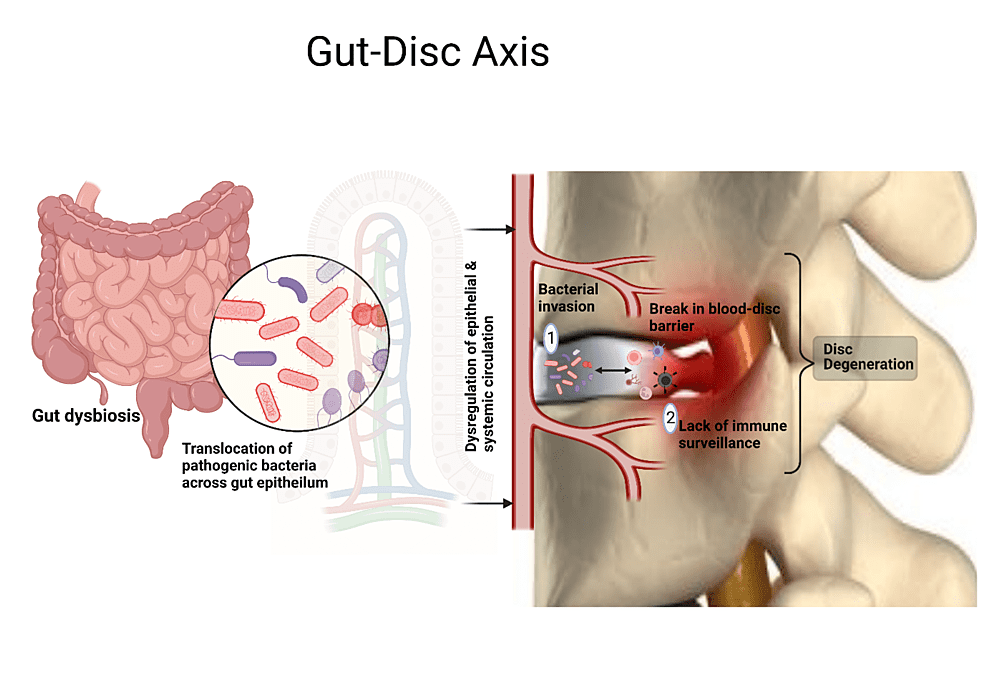
Do you feel extremely tired in the morning, even after a full night? Have you experienced any soreness or tenderness in your gut or different back portions? Or do you experience any muscle aches or joint stiffness throughout your lower back? When people are experiencing these inflammatory issues, it could be due to their gut system feeling these pain-like issues. The gut system is in a relationship with the central nervous system as it is part of the gut-brain axis and helps the autonomic system actively influence the immune system. This allows the musculoskeletal system to promote normal body function. When environmental factors or traumatic injuries start to negatively affect the gut-brain axis and cause the immune system to mass produce inflammatory cytokines and cortisol to cause musculoskeletal and gut issues. The inflammatory effects of the gut system cause impairments within the intestinal barrier function and the translocation of the gut microbes and even promote the hyper-activation of the mucosal immune system to produce pro-inflammatory cytokines that fuel gut inflammation. (Amoroso et al., 2020) When that happens, it can have a major impact on the immune system, and where the gut microbiota can be triggered by environmental factors like metabolic syndrome, obesity, and type-2 diabetes, which has detrimental consequences for the human body. (Scheithauer et al., 2020) What this does to the body is that gut inflammation can affect the immune system, vital organs, and the musculoskeletal system.
Gut Inflammation Correlates With Back Pain
So, back pain usually follows when many individuals have gut issues associated with environmental factors. When the intestinal permeability in the gut starts to deal with inflammation, all the bacteria and the cytokines from the immune system will rapidly produce and travel their way to the various muscles, tissues, and ligaments that start to be affected. Since back pain is a common musculoskeletal condition many people endure, gut inflammation can also be present. Since the bacterial microbes and inflammatory cytokines are reaching the spine’s back muscles and skeletal structures, they can start causing degenerative issues, leading to back pain. The skeletal structure of the spine has facet joints, spinal discs, and bones that protect the spinal cord and can also be affected by gut inflammation. The blood-disc barrier within the spine protects the spinal disc from inflammatory effects that may invoke musculoskeletal issues. However, when the bacterial microbes from the gut start to attach and break down the blood-disc barrier, they can rapidly multiply since the immune system surveillance is unavailable, causing low oxygen levels to degenerate the spinal discs and causing back pain issues. (Ratna et al., 2023) At the same time, environmental factors also play an issue in the development of back pain associated with gut inflammation. Luckily, numerous treatments can help not only reduce gut inflammation but also provide pain relief to back pain.
Fighting Inflammation Naturally- Video
Have you been dealing with various mood changes affecting your daily routine? Do you feel constantly sluggish or tired throughout the day? Or do you feel aches and pains in your mid-section and lower back? Many people experiencing these pain-like issues in their bodies are dealing with gut inflammation that is affecting their backs. When environmental factors start to cause an overproduction of bacterial microbes in the intestinal permeability, the inflammatory cytokines begin to induce inflammation in the musculoskeletal system. This can lead to the development of back pain and cause issues to the body when it is not treated right away. This is where various treatments help reduce the inflammatory effects of the gut system and help reduce numerous issues it has caused. Many treatments are non-surgical and customizable to individuals dealing with gut inflammation associated with back pain. The video above shows how non-surgical treatments can help reduce inflammation naturally and benefit many people dealing with gut inflammation.
Acupuncture Reducing Gut Inflammation
Various non-surgical treatments can range from traction therapy to chiropractic care, depending on the pain severity and environmental factors causing the issue. For gut inflammation, many individuals might try acupuncture, one of the oldest forms of non-surgical treatment that can help reduce inflammatory cytokines. Acupuncture originates from China and is used by highly trained medical professionals who use fine, solid, thin needles to be placed on various body acupoints to restore body energy. Acupuncture can also serve as a multifaceted regulatory therapy that involves multiple therapeutic mechanisms to regulate the HPA axis and reduce pro-inflammatory cytokines levels. (Landgraaf et al., 2023) At the same time, acupuncture can help recover gastrointestinal dysfunction from various gut disorders by blocking the brain’s neuron signals that are causing inflammatory responses to the gut and musculoskeletal system. (Jang et al., 2020). Acupuncture can also be combined with other non-surgical therapies to help improve body functionality, as acupuncturists find the acupoints within the body to regulate the intestinal microbiota and inflammation, thus regulating the central nervous system function to enhance a person’s quality of life. (Bao et al., 2022) By incorporating acupuncture as part of a person’s health and well-being, many people can make small changes in their daily routine to reduce gut inflammation from overproducing and prevent their associated comorbidities from returning.
References
Amoroso, C., Perillo, F., Strati, F., Fantini, M. C., Caprioli, F., & Facciotti, F. (2020). The Role of Gut Microbiota Biomodulators on Mucosal Immunity and Intestinal Inflammation. Cells, 9(5). https://doi.org/10.3390/cells9051234
Bao, C., Wu, L., Wang, D., Chen, L., Jin, X., Shi, Y., Li, G., Zhang, J., Zeng, X., Chen, J., Liu, H., & Wu, H. (2022). Acupuncture improves the symptoms, intestinal microbiota, and inflammation of patients with mild to moderate Crohn’s disease: A randomized controlled trial. EClinicalMedicine, 45, 101300. https://doi.org/10.1016/j.eclinm.2022.101300
Jang, J. H., Yeom, M. J., Ahn, S., Oh, J. Y., Ji, S., Kim, T. H., & Park, H. J. (2020). Acupuncture inhibits neuroinflammation and gut microbial dysbiosis in a mouse model of Parkinson’s disease. Brain Behav Immun, 89, 641-655. https://doi.org/10.1016/j.bbi.2020.08.015
Landgraaf, R. G., Bloem, M. N., Fumagalli, M., Benninga, M. A., de Lorijn, F., & Nieuwdorp, M. (2023). Acupuncture as multi-targeted therapy for the multifactorial disease obesity: a complex neuro-endocrine-immune interplay. Front Endocrinol (Lausanne), 14, 1236370. https://doi.org/10.3389/fendo.2023.1236370
Ratna, H. V. K., Jeyaraman, M., Yadav, S., Jeyaraman, N., & Nallakumarasamy, A. (2023). Is Dysbiotic Gut the Cause of Low Back Pain? Cureus, 15(7), e42496. https://doi.org/10.7759/cureus.42496
Scheithauer, T. P. M., Rampanelli, E., Nieuwdorp, M., Vallance, B. A., Verchere, C. B., van Raalte, D. H., & Herrema, H. (2020). Gut Microbiota as a Trigger for Metabolic Inflammation in Obesity and Type 2 Diabetes. Front Immunol, 11, 571731. https://doi.org/10.3389/fimmu.2020.571731
For individuals dealing with lower back pain, it could be quadricep muscle tightness causing the symptoms and posture problems. Can knowing the signs of quadricep tightness help prevent pain and avoid injury?
Quadriceps Tightness
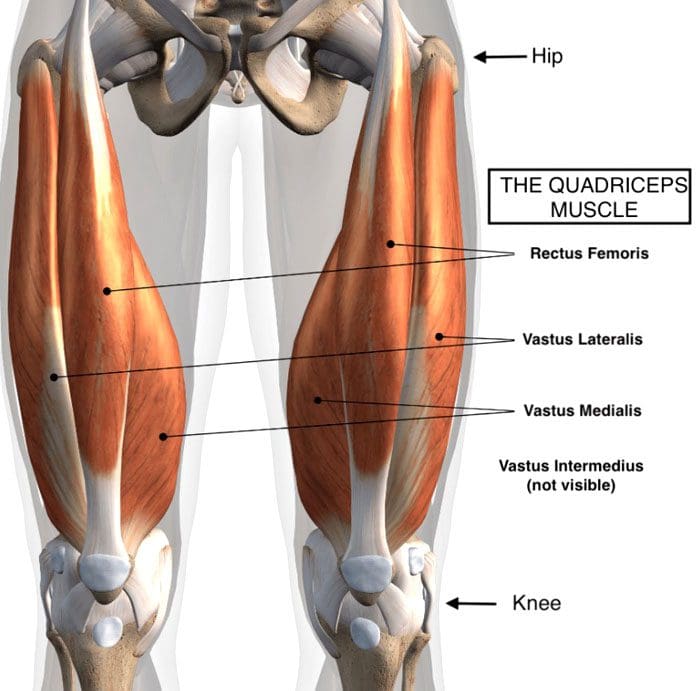
Quadriceps muscles are in the front of the thigh. Forces that could be creating chronic pain and posture problems could be happening at the same time are:
Quadricep tightness causes lower back pain as the pelvis gets pulled down.
Tight quadriceps lead to weakened hamstring muscles.
These are the opposing muscles behind the thigh.
Stress and pressure on the hamstrings can cause back pain and problems.
The rectus femoris attaches to the pelvis at the anterior superior iliac spine, which is the front part of the hip bone.
The rectus femoris is the only muscle in the group that crosses over the hip joint, which also affects movement.
When the quadriceps, especially the rectus femoris, become tight, they pull down on the hips.
The pelvis tilts downward or forward, technically referred to as the anterior tilt of the pelvis. (Anita Król et al., 2017)
The spine is between the pelvis, and if the pelvis tilts forward, the lumbar spine compensates by arching.
A larger arch in the lower back is referred to as excessive lordosis and often causes tightness and pain in the back muscles. (Sean G. Sadler et al., 2017)
Hamstring Compensation
When the quadriceps tighten and the pelvis gets pulled down, the back has an abnormal lift. This puts the hamstring on a consistent stretch that can cause pain symptoms.
Healthy posture and hamstring muscle tone help maintain correct pelvic positioning in the back.
This is correct because it helps maintain a comfortable position.
Quadricep tightness can set off a reaction as the pelvis tilts down in front and up in the back while overly stretching the hamstrings.
Pain and soreness are the usual result
Lack of hamstring strength and quadriceps stretching can cause the hamstrings to lose their ability to support correct pelvic and spinal positions. (American Council on Exercise. 2015)
Knowing When Quads Are Tightening
Individuals often don’t realize their quadriceps are tight, especially those who spend most of the day sitting.
The more time spent in a chair can cause the quadriceps and lower back muscles to tighten steadily.
Individuals can try a few tests at home:
Standing Up
Push the hips forward.
Push from the sitting bones so you’re at the correct level.
How far forward do the hips go?
What is felt?
Pain could indicate tight quadriceps.
In A Lunge Position
With one leg forward and bent in front of the other.
The back leg is straight.
How far forward does the leg go?
What is felt?
How does the front of the hip on the back leg feel?
Standing Bent Leg
Stand with the front leg bent and the back leg straight.
Discomfort in the back leg could mean tight quadriceps.
In A Kneeling Position
Arch the back
Grab the ankles
Modify the position to adjust for any pain or joint issues.
If you have to prop yourself up or modify the pose to reduce pain, it could be tight quadriceps.
Helping to understand the condition can help in communication with a healthcare provider.
A healthcare provider and/or physical therapist can conduct a posture evaluation examination to test the quadriceps.
Understanding Academic Low Back Pain: Impact and Chiropractic Solutions
References
Kripa, S., Kaur, H. (2021). Identifying relations between posture and pain in lower back pain patients: a narrative review. Bulletin of Faculty of Physical Therapy, 26(34). https://doi.org/doi: 10.1186/s43161-021-00052-w
Król, A., Polak, M., Szczygieł, E., Wójcik, P., & Gleb, K. (2017). Relationship between mechanical factors and pelvic tilt in adults with and without low back pain. Journal of back and musculoskeletal rehabilitation, 30(4), 699–705. https://doi.org/10.3233/BMR-140177
Sadler, S. G., Spink, M. J., Ho, A., De Jonge, X. J., & Chuter, V. H. (2017). Restriction in lateral bending range of motion, lumbar lordosis, and hamstring flexibility predicts the development of low back pain: a systematic review of prospective cohort studies. BMC musculoskeletal disorders, 18(1), 179. https://doi.org/10.1186/s12891-017-1534-0
American Council on Exercise. (2015). 3 Stretches for Opening Up Tight Hips (Fitness, Issue. https://www.acefitness.org/resources/everyone/blog/5681/3-stretches-for-opening-up-tight-hips/
Can nonsurgical therapeutic options help individuals with chronic low back pain find the relief they are looking for to restore body function?
Introduction
Between the upper, middle, and lower back portions of the musculoskeletal system, many individuals have succumbed to traumatic injuries, repetitive motions, and overlapping environmental risk profiles that cause pain and disability, thus affecting their everyday routine. As one of the most common work conditions, back pain can cause individuals to deal with socio-economic burdens and can range from acute to chronic, depending on the injuries and factors that correlate with this issue. As part of the musculoskeletal system, the back has various muscles in the three quadrants that support the upper and lower extremities and have an outstanding relationship with the spine as each muscle group surrounds the spine and protects the spinal cord. When environmental factors and traumatic injuries start to cause pain-like symptoms in the back, it can put a person in excruciating pain, hence why many seek non-surgical treatments to reduce the pain-like effects of back pain and find the relief they are seeking. Today’s article looks at the impact of chronic low back pain and how non-surgical treatments can positively affect individuals dealing with chronic low back pain. We talk with certified medical providers who consolidate our patients’ information to provide numerous non-surgical treatment options to minimize chronic lower back pain affecting their extremities. We also inform and guide patients on how various non-surgical treatments can benefit their health and wellness as they can help reduce musculoskeletal conditions like chronic back pain. We encourage our patients to ask their associated medical providers intricated and important questions about their chronic low back pain and what small changes they can incorporate to reduce its pain-like symptoms. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Impact Of Chronic Low Back Pain
Do you constantly feel severe muscle aches or pains in your back after an excruciating long workday? Do you experience muscle tiredness from your back to your legs after carrying a heavy object? Or have you noticed that twisting or turning motions temporarily relieve your lower back, only to worsen after a while? Often, many of these pain-like scenarios are correlated with chronic low back pain, and it can be due to the various factors that correlate with this common musculoskeletal condition. When it comes to musculoskeletal conditions associated with chronic low back pain, they are prevalent while their impact is pervasive. To that point, they affect many individuals as they are the number one most common cause of severe long-term pain and physical disability. (Woolf & Pfleger, 2003) Since back pain can be either acute or chronic, it can become multifactorial as many other pain symptoms tend to cause overlapping risk profiles in the body. The impact of chronic low back pain has underlying pathological causes that are not well-defined but can be related to psychosocial dysfunction. (Andersson, 1999)
Additionally, degenerative changes within the spine can also cause an impact on the development of chronic lower back pain. The risk factors that cause overlapping risk profiles can range from smoking and obesity to various occupations that require excessive motions. (Atkinson, 2004) When that happens, it causes people to have unnecessary stress that impacts their lives and causes them to be miserable. This is where many individuals start seeking treatment to reduce the effects of chronic lower back pain and reduce the chances of seeking surgical intervention.
The Role Of Chiropractic Care On Improving Your Health- Video
Non-Surgical Treatments For Chronic Back Pain
When people deal with chronic lower back pain, many often don’t realize that various motions, ages, and pathologies can modify the spine, causing the spinal discs to go through degenerative changes that correspond to the development of chronic lower back pain. (Benoist, 2003) When degenerative changes start to cause pain-like symptoms in the back, many will begin looking for affordable and effective treatments. Hence, this is why non-surgical treatments can help reduce the pain-like symptoms of chronic lower back pain and help restore body mobility. Non-surgical treatments are personalized to the person’s pain and range from acupuncture to massage therapy and spinal decompression. Non-surgical treatments are also affordable and help reduce the overlapping risk profiles of chronic low back pain while reducing its associated conditions.
Spinal Decompression Effects On Chronic Low Back Pain
Spinal decompression, as stated before, is a form of non-surgical treatment that incorporates mechanical gentle traction on the spine to alleviate chronic low back pain and can reduce the pain-like symptoms associated with it. Spinal decompression helps reduce the friction of the lumbar muscles, affecting the lumbar spine but also provides pain relief and body function. (Choi et al., 2022) Spinal decompression is safe while being gentle on the spine, combined with stabilization exercises to enhance intra-abdominal pressure and spinal ability to the lumbar. (Hlaing et al., 2021) When a person incorporates spinal decompression as part of their health and wellness journey, their pain and disability will lower over time while strengthening weakened muscles that were affected by chronic lower back pain. Incorporating these non-surgical treatments can help a person be more mindful of the environmental impact they are inflicting on their backs and live a better and healthier life.
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. https://doi.org/10.1155/2022/6343837
Hlaing, S. S., Puntumetakul, R., Khine, E. E., & Boucaut, R. (2021). Effects of core stabilization exercise and strengthening exercise on proprioception, balance, muscle thickness and pain related outcomes in patients with subacute nonspecific low back pain: a randomized controlled trial. BMC Musculoskelet Disord, 22(1), 998. https://doi.org/10.1186/s12891-021-04858-6
Can individuals with leg and back pain find the relief by incorporating decompression to reduce pain-like associated symptoms?
Introduction
The lower extremities help stabilize the upper body’s weight and provide movement to the individual. The lower body portions include the lower back, pelvis, hips, thighs, legs, and feet, as they all have specific jobs to do and have an outstanding relationship with each other. However, their lower back and legs are susceptible to injuries. When environmental factors or injuries start to cause issues in the musculoskeletal system, it can lead to referred pain and overlapping risk profiles that can cause a person to have mobility and stability issues. The affected muscles, tissues, ligaments, and nerve roots can become irritated, weak, and tight when environmental factors start to compress the spine and lead to pain over time. Today’s article looks at how the back and legs work together in the body, how they are impacted by pain from environmental factors, and how spinal decompression can reduce leg and back pain. We talk with certified medical providers who consolidate our patients’ information to provide numerous treatments to minimize back and leg pain affecting their mobility. We also inform and guide patients on how treatments like decompression can help reduce pain-like symptoms within the legs and back. We encourage our patients to ask their associated medical providers intricated and important questions about the referred pain-like symptoms they are experiencing from their legs and since that is disrupting their daily routine. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
How The Back & Legs Work Together?
Do you feel radiating pain in your back that is affecting your ability to walk? Do you experience muscle aches or tiredness in your legs after a long workday? Or do you feel stiffness in your back and legs after waking up? Many of these scenarios are correlated with leg and back pain that can impact a person’s gait and lead to associated pain-like symptoms. The back and leg muscles work together through the sciatic nerve, a long nerve from the lumbar spinal region, past the gluteal muscles, traveling down the back of the legs and stopping at the knees. The back consists of the core muscles and the lumbar spinal region, allowing the person to bend, twist, and extend.
Meanwhile, the leg muscles help a person become mobile while stabilizing the person’s weight. These two muscle groups have an outstanding relationship in the lower extremities, as people need to be mobile when doing activities. However, they can also become vulnerable to injuries and pain that can cause disability issues.
How Pain Is Associated With The Back & Legs?
When it comes to the lower back and the legs, environmental factors and traumatic injuries can affect the surrounding muscles, tendons, ligaments, and nerve roots. For example, when working individuals routinely lift heavy objects, it can increase the risk of developing lower back pain while causing whole-body vibrations in the legs. (Becker & Childress, 2019) This is because what the heavy loading object does to the lower back is that it causes the spine to be compressed and contract the surrounding muscle. When it is repeated constantly, it can cause the spinal disc to herniate and aggravate the nerve roots. When these nerve roots become aggravated, it can lead to nerve entrapment and inflammation, thus causing individuals to experience chronic leg pain, foot drop, or ankle stability that affects their mobility. (Fortier et al., 2021)
Additionally, back and leg pain can even happen when the spine starts to experience degeneration, a natural process when the spinal disc shrinks over time. When the spinal disc in the lumbar spinal region degenerates over time, the nutrient supplies and changes in the extracellular composition cause the discs to be less capable of maintaining their load distribution function in the lower extremities. (Kim et al., 2020) However, many people who are experiencing leg and back pain can seek treatment to reduce the pain-like symptoms.
Chiropractic Care For Leg Instability- Video
Spinal Decompression Reducing Pain On The Legs & Back
When it comes to treating leg and back pain, many individuals will start to seek affordable treatment that can reduce pain-like symptoms. Many non-surgical treatments like spinal decompression are excellent for reducing pain that is affecting the back and legs. Spinal decompression uses a traction machine that can help stretch out the tight muscles from the lower back and provide negative pressure to the affected disc by increasing the blood nutrient flow back to the disc while reducing pressure off the aggravated nerve root. (Choi et al., 2022) Spinal decompression can be combined with core stabilizing exercises that can help reduce pain and disability and improve stability in the legs and lower extremities. (Hlaing et al., 2021) With spinal decompression to reduce back and leg pain, many individuals can notice positive results after consecutive treatment, and their mobility is improved. (Vanti et al., 2021) When individuals who are experiencing leg and back pain and are looking for treatment can find the benefits of spinal decompression to be incorporated into their daily routine since it can be customizable and help them be more mindful of what movements and environmental factors are causing them pain. Making these small changes over time can improve their health and help them live healthier lives.
References
Becker, B. A., & Childress, M. A. (2019). Nonspecific Low Back Pain and Return To Work. American Family Physician, 100(11), 697-703. https://www.ncbi.nlm.nih.gov/pubmed/31790184
Choi, E., Gil, H. Y., Ju, J., Han, W. K., Nahm, F. S., & Lee, P. B. (2022). Effect of Nonsurgical Spinal Decompression on Intensity of Pain and Herniated Disc Volume in Subacute Lumbar Herniated Disc. International Journal of Clinical Practice, 2022, 6343837. https://doi.org/10.1155/2022/6343837
Fortier, L. M., Markel, M., Thomas, B. G., Sherman, W. F., Thomas, B. H., & Kaye, A. D. (2021). An Update on Peroneal Nerve Entrapment and Neuropathy. Orthop Rev (Pavia), 13(2), 24937. https://doi.org/10.52965/001c.24937
Hlaing, S. S., Puntumetakul, R., Khine, E. E., & Boucaut, R. (2021). Effects of core stabilization exercise and strengthening exercise on proprioception, balance, muscle thickness and pain related outcomes in patients with subacute nonspecific low back pain: a randomized controlled trial. BMC Musculoskelet Disord, 22(1), 998. https://doi.org/10.1186/s12891-021-04858-6
Kim, H. S., Wu, P. H., & Jang, I. T. (2020). Lumbar Degenerative Disease Part 1: Anatomy and Pathophysiology of Intervertebral Discogenic Pain and Radiofrequency Ablation of Basivertebral and Sinuvertebral Nerve Treatment for Chronic Discogenic Back Pain: A Prospective Case Series and Review of Literature. Int J Mol Sci, 21(4). https://doi.org/10.3390/ijms21041483
Vanti, C., Turone, L., Panizzolo, A., Guccione, A. A., Bertozzi, L., & Pillastrini, P. (2021). Vertical traction for lumbar radiculopathy: a systematic review. Arch Physiother, 11(1), 7. https://doi.org/10.1186/s40945-021-00102-5
Can individuals dealing with low back pain find the relief they are looking for by incorporating acupuncture to reduce muscle spasms?
Introduction
Around the world, many individuals, young and old, have dealt with low back pain, which has an impact on their lives and affects their routines. Since low back pain is a multifactorial musculoskeletal issue, it can range from acute to chronic, depending on the severity and environmental factors that are in play. The lower back or the lumbar spinal region has thicker joints and helps stabilize the upper body portion’s weight. However, it is more susceptible to injury, and it causes the surrounding ligaments, soft tissues, and muscles to be overstretched, tight, and weak. When a person is in excruciating pain from the effects of low back pain, it can impact their day and cause them to be miserable. Today’s article focuses on how lower back pain is associated with pain-like symptoms like muscle spasms and how treatments like acupuncture can help reduce muscle spasms associated with lower back pain. We talk with certified medical providers who consolidate our patients’ information to provide numerous treatments to relieve low back pain correlated with muscle spasms. We also inform and guide patients on how treatments like acupuncture can help minimize the pain in their lower back. We encourage our patients to ask their associated medical providers intricated and important questions about the referred pain-like symptoms they are experiencing from low back pain that is affecting their daily routine. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
Low Back Pain Associated With Muscle Spasms
Do you feel radiating or localized pain in your lower back after a long workday? Do you feel stiffness in your lower back region after stretching in the morning? Or have you noticed you are more tense in the different areas of your back and looking for relief? While it is a common problem that many people experience, low back pain can occur to many individuals worldwide and can significantly impact a person. As a major public health concern, low back pain globally transcends through ages, occupations, and socio-economic backgrounds, causing pain-like symptoms to develop over time. (Emorinken et al., 2023) Numerous factors can lead to low back pain and the symptoms that can occur in the lumbar region. Since low back pain can affect many individuals worldwide, this musculoskeletal condition can cause activity limitations in people. It can progressively increase spine degeneration, affecting the joints, bones, and discs. (Hauser et al., 2022) Some of the symptoms that correlate with low back pain include:
Stiffness
Gait instability
Numbing or tingling sensations in the extremities
Myofascial referred pain
Muscle spasms
The painful effects of low back pain can cause muscle spasms in the lumbar region as many people continuously make repetitive motions that cause the surrounding muscles to become overworked and develop trigger points to cause muscle spasms. When a person goes to a doctor to treat their lower back pain, they undergo a physical examination to evaluate their lower extremities’ strength, sensation, and reflexes. These examinations help doctors determine the proper protocol for low back pain through inspection, palpation, and range of motion of the lumbosacral musculature to identify point tenderness, restriction, and muscle spasms. (Will et al., 2018) These identity markers allow doctors to devise a personalized plan to reduce the effects of low back pain and help individuals regain their health.
Exploring Integrative Medicine- Video
Acupuncture Effects On Low Back Pain
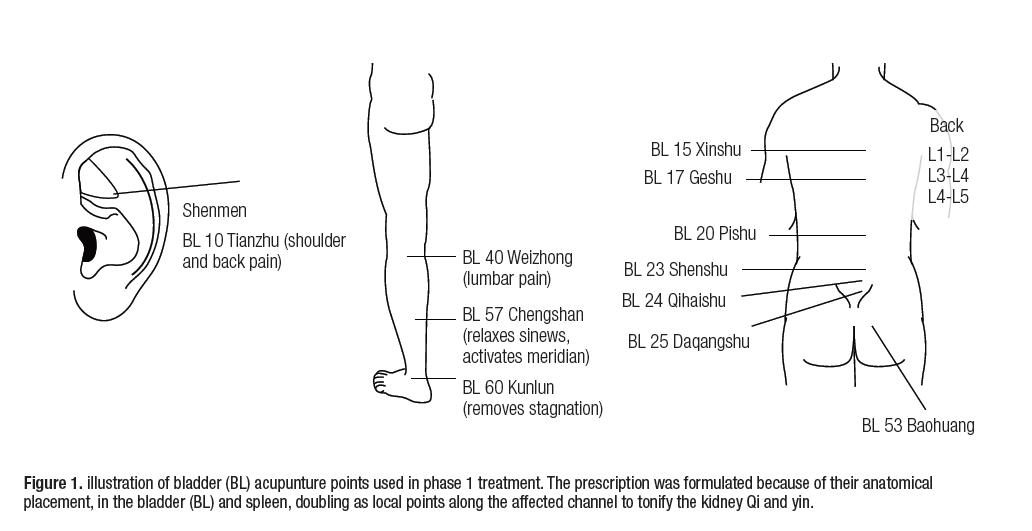
When people with back pain are looking for treatment, they are looking for something affordable and can work with their busy schedule. Hence, non-surgical treatments could be the answer to reducing low back pain. Numerous non-surgical treatments can help individuals with specific pain-like symptoms that correlate with various factors. Each treatment, from chiropractic care to traction therapy, is personalized for the individual. Now, one of the oldest forms of non-surgical treatment is acupuncture. Originating from China, acupuncture incorporates solid thin needles at specific body points to balance the energy flow in the body that highly trained professionals perform. The effects of acupuncture can help stimulate the release of adenosine at the sight of needle stimulation while increasing local blood flow to the affected area to promote natural healing. (Mu et al., 2020) So, how does acupuncture help individuals reduce low back pain?
Since low back pain can cause a socio-economic burden many people are affected by, acupuncture can help reduce pain and disability in the affected muscle areas while improving the person’s quality of life. (Baroncini et al., 2022) Acupuncture for low back pain benefits individuals by releasing endorphins and other neurohumoral factors that change brain and spinal cord processing. At the same time, acupuncture can also increase microcirculation and reduce the inflammatory effects of low back pain. (Sudhakaran, 2021) Acupuncture can also be part of a person’s personalized treatment plan, as physical and massage therapy can help strengthen the affected muscles caused by low back pain. When people dealing with low back pain are finally getting the relief they need, they can get their quality of life back through small changes to better themselves. This allows them to be more mindful of the various factors that can cause their bodies pain and prevent them from returning over time.
References
Baroncini, A., Maffulli, N., Eschweiler, J., Molsberger, F., Klimuch, A., & Migliorini, F. (2022). Acupuncture in chronic aspecific low back pain: a Bayesian network meta-analysis. J Orthop Surg Res, 17(1), 319. https://doi.org/10.1186/s13018-022-03212-3
Emorinken, A., Erameh, C. O., Akpasubi, B. O., Dic-Ijiewere, M. O., & Ugheoke, A. J. (2023). Epidemiology of low back pain: frequency, risk factors, and patterns in South-South Nigeria. Reumatologia, 61(5), 360-367. https://doi.org/10.5114/reum/173377
Hauser, R. A., Matias, D., Woznica, D., Rawlings, B., & Woldin, B. A. (2022). Lumbar instability as an etiology of low back pain and its treatment by prolotherapy: A review. J Back Musculoskelet Rehabil, 35(4), 701-712. https://doi.org/10.3233/BMR-210097
Mu, J., Furlan, A. D., Lam, W. Y., Hsu, M. Y., Ning, Z., & Lao, L. (2020). Acupuncture for chronic nonspecific low back pain. Cochrane Database Syst Rev, 12(12), CD013814. https://doi.org/10.1002/14651858.CD013814
Can working individuals with low back pain incorporate nonsurgical treatments to reduce limited mobility and provide relief?
Introduction
Many working individuals will slowly develop low back pain due to excessive standing or sitting, physical demands that cause them to lift heavy objects, or improper footwear that causes them to be imbalanced. Since the spine is part of the musculoskeletal system, the spinal discs in the lumbar region are the most susceptible to being compressed. They can be one of the issues why many individuals tend to develop lower back pain. Low back pain is common for working individuals and is a multifactorial musculoskeletal disorder that causes many working people to miss out on work. However, many people with low back pain often seek treatment to reduce the pain and help them get back to work. Today’s article looks at the causes of low back pain and how nonsurgical treatments can help reduce low back pain and restore mobility to the body. We speak with certified medical providers who incorporate our patients’ information to provide various treatments to ease low back pain. We also inform patients how nonsurgical treatments can help restore mobility to the body while giving numerous techniques to reduce the chances of low back pain returning. We encourage our patients to ask intricated questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with their backs. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
The Causes For Low Back Pain
Do you feel stiffness in your lower back after a hard workday? Do you experience muscle aches or pain in your lower back after picking up a heavy object? Or do you experience limited mobility and stiffness over time after excessive standing or sitting at your job? Many individuals in these pain-like scenarios have experienced low back pain at some point in their lives, and it has impacted them to miss out on work. Since many people worldwide have experienced low back pain at some point in their lives, it has become a common problem that has become the leading cause of disability and is often associated with high cost. (Chou, 2021) Low back pain is a multifactorial condition that is specific or non-specific depending on the severity of the person’s experience. Non-specific low back pain often refers to when there isn’t a particular disease or structural reason for the pain to occur. This causes many people to go into early retirement due to losing their ability to work and become a socio-economic burden when seeking treatment. (Chenot et al., 2017) Specific low back pain is due to repetitive trauma and overusing the surrounding muscles that can cause the spine and spinal disc to be constantly compressed. This causes musculoskeletal pain symptoms and affects the rest of the lower extremities. (Will et al., 2018)
Some of the causes that low back pain is associated with can range from normal environmental factors to traumatic injuries that many working individuals have endured. Since low back pain is one of the leading causes of lost workdays around the world, some of the common causes that are contributed to low back pain include:
Mechanical strain
Obesity
Poor body mechanics
Trauma
Repetitive motions (twisting, bending, or lifting)
Herniated disc
Spinal stenosis
These pain-like causes can affect the upper and lower extremities and, when not being treated, lead to pain-like symptoms from radiating pain to limited mobility. However, when many people decide that enough is enough and want to get the treatment they need, they will seek out something that is not only affordable but can reduce the pain while restoring mobility.
The Power Of Chiropractic Care-Video
Nonsurgical Treatments For Low Back Pain
When it comes to seeking treatment for low back pain, many individuals are looking for something that is not only cost-effective but can help reduce the pain-like symptoms associated with the lower back. Nonsurgical treatments can help reduce low back pain and are cost-effective for many individuals including working individuals. Treatments like acupuncture, chiropractic care, and spinal decompression have various techniques and methods to provide pain relief to many individuals dealing with low back pain. Knowing the prevalence of the multiple pathologies of low back pain, a detailed history, and physical examination maneuvers allow doctors to accurately and quickly classify the most common causes of low back pain. (Kinkade, 2007) This will give them a better understanding of what kind of low back pain treatment they need to restore mobility to their bodies.
Chiropractic Care
Chiropractic care is a nonsurgical treatment that incorporates manual and mechanical manipulation to realign the body out of subluxation from low back pain. Chiropractic care can be incorporated into a person’s health and wellness treatment plan as it can help improve pain and disability associated with low back pain. (Bussieres et al., 2018) Chiropractors combine various techniques to stretch and strengthen weak muscles around the lower back and reduce low back pain intensity and disability. (Vining et al., 2020) Chiropractic care can also work with other forms of therapies to reduce the chances of low back pain from returning.
Spinal Decompression
Spinal decompression is another form of nonsurgical treatment that can help the lumbar spine through gentle traction and help decompress affected spinal discs from causing mechanical back pain. Spinal decompression can also alleviate the referred pain-like symptoms from the nerve roots involved in the lumbar region while rehydrating herniated discs. Spinal decompression can also help many individuals have their lumbar range of motion back and improve their pain and endurance while restoring their quality of life. (Amjad et al., 2022) Just like chiropractic care, spinal decompression can be combined with other therapies to strengthen the surrounding muscles and ligaments.
Acupuncture
With low back pain being a common problem for many individuals, sometimes it could be due to aggravated nerve roots along the surrounding muscles that are causing referred trigger pain correlating with low back pain. When that happens, many individuals will seek out acupuncture to reduce the pain and improve their quality of life. (Baroncini et al., 2022) Acupuncture can reduce the inflammatory effects caused by inflammation associated with low back pain and can increase mobility in the sacroiliac joint to improve mobility. (Sudhakaran, 2021) Depending on the source of pain in the back, acupuncture can help reduce the pain and provide relief. Many individuals seeking treatment for their lower back can incorporate these treatments to improve their health and restore their quality of life.
References
Amjad, F., Mohseni-Bandpei, M. A., Gilani, S. A., Ahmad, A., & Hanif, A. (2022). Effects of non-surgical decompression therapy in addition to routine physical therapy on pain, range of motion, endurance, functional disability and quality of life versus routine physical therapy alone in patients with lumbar radiculopathy; a randomized controlled trial. BMC Musculoskelet Disord, 23(1), 255. https://doi.org/10.1186/s12891-022-05196-x
Baroncini, A., Maffulli, N., Eschweiler, J., Molsberger, F., Klimuch, A., & Migliorini, F. (2022). Acupuncture in chronic aspecific low back pain: a Bayesian network meta-analysis. J Orthop Surg Res, 17(1), 319. https://doi.org/10.1186/s13018-022-03212-3
Bussieres, A. E., Stewart, G., Al-Zoubi, F., Decina, P., Descarreaux, M., Haskett, D., Hincapie, C., Page, I., Passmore, S., Srbely, J., Stupar, M., Weisberg, J., & Ornelas, J. (2018). Spinal Manipulative Therapy and Other Conservative Treatments for Low Back Pain: A Guideline From the Canadian Chiropractic Guideline Initiative. J Manipulative Physiol Ther, 41(4), 265-293. https://doi.org/10.1016/j.jmpt.2017.12.004
Chenot, J. F., Greitemann, B., Kladny, B., Petzke, F., Pfingsten, M., & Schorr, S. G. (2017). Non-Specific Low Back Pain. Dtsch Arztebl Int, 114(51-52), 883-890. https://doi.org/10.3238/arztebl.2017.0883
Vining, R., Long, C. R., Minkalis, A., Gudavalli, M. R., Xia, T., Walter, J., Coulter, I., & Goertz, C. M. (2020). Effects of Chiropractic Care on Strength, Balance, and Endurance in Active-Duty U.S. Military Personnel with Low Back Pain: A Randomized Controlled Trial. J Altern Complement Med, 26(7), 592-601. https://doi.org/10.1089/acm.2020.0107
Can individuals dealing with neck and back pain find the relief they need from the effects of spinal decompression therapy?
Introduction
Across the world, many individuals deal with neck or back pain from excessive sitting or standing, poor posture, or lifting heavy objects that cause their spine and muscles to ache constantly. Since the body is in constant movement, the spine is being compressed through repetitive movement that can cause the spinal discs to pop out of their original position and aggravate the surrounding nerves to cause pain-like symptoms in the neck and back regions. Many people start to complain about their necks and backs hurting and feeling referred pain in different locations in the upper and lower body portions. This can range from acute to chronic, depending on the severity of the pain. When people are experiencing these musculoskeletal pain disorders in their bodies, many will seek treatment to alleviate the pain in their necks and backs to return to their daily routines. Hence why, treatments like spinal decompression can have a positive effect on providing the relief that many individuals deserve. Today’s article looks at why the neck and back in the human body are the most common pain areas many people endure and how spinal decompression can reduce neck and back pain. We speak with certified medical providers who incorporate our patients’ information to provide various techniques to relieve neck and back pain from the body. We also inform patients how treatments like decompression can reduce musculoskeletal pain disorders from the neck and back. We encourage our patients to ask intricated questions to our associated medical providers about the pain-like symptoms they are experiencing correlating with their neck and back. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
Why Are The Neck & Back Common Pain Areas?
Do you feel muscle tension in your neck after being hunched on the computer or your phone for a long time? Do you feel aches and pains in your back after carrying or lifting a heavy object? Or do you feel tingling or numbness in your arms or legs? Many of these pain-like symptoms are often correlated with neck and back pain that can be a nuisance to many individuals. So why is it that the neck and back of the human body are the most common pain areas that many people worldwide endure? Many people with highly demanding jobs often perform normal movements repetitively, which causes stress on the surrounding muscles, ligaments, and joints, and the accessory muscles will begin to be overworked and tight. Neck and back pain are amongst the most common symptom-related complaints that contribute to high levels of lost workdays, disability, and health care use. (Corwell & Davis, 2020) This causes many individuals to have unwanted socio-economic stress when they visit their primary care doctors. Additionally, neck and back pain are non-neurologic causes in the musculoskeletal system; these can generate pain in the muscles, tendons, ligaments, spinal discs, articular cartilage, and bone. (Meleger & Krivickas, 2007) To that point, when neck and back pain are not treated right away, it can lead to correlating pain symptoms that can lead to a life of disability. Since the spine has multiple structures, from the neck to the lower back, when a person is in pain, it can lead to various pain generators that can cause some visceral pain. (Patel et al., 2015) Hence why, neck and back pain are multi-factorial and lead to numerous disorders.
When it comes to reducing neck and back pain from the body, many individuals will seek medical treatment to relieve themselves from the pain. However, many primary care doctors will assess their patients to determine what the root cause of their pain by taking notes of their daily routine. Many normal causes of neck and back pain can be due to:
Poor Posture
Stress
Physical Inactivity
Trauma/Injuries
Excessive sitting/standing
Lifting/carrying heavy objects
These causes can lead to a life of disability and affect a person’s quality of life; however, luckily, many individuals have researched and looked for treatment that is cost-effective and can help reduce the pain they are experiencing.
Understanding Academic Low Back Pain- Video
Do you feel aches and pains in your neck and back? Do you feel stress in your muscles that cause you to feel miserable? Or do you feel pain in your upper or lower body portions affecting your daily routine? Many of these scenarios correlate with neck and back pain, a common issue many individuals experience. If not treated right away, it can lead to a life of disability and, for working individuals, lose a day of work. However, many individuals seek cost-effective treatments that can help reduce the pain affecting their necks and back. Treatments like chiropractic care, traction therapy, massage therapy, and spinal decompression are all non-surgical, affordable, and can help reduce pain-like symptoms associated with neck and back pain. The video above explains the causes of academic low back pain and how non-surgical treatments like chiropractic care can work with additional therapies to prevent back and neck pain from returning. At the same time, when individuals begin to reduce their workload and educate themselves on what to do to avoid neck and back pain from returning, they can start feeling better. (Tyrdal et al., 2022)
The Effects Of Decompression On Neck & Back Pain
As part of the non-surgical treatments, spinal decompression can help many individuals dealing with neck and back pain. What spinal decompression does is incorporate gentle traction on the spine to decompress the affected spinal disc that can be associated with neck and back pain. When the spine is being treated with spinal decompression, the gravitational traction pull helps produce a greater disc space on the spine to decrease intradiscal pressure and pain. (Vanti et al., 2021) This allows all the nutrients and fluids to return to the spine and spinal discs while promoting the body’s natural healing process.
Additionally, many individuals with neck and back pain will begin to notice a huge reduction in their pain and disability through consecutive treatment. (Vanti et al., 2023) By incorporating healthy habits to reduce the chances of neck and back pain from returning, many individuals can make small changes to their daily routine. This allows them to have a positive outlook and continue their health and wellness journey.
References
Corwell, B. N., & Davis, N. L. (2020). The Emergent Evaluation and Treatment of Neck and Back Pain. Emerg Med Clin North Am, 38(1), 167-191. https://doi.org/10.1016/j.emc.2019.09.007
Patel, V. B., Wasserman, R., & Imani, F. (2015). Interventional Therapies for Chronic Low Back Pain: A Focused Review (Efficacy and Outcomes). Anesth Pain Med, 5(4), e29716. https://doi.org/10.5812/aapm.29716
Tyrdal, M. K., Veierod, M. B., Roe, C., Natvig, B., Wahl, A. K., & Stendal Robinson, H. (2022). Neck and back pain: Differences between patients treated in primary and specialist health care. J Rehabil Med, 54, jrm00300. https://doi.org/10.2340/jrm.v54.363
Vanti, C., Saccardo, K., Panizzolo, A., Turone, L., Guccione, A. A., & Pillastrini, P. (2023). The effects of the addition of mechanical traction to physical therapy on low back pain? A systematic review with meta-analysis. Acta Orthop Traumatol Turc, 57(1), 3-16. https://doi.org/10.5152/j.aott.2023.21323
Vanti, C., Turone, L., Panizzolo, A., Guccione, A. A., Bertozzi, L., & Pillastrini, P. (2021). Vertical traction for lumbar radiculopathy: a systematic review. Arch Physiother, 11(1), 7. https://doi.org/10.1186/s40945-021-00102-5
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine